
Finding the Needle in the Haystack: Serological and Urinary Biomarkers in Behçet’s Disease: A Systematic Review

 , ,
, , 
 , and
, and 
Abstract
:1. Introduction
2. Methods
2.1. Literature Search Strategy
2.2. Selection of the Studies
2.3. Data Extraction and Data Synthesis
3. Results and Discussion
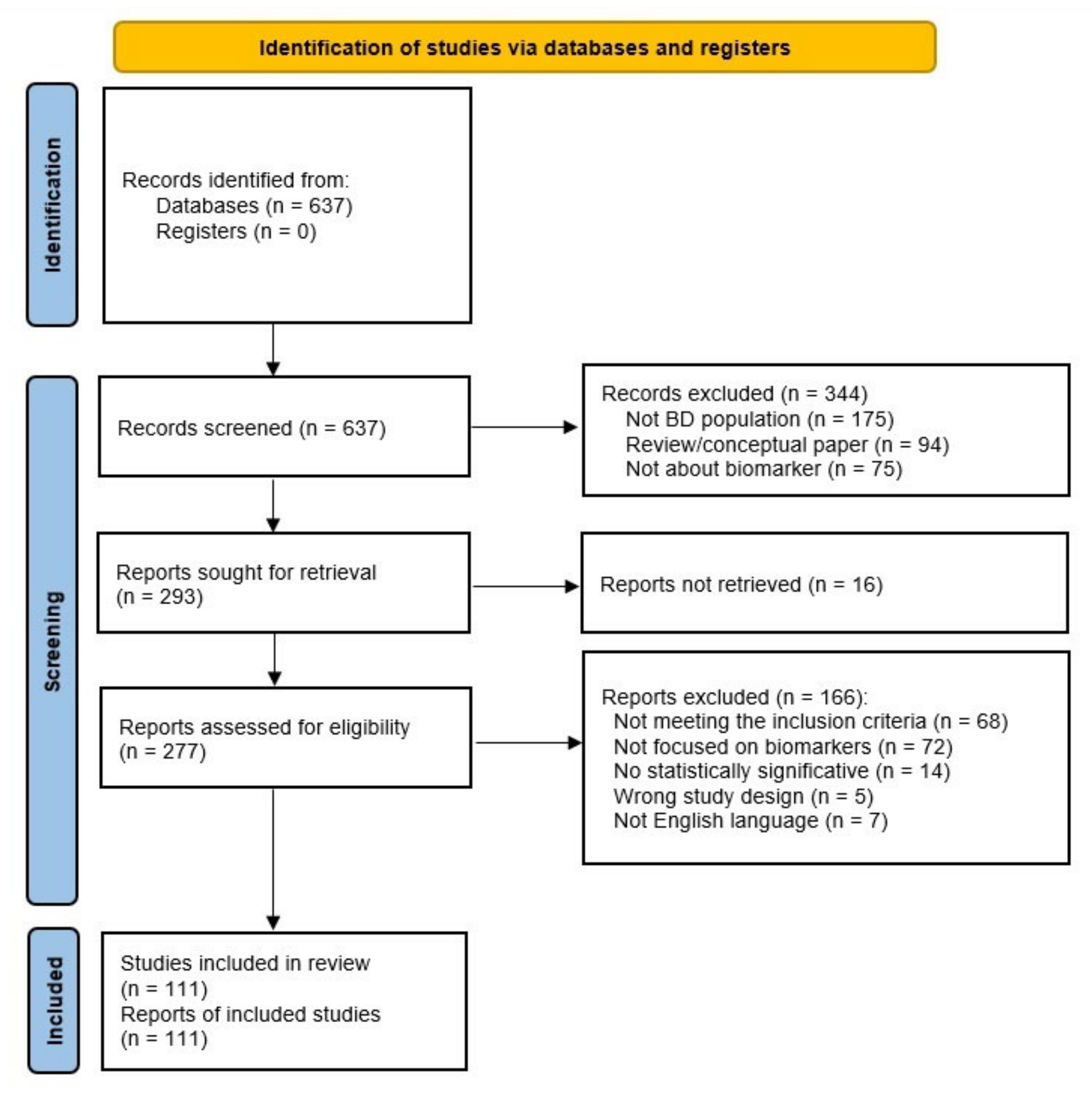
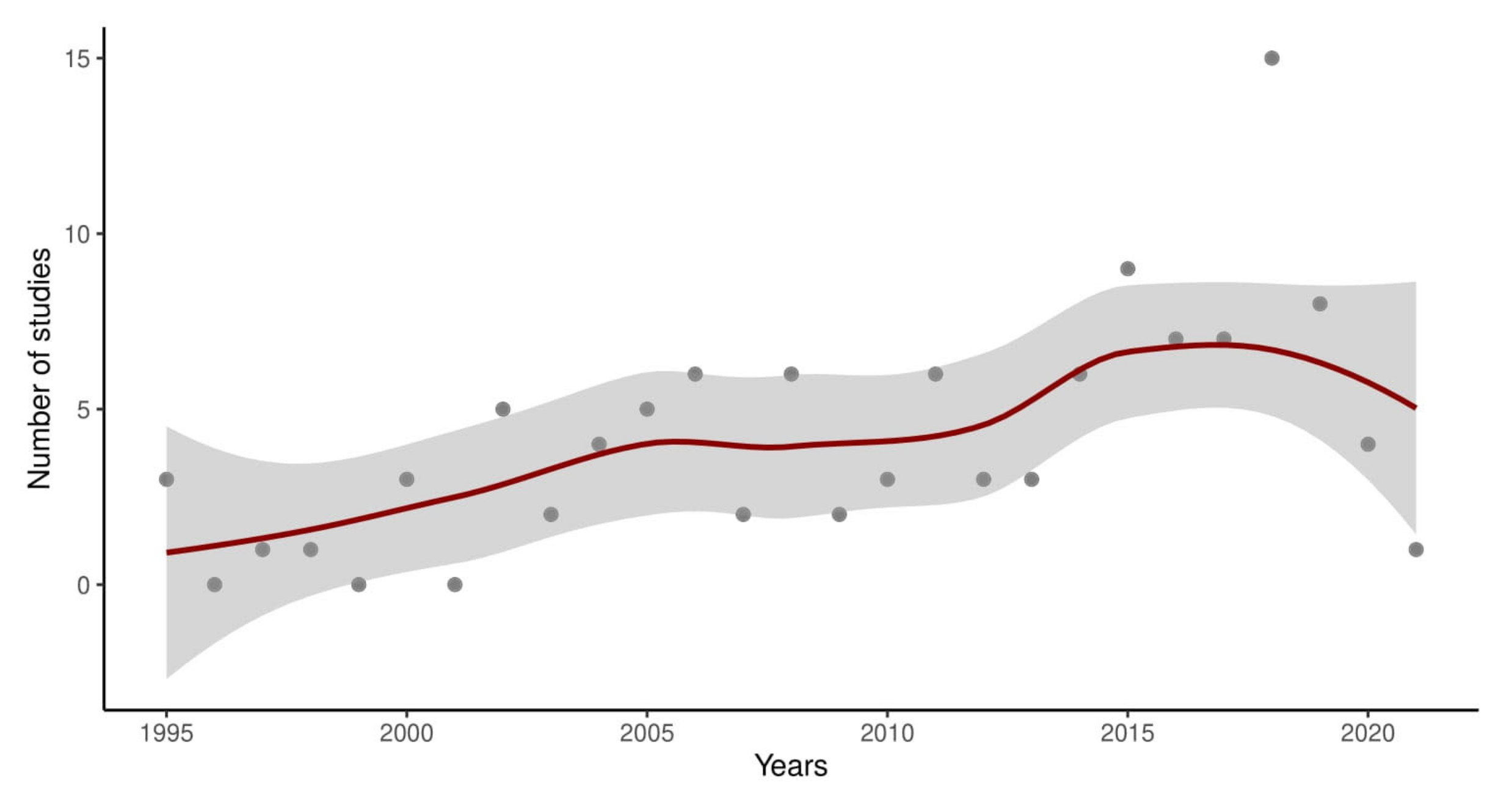
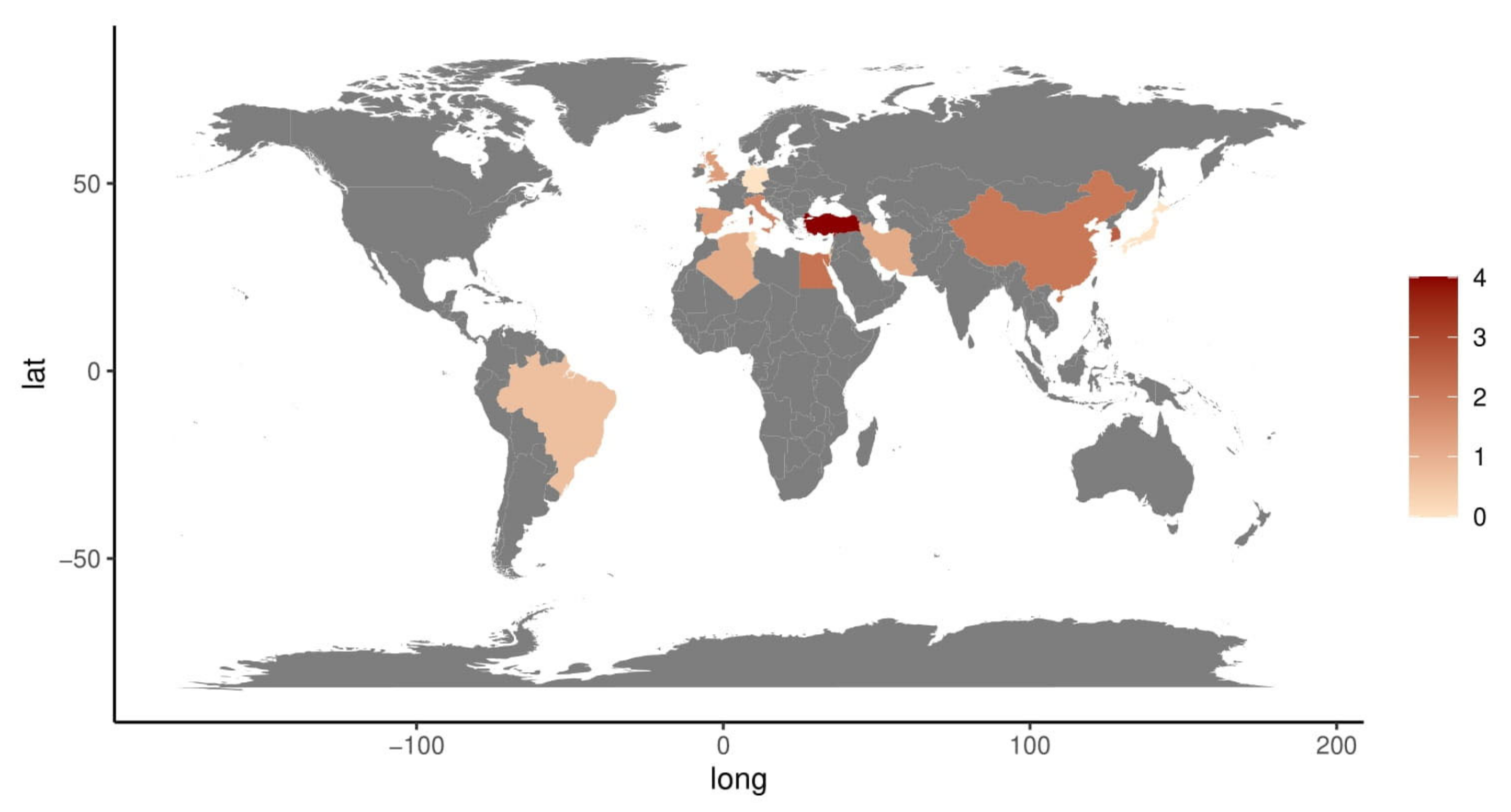
3.1. Systematic Literature Search
3.2. Biomarkers and Their Roles in Diagnosis and Disease Activity
3.2.1. Conventional Inflammation Markers and Soluble Proteins
3.2.2. Oxidant and Anti-Oxidant Molecules
3.2.3. microRNAs
3.2.4. New “Omics” Sciences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leccese, P.; Alpsoy, E. Behçet’s Disease: An Overview of Etiopathogenesis. Front. Immunol. 2019, 10, 1067. [Google Scholar] [CrossRef] [PubMed]
- Bettiol, A.; Prisco, D.; Emmi, G. Behçet: The syndrome. Rheumatology 2020, 59, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Oguz, I.D.; Hizli, P.; Gonul, M. The Epidemiology of Behçet’s Disease. In Behcet’s Disease; Gonul, M., Kartal, S.P., Eds.; BoD—Books on Demand: Norderstedt, Germany, 2017. [Google Scholar] [CrossRef]
- Alpsoy, E. Behçet’s Disease: A Comprehensive Review with a Focus on Epidemiology, Etiology and Clinical Features, and Management of Mucocutaneous Lesions. J. Dermatol. 2016, 43, 620–632. [Google Scholar] [CrossRef] [PubMed]
- International Study Group for Behçet’s Disease. Criteria Fordiagnosis of Behçet’s Disease. Lancet 1990, 335, 1078–1080. [Google Scholar]
- Kim, D.H.; Cheon, J.H. Intestinal Behçet’s Disease: A True Inflammatory Bowel Disease or Merely an Intestinal Complication of Systemic Vasculitis? Yonsei Med. J. 2016, 57, 22–32. [Google Scholar] [CrossRef]
- Valenti, S.; Gallizzi, R.; De Vivo, D.; Romano, C. Intestinal Behçet and Crohn’s Disease: Two Sides of the Same Coin. Pediatr. Rheumatol. Online J. 2017, 15, 1–8. [Google Scholar] [CrossRef]
- Shi, G.; Zhang, Z.; Li, Q. New Biomarkers in Autoimmune Disease. J. Immunol. Res. 2017, 2017, 1–4. [Google Scholar] [CrossRef]
- Guma, M.; Tiziani, S.; Firestein, G.S. Metabolomics in Rheumatic Diseases: Desperately Seeking Biomarkers. Nat. Rev. Rheumatol. 2016, 12, 269–281. [Google Scholar] [CrossRef]
- Giacomelli, R.; Afeltra, A.; Alunno, A.; Bartoloni-Bocci, E.; Berardicurti, O.; Bombardieri, M.; Bortoluzzi, A.; Caporali, R.; Caso, F.; Cervera, R.; et al. Guidelines for Biomarkers in Autoimmune Rheumatic Diseases—Evidence Based Analysis. Autoimmun. Rev. 2019, 18, 93–106. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wickham, H. 2016. ggplot2: Elegant Graphics for Data Analysis, Springer-Verlag New York. Available online: https://ggplot2.tidyverse.org/ (accessed on 16 January 2023).
- R Core Team, version 0.98.1091. 2014. Available online: https://support.posit.co/hc/en-us/articles/200716783-RStudio-IDE-Release-History (accessed on 16 January 2023).
- Yosipovitch, G.; Shohat, B.; Bshara, J.; Wysenbeek, A.; Weinberger, A. Elevated Serum Interleukin 1 Receptors and Interleukin 1B in Patients with Behçet’s Disease: Correlations with Disease Activity and Severity. Isr. J. Med. Sci. 1995, 31, 345–348. [Google Scholar] [CrossRef]
- Deǧer, O.; Örem, A.; Akyol, N.; Bahadir, S.; Yildirmiş, S. Polymorphonuclear leukocyte elastase levels in patients with Behçet’s disease. Clin. Chim. Acta 1995, 236, 129–134. [Google Scholar] [CrossRef]
- Direskeneli, H.; Keser, G.; D’Cruz, D.; Khamashta, M.A.; Akoglu, T.; Yazici, H.; Yurdakul, S.; Hamuryudan, V.; Özgün, S.; Goral, A.J.; et al. Anti-endothelial cell antibodies, endothelial proliferation and von Willebrand factor antigen in Behçet’s disease. Clin. Rheumatol. 1995, 14, 55–61. [Google Scholar] [CrossRef]
- Uslu, T.; Erem, C.; Tosun, M.; Deger, O. Plasma endothelin-1 levels in Behçet’s disease. Clin. Rheumatol. 1997, 16, 59–61. [Google Scholar] [CrossRef]
- Çayirli, E.A.; Er, H.; Yilmaz, E. The Levels of Plasma Interleukin-2 and Soluble Interleukin-2R in Behçet’s Disease: A Marker of Disease Activity. J. Dermatol. 1998, 25, 513–516. [Google Scholar] [CrossRef]
- Katsantonis, J.; Adler, Y.; Orfanos, C.E.; Zouboulis, C.C. Adamantiades-Behçet’s Disease: Serum IL-8 Is a More Reliable Marker for Disease Activity than C-Reactive Protein and Erythrocyte Sedimentation Rate. Dermatology 2000, 201, 37–39. [Google Scholar] [CrossRef]
- Eksioglu-Demiralp, E.; Direskeneli, H.; Ergun, T.; Fresko, I.; Akoglu, T. Increased CD4 + CD16 + and CD4 + CD56 + T cell subsets in Behçet’s disease. Rheumatol. Int. 1999, 19, 23–26. [Google Scholar] [CrossRef]
- Freysdottir, J.; Lau, S.-H.; Fortune, F. γδ T cells in Behçet’s disease (BD) and recurrent aphthous stomatitis (RAS). Clin. Exp. Immunol. 1999, 118, 451–457. [Google Scholar] [CrossRef]
- Krause, I.; Monselise, Y.; Milo, G.; Weinberger, A. Anti-Saccharomyces cerevisiae Antibodies. Adamantiades-Behçet’s Dis. 2003, 528, 201–204. [Google Scholar] [CrossRef]
- Evereklioglu, C.; Inaloz, H.; Kirtak, N.; Doganay, S.; Bulbul, M.; Otlu, B.; Ozerol, E.; Er, H.; Ozbek, E. Serum leptin concentration is increased in patients with Behcet’s syndrome and is correlated with disease activity. Br. J. Dermatol. 2002, 147, 331–336. [Google Scholar] [CrossRef]
- Er, H.; Evereklioglu, C.; Cumurcu, T.; Türköz, Y.; Özerol, E.; Şahin, K.; Daganay, S. Serum Homocysteine Level Is Increased and Correlated with Endothelin-1 and Nitric Oxide in Behçet’s Disease. Br. J. Ophthalmol. 2002, 86, 653–657. [Google Scholar] [CrossRef] [PubMed]
- Saglam, K.; Yilmaz, I.M.; Saglam, A.; Ulgey, M.; Bulucu, F.; Baykal, Y. Levels of circulating intercellular adhesion molecule-1 in patients with Behçet’s disease. Rheumatol. Int. 2001, 21, 146–148. [Google Scholar] [CrossRef] [PubMed]
- Evereklioglu, C.; Turkoz, Y.; Er, H.; Inaloz, H.S.; Ozbek, E.; Cekmen, M. Increased Nitric Oxide Production in Patients with Behçet’s Disease: Is It a New Activity Marker? J. Am. Acad. Dermatol. 2002, 46, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Evereklioglu, C.; Özbek, E.; Çekmen, M.; Mehmet, N.; Duygulu, F.; Ozkiris, A.; Çalip, M.; Er, H.; Türköz, Y. Urinary Nitric Oxide Levels Are Increased and Correlated with Plasma Concentrations in Patients with Behçet’s Disease: Is It a New Urinary Activity Marker? Nephrology. 2003, 8, 231–238. [Google Scholar] [CrossRef]
- Erkiliç, K.; Evereklioglu, C.; Çekmen, M.; Özkiris, A.; Duygulu, F.; Dogan, H. Adenosine Deaminase Enzyme Activity Is Increased and Negatively Correlates with Catalase, Superoxide Dismutase and Glutathione Peroxidase in Patients with Behçet’s Disease: Original Contributions/Clinical and Laboratory Investigations. Mediat. Inflamm. 2003, 12, 107–116. [Google Scholar] [CrossRef]
- Akdeniz, N.; Esrefoglu, M.; Keles, M.; Karakuzu, A.; Atasoy, M. Serum Interleukin-2, Interleukin-6, Tumour Necrosis Factor-Alpha and Nitric Oxide Levels in Patients With Behçet’s Disease. Ann. Acad. Med. 2004, 33, 596–599. [Google Scholar]
- Sari, R.A.; Kiziltunc, A.; Tays’Y, S.; Akdem’Yr, S.; Gündogdu, M. Levels of soluble E-selectin in patients with active Behçet’s disease. Clin. Rheumatol. 2004, 24, 55–59. [Google Scholar] [CrossRef]
