
In the Search for Biomarkers of Pulmonary Arterial Hypertension, Are Cytokines IL-2, IL-4, IL-6, IL-10, and IFN-Gamma the Right Indicators to Use?

 , , , , , , and
, , , , , , and 
Abstract
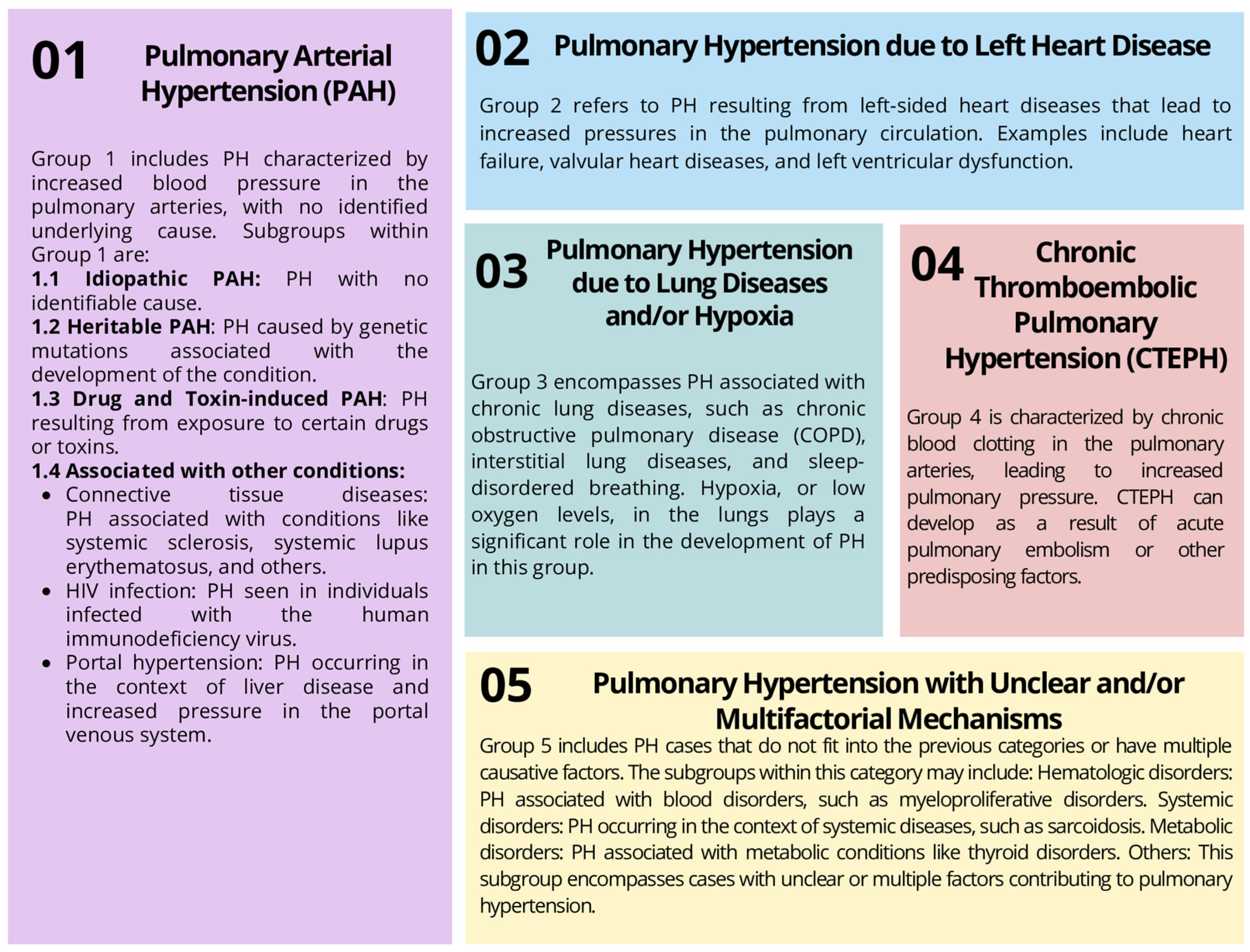
:1. Introduction
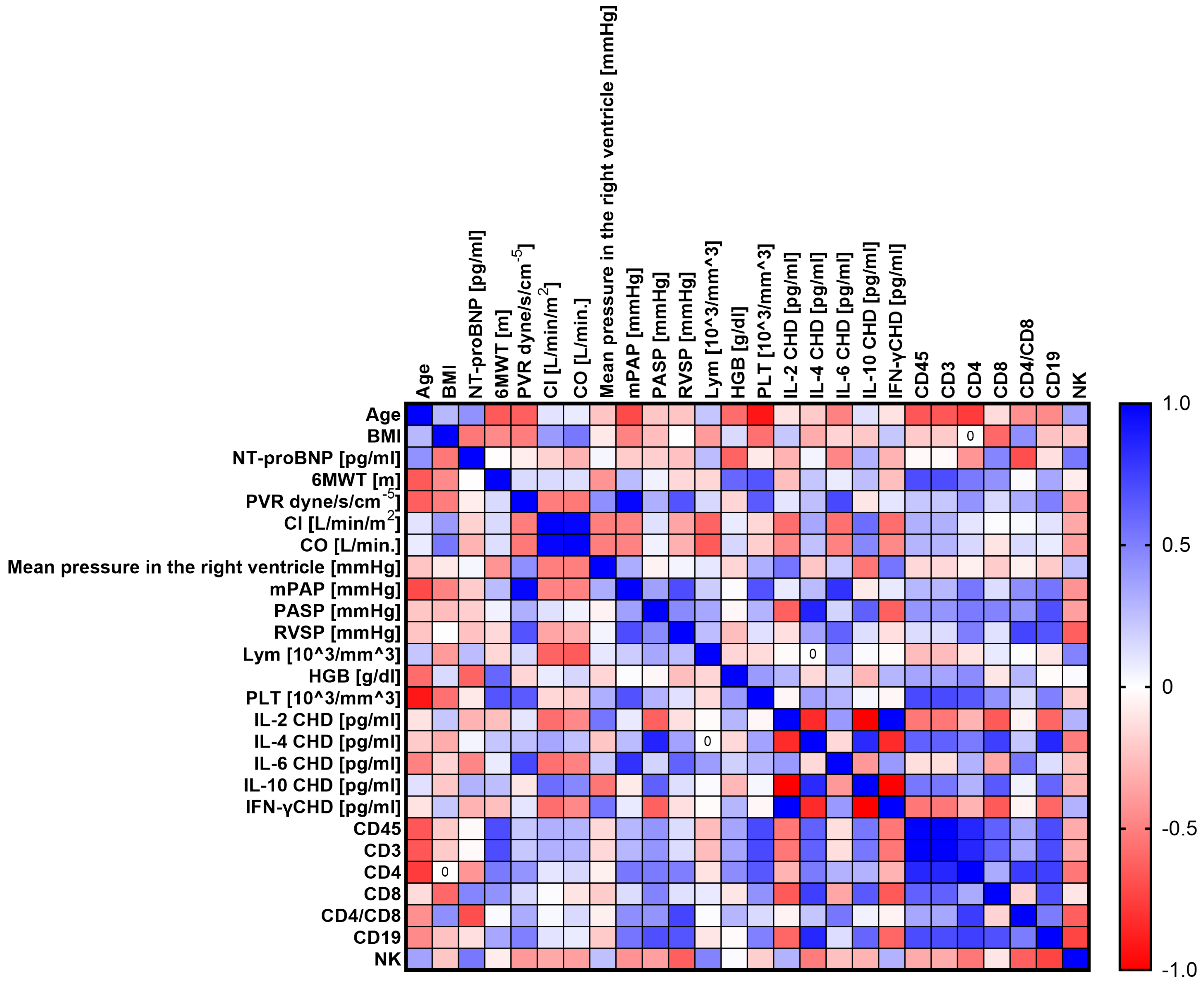
2. Results
3. Discussion
3.1. IL-6
3.2. IL-2
3.3. IL-10
3.4. IL-4
3.5. IFN-Gamma
4. Materials and Methods
4.1. Examined Patients and the Control Group Characteristics
4.2. Tested Material: Assessment of Peripheral Blood Immunophenotype and Plasma Interleukin Concentration
- Human IFN-gamma Platinum ELISA, sensitivity = 0.99 pg/mL (eBioscience, San Diego, CA, USA);
- Human IL-2 Quantikine ELISA Kit, sensitivity = 0.066 pg/mL (R&D Systems, Minneapolis, MN, USA);
- Human IL-4 Quantikine ELISA Kit, sensitivity = 0.22 pg/mL (R&D Systems, USA);
- Human IL-10 Quantikine ELISA Kit, sensitivity = 0.17 pg/mL (R&D Systems, USA);
- Human IL-6 Quantikine ELISA Kit, sensitivity = 0.11 pg/mL (R&D Systems, USA).
