
The Glycoprotein (GP)Ib-IX-V Complex on Platelets: GPIbα Protein Expression Is Reduced in HeartMate 3 Patients with Bleeding Complications within the First 3 Months
 ,
,
Abstract
:1. Introduction
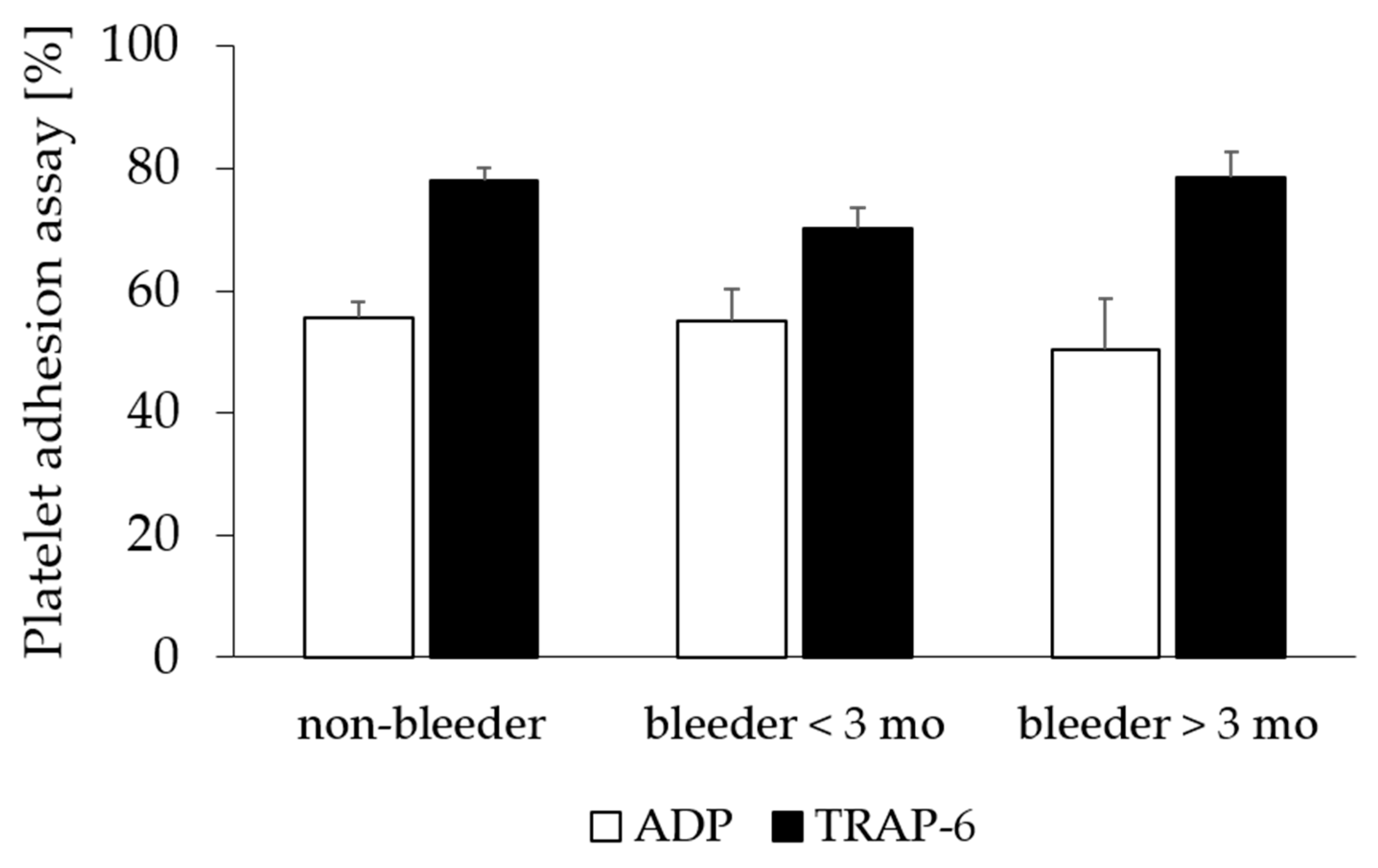
2. Results
2.1. Patient Characteristics
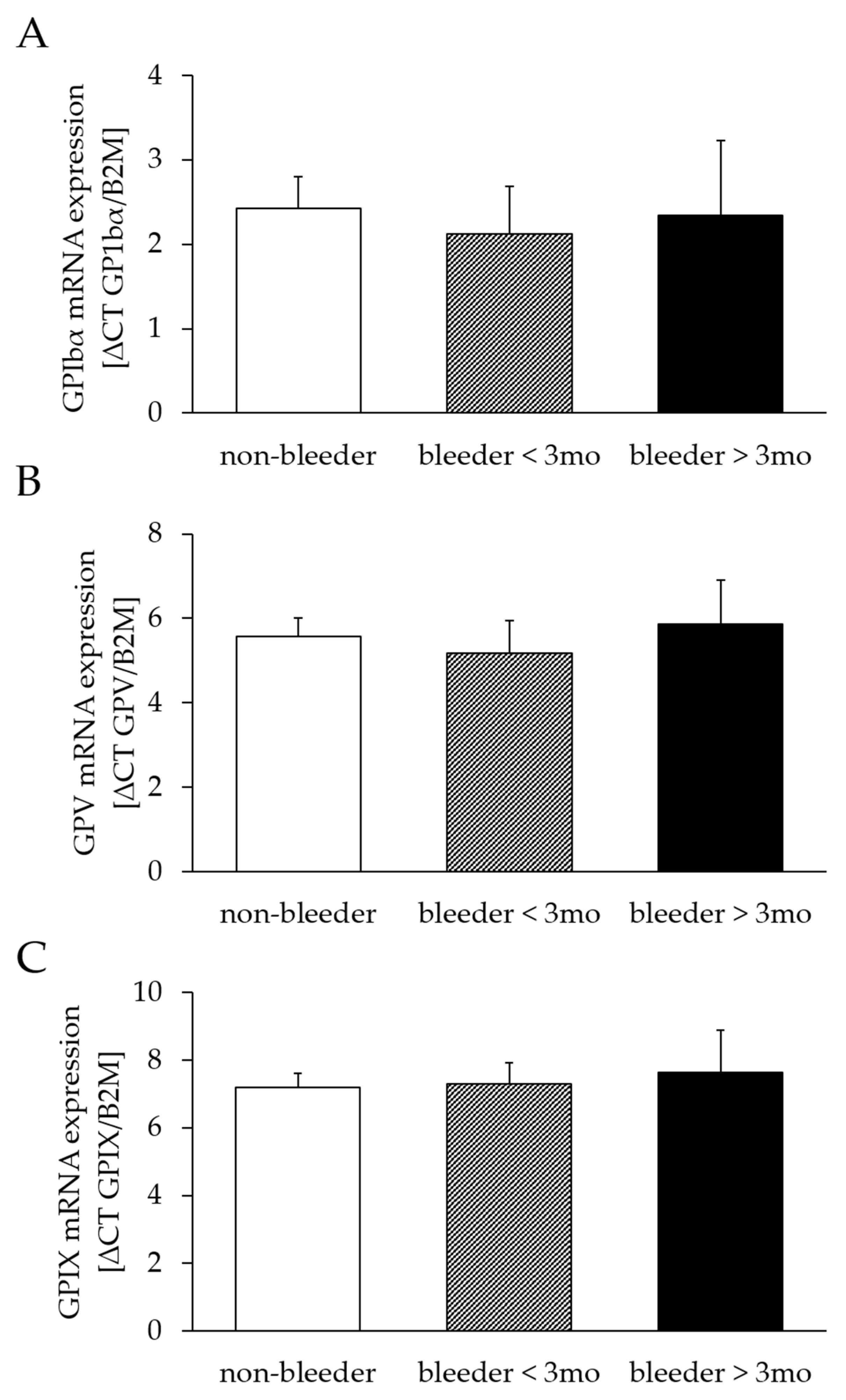
2.2. Analysis of Platelet Receptor mRNA Expression
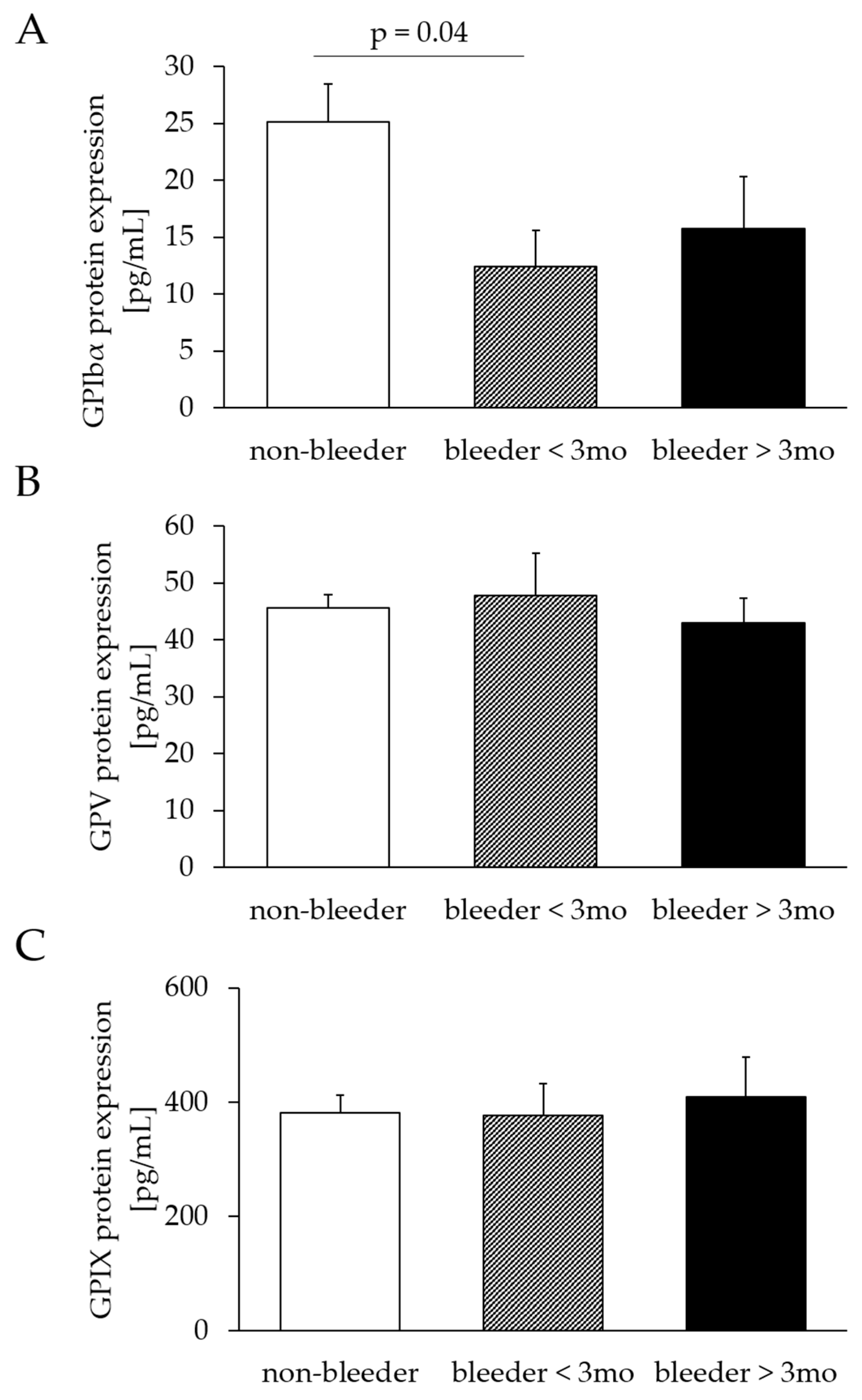
2.3. Analysis of Platelet Receptor Protein Expression
2.4. Assessment of Serum Levels of GPIbα
3. Discussion
4. Materials and Methods
4.1. Study Groups and Clinical Characteristics
4.2. Sample Collection
4.3. RNA Extraction and cDNA Synthesis
4.4. Real-Time Quantitative PCR Analysis
4.5. Protein Extraction and Quantification
4.6. Elisa
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kapuria, D.; Khumri, T.; Shamim, S.; Surana, P.; Khan, S.; Al-Khalisi, N.; Aggarwal, S.; Koh, C.; Chhabra, R. Characterization and timing of gastrointestinal bleeding in continuous flow left ventricular assist device recipients. Heliyon 2020, 6, e04695. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Mondal, N.K.; Sorensen, E.N.; Cai, L.; Fang, H.B.; Griffith, B.P.; Wu, Z.J. Platelet glycoprotein Ibα ectodomain shedding and non-surgical bleeding in heart failure patients supported by continuous-flow left ventricular assist devices. J. Heart Lung. Transplant. 2014, 33, 71–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koliopoulou, A.; McKellar, S.H.; Rondina, M.; Selzman, C.H. Bleeding and thrombosis in chronic VAD therapy: Focus on platelets. Curr. Opin. Cardiol. 2016, 31, 299–307. [Google Scholar] [CrossRef] [Green Version]
- Mehra, M.R.; Goldstein, D.J.; Cleveland, J.C.; Cowger, J.A.; Hall, S.; Salerno, C.T.; Naka, Y.; Horstmanshof, D.; Chuang, J.; Wang, A.; et al. Five-Year Outcomes in Patients with Fully Magnetically Levitated vs. Axial-Flow Left Ventricular Assist Devices in the MOMENTUM 3 Randomized Trial. JAMA 2022, 328, 1233–1242. [Google Scholar] [CrossRef]
