
Changes in Metabolomic Profiles Induced by Switching from an Erythropoiesis-Stimulating Agent to a Hypoxia-Inducible Factor Prolyl Hydroxylase Inhibitor in Hemodialysis Patients: A Pilot Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
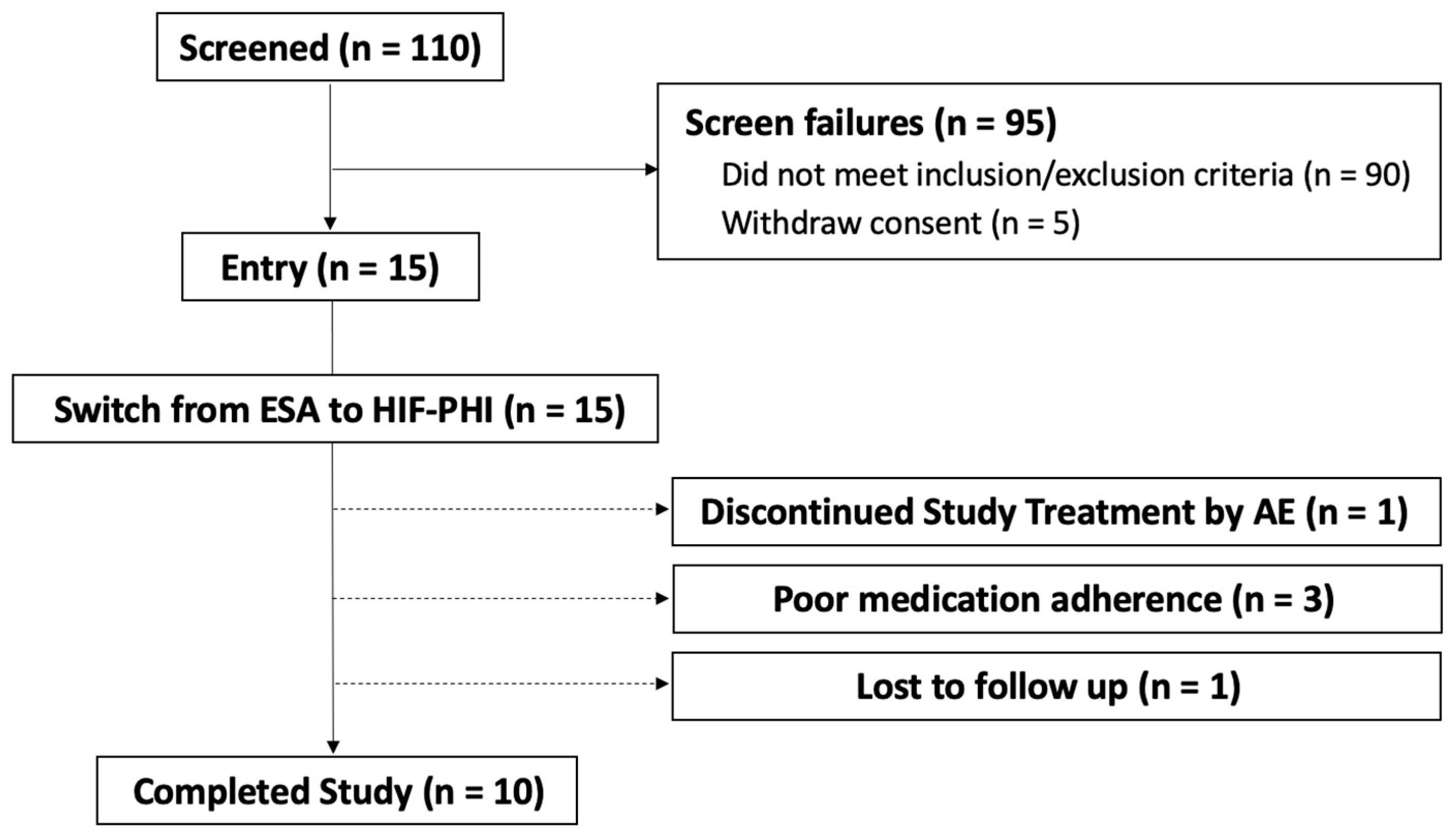
2.1. Patient Disposition and Characteristics
2.2. Changes in Parameters Following Switching from an ESA to an HIF-PHI
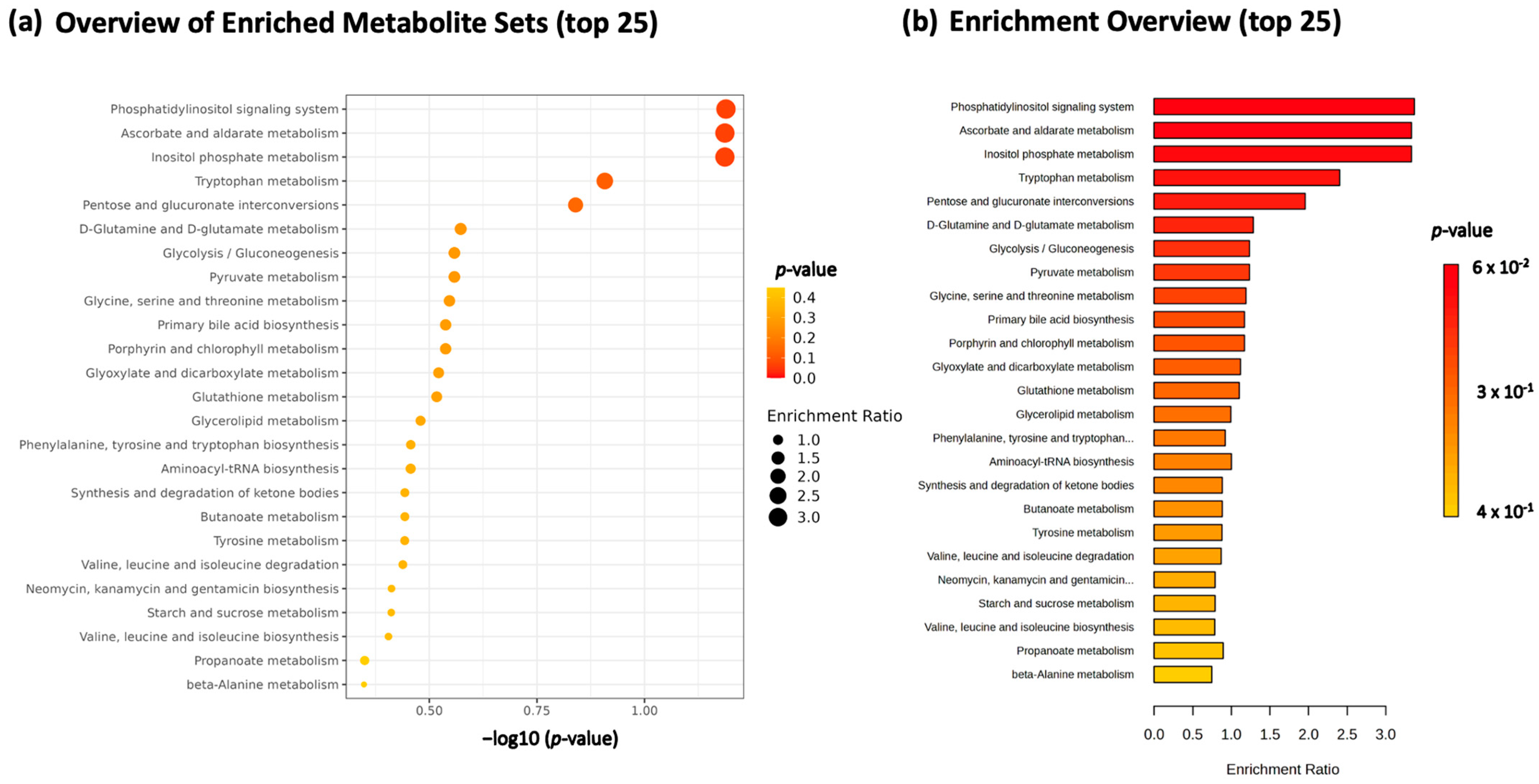
2.3. Overall Metabolomic Analysis of Serum Samples
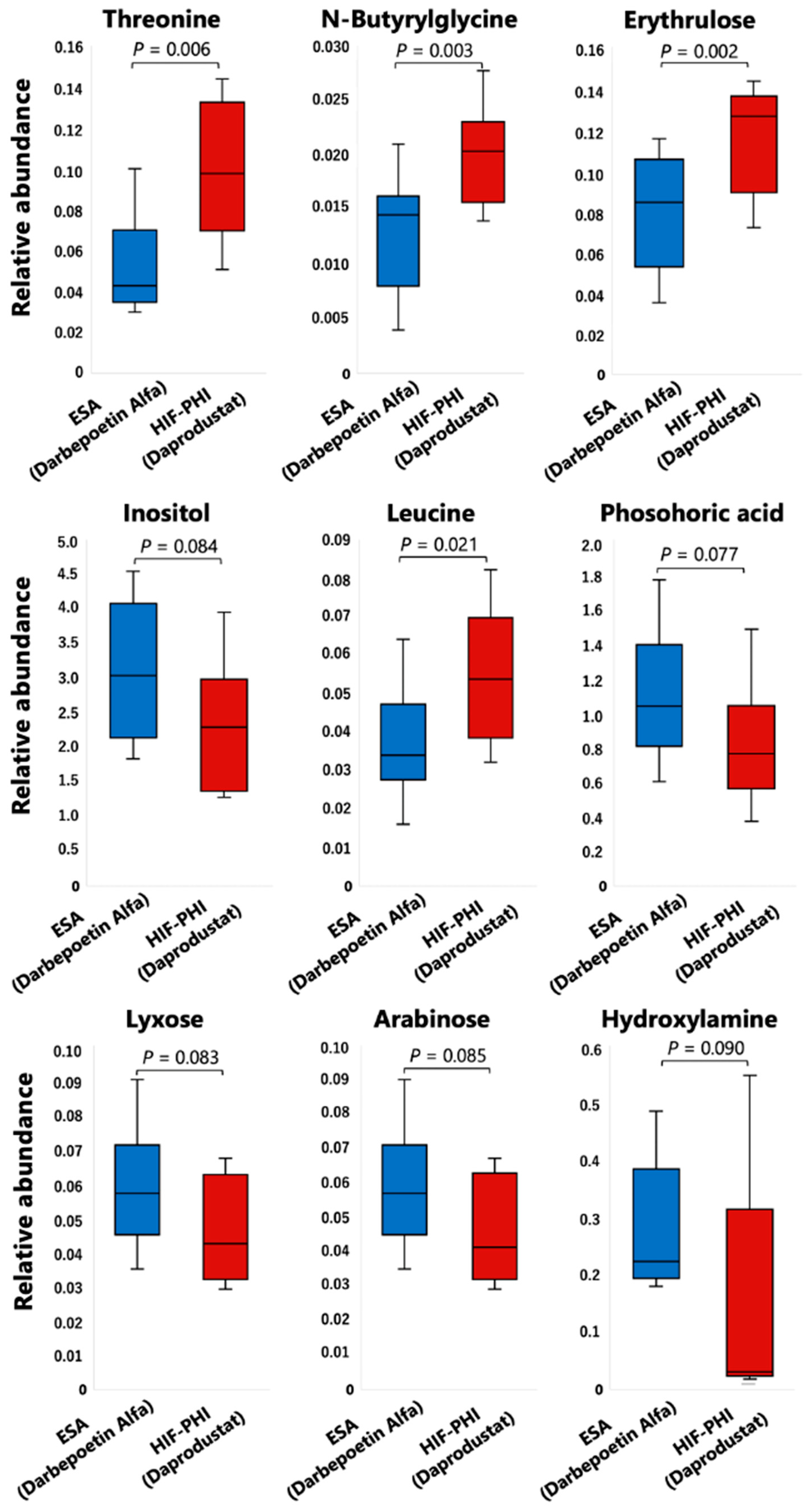
2.4. Specific Compounds Whose Levels Are Potentiated by an HIF-PHI and Are Detected by Comprehensive Metabolomic Analysis
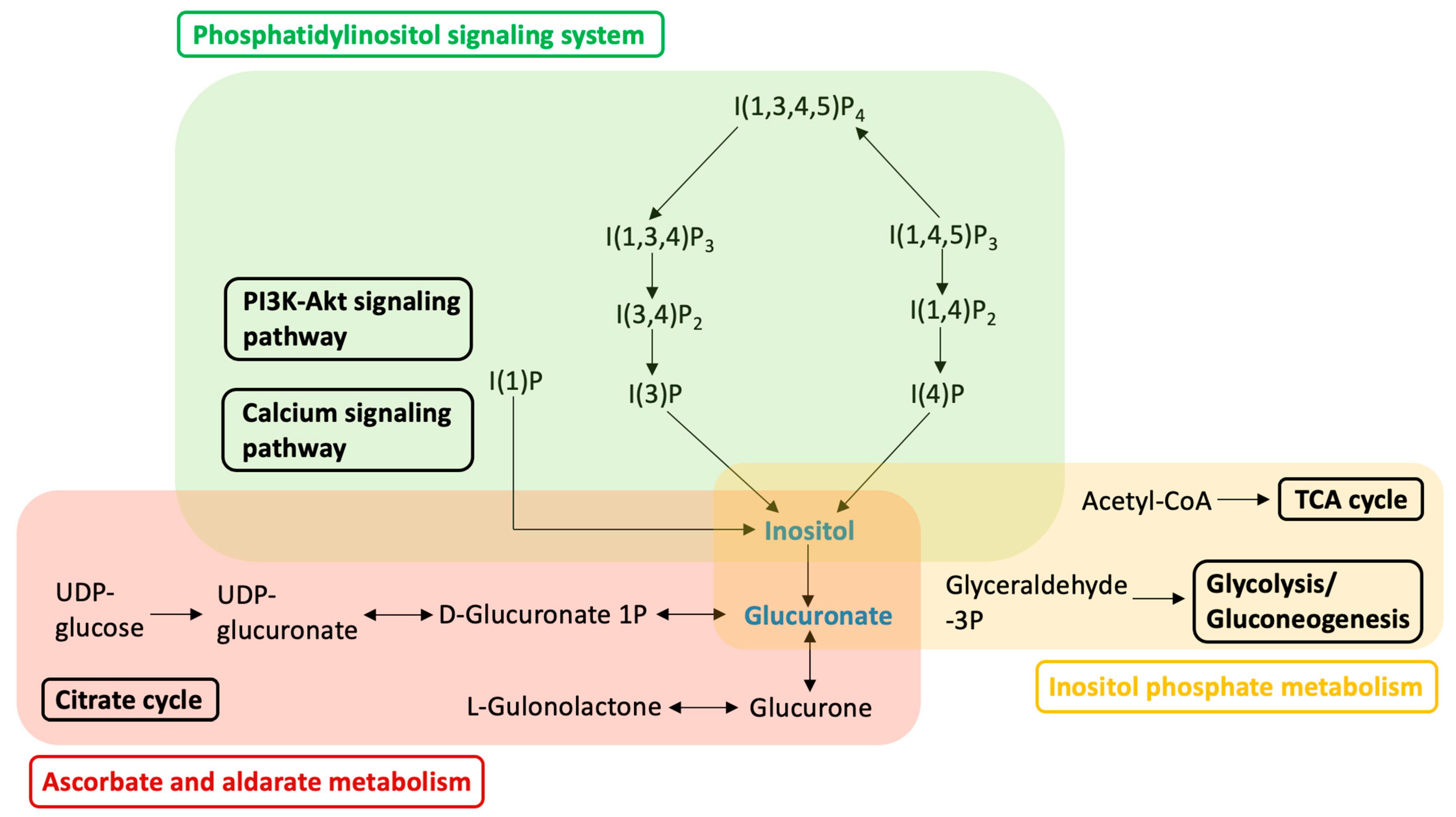
3. Discussion
4. Materials and Methods
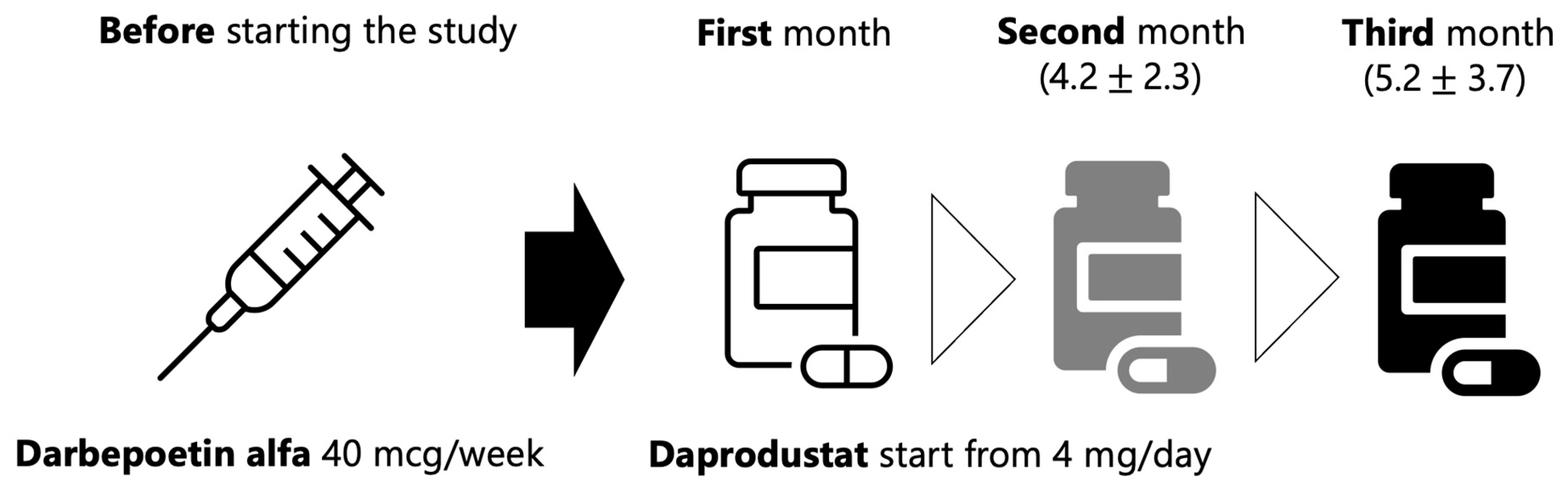
4.1. Study Design
4.2. Sample Preparation for GC-MS Measurements
4.3. GC-MS/MS Measurements
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haase, V.H. Hypoxia-inducible factor-prolyl hydroxylase inhibitors in the treatment of anemia of chronic kidney disease. Kidney Int. Suppl. 2021, 11, 8–25. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Cizman, B.; Carroll, K.; McMurray, J.J.V.; Perkovic, V.; Jha, V.; Johansen, K.L.; Lopes, R.D.; Macdougall, I.C.; Obrador, G.T.; et al. Efficacy and Safety of Daprodustat for Treatment of Anemia of Chronic Kidney Disease in Incident Dialysis Patients: A Randomized Clinical Trial. JAMA Intern. Med. 2022, 182, 592–602. [Google Scholar] [CrossRef]
- Fishbane, S.; Pollock, C.A.; El-Shahawy, M.; Escudero, E.T.; Rastogi, A.; Van, B.P.; Frison, L.; Houser, M.; Pola, M.; Little, D.J.; et al. Roxadustat Versus Epoetin Alfa for Treating Anemia in Patients with Chronic Kidney Disease on Dialysis: Results from the Randomized Phase 3 ROCKIES Study. J. Am. Soc. Nephrol. 2022, 33, 850–866. [Google Scholar] [CrossRef] [PubMed]
- Coyne, D.W.; Singh, A.K.; Lopes, R.D.; Bailey, C.K.; DiMino, T.L.; Huang, C.; Connaire, J.; Rastogi, A.; Kim, S.G.; Orias, M.; et al. Three Times Weekly Dosing of Daprodustat versus Conventional Epoetin for Treatment of Anemia in Hemodialysis Patients: ASCEND-TD: A Phase 3 Randomized, Double-Blind, Noninferiority Trial. Clin. J. Am. Soc. Nephrol. 2022, 17, 1325–1336. [Google Scholar] [CrossRef]