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Humbert, M. Treatment of Pulmonary Arterial Hypertension. N. Engl. J. Med. 2004, 351, 1425–1436. [Google Scholar] [CrossRef]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension. Eur. Heart J. 2022, 43, 3618–3731. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.M.; Chen, H.; Halpern, S.; Taichman, D.; McGoon, M.D.; Farber, H.W.; Frost, A.E.; Liou, T.G.; Turner, M.; Feldkircher, K.; et al. Delay in Recognition of Pulmonary Arterial Hypertension: Factors Identified from the REVEAL Registry. Chest 2011, 140, 19–26. [Google Scholar] [CrossRef]
- Tomaszewski, M.; Małkowska, P.; Sierawska, O.; Hrynkiewicz, R.; Mroczek, E.; Darocha, S.; Hymos, A.; Błaszczak, P.; Grywalska, E.; Niedźwiedzka-Rystwej, P. CTLA-4 Expression Is a Promising Biomarker of Idiopathic Pulmonary Arterial Hypertension and Allows Differentiation of the Type of Pulmonary Hypertension. Int. J. Mol. Sci. 2022, 23, 15910. [Google Scholar] [CrossRef] [PubMed]
- Koudstaal, T.; van Uden, D.; van Hulst, J.A.C.; Heukels, P.; Bergen, I.M.; Geenen, L.W.; Baggen, V.J.M.; van den Bosch, A.E.; van den Toorn, L.M.; Chandoesing, P.P.; et al. Plasma Markers in Pulmonary Hypertension Subgroups Correlate with Patient Survival. Respir. Res. 2021, 22, 137. [Google Scholar] [CrossRef] [PubMed]
- Thenappan, T.; Ormiston, M.L.; Ryan, J.J.; Archer, S.L. Pulmonary Arterial Hypertension: Pathogenesis and Clinical Management. BMJ 2018, 360, j5492. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.-M.; An, J. Cytokines, Inflammation and Pain. Int. Anesthesiol. Clin. 2007, 45, 27–37. [Google Scholar] [CrossRef]
- Kany, S.; Vollrath, J.T.; Relja, B. Cytokines in Inflammatory Disease. Int. J. Mol. Sci. 2019, 20, 6008. [Google Scholar] [CrossRef]
- Humbert, M.; Monti, G.; Brenot, F.; Sitbon, O.; Portier, A.; Grangeot-Keros, L.; Duroux, P.; Galanaud, P.; Simonneau, G.; Emilie, D. Increased Interleukin-1 and Interleukin-6 Serum Concentrations in Severe Primary Pulmonary Hypertension. Am. J. Respir. Crit. Care Med. 1995, 151, 1628–1631. [Google Scholar] [CrossRef]
- Steiner, M.K.; Syrkina, O.L.; Kolliputi, N.; Mark, E.J.; Hales, C.A.; Waxman, A.B. Interleukin-6 Overexpression Induces Pulmonary Hypertension. Circ. Res. 2009, 104, 236–244. [Google Scholar] [CrossRef]
- Soon, E.; Holmes, A.M.; Treacy, C.M.; Doughty, N.J.; Southgate, L.; Machado, R.D.; Trembath, R.C.; Jennings, S.; Barker, L.; Nicklin, P.; et al. Elevated Levels of Inflammatory Cytokines Predict Survival in Idiopathic and Familial Pulmonary Arterial Hypertension. Circulation 2010, 122, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Cracowski, J.-L.; Chabot, F.; Labarère, J.; Faure, P.; Degano, B.; Schwebel, C.; Chaouat, A.; Reynaud-Gaubert, M.; Cracowski, C.; Sitbon, O.; et al. Proinflammatory Cytokine Levels Are Linked to Death in Pulmonary Arterial Hypertension. Eur. Respir. J. 2014, 43, 915–917. [Google Scholar] [CrossRef]
- Tomaszewski, M.; Bębnowska, D.; Hrynkiewicz, R.; Dworzyński, J.; Niedźwiedzka-Rystwej, P.; Kopeć, G.; Grywalska, E. Role of the Immune System Elements in Pulmonary Arterial Hypertension. J. Clin. Med. 2021, 10, 3757. [Google Scholar] [CrossRef] [PubMed]
- Groth, A.; Vrugt, B.; Brock, M.; Speich, R.; Ulrich, S.; Huber, L.C. Inflammatory Cytokines in Pulmonary Hypertension. Respir. Res. 2014, 15, 47. [Google Scholar] [CrossRef] [PubMed]
