


Increased Levels of Galectin-3 in Critical COVID-19

 , , , , ,
, , , , ,  ,
,  and
and 
Abstract
:1. Introduction
2. Results
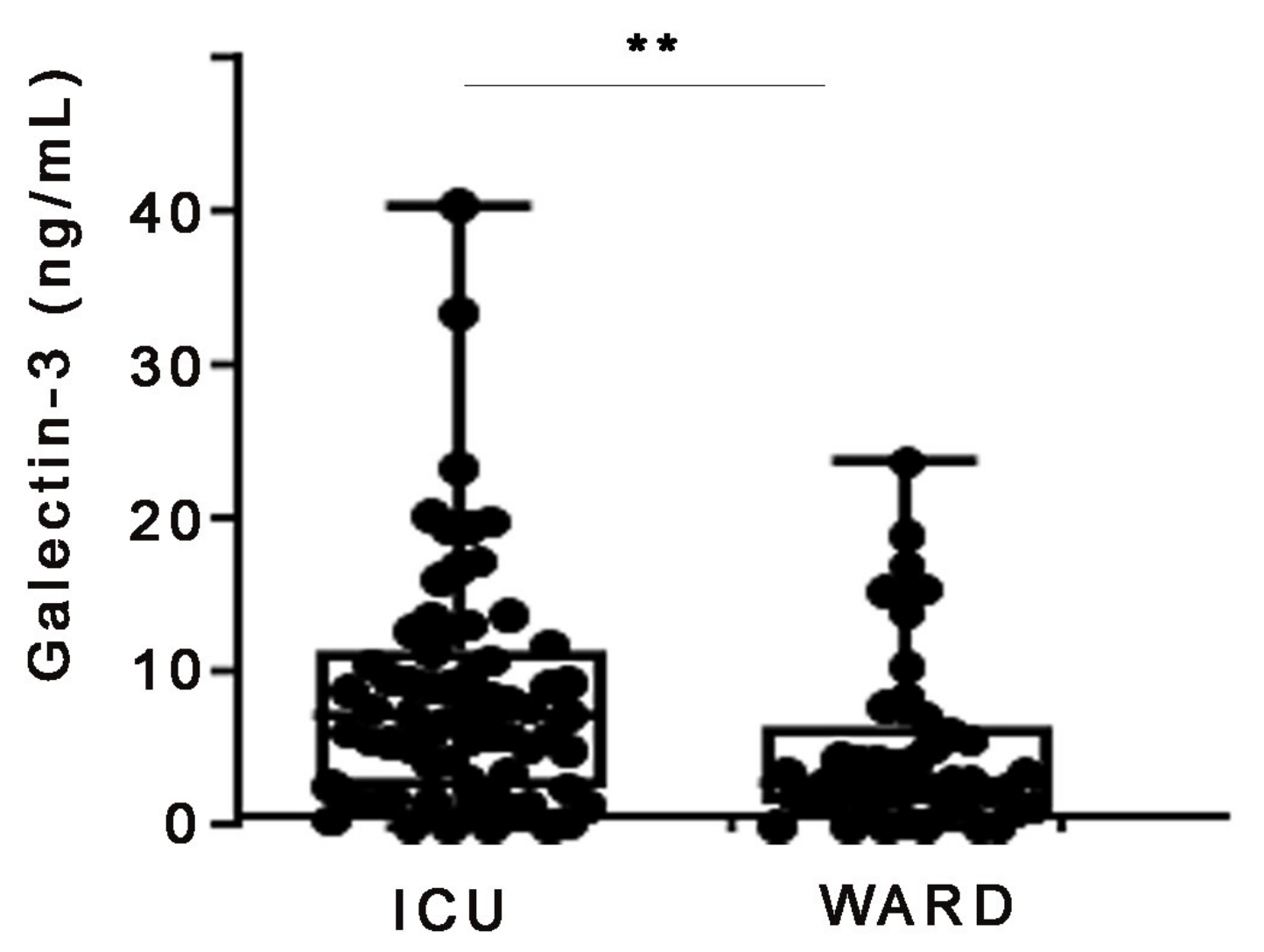
2.1. Increased Serum Galectin-3 Protein Levels in Severe COVID-19 Patients
2.2. Increased Levels of Galectin-3 Correlate with Poor ICU Prognosis
2.3. Validation of the Role of Galectin-3 in COVID-19 Severity
3. Discussion
4. Materials and Methods
4.1. Study Design and Data Collection
4.2. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Moutchia, J.; Pokharel, P.; Kerri, A.; McGaw, K.; Uchai, S.; Nji, M.; Goodman, M. Clinical laboratory parameters associated with severe or critical novel coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. PLoS ONE 2020, 15, e0239802. [Google Scholar] [CrossRef]
- Tan, L.; Wang, Q.; Zhang, D.; Ding, J.; Huang, Q.; Tang, Y.Q.; Wang, Q.; Miao, H. Lymphopenia predicts disease severity of COVID-19: A descriptive and predictive study. Signal Transduct. Target. Ther. 2020, 5, 33. [Google Scholar] [CrossRef]
- Yang, R.Y.; Rabinovich, G.A.; Liu, F.T. Galectins: Structure, function and therapeutic potential. Expert Rev. Mol. Med. 2008, 10, e17. [Google Scholar] [CrossRef] [PubMed]
- Nieminen, J.; St-Pierre, C.; Sato, S. Galectin-3 interacts with naive and primed neutrophils, inducing innate immune responses. J. Leukoc. Biol. 2005, 78, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Stillman, B.N.; Hsu, D.K.; Pang, M.; Brewer, C.F.; Johnson, P.; Liu, F.T.; Baum, L.G. Galectin-3 and galectin-1 bind distinct cell surface glycoprotein receptors to induce T cell death. J. Immunol. 2006, 176, 778–789. [Google Scholar] [CrossRef]
- Stojanovic, B.S.; Stojanovic, B.; Milovanovic, J.; Arsenijević, A.; Dimitrijevic Stojanovic, M.; Arsenijevic, N.; Milovanovic, M. The Pivotal Role of Galectin-3 in Viral Infection: A Multifaceted Player in Host-Pathogen Interactions. Int. J. Mol. Sci. 2023, 24, 9617. [Google Scholar] [CrossRef]
- Gao, P.; Simpson, J.L.; Zhang, J.; Gibson, P.G. Galectin-3: Its role in asthma and potential as an anti-inflammatory target. Respir. Res. 2013, 14, 136. [Google Scholar] [CrossRef]
- Liu, F.T.; Rabinovich, G.A. Galectins: Regulators of acute and chronic inflammation. Ann. N. Y. Acad. Sci. 2010, 1183, 158–182. [Google Scholar] [CrossRef]
- Mackinnon, A.C.; Gibbons, M.A.; Farnworth, S.L.; Leffler, H.; Nilsson, U.J.; Delaine, T.; Simpson, A.J.; Forbes, S.J.; Hirani, N.; Gauldie, J.; et al. Regulation of transforming growth factor-β1-driven lung fibrosis by galectin-3. Am. J. Respir. Crit. Care Med. 2012, 185, 537–546. [Google Scholar] [CrossRef]