- Singh, A.K.; Carroll, K.; McMurray, J.J.V.; Solomon, S.; Jha, V.; Johansen, K.L.; Lopes, R.D.; Macdougall, I.C.; Obrador, G.T.; Waikar, S.S.; et al. Daprodustat for the Treatment of Anemia in Patients Not Undergoing Dialysis. N. Engl. J. Med. 2021, 385, 2313–2324. [Google Scholar] [CrossRef]
- Barratt, J.; Andric, B.; Tataradze, A.; Schomig, M.; Reusch, M.; Valluri, U.; Mariat, C. Roxadustat for the treatment of anaemia in chronic kidney disease patients not on dialysis: A Phase 3, randomized, open-label, active-controlled study (DOLOMITES). Nephrol. Dial. Transpl. 2021, 36, 1616–1628. [Google Scholar] [CrossRef]
- Fishbane, S.; El-Shahawy, M.A.; Pecoits-Filho, R.; Van, B.P.; Houser, M.T.; Frison, L.; Little, D.J.; Guzman, N.J.; Pergola, P.E. Roxadustat for Treating Anemia in Patients with CKD Not on Dialysis: Results from a Randomized Phase 3 Study. J. Am. Soc. Nephrol. 2021, 32, 737–755. [Google Scholar] [CrossRef]
- Eckardt, K.U.; Agarwal, R.; Aswad, A.; Awad, A.; Block, G.A.; Bacci, M.R.; Farag, Y.M.K.; Fishbane, S.; Hubert, H.; Jardine, A.; et al. Safety and Efficacy of Vadadustat for Anemia in Patients Undergoing Dialysis. N. Engl. J. Med. 2021, 384, 1601–1612. [Google Scholar] [CrossRef]
- Shutov, E.; Sulowicz, W.; Esposito, C.; Tataradze, A.; Andric, B.; Reusch, M.; Valluri, U.; Dimkovic, N. Roxadustat for the treatment of anemia in chronic kidney disease patients not on dialysis: A Phase 3, randomized, double-blind, placebo-controlled study (ALPS). Nephrol. Dial. Transpl. 2021, 36, 1629–1639. [Google Scholar] [CrossRef]
- Nangaku, M.; Kondo, K.; Ueta, K.; Kokado, Y.; Kaneko, G.; Matsuda, H.; Kawaguchi, Y.; Komatsu, Y. Efficacy and safety of vadadustat compared with darbepoetin alfa in Japanese anemic patients on hemodialysis: A Phase 3, multicenter, randomized, double-blind study. Nephrol. Dial. Transpl. 2021, 36, 1731–1741. [Google Scholar] [CrossRef]
- Akizawa, T.; Nangaku, M.; Yonekawa, T.; Okuda, N.; Kawamatsu, S.; Onoue, T.; Endo, Y.; Hara, K.; Cobitz, A.R. Efficacy and Safety of Daprodustat Compared with Darbepoetin Alfa in Japanese Hemodialysis Patients with Anemia: A Randomized, Double-Blind, Phase 3 Trial. Clin. J. Am. Soc. Nephrol. 2020, 15, 1155–1165. [Google Scholar] [CrossRef]