- Prins, K.W.; Archer, S.L.; Pritzker, M.; Rose, L.; Weir, E.K.; Sharma, A.; Thenappan, T. Interleukin-6 Is Independently Associated with Right Ventricular Function in Pulmonary Arterial Hypertension. J. Heart Lung Transplant. 2018, 37, 376–384. [Google Scholar] [CrossRef]
- Jasiewicz, M.; Knapp, M.; Waszkiewicz, E.; Ptaszynska-Kopczynska, K.; Szpakowicz, A.; Sobkowicz, B.; Musial, W.J.; Kaminski, K.A. Enhanced IL-6 Trans-Signaling in Pulmonary Arterial Hypertension and Its Potential Role in Disease-Related Systemic Damage. Cytokine 2015, 76, 187–192. [Google Scholar] [CrossRef]
- Glauser, F.L.; DeBlois, G.G.; Bechard, D.E.; Merchant, R.E.; Grant, A.J.; Fowler, A.A.; Fairman, R.P. Cardiopulmonary Effects of Recombinant Interleukin-2 Infusion in Sheep. J. Appl. Physiol. 1988, 64, 1030–1037. [Google Scholar] [CrossRef]
- Shigematsu, T.; Miura, S.; Hirokawa, M.; Hokari, R.; Higuchi, H.; Watanabe, N.; Tsuzuki, Y.; Kimura, H.; Tada, S.; Nakatsumi, R.C.; et al. Induction of Endothelin-1 Synthesis by IL-2 and Its Modulation of Rat Intestinal Epithelial Cell Growth. Am. J. Physiol. 1998, 275, G556–G563. [Google Scholar] [CrossRef]
- Ferro, T.J.; Johnson, A.; Everitt, J.; Malik, A.B. IL-2 Induces Pulmonary Edema and Vasoconstriction Independent of Circulating Lymphocytes. J. Immunol. 1989, 142, 1916–1921. [Google Scholar] [CrossRef]
- Ito, T.; Ikeda, U. Inflammatory Cytokines and Cardiovascular Disease. Curr. Drug Targets Inflamm. Allergy 2003, 2, 257–265. [Google Scholar] [CrossRef]
- Ito, T.; Okada, T.; Miyashita, H.; Nomoto, T.; Nonaka-Sarukawa, M.; Uchibori, R.; Maeda, Y.; Urabe, M.; Mizukami, H.; Kume, A.; et al. Interleukin-10 Expression Mediated by an Adeno-Associated Virus Vector Prevents Monocrotaline-Induced Pulmonary Arterial Hypertension in Rats. Circ. Res. 2007, 101, 734–741. [Google Scholar] [CrossRef]
- Taraseviciene-Stewart, L.; Nicolls, M.R.; Kraskauskas, D.; Scerbavicius, R.; Burns, N.; Cool, C.; Wood, K.; Parr, J.E.; Boackle, S.A.; Voelkel, N.F. Absence of T Cells Confers Increased Pulmonary Arterial Hypertension and Vascular Remodeling. Am. J. Respir. Crit. Care Med. 2007, 175, 1280–1289. [Google Scholar] [CrossRef] [PubMed]
- Kurzyna, M.; Darocha, S.; Pietura, R.; Pietrasik, A.; Norwa, J.; Mańczak, R.; Wieteska, M.; Biederman, A.; Matsubara, H.; Torbicki, A. Changing the Strategy of Balloon Pulmonary Angioplasty Resulted in a Reduced Complication Rate in Patients with Chronic Thromboembolic Pulmonary Hypertension. A Single-Centre European Experience. Kardiol. Polska/Pol. Heart J. 2017, 75, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Yamaji-Kegan, K.; Su, Q.; Angelini, D.J.; Champion, H.C.; Johns, R.A. Hypoxia-Induced Mitogenic Factor Has Proangiogenic and Proinflammatory Effects in the Lung via VEGF and VEGF Receptor-2. Am. J. Physiol. Lung Cell Mol. Physiol. 2006, 291, L1159–L1168. [Google Scholar] [CrossRef] [PubMed]
- Angelini, D.J.; Su, Q.; Yamaji-Kegan, K.; Fan, C.; Skinner, J.T.; Poloczek, A.; El-Haddad, H.; Cheadle, C.; Johns, R.A. Hypoxia-Induced Mitogenic Factor (HIMF/FIZZ1/RELMα) in Chronic Hypoxia- and Antigen-Mediated Pulmonary Vascular Remodeling. Respir. Res. 2013, 14, 1. [Google Scholar] [CrossRef]
- Yamaji-Kegan, K.; Takimoto, E.; Zhang, A.; Weiner, N.C.; Meuchel, L.W.; Berger, A.E.; Cheadle, C.; Johns, R.A. Hypoxia-Induced Mitogenic Factor (FIZZ1/RELMα) Induces Endothelial Cell Apoptosis and Subsequent Interleukin-4-Dependent Pulmonary Hypertension. Am. J. Physiol. Lung Cell Mol. Physiol. 2014, 306, L1090–L1103. [Google Scholar] [CrossRef]