- Henderson, N.C.; Mackinnon, A.C.; Farnworth, S.L.; Poirier, F.; Russo, F.P.; Iredale, J.P.; Haslett, C.; Simpson, K.J.; Sethi, T. Galectin-3 regulates myofibroblast activation and hepatic fibrosis. Proc. Natl. Acad. Sci. USA 2006, 103, 5060–5065. [Google Scholar] [CrossRef]
- Cervantes-Alvarez, E.; la Rosa, N.L.; la Mora, M.S.; Valdez-Sandoval, P.; Palacios-Jimenez, M.; Rodriguez-Alvarez, F.; Vera-Maldonado, B.I.; Aguirre-Aguilar, E.; Escobar-Valderrama, J.M.; Alanis-Mendizabal, J.; et al. Galectin-3 as a potential prognostic biomarker of severe COVID-19 in SARS-CoV-2 infected patients. Sci. Rep. 2022, 12, 1856. [Google Scholar] [CrossRef]
- Gajovic, N.; Markovic, S.S.; Jurisevic, M.; Jovanovic, M.; Arsenijevic, N.; Mijailovic, Z.; Jovanovic, M.; Jovanovic, I. Galectin-3 as an important prognostic marker for COVID-19 severity. Sci. Rep. 2023, 13, 1460. [Google Scholar] [CrossRef]
- Özcan, S.; Dönmez, E.; Yavuz, S.T.; Ziyrek, M.; İnce, O.; Küçük, H.S.; Taşdemir, Z.A.; Yılmaz, İ.; Varol, S.; Şahin, İ.; et al. Prognostic significance of serum galectin-3 in hospitalized patients with COVID-19. Cytokine 2022, 158, 155970. [Google Scholar] [CrossRef]
- Kazancioglu, S.; Yilmaz, F.M.; Bastug, A.; Ozbay, B.O.; Aydos, O.; Yücel, Ç.; Bodur, H.; Yilmaz, G. Assessment of Galectin-1, Galectin-3, and Prostaglandin E2 Levels in Patients with COVID-19. Jpn. J. Infect. Dis. 2021, 74, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Kuśnierz-Cabala, B.; Maziarz, B.; Dumnicka, P.; Dembiński, M.; Kapusta, M.; Bociąga-Jasik, M.; Winiarski, M.; Garlicki, A.; Grodzicki, T.; Kukla, M. Diagnostic Significance of Serum Galectin-3 in Hospitalized Patients with COVID-19—A Preliminary Study. Biomolecules 2021, 11, 1136. [Google Scholar] [CrossRef] [PubMed]
- Puccini, M.; Jakobs, K.; Reinshagen, L.; Friebel, J.; Schencke, P.A.; Ghanbari, E.; Landmesser, U.; Haghikia, A.; Kränkel, N.; Rauch, U. Galectin-3 as a Marker for Increased Thrombogenicity in COVID-19. Int. J. Mol. Sci. 2023, 24, 7683. [Google Scholar] [CrossRef] [PubMed]
- Vasta, G.R. Galectins as pattern recognition receptors: Structure, function, and evolution. Adv. Exp. Med. Biol. 2012, 946, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Vasta, G.R. Roles of galectins in infection. Nat. Rev. Microbiol. 2009, 7, 424–438. [Google Scholar] [CrossRef] [PubMed]
- Morrison, H.M.; Craft, J.; Rivera-Lugo, R.; Johnson, J.R.; Golovkine, G.R.; Bell, S.L.; Dodd, C.E.; Van Dis, E.; Beatty, W.L.; Margolis, S.R.; et al. Deficiency in Galectin-3, -8, and -9 impairs immunity to chronic Mycobacterium tuberculosis infection but not acute infection with multiple intracellular pathogens. PLoS Pathog. 2023, 19, e1011088. [Google Scholar] [CrossRef]