- Hanke, J.S.; Dogan, G.; Zoch, A.; Ricklefs, M.; Wert, L.; Feldmann, C.; Bara, C.; Shrestha, M.; Tillmanns, J.; Kempf, T.; et al. One-year outcomes with the HeartMate 3 left ventricular assist device. J. Thorac. Cardiovasc. Surg. 2018, 156, 662–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mondal, N.K.; Chen, Z.; Trivedi, J.R.; Sorensen, E.N.; Pham, S.M.; Slaughter, M.S.; Griffith, B.P.; Wu, Z.J. Association of Oxidative Stress and Platelet Receptor Glycoprotein GPIbα and GPVI Shedding during Nonsurgical Bleeding in Heart Failure Patients with Continuous-Flow Left Ventricular Assist Device Support. ASAIO J. 2018, 64, 462–471. [Google Scholar] [CrossRef]
- Li, R.; Emsley, J. The organizing principle of the platelet glycoprotein Ib-IX-V complex. J. Thromb. Haemost. 2013, 11, 605–614. [Google Scholar] [CrossRef] [Green Version]
- Gardiner, E.E.; Arthur, J.F.; Shen, Y.; Karunakaran, D.; Moore, L.A.; Am Esch, J.S., 2nd; Andrews, R.K.; Berndt, M.C. GPIbalpha-selective activation of platelets induces platelet signaling events comparable to GPVI activation events. Platelets 2010, 21, 244–252. [Google Scholar] [CrossRef]
- Gardiner, E.E.; Al-Tamimi, M.; Andrews, R.K.; Berndt, M.C. Platelet receptor shedding. Methods Mol. Biol. 2012, 788, 321–339. [Google Scholar]
- Chen, Z.; Mondal, N.K.; Ding, J.; Gao, J.; Griffith, B.P.; Wu, Z.J. Shear-induced platelet receptor shedding by non-physiological high shear stress with short exposure time: Glycoprotein Ibα and glycoprotein VI. Thromb. Res. 2015, 135, 692–698. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Mondal, N.K.; Ding, J.; Koenig, S.C.; Slaughter, M.S.; Griffith, B.P.; Wu, Z.J. Activation and shedding of platelet glycoprotein IIb/IIIa under non-physiological shear stress. Mol. Cell Biochem. 2015, 409, 93–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Mondal, N.K.; Ding, J.; Koenig, S.C.; Slaughter, M.S.; Wu, Z.J. Paradoxical Effect of Nonphysiological Shear Stress on Platelets and von Willebrand Factor. Artif. Organs 2016, 40, 659–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Zhang, J.; Kareem, K.; Tran, D.; Conway, R.G.; Arias, K.; Griffith, B.P.; Wu, Z.J. Device-induced