- Yi, M.-H.; Zhang, E.; Kang, J.W.; Shin, Y.N.; Byun, J.Y.; Oh, S.-H.; Seo, J.H.; Lee, Y.H.; Kim, D.W. Expression of CD200 in Alternative Activation of Microglia Following an Excitotoxic Lesion in the Mouse Hippocampus. Brain Res. 2012, 1481, 90–96. [Google Scholar] [CrossRef]
- Kojima, T.; Tsuchiya, K.; Ikemizu, S.; Yoshikawa, S.; Yamanishi, Y.; Watanabe, M.; Karasuyama, H. Novel CD200 Homologues ISEC1 and ISEC2 Are Gastrointestinal Secretory Cell-Specific Ligands of Inhibitory Receptor CD200R. Sci. Rep. 2016, 6, 36457. [Google Scholar] [CrossRef]
- Wright, G.J.; Cherwinski, H.; Foster-Cuevas, M.; Brooke, G.; Puklavec, M.J.; Bigler, M.; Song, Y.; Jenmalm, M.; Gorman, D.; McClanahan, T.; et al. Characterization of the CD200 Receptor Family in Mice and Humans and Their Interactions with CD200. J. Immunol. 2003, 171, 3034–3046. [Google Scholar] [CrossRef]
- Najar, M.; Raicevic, G.; Jebbawi, F.; De Bruyn, C.; Meuleman, N.; Bron, D.; Toungouz, M.; Lagneaux, L. Characterization and Functionality of the CD200-CD200R System during Mesenchymal Stromal Cell Interactions with T-Lymphocytes. Immunol. Lett. 2012, 146, 50–56. [Google Scholar] [CrossRef]
- Soberman, R.J.; MacKay, C.R.; Vaine, C.A.; Ryan, G.B.; Cerny, A.M.; Thompson, M.R.; Nikolic, B.; Primo, V.; Christmas, P.; Sheiffele, P.; et al. CD200R1 Supports HSV-1 Viral Replication and Licenses Pro-Inflammatory Signaling Functions of TLR2. PLoS ONE 2012, 7, e47740. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.; Hao, B.; Yang, X.F.; Chen, W.Q. Decreased CD200R Expression on Monocyte-Derived Macrophages Correlates with Th17/Treg Imbalance and Disease Activity in Rheumatoid Arthritis Patients. Inflamm. Res. 2014, 63, 441–450. [Google Scholar] [CrossRef]
- Van Uden, D.; Koudstaal, T.; van Hulst, J.A.C.; Vink, M.; van Nimwegen, M.; van den Toorn, L.M.; Chandoesing, P.P.; van den Bosch, A.E.; Kool, M.; Hendriks, R.W.; et al. Peripheral Blood T Cells of Patients with IPAH Have a Reduced Cytokine-Producing Capacity. Int. J. Mol. Sci. 2022, 23, 6508. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Cherwinski, H.; Sedgwick, J.D.; Phillips, J.H. Molecular Mechanisms of CD200 Inhibition of Mast Cell Activation. J. Immunol. 2004, 173, 6786–6793. [Google Scholar] [CrossRef] [PubMed]
- Walker, D.G.; Dalsing-Hernandez, J.E.; Campbell, N.A.; Lue, L.-F. Decreased Expression of CD200 and CD200 Receptor in Alzheimer’s Disease: A Potential Mechanism Leading to Chronic Inflammation. Exp. Neurol. 2009, 215, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Gołąb, J.; Jakóbisiak, M.; Lasek, W.; Stokłosa, T. Immunologia; Wydawnictwo Naukowe PWN: Daimlera, Poland, 2017. [Google Scholar]
- Hemmerich, M.; Malorny, N.; Lewen, A.; Hollnagel, J.-O.; Chausse, B.; Kann, O. Priming of Microglia by Type II Interferon Is Lasting and Resistant to Modulation by Interleukin-10 in Situ. J. Neuroimmunol. 2022, 368, 577881. [Google Scholar] [CrossRef]
- Dhillon, S.; Kaker, A.; Dosanjh, A.; Japra, D.; Vanthiel, D.H. Irreversible Pulmonary Hypertension Associated with the Use of Interferon Alpha for Chronic Hepatitis C. Dig. Dis. Sci. 2010, 55, 1785–1790. [Google Scholar] [CrossRef]
- Al-Zahrani, H.; Gupta, V.; Minden, M.D.; Messner, H.A.; Lipton, J.H. Vascular Events Associated with Alpha Interferon Therapy. Leuk. Lymphoma 2003, 44, 471–475. [Google Scholar] [CrossRef]
