

Association of SLC12A1 and GLUR4 Ion Transporters with Neoadjuvant Chemoresistance in Luminal Locally Advanced Breast Cancer

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
2.1. Clinicopathological Features in the Breast Cancer Cohort
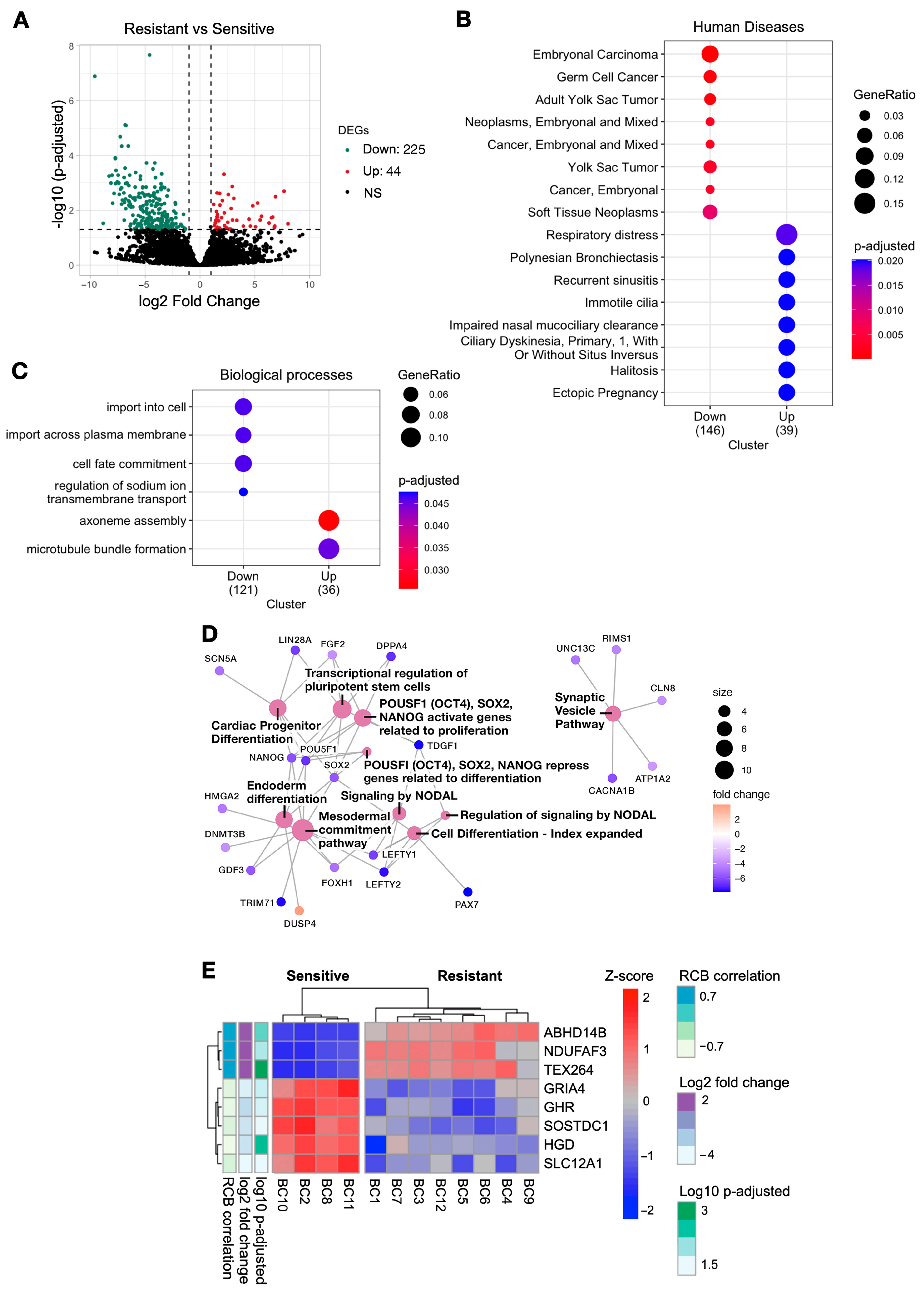
2.2. Downregulated Genes in Resistant Patients Were Associated with Pathways Involved in Cancer and Membrane Transport