platelet dysfunction in mechanically assisted circulation increases the risks of thrombosis and bleeding. Artif. Organs 2019, 43, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Lukito, P.; Wong, A.; Jing, J.; Arthur, J.F.; Marasco, S.F.; Murphy, D.A.; Bergin, P.J.; Shaw, J.A.; Collecutt, M.; Andrews, R.K.; et al. Mechanical circulatory support is associated with loss of platelet receptors glycoprotein Ibα and glycoprotein, V.I. J. Thromb. Haemost. 2016, 14, 2253–2260. [Google Scholar] [CrossRef]
- Roka-Moiia, Y.; Miller-Gutierrez, S.; Palomares, D.E.; Italiano, J.E.; Sheriff, J.; Bluestein, D.; Slepian, M.J. Platelet Dysfunction During Mechanical Circulatory Support: Elevated Shear Stress Promotes Downregulation of αIIbβ3 and GPIb via Microparticle Shedding Decreasing Platelet Aggregability. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 1319–1336. [Google Scholar] [CrossRef]
- Klaeske, K.; Dieterlen, M.T.; Eifert, S.; Scholz, U.; Garbade, J.; Jawad, K.; Sieg, F.; Borger, M.A.; Meyer, A.L. Device-induced platelet dysfunction in patients after left ventricular assist device implantation. J. Thromb. Haemost. 2021, 19, 1331–1341. [Google Scholar] [CrossRef]
- Arias, K.; Sun, W.; Wang, S.; Sorensen, E.N.; Feller, E.; Kaczorowski, D.; Griffith, B.; Wu, Z.J. Acquired platelet defects are responsible for nonsurgical bleeding in left ventricular assist device recipients. Artif. Organs 2022, 46, 2244–2256. [Google Scholar] [CrossRef]
- Leebeek, F.W.G.; Muslem, R. Bleeding in critical care associated with left ventricular assist devices: Pathophysiology, symptoms, and management. Hematol. Am. Soc. Hematol. Educ. Program. 2019, 1, 88–96. [Google Scholar] [CrossRef]
- Sun, S.; Qiao, B.; Han, Y.; Wang, B.; Wei, S.; Chen, Y. Posttranslational modifications of platelet adhesion receptors. Pharmacol. Res. 2022, 183, 106413. [Google Scholar] [CrossRef]
- Schubert, P.; Devine, D.V. De novo protein synthesis in mature platelets: A consideration for transfusion medicine. Vox Sang. 2010, 99, 112–122. [Google Scholar] [CrossRef]
