
Searching for Biomarkers in the Blood of Patients at Risk of Developing Parkinson’s Disease at the Prodromal Stage

 , , and
, , and 
Abstract
:1. Introduction
2. Results
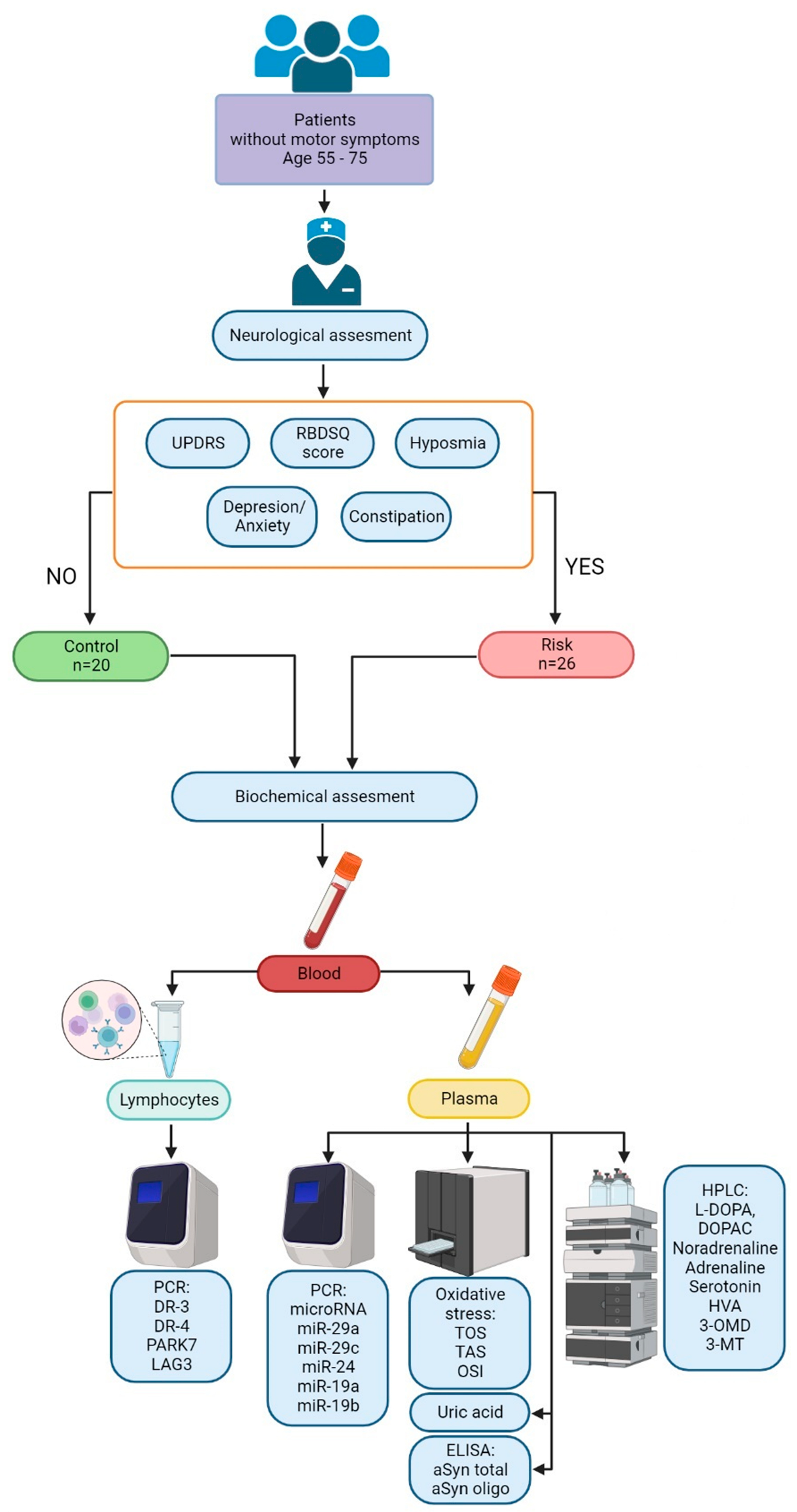
2.1. Selection and Examination of Patients at Risk for Developing Parkinson’s Disease at the Prodromal Stage
2.2. Biochemical and Molecular-Biological Data on Changes in the Blood of Patients at Risk of Developing Parkinson’s Disease and in Controls
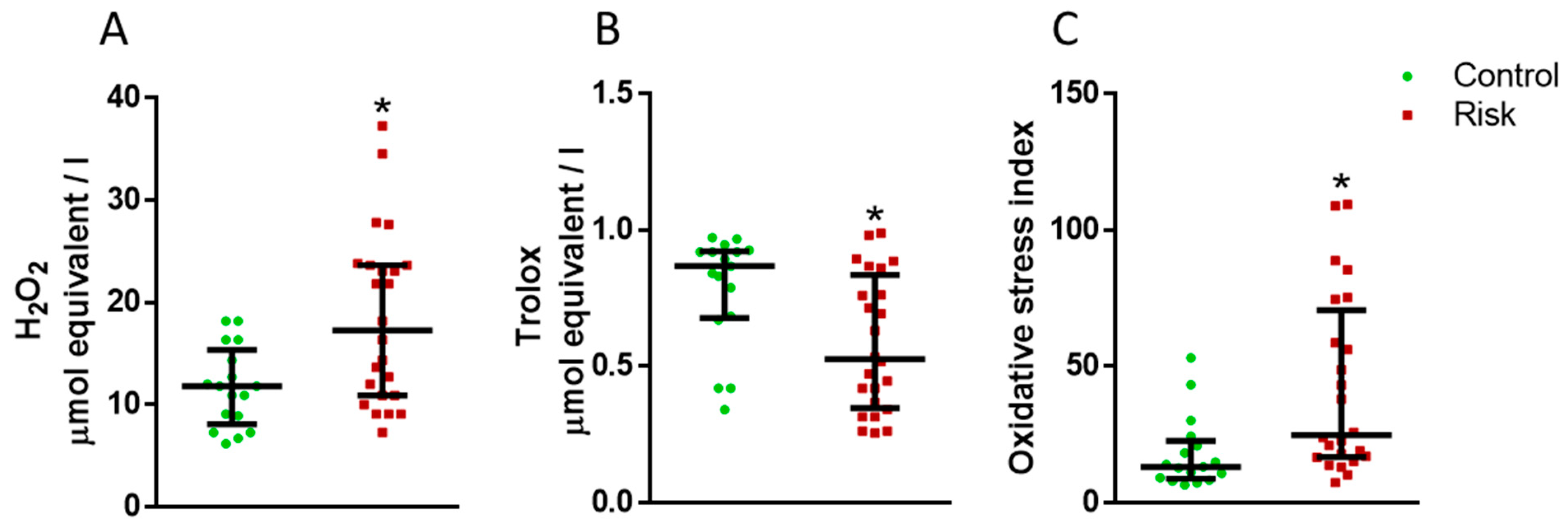
2.2.1. Markers of Oxidative Stress in Plasma
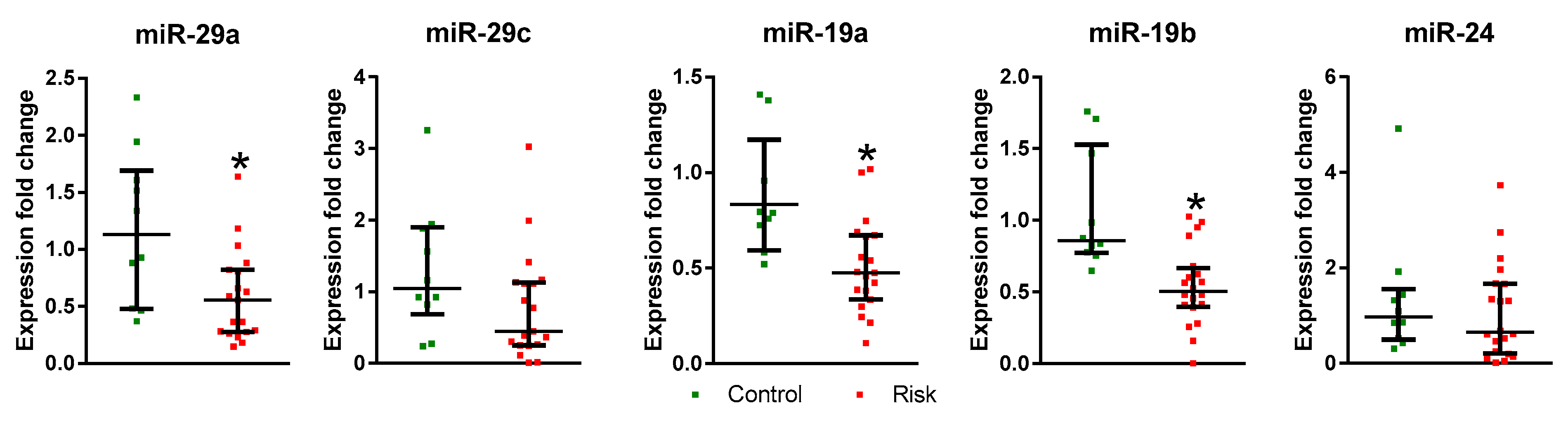
2.2.2. microRNA Expression in the Plasma of Patients at Risk of Developing Parkinson’s Disease and in the Controls
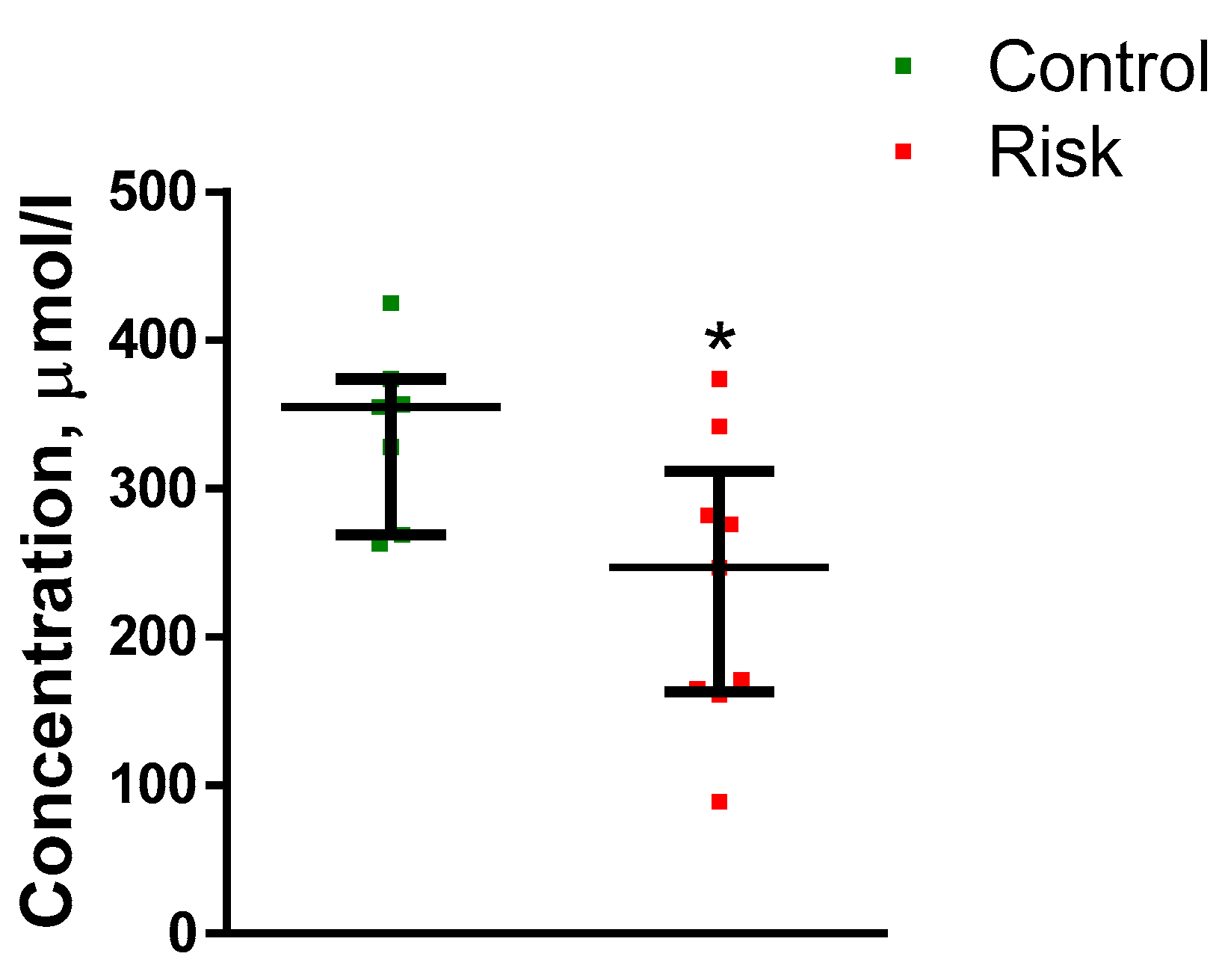
2.2.3. Urates in Plasma
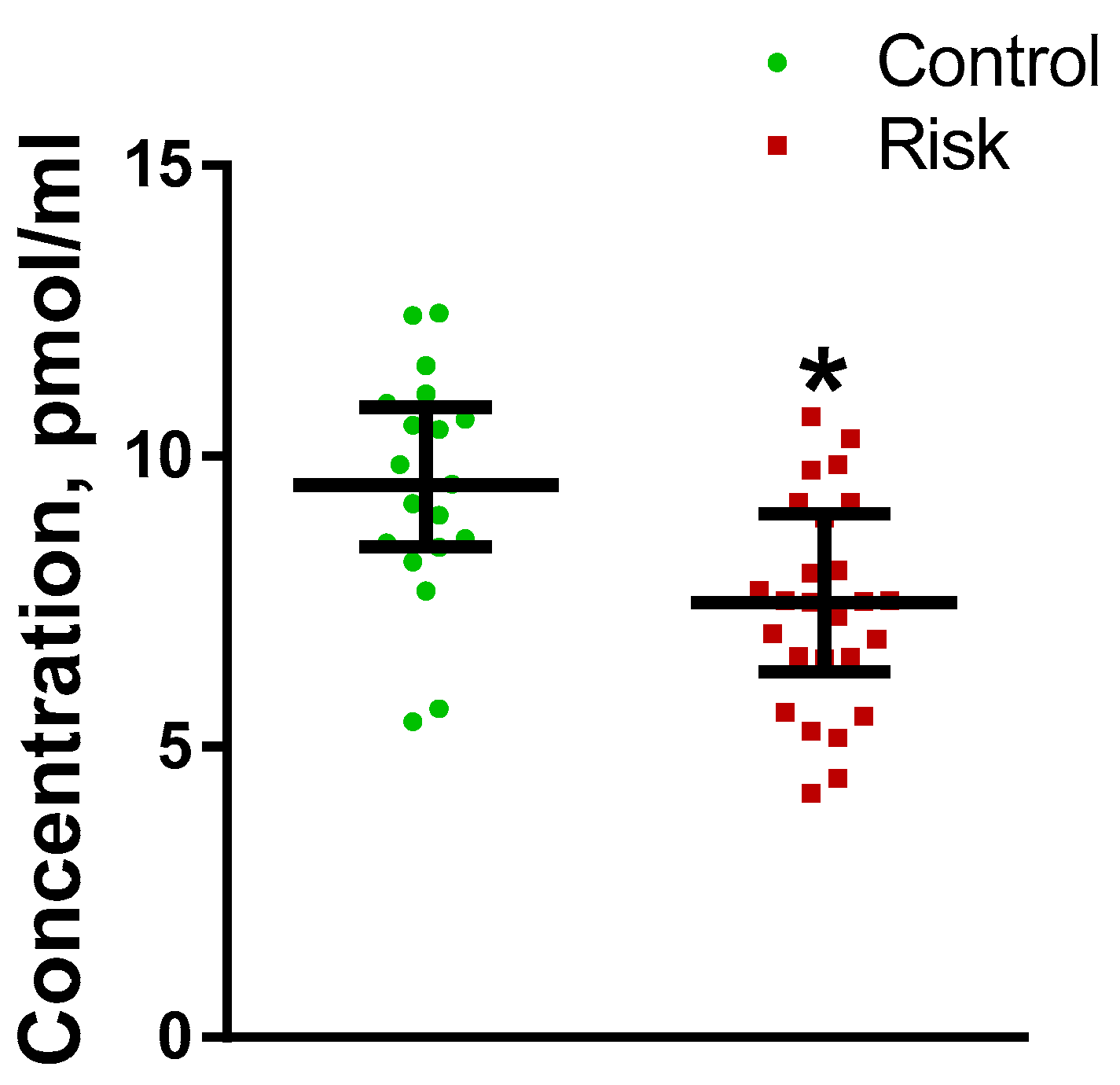
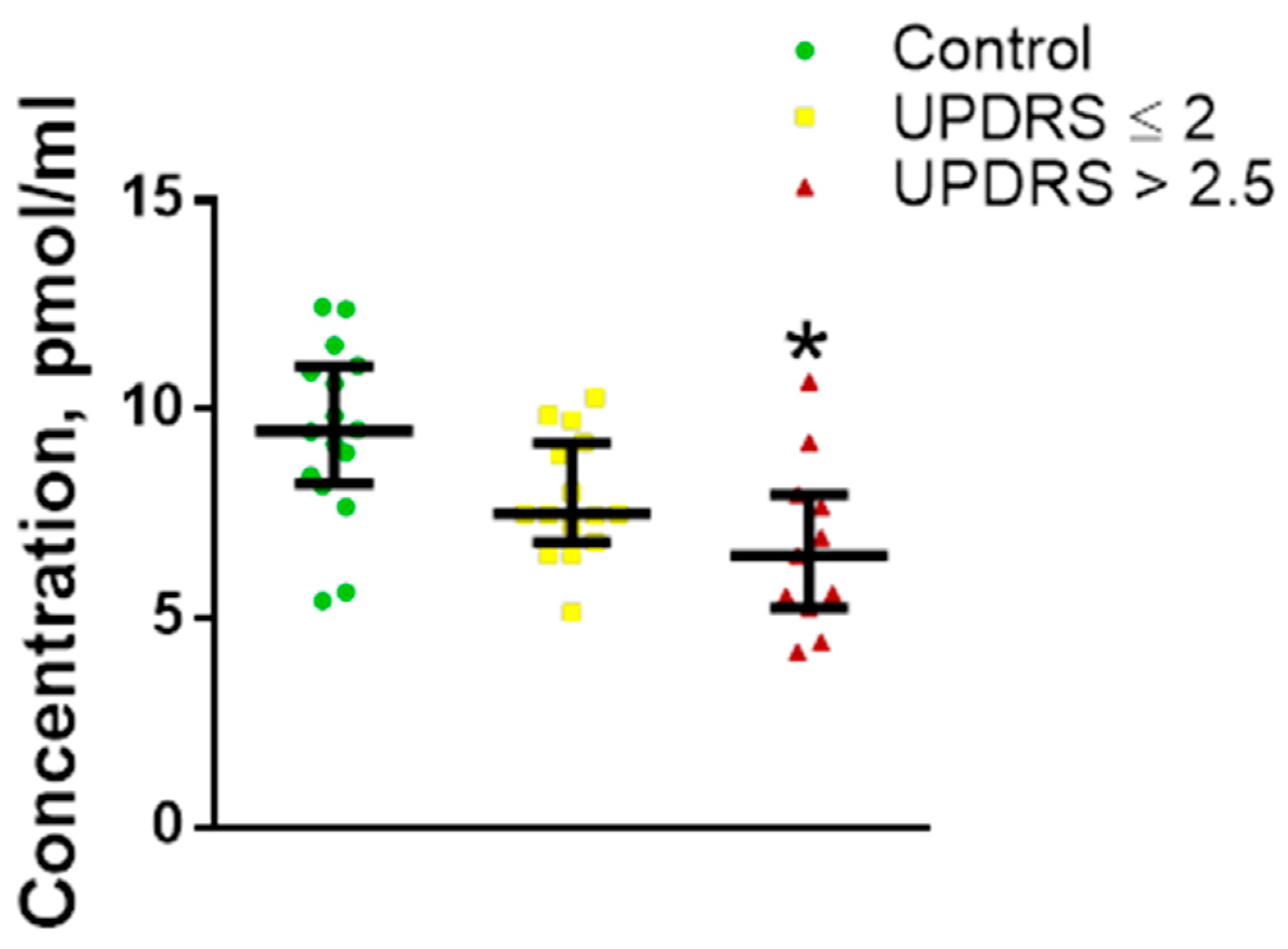
2.2.4. Monoamines and Their Metabolites in Plasma
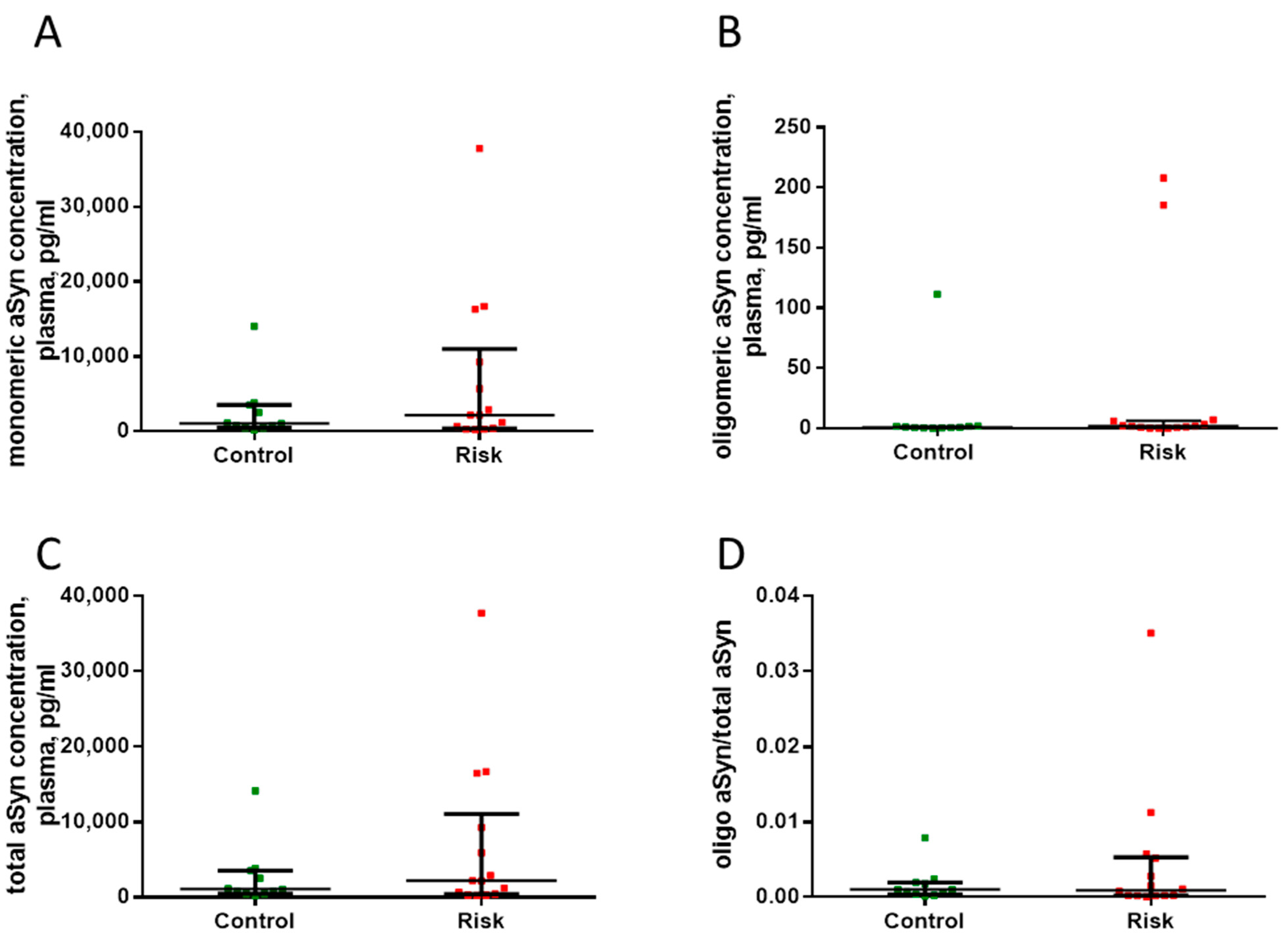
2.3. Quantification of Total, Monomeric, and Oligomeric Plasma α-Synuclein in Patients at Risk for Developing Parkinson’s Disease
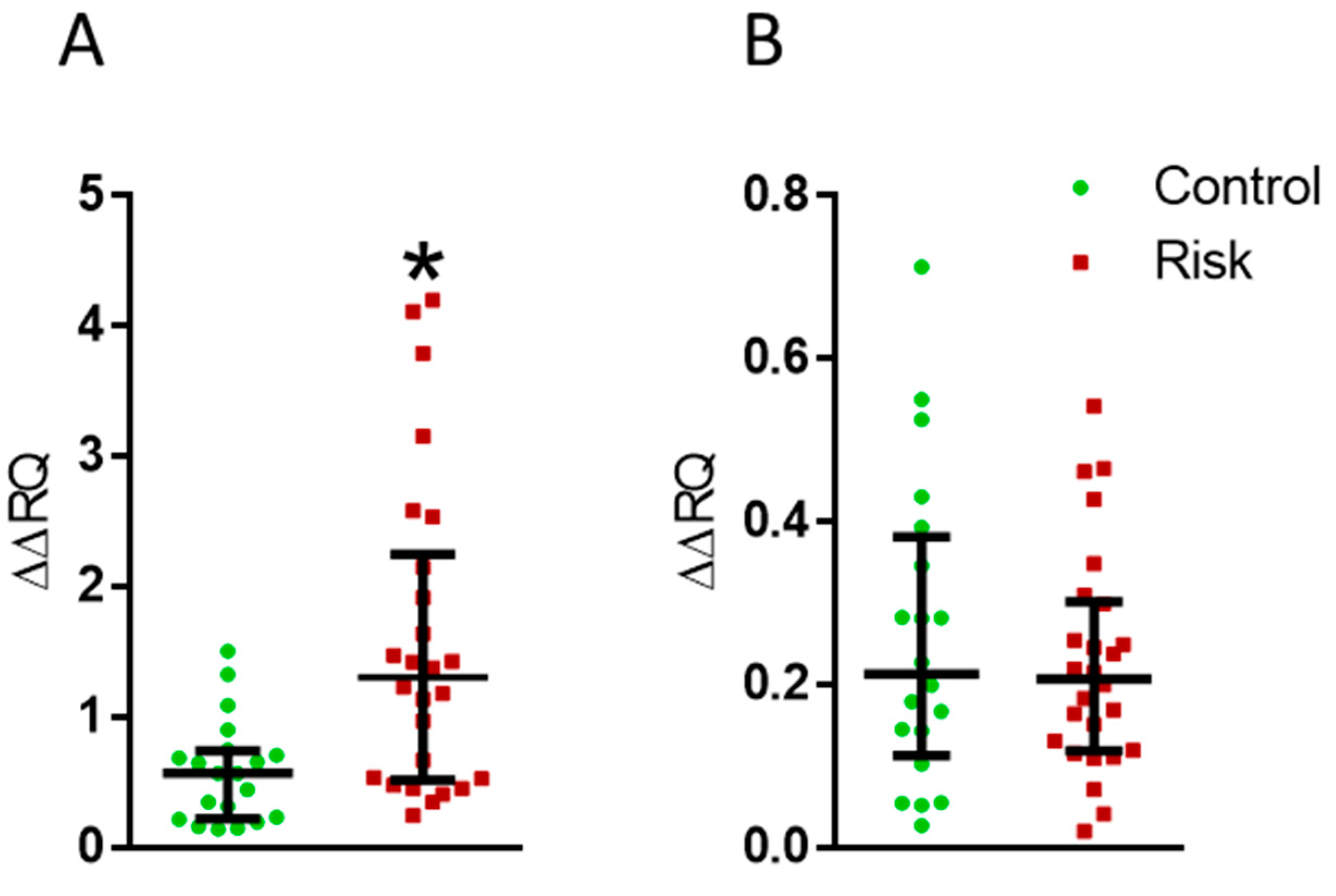
2.4. Dopamine Receptor Genes in Lymphocytes
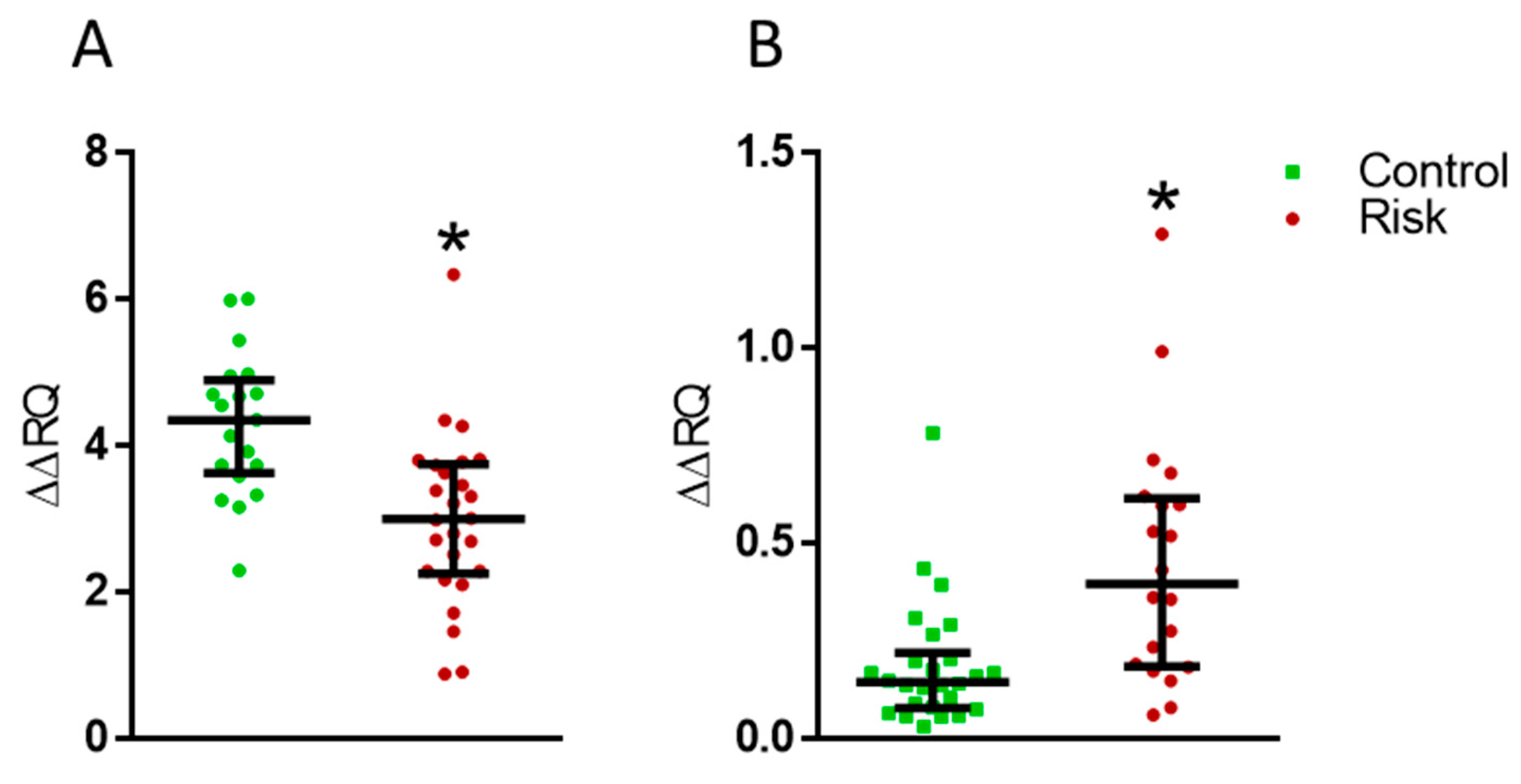
2.5. Expression of the PARK7 and LAG3 Genes in Lymphocytes
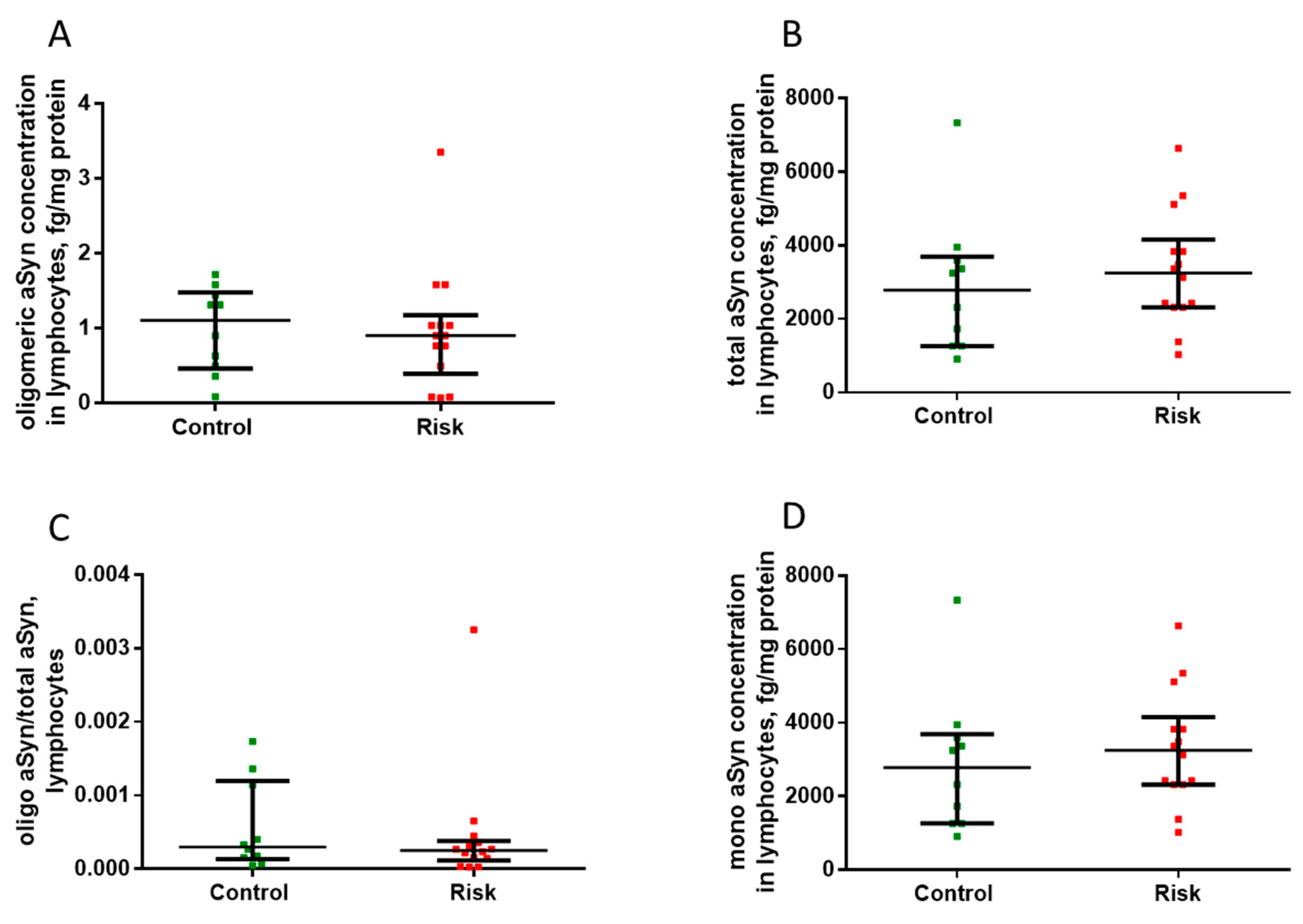
2.6. Alpha-Synucleins in Lymphocytes
3. Discussion
3.1. Selection of Patients at Risk for Developing Parkinson’s Disease at the Prodromal Stage: Methodology and Results
3.2. Search for Blood Biomarkers in Patients at Risk of Developing Parkinson’s Disease at the Prodromal Stage: Methodology and Results
3.2.1. Plasma Monoamines and Their Metabolites in Patients at Risk
3.2.2. Plasma Urates in Patients at Risk of Developing Parkinson’s Disease
3.2.3. Plasma Oxidative Stress Index in Patients at Risk of Developing Parkinson’s Disease
3.2.4. Plasma Synucleins in Patients at Risk of Developing Parkinson’s Disease
3.2.5. MicroRNAs in Plasma in Patients at Risk of Developing Parkinson’s Disease
3.2.6. Expression of Dopamine Receptor Genes in Lymphocytes in Patients at Risk of Developing Parkinson’s Disease
3.2.7. Changes in the Expression of PARK7 and LAG3 in Lymphocytes in Patients at Risk of Developing Parkinson’s Disease
4. Materials and Methods
4.1. Patients
4.2. Approaches to the Neurological Examination of Patients
4.3. Criteria for the Inclusion of Patients in the Risk Group
4.4. Criteria for the Inclusion of Patients in the Control Group
4.5. Criteria for the Exclusion of Patients from the Trial
4.6. Additional Examination of Patients at Risk and of Patients in Control Group
4.6.1. Cognitive Function
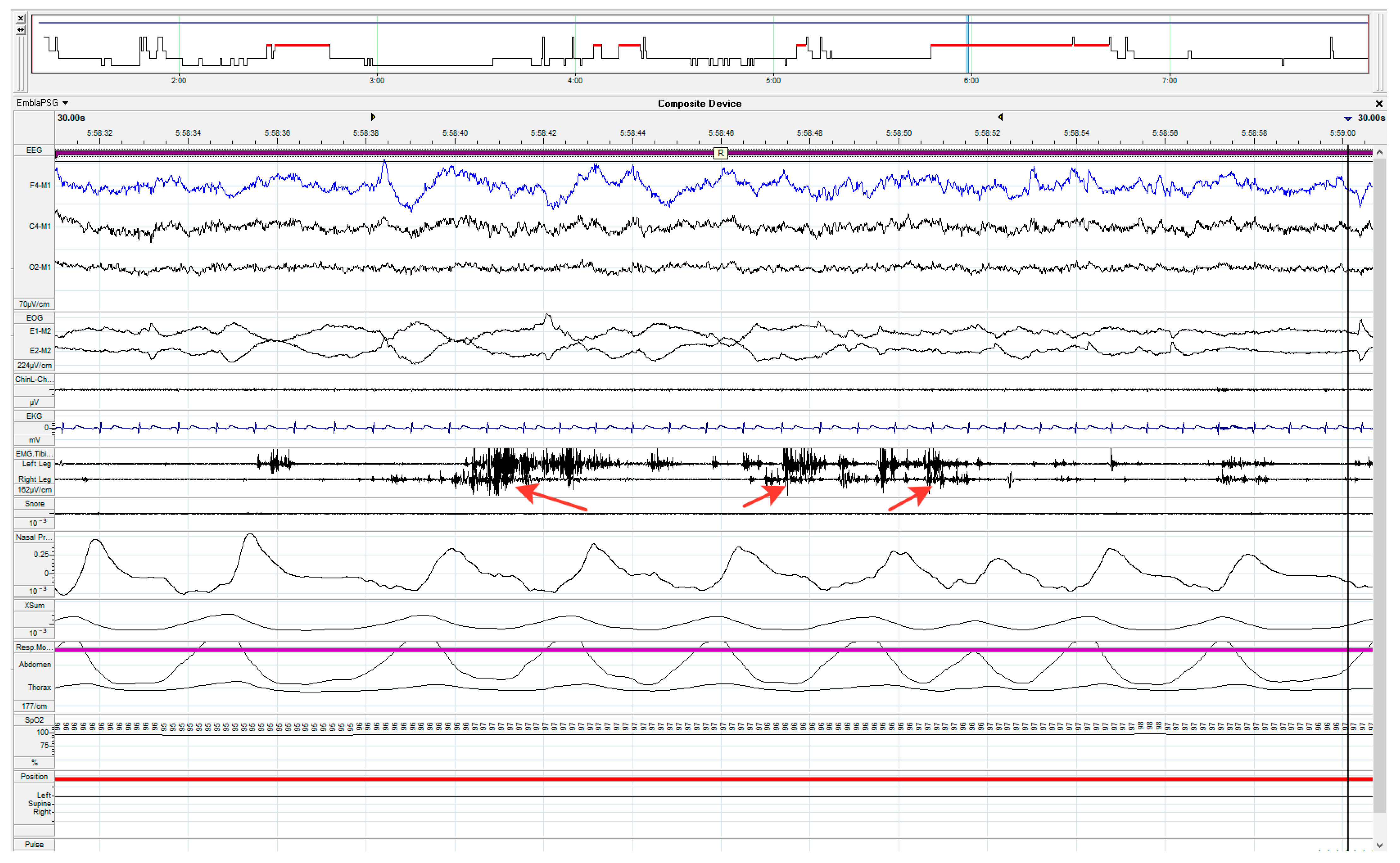
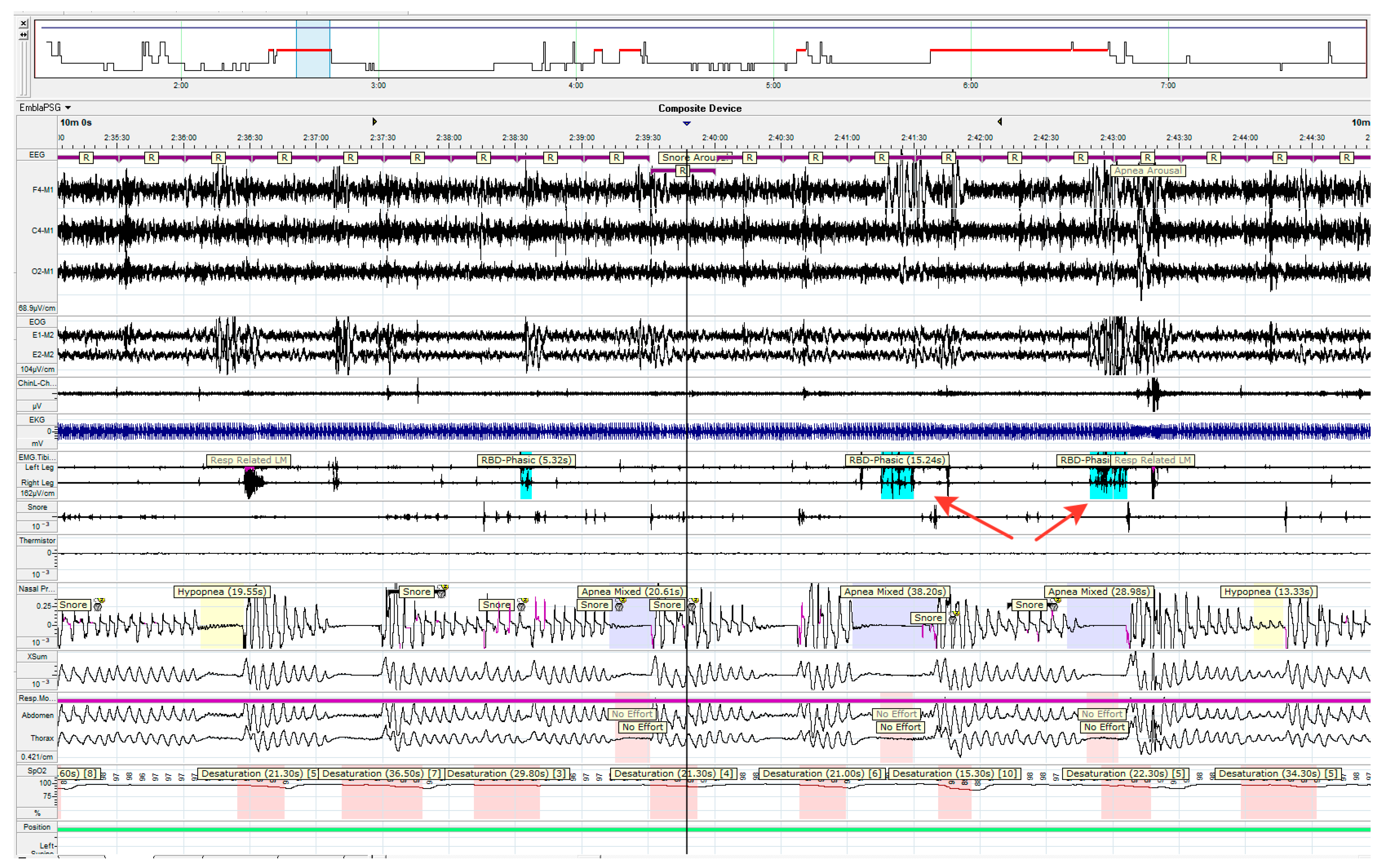
4.6.2. Polysomnography Study
4.7. The Collection and Processing of Blood
4.8. High-Performance Liquid Chromatography
4.9. Determination of the Oxidative Stress Index
4.10. Measurement of Urates in Plasma
4.11. Isolation of Total RNA from Lymphocytes
4.12. cDNA Synthesis
4.13. PCR in Real Time
4.14. Isolation of microRNA from Plasma and cDNA Synthesis
4.15. PCR of microRNA
- Measurement of α-synuclein and its derivatives in plasma and lymphocytes
- Statistical analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Tysnes, O.-B.; Storstein, A. Epidemiology of Parkinson’s Disease. J. Neural. Transm. 2017, 124, 901–905. [Google Scholar] [CrossRef]
- Fahn, S.; Oakes, D.; Shoulson, I.; Kieburtz, K.; Rudolph, A.; Lang, A.; Olanow, C.W.; Tanner, C.; Marek, K. Parkinson Study Group Levodopa and the Progression of Parkinson’s Disease. N. Engl. J. Med. 2004, 351, 2498–2508. [Google Scholar] [CrossRef] [PubMed]
- Agid, Y. Parkinson’s Disease: Pathophysiology. Lancet 1991, 337, 1321–1324. [Google Scholar] [CrossRef] [PubMed]
- Blesa, J.; Trigo-Damas, I.; Dileone, M.; Rey, N.L.-G.D.; Hernandez, L.F.; Obeso, J.A. Compensatory Mechanisms in Parkinson’s Disease: Circuits Adaptations and Role in Disease Modification. Exp. Neurol. 2017, 298, 148–161. [Google Scholar] [CrossRef] [PubMed]
- Ugrumov, M. Development of Early Diagnosis of Parkinson’s Disease: Illusion or Reality? CNS Neurosci. Ther. 2020, 26, 997–1009. [Google Scholar] [CrossRef] [PubMed]
- Espay, A.J.; Kalia, L.V.; Gan-Or, Z.; Williams-Gray, C.H.; Bedard, P.L.; Rowe, S.M.; Morgante, F.; Fasano, A.; Stecher, B.; Kauffman, M.A.; et al. Disease Modification and Biomarker Development in Parkinson Disease: Revision or Reconstruction? Neurology 2020, 94, 481–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaasinen, V.; Vahlberg, T. Striatal Dopamine in Parkinson Disease: A Meta-Analysis of Imaging Studies. Ann. Neurol. 2017, 82, 873–882. [Google Scholar] [CrossRef]