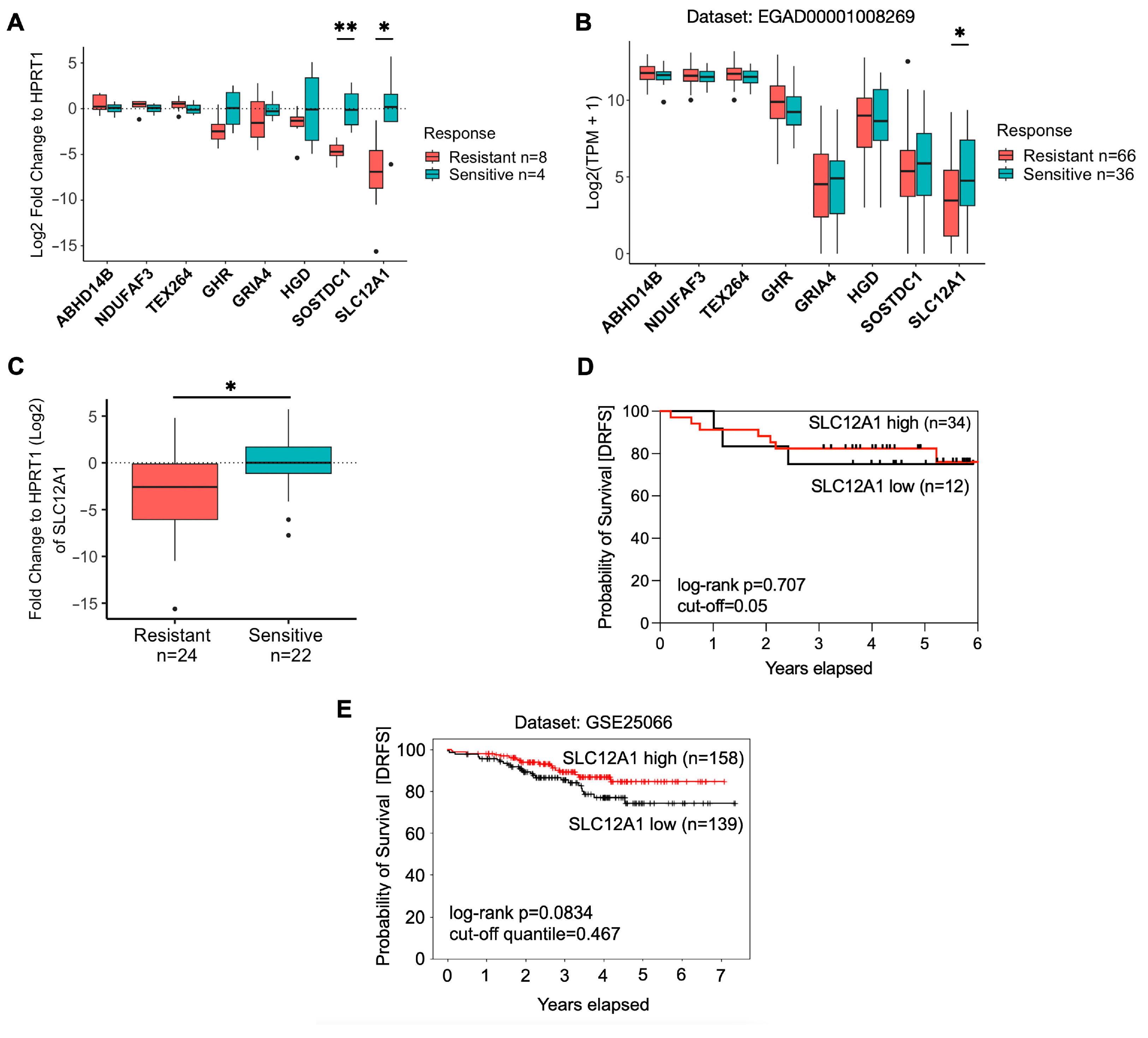
2.3. Validation of the DEGs in Breast Cancer Patients
2.4. SLC12A1 Is Associated with Chemosensitivity to NAC
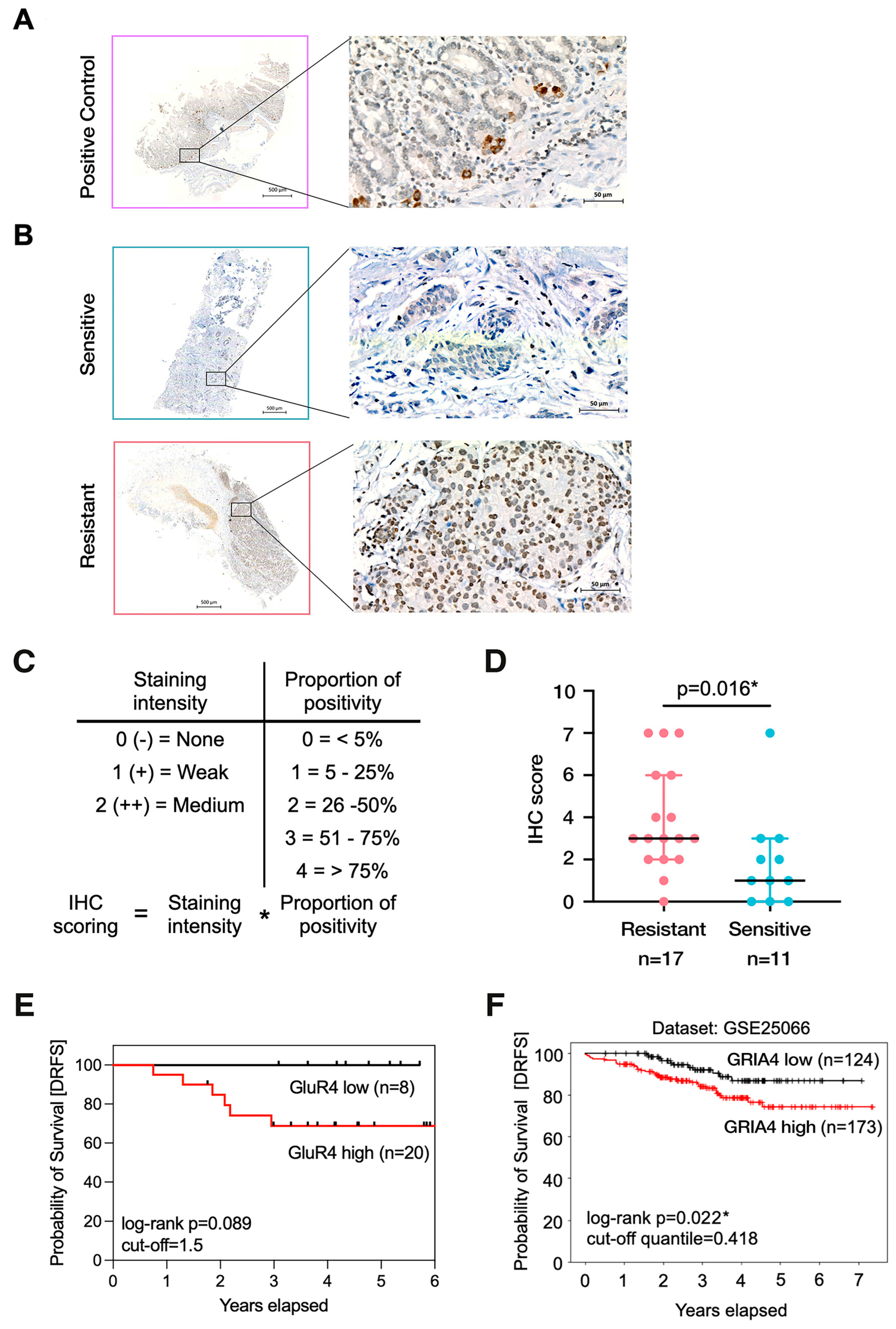
2.5. High Levels of GLUR4 Are Associated with Chemoresistance and Worse Prognoses
2.6. GLUR4 Is a Potential Predictive Marker of Resistance to NAC in Breast Cancer
3. Discussion