- Bendas, G.; Schlesinger, M. The GPIb-IX complex on platelets: Insight into its novel physiological functions affecting immune surveillance, hepatic thrombopoietin generation, platelet clearance and its relevance for cancer development and metastasis. Exp. Hematol. Oncol. 2022, 11, 19. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Griffith, B.P.; Wu, Z.J. Device-Induced Hemostatic Disorders in Mechanically Assisted Circulation. Clin. Appl. Thromb. Hemost. 2021, 27, 1076029620982374. [Google Scholar] [CrossRef]
- Huizinga, E.G.; Tsuji, S.; Romijn, R.A.; Schiphorst, M.E.; de Groot, P.G.; Sixma, J.J.; Gros, P. Structures of glycoprotein Ibalpha and its complex with von Willebrand factor A1 domain. Science 2002, 297, 1176–1179. [Google Scholar] [CrossRef] [PubMed]
- Bergmeier, W.; Piffath, C.L.; Cheng, G.; Dole, V.S.; Zhang, Y.; von Andrian, U.H.; Wagner, D.D. Tumor necrosis factor-alpha-converting enzyme (ADAM17) mediates GPIbalpha shedding from platelets in vitro and in vivo. Circ. Res. 2004, 95, 677–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardiner, E.E.; Karunakaran, D.; Shen, Y.; Arthur, J.F.; Andrews, R.K.; Berndt, M.C. Controlled shedding of platelet glycoprotein (GP)VI and GPIb-IX-V by ADAM family metalloproteinases. J. Thromb. Haemost. 2007, 5, 1530–1537. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Yan, R.; Li, S.; Yuan, Y.; Liu, J.; Ruan, C.; Dai, K. Shear-induced interaction of platelets with von Willebrand factor results in glycoprotein Ibalpha shedding. Am. J. Physiol. Heart Circ. Physiol. 2009, 297, H2128–H2135. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Tran, D.; Li, T.; Arias, K.; Griffith, B.P.; Wu, Z.J. The role of a disintegrin and metalloproteinase proteolysis and mechanical damage in nonphysiological shear stress-induced platelet receptor shedding. ASAIO J. 2020, 66, 524–531. [Google Scholar] [CrossRef]