- Yazici, C.; Köse, K.; Çaliş, M.; Demir, M.; Kirnap, M.; Ateş, F. Increased Advanced Oxidation Protein Products in Behçet’s Disease: A New Activity Marker? Br. J. Dermatol. 2004, 151, 105–111. [Google Scholar] [CrossRef]
- Duygulu, F.; Evereklioglu, C.; Calis, M.; Borlu, M.; Çekmen, M.; Ascioglu, O. Synovial Nitric Oxide Concentrations Are Increased and Correlated with Serum Levels in Patients with Active Behçet’s Disease: A Pilot Study. Clin. Rheumatol. 2005, 24, 324–330. [Google Scholar] [CrossRef]
- Ureten, K.; Ertenli, I.; Oztürk, M.A.; Kiraz, S.; Onat, A.M.; Tuncer, M.; Okur, H.; Akdogan, A.; Apras, S.; Calgüneri, M. Neutrophil CD64 expression in Behçet’s disease. J. Rheumatol. 2005, 32(5), 849–852. [Google Scholar] [PubMed]
- Calis, M.; Ates, F.; Yazici, C.; Kose, K.; Kirnap, M.; Demir, M.; Borlu, M.; Evereklioglu, C. Adenosine Deaminase Enzyme Levels, Their Relation with Disease Activity, and the Effect of Colchicine on Adenosine Deaminase Levels in Patients with Behçet’s Disease. Rheumatol. Int. 2005, 25, 452–456. [Google Scholar] [CrossRef]
- Qiao, H.; Sonoda, K.-H.; Ariyama, A.; Kuratomi, Y.; Kawano, Y.-I.; Ishibashi, T. CXCR2 Expression on Neutrophils is Upregulated During the Relapsing Phase of Ocular Behçet Disease. Curr. Eye Res. 2005, 30, 195–203. [Google Scholar] [CrossRef]
- Gür-Toy, G.; Lenk, N.; Yalcin, B.; Aksaray, S.; Alli, N. Serum Interleukin-8 as a Serologic Marker of Activity in Behçet’s Disease. Int. J. Dermatol. 2005, 44, 657–660. [Google Scholar] [CrossRef]
- Basak, C.; Yunus, S.; Ahmet, G.; Ilker, E.; Naci, C. Activation Markers in Behçet’s Disease. SKINmed. Dermatol. Clin. 2005, 4, 282–286. [Google Scholar] [CrossRef]
- Yardim-Akaydin, S.; Sepici, A.; Özkan, Y.; Şimşek, B.; Sepici, V. Evaluation of Allantoin Levels as a New Marker of Oxidative Stress in Behçet’s Disease. Scand. J. Rheumatol. 2006, 35, 61–64. [Google Scholar] [CrossRef]
- Köse, O.; Arca, E.; Akgül, Ö.; Erbil, K. The levels of serum neopterin in Behçet’s disease—Objective marker of disease activity. J. Dermatol. Sci. 2006, 42, 128–130. [Google Scholar] [CrossRef]
- Canpolat, F.; Ünver, M.; Eskioǧlu, F.; Kösebalaban, Ş.; Durmazlar, S.P.K. Serum and Erythrocyte Adenosine Deaminase Activities in Patients with Behçet’s Disease. Int. J. Dermatol. 2006, 45, 1053–1056. [Google Scholar] [CrossRef]
- Kwon, S.R.; Lim, M.J.; Park, S.G.; Moon, Y.S.; Park, W. Decreased protein S activity is related to the disease activity of Behcet’s disease. Rheumatol. Int. 2006, 27, 39–43. [Google Scholar] [CrossRef]
- Briani, C.; Doria, A.; Marcolongo, R.; Tognon, S.; Ruggero, S.; Toffanin, E.; Ermani, M.; Ghirardello, A.; Zampieri, S.; Semenzato, G. Increased titres of IgM anti-heparan sulfate antibody in Behçet’s disease. Ann. Rheum. Dis. 2006, 24. [Google Scholar]
- Sarican, T.; Ayabakan, H.; Turkmen, S.; Kalaslioglu, V.; Baran, F.; Yenice, N. Homocysteine: An activity marker in Behçet’s disease? J. Dermatol. Sci. 2007, 45, 121–126. [Google Scholar] [CrossRef]
- Lee, Y.J.; Kang, S.W.; Song, J.K.; Park, J.J.; Bae, Y.D.; Lee, E.Y.; Song, Y.W. Serum galectin-3 and galectin-3 binding protein levels in Behçet’s disease and their association with disease activity. Ann. Rheum. Dis. 2007, 25. [Google Scholar]
- Pay, S.; Abbasov, T.; Erdem, H.; Musabak, U.; Simsek, I.; Pekel, A.; Akdogan, A.; Sengul, A.; Dinc, A. Serum MMP-2 and MMP-9 in Patients with Behçet’s Disease: Do Their Higher Levels Correlate to Vasculo-Behçet’s Disease Associated with Aneurysm Formation? Clin. Exp. Rheumatol. 2007, 25 Suppl. 45, S70–S75. [Google Scholar] [PubMed]
- Öztürk, M.A.; Ünverdi, S.; Oktar, S.O.; Bukan, N.; Gülbahar, Ö.; Üreten, K.; Göker, B.; Haznedaroglu, S.; Sungur, G.; Çiftçi, T.U.; et al. Vascular endothelial growth factor and carotid intima-media thickness in patients with Behçet’s disease. Clin. Rheumatol. 2008, 27, 961–966. [Google Scholar] [CrossRef] [PubMed]
- Turan, B.; Pfister, K.; Diener, P.; Hell, M.; Möller, B.; Boyvat, A.; Ergin, S.; Villiger, P.M. Soluble tumour necrosis factor receptors sTNFR1 and sTNFR2 are produced at sites of inflammation and are markers of arthritis activity in Behçet’s disease. Scand. J. Rheumatol. 2008, 37, 135–141. [Google Scholar] [CrossRef]
- Kutlay, S.; Calayoglu, R.; Boyvat, A.; Turkcapar, N.; Sengul, S.; Keven, K.; Nergizoglu, G. Circulating endothelial cells: A disease activity marker in Behçet’s vasculitis? Rheumatol. Int. 2008, 29, 159–162. [Google Scholar] [CrossRef]
- Curnow, S.J.; Pryce, K.; Modi, N.; Knight, B.; Graham, E.M.; Stewart, J.E.; Fortune, F.; Stanford, M.R.; Murray, P.I.; Wallace, G.R. Serum Cytokine Profiles in Behçet’s Disease: Is There a Role for IL-15 in Pathogenesis? Immunol. Lett. 2008, 121, 7–12. [Google Scholar] [CrossRef]
- Polat, M.; Vahaboglu, G.; Önde, U.; Eksioglu, M. Classifying Patients with Behçet’s Disease for Disease Severity, Using a Discriminating Analysis Method. Clin. Exp. Dermatol. 2009, 34, 151–155. [Google Scholar] [CrossRef]
- Durmazlar, S.P.K.; Ulkar, G.B.; Eskioglu, F.; Tatlican, S.; Mert, A.; Akgul, A. Significance of Serum Interleukin-8 Levels in Patients with Behcet’s Disease: High Levels May Indicate Vascular Involvement. Int. J. Dermatol. 2009, 48, 259–264. [Google Scholar] [CrossRef]
- Habibagahi, Z.; Habibagahi, M.; Heidari, M. Raised concentration of soluble form of vascular endothelial cadherin and IL-23 in sera of patients with Behçet’s disease. Mod. Rheumatol. 2009, 20, 154–159. [Google Scholar] [CrossRef]
- Fadini, G.P.; Tognon, S.; Rodriguez, L.; Boscaro, E.; Baesso, I.; Avogaro, A.; Semenzato, G.; Agostini, C.; Marcolongo, R. Low levels of endothelial progenitor cells correlate with disease duration and activity in patients with Behçet’s disease. Ann. Rheum. Dis. 2009, 27. [Google Scholar]
- Choe, J.-Y.; Park, S.-H.; Kim, S.-K. Serum angiopoietin-1 level is increased in patients with Behçet’s disease. Jt. Bone Spine 2010, 77, 340–344. [Google Scholar] [CrossRef]
- Donmez, A.; Aksu, K.; Aydın, H.; Keser, G.; Cagirgan, S.; Doganavsargil, E.; Tombuloglu, M. The plasma levels of activated thrombin activatable fibrinolysis inhibitor and thrombomodulin in Behçet Disease and their association with thrombosis. Thromb. Res. 2010, 126, 207–210. [Google Scholar] [CrossRef]
- Sezer, E.D.; Aksu, K.; Caglayan, O.; Keser, G.; Karabulut, G.; Ercan, G. DNA Damage and Its Relationship with Other Oxidative Stress Parameters in Behcet’s Disease. Rheumatol. Int. 2012, 32, 217–222. [Google Scholar] [CrossRef]
- Özden, M.; Çaycı, Y.; Tekin, H.; Çoban, A.; Aydın, F.; Şentürk, N.; Bek, Y.; Cantürk, T.; Turanlı, A. Serum galectin-3 levels in patients with Behçet’s disease: Association with disease activity over a long-term follow-up. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 1168–1173. [Google Scholar] [CrossRef]
- Pehlivan, Y.; Onat, A.M.; Okumuş, S.; Kisacik, B.; Comez, G.; Comez, A.; Goktepe, F.; Ceylan, N.O. The Role of Resistin in Behçet’s Disease: A Turkish Experiment. Mod. Rheumatol. 2012, 22, 571–575. [Google Scholar] [CrossRef]