- Seibyl, J.P.; Kuo, P. What Is the Role of Dopamine Transporter Imaging in Parkinson Prevention Clinical Trials? Neurology 2022, 99, 61–67. [Google Scholar] [CrossRef]
- Goldstein, D.S. Dysautonomia in Parkinson Disease. Compr. Physiol. 2014, 4, 805–826. [Google Scholar] [CrossRef] [Green Version]
- Braak, H.; Tredici, K.D.; Rüb, U.; de Vos, R.A.I.; Steur, E.N.H.J.; Braak, E. Staging of Brain Pathology Related to Sporadic Parkinson’s Disease. Neurobiol. Aging 2003, 24, 197–211. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS Clinical Diagnostic Criteria for Parkinson’s Disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef] [PubMed]
- Mahlknecht, P.; Seppi, K.; Poewe, W. The Concept of Prodromal Parkinson’s Disease. J. Park. Dis. 2015, 5, 681–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Postuma, R.B.; Berg, D. Advances in Markers of Prodromal Parkinson Disease. Nat. Rev. Neurol. 2016, 12, 622–634. [Google Scholar] [CrossRef]
- Berg, D.; Postuma, R.B.; Adler, C.H.; Bloem, B.R.; Chan, P.; Dubois, B.; Gasser, T.; Goetz, C.G.; Halliday, G.; Joseph, L.; et al. MDS Research Criteria for Prodromal Parkinson’s Disease. Mov. Disord. 2015, 30, 1600–1611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pont-Sunyer, C.; Hotter, A.; Gaig, C.; Seppi, K.; Compta, Y.; Katzenschlager, R.; Mas, N.; Hofeneder, D.; Brücke, T.; Bayés, A.; et al. The Onset of Nonmotor Symptoms in Parkinson’s Disease (the ONSET PD Study). Mov. Disord. 2015, 30, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Izawa, M.O.; Miwa, H.; Kajimoto, Y.; Kondo, T. Combination of Transcranial Sonography, Olfactory Testing, and MIBG Myocardial Scintigraphy as a Diagnostic Indicator for Parkinson’s Disease. Eur. J. Neurol. 2012, 19, 411–416. [Google Scholar] [CrossRef]
- Shin, H.Y.; Joo, E.Y.; Kim, S.T.; Dhong, H.-J.; Cho, J.W. Comparison Study of Olfactory Function and Substantia Nigra Hyperechogenicity in Idiopathic REM Sleep Behavior Disorder, Parkinson’s Disease and Normal Control. Neurol. Sci. 2013, 34, 935–940. [Google Scholar] [CrossRef]
- Eller, M.; Williams, D.R. Biological Fluid Biomarkers in Neurodegenerative Parkinsonism. Nat. Rev. Neurol. 2009, 5, 561–570. [Google Scholar] [CrossRef]
- Le, W.; Dong, J.; Li, S.; Korczyn, A.D. Can Biomarkers Help the Early Diagnosis of Parkinson’s Disease? Neurosci. Bull. 2017, 33, 535–542. [Google Scholar] [CrossRef]
- Kim, A.; Nigmatullina, R.; Zalyalova, Z.; Soshnikova, N.; Krasnov, A.; Vorobyeva, N.; Georgieva, S.; Kudrin, V.; Narkevich, V.; Ugrumov, M. Upgraded Methodology for the Development of Early Diagnosis of Parkinson’s Disease Based on Searching Blood Markers in Patients and Experimental Models. Mol. Neurobiol. 2019, 56, 3437–3450. [Google Scholar] [CrossRef]
- Parnetti, L.; Gaetani, L.; Eusebi, P.; Paciotti, S.; Hansson, O.; El-Agnaf, O.; Mollenhauer, B.; Blennow, K.; Calabresi, P. CSF and Blood Biomarkers for Parkinson’s Disease. Lancet Neurol. 2019, 18, 573–586. [Google Scholar] [CrossRef] [PubMed]
- Bogdanov, V.; Kim, A.; Nodel, M.; Pavlenko, T.; Pavlova, E.; Blokhin, V.; Chesnokova, N.; Ugrumov, M. A Pilot Study of Changes in the Level of Catecholamines and the Activity of α-2-Macroglobulin in the Tear Fluid of Patients with Parkinson’s Disease and Parkinsonian Mice. Int. J. Mol. Sci. 2021, 22, 4736. [Google Scholar] [CrossRef] [PubMed]
- Berg, D.; Borghammer, P.; Fereshtehnejad, S.-M.; Heinzel, S.; Horsager, J.; Schaeffer, E.; Postuma, R.B. Prodromal Parkinson Disease Subtypes-Key to Understanding Heterogeneity. Nat. Rev. Neurol. 2021, 17, 349–361. [Google Scholar] [CrossRef] [PubMed]
- Gusev, E.I.; Blokhin, V.E.; Vartanov, S.A.; Martynov, M.Y.; Katunina, E.A.; Alesenko, A.V.; Denisova, I.A.; Pavlova, E.N.; Polterovich, V.M.; Kucheryanu, V.G.; et al. Development of early diagnosis of Parkinson’s disease and comprehensive economic analysis of the effect of its implementation. Zhurnal Nevrol. Psikhiatrii Im. S.S. Korsakova 2021, 121, 9–20. [Google Scholar] [CrossRef]
- Antoniades, C.A.; Barker, R.A. The Search for Biomarkers in Parkinson’s Disease: A Critical Review. Expert Rev. Neurother. 2008, 8, 1841–1852. [Google Scholar] [CrossRef]
- Yu, Z.; Stewart, T.; Aasly, J.; Shi, M.; Zhang, J. Combining Clinical and Biofluid Markers for Early Parkinson’s Disease Detection. Ann. Clin. Transl. Neurol. 2018, 5, 109–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, T.; Le, W. Biomarkers for Parkinson’s Disease: How Good Are They? Neurosci. Bull. 2020, 36, 183–194. [Google Scholar] [CrossRef]