- Akizawa, T.; Iwasaki, M.; Yamaguchi, Y.; Majikawa, Y.; Reusch, M. Phase 3, Randomized, Double-Blind, Active-Comparator (Darbepoetin Alfa) Study of Oral Roxadustat in CKD Patients with Anemia on Hemodialysis in Japan. J. Am. Soc. Nephrol. 2020, 31, 1628–1639. [Google Scholar] [CrossRef]
- Chen, N.; Hao, C.; Liu, B.C.; Lin, H.; Wang, C.; Xing, C.; Liang, X.; Jiang, G.; Liu, Z.; Li, X.; et al. Roxadustat Treatment for Anemia in Patients Undergoing Long-Term Dialysis. N. Engl. J. Med. 2019, 381, 1011–1022. [Google Scholar] [CrossRef]
- Semenza, G.L. Oxygen sensing, homeostasis, and disease. N. Engl. J. Med. 2011, 365, 537–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, G.L.; Semenza, G.L. General involvement of hypoxia-inducible factor 1 in transcriptional response to hypoxia. Proc. Natl. Acad. Sci. USA 1993, 90, 4304–4308. [Google Scholar] [CrossRef]
- Maxwell, P.H.; Pugh, C.W.; Ratcliffe, P.J. Inducible operation of the erythropoietin 3’ enhancer in multiple cell lines: Evidence for a widespread oxygen-sensing mechanism. Proc. Natl. Acad. Sci. USA 1993, 90, 2423–2427. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.D.; Ebert, B.L.; Pugh, C.W.; Ratcliffe, P.J. Oxygen-regulated control elements in the phosphoglycerate kinase 1 and lactate dehydrogenase A genes: Similarities with the erythropoietin 3’ enhancer. Proc. Natl. Acad. Sci. USA 1994, 91, 6496–6500. [Google Scholar] [CrossRef] [PubMed]
- Levy, A.P.; Levy, N.S.; Wegner, S.; Goldberg, M.A. Transcriptional regulation of the rat vascular endothelial growth factor gene by hypoxia. J. Biol. Chem. 1995, 270, 13333–13340. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, K.; Sato, E.; Mishima, E.; Miyazaki, M.; Tanaka, T. What’s New in the Molecular Mechanisms of Diabetic Kidney Disease: Recent Advances. Int. J. Mol. Sci. 2022, 24, 570. [Google Scholar] [CrossRef]
- Kiani, A.K.; Paolacci, S.; Calogero, A.E.; Cannarella, R.; Di Renzo, G.C.; Gerli, S.; Della Morte, C.; Busetto, G.M.; De Berardinis, E.; Del Giudice, F.; et al. From Myo-inositol to D-chiro-inositol molecular pathways. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 2390–2402. [Google Scholar]