- Ledinek, A.H.; Jazbec, S.S.; Drinovec, I.; Rot, U. Pulmonary Arterial Hypertension Associated with Interferon Beta Treatment for Multiple Sclerosis: A Case Report. Mult. Scler. 2009, 15, 885–886. [Google Scholar] [CrossRef]
- Galiè, N.; Humbert, M.; Vachiery, J.-L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [CrossRef]
- Foster, G.R.; Zeuzem, S.; Pianko, S.; Sarin, S.K.; Piratvisuth, T.; Shah, S.; Andreone, P.; Sood, A.; Chuang, W.-L.; Lee, C.-M.; et al. Decline in Pulmonary Function during Chronic Hepatitis C Virus Therapy with Modified Interferon Alfa and Ribavirin. J. Viral Hepat. 2013, 20, e115–e123. [Google Scholar] [CrossRef] [PubMed]
- Tomaszewski, M.; Grywalska, E.; Tomaszewski, A.; Błaszczak, P.; Kurzyna, M.; Roliński, J.; Kopeć, G. Overexpression of PD-1 on Peripheral Blood Lymphocytes in Patients with Idiopathic Pulmonary Arterial Hypertension and Its Association with High Viral Loads of Epstein-Barr Virus and Poor Clinical Parameters. J. Clin. Med. 2020, 9, 1966. [Google Scholar] [CrossRef] [PubMed]
- Stadhouders, R.; Lubberts, E.; Hendriks, R.W. A Cellular and Molecular View of T Helper 17 Cell Plasticity in Autoimmunity. J. Autoimmun. 2018, 87, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Hautefort, A.; Girerd, B.; Montani, D.; Cohen-Kaminsky, S.; Price, L.; Lambrecht, B.N.; Humbert, M.; Perros, F. T-Helper 17 Cell Polarization in Pulmonary Arterial Hypertension. Chest 2015, 147, 1610–1620. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Study Group (n = 70) | Healthy Volunteers (n = 20) | p-Value | ||
|---|---|---|---|---|---|
| Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | ||
| CD45+ [%] | 75.19 ± 3.20 | 74.58 (62.81–81.57) | 96.27 ± 0.73 | 96.23 (95.20–97.87) | 0.000 * |
| CD3+ [%] | 60.91 ± 2.59 | 60.41 (45.20–68.93) | 81.39 ± 0.98 | 81.42 (80.00–82.74) | 0.000 * |
| CD4+ [%] | 35.54 ± 1.95 | 35.73 (25.64–41.23) | 48.73 ± 3.38 | 48.38 (44.11–54.13) | 0.000 * |
| CD8+ [%] | 25.37 ± 2.98 | 25.36 (16.53–34.24) | 32.66 ± 3.41 | 33.13 (27.75–38.48) | 0.000 * |
| Ratio of CD4+/CD8+ | 1.43 ± 0.23 | 1.37 (0.83–2.04) | 1.52 ± 0.26 | 1.44 (1.15–1.95) | 0.429 |
| CD19+ [%] | 5.93 ± 0.58 | 5.83 (3.89–7.25) | 7.94 ± 0.66 | 7.96 (7.04–8.93) | 0.000 * |
| NK [%] | 3.53 ± 0.84 | 3.40 (1.98–5.02) | 7.13 ± 0.65 | 7.34 (6.19–7.98) | 0.000 * |
| Parameters | CTEPH (n = 10) | CHD (n = 26) | CTD (n = 9) | IPAH (n = 25) | Healthy Volunteers (n = 20) | p-Value | p-Value | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | CHD vs. CTEPH | CHD vs. CTD | CHD vs. IPAH | CTEPH vs. CTD | CTEPH vs. IPAH | CTD vs. IPAH | CHD vs. HV | CTEPH vs. HV | CTD vs. HV | IPAH vs. HV | ||
| CD45+ [%] | 65.77 ± 2.34 | 64.29 (62.81–71.93) | 69.11 ± 3.93 | 69.08 (60.01–76.67) | 65.21 ± 5.67 | 64.97 (55.80–75.74) | 71.37 ± 8.03 | 74.26 (56.53–85.10) | 96.27 ± 0.73 | 96.23 (95.20–97.87) | 0.000 * | 0.006 * | 0.057 | 0.199 | 0.905 | 0.07 | 0.072 | 0.000 * | 0.000 * | 0.000 * | 0.000 * |
| CD3+ [%] | 53.27 ± 1.90 | 52.08 (50.87–58.26) | 55.98 ± 3.16 | 55.95 (48.61–62.10) | 52.82 ± 4.59 | 52.63 (45.20–61.35) | 57.81 ± 6.51 | 60.15 (45.79–68.93) | 81.39 ± 0.98 | 81.42 (80.00–82.74) | 0.000 * | 0.006 * | 0.057 | 0.199 | 0.905 | 0.07 | 0.072 | 0.000 * | 0.000 * | 0.000 * | 0.000* |
| CD4+ [%] | 30.73 ± 1.34 | 30.65 (29.28–33.31) | 32.67 ± 2.07 | 32.87 (28.68–37.14) | 30.60 ± 2.89 | 30.84 (25.64–36.69) | 33.73 ± 4.09 | 34.69 (26.38–41.23) | 48.73 ± 3.38 | 48.38 (44.11–54.13) | 0.000 * | 0.011 * | 0.016 * | 0.281 | 0.905 | 0.064 | 0.072 | 0.000 * | 0.000 * | 0.000 * | 0.000 * |