- Boeve, B.F. Idiopathic REM Sleep Behaviour Disorder in the Development of Parkinson’s Disease. Lancet Neurol. 2013, 12, 469–482. [Google Scholar] [CrossRef] [Green Version]
- Iranzo, A. Parkinson Disease and Sleep: Sleep-Wake Changes in the Premotor Stage of Parkinson Disease; Impaired Olfaction and Other Prodromal Features. Curr. Neurol. Neurosci. Rep. 2013, 13, 373. [Google Scholar] [CrossRef]
- Howell, M.J.; Schenck, C.H. Rapid Eye Movement Sleep Behavior Disorder and Neurodegenerative Disease. JAMA Neurol. 2015, 72, 707–712. [Google Scholar] [CrossRef]
- Iranzo, A.; Gelpi, E.; Tolosa, E.; Molinuevo, J.L.; Serradell, M.; Gaig, C.; Santamaria, J. Neuropathology of Prodromal Lewy Body Disease. Mov. Disord. 2014, 29, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Yoon, I.-Y.; Kim, J.-M.; Jeong, S.-H.; Kim, K.W.; Shin, Y.-K.; Kim, B.S.; Kim, S.E. The Implication of Nigrostriatal Dopaminergic Degeneration in the Pathogenesis of REM Sleep Behavior Disorder. Eur. J. Neurol. 2010, 17, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Iranzo, A.; Isetta, V.; Molinuevo, J.L.; Serradell, M.; Navajas, D.; Farre, R.; Santamaria, J. Electroencephalographic Slowing Heralds Mild Cognitive Impairment in Idiopathic REM Sleep Behavior Disorder. Sleep Med. 2010, 11, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Heller, J.; Brcina, N.; Dogan, I.; Holtbernd, F.; Romanzetti, S.; Schulz, J.B.; Schiefer, J.; Reetz, K. Brain Imaging Findings in Idiopathic REM Sleep Behavior Disorder (RBD)—A Systematic Review on Potential Biomarkers for Neurodegeneration. Sleep Med. Rev. 2017, 34, 23–33. [Google Scholar] [CrossRef]
- Rupprecht, S.; Walther, B.; Gudziol, H.; Steenbeck, J.; Freesmeyer, M.; Witte, O.W.; Günther, A.; Schwab, M. Clinical Markers of Early Nigrostriatal Neurodegeneration in Idiopathic Rapid Eye Movement Sleep Behavior Disorder. Sleep Med. 2013, 14, 1064–1070. [Google Scholar] [CrossRef] [PubMed]
- Sringean, J.; Stefani, A.; Marini, K.; Bergmann, M.; Werkmann, M.; Holzknecht, E.; Marzi, R.D.; Brandauer, E.; Hackner, H.; Djamshidian, A.; et al. Rapid Eye Movement Sleep Behavior Disorder and Rapid Eye Movement Sleep without Atonia Are More Frequent in Advanced versus Early Parkinson’s Disease. Sleep 2021, 44, zsab067. [Google Scholar] [CrossRef]
- Fereshtehnejad, S.-M.; Yao, C.; Pelletier, A.; Montplaisir, J.Y.; Gagnon, J.-F.; Postuma, R.B. Evolution of Prodromal Parkinson’s Disease and Dementia with Lewy Bodies: A Prospective Study. Brain 2019, 142, 2051–2067. [Google Scholar] [CrossRef]
- Horsager, J.; Andersen, K.B.; Knudsen, K.; Skjærbæk, C.; Fedorova, T.D.; Okkels, N.; Schaeffer, E.; Bonkat, S.K.; Geday, J.; Otto, M.; et al. Brain-First versus Body-First Parkinson’s Disease: A Multimodal Imaging Case-Control Study. Brain 2020, 143, 3077–3088. [Google Scholar] [CrossRef]
- Borghammer, P.; Berge, N.V.D. Brain-First versus Gut-First Parkinson’s Disease: A Hypothesis. J. Park. Dis. 2019, 9, S281–S295. [Google Scholar] [CrossRef] [Green Version]
- Borghammer, P.; Just, M.K.; Horsager, J.; Skjærbæk, C.; Raunio, A.; Kok, E.H.; Savola, S.; Murayama, S.; Saito, Y.; Myllykangas, L.; et al. A Postmortem Study Suggests a Revision of the Dual-Hit Hypothesis of Parkinson’s Disease. NPJ Park. Dis. 2022, 8, 166. [Google Scholar] [CrossRef]
- McKenna, D.; Peever, J. Degeneration of Rapid Eye Movement Sleep Circuitry Underlies Rapid Eye Movement Sleep Behavior Disorder. Mov. Disord. 2017, 32, 636–644. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, K.; Fedorova, T.D.; Horsager, J.; Andersen, K.B.; Skjærbæk, C.; Berg, D.; Schaeffer, E.; Brooks, D.J.; Pavese, N.; Berge, N.V.D.; et al. Asymmetric Dopaminergic Dysfunction in Brain-First versus Body-First Parkinson’s Disease Subtypes. J. Park. Dis. 2021, 11, 1677–1687. [Google Scholar] [CrossRef] [PubMed]
- Wenning, G.K.; Stankovic, I.; Vignatelli, L.; Fanciulli, A.; Calandra-Buonaura, G.; Seppi, K.; Palma, J.; Meissner, W.G.; Krismer, F.; Berg, D.; et al. The Movement Disorder Society Criteria for the Diagnosis of Multiple System Atrophy. Mov. Disord. 2022, 37, 1131–1148. [Google Scholar] [CrossRef]
- Ferman, T.J.; Smith, G.E.; Kantarci, K.; Boeve, B.F.; Pankratz, V.S.; Dickson, D.W.; Graff-Radford, N.R.; Wszolek, Z.; Gerpen, J.V.; Uitti, R.; et al. Nonamnestic Mild Cognitive Impairment Progresses to Dementia with Lewy Bodies. Neurology 2013, 81, 2032–2038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonanni, L.; Perfetti, B.; Bifolchetti, S.; Taylor, J.-P.; Franciotti, R.; Parnetti, L.; Thomas, A.; Onofrj, M. Quantitative Electroencephalogram Utility in Predicting Conversion of Mild Cognitive Impairment to Dementia with Lewy Bodies. Neurobiol. Aging 2015, 36, 434–445. [Google Scholar] [CrossRef] [Green Version]