- Andrews, R.K.; Karunakaran, D.; Gardiner, E.E.; Berndt, M.C. Platelet receptor proteolysis: A mechanism for downregulating platelet reactivity. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 1511–1520. [Google Scholar] [CrossRef]
- Zhalbinova, M.R.; Rakhimova, S.E.; Kozhamkulov, U.A.; Akilzhanova, G.A.; Kaussova, G.K.; Akilzhanov, K.R.; Pya, Y.V.; Lee, J.H.; Bekbossynova, M.S.; Akilzhanova, A.R. Association of Genetic Polymorphisms with Complications of Implanted LVAD Devices in Patients with Congestive Heart Failure: A Kazakhstani Study. J. Pers. Med. 2022, 12, 744. [Google Scholar] [CrossRef]
- Potapov, E.V.; Ignatenko, S.; Nasseri, B.A.; Loebe, M.; Harke, C.; Bettmann, M.; Doller, A.; Regitz-Zagrosek, V.; Hetzer, R. Clinical significance of PlA polymorphism of platelet GP IIb/IIIa receptors during long-term VAD support. Ann. Thorac. Surg. 2004, 77, 869–874, discussion 874. [Google Scholar] [CrossRef]
- Leytin, V.; Allen, D.J.; Mykhaylov, S.; Mis, L.; Lyubimov, E.V.; Garvey, B.; Freedman, J. Pathologic high shear stress induces apoptosis events in human platelets. Biochem. Biophys. Res. Commun. 2004, 320, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Mondal, N.K.; Li, T.; Chen, Z.; Chen, H.H.; Sorensen, E.N.; Pham, S.M.; Sobieski, M.A.; Koenig, S.C.; Slaughter, M.S.; Griffith, B.P.; et al. Mechanistic insight of platelet apoptosis leading to non-surgical bleeding among heart failure patients supported by continuous-flow left ventricular assist devices. Mol. Cell Biochem. 2017, 433, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Schuhmann, M.K.; Guthmann, J.; Stoll, G.; Nieswandt, B.; Kraft, P.; Kleinschnitz, C. Blocking of platelet glycoprotein receptor Ib reduces “thrombo-inflammation” in mice with acute ischemic stroke. J. Neuroinflamm. 2017, 14, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stapor, M.; Pilat, A.; Gackowski, A.; Misiuda, A.; Gorkiewicz-Kot, I.; Kaleta, M.; Kleczynski, P.; Zmudka, K.; Legutko, J.; Kapelak, B.; et al. Echo-guided left ventricular assist device speed optimisation for exercise maximization. Heart 2022, 108, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Nascimbene, A.; Neelamegham, S.; Frazier, O.H.; Moake, J.L.; Dong, J.F. Acquired von Willebrand syndrome associated with left ventricular assist device. Blood 2016, 127, 3133–3142. [Google Scholar] [CrossRef] [Green Version]