- Ahn, J.K.; Hwang, J.-W.; Oh, J.-M.; Bae, E.-K.; Lee, J.; Lee, Y.S.; Koh, E.-M.; Cha, H.-S. Increased α-defensin-1 expression in Korean patients with Behcet’s disease. Jt. Bone Spine 2011, 78, 593–597. [Google Scholar] [CrossRef]
- Shin, S.J.; Kim, B.C.; Il Kim, T.; Lee, S.K.; Lee, K.H.; Kim, W.H. Anti-Alpha-Enolase Antibody as a Serologic Marker and Its Correlation with Disease Severity in Intestinal Behçet’s Disease. Dig. Dis. Sci. 2011, 56, 812–818. [Google Scholar] [CrossRef]
- Jung, Y.S.; Kim, S.W.; Yoon, J.Y.; Lee, J.H.; Jeon, S.M.; Hong, S.P.; Il Kim, T.; Kim, W.H.; Cheon, J.H. Expression of a Soluble Triggering Receptor Expressed on Myeloid Cells-1 (STREM-1) Correlates with Clinical Disease Activity in Intestinal Behcet’s Disease. Inflamm. Bowel Dis. 2011, 17, 2130–2137. [Google Scholar] [CrossRef]
- Vural, B.; Uğurel, E.; Tüzün, E.; Kürtüncü, M.; Zuliani, L.; Çavuş, F.; Içöz, S.; Erdağ, E.; Gül, A.; Güre, A.O.; et al. Anti-neuronal and stress-induced-phosphoprotein 1 antibodies in neuro-Behçet’s disease. J. Neuroimmunol. 2011, 239, 91–97. [Google Scholar] [CrossRef]
- López-Longo, F.J.; Arias-Salgado, E.G.; Martín, M.; Jiménez-Yuste, V.; de la Rúa, A.R.; Bello, I.F.; Álvarez, M.T.; Butta, N.V. Platelet soluble CD40L and matrix metalloproteinase 9 activity are proinflammatory mediators in Behçet disease patients. Thromb. Haemost. 2012, 107, 88–98. [Google Scholar] [CrossRef]
- Gündüz, E.; Teke, H.; Bilge, N..Y.; Cansu, D..; Bal, C.; Korkmaz, C.; Gülbaş, Z. Regulatory T cells in Behçet’s disease: Is there a correlation with disease activity? Does regulatory T cell type matter? Rheumatol. Int. 2013, 33, 3049–3054. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, M.F.; Xie, J.; Li, Z.L.; Wang, P. Behcet’s Disease with Active Uveitis: Detection of Serum Protein Biomarkers Using MALDI-TOF-MS. Anat. Rec. 2012, 295, 1168–1173. [Google Scholar] [CrossRef]
- Örem, A.; Yayli, S.; Arıca, D.; Akcan, B.; Yücesan, F.; Bahadir, S. Lipoprotein-associated phospholipase A2level in patients with Behçet’s disease. J. Eur. Acad. Dermatol. Venereol. 2012, 27, e289–e293. [Google Scholar] [CrossRef]
- Hamzaoui, K.; Kaabachi, W.; Fazaa, B.; Zakraoui, L.; Mili-Boussen, I.; Haj-Sassi, F. Serum IL-33 levels and skin mRNA expression in Behçet’s disease. Ann. Rheum. Dis. 2013, 31, S6–S14. [Google Scholar]
- Vural, B.; Şehitoğlu, E.; Çavuş, F.; Yalçınkaya, N.; Haytural, H.; Küçükerden, M.; Ulusoy, C.; Uğurel, E.; Turan, S.; Bulut, L.; et al. Mitochondrial carrier homolog 1 (Mtch1) antibodies in neuro-Behçet’s disease. J. Neuroimmunol. 2013, 263, 139–144. [Google Scholar] [CrossRef]
- Shaker, O.G.; Tawfic, S.O.; El-Tawdy, A.M.; El-Komy, M.H.M.; El Menyawi, M.; Heikal, A.A. Expression of TNF-α, APRIL and BCMA in Behcet’s Disease. J. Immunol. Res. 2014, 2014, 380–405. [Google Scholar] [CrossRef]
- Xun, Y.; Chen, P.; Yan, H.; Yang, W.; Shi, L.; Chen, G.; Du, H. Identification of prohibitin as an antigen in Behcet’s disease. Biochem. Biophys. Res. Commun. 2014, 451, 389–393. [Google Scholar] [CrossRef]
- Vayá, A.; Rivera, L.; Todolí, J.; Hernandez, J.L.; Laiz, B.; Ricart, J.M. Haematological, biochemical and inflammatory parameters in inactive Behçet’s disease. Its association with red blood cell distribution width. Clin. Hemorheol. Microcirc. 2014, 56, 319–324. [Google Scholar] [CrossRef]
- Balta, I.; Balta, S.; Koryurek, O.M.; Demirkol, S.; Mikhailidis, D.P.; Celik, T.; Cakar, M.; Kucuk, U.; Eksioglu, M.; Kurt, Y.G. Serum endocan levels as a marker of disease activity in patients with Behçet disease. J. Am. Acad. Dermatol. 2013, 70, 291–296. [Google Scholar] [CrossRef]
- Ozuguz, P.; Karabulut, A.A.; Tulmac, M.; Kisa, U.; Kocak, M.; Gunduz, O. Markers of Endothelial Dysfunction and Evaluation of Vascular Reactivity Tests in Behçet Disease. Angiology 2013, 65, 937–943. [Google Scholar] [CrossRef]
- Mejía, J.-C.; Espinosa, G.; Tàssies, D.; Reverter, J.-C.; Cervera, R. Endogenous thrombin potential in Behçet’s disease: Relationship with thrombosis and anticoagulant therapy. Ann. Rheum. Dis. 2014, 32. [Google Scholar]
- Lopalco, G.; Lucherini, O.M.; Vitale, A.; Talarico, R.; Lopalco, A.; Galeazzi, M.; Lapadula, G.; Cantarini, L.; Iannone, F. Putative Role of Serum Amyloid-A and Proinflammatory Cytokines as Biomarkers for Behcet’s Disease. Medicine. 2015, 94, e1858. [Google Scholar] [CrossRef]
- Yuksel, M.; Yildiz, A.; Oylumlu, M.; Turkcu, F.M.; Bilik, M.Z.; Ekinci, A.; Elbey, B.; Tekbas, E.; Alan, S. Novel Markers of Endothelial Dysfunction and Inflammation in Behçet’s Disease Patients with Ocular Involvement: Epicardial Fat Thickness, Carotid Intima Media Thickness, Serum ADMA Level, and Neutrophil-to-Lymphocyte Ratio. Clin. Rheumatol. 2016, 35, 701–708. [Google Scholar] [CrossRef]
- Bassyouni, I.H.; Sharaf, M.; Wali, I.E.; Mansour, H.M. Clinical significance of Angiopoietin-1 in Behcet’s disease patients with vascular involvement. Hear. Vessel. 2015, 31, 918–924. [Google Scholar] [CrossRef]
- Tulunay, A.; Dozmorov, M.G.; Ture-Ozdemir, F.; Yilmaz, V.; Eksioglu-Demiralp, E.; Alibaz-Oner, F.; Ozen, G.; Wren, J.D.; Saruhan-Direskeneli, G.; Sawalha, A.H.; et al. Activation of the JAK/STAT pathway in Behcet’s disease. Genes Immun. 2014, 16, 170–175. [Google Scholar] [CrossRef]
- Belguendouz, H.; Messaoudene, D.; Lahmar-Belguendouz, K.; Djeraba, Z.; Otmani, F.; Terahi, M.; Tiar, M.; Hartani, D.; Lahlou-Boukoffa, O.; Touil-Boukoffa, C. In vivo and in vitro IL-18 production during uveitis associated with Behçet disease: Effect of glucocorticoid therapy. J. Fr. Ophtalmol. 2015, 38, 206–212. [Google Scholar] [CrossRef]
- Ozturk, C.; Balta, S.; Balta, I.; Demirkol, S.; Celik, T.; Turker, T.; Iyisoy, A.; Eksioglu, M. Neutrophil-Lymphocyte Ratio and Carotid-Intima Media Thickness in Patients with Behçet Disease without Cardiovascular Involvement. Angiology 2015, 66, 291–296. [Google Scholar] [CrossRef]
- Türkcü, F.M.; Şahin, A.; Cingü, A.K.; Kaya, S.; Yüksel, H.; Cinar, Y.; Batmaz, İ. Serum Omentin, Resistin and Tumour Necrosis Factor-α Levels in Behcet Patients with and without Ocular Involvement. Graefes Arch. Clin. Exp. Ophthalmol. 2015, 253, 1565–1568. [Google Scholar] [CrossRef]
- de Souza, A.W.S.; Perazzio, S.F.; de França, N.R.; Andrade, L.E.C.; Bijl, M.; Westra, J.; Kallenberg, C.G.M. High mobility group box 1 serum levels are increased in Behçet’s disease, but not associated with disease activity or disease manifestations. Rheumatology 2015, 54, 2151–2155. [Google Scholar] [CrossRef]
- Seo, J.; Ahn, Y.; Zheng, Z.; Kim, B.; Choi, M.; Bang, D.; Kim, D. Clinical significance of serum YKL -40 in Behçet disease. Br. J. Dermatol. 2015, 174, 1337–1344. [Google Scholar] [CrossRef]