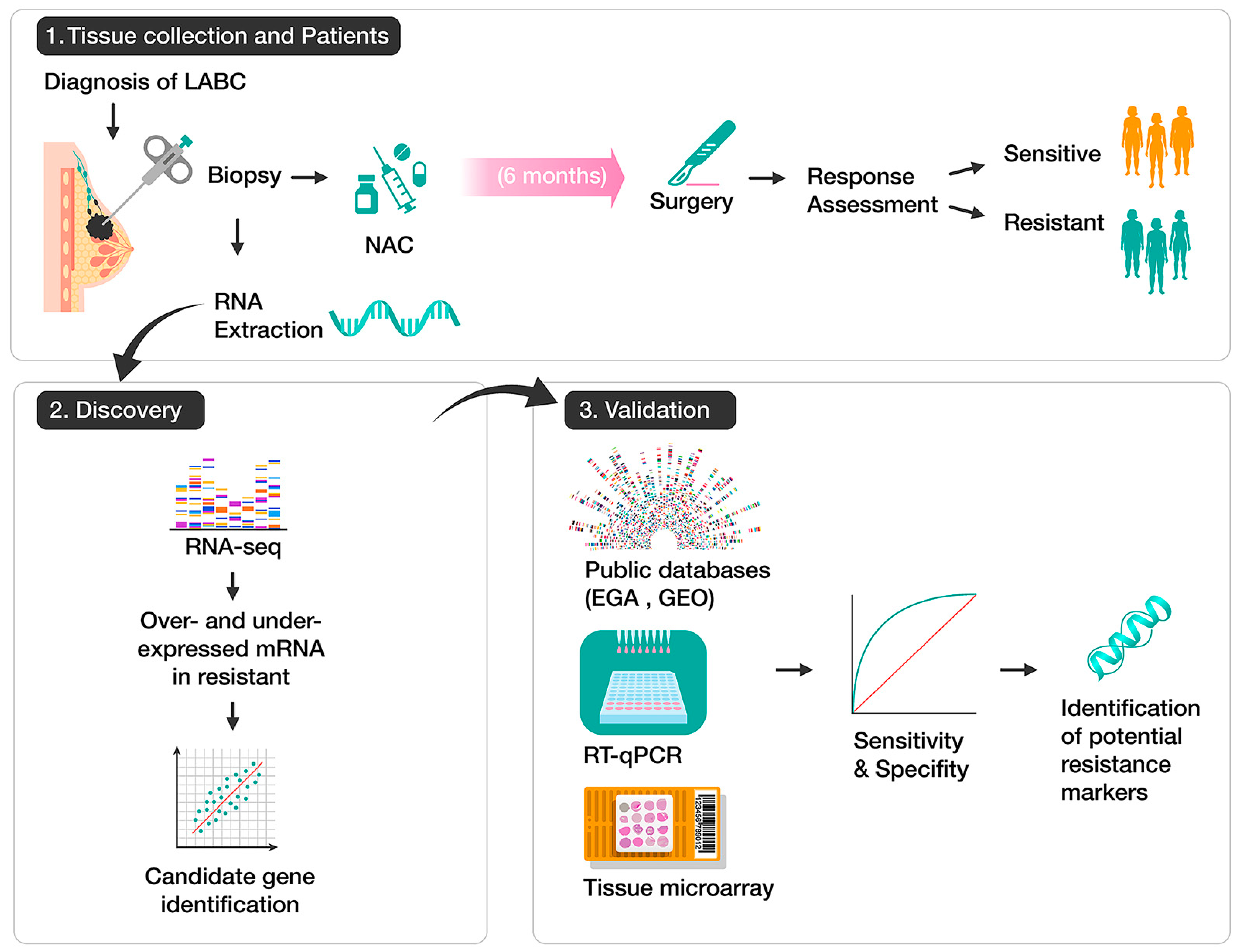
4. Materials and Methods
4.1. Patients and Collection of Tissue Samples
4.2. RNA Extraction and RT-qPCR
4.3. RNA-Seq and Data Analysis
4.4. External Breast Cancer Datasets
4.5. Tissue Microarrays and Immunohistochemical Assay
4.6. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer Today. Available online: https://gco.iarc.fr/today (accessed on 27 February 2023).