- Fradin, C.; Poulain, D.; Jouault, T. Beta-1,2-linked oligomannosides from Candida albicans bind to a 32-kilodalton macrophage membrane protein homologous to the mammalian lectin galectin-3. Infect. Immun. 2000, 68, 4391–4398. [Google Scholar] [CrossRef]
- Weigand, K.; Peschel, G.; Grimm, J.; Müller, M.; Buechler, C. Serum Galectin-3 in Hepatitis C Virus Infection Declines after Successful Virus Eradication by Direct-Acting Antiviral Therapy. J. Gastrointest. Liver Dis. JGLD 2022, 31, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, R.; Prasad, A. Exosomes Derived from HIV-1 Infected DCs Mediate Viral trans-Infection via Fibronectin and Galectin-3. Sci. Rep. 2017, 7, 14787. [Google Scholar] [CrossRef]
- Xue, J.; Fu, C.; Cong, Z.; Peng, L.; Peng, Z.; Chen, T.; Wang, W.; Jiang, H.; Wei, Q.; Qin, C. Galectin-3 promotes caspase-independent cell death of HIV-1-infected macrophages. FEBS J. 2017, 284, 97–113. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Revilla, J.; Deierborg, T.; Venero, J.L.; Boza-Serrano, A. Hyperinflammation and Fibrosis in Severe COVID-19 Patients: Galectin-3, a Target Molecule to Consider. Front. Immunol. 2020, 11, 2069. [Google Scholar] [CrossRef] [PubMed]
- Kaur, M.; Kumar, D.; Butty, V.; Singh, S.; Esteban, A.; Fink, G.R.; Ploegh, H.L.; Sehrawat, S. Galectin-3 Regulates γ-Herpesvirus Specific CD8 T Cell Immunity. iScience 2018, 9, 101–119. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.J.; Wang, S.F.; Weng, I.C.; Hong, M.H.; Lo, T.H.; Jan, J.T.; Hsu, L.C.; Chen, H.Y.; Liu, F.T. Galectin-3 Enhances Avian H5N1 Influenza A Virus-Induced Pulmonary Inflammation by Promoting NLRP3 Inflammasome Activation. Am. J. Pathol. 2018, 188, 1031–1042. [Google Scholar] [CrossRef]
- Salah, A.; Yoshifuji, H.; Ito, S.; Kitagori, K.; Kiso, K.; Yamada, N.; Nakajima, T.; Haga, H.; Tsuruyama, T.; Miyagawa-Hayashino, A. High Expression of Galectin-3 in Patients with IgG4-Related Disease: A Proteomic Approach. Pathol. Res. Int. 2017, 2017, 9312142. [Google Scholar] [CrossRef]
- Beltramo, G.; Cottenet, J.; Mariet, A.S.; Georges, M.; Piroth, L.; Tubert-Bitter, P.; Bonniaud, P.; Quantin, C. Chronic respiratory diseases are predictors of severe outcome in COVID-19 hospitalised patients: A nationwide study. Eur. Respir. J. 2021, 58, 2004474. [Google Scholar] [CrossRef] [PubMed]