- Claassen, D.O.; Josephs, K.A.; Ahlskog, J.E.; Silber, M.H.; Tippmann-Peikert, M.; Boeve, B.F. REM Sleep Behavior Disorder Preceding Other Aspects of Synucleinopathies by up to Half a Century. Neurology 2010, 75, 494–499. [Google Scholar] [CrossRef] [Green Version]
- Sixel-Döring, F.; Schweitzer, M.; Mollenhauer, B.; Trenkwalder, C. Polysomnographic Findings, Video-Based Sleep Analysis and Sleep Perception in Progressive Supranuclear Palsy. Sleep Med. 2009, 10, 407–415. [Google Scholar] [CrossRef]
- Nomura, T.; Inoue, Y.; Takigawa, H.; Nakashima, K. Comparison of REM Sleep Behaviour Disorder Variables between Patients with Progressive Supranuclear Palsy and Those with Parkinson’s Disease. Park. Relat. Disord. 2012, 18, 394–396. [Google Scholar] [CrossRef]
- Boini, S.Y.; Mahale, R.; Donaparthi, S.; Kamble, N.; Holla, V.V.; Pal, P.K.; Kutty, B.; Yadav, R. Sleep Architecture in Progressive Supranuclear Palsy: A Video-Polysomnography Study. Ann. Indian Acad. Neurol. 2022, 25, 858–863. [Google Scholar] [CrossRef]
- Lotankar, S.; Prabhavalkar, K.S.; Bhatt, L.K. Biomarkers for Parkinson’s Disease: Recent Advancement. Neurosci. Bull. 2017, 33, 585–597. [Google Scholar] [CrossRef]
- Meles, S.K.; Oertel, W.H.; Leenders, K.L. Circuit Imaging Biomarkers in Preclinical and Prodromal Parkinson’s Disease. Mol. Med. 2021, 27, 111. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.S.; Holmes, C.; Lopez, G.J.; Wu, T.; Sharabi, Y. Cerebrospinal Fluid Biomarkers of Central Dopamine Deficiency Predict Parkinson’s Disease. Park. Relat. Disord. 2018, 50, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Kustrimovic, N.; Rasini, E.; Legnaro, M.; Bombelli, R.; Aleksic, I.; Blandini, F.; Comi, C.; Mauri, M.; Minafra, B.; Riboldazzi, G.; et al. Dopaminergic Receptors on CD4+ T Naive and Memory Lymphocytes Correlate with Motor Impairment in Patients with Parkinson’s Disease. Sci. Rep. 2016, 6, 33738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, M.; Zhou, B.; Chen, Y.-H.; Ma, Z.-L.; Gou, Y.; Zhang, C.-L.; Yu, W.-F.; Jiao, L. Serum Uric Acid Levels in Patients with Parkinson’s Disease: A Meta-Analysis. PLoS ONE 2017, 12, e0173731. [Google Scholar] [CrossRef] [Green Version]
- Katayama, T.; Sawada, J.; Takahashi, K.; Yahara, O. Cerebrospinal Fluid Biomarkers in Parkinson’s Disease: A Critical Overview of the Literature and Meta-Analyses. Brain Sci. 2020, 10, 466. [Google Scholar] [CrossRef]
- Pahuja, R.; Seth, K.; Shukla, A.; Shukla, R.K.; Bhatnagar, P.; Chauhan, L.K.S.; Saxena, P.N.; Arun, J.; Chaudhari, B.P.; Patel, D.K.; et al. Trans-Blood Brain Barrier Delivery of Dopamine-Loaded Nanoparticles Reverses Functional Deficits in Parkinsonian Rats. ACS Nano 2015, 9, 4850–4871. [Google Scholar] [CrossRef]
- Suominen, T.; Piepponen, T.P.; Kostiainen, R. Permeation of Dopamine Sulfate through the Blood-Brain Barrier. PLoS ONE 2015, 10, e0133904. [Google Scholar] [CrossRef]
- Goldman, J.G.; Andrews, H.; Amara, A.; Naito, A.; Alcalay, R.N.; Shaw, L.M.; Taylor, P.; Xie, T.; Tuite, P.; Henchcliffe, C.; et al. Cerebrospinal Fluid, Plasma, and Saliva in the BioFIND Study: Relationships among Biomarkers and Parkinson’s Disease Features. Mov. Disord. 2018, 33, 282–288. [Google Scholar] [CrossRef] [Green Version]
- Palermo, G.; Ceravolo, R. Molecular Imaging of the Dopamine Transporter. Cells 2019, 8, 872. [Google Scholar] [CrossRef] [Green Version]
- Kageyama, T.; Nakamura, M.; Matsuo, A.; Yamasaki, Y.; Takakura, Y.; Hashida, M.; Kanai, Y.; Naito, M.; Tsuruo, T.; Minato, N.; et al. The 4F2hc/LAT1 Complex Transports L-DOPA across the Blood-Brain Barrier. Brain Res. 2000, 879, 115–121. [Google Scholar] [CrossRef]
- Pavese, N.; Rivero-Bosch, M.; Lewis, S.J.; Whone, A.L.; Brooks, D.J. Progression of Monoaminergic Dysfunction in Parkinson’s Disease: A Longitudinal 18F-Dopa PET Study. Neuroimage 2011, 56, 1463–1468. [Google Scholar] [CrossRef] [PubMed]