- Yolbas, S.; Yildirim, A.; Gozel, N.; Uz, B.; Koca, S.S. Hematological Indices May Be Useful in the Diagnosis of Systemic Lupus Erythematosus and in Determining Disease Activity in Behçet’s Disease. Med. Princ. Pract. 2016, 25, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.-J.; Pan, J.-B.; Song, G.; Wen, X.-T.; Wu, Z.-Y.; Chen, S.; Mo, W.-X.; Zhang, F.-C.; Qian, J.; Zhu, H.; et al. Identification of Novel Biomarkers for Behcet Disease Diagnosis Using Human Proteome Microarray Approach. Mol. Cell. Proteom. 2017, 16, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Mejía, J.C.; Ortiz, T.; Tàssies, D.; Solanich, X.; Vidaller, A.; Cervera, R.; Reverter, J.C.; Espinosa, G. Procoagulant microparticles are increased in patients with Behçet’s disease but do not define a specific subset of clinical manifestations. Clin. Rheumatol. 2015, 35, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Balkarli, A.; Kucuk, A.; Babur, H.; Erbasan, F. Neutrophil/Lymphocyte Ratio and Mean Platelet Volume in Behçet’ s Disease. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 3045–3050. [Google Scholar]
- Park, J.-S.; Kang, M.-I.; Ha, Y.-J.; Song, J.J.; Park, Y.-B.; Lee, S.-K.; Lee, S.-W. Serum anti-lysozyme is associated with disease activity of Behçet’s disease. Int. J. Rheum. Dis. 2016, 20, 261–268. [Google Scholar] [CrossRef]
- Cantarini, L.; Pucino, V.; Vitale, A.; Talarico, R.; Lucherini, O.M.; Magnotti, F.; De Rosa, V.; Galgani, M.; Alviggi, C.; Marone, G.; et al. Immunometabolic biomarkers of inflammation in Behçet’s disease: Relationship with epidemiological profile, disease activity and therapeutic regimens. Clin. Exp. Immunol. 2016, 184, 197–207. [Google Scholar] [CrossRef]
- Cure, E.; Icli, A.; Uslu, A.U.; Baykara, R.A.; Sakiz, D.; Ozucan, M.; Yavuz, F.; Arslan, S.; Cure, M.C.; Kucuk, A. Atherogenic index of plasma may be strong predictor of subclinical atherosclerosis in patients with Behçet disease. Z. Rheumatol. 2016, 76, 259–266. [Google Scholar] [CrossRef]
- Jiang, Y.; Zang, M.; Li, S. Serum PLR and LMR in Behçet’s disease. Medicine 2017, 96, e6981. [Google Scholar] [CrossRef]
- Kang, S.E.; Lee, S.J.; Lee, J.Y.; Yoo, H.J.; Park, J.K.; Lee, E.Y.; Lee, E.B.; Song, Y.W. Serum Levels of IgG Antibodies against Alpha-Enolase Are Increased in Patients with Behçet’s Disease and Are Associated with the Severity of Oral Ulcer, Erythrocyte Sedimentation Rates, and C-Reactive Protein. Clin. Exp. Rheumatol. 2017, 35, S67–S74. [Google Scholar]
- Ahn, J.K.; Kim, J.; Hwang, J.; Song, J.; Kim, K.H.; Cha, H.S. Urinary Metabolomic Profiling to Identify Potential Biomarkers for the Diagnosis of Behcet’s Disease by Gas Chromatography/Time-of-Flight-Mass Spectrometry. Int. J. Mol. Sci. 2017, 18, 2309. [Google Scholar] [CrossRef]
- Lee, H.J.; Kim, J.H.; Kim, S.W.; Joo, H.A.; Lee, H.W.; Kim, Y.S.; Park, S.J.; Hong, S.P.; Il Kim, T.; Kim, W.H.; et al. Proteomic Analysis of Serum Amyloid A as a Potential Marker in Intestinal Behçet’s Disease. Dig. Dis. Sci. 2017, 62, 1953–1962. [Google Scholar] [CrossRef]
- Ha, Y.-J.; Park, J.-S.; Kang, M.-I.; Lee, S.-K.; Park, Y.-B.; Lee, S.-W. Increased serum interleukin-32 levels in patients with Behçet’s disease. Int. J. Rheum. Dis. 2017, 21, 2167–2174. [Google Scholar] [CrossRef]
- Lopalco, G.; Lucherini, O.M.; Lopalco, A.; Venerito, V.; Fabiani, C.; Frediani, B.; Galeazzi, M.; Lapadula, G.; Cantarini, L.; Iannone, F. Cytokine Signatures in Mucocutaneous and Ocular Behçet’s Disease. Front. Immunol. 2017, 8, 200. [Google Scholar] [CrossRef]
- Omma, A.; Sandikci, S.C.; Colak, S.; Tecer, D.; Yücel, C.; Ozbalkan, Z. Serum calprotectin and ischemia modified albumin levels as markers of disease activity in Behçet’s disease. Adv. Dermatol. Allergol. 2018, 35, 609–613. [Google Scholar] [CrossRef]
- Koca, T.T. Clinical Significance of Serum Bilirubin in Behçet’s Disease. J. Transl. Intern. Med. 2018, 6, 185–188. [Google Scholar] [CrossRef]
- Enecik, M.; Mavi, B.; Yücel, C.; Keskin, G.; Yıldız, M. The importance of Serum Interleukin-20 Levels in Patients with Behçet’s Disease. Adv. Clin. Exp. Med. 2018, 27, 1391–1395. [Google Scholar] [CrossRef]
- Harmanci, K.; Akan, O.Y.; Pirildar, T.; Ortan, P.; Ulman, C. The Evaluation of the Relationship between sTREM-1, VEGF-B, and VEGF Gene Expression Levels with Disease Activity of Behçet’s Patients. Dis. Markers 2018, 2018, 1–5. [Google Scholar] [CrossRef]
- Lucherini, O.M.; Vitale, A.; Orlando, I.; Sota, J.; Fabiani, C.; Franceschini, R.; Simpatico, A.; Frediani, B.; Galeazzi, M.; Tosi, G.M.; et al. Serum immunoglobulin D levels in patients with Behçet’s disease according to different clinical manifestations. Ann. Rheum. Dis. 2018, 36, 110–115. [Google Scholar]
- Chekaoui, A.; Lahmar, K.; Belguendouz, H.; Mazari, F.; Terahi, M.; Hakem, D.; Youinou, P.; Touil-Boukoffa, C. Increased IL-1β Levels Are Associated with an Imbalance of “Oxidant/Antioxidant” Status during Behçet’s Disease. Eur. Cytokine Netw. 2018, 29, 95–102. [Google Scholar] [CrossRef]
- Kolahi, S.; Farajzadeh, M.J.; Alipour, S.; Abhari, A.; Farhadi, J.; Bahavarnia, N.; Malek Mahdavi, A.; Khabbazi, A.; Sakhinia, E. Determination of Mir-155 and Mir-146a Expression Rates and Its Association with Expression Level of TNF-α and CTLA4 Genes in Patients with Behcet’s Disease. Immunol. Lett. 2018, 204, 55–59. [Google Scholar] [CrossRef]
- Hassouna, S.S.; Tayel, M.Y.; ElKaffash, D.M.; Abdelhady, A.M.; Elsayed, E.H. MicroRNA155 Expression in Relation to BDCAF Scored Behçet’s Disease in an Egyptian Patients’ Sample. Open Rheumatol. J. 2018, 12, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Kurtipek, G.S.; Kesli, R.; Akyurek, F.T.; Akyurek, F.; Ataseven, A.; Terzi, Y. Plasma-soluble urokinase plasminogen activator receptor (suPAR) levels in Behçet’s disease and correlation with disease activity. Int. J. Rheum. Dis. 2016, 21, 866–870. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, M.; Yousefi, M.; Abbaspour-Aghdam, S.; Dolati, S.; Aghebati-Maleki, L.; Eghbal-Fard, S.; Khabbazi, A.; Rostamzadeh, D.; Alipour, S.; Shabani, M.; et al. Disturbed Th17/Treg Balance, Cytokines, and MiRNAs in Peripheral Blood of Patients with Behcet’s Disease. J. Cell. Physiol. 2019, 234, 3985–3994. [Google Scholar] [CrossRef] [PubMed]
- Prado, L.L.; Goncalves, C.R.; Viana, V.T.; Saad, C.G.S.; Bonfa, E. Anti-Alpha-Enolase Antibodies in Behçet’s Disease: A Marker of Mucocutaneous and Articular Disease Activity? Clin. Exp. Rheumatol. 2018, 36, 28–32. [Google Scholar] [PubMed]
- Acikgoz, N.; Kurtoğlu, E.; Yagmur, J.; Kapicioglu, Y.; Cansel, M.; Ermis, N. Elevated Monocyte to High-Density Lipoprotein Cholesterol Ratio and Endothelial Dysfunction in Behçet Disease. Angiology 2017, 69, 65–70. [Google Scholar] [CrossRef]
- Hasan, M.S.; Ryan, P.L.; A Bergmeier, L.; Fortune, F. Circulating NK cells and their subsets in Behçet’s disease. Clin. Exp. Immunol. 2017, 188, 311–322. [Google Scholar] [CrossRef]
- Zheng, W.; Wu, X.; Goudarzi, M.; Shi, J.; Song, W.; Li, C.; Liu, J.; Chen, H.; Zhang, X.; Zeng, X.; et al. Metabolomic Alterations Associated with Behçet’s Disease. Arthritis Res. Ther. 2018, 20, 1–10. [Google Scholar] [CrossRef]
- Şahin, A.; Ilhan, A.; Derin, M.E.; Doğan, H.O.; Şahin, M. Low levels of pannexin-1 in Behçet’s syndrome. Int. J. Rheum. Dis. 2019, 22, 1474–1478. [Google Scholar] [CrossRef]
- Bassyouni, I.H.; Mohammed, W.H.S.; Taha, F.M.; El Refai, R.M. Clinical significance of CCN2/connective tissue growth factor in Behçet’s disease patients. Int. J. Rheum. Dis. 2019, 22, 1459–1465. [Google Scholar] [CrossRef]