- Villarreal-Garza, C.; Lopez-Martinez, E.A.; Muñoz-Lozano, J.F.; Unger-Saldaña, K. Locally Advanced Breast Cancer in Young Women in Latin America. Ecancermedicalscience 2019, 13, 894. [Google Scholar] [CrossRef] [PubMed]
- Werutsky, G.; Nunes, P.; Barrios, C. Locally Advanced Breast Cancer in Brazil: Current Status and Future Perspectives. Ecancermedicalscience 2018, 13, 895. [Google Scholar] [CrossRef] [PubMed]
- Pinto, J.A.; Pinillos, L.; Villarreal-Garza, C.; Morante, Z.; Villarán, M.V.; Mejía, G.; Caglevic, C.; Aguilar, A.; Fajardo, W.; Usuga, F.; et al. Barriers in Latin America for the Management of Locally Advanced Breast Cancer. Ecancermedicalscience 2019, 13, 897. [Google Scholar] [CrossRef]
- Pernaut, C.; Lopez, F.; Ciruelos, E. Standard Neoadjuvant Treatment in Early/Locally Advanced Breast Cancer. Breast Care 2018, 13, 244–249. [Google Scholar] [CrossRef] [PubMed]
- See, S.H.C.; Siziopikou, K.P. Pathologic Evaluation of Specimens after Neoadjuvant Chemotherapy in Breast Cancer: Current Recommendations and Challenges. Pathol.-Res. Pract. 2022, 230, 153753. [Google Scholar] [CrossRef]
- Symmans, W.F.; Peintinger, F.; Hatzis, C.; Rajan, R.; Kuerer, H.; Valero, V.; Assad, L.; Poniecka, A.; Hennessy, B.; Green, M.; et al. Measurement of Residual Breast Cancer Burden to Predict Survival After Neoadjuvant Chemotherapy. J. Clin. Oncol. 2007, 25, 4414–4422. [Google Scholar] [CrossRef]
- Prihantono; Faruk, M. Breast Cancer Resistance to Chemotherapy: When Should We Suspect It and How Can We Prevent It? Ann. Med. Surg. 2021, 70, 102793. [Google Scholar] [CrossRef]
- Li, Y.; Ma, L. Efficacy of Chemotherapy for Lymph Node-Positive Luminal A Subtype Breast Cancer Patients: An Updated Meta-Analysis. World J. Surg. Oncol. 2020, 18, 316. [Google Scholar] [CrossRef]
- Straver, M.E.; Glas, A.M.; Hannemann, J.; Wesseling, J.; van de Vijver, M.J.; Rutgers, E.J.T.; Peeters, M.-J.T.F.D.V.; van Tinteren, H.; Veer, L.J.v.; Rodenhuis, S. The 70-Gene Signature as a Response Predictor for Neoadjuvant Chemotherapy in Breast Cancer. Breast Cancer Res. Treat. 2010, 119, 551–558. [Google Scholar] [CrossRef]
- Hamy, A.-S.; Darrigues, L.; Laas, E.; Croze, D.D.; Topciu, L.; Lam, G.-T.; Evrevin, C.; Rozette, S.; Laot, L.; Lerebours, F.; et al. Prognostic Value of the Residual Cancer Burden Index According to Breast Cancer Subtype: Validation on a Cohort of BC Patients Treated by Neoadjuvant Chemotherapy. PLoS ONE 2020, 15, e0234191. [Google Scholar] [CrossRef]
- Barbieri, E.; Gentile, D.; Bottini, A.; Sagona, A.; Gatzemeier, W.; Losurdo, A.; Fernandes, B.; Tinterri, C. Neo-Adjuvant Chemotherapy in Luminal, Node Positive Breast Cancer: Characteristics, Treatment and Oncological Outcomes: A Single Center’s Experience. Eur. J. Breast Health 2021, 17, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Zhang, M.; Wang, B.; Zhang, L.; Zhou, F.; Fang, M. Chemoresistance and Metastasis in Breast Cancer Molecular Mechanisms and Novel Clinical Strategies. Front. Oncol. 2021, 11, 658552. [Google Scholar] [CrossRef]
- Sammut, S.-J.; Crispin-Ortuzar, M.; Chin, S.-F.; Provenzano, E.; Bardwell, H.A.; Ma, W.; Cope, W.; Dariush, A.; Dawson, S.-J.; Abraham, J.E.; et al. Multi-Omic Machine Learning Predictor of Breast Cancer Therapy Response. Nature 2022, 601, 623–629. [Google Scholar] [CrossRef]