- Li, S.A.; Jiang, W.D.; Feng, L.; Liu, Y.; Wu, P.; Jiang, J.; Kuang, S.Y.; Tang, L.; Tang, W.N.; Zhang, Y.A.; et al. Dietary myo-inositol deficiency decreased intestinal immune function related to NF-kappaB and TOR signaling in the intestine of young grass carp (Ctenopharyngodon idella). Fish Shellfish Immunol. 2018, 76, 333–346. [Google Scholar] [CrossRef] [PubMed]
- Bizzarri, M.; Fuso, A.; Dinicola, S.; Cucina, A.; Bevilacqua, A. Pharmacodynamics and pharmacokinetics of inositol(s) in health and disease. Expert Opin. Drug Metab. Toxicol. 2016, 12, 1181–1196. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.A.; Nagalakshmi, D.; Raju, M.; Rama Rao, S.V.; Bedford, M.R. Effect of phytase superdosing, myo-inositol and available phosphorus concentrations on performance and bone mineralisation in broilers. Anim. Nutr. 2017, 3, 247–251. [Google Scholar] [CrossRef]
- Farhadi, D.; Karimi, A.; Sadeghi, G.; Rostamzadeh, J.; Bedford, M.R. Effects of a high dose of microbial phytase and myo-inositol supplementation on growth performance, tibia mineralization, nutrient digestibility, litter moisture content, and foot problems in broiler chickens fed phosphorus-deficient diets. Poult. Sci. 2017, 96, 3664–3675. [Google Scholar] [CrossRef]
- Di Daniel, E.; Kew, J.N.; Maycox, P.R. Investigation of the H+-myo-inositol transporter (HMIT) as a neuronal regulator of phosphoinositide signalling. Biochem. Soc. Trans. 2009, 37 Pt 5, 1139–1143. [Google Scholar] [CrossRef] [Green Version]
- Kanehisa, M.; Sato, Y.; Furumichi, M.; Morishima, K.; Tanabe, M. New approach for understanding genome variations in KEGG. Nucleic Acids Res. 2019, 47, D590–D595. [Google Scholar] [CrossRef] [Green Version]
- Di Daniel, E.; Mok, M.H.; Mead, E.; Mutinelli, C.; Zambello, E.; Caberlotto, L.L.; Pell, T.J.; Langmead, C.J.; Shah, A.J.; Duddy, G.; et al. Evaluation of expression and function of the H+/myo-inositol transporter HMIT. BMC Cell Biol. 2009, 10, 54. [Google Scholar] [CrossRef] [Green Version]
- Posor, Y.; Jang, W.; Haucke, V. Phosphoinositides as membrane organizers. Nat. Rev. Mol. Cell Biol. 2022, 23, 797–816. [Google Scholar] [CrossRef] [PubMed]