- Arica, D.A.; Akşan, B.; Örem, A.; Altinkaynak, B.A.; Yayli, S.; Sönmez, M. High levels of endothelial progenitor cells and circulating endothelial cells in patients with Behçet’s disease and their relationship to disease activity. An. Bras. de Dermatol. 2019, 94, 320–326. [Google Scholar] [CrossRef]
- Sandikci, S.C.; Colak, S.; Omma, A.; Enecik, M.E.; Ozbalkan, Z.; Neselioglu, S.; Erel, O. An investigation of thiol/disulfide homeostasis in patients with Behçet’s disease. Arch. Med Sci. 2020, 16, 1353–1359. [Google Scholar] [CrossRef]
- Talaat, R.M.; Sibaii, H.; Bassyouni, I.H.; El-Wakkad, A. IL-17, IL-10, IL-6, and IFN-γ in Egyptian Behçet’s Disease: Correlation with Clinical Manifestations. Eur. Cytokine Netw. 2019, 30, 15–22. [Google Scholar] [CrossRef]
- Gheita, T.A.; Sakr, B.R.; Rabea, R.E.; Abd ElHamid, S.M. Value of Hematological Indices versus VEGF as Biomarkers of Activity in Behçet’s Disease. Clin. Rheumatol. 2019, 38, 2201–2210. [Google Scholar] [CrossRef]
- El Boghdady, N.A.; Shaker, O.G. Role of Serum MiR-181b, Proinflammatory Cytokine, and Adhesion Molecules in Behçet’s Disease. J. Interferon Cytokine Res. 2019, 39, 347–354. [Google Scholar] [CrossRef]
- Balbaba, M.; Ulaş, F.; Postacı, S.A.; Öz, B.; Aydın, S. Serum Cortistatin Levels in Patients with Ocular Active and Ocular Inactive Behçet Disease. Ocul. Immunol. Inflamm. 2019, 28, 601–605. [Google Scholar] [CrossRef]
- A Hassan, W.; Behiry, E.G.; Abdelshafy, S.; Salem, T.; A Baraka, E. Assessment of Endocan Serum Level in Patients with Behçet Disease: Relation to Disease Activity and Carotid Intima Media Thickness. Egypt J. Immunol. 2020, 27, 129–139. [Google Scholar]
- Hussain, M.; Chen, P.; Zhang, Y.; Tian, Y.; Du, H. Moesin expression is correlated with its involvement in patients with Behcet’s disease. Arch. Med Sci. 2020, 16, 924–930. [Google Scholar] [CrossRef]
- Hussain, M.; Ma, F.; Chen, P.; Tian, Y.; Du, H. Circulation autoantibodies against C-terminus of NuMA in patients with Behçet’s disease. Central Eur. J. Immunol. 2020, 45, 86–92. [Google Scholar] [CrossRef]
- Djaballah-Ider, F.; Touil-Boukoffa, C. Effect of Combined Colchicine-Corticosteroid Treatment on Neutrophil/Lymphocyte Ratio: A Predictive Marker in Behçet Disease Activity. Inflammopharmacology 2020, 28, 819–829. [Google Scholar] [CrossRef]
- Cheng, L.; Li, L.; Liu, C.; Yan, S.; Chen, H.; Li, H.; Zhang, F.; Chen, H.; Li, Y. Variation of Red Blood Cell Parameters in Behcet’s Disease: Association with Disease Severity and Vascular Involvement. Clin. Rheumatol. 2021, 40, 1457–1464. [Google Scholar] [CrossRef]
- Choi, H.J.; Seo, M.R.; Ryu, H.J.; Baek, H.J. Cross-Cultural Adaptation and Validation of the Behcet’s Disease Current Activity Form in Korea. Korean J. Intern. Med. 2015, 30, 714. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.K.; Kim, J.; Hwang, J.; Song, J.; Kim, K.H.; Cha, H.S. Potential Metabolomic Biomarkers for Reliable Diagnosis of Behcet’s Disease Using Gas Chromatography/ Time-of-Flight-Mass Spectrometry. Jt. Bone Spine 2018, 85, 337–343. [Google Scholar] [CrossRef]
- Filleron, A.; Tran, T.A.; Hubert, A.; Letierce, A.; Churlaud, G.; KonCrossed, D.; Sign-Paut, I.; Saadoun, D.; Cezar, R.; Corbeau, P.; et al. Regulatory T Cell/Th17 Balance in the Pathogenesis of Paediatric Behçet Disease. Rheumatology. 2021, 61, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Na, S.Y.; Park, M.J.; Park, S.; Lee, E.S. Up-Regulation of Th17 and Related Cytokines in Behçet’s Disease Corresponding to Disease Activity. Clin. Exp. Rheumatol. 2013, 31, 32–40. [Google Scholar] [PubMed]
- Zhou, L.; Lopes, J.E.; Chong, M.M.W.; Ivanov, I.I.; Min, R.; Victora, G.D.; Shen, Y.; Du, J.; Rubtsov, Y.P.; Rudensky, A.Y.; et al. TGF-β-Induced Foxp3 Inhibits Th17 Cell Differentiation by Antagonizing RORγt Function. Nature 2008, 453, 236. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, I.I.; Tuganbaev, T.; Skelly, A.N.; Honda, K. T Cell Responses to the Microbiota. Annu. Rev. Immunol. 2022, 40, 559–587. [Google Scholar] [CrossRef]
- Zhou, Q.; Xiao, X.; Wang, C.; Zhang, X.; Li, F.; Zhou, Y.; Kijlstra, A.; Yang, P. Decreased MicroRNA-155 Expression in Ocular Behcet’s Disease but Not in Vogt Koyanagi Harada Syndrome. Invest. Ophthalmol. Vis. Sci. 2012, 53, 5665–5674. [Google Scholar] [CrossRef]
- Na, S.Y.; Park, M.J.; Park, S.; Lee, E.S. MicroRNA-155 Regulates the Th17 Immune Response by Targeting Ets-1 in Behçet’s Disease. Clin. Exp. Rheumatol. 2016, 34, 56–63. [Google Scholar]
- Seyahi, E. Phenotypes in Behçet’s syndrome. Intern. Emerg. Med. 2019, 14, 67. [Google Scholar] [CrossRef]
- Consolandi, C.; Turroni, S.; Emmi, G.; Severgnini, M.; Fiori, J.; Peano, C.; Biagi, E.; Grassi, A.; Rampelli, S.; Silvestri, E.; et al. Behçet’s syndrome patients exhibit specific microbiome signature. Autoimmun. Rev. 2015, 14, 269–276. [Google Scholar] [CrossRef]
- Wang, Q.; Yi, S.; Su, G.; Du, Z.; Pan, S.; Huang, X.; Cao, Q.; Yuan, G.; Kijlstra, A.; Yang, P. Changes in the Gut Microbiome Contribute to the Development of Behcet’s Disease via Adjuvant Effects. Front Cell Dev Biol. 2021, 9, 716760. [Google Scholar] [CrossRef] [PubMed]
- Pagliai, G.; Dinu, M.; Fiorillo, C.; Becatti, M.; Turroni, S.; Emmi, G.; Sofi, F. Modulation of gut microbiota through nutritional interventions in Behçet’s syndrome patients (the MAMBA study): Study protocol for a randomized controlled trial. Trials 2020, 21, 511. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| REF | Year | First Author | Country | Design | BD Patients, n | Controls, n | Biomarker Tested | Urinary/ Serologic | Diagnostic/Activity |
|---|---|---|---|---|---|---|---|---|---|
| [14] | 1995 | Yosipovitch et al. | Israel | Retrospective | 25 | 20 | IL-1B | S | Diagnostic |
| SIL-2R | S | Diagnostic | |||||||
| [15] | 1995 | Deǧer et al. | Turkey | Retrospective | 42 (20 active) | 40 | PMN elastase | S | Diagnostic/Activity |
| [16] | 1995 | Direskeneli et al. | UK | Retrospective | 70 (56 active) | 52 | AECA | S | Diagnostic/Activity |
| vVF | S | Diagnostic | |||||||
| [17] | 1997 | Uslu et al. | Turkey | Retrospective | 27 | 18 | ET-1 | S | Diagnostic |
| [18] | 1998 | Alpsoy et al. | Turkey | Retrospective | 32 (14 active) | 20 | IL-2 | S | Diagnostic |
| SIL-2R | S | Activity | |||||||
| [19] | 2000 | Katsantonis et al. | Germany | Retrospective | 34 (25 active) | N/A | IL-8 | S | Activity |
| [20] | 2000 | Eksioglu-Demiralp et al. | Turkey | Retrospective | 37 | 55 | CD4+CD16+ | S | Diagnostic |
| CD4+CD56+ | S | Diagnostic | |||||||
| [21] | 2000 | Freysdottir et al. | UK | Retrospective | 20 | 26 | T-γδ | S | Diagnostic |
| CD56 | S | Diagnostic | |||||||
| [22] | 2002 | Krause et al. | Israel | Retrospective | 27 | 20 | IgG ASCA | S | Diagnostic |
| IgA ASCA | S | Diagnostic | |||||||
| [23] | 2002 | Evereklioglu et al. | Turkey | Retrospective | 35 (18 active) | 20 | Leptin | S | Diagnostic/Activity |
| [24] | 2002 | Er et al. | Turkey | Retrospective | 43 (20 active) | 52 | ET-1 | S | Diagnostic/Activity |
| Homocysteine | S | Diagnostic/Activity | |||||||
| NO | S | Diagnostic/Activity | |||||||
| [25] | 2002 | Saglam et al. | Turkey | Retrospective | 44 (23 active) | 30 | cICAM-1 | S | Diagnostic/Activity |