- Hatzis, C.; Pusztai, L.; Valero, V.; Booser, D.J.; Esserman, L.; Lluch, A.; Vidaurre, T.; Holmes, F.; Souchon, E.; Wang, H.; et al. A Genomic Predictor of Response and Survival Following Taxane-Anthracycline Chemotherapy for Invasive Breast Cancer. JAMA 2011, 305, 1873–1881. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Anderle, P.; Bussey, K.J.; Barbacioru, C.; Shankavaram, U.; Dai, Z.; Reinhold, W.C.; Papp, A.; Weinstein, J.N.; Sadée, W. Membrane Transporters and Channels Role of the Transportome in Cancer Chemosensitivity and Chemoresistance. Cancer Res. 2004, 64, 4294–4301. [Google Scholar] [CrossRef] [PubMed]
- Kischel, P.; Girault, A.; Rodat-Despoix, L.; Chamlali, M.; Radoslavova, S.; Daya, H.A.; Lefebvre, T.; Foulon, A.; Rybarczyk, P.; Hague, F.; et al. Ion Channels: New Actors Playing in Chemotherapeutic Resistance. Cancers 2019, 11, 376. [Google Scholar] [CrossRef] [PubMed]
- Lukacova, E.; Burjanivova, T.; Podlesniy, P.; Grendar, M.; Turyova, E.; Kasubova, I.; Laca, L.; Mikolajcik, P.; Kudelova, E.; Vanochova, A.; et al. Hypermethylated GRIA4, a Potential Biomarker for an Early Non-Invasive Detection of Metastasis of Clinically Known Colorectal Cancer. Front. Oncol. 2023, 13, 1205791. [Google Scholar] [CrossRef]
- Hauptman, N.; Skok, D.J.; Spasovska, E.; Boštjančič, E.; Glavač, D. Genes CEP55, FOXD3, FOXF2, GNAO1, GRIA4, and KCNA5 as Potential Diagnostic Biomarkers in Colorectal Cancer. BMC Med. Genom. 2019, 12, 54. [Google Scholar] [CrossRef]
- Vega-Benedetti, A.F.; Loi, E.; Moi, L.; Restivo, A.; Cabras, F.; Deidda, S.; Pretta, A.; Ziranu, P.; Orrù, S.; Scartozzi, M.; et al. Colorectal Cancer Promoter Methylation Alteration Affects the Expression of Glutamate Ionotropic Receptor AMPA Type Subunit 4 Alternative Isoforms Potentially Relevant in Colon Tissue. Hum. Cell 2022, 35, 310–319. [Google Scholar] [CrossRef]
- Collins, P.M.; Brennan, M.J.; Elliott, J.A.; Elwahab, S.A.; Barry, K.; Sweeney, K.; Malone, C.; Lowery, A.; Mclaughlin, R.; Kerin, M.J. Neoadjuvant Chemotherapy for Luminal a Breast Cancer: Factors Predictive of Histopathologic Response and Oncologic Outcome. Am. J. Surg. 2021, 222, 368–376. [Google Scholar] [CrossRef]
- Zhu, X.; Xue, D.; Liu, J.; Dong, F.; Li, Y.; Liu, Y. Nodal Is Involved in Chemoresistance of Renal Cell Carcinoma Cells via Regulation of ABCB1. J. Cancer 2021, 12, 2041–2049. [Google Scholar] [CrossRef] [PubMed]
- Koo, B.S.; Lee, S.H.; Kim, J.M.; Huang, S.; Kim, S.H.; Rho, Y.S.; Bae, W.J.; Kang, H.J.; Kim, Y.S.; Moon, J.H.; et al. Oct4 Is a Critical Regulator of Stemness in Head and Neck Squamous Carcinoma Cells. Oncogene 2015, 34, 2317–2324. [Google Scholar] [CrossRef] [PubMed]
- Jeon, H.-M.; Sohn, Y.-W.; Oh, S.-Y.; Kim, S.-H.; Beck, S.; Kim, S.; Kim, H. ID4 Imparts Chemoresistance and Cancer Stemness to Glioma Cells by Derepressing MiR-9*–Mediated Suppression of SOX2. Cancer Res. 2011, 71, 3410–3421. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.-J.; Deng, X.-G.; He, X.-Y.; Zhou, Y.; Yu, M.; Gao, W.-C.; Zeng, B.; Zhou, Q.-B.; Li, Z.-H.; Chen, R.-F. Knockdown of NANOG Enhances Chemosensitivity of Liver Cancer Cells to Doxorubicin by Reducing MDR1 Expression. Int. J. Oncol. 2014, 44, 2034–2040. [Google Scholar] [CrossRef]
- Fletcher, J.I.; Williams, R.T.; Henderson, M.J.; Norris, M.D.; Haber, M. ABC Transporters as Mediators of Drug Resistance and Contributors to Cancer Cell Biology. Drug Resist. Updates 2016, 26, 1–9. [Google Scholar] [CrossRef]
- Markadieu, N.; Delpire, E. Physiology and Pathophysiology of SLC12A1/2 Transporters. Pflügers Arch.-Eur. J. Physiol. 2013, 466, 91–105. [Google Scholar] [CrossRef]