- Bilanges, B.; Posor, Y.; Vanhaesebroeck, B. PI3K isoforms in cell signalling and vesicle trafficking. Nat. Rev. Mol. Cell Biol. 2019, 20, 515–534. [Google Scholar] [CrossRef]
- Goncalves, M.D.; Hopkins, B.D.; Cantley, L.C. Phosphatidylinositol 3-Kinase, Growth Disorders, and Cancer. N. Engl. J. Med. 2018, 379, 2052–2062. [Google Scholar] [CrossRef]
- Li, C.; Chen, N.; Zhang, X.; Shahzad, K.; Qi, R.; Zhang, Z.; Lu, Z.; Lu, Y.; Yu, X.; Zafar, M.H.; et al. Mixed silage with Chinese cabbage waste enhances antioxidant ability by increasing ascorbate and aldarate metabolism through rumen Prevotellaceae UCG-004 in Hu sheep. Front. Microbiol. 2022, 13, 978940. [Google Scholar] [CrossRef] [PubMed]
- Chatree, S.; Thongmaen, N.; Tantivejkul, K.; Sitticharoon, C.; Vucenik, I. Role of Inositols and Inositol Phosphates in Energy Metabolism. Molecules 2020, 25, 5079. [Google Scholar] [CrossRef] [PubMed]
- Spoto, B.; Pisano, A.; Zoccali, C. Insulin resistance in chronic kidney disease: A systematic review. Am. J. Physiol. Renal Physiol. 2016, 311, F1087–F1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navaneethan, S.D.; Kirwan, J.P.; Remer, E.M.; Schneider, E.; Addeman, B.; Arrigain, S.; Horwitz, E.; Fink, J.C.; Lash, J.P.; McKenzie, C.A.; et al. Adiposity, Physical Function, and Their Associations With Insulin Resistance, Inflammation, and Adipokines in CKD. Am. J. Kidney Dis. 2021, 77, 44–55. [Google Scholar] [CrossRef]
- Leyking, S.; Fliser, D. Insulin resistance in CKD. Clin. J. Am. Soc. Nephrol. 2014, 9, 638–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar]
- In, J. Introduction of a pilot study. Korean J. Anesthesiol. 2017, 70, 601–605. [Google Scholar] [CrossRef] [Green Version]
- Lancaster, G.A.; Dodd, S.; Williamson, P.R. Design and analysis of pilot studies: Recommendations for good practice. J. Eval. Clin. Pract. 2004, 10, 307–312. [Google Scholar]
- Sugahara, M.; Tanaka, T.; Nangaku, M. Future perspectives of anemia management in chronic kidney disease using hypoxia-inducible factor-prolyl hydroxylase inhibitors. Pharmacol. Ther. 2022, 239, 108272. [Google Scholar] [CrossRef]