- Hennessy-Strahs, S.; Kang, J.; Krause, E.; Dowling, R.D.; Rame, J.E.; Bartoli, C.R. Patient-specific severity of von Willebrand factor degradation identifies patients with a left ventricular assist device at high risk for bleeding. J. Thorac. Cardiovasc. Surg. 2022; in press. [Google Scholar] [CrossRef]
- Beverborg, N.G.; van Veldhuisen, D.J.; van der Meer, P. Anemia in Heart Failure: Still Relevant? JACC Heart Fail. 2018, 6, 201–208. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Bleeders (n = 27) | Non-Bleeders (n = 55) | p-Value |
|---|---|---|---|
| age at LVAD implantation [y] | 60.9 ± 9.9 | 59.2 ± 9.5 | 0.46 |
| male gender | 22 (82%) | 48 (87%) | 0.52 |
| body mass index [kg/m2] | 28.3 ± 5.5 | 28.6 ± 5.5 | 0.86 |
| blood type * | 0.81 | ||
| A | 11 (41%) | 28 (52%) | |
| B | 4 (15%) | 5 (9%) | |
| AB | 1 (4%) | 2 (4%) | |
| 0 | 11 (41%) | 19 (35%) | |
| etiology of heart disease | 0.35 | ||
| NICM | 12 (44%) | 32 (58%) | |
| ICM | 15 (56%) | 23 (42%) | |
| alcohol abusus | 0.62 | ||
| current | 5 (19%) | 6 (11%) | |
| former | 14 (52%) | 25 (45%) | |
| occasional | 5 (19%) | 13 (24%) | |
| unknown | 3 (11%) | 11 (20%) | |
| smoking | 0.61 | ||
| current | 3 (11%) | 10 (18%) | |
| former | 16 (59%) | 29 (53%) | |
| never | 3 (11%) | 9 (16%) | |
| unknown | 5 (19%) | 7 (13%) | |
| pump characteristics | |||
| pump speed [rpm] | 5141 ± 571 | 5271 ± 2665 | 0.16 |
| pump flow [L/min] | 4.2 ± 0.6 | 4.3 ± 0.7 | 0.27 |
| pump power [W] | 3.9 ± 0.5 | 4.0 ± 0.4 | 0.45 |
| pulse index | 4.5 ± 2.0 | 4.4 ± 1.6 | 0.82 |
| anticoagulation at study begin | |||
| Phenprocoumon/warfarin | 27 (100%) | 55 (100%) | 1.00 |
| clopidogrel | 7 (26%) | 11 (20%) | 0.58 |
| acetylsalicylic acid | 16 (59%) | 45 (82%) | 0.04 |
| prasugrel | 1 (4%) | 0 (0%) | 0.33 |
| Parameter | Bleeders (n = 27) | Non-Bleeders (n = 55) | p-Value |