- Teng, F.; Guo, M.; Liu, F.; Wang, C.; Dong, J.; Zhang, L.; Zou, Y.; Chen, R.; Sun, K.; Fu, H.; et al. Treatment with an SLC12A1 Antagonist Inhibits Tumorigenesis in a Subset of Hepatocellular Carcinomas. Oncotarget 2016, 7, 53571–53582. [Google Scholar] [CrossRef]
- Chen, Y.; Gu, D.; Wen, Y.; Yang, S.; Duan, X.; Lai, Y.; Yang, J.; Yuan, D.; Khan, A.; Wu, W.; et al. Identifying the Novel Key Genes in Renal Cell Carcinoma by Bioinformatics Analysis and Cell Experiments. Cancer Cell Int. 2020, 20, 331. [Google Scholar] [CrossRef]
- Januchowski, R.; Zawierucha, P.; Andrzejewska, M.; Ruciński, M.; Zabel, M. Microarray-Based Detection and Expression Analysis of ABC and SLC Transporters in Drug-Resistant Ovarian Cancer Cell Lines. Biomed. Pharmacother. 2013, 67, 240–245. [Google Scholar] [CrossRef]
- Kim, J.-E.; Choi, J.; Park, J.; Park, C.; Lee, S.M.; Park, S.E.; Song, N.; Chung, S.; Sung, H.; Han, W.; et al. Associations between Genetic Polymorphisms of Membrane Transporter Genes and Prognosis after Chemotherapy: Meta-Analysis and Finding from Seoul Breast Cancer Study (SEBCS). Pharmacogenomics J. 2018, 18, 633–645. [Google Scholar] [CrossRef]
- El-Ansari, R.; Craze, M.L.; Alfarsi, L.; Soria, D.; Diez-Rodriguez, M.; Nolan, C.C.; Ellis, I.O.; Rakha, E.A.; Green, A.R. The Combined Expression of Solute Carriers Is Associated with a Poor Prognosis in Highly Proliferative ER+ Breast Cancer. Breast Cancer Res. Treat. 2019, 175, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; He, J.; Liao, X.; Liang, T.; Zhu, J.; Wei, W.; He, Y.; Zhou, X.; Peng, T. A Comprehensive Analysis of the Diagnostic and Prognostic Value Associated with the SLC7A Family Members in Breast Cancer. Gland Surg. 2022, 11, 389–411. [Google Scholar] [CrossRef] [PubMed]
- Okabe, M.; Szakács, G.; Reimers, M.A.; Suzuki, T.; Hall, M.D.; Abe, T.; Weinstein, J.N.; Gottesman, M.M. Profiling SLCO and SLC22 Genes in the NCI-60 Cancer Cell Lines to Identify Drug Uptake Transporters. Mol. Cancer Ther. 2008, 7, 3081–3091. [Google Scholar] [CrossRef] [PubMed]
- Kushwaha, P.P.; Verma, S.S.; Shankar, E.; Lin, S.; Gupta, S. Role of Solute Carrier Transporters SLC25A17 and SLC27A6 in Acquired Resistance to Enzalutamide in Castration-resistant Prostate Cancer. Mol. Carcinog. 2022, 61, 397–407. [Google Scholar] [CrossRef]
- Okabe, M.; Unno, M.; Harigae, H.; Kaku, M.; Okitsu, Y.; Sasaki, T.; Mizoi, T.; Shiiba, K.; Takanaga, H.; Terasaki, T.; et al. Characterization of the Organic Cation Transporter SLC22A16: A Doxorubicin Importer. Biochem. Biophys. Res. Commun. 2005, 333, 754–762. [Google Scholar] [CrossRef]
- Zhao, W.; Wang, Y.; Yue, X. SLC22A16 Upregulation Is an Independent Unfavorable Prognostic Indicator in Gastric Cancer. Future Oncol. 2018, 14, 2139–2148. [Google Scholar] [CrossRef]
- Stepulak, A.; Rola, R.; Polberg, K.; Ikonomidou, C. Glutamate and Its Receptors in Cancer. J. Neural Transm. 2014, 121, 933–944. [Google Scholar] [CrossRef]
- Gynther, M.; Silvestri, I.P.; Hansen, J.C.; Hansen, K.B.; Malm, T.; Ishchenko, Y.; Larsen, Y.; Han, L.; Kayser, S.; Auriola, S.; et al. Augmentation of Anticancer Drug Efficacy in Murine Hepatocellular Carcinoma Cells by a Peripherally Acting Competitive N-Methyl-d-aspartate (NMDA) Receptor Antagonist. J. Med. Chem. 2017, 60, 9885–9904. [Google Scholar] [CrossRef]
- Choi, C.H.; Choi, J.-J.; Park, Y.-A.; Lee, Y.-Y.; Song, S.Y.; Sung, C.O.; Song, T.; Kim, M.-K.; Kim, T.-J.; Lee, J.-W.; et al. Identification of Differentially Expressed Genes According to Chemosensitivity in Advanced Ovarian Serous Adenocarcinomas: Expression of GRIA2 Predicts Better Survival. Br. J. Cancer 2012, 107, 91–99. [Google Scholar] [CrossRef]