- Singh, A.K.; Carroll, K.; Perkovic, V.; Solomon, S.; Jha, V.; Johansen, K.L.; Lopes, R.D.; Macdougall, I.C.; Obrador, G.T.; Waikar, S.S.; et al. Daprodustat for the Treatment of Anemia in Patients Undergoing Dialysis. N. Engl. J. Med. 2021, 385, 2325–2335. [Google Scholar] [CrossRef] [PubMed]
- Nangaku, M.; Hamano, T.; Akizawa, T.; Tsubakihara, Y.; Nagai, R.; Okuda, N.; Kurata, K.; Nagakubo, T.; Jones, N.P.; Endo, Y.; et al. Daprodustat Compared with Epoetin Beta Pegol for Anemia in Japanese Patients Not on Dialysis: A 52-Week Randomized Open-Label Phase 3 Trial. Am. J. Nephrol. 2021, 52, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Kumakura, S.; Sato, E.; Sekimoto, A.; Hashizume, Y.; Yamakage, S.; Miyazaki, M.; Ito, S.; Harigae, H.; Takahashi, N. Nicotinamide Attenuates the Progression of Renal Failure in a Mouse Model of Adenine-Induced Chronic Kidney Disease. Toxins 2021, 13, 50. [Google Scholar] [CrossRef]
- Nishiumi, S.; Kobayashi, T.; Kawana, S.; Unno, Y.; Sakai, T.; Okamoto, K.; Yamada, Y.; Sudo, K.; Yamaji, T.; Saito, Y.; et al. Investigations in the possibility of early detection of colorectal cancer by gas chromatography/triple-quadrupole mass spectrometry. Oncotarget 2017, 8, 17115–17126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishiumi, S.; Kobayashi, T.; Ikeda, A.; Yoshie, T.; Kibi, M.; Izumi, Y.; Okuno, T.; Hayashi, N.; Kawano, S.; Takenawa, T.; et al. A novel serum metabolomics-based diagnostic approach for colorectal cancer. PLoS ONE 2012, 7, e40459. [Google Scholar] [CrossRef]
- Bae, J.E.; Min, D.; Choi, J.Y.; Choi, H.; Kim, J.B.; Park, N.Y.; Jo, D.S.; Kim, Y.H.; Na, H.W.; Kim, Y.J.; et al. Primary Ciliogenesis by 2-Isopropylmalic Acid Prevents PM2.5-Induced Inflammatory Response and MMP-1 Activation in Human Dermal Fibroblasts and a 3-D-Skin Model. Int. J. Mol. Sci. 2021, 22, 10941. [Google Scholar] [CrossRef]
- Malla, M.A.; Dubey, A.; Kori, R.K.; Sharma, V.; Kumar, A.; Yadav, S.; Kumari, S. GC-MS based untargeted metabolomics reveals the metabolic response of earthworm (Eudrilus eugeniae) after chronic combinatorial exposure to three different pesticides. Sci. Rep. 2023, 13, 8583. [Google Scholar] [CrossRef]