- Esposito, A.J.; Menon, A.A.; Ghosh, A.J.; Putman, R.K.; Fredenburgh, L.E.; El-Chemaly, S.Y.; Goldberg, H.J.; Baron, R.M.; Hunninghake, G.M.; Doyle, T.J. Increased Odds of Death for Patients with Interstitial Lung Disease and COVID-19: A Case-Control Study. Am. J. Respir. Crit. Care Med. 2020, 202, 1710–1713. [Google Scholar] [CrossRef]
- De Roquetaillade, C.; Bredin, S.; Lascarrou, J.B.; Soumagne, T.; Cojocaru, M.; Chousterman, B.G.; Leclerc, M.; Gouhier, A.; Piton, G.; Pène, F.; et al. Timing and causes of death in severe COVID-19 patients. Crit. Care 2021, 25, 224. [Google Scholar] [CrossRef] [PubMed]
- Hara, A.; Niwa, M.; Kanayama, T.; Noguchi, K.; Niwa, A.; Matsuo, M.; Kuroda, T.; Hatano, Y.; Okada, H.; Tomita, H. Galectin-3: A Potential Prognostic and Diagnostic Marker for Heart Disease and Detection of Early Stage Pathology. Biomolecules 2020, 10, 1277. [Google Scholar] [CrossRef]
- Ho, J.E.; Gao, W.; Levy, D.; Santhanakrishnan, R.; Araki, T.; Rosas, I.O.; Hatabu, H.; Latourelle, J.C.; Nishino, M.; Dupuis, J.; et al. Galectin-3 Is Associated with Restrictive Lung Disease and Interstitial Lung Abnormalities. Am. J. Respir. Crit. Care Med. 2016, 194, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Nishi, Y.; Sano, H.; Kawashima, T.; Okada, T.; Kuroda, T.; Kikkawa, K.; Kawashima, S.; Tanabe, M.; Goto, T.; Matsuzawa, Y.; et al. Role of galectin-3 in human pulmonary fibrosis. Allergol. Int. Off. J. Jpn. Soc. Allergol. 2007, 56, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Hirani, N.; MacKinnon, A.C.; Nicol, L.; Ford, P.; Schambye, H.; Pedersen, A.; Nilsson, U.J.; Leffler, H.; Sethi, T.; Tantawi, S.; et al. Target inhibition of galectin-3 by inhaled TD139 in patients with idiopathic pulmonary fibrosis. Eur. Respir. J. 2021, 57, 2002559. [Google Scholar] [CrossRef]
- Liao, M.; Liu, Y.; Yuan, J.; Wen, Y.; Xu, G.; Zhao, J.; Cheng, L.; Li, J.; Wang, X.; Wang, F.; et al. Single-cell landscape of bronchoalveolar immune cells in patients with COVID-19. Nat. Med. 2020, 26, 842–844. [Google Scholar] [CrossRef]
- Gaughan, E.E.; Quinn, T.M.; Mills, A.; Bruce, A.M.; Antonelli, J.; MacKinnon, A.C.; Aslanis, V.; Li, F.; O’Connor, R.; Boz, C.; et al. An Inhaled Galectin-3 Inhibitor in COVID-19 Pneumonitis: A Phase Ib/IIa Randomized Controlled Clinical Trial (DEFINE). Am. J. Respir. Crit. Care Med. 2023, 207, 138–149. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patient Clinical Characteristics | ICU | Ward |
|---|---|---|
| Number of patients (n) | 67 | 49 |
| Sex | ||
| Male | 51 (76.1%) | 33 (67.3%) |
| Female | 16 (23.9%) | 16 (32.7%) |
| Age (years, mean ± SD) | 64.3 ± 10.5 | 56.6 ± 16 |
| Comorbidities n (%) | ||
| Hypertension | 23 (34.3%) | 9 (18.4%) |
| Diabetes | 7 (10.4%) | 4 (8.1%) |
| Hyperlipidaemia | 16 (23.8%) | 9 (18.4%) |