- Tsuji, S.; Nakamura, S.; Shoda, K.; Yamada, T.; Shimazawa, M.; Nakayama, N.; Iwama, T.; Hara, H. NMDA Receptor Signaling Induces the Chemoresistance of Temozolomide via Upregulation of MGMT Expression in Glioblastoma Cells. J. Neuro-Oncol. 2022, 160, 375–388. [Google Scholar] [CrossRef]
- Greenbaum, D.; Colangelo, C.; Williams, K.; Gerstein, M. Comparing Protein Abundance and MRNA Expression Levels on a Genomic Scale. Genome Biol. 2003, 4, 117. [Google Scholar] [CrossRef] [PubMed]
- Contreras-Espinosa, L.; Alcaraz, N.; Rosa-Velázquez, I.A.D.L.; Díaz-Chávez, J.; Cabrera-Galeana, P.; Rebollar-Vega, R.; Reynoso-Noverón, N.; Maldonado-Martínez, H.A.; González-Barrios, R.; Montiel-Manríquez, R.; et al. Transcriptome Analysis Identifies GATA3-AS1 as a Long Noncoding RNA Associated with Resistance to Neoadjuvant Chemotherapy in Locally Advanced Breast Cancer Patients. J. Mol. Diagn. 2021, 23, 1306–1323. [Google Scholar] [CrossRef] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of Relative Gene Expression Data Using Real-Time Quantitative PCR and the 2−ΔΔCT Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Patro, R.; Duggal, G.; Love, M.I.; Irizarry, R.A.; Kingsford, C. Salmon: Fast and Bias-Aware Quantification of Transcript Expression Using Dual-Phase Inference. Nat. methods 2017, 14, 417–419. [Google Scholar] [CrossRef] [PubMed]
- Love, M.I.; Huber, W.; Anders, S. Moderated Estimation of Fold Change and Dispersion for RNA-Seq Data with DESeq2. Genome Biol. 2014, 15, 550. [Google Scholar] [CrossRef]
- Kamburov, A.; Wierling, C.; Lehrach, H.; Herwig, R. ConsensusPathDB—A Database for Integrating Human Functional Interaction Networks. Nucleic Acids Res. 2009, 37, D623–D628. [Google Scholar] [CrossRef]
- Wang, M.; Dai, M.; Wu, Y.; Yi, Z.; Li, Y.; Ren, G. Immunoglobulin Superfamily Member 10 Is a Novel Prognostic Biomarker for Breast Cancer. PeerJ 2020, 8, e10128. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Chemosensitive (n = 28) | Chemoresistant (n = 34) | p-Value |
|---|---|---|---|
| Age, yrs | |||
| Mean (range) | 49.7 (34–68) | 50.7 (34–68) | 0.865 a |
| BMI, kg/m2 | |||
| Mean (range) | 29.2 (19.7–40.2) | 29.5 (22.7–42.6) | 0.932 a |
| Tumor size, cm | |||
| Mean (range) | 6.6 (3–15) | 6.4 (1.5–14) | 0.691 a |
| Menopausal status | |||
| Pre | 13 (46.4%) | 15 (44.1%) | 1 b |
| Post | 15 (53.6%) | 19 (55.9%) | |
| Histological subtype | |||
| Ductal | 25 (89.3%) | 31 (91.2%) | 1 b |
| Lobular | 3 (10.7%) | 3 (8.8%) | |
| Clinical stage | |||
| II | 8 (28.6%) | 3 (8.8%) | 0.029 b,* |
| III | 20 (71.4%) | 31 (91.2%) | |
| Grade | |||
| Low | 4 (14.3%) | 4 (11.7%) | 0.249 b |
| Intermediate | 9 (32.1%) | 19 (55.9%) | |
| High | 15 (53.6%) | 12 (35.3%) | |
| KI67 | |||
| Low (<20%) | 2 (7.1%) | 11 (32.4%) | 0.089 b |
| High (≥20%) | 26 (92.9%) | 23 (67.6%) | |
| ER status | |||
| Positive | 21 (75%) | 34 (100%) | 0.007 b,* |
| Negative | 7 (25%) | 0 (0%) | |
| PR status | |||
| Positive | 33 (75%) | 34 (100%) | 0.389 b |
| Negative | 2 (25%) | 0 (0%) | |
| HER2 status | |||
| Positive | 13 (46.4%) | 3 (8.8%) | 0.002 b,* |
| Negative | 15 (53.6%) | 31 (91.2%) | |
| Subtype | |||
| Luminal A | 2 (7.1%) | 11 (32.4%) | 0.001 b,* |
| Luminal B HER2- | 13 (46.4%) | 20 (58.8%) | |
| Luminal B HER2+ | 13 (46.4%) | 3 (8.8%) | |
| Recurrence | |||
| Yes | 4 (14.3%) | 9 (26.5%) | 0.39 b |
| No | 24 (85.7%) | 25 (73.5%) | |