- Olivola, E.; Pierantozzi, M.; Imbriani, P.; Liguori, C.; Bassi, M.S.; Conti, M.; D’Angelo, V.; Mercuri, N.B.; Stefani, A. Serotonin Impairment in CSF of PD Patients, without an Apparent Clinical Counterpart. PLoS ONE 2014, 9, e101763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eldrup, E.; Mogensen, P.; Jacobsen, J.; Pakkenberg, H.; Christensen, N.J. CSF and Plasma Concentrations of Free Norepinephrine, Dopamine, 3,4-Dihydroxyphenylacetic Acid (DOPAC), 3,4-Dihydroxyphenylalanine (DOPA), and Epinephrine in Parkinson’s Disease. Acta Neurol. Scand. 1995, 92, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Kremer, T.; Taylor, K.I.; Siebourg-Polster, J.; Gerken, T.; Staempfli, A.; Czech, C.; Dukart, J.; Galasko, D.; Foroud, T.; Chahine, L.M.; et al. Longitudinal Analysis of Multiple Neurotransmitter Metabolites in Cerebrospinal Fluid in Early Parkinson’s Disease. Mov. Disord. 2021, 36, 1972–1978. [Google Scholar] [CrossRef]
- Ames, B.N.; Cathcart, R.; Schwiers, E.; Hochstein, P. Uric Acid Provides an Antioxidant Defense in Humans against Oxidant- and Radical-Caused Aging and Cancer: A Hypothesis. Proc. Natl. Acad. Sci. USA 1981, 78, 6858–6862. [Google Scholar] [CrossRef] [Green Version]
- Kaur, H.; Halliwell, B. Action of Biologically-Relevant Oxidizing Species upon Uric Acid. Identification of Uric Acid Oxidation Products. Chem. Biol. Interact. 1990, 73, 235–247. [Google Scholar] [CrossRef]
- Martín, R.U.-S.; Francke, P.V.; Illanes, F.L.; Gazmuri, A.J.; Rivera, J.S.; Ferńndez, J.G.; Martínez, J.S.; Juri, C. Plasma Urate in REM Sleep Behavior Disorder. Mov. Disord. 2013, 28, 1150–1151. [Google Scholar] [CrossRef]
- van Wamelen, D.J.; Taddei, R.N.; Calvano, A.; Titova, N.; Leta, V.; Shtuchniy, I.; Jenner, P.; Martinez-Martin, P.; Katunina, E.; Chaudhuri, K.R. Serum Uric Acid Levels and Non-Motor Symptoms in Parkinson’s Disease. J. Park. Dis. 2020, 10, 1003–1010. [Google Scholar] [CrossRef]
- Davis, J.W.; Grandinetti, A.; Waslien, C.I.; Ross, G.W.; White, L.R.; Morens, D.M. Observations on Serum Uric Acid Levels and the Risk of Idiopathic Parkinson’s Disease. Am. J. Epidemiol. 1996, 144, 480–484. [Google Scholar] [CrossRef] [Green Version]
- Sun, J.; Ludvigsson, J.F.; Roelstraete, B.; Pedersen, N.L.; Pawitan, Y.; Wirdefeldt, K.; Fang, F. Gastrointestinal Biopsy of Normal Mucosa or Nonspecific Inflammation and Risk of Neurodegenerative Disease: Nationwide Matched Cohort Study. Eur. J. Neurol. 2022. [Google Scholar] [CrossRef]
- Contaldi, E.; Magistrelli, L.; Cosentino, M.; Marino, F.; Comi, C. Lymphocyte Count and Neutrophil-to-Lymphocyte Ratio Are Associated with Mild Cognitive Impairment in Parkinson’s Disease: A Single-Center Longitudinal Study. J. Clin. Med. 2022, 11, 5543. [Google Scholar] [CrossRef] [PubMed]
- Madetko, N.; Migda, B.; Alster, P.; Turski, P.; Koziorowski, D.; Friedman, A. Platelet-to-Lymphocyte Ratio and Neutrophil-Tolymphocyte Ratio May Reflect Differences in PD and MSA-P Neuroinflammation Patterns. Neurol. Neurochir. Pol. 2022, 56, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Block, M.L.; Zecca, L.; Hong, J.-S. Microglia-Mediated Neurotoxicity: Uncovering the Molecular Mechanisms. Nat. Rev. Neurosci. 2007, 8, 57–69. [Google Scholar] [CrossRef]
- Choi, I.; Zhang, Y.; Seegobin, S.P.; Pruvost, M.; Wang, Q.; Purtell, K.; Zhang, B.; Yue, Z. Microglia Clear Neuron-Released α-Synuclein via Selective Autophagy and Prevent Neurodegeneration. Nat. Commun. 2020, 11, 1386. [Google Scholar] [CrossRef] [Green Version]
- Bido, S.; Muggeo, S.; Massimino, L.; Marzi, M.J.; Giannelli, S.G.; Melacini, E.; Nannoni, M.; Gambarè, D.; Bellini, E.; Ordazzo, G.; et al. Microglia-Specific Overexpression of α-Synuclein Leads to Severe Dopaminergic Neurodegeneration by Phagocytic Exhaustion and Oxidative Toxicity. Nat. Commun. 2021, 12, 6237. [Google Scholar] [CrossRef] [PubMed]
- Redza-Dutordoir, M.; Averill-Bates, D.A. Activation of Apoptosis Signalling Pathways by Reactive Oxygen Species. Biochim. Biophys. Acta 2016, 1863, 2977–2992. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.-H.; Chen, C.-M. The Role of Oxidative Stress in Parkinson’s Disease. Antioxidants 2020, 9, 597. [Google Scholar] [CrossRef]
- Dorszewska, J.; Kowalska, M.; Prendecki, M.; Piekut, T.; Kozłowska, J.; Kozubski, W. Oxidative Stress Factors in Parkinson’s Disease. Neural. Regen. Res. 2021, 16, 1383–1391. [Google Scholar] [CrossRef]
- Verma, A.K.; Raj, J.; Sharma, V.; Singh, T.B.; Srivastava, S.; Srivastava, R. Plasma Prolidase Activity and Oxidative Stress in Patients with Parkinson’s Disease. Park. Dis. 2015, 2015, 598028. [Google Scholar] [CrossRef] [Green Version]
- Emir, G.K.; Ünal, Y.; Yılmaz, N.; Tosun, K.; Kutlu, G. The Association of Low Levels of Nesfatin-1 and Glucagon-like Peptide-1 with Oxidative Stress in Parkinson’s Disease. Neurol. Sci. 2019, 40, 2529–2535. [Google Scholar] [CrossRef]