| [26] | 2002 | Evereklioglu et al. | Turkey | Retrospective | 52 (27 active) | 32 | NO | S | Diagnostic/Activity |
| [27] | 2003 | Evereklioglu et al. | Turkey | Retrospective | 36 (16 active) | 20 | NO (urinary) | U | Diagnostic/Activity |
| NO (serum) | S | Diagnostic/Activity | |||||||
| [28] | 2003 | Erkiliç et al. | Turkey | Retrospective | 35 (17 active) | 20 | ADA | S | Diagnostic/Activity |
| TBARS | S | Diagnostic | |||||||
| Plasmatic SOD | S | Diagnostic/Activity | |||||||
| RBC SOD | S | Diagnostic/Activity | |||||||
| Plasmatic GSHPx | S | Diagnostic/Activity | |||||||
| RBC GSHPx | S | Diagnostic/Activity | |||||||
| RBC Catalase | S | Diagnostic | |||||||
| [29] | 2004 | Akdeniz et al. | Turkey | Retrospective | 27 | 16 | IL-6 | S | Diagnostic |
| Il-2 | S | Diagnostic | |||||||
| TNF-α | S | Diagnostic | |||||||
| NO | S | Diagnostic | |||||||
| [30] | 2004 | Sari et al. | Turkey | Retrospective | 23 | 20 | E-selectine | S | Diagnostic |
| ESR | S | Diagnostic | |||||||
| PCR | S | Diagnostic | |||||||
| [31] | 2004 | Yazici et al. | Turkey | Retrospective | 49 (31 active) | 40 | MPO | S | Diagnostic/Activity |
| AOPP | S | Diagnostic/Activity | |||||||
| Thiol | S | Diagnostic/Activity | |||||||
| [32] | 2004 | Duygulu et al. | Turkey | Retrospective | 23 (11 active) | 15 | NO | S | Diagnostic/Activity |
| [33] | 2005 | Ureten et al. | Turkey | Retrospective | 72 (37 active) | 73 | CD64 | S | Diagnostic/Activity |
| [34] | 2005 | Calis et al. | Turkey | Retrospective | 75 (50 active) | 25 | ADA | S | Diagnostic/Activity |
| [35] | 2005 | Qiao et al. | Japan | Retrospective | 35 (15 active) | 16 | CXCR2 | S | Diagnostic/Activity |
| [36] | 2005 | Gür-Toy et al. | Turkey | Retrospective | 67 | 0 | IL-8 | S | Activity |
| CRP | S | Diagnostic | |||||||
| ESR | S | Diagnostic | |||||||
| [37] | 2005 | Coskun et al. | Turkey | Retrospective | 40 (25 active) | 30 | Neopterin | S | Diagnostic/Activity |
| ESR | P | Diagnostic/Activity | |||||||
| CRP | S | Diagnostic/Activity | |||||||
| [38] | 2006 | Yardim-Akaydin et al. | Turkey | Retrospective | 23 | 43 | Allantoin | S | Diagnostic |
| MDA | S | Diagnostic | |||||||
| Ascorbic acid | S | Diagnostic | |||||||
| [39] | 2006 | Kose et al. | Turkey | Retrospective | 68 (51 active) | 17 | Neopterin | S | Diagnostic/Activity |
| [40] | 2006 | Canpolat et al. | Turkey | Retrospective | 23 (10 active) | 20 | ADA | S | Diagnostic/Activity |
| Erythrocyte ADA | S | Diagnostic/Activity | |||||||
| [41] | 2006 | Kwon et al. | South Korea | Prospective | 211 (92 active) | N/A | Protein S | S | Activity |
| [42] | 2006 | Briani et al. | Italy | Retrospective | 32 | 118 | Anti-HS igM | S | Diagnostic |
| Anti-HS igG | S | Diagnostic | |||||||
| [43] | 2006 | Sarican et al. | Turkey | Retrospective | 64 (25 active) | 26 | Homocysteine | S | Diagnostic/Activity |
| [44] | 2007 | Lee et al. | South Korea | Retrospective | 50 (26 active) | UK | Gal-3 | S | Diagnostic/Activity |
| G3BP | S | Activity | |||||||
| [45] | 2007 | Pay S et al. | Turkey | Retrospective | 58 (23 active) | 20 | MMP-2 | S | Diagnostic |
| MMP-9 | S | Diagnostic/Activity | |||||||
| [46] | 2008 | Öztürk et al. | Turkey | Retrospective | 21 | 21 | VEGF | S | Diagnostic |
| ESR | S | Diagnostic | |||||||
| CRP | S | Diagnostic | |||||||
| [47] | 2008 | Turan et al. | Turkey | Prospective | 35 | N/A | sTNFR1 | S | Activity |
| sTNFR2 | S | Activity | |||||||
| [48] | 2008 | Kutlay et al. | Turkey | Retrospective | 45 (33 active) | 15 | CEC | S | Diagnostic/Activity |
| [49] | 2008 | Curnow et al. | UK | Retrospective | 52 (24 active) | 35 | IL-15 | S | Diagnostic/Activity |
| CXCL-8 | S | Diagnostic/Activity | |||||||
| TNF-α | S | Diagnostic/Activity | |||||||
| [50] | 2008 | Polat et al. | Turkey | Retrospective | 32 | 16 | IL-8 | S | Diagnostic/Activity |
| [51] | 2008 | Durmazlar et al. | Turkey | Retrospective | 45 (33 active) | 29 | IL-8 | S | Diagnostic/Activity |
| [52] | 2009 | Habibagah et al. | Iran | Retrospective | 53 (15 active) | 44 | IL-23 | S | Diagnostic/Activity |
| E–cadherin | S | Diagnostic | |||||||
| [53] | 2009 | Fadini et al. | Italy | Retrospective | 30 | 27 | CD34+KDR+ EPCs | S | Diagnostic |
| CD34+CD133+KDR+ EPCs | S | Diagnostic | |||||||
| [54] | 2010 | Choe et al. | South Korea | Retrospective | 59 (21 active) | 65 | Angiopoietin-1 | S | Diagnostic |
| Angiopoietin-2 | S | Diagnostic | |||||||
| [55] | 2010 | Donmez et al. | Turkey | Retrospective | 89 (17 active) | 86 | aTAFI | S | Diagnostic |
| Thrombomodulin | Diagnostic | ||||||||
| [56] | 2010 | Sezer et al. | Turkey | Retrospective | 60 (33 active) | 46 | MDA | S | Diagnostic |
| 8-OHdG | S | Diagnostic/Activity | |||||||
| T-SH | S | Diagnostic | |||||||
| [57] | 2011 | Özden et al. | Turkey | Retrospective | 70 | 61 | Gal-3 | S | Diagnostic/Activity |
| [58] | 2011 | Pehlivan et al. | Turkey | Retrospective | 45 (25 active) | 30 | Resistin | S | Diagnostic/Activity |
| TNF-α | S | Diagnostic/Activity | |||||||
| [59] | 2011 | Ahn et al. | South Korea | Retrospective | 71 (21 active) | 34 | α defensin1 | S | Activity |
| αdefensin1 mRNA | S | Diagnostic/Activity | |||||||
| [60] | 2011 | Shin et al. | South Korea | Retrospective | 80 | 23 | AAEA | S | Diagnostic |
| [61] | 2011 | Jung et al. | South Korea | Retrospective | 88 (30 severe, 12 moderate) | 10 | sTREM1 | S | Diagnostic/Activity |
| TNF-α | Diagnostic | ||||||||
| [62] | 2011 | Vural et al. | Turkey | Retrospective | 20 | 40 | STIP-1 | S | Diagnostic |
| [63] | 2012 | Bello et al. | Spain | Retrospective | 30 | 28 | sCD40L | S | Diagnostic |
| MMP-9 | S | Diagnostic | |||||||
| [64] | 2012 | Gündüz et al. | Turkey | Retrospective | 40 (11 active) | 20 | CD4+CD25+FOXP3+Treg | S | Diagnostic/Activity |
| CD4+FOXP3+Treg | S | Diagnostic/Activity | |||||||
| [65] | 2012 | Wang et al. | China | Retrospective | 49 | 79 | Proteomic analysis | S | Diagnostic |
| [66] | 2013 | Örem et al. | Turkey | Retrospective | 72 (40 active) | 30 | Lipoprotein-associated phospholipase A2 | S | Diagnostic/Activity |
| CRP | S | Diagnostic/Activity | |||||||
| ESR | S | Diagnostic/Activity | |||||||
| [67] | 2013 | Hamzaoui et al. | Tunisia | Retrospective | 46 (20 active) | 70 | IL-33 | S | Diagnostic/Activity |
| IL6 | S | Diagnostic | |||||||
| IL7 | S | Diagnostic | |||||||
| [68] | 2013 | Vural et al. | Turkey | Retrospective | 144 | 168 | MTCH1 Ab | S | Diagnostic |
| [69] | 2014 | Shaker et al. | Egypt | Retrospective | 30 (20 active) | 20 | TNF- α | S | Diagnostic/Activity |
| APRIL | S | Diagnostic/Activity | |||||||
| BCMA | S | Diagnostic/Activity | |||||||
| BAFF | S | Diagnostic/Activity | |||||||
| CRP | S | Diagnostic/Activity | |||||||
| ESR | S | Diagnostic/Activity | |||||||
| [70] | 2014 | Xun et al. | China | Retrospective | 58 | 106 | Prohibitin | S | Diagnostic |
| [71] | 2014 | Vayà et al. | Spain | Retrospective | 89 | 94 | RDW | S | Diagnostic |
| CRP | S | Diagnostic | |||||||
| Fibrinogen | S | Diagnostic | |||||||
| Leucocytes | S | Diagnostic | |||||||
| Neutrophils | S | Diagnostic | |||||||