| Status | |||
| Death | 2 (7.1%) | 4 (11.8%) | 0.856 b |
| Alive | 26 (92.9%) | 30 (88.2%) |
| Bivariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age (≥50 vs. <50) | 4.50 | [1.12–23.07] | 0.045 * | 6.06 | [0.20–133.15] | 0.243 |
| Menopausal status (positive vs. negative) | 4.36 | [1.13–19.42] | 0.039 * | 1.22 | [0.07–34.70] | 0.891 |
| Tumor size (T3/T4 vs. T1/T2) | 1.25 | [0.28–4.99] | 0.756 | |||
| Clinical stage (III vs. II) | 0.80 | [0.20–3.57] | 0.756 | |||
| Luminal A (positive vs. negative) | 0.47 | [0.07–3.94] | 0.440 | |||
| Luminal B HER2- (positive vs. negative) | 0.40 | [0.08–1.59] | 0.215 | |||
| Luminal B HER2+ (positive vs. negative) | 6.5 | [1.07–125.78] | 0.089 | |||
| Resistance (positive vs. negative) | 0.13 | [0.02–0.60] | 0.017 * | 0.09 | [0.01–0.48] | 0.011 * |
| Biomarker | Detection Method | AUC (95% Cl) | p-Value | Cut-Off | Sensitivity (95% Cl) | Specificity (95% Cl) |
|---|---|---|---|---|---|---|
| SLC12A1 | Real-time PCR | 0.70 (0.54–0.85) | 0.026 | 0.05 | 41.67 (24.47–61.17) | 90.91 (72.19–98.38) |
| GLUR4 | IHC | 0.77 (0.58–0.96) | 0.019 | 1.5 | 88.24 (65.66–97.91) | 54.55 (28.01–78.73) |
| OR | 95% CI | p-Value | |
|---|---|---|---|
| Age (≥50 vs. <50) | 2.46 | [0.44–19.66] | 0.335 |
| Tumor size (T3/T4 vs. T1/T2) | 0.21 | [0.01–1.55] | 0.185 |
| Lymph nodes (N1, N2, N3 vs. N0) | 11.40 | [1.18–260.86] | 0.053 |
| Clinical stage (III vs. II) | 0.57 | [0.03–4.81] | 0.643 |
| Luminal A (positive vs. negative) | 0.90 | [0.17–5.43] | 0.901 |
| Luminal B HER2- (positive vs. negative) | 1.50 | [0.28–8.16] | 0.630 |
| Luminal B HER2+ (positive vs. negative) | 0.37 | [0.01–10.16] | 0.500 |
| Resistance (positive vs. negative) | 9.00 | [1.53–77.22] | 0.023 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Justo-Garrido, M.; López-Saavedra, A.; Alcaraz, N.; Cortés-González, C.C.; Oñate-Ocaña, L.F.; Caro-Sánchez, C.H.S.; Castro-Hernández, C.; Arriaga-Canon, C.; Díaz-Chávez, J.; Herrera, L.A. Association of SLC12A1 and GLUR4 Ion Transporters with Neoadjuvant Chemoresistance in Luminal Locally Advanced Breast Cancer. Int. J. Mol. Sci. 2023, 24, 16104. https://doi.org/10.3390/ijms242216104
Justo-Garrido M, López-Saavedra A, Alcaraz N, Cortés-González CC, Oñate-Ocaña LF, Caro-Sánchez CHS, Castro-Hernández C, Arriaga-Canon C, Díaz-Chávez J, Herrera LA. Association of SLC12A1 and GLUR4 Ion Transporters with Neoadjuvant Chemoresistance in Luminal Locally Advanced Breast Cancer. International Journal of Molecular Sciences. 2023; 24(22):16104. https://doi.org/10.3390/ijms242216104
Chicago/Turabian StyleJusto-Garrido, Montserrat, Alejandro López-Saavedra, Nicolás Alcaraz, Carlo C. Cortés-González, Luis F. Oñate-Ocaña, Claudia Haydee Sarai Caro-Sánchez, Clementina Castro-Hernández, Cristian Arriaga-Canon, José Díaz-Chávez, and Luis A. Herrera. 2023. "Association of SLC12A1 and GLUR4 Ion Transporters with Neoadjuvant Chemoresistance in Luminal Locally Advanced Breast Cancer" International Journal of Molecular Sciences 24, no. 22: 16104. https://doi.org/10.3390/ijms242216104
APA StyleJusto-Garrido, M., López-Saavedra, A., Alcaraz, N., Cortés-González, C. C., Oñate-Ocaña, L. F., Caro-Sánchez, C. H. S., Castro-Hernández, C., Arriaga-Canon, C., Díaz-Chávez, J., & Herrera, L. A. (2023). Association of SLC12A1 and GLUR4 Ion Transporters with Neoadjuvant Chemoresistance in Luminal Locally Advanced Breast Cancer. International Journal of Molecular Sciences, 24(22), 16104. https://doi.org/10.3390/ijms242216104