- Maiuolo, J.; Oppedisano, F.; Gratteri, S.; Muscoli, C.; Mollace, V. Regulation of Uric Acid Metabolism and Excretion. Int. J. Cardiol. 2016, 213, 8–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaidi, A.A.; Khan, M.A.; Shahreyar, Z.A.; Ahmed, H. Lauric Acid: Its Role in Behavioral Modulation, Neuro-Inflammatory and Oxidative Stress Markers in Haloperidol Induced Parkinson’s Disease. Pak. J. Pharm. Sci. 2020, 33, 755–763. [Google Scholar]
- Dănău, A.; Dumitrescu, L.; Lefter, A.; Popescu, B.O. Serum Uric Acid Levels in Parkinson’s Disease: A Cross-Sectional Electronic Medical Record Database Study from a Tertiary Referral Centre in Romania. Medicina 2022, 58, 245. [Google Scholar] [CrossRef]
- Ridi, R.E.; Tallima, H. Physiological Functions and Pathogenic Potential of Uric Acid: A Review. J. Adv. Res. 2017, 8, 487–493. [Google Scholar] [CrossRef]
- Villar-Piqué, A.; da Fonseca, T.L.; Outeiro, T.F. Structure, Function and Toxicity of Alpha-Synuclein: The Bermuda Triangle in Synucleinopathies. J. Neurochem. 2016, 139 (Suppl. 1), 240–255. [Google Scholar] [CrossRef] [PubMed]
- Longhena, F.; Faustini, G.; Missale, C.; Pizzi, M.; Spano, P.; Bellucci, A. The Contribution of α-Synuclein Spreading to Parkinson’s Disease Synaptopathy. Neural. Plast. 2017, 2017, 5012129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bengoa-Vergniory, N.; Roberts, R.F.; Wade-Martins, R.; Alegre-Abarrategui, J. Alpha-Synuclein Oligomers: A New Hope. Acta Neuropathol. 2017, 134, 819–838. [Google Scholar] [CrossRef] [Green Version]
- Helwig, M.; Klinkenberg, M.; Rusconi, R.; Musgrove, R.E.; Majbour, N.K.; El-Agnaf, O.M.A.; Ulusoy, A.; Monte, D.A.D. Brain Propagation of Transduced α-Synuclein Involves Non-Fibrillar Protein Species and Is Enhanced in α-Synuclein Null Mice. Brain 2016, 139, 856–870. [Google Scholar] [CrossRef] [Green Version]
- Htike, T.T.; Mishra, S.; Kumar, S.; Padmanabhan, P.; Gulyás, B. Peripheral Biomarkers for Early Detection of Alzheimer’s and Parkinson’s Diseases. Mol. Neurobiol. 2019, 56, 2256–2277. [Google Scholar] [CrossRef]
- Tokuda, T.; Qureshi, M.M.; Ardah, M.T.; Varghese, S.; Shehab, S.A.S.; Kasai, T.; Ishigami, N.; Tamaoka, A.; Nakagawa, M.; El-Agnaf, O.M.A. Detection of Elevated Levels of α-Synuclein Oligomers in CSF from Patients with Parkinson Disease. Neurology 2010, 75, 1766–1772. [Google Scholar] [CrossRef]
- Gao, L.; Tang, H.; Nie, K.; Wang, L.; Zhao, J.; Gan, R.; Huang, J.; Zhu, R.; Feng, S.; Duan, Z.; et al. Cerebrospinal Fluid Alpha-Synuclein as a Biomarker for Parkinson’s Disease Diagnosis: A Systematic Review and Meta-Analysis. Int. J. Neurosci. 2015, 125, 645–654. [Google Scholar] [CrossRef]
- Majbour, N.K.; Vaikath, N.N.; Eusebi, P.; Chiasserini, D.; Ardah, M.; Varghese, S.; Haque, M.E.; Tokuda, T.; Auinger, P.; Calabresi, P.; et al. Longitudinal Changes in CSF Alpha-Synuclein Species Reflect Parkinson’s Disease Progression. Mov. Disord. 2016, 31, 1535–1542. [Google Scholar] [CrossRef]
- He, R.; Yan, X.; Guo, J.; Xu, Q.; Tang, B.; Sun, Q. Recent Advances in Biomarkers for Parkinson’s Disease. Front. Aging Neurosci. 2018, 10, 305. [Google Scholar] [CrossRef] [PubMed]
- Mollenhauer, B.; Zhang, J. Biochemical Pre-Motor Biomarkers for Parkinson Disease. Mov. Disord. 2012, 27, 644–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, L.; Pu, J. Alpha-Synuclein in Parkinson’s Disease: From Pathogenetic Dysfunction to Potential Clinical Application. Park. Dis. 2016, 2016, 1720621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ardekani, A.M.; Naeini, M.M. The Role of MicroRNAs in Human Diseases. Avicenna J. Med. Biotechnol. 2010, 2, 161–179. [Google Scholar] [PubMed]
- Nies, Y.H.; Mohamad Najib, N.H.; Lim, W.L.; Kamaruzzaman, M.A.; Yahaya, M.F.; Teoh, S.L. MicroRNA Dysregulation in Parkinson’s Disease: A Narrative Review. Front. Neurosci. 2021, 15, 660379. [Google Scholar] [CrossRef]
- Chen, Y.; Gao, C.; Sun, Q.; Pan, H.; Huang, P.; Ding, J.; Chen, S. MicroRNA-4639 Is a Regulator of DJ-1 Expression and a Potential Early Diagnostic Marker for Parkinson’s Disease. Front. Aging Neurosci. 2017, 9, 232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Zhang, J.; Wang, K.; Wang, R. Serum MicroRNA-30c-5p and MicroRNA-373 Expressions as Potential Biomarkers for Parkinson’s Disease. All Life 2020, 13, 194–200. [Google Scholar] [CrossRef] [Green Version]
- Bossers, K.; Meerhoff, G.; Balesar, R.; van Dongen, J.W.; Kruse, C.G.; Swaab, D.F.; Verhaagen, J. Analysis of Gene Expression in Parkinson’s Disease: Possible Involvement of Neurotrophic Support and Axon Guidance in Dopaminergic Cell Death. Brain Pathol. 2009, 19, 91–107. [Google Scholar] [CrossRef]