| COPD | 3 (4.4%) | 2 (4%) |
| Chronic kidney disease | 0 | 0 |
| Coronary artery disease | 7 (10.4%) | 8 (16.3%) |
| COVID 19 treatment | ||
| Azithromycin/chloroquine/ | ||
| lopinavir/ritonavir | 11 | |
| Azithromycin/chloroquine | 7 | 6 |
| Lopinavir/ritonavir/ | ||
| chloroquine | 2 | |
| Chloroquine | 3 | |
| Azithromycin | 8 | 29 |
| Plasma | 1 | |
| Mechanical Ventilation (days), (median, IQR) | 11 (4–30) | N/A |
| Hospital mortality (%) | 31.3 | 8.2 * |
| Hospital length of stay (days), (median, IQR) | 18 (12–31) | 9 (7–12) |
| Days sick before admission (median, IQR) | 7 (5–8) | 6 (5–9) |
| Diffuse lung infiltrates in X-ray | 62 (92.5%) | 30 (61.2%) |
| Pneumonia | 67 (100%) | 34 (69.4%) |
| Glucose (mg/dL) (median, IQR) | 141 (108–204) | 101 (82–127) * |
| Creatinine (mg/dL) | 1.02 ± 0.32 | 0.9 ± 0.33 |
| CRP (mg/dL), (median, IQR) | 13.3 (5.3–21) | 6.4 (2–15) * |
| Na+ (mEq/L) | 140 ± 7 | 135 ± 4 |
| Total bilirubin (mg/dL) | 0.6 (0.4–0.88) | 0.4 (0.3–0.57) |
| White blood cell count (per μL) | 10,300 (8200–13,200) | 6900 (4600–9800) |
| Neutrophils (%) | 82.5 ± 11.4 | 69.2 ± 13.2 |
| Lymphocytes (%) | 12.5 ± 6.34 | 24.03 ± 10.89 |
| D-dimer (pg/mL) | 1.71 ± 0.29 | 1.14 ± 0.23 |
| LDH (U/L), (median, IQR) | 422 (334–590) | 263 (209–366) * |
| Fibrinogen (mg/dL | 638 ± 168 | 521 ± 174 |
| Ferritin (pg/mL), (median, IQR) | 621 (198–1124) | 264 (108–513) * |
| Patient Clinical Characteristics | Survivors | Non-Survivors |
|---|---|---|
| Number of patients (n) | 42 | 25 |
| Sex | ||
| Male | 30 (71.4%) | 21 (84%) |
| Female | 12 (28.6%) | 4 (16%) |
| Age (years, mean ± SD) | 61.5 ± 10.1 | 68.3 ± 9.3 |
| SOFA (median, IQR) | 6 (4–8) | 7 (4–9) |
| APACHE II (median, IQR) | 15 (11–17) | 17 (14–18) * |
| Mechanical Ventilation (days) (median, IQR) | 11 (4–30) | 24 (12–31) |
| D-dimer (pg/mL) | 1.54 ± 2 | 2 ± 2.2 |
| LDH (U/L) | 414 (322–498) | 532 (375–726) * |
| CRP (mg/dL) | 11.3 (5–18.4) | 15 (5.3–27) |
| Ferritin (pg/mL) | 576 (117–1850) | 744 (486–2740) |
| Variable | Univariate Model | Multivariate Model | ||
|---|---|---|---|---|
| OR (95%CI) | p-Value | OR (95%CI) | p-Value | |
| Galectin-3 | 1.044 (1.007–1.083) | 0.018 | 1.069 (1.013–1.128) | 0.016 |
| Age | 1.018 (0.980–1.057) | 0.359 | 1.016 (0.974–1.060) | 0.465 |
| LDH | 1.001 (1.000–1.002) | 0.053 | 1.001 (1.000–1.002) | 0.065 |
| APACHE | 1.008 (0.915–1.110) | 0.878 | 1.014 (0.904–1.138) | 0.810 |
| Patient Clinical Characteristics | ICU | Ward |
|---|---|---|
| Number of patients (n) | 24 | 95 |
| Sex | ||
| Male | 20 (83.3%) | 49 (51.6%) |
| Female | 4 (16.7%) | 46 (48.4%) |