- Kanani, H.; Chrysanthopoulos, P.K.; Klapa, M.I. Standardizing GC-MS metabolomics. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2008, 871, 191–201. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n = 10 |
|---|---|
| Age, year | 65.6 (11.3) |
| Men, n (%) | 9 (90) |
| Race, n (%) | |
| Asian | 10 (100) |
| Dialysis modality, n (%) | |
| Hemodialysis | 10 (100) |
| Hemodiafiltration/hemofiltration | 0 (0) |
| Dialysis vintage, year, n (%) | 5.1 (4.4) |
| Postdialysis weight, kg | 69.4 (15.4) |
| Postdialysis BP, mmHg | |
| Systolic BP | 157.6 (20.3) |
| Diastolic BP | 79.9 (11.4) |
| Prior ESA dose, darbepoetin alfa, mcg/w | 41.0 (26.8) |
| Iron use, n (%) | |
| Intravenous iron | 6 (60.0) |
| Oral only | 4 (40.0) |
| No iron therapy | 0 (0.0) |
| Hemoglobin, g/dL | 11.1 (1.2) |
| Ferritin, ng/mL | 117.1 (117.6) |
| Serum iron, mcg/dL | 73.5 (24.1) |
| TIBC, mcg/dL | 270.4 (42.0) |
| Transferrin saturation, % | 28.5 (10.8) |
| Serum albumin, g/dL | 3.7 (0.2) |
| Plasma glucose, mg/dL | 116.4 (23.2) |
| LDL cholesterol, mg/dL | 73.1 (15.0) |
| Triglyceride, mg/dL | 80.3 (33.0) |
| CRP, mg/dL | 0.13 (0.17) |
| History of cardiovascular disease, n (%) | 3 (30.0) |
| History of stroke, n (%) | 1 (10.0) |
| History of myocardial infarction, n (%) | 1 (10.0) |
| History of heart failure, n (%) | 1 (10.0) |
| History of thromboembolic events, n (%) | 0 (0.0) |
| Smoking history, n (%) | |
| Never smoked | 7 (70.0) |
| Current smoker | 3 (30.0) |
| Former smoker | 0 (0.0) |
| Statin use at entry, n (%) | 6 (60.0) |
| Aspirin use at entry, n (%) | 3 (30.0) |
| Vitamin K antagonist use at entry, n (%) | 0 (0.0) |
| History of diabetes, n (%) | 6 (60.0) |
| Characteristic | Before (n = 10) | After (n = 10) | p Value |
|---|---|---|---|
| Postdialysis weight, kg | 69.4 (15.4) | 68.0 (15.2) | 0.168 |
| Postdialysis BP, mmHg | |||
| Systolic BP | 157.6 (20.3) | 143.0 (19.0) | 0.086 |
| Diastolic BP | 79.9 (11.4) | 81.1 (15.2) | 0.680 |
| Iron use, n (%) | |||
| Intravenous iron | 6 (60.0) | 0 (0.0) | |
| Oral only | 4 (40.0) | 4 (40.0) | |
| No iron therapy | 0 (0.0) | 6 (60.0) | |
| Hemoglobin, g/dL | 11.1 (1.2) | 9.8 (1.3) | 0.086 |
| Ferritin, ng/mL | 117.1 (117.6) | 152.8 (111.2) | 0.500 |
| Serum iron, mcg/dL | 73.5 (24.1) | 85.4 (24.6) | 0.110 |