- Su, L.; Wang, C.; Zheng, C.; Wei, H.; Song, X. A Meta-Analysis of Public Microarray Data Identifies Biological Regulatory Networks in Parkinson’s Disease. BMC Med. Genom. 2018, 11, 40. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Tang, Y.; Yu, M.; Wu, L.; Liu, F.; Ni, J.; Wang, Z.; Wang, J.; Fei, J.; Wang, W.; et al. Downregulation of Blood Serum MicroRNA 29 Family in Patients with Parkinson’s Disease. Sci. Rep. 2017, 7, 5411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uwatoko, H.; Hama, Y.; Iwata, I.T.; Shirai, S.; Matsushima, M.; Yabe, I.; Utsumi, J.; Sasaki, H. Identification of Plasma MicroRNA Expression Changes in Multiple System Atrophy and Parkinson’s Disease. Mol. Brain 2019, 12, 49. [Google Scholar] [CrossRef] [Green Version]
- Ricci, A.; Bronzetti, E.; Felici, L.; Greco, S.; Amenta, F. Labeling of Dopamine D3 and D4 Receptor Subtypes in Human Peripheral Blood Lymphocytes with [3H]7-OH-DPAT: A Combined Radioligand Binding Assay and Immunochemical Study. J. Neuroimmunol. 1998, 92, 191–195. [Google Scholar] [CrossRef]
- Sarkar, C.; Basu, B.; Chakroborty, D.; Dasgupta, P.S.; Basu, S. The Immunoregulatory Role of Dopamine: An Update. Brain Behav. Immun. 2010, 24, 525–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buttarelli, F.R.; Fanciulli, A.; Pellicano, C.; Pontieri, F.E. The Dopaminergic System in Peripheral Blood Lymphocytes: From Physiology to Pharmacology and Potential Applications to Neuropsychiatric Disorders. Curr. Neuropharmacol. 2011, 9, 278–288. [Google Scholar] [CrossRef] [Green Version]
- Nagai, Y.; Ueno, S.; Saeki, Y.; Soga, F.; Hirano, M.; Yanagihara, T. Decrease of the D3 Dopamine Receptor MRNA Expression in Lymphocytes from Patients with Parkinson’s Disease. Neurology 1996, 46, 791–795. [Google Scholar] [CrossRef]
- González, H.; Contreras, F.; Prado, C.; Elgueta, D.; Franz, D.; Bernales, S.; Pacheco, R. Dopamine Receptor D3 Expressed on CD4+ T Cells Favors Neurodegeneration of Dopaminergic Neurons during Parkinson’s Disease. J. Immunol. 2013, 190, 5048–5056. [Google Scholar] [CrossRef] [Green Version]
- Levite, M. Dopamine and T Cells: Dopamine Receptors and Potent Effects on T Cells, Dopamine Production in T Cells, and Abnormalities in the Dopaminergic System in T Cells in Autoimmune, Neurological and Psychiatric Diseases. Acta Physiol. 2016, 216, 42–89. [Google Scholar] [CrossRef]
- Raninga, P.V.; Trapani, G.D.; Tonissen, K.F. The Multifaceted Roles of DJ-1 as an Antioxidant. Adv. Exp. Med. Biol. 2017, 1037, 67–87. [Google Scholar] [CrossRef]
- Bonifati, V.; Rizzu, P.; van Baren, M.J.; Schaap, O.; Breedveld, G.J.; Krieger, E.; Dekker, M.C.J.; Squitieri, F.; Ibanez, P.; Joosse, M.; et al. Mutations in the DJ-1 Gene Associated with Autosomal Recessive Early-Onset Parkinsonism. Science 2003, 299, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Angelopoulou, E.; Paudel, Y.N.; Villa, C.; Shaikh, M.F.; Piperi, C. Lymphocyte-Activation Gene 3 (LAG3) Protein as a Possible Therapeutic Target for Parkinson’s Disease: Molecular Mechanisms Connecting Neuroinflammation to α-Synuclein Spreading Pathology. Biology 2020, 9, 86. [Google Scholar] [CrossRef] [PubMed]
- Gu, H.; Yang, X.; Mao, X.; Xu, E.; Qi, C.; Wang, H.; Brahmachari, S.; York, B.; Sriparna, M.; Li, A.; et al. Lymphocyte Activation Gene 3 (Lag3) Contributes to α-Synucleinopathy in α-Synuclein Transgenic Mice. Front. Cell. Neurosci. 2021, 15, 656426. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.; Ou, M.T.; Karuppagounder, S.S.; Kam, T.-I.; Yin, X.; Xiong, Y.; Ge, P.; Umanah, G.E.; Brahmachari, S.; Shin, J.-H.; et al. Pathological α-Synuclein Transmission Initiated by Binding Lymphocyte-Activation Gene 3. Science 2016, 353, aah3374. [Google Scholar] [CrossRef] [Green Version]
- Stiasny-Kolster, K.; Mayer, G.; Schäfer, S.; Möller, J.C.; Heinzel-Gutenbrunner, M.; Oertel, W.H. The REM Sleep Behavior Disorder Screening Questionnaire—A New Diagnostic Instrument. Mov. Disord. 2007, 22, 2386–2393. [Google Scholar] [CrossRef]
- Visser, M.; Marinus, J.; Stiggelbout, A.M.; Van Hilten, J.J. Assessment of Autonomic Dysfunction in Parkinson’s Disease: The SCOPA-AUT. Mov. Disord. 2004, 19, 1306–1312. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Fahn, S.; Elton, R.L. Members of the UPDRS Development Committee. Unified Parkinson’s Disease Rating Scale. Recent Developments in Parkinson’s Disease; Fahn, S., Marsden, C.D., Calne, D.B., Goldstein, M., Eds.; Macmillan Health Care Information: Florham Park, NJ, USA, 1987; Volume 2, pp. 153–164. [Google Scholar]