| [72] | 2014 | Balta et al. | Turkey | Retrospective | 33 (16 active) | 35 | Endocan | S | Diagnostic/Activity |
| CRP | S | Diagnostic | |||||||
| ESR | S | Diagnostic | |||||||
| [73] | 2014 | Ozuguz et al. | Turkey | Prospective | 40 | 20 | ADMA | S | Diagnostic |
| CRP | S | Diagnostic/Activity | |||||||
| ESR | S | Diagnostic/Activity | |||||||
| Homocysteine | S | Diagnostic/Activity | |||||||
| [74] | 2014 | Mejia et al. | Spain | Prospective | 56 (17 active) | 56 | Prothrombin fragm. 1.2 | S | Diagnostic/Activity |
| Factor VIII | S | Diagnostic/Activity | |||||||
| vWF | S | Diagnostic | |||||||
| [75] | 2015 | Lopalco et al. | Italy | Prospective | 58 | 32 | IL-6 | S | Diagnostic |
| IL-8 | S | Diagnostic | |||||||
| IL-18 | S | Diagnostic | |||||||
| IFN-α | S | Diagnostic | |||||||
| CXCL11 | S | Diagnostic | |||||||
| [76] | 2015 | Yuksel et al. | Turkey | Retrospective | 36 (17 active) | 35 | ADMA | S | Diagnostic/Activity |
| NLR | S | Diagnostic/Activity | |||||||
| [77] | 2015 | Bassyouni et al. | Egypt | Retrospective | 47 | 30 | Angiopoietin-1 | S | Diagnostic |
| [78] | 2015 | Tulunay et al. | Turkey | Retrospective | 26 | 26 | STAT3 | S | Diagnostic |
| [79] | 2015 | Belguendouz et al. | Algeria | Retrospective | 26 (16 active) | 17 | IL-18 | S | Activity |
| [80] | 2015 | Ozturk et al. | Turkey | Retrospective | 65 (40 active) | 62 | NLR | S | Diagnostic/Activity |
| [81] | 2015 | Turkcu et al. | Turkey | Retrospective | 51 (25 active) | 24 | TNF-α | S | Diagnostic |
| Resistin | S | Diagnostic | |||||||
| Omentin | S | Diagnostic | |||||||
| [82] | 2015 | De Souza et al. | Brazil | Retrospective | 26 (13 active) | 20 | HMGB1 | S | Diagnostic |
| [83] | 2015 | Seo et al. | South Korea | Retrospective | 112 (66 active) | 45 | YKL-40 | S | Diagnostic/Activity |
| [84] | 2016 | Yolbas et al. | Turkey | Retrospective | 53 (6 active) | 55 | NLR | S | Activity |
| 91 | |||||||||
| 51+39 | |||||||||
| [85] | 2016 | Hu et al. | China | Retrospective Phase I | 40 (identification) | 35 | Protein microarray | ||
| Phase II | 130 (validation) | 223 | Anti-CTDP1 Ab | S | Diagnostic | ||||
| [86] | 2016 | Mejia et al. | Spain | Retrospective | 55 | 73 | Procoagulant microparticles | S | Diagnostic |
| [87] | 2016 | Balkarli et al. | Turkey | Retrospective | 186 (120 active) | 79 | NLR | S | Diagnostic |
| ESR | S | Diagnostic/Activity | |||||||
| CRP | S | Diagnostic | |||||||
| [88] | 2016 | Park et al. | South Korea | Retrospective | 51 (29 active) | N/A | Anti-lysozyme | S | Activity |
| [89] | 2016 | Cantarini et al. | Italy | Retrospective | 27 (57 total samples: 21 from active, 36 inactive) | 36 | CD40L | S | Diagnostic |
| Leptin | S | Diagnostic | |||||||
| sTNFR | S | Diagnostic | |||||||
| IL-6 | S | Diagnostic | |||||||
| ESR | S | Activity | |||||||
| [90] | 2017 | Cure et al. | Turkey | Retrospective | 84 | 84 | AIP | S | Diagnostic/Activity |
| CRP | S | Diagnostic | |||||||
| [91] | 2017 | Jiang et al. | China | Retrospective | 140 (108 active) | 107 | PLR | S | Diagnostic/Activity |
| LMR | S | Diagnostic | |||||||
| ESR | S | Activity | |||||||
| CRP | S | Activity | |||||||
| [92] | 2017 | Kang et al. | South Korea | Retrospective | 110 | 110 | AAEA IgG | S | Diagnostic |
| [93] | 2017 | Ahn JK et al. | South Korea | Retrospective | 44 | 41 | Panel of 10 urinary biomarkers: guanine, pyrrole-2-carboxylate, 3-hydroxypyroline, mannose, L-citrulline, galactonate, isothreonate, sedoheptulose, hypoxanthine, and gluconic acidlactonate | U | Diagnostic |
| Guanine | U | Diagnostic | |||||||
| Pyrrole-2-carboxylate | U | Diagnostic | |||||||
| 3-hydroxypyroline | U | Diagnostic | |||||||
| Mannose | U | Diagnostic | |||||||
| L-citrulline | U | Diagnostic | |||||||
| Galactonate | U | Diagnostic | |||||||
| Isothreonate | U | Diagnostic | |||||||
| Sedoheptulose | U | Diagnostic | |||||||
| Hypoxanthine | U | Diagnostic | |||||||
| Gluconic acidlactonate | U | Diagnostic | |||||||
| [94] | 2017 | Lee et al. | South Korea | Retrospective Phase I | 15 (identification) | 15 | Fibrin, apoliprorotein A-IV and SAA | S | Diagnostic |
| Phase II | 49 (validation) | 41 | SAA | S | Diagnostic | ||||
| IL-1β | S | Diagnostic | |||||||
| [95] | 2017 | Ha et al. | South Korea | Retrospective | 50 (29 active) | 35 | IL-32 | S | Diagnostic |
| [96] | 2017 | Lopalco et al. | Italy | Retrospective | 46 | 19 | sTNFR1 | S | Diagnostic |
| sTNFR2 | S | Diagnostic | |||||||
| Chitinase3-like1 | S | Diagnostic | |||||||
| gp130/sIL-6Rb | S | Diagnostic | |||||||
| IL-26 | S | Diagnostic | |||||||
| [97] | 2018 | Omma et al. | Turkey | Retrospective | 93 (57 active) | 62 | Calprotectin | S | Diagnostic |
| CRP | S | Diagnostic | |||||||
| IMA | S | Diagnostic | |||||||
| [98] | 2018 | Koca et al. | Turkey | Retrospective | 71 | 75 | Bilirubin | S | Diagnostic |
| [99] | 2018 | Enecik et al. | Turkey | Retrospective | 45 (28 active) | 25 | IL-20 | S | Diagnostic |
| [100] | 2018 | Harmanci et al. | Turkey | Retrospective | 30 | 30 | VEGF gene expression levels | S | Diagnostic |
| [101] | 2018 | Lucherini et al. | Italy | Retrospective | 72 | 29 | IgD | S | Diagnostic |
| [102] | 2018 | Chekaoui et al. | Algeria | Retrospective | 48 (28 active) | 41 | IL-1β | S | Diagnostic/Activity |
| NO | S | Diagnostic/Activity | |||||||
| AOPP | S | Diagnostic/Activity | |||||||
| MDA | S | Diagnostic | |||||||
| SOD | S | Diagnostic/Activity | |||||||
| [103] | 2018 | Kolahi et al. | Iran | Retrospective | 47 | 61 | mir-155 | S | Diagnostic |
| TNF-α expression | S | Diagnostic | |||||||
| [104] | 2018 | Ahn et al. | South Korea | Retrospective | 45 | 45 | Panel of 5 biomarkers: DA, fructose, tagatose, LA, and OA | S | Diagnostic |
| [105] | 2018 | Saylam et al. | Turkey | Retrospective | 30 | 41 | suPAR | S | Diagnostic |
| CRP | S | Diagnostic | |||||||
| [106] | 2018 | Ahmadi et al. | Iran | Retrospective | 47 | 58 | Th17 | S | Diagnostic |
| Treg | S | Diagnostic | |||||||
| RORɣt mRNA | S | Diagnostic | |||||||
| FoxP3 mRNA | S | Diagnostic | |||||||
| IL-17mRNA | S | Diagnostic | |||||||
| IL-23 mRNA | S | Diagnostic | |||||||
| TGF mRNA | S | Diagnostic | |||||||
| IL-10 mRNA | S | Diagnostic | |||||||
| IL-17 | S | Diagnostic | |||||||
| IL-23 | S | Diagnostic | |||||||
| IL-10 | S | Diagnostic | |||||||
| TFG-beta | S | Diagnostic | |||||||
| miR-93 | S | Diagnostic | |||||||
| miR-106b | S | Diagnostic | |||||||
| miR-25 | S | Diagnostic | |||||||
| miR-146° | S | Diagnostic | |||||||
| miR-155 | S | Diagnostic | |||||||
| miR-326 | S | Diagnostic | |||||||
| [104] | 2018 | Hassouna et al. | Egypt | Retrospective | 30 | 15 | miR-155 | S | Diagnostic |
| [107] | 2018 | Prado et al. | Brazil | Retrospective | 97 (43 active) | 123 | AAEA IgM | S | Diagnostic/Activity |
| [108] | 2018 | Acikgoz et al. | Turkey | Retrospective | 60 | 50 | MHR | S | Diagnostic |
| [109] | 2018 | Hasan et al. | UK | Retrospective | 60 (44 active) | 60 | NK | S | Diagnostic |
| CD56Dim | S | Diagnostic | |||||||
| CD56Brigh | S | Diagnostic | |||||||
| [110] | 2018 | Zheng et al. | China | Retrospective Phase I | 24 (identification) | 26 | PC (34:3) | S | Diagnostic |