| CD8+ [%] | 22.54 ± 2.76 | 21.43 (17.56–28.94) | 23.34 ± 3.04 | 23.14 (17.96–30.85) | 22.22 ± 3.40 | 21.79 (17.74–30.48) | 24.11 ± 3.81 | 24.46 (16.53–34.24) | 32.66 ± 3.41 | 33.13 (27.75–38.48) | 0.000 * | 0.392 | 0.171 | 0.437 | 0.604 | 0.211 | 0.151 | 0.000 * | 0.000 * | 0.000 * | 0.000 * |
| Ratio of CD4+/CD8+ | 1.23 ± 0.19 | 1.30 (0.92–1.65) | 1.31 ± 0.22 | 1.26 (0.90–1.84) | 1.24 0.24 | 1.21 (0.91–1.82) | 1.36 ± 0.28 | 1.35 (0.83–2.04) | 1.52 ± 0.26 | 1.44 (1.15–1.95) | 0.023 * | 0.392 | 0.402 | 0.786 | 0.905 | 0.339 | 0.376 | 0.000 * | 0.005 * | 0.011 * | 0.053 |
| CD19+ [%] | 5.09 ± 0.55 | 4.62 (4.36–6.12) | 5.46 ± 0.55 | 5.34 (4.46–6.53) | 5.15 ± 0.80 | 5.09 (3.87–6.45) | 5.62 ± 0.84 | 5.54 (4.10–7.25) | 7.94 ± 0.66 | 7.96 (7.04–8.93) | 0.000 * | 0.109 | 0.342 | 0.507 | 0.905 | 0.097 | 0.216 | 0.000 * | 0.000 * | 0.000 * | 0.000 * |
| NK [%] | 3.05 ± 0.74 | 2.61 (1.86–4.18) | 3.22 ± 0.80 | 3.15 (1.90–4.53) | 3.11 ± 0.50 | 3.12 (1.98–3.83) | 3.35 ± 0.83 | 3.33 (1.75–5.02) | 7.13 ± 0.65 | 7.34 (6.19–7.98) | 0.000 * | 0.475 | 0.753 | 0.647 | 0.780 | 0.460 | 0.618 | 0.000 * | 0.000 * | 0.000 * | 0.000 * |
| Cytokine Concentration [pg/mL] | Study Group (n = 70) | Healthy Volunteers (n = 20) | p-Value | ||
|---|---|---|---|---|---|
| Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | ||
| IL-2 | 18.82 ± 4.86 | 18.12 (4.30–50.12) | 2.76 ± 1.00 | 2.36 (0.48–7.16) | 0.000 * |
| IL-4 | 4.35 ± 1.56 | 4.25 (0.64–14.33) | 4.80 ± 0.31 | 4.67 (4.29–5.31) | 0.236 |
| IL-6 | 30.52 ± 9.63 | 29.53 (9.35–60.30) | 4.13 ± 2.11 | 3.17 (0.15–17.20) | 0.000 * |
| IL-10 | 10.87 ± 2.91 | 10.62 (2.07–35.30) | 4.06 ± 1.02 | 4.08 (2.77–6.16) | 0.000 * |
| IFN-γ | 5.95 ± 1.41 | 6.02 (0.40–23.30) | 2.38 ± 1.19 | 2.34 (0.61–4.38) | 0.000 * |
| Parameters | CHD (n = 26) | CTEPH (n = 10) | CTD (n = 9) | IPAH (n = 25) | p-Value | p-Value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | Mean ± SD | Median (Range) | CHD vs. CTEPH | CHD vs. CTD | CHD vs. IPAH | CTEPH vs. CTD | CTEPH vs. IPAH | CTD vs. IPAH | ||
| Sex | 7 males 19 females | 3 males 7 females | 0 males 9 females | 10 males 5 females | |||||||||||
| Age | 55.69 ± 17.00 | 57.00 (23.00–81.00) | 71.10 ± 8.40 | 72.40 (54.00–81.00) | 52.22 ± 17.62 | 54.00 (28.00–77.00) | 56.52 ± 16.88 | 62.00 (23.00–81.00) | 0.043 * | 0.014 * | 0.724 | 0.829 | 0.010 * | 0.013 * | 0.489 |
| BMI | 25.54 ± 4.10 | 24.90 (19.50–38.15) | 24.74 ± 3.97 | 23.67 (20.44–35.04) | 26.35 ± 6.93 | 25.70 (20.32–44.44) | 27.53 ± 9.67 | 26.00 (17.10–40.52) | 0.318 | 0.475 | 0.867 | 0.186 | 0.905 | 0.090 | 0.355 |
| NT-proBNP [pg/mL] | 1507.04 ± 1898.37 | 804.00 (106.80–9350.00) | 1899.62 ± 1635.75 | 1462.50 (53.00–5991.00) | 734.94 ± 436.55 | 454.00 (127.00–1469.00) | 1192.47 ± 1019.51 | 1076.00 (73.98–3895.00) | 0.391 | 0.271 | 0.402 | 0.933 | 0.095 | 0.286 | 0.316 |
| 6MWT [m] | 323.48 ± 153.14 | 378.00 (0.00–578.00) | 361.80 ± 122.44 | 301.00 (202.00–539.00) | 358.15 ± 156.04 | 420.00 (80.00–577.50) | 381.04 ± 100.29 | 374.00 (136.00–556.00) | 0.734 | 0.505 | 0.564 | 0.316 | 0.905 | 0.578 | 0.939 |
| PVR [dyne/s/cm−5] | 1317.12 ± 812.60 | 1123.43 (134.00–2803.00) | 723.89 ± 233.86 | 742.00 (305.51–1125.80) | 424.53 ± 348.41 | 355.00 (139.00–1292.00) | 697.60 ± 308.26 | 651.00 (158.00–1599.00) | 0.001 * | 0.072 | 0.001 * | 0.005 * | 0.04 * | 0.645 | 0.017 * |
| CI [L/min/m2] | 2.40 ± 1.07 | 2.10 (1.65–7.32) | 2.59 ± 1.23 | 2.10 (1.75–5.80) | 3.16 ± 0.78 | 3.21 (1.83–4.67) | 2.54 ± 0.64 | 2.60 (1.43–3.75) | 0.02 * | 0.838 | 0.003 * | 0.055 | 0.094 | 0.355 | 0.055 |