| Mechanical Ventilation (days) (median, IQR) | 15 (6–23) | N/A |
| Hospital mortality (%) | 41.6 | 4.2 * |
| Comorbidities n (%) | ||
| Hypertension | 5 (20.8%) | 44 (46.3%) |
| Diabetes | 0 (0%) | 18 (18.9%) |
| Hyperlipidaemia | 3 (12.5%) | 38 (40%) |
| Coronary artery disease | 3 (12.5%) | 5 (5.2%) |
| COPD | 2 (8.3%) | 4 (4.2%) |
| Age (years, mean ± SD) | 62.3 ± 15.5 | 59 ± 15 |
| Hospital length of stay (days), (median, IQR) | 20 (12–25) | 9 (6–12) |
| Days sick before admission (median, IQR) | 7 (5–9) | 6 (3–7) |
| Diffuse lung infiltrates in X-ray | 23 (95.8%) | 74 (77.9%) |
| Glucose (mg/dL) (median, IQR) | 127 (102–165) | 115 (101–138) |
| Creatinine (mg/dL) | 1.14 ± 1.28 | 0.95 ± 0.41 |
| CRP (mg/dL) (median, IQR) | 12.3 (4.5–16) | 4 (1.5–8.2) * |
| Na+ (mEq/L) | 139 ± 5.8 | 136 ± 3.3 |
| Total bilirubin (mg/dL) (median, IQR) | 0.67 (0.46–0.94) | 0.5 (0.39–0.66) |
| White blood cell count (per μL) (median, IQR) | 7000 (4000–9700) | 5400 (4300–7000) |
| LDH (U/L) (median, IQR) | 412 (280–522) | 289 (246–355) * |
| D-dimer (pg/mL) | 1.67 ± 1.96 | 1.12 ± 1.6 * |
| Fibrinogen (mg/dL) | 799 ± 120 | 530 ± 133 |
| Ferritin (pg/mL) (median, IQR) | 855 (411–1720) | 351 (190–745) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikitopoulou, I.; Vassiliou, A.G.; Athanasiou, N.; Jahaj, E.; Akinosoglou, K.; Dimopoulou, I.; Orfanos, S.E.; Dimakopoulou, V.; Schinas, G.; Tzouvelekis, A.; et al. Increased Levels of Galectin-3 in Critical COVID-19. Int. J. Mol. Sci. 2023, 24, 15833. https://doi.org/10.3390/ijms242115833
Nikitopoulou I, Vassiliou AG, Athanasiou N, Jahaj E, Akinosoglou K, Dimopoulou I, Orfanos SE, Dimakopoulou V, Schinas G, Tzouvelekis A, et al. Increased Levels of Galectin-3 in Critical COVID-19. International Journal of Molecular Sciences. 2023; 24(21):15833. https://doi.org/10.3390/ijms242115833
Chicago/Turabian StyleNikitopoulou, Ioanna, Alice G. Vassiliou, Nikolaos Athanasiou, Edison Jahaj, Karolina Akinosoglou, Ioanna Dimopoulou, Stylianos E. Orfanos, Vasiliki Dimakopoulou, Georgios Schinas, Argyrios Tzouvelekis, and et al. 2023. "Increased Levels of Galectin-3 in Critical COVID-19" International Journal of Molecular Sciences 24, no. 21: 15833. https://doi.org/10.3390/ijms242115833
APA StyleNikitopoulou, I., Vassiliou, A. G., Athanasiou, N., Jahaj, E., Akinosoglou, K., Dimopoulou, I., Orfanos, S. E., Dimakopoulou, V., Schinas, G., Tzouvelekis, A., Aidinis, V., & Kotanidou, A. (2023). Increased Levels of Galectin-3 in Critical COVID-19. International Journal of Molecular Sciences, 24(21), 15833. https://doi.org/10.3390/ijms242115833