| PC (40:8) | S | Diagnostic | |||||||
| LA | S | Diagnostic | |||||||
| AA | S | Diagnostic | |||||||
| Phase II | 25 (validation) | 19 | LA | S | Diagnostic | ||||
| 27 | AA | S | Diagnostic | ||||||
| [111] | 2019 | Şahin et al. | Turkey | Retrospective | 46 | 44 | Pannexin-1 | S | Diagnostic |
| [112] | 2019 | Bassyouni et al. | Egypt | Retrospective | 87 | 60 | CCN2 | S | Diagnostic |
| [113] | 2019 | Arica et al. | Turkey | Retrospective | 45 (32 active) | 28 | Early EPCs | S | Diagnostic/Activity |
| Late EPCs | S | Diagnostic/Activity | |||||||
| MMP9 | S | Diagnostic | |||||||
| VEGF | S | Diagnostic/Activity | |||||||
| CRP | S | Diagnostic/Activity | |||||||
| ESR | S | Diagnostic | |||||||
| [114] | 2019 | Sandikci et al. | Turkey | Retrospective | 150 | 100 | Serumnativethiol | S | Diagnostic |
| Total thiol | S | Diagnostic | |||||||
| T-SH | S | Diagnostic | |||||||
| [115] | 2019 | Talaat et al. | Egypt | Retrospective | 64 | 20 | IL-6 | S | Diagnostic/Activity |
| IL-10 | S | Diagnostic | |||||||
| IL-17 | S | Diagnostic | |||||||
| [116] | 2019 | Gheita et al. | Egypt | Retrospective | 96 | 60 | NLR | S | Diagnostic |
| PLR | S | Diagnostic | |||||||
| RDW | S | Diagnostic | |||||||
| MPV | S | Diagnostic | |||||||
| VEGF | S | Diagnostic | |||||||
| [117] | 2019 | El Boghdady et al. | Egypt | Retrospective | 51 | 45 | TNF-α | S | Diagnostic |
| IL-6 | S | Diagnostic | |||||||
| E-selectine | S | Diagnostic | |||||||
| VCAM | S | Diagnostic | |||||||
| miR-181b | S | Diagnostic | |||||||
| [118] | 2019 | Balbaba et al. | Turkey | Retrospective | 48 (24 active) | 24 | Cortistatin | S | Diagnostic |
| [119] | 2020 | Hassan et al. | Egypt | Retrospective | 42 | 42 | Endocan | S | Diagnostic/Activity |
| [120] | 2020 | Hussain et al. | China | Retrospective | 50 | 100 | Moesin | S | Diagnostic |
| [121] | 2020 | Hussain et al. | China | Retrospective | 32 | 64 | NuMA Ab | S | Diagnostic |
| [122] | 2020 | Djaballah-Ider et al. | Algeria | Retrospective | 61 (47 active) | 25 | NLR | S | Activity |
| NO | S | Activity | |||||||
| IL-4 | S | Activity | |||||||
| IFN-gamma | S | Activity | |||||||
| [123] | 2021 | Cheng et al. | China | Retrospective | 48 (34 active) | 96 | Lymphocyte count | S | Diagnostic/Activity |
| White blood cell count | S | Diagnostic | |||||||
| Neutrophil count | S | Diagnostic | |||||||
| Basophil count | S | Diagnostic/Activity | |||||||
| RDW | S | Diagnostic/Activity | |||||||
| MCH | S | Diagnostic | |||||||
| MCHC | S | Diagnostic | |||||||
| Platelet count | S | Diagnostic/Activity | |||||||
| Plateletcount | S | Diagnostic/Activity | |||||||
| MPV | S | Diagnostic/Activity | |||||||
| CRS | S | Diagnostic | |||||||
| PLR | S | Diagnostic/Activity | |||||||
| NLR | S | Diagnostic | |||||||
| Monocyte | S | Activity | |||||||
| LMRcount | S | Diagnostic |
| ILs | IL-1β [14,94,102] | IL-2 [18,29] | IL-4 [122] | IL-6 [29,67,75,89,115,117] | IL-7 [67] | IL-8 [19,36,49,50,51,75] | IL-10 [106,115] | IL-15 [49] | IL-17 [106,115] | IL-18 [75,79] | IL-20 [99] | IL-23 [52,106] |
| IL-26 [96] | IL-32 [95] | IL-33 [67] | ||||||||||
| Cytokines | TNF-α [29,49,58,61,69,81,103,117] | TGF-β [106] | APRIL [69] | BAFF [69] | INF-α [75] | IFN-γ [122] | CTGF [112] | STAT3 [78] | CXCL11 [75] | |||
| Surface proteins | CD64 [33] | CXCR2 [35] | BMCA [69] | VCAM [117] | ||||||||
| Soluble proteins | SIL-2R [14,18] | PMN leukocyte elastase [15] | AECA [16] | vWF [16,74] | ET-1 [17,24] | Anti-ASCA Ab [22] | Leptin [23,89] | Homocysteine [24,43,73] | CRP [30,31,36,37,64,66,69,71,72,73,87,90,91,93,99,105,113,123] | cICAM-1 [23] | Catalase [28] | ADA [28,34,40] |
| SOD [28,102] | TBARS [28] | E-selectine [30,117] | MPO [31] | Neopterin [37,39] | VEGF [46,100,113,116] | Protein S [41] | antiHS [42] | Gal-3 [44,57] | G3BP [44] | MMP2 [45] | α-defensin1 [59] | |
| sTNFR1 e 2 [47,89,96] | E-Caderin [52] | Angiopoietin1 [54,77] | Resistin [58,81] | Thrombomodulin [55] | aTAFI [55] | AAEA [60,92,107] | sTREM1 [61,100] | STIP [62] | sCD40L [63,89] | MMP9 [63,113] | Lp-PLA2 [66] | |
| MTCH1 Ab [68] | Prohibitin [70] | Endocan [72,119] | ADMA [73,76] | Omentin [81] | HMBG1 [82] | Anti-lysozyme [88] | Fibrinogen [71] | Factor VIII [74] | cNuMA Ab [121] | anti-CTDP1 Ab [85] | SAA [94] | |
| sIL6-RB [96] | Chitinase3-like1 [83,96] | Bilirubin [98] | Calprotectin [97] | IMA [97] | IgD [101] | suPAR [105] | Pannexin-1 [111] | Cortistatin [118] | Moesin [120] | |||
| Cells | CD4+CD16+ [19,20] | CD4+CD56+ [19,20] | T γδ [21] | CEC [48] | CD34+KDR+EPCs [53,113] | CD34+CD133+KDR+ EPCs [53] | CD4+CD25+FOXP3+Treg [64] | CD4+FOXP3+Treg [64] | Treg [106] | Th17 [106] | CD56 + [109] | |
| miRNA | α-defensin 1 [59] | miR-155 [103,104,106] | miR-181b [117] | miR-93 [106] | miR-106b [106] | miR-25 [106] | miR-146a [106] | miR-326 [106] | ||||
| Metabolomic/ proteomic markers | DA, OA Fructose, tagatose [125] | LA [110,125] | PC [110] | AA [110] | Panel of six proteomic biomarkers [65] | |||||||
| Others | ESR [30,31,36,37,46,52,66,69,72,87,89,91,99,113] | NO [24,26,27,29,32,102,122] | Thiol [31,114] | AOPP [31,102] | Allantoin [38] | MDA [38,56,102] | Ascorbic acid [38] | 8-OhdG [56] | T-SH [56,114] | PLR [31,91,116] | LMR [91,123] | NLR [31,76,80,84,87,116,122] |
| AIP [90] | RDW [71] | ETP [74] | MPV [123] | RDW [71,123] | Procoagulant MP [86] | MHR [108] | ||||||
| Urinary markers | Metabolomic panel: Guanine Pyrrole-2-carboxylate 3-hydroxypyroline Mannose L-citrulline Galactonate Isothreonate Sedoheptulose Hypoxanthine Gluconic acidlactonate [93] | NO [14] | ||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arbrile, M.; Radin, M.; Medica, D.; Miraglia, P.; Rilat, L.; Cecchi, I.; Foddai, S.G.; Barinotti, A.; Menegatti, E.; Roccatello, D.; et al. Finding the Needle in the Haystack: Serological and Urinary Biomarkers in Behçet’s Disease: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 3041. https://doi.org/10.3390/ijms24033041
Arbrile M, Radin M, Medica D, Miraglia P, Rilat L, Cecchi I, Foddai SG, Barinotti A, Menegatti E, Roccatello D, et al. Finding the Needle in the Haystack: Serological and Urinary Biomarkers in Behçet’s Disease: A Systematic Review. International Journal of Molecular Sciences. 2023; 24(3):3041. https://doi.org/10.3390/ijms24033041
Chicago/Turabian StyleArbrile, Marta, Massimo Radin, Davide Medica, Paolo Miraglia, Letizia Rilat, Irene Cecchi, Silvia Grazietta Foddai, Alice Barinotti, Elisa Menegatti, Dario Roccatello, and et al. 2023. "Finding the Needle in the Haystack: Serological and Urinary Biomarkers in Behçet’s Disease: A Systematic Review" International Journal of Molecular Sciences 24, no. 3: 3041. https://doi.org/10.3390/ijms24033041
APA StyleArbrile, M., Radin, M., Medica, D., Miraglia, P., Rilat, L., Cecchi, I., Foddai, S. G., Barinotti, A., Menegatti, E., Roccatello, D., & Sciascia, S. (2023). Finding the Needle in the Haystack: Serological and Urinary Biomarkers in Behçet’s Disease: A Systematic Review. International Journal of Molecular Sciences, 24(3), 3041. https://doi.org/10.3390/ijms24033041