| CO [L/min] | 4.01 ± 2.08 | 3.52 (2.29–13.90) | 4.37 ± 2.09 | 3.72 (2.48–9.51) | 5.37 ± 1.48 | 5.76 (3.02–8.47) | 4.64 ± 1.13 | 4.46 (2.11–6.42) | 0.003 * | 0.955 | 0.002 * | 0.002 * | 0.094 | 0.188 | 0.298 |
| Mean pressure in the right ventricle [mmHg] | 8.00 ± 3.27 | 8.00 (1.00–16.00) | 9.11 ± 4.86 | 7.00 (3.00–18.00) | 8.56 ± 3.80 | 8.00 (3.00–15.00) | 8.80 ± 5.58 | 9.00 (2.00–23.00) | 0.994 | 0.867 | 0.955 | 0.874 | 0.931 | 0.730 | 0.878 |
| mPAP [mmHg] | 59.15 ± 26.64 | 51.00 (26.00–106.00) | 45.85 ± 8.74 | 46.00 (25.60–56.00) | 35.30 ± 12.49 | 34.00 (25.00–68.00) | 45.24 ± 12.43 | 48.00 (17.00–66.00) | 0.038 * | 0.491 | 0.005 * | 0.026 | 0.019 * | 0.908 | 0.06 |
| PASP [mmHg] | 88.04 ± 32.77 | 83.00 (41.00–150.00) | 82.00 ± 20.97 | 85.00 (39.00–110.00) | 62.56 ± 18.58 | 61.00 (35.00–110.00) | 71.48 ± 20.53 | 77.00 (37.00–96.00) | 0.085 | 0.697 | 0.034 * | 0.092 | 0.024 * | 0.270 | 0.442 |
| RVSP [mmHg] | 91.88 ± 33.16 | 100.00 (47.00–150.00) | 81.56 ± 17.59 | 80.00 (50.00–110.00) | 64.22 ± 19.94 | 61.00 (36.00–115.00) | 72.44 ± 20.29 | 79.00 (42.00–96.00) | 0.053 | 0.445 | 0.046 * | 0.029 * | 0.040 * | 0.298 | 0.514 |
| Lymphocytes [103/mm3] | 1.72 ± 0.46 | 1.62 (1.10–2.77) | 2.51 ± 0.91 | 2.43 (1.30–3.83) | 2.47 ± 0.38 | 2.60 (1.67–3.04) | 2.15 ± 0.55 | 2.01 (1.20–3.14) | 0.002 * | 0.03 * | 0.000 * | 0.006 * | 0.905 | 0.321 | 0.120 |
| Hemoglobin [g/dL] | 15.40 ± 4.30 | 15.70 (7.40–22.10) | 13.24 ± 2.51 | 13.75 (8.50–16.70) | 13.76 ± 2.28 | 13.50 (11.30–19.40) | 13.66 ± 2.03 | 13.60 (9.50–18.50) | 0.491 | 0.200 | 0.424 | 0.205 | 0.968 | 0.928 | 0.818 |
| Platelet count [103/mm3] | 164.11 ± 63.13 | 153.00 (62.00–299.00) | 189.00 ± 69.38 | 182.50 (93.00–348.00) | 147.88 ± 87.08 | 114.00 (55.00–309.00) | 211.40 ± 78.95 | 210.00 (79.00–474.00) | 0.048 * | 0.355 | 0.271 | 0.022 * | 0.156 | 0.377 | 0.037 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomaszewski, M.; Mertowska, P.; Janczewska, M.; Styczeń, A.; Mertowski, S.; Jonas, K.; Grywalska, E.; Kopeć, G. In the Search for Biomarkers of Pulmonary Arterial Hypertension, Are Cytokines IL-2, IL-4, IL-6, IL-10, and IFN-Gamma the Right Indicators to Use? Int. J. Mol. Sci. 2023, 24, 13694. https://doi.org/10.3390/ijms241813694
Tomaszewski M, Mertowska P, Janczewska M, Styczeń A, Mertowski S, Jonas K, Grywalska E, Kopeć G. In the Search for Biomarkers of Pulmonary Arterial Hypertension, Are Cytokines IL-2, IL-4, IL-6, IL-10, and IFN-Gamma the Right Indicators to Use? International Journal of Molecular Sciences. 2023; 24(18):13694. https://doi.org/10.3390/ijms241813694
Chicago/Turabian StyleTomaszewski, Michał, Paulina Mertowska, Martyna Janczewska, Agnieszka Styczeń, Sebastian Mertowski, Kamil Jonas, Ewelina Grywalska, and Grzegorz Kopeć. 2023. "In the Search for Biomarkers of Pulmonary Arterial Hypertension, Are Cytokines IL-2, IL-4, IL-6, IL-10, and IFN-Gamma the Right Indicators to Use?" International Journal of Molecular Sciences 24, no. 18: 13694. https://doi.org/10.3390/ijms241813694
APA StyleTomaszewski, M., Mertowska, P., Janczewska, M., Styczeń, A., Mertowski, S., Jonas, K., Grywalska, E., & Kopeć, G. (2023). In the Search for Biomarkers of Pulmonary Arterial Hypertension, Are Cytokines IL-2, IL-4, IL-6, IL-10, and IFN-Gamma the Right Indicators to Use? International Journal of Molecular Sciences, 24(18), 13694. https://doi.org/10.3390/ijms241813694