- Starkstein, S.E.; Mayberg, H.S.; Preziosi, T.J.; Andrezejewski, P.; Leiguarda, R.; Robinson, R.G. Reliability, Validity, and Clinical Correlates of Apathy in Parkinson’s Disease. J. Neuropsychiatry Clin. Neurosci. 1992, 4, 134–139. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.G.; Dittner, A.; Findley, L.; Wessely, S.C. The Parkinson Fatigue Scale. Park. Relat. Disord. 2005, 11, 49–55. [Google Scholar] [CrossRef]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.H.; Alves, G.; Hagell, P.; Marinus, J.; Marsh, L.; Martinez-Martin, P.; Goetz, C.G.; Poewe, W.; Rascol, O.; Sampaio, C.; et al. Fatigue Rating Scales Critique and Recommendations by the Movement Disorders Society Task Force on Rating Scales for Parkinson’s Disease. Mov. Disord. 2010, 25, 805–822. [Google Scholar] [CrossRef] [PubMed]
- Kumari, R.; Srivastava, R.; Verma, A.; Agarwal, N. Co-Relative Study of Serum Prolidase Activity and Oxidative Status in Patients with Diabetic Neuropathy. BJMMR 2017, 20, 1–9. [Google Scholar] [CrossRef]
- Erel, O. A New Automated Colorimetric Method for Measuring Total Oxidant Status. Clin. Biochem. 2005, 38, 1103–1111. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Scales | Control Group n = 20 (12 Men, 8 Women) | Risk Group n = 26 (15 Men, 11 Women) |
|---|---|---|
| Age, years | 64.1 ± 6.3 | 61.0 ± 8.3 |
| RBDSQ score | 2.0 ± 0.5 | 6.2 ± 3.3 * |
| SST | 14.0 ± 2.5 | 9.1 ± 4.5 * |
| SCOPA-AUT | 1.05 ± 1.3 | 1.65 ± 1.20 |
| UPDRS (motor, III part) | 0 | 2.25 ± 2.19 * |
| HADS anxiety HADS depression | 11.6 ± 2.8 9.0 ± 3.2 | 10.3 ± 2.6 9.8 ± 2.2 |
| SAS | 12.5 ± 4.3 | 14.2 ± 6.3 |
| FSS | 3.1 ± 2.3 | 4.3 ± 2.4 |
| MoCA | 27.1 ± 1.9 | 24.3 ± 2.9 * |
| ESS | 6.5 ± 1.5 | 7.1 ± 3.9 |
| Variables | RBDSQ | SST | SCOPA-AUT | UPDRS | HADS Anxiety | HADS Depression | SAS | FSS | MoCA | ESS |
|---|---|---|---|---|---|---|---|---|---|---|
| RBDSQ | 0.476 p = 0.014 | |||||||||
| HADS Anxiety | −0.388 p = 0.050 | 0.449 p = 0.021 | −0.749 p = 0.002 | |||||||
| HADS Depression | 0.449 p = 0.021 | 0.420 p = 0.033 | ||||||||
| SAS | 0.4201 p = 0.033 | |||||||||
| FSS | 0.476 p = 0.014 | −0.544 p= 0.005 | ||||||||
| MoCA | −0.543 p = 0.005 | |||||||||
| ESS | −0.749 p = 0.002 |
| Parameter | Patients | |
|---|---|---|
| UPDRS ≤ 2 | UPDRS > 2.5 | |
| Norepinephrine | → | → |
| Epinephrine | → | → |
| L-DOPA | ↓ | ↓ |
| Dopamine | → | → |
| DOPAC | → | → |
| 5-HTP | → | → |
| HIAA | → | → |
| 3-MT | → | → |
| HVA | → | → |
| 3-OMD | → | → |
| Serotonin | → | → |
| Clinical Scales | Risk Group | Control Group |
|---|---|---|
| RBDSQ | ≥5 | <5 |
| UPDRS | ≥2, ≤6 | 0 |
| SST | ≤12 | >12 |
| SCOPA-AUT | >1 | ≤1 |
| HADS | ||
| Anxiety | ≥8 | <8 |
| Depression | ≥8 | <8 |
| Gene | Forward Primers | Reverse Primers |
|---|---|---|
| D3 | GTACAGCCAGCATCCTTAATCTCT | ACAGAAGAGGGCAGGACACA |
| D4 | GACGCCCTTCTTCGTGGT | GACAGTGTAGATGACGGGGTTG |
| PARK7 | GCTGGCGTGCGTTCATT | ACCGTCTCCATTTCCTCTGC |
| B2M | GGGTTTCATCCATCCGACATTG | ACACGGCAGGCATACTCATCTTTT |
| LAG3 | TCACAGTGACTCCCAAATCCT | GCTCCACACAAAGCGTTCTT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katunina, E.A.; Blokhin, V.; Nodel, M.R.; Pavlova, E.N.; Kalinkin, A.L.; Kucheryanu, V.G.; Alekperova, L.; Selikhova, M.V.; Martynov, M.Y.; Ugrumov, M.V. Searching for Biomarkers in the Blood of Patients at Risk of Developing Parkinson’s Disease at the Prodromal Stage. Int. J. Mol. Sci. 2023, 24, 1842. https://doi.org/10.3390/ijms24031842
Katunina EA, Blokhin V, Nodel MR, Pavlova EN, Kalinkin AL, Kucheryanu VG, Alekperova L, Selikhova MV, Martynov MY, Ugrumov MV. Searching for Biomarkers in the Blood of Patients at Risk of Developing Parkinson’s Disease at the Prodromal Stage. International Journal of Molecular Sciences. 2023; 24(3):1842. https://doi.org/10.3390/ijms24031842
Chicago/Turabian StyleKatunina, Elena A., Victor Blokhin, Marina R. Nodel, Ekaterina N. Pavlova, Alexander L. Kalinkin, Valerian G. Kucheryanu, Leyla Alekperova, Marianna V. Selikhova, Mikhail Yu. Martynov, and Michael V. Ugrumov. 2023. "Searching for Biomarkers in the Blood of Patients at Risk of Developing Parkinson’s Disease at the Prodromal Stage" International Journal of Molecular Sciences 24, no. 3: 1842. https://doi.org/10.3390/ijms24031842
APA StyleKatunina, E. A., Blokhin, V., Nodel, M. R., Pavlova, E. N., Kalinkin, A. L., Kucheryanu, V. G., Alekperova, L., Selikhova, M. V., Martynov, M. Y., & Ugrumov, M. V. (2023). Searching for Biomarkers in the Blood of Patients at Risk of Developing Parkinson’s Disease at the Prodromal Stage. International Journal of Molecular Sciences, 24(3), 1842. https://doi.org/10.3390/ijms24031842