| TIBC, mcg/dL | 270.4 (42.0) | 267.5 (40.4) | 0.856 |
| Transferrin saturation, % | 28.5 (10.8) | 32.5 (11.3) | 0.308 |
| Serum albumin, g/dL | 3.7 (0.2) | 3.6 (0.2) | 0.159 |
| Plasma glucose, mg/dL | 116.4 (23.2) | 121.2 (34.3) | 0.603 |
| LDL cholesterol, mg/dL | 73.1 (15.0) | 69.5 (21.1) | 0.649 |
| Triglyceride, mg/dL | 80.3 (33.0) | 91.9 (53.3) | 0.338 |
| CRP, mg/dL | 0.13 (0.17) | 0.21 (0.29) | 0.345 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watanabe, K.; Sato, E.; Mishima, E.; Moriya, S.; Sakabe, T.; Sato, A.; Fujiwara, M.; Fujimaru, T.; Ito, Y.; Taki, F.; et al. Changes in Metabolomic Profiles Induced by Switching from an Erythropoiesis-Stimulating Agent to a Hypoxia-Inducible Factor Prolyl Hydroxylase Inhibitor in Hemodialysis Patients: A Pilot Study. Int. J. Mol. Sci. 2023, 24, 12752. https://doi.org/10.3390/ijms241612752
Watanabe K, Sato E, Mishima E, Moriya S, Sakabe T, Sato A, Fujiwara M, Fujimaru T, Ito Y, Taki F, et al. Changes in Metabolomic Profiles Induced by Switching from an Erythropoiesis-Stimulating Agent to a Hypoxia-Inducible Factor Prolyl Hydroxylase Inhibitor in Hemodialysis Patients: A Pilot Study. International Journal of Molecular Sciences. 2023; 24(16):12752. https://doi.org/10.3390/ijms241612752
Chicago/Turabian StyleWatanabe, Kimio, Emiko Sato, Eikan Mishima, Shinobu Moriya, Takuma Sakabe, Atsuya Sato, Momoko Fujiwara, Takuya Fujimaru, Yugo Ito, Fumika Taki, and et al. 2023. "Changes in Metabolomic Profiles Induced by Switching from an Erythropoiesis-Stimulating Agent to a Hypoxia-Inducible Factor Prolyl Hydroxylase Inhibitor in Hemodialysis Patients: A Pilot Study" International Journal of Molecular Sciences 24, no. 16: 12752. https://doi.org/10.3390/ijms241612752
APA StyleWatanabe, K., Sato, E., Mishima, E., Moriya, S., Sakabe, T., Sato, A., Fujiwara, M., Fujimaru, T., Ito, Y., Taki, F., Nagahama, M., Tanaka, K., Kazama, J. J., & Nakayama, M. (2023). Changes in Metabolomic Profiles Induced by Switching from an Erythropoiesis-Stimulating Agent to a Hypoxia-Inducible Factor Prolyl Hydroxylase Inhibitor in Hemodialysis Patients: A Pilot Study. International Journal of Molecular Sciences, 24(16), 12752. https://doi.org/10.3390/ijms241612752