|---|---|---|---|
| thromboembolic event prior LVAD implantation | |||
| ischemic stroke | 3 (%) | 9 (%) | 0.74 |
| pulmonary embolism | 1 (%) | 1 (%) | 1.00 |
| venous thrombosis | 2 (%) | 5 (%) | 1.00 |
| ventricle thrombosis | 3 (%) | 14 (%) | 0.16 |
| myocardial infarction | 7 (%) | 15 (%) | 1.00 |
| hemorrhagic events after LVAD implantation * | |||
| gastrointestinal tract bleeding | 12 (44%) | - | |
| vascular (epistaxis) | 7 (26%) | - | |
| haemothorax | 4 (15%) | - | - |
| dermal bleeding (haematoma) | 3 (11%) | - | |
| intracranial bleeding | 2 (7%) | - | |
| other | 4 (15%) | - | |
| thromboembolic event after LVAD implantation | |||
| ischemic stroke | 0 (0%) | 3 (6%) | 1.00 |
| pAVK | 2 (7%) | 3 (6%) | 1.00 |
| pump thrombosis | 0 (0%) | 1 (2%) | 1.00 |
| rethoracothomy after LVAD implantation | 13 (48%) | 29 (53%) | 0.82 |
| Parameter | Bleeders (n = 27) | Non-Bleeders (n = 55) | p-Value |
|---|---|---|---|
| erythrocytes [Tpt/L] | 3.8 ± 0.8 | 4.4 ± 0.8 | <0.01 |
| hematocrit | 0.3 ± 0.1 | 0.4 ± 0.1 | <0.01 |
| hemoglobin [mmol/L] | 7.2 ± 1.3 | 8.3 ± 1.5 | <0.01 |
| platelets [×109/L] at study begin | 211 ± 82 | 221 ± 67 | 0.55 |
| platelets [×109/L] at bleeding event | 234 ± 115 | - | - |
| leucocytes [Gpt/L] | 7.7 ± 2.3 | 7.8 ± 1.9 | 0.83 |
| INR | 2.1 ± 0.5 | 2.2 ± 0.4 | 0.10 |
| CRP [mg/L] | 12.4 ± 16.4 | 8.2 ± 10.3 | 0.23 |
| LDH [µmol/(L/s)] | 3.9 ± 1.0 | 4.2 ± 0.8 | 0.28 |
| Parameter | Bleeders (n = 27) | Non-Bleeders (n = 55) | p-Value |
|---|---|---|---|
| Platelet adhesion assay [%] | |||
| ADP | 54 ± 24 | 56 ± 20 | 0.70 |
| TRAP-6 | 73 ± 15 | 78 ± 15 | 0.13 |
| VASP-phosphorylation | 70 ± 22 | 77 ± 18 | 0.12 |
| aPTT [s] | 44.2 ± 7.4 | 42.6 ± 6.4 | 0.32 |
| vWF antigen [%] | 198.6 ± 65.5 | 176.1 ± 61.0 | 0.26 |
| vWF activity [%] | 136.7 ± 28.7 | 128.5 ± 34.1 | 0.43 |
| vWF CB activity [%] | 135.5 ± 41.9 | 116.1 ± 37.3 | 0.22 |
| factor VIII, procoagulant [%] | 188.5 ± 62.4 | 171.0 ± 57.5 | 0.36 |
| Target | Forward Primer 5′-3′ | Reverse Primer 5′-3′ |
|---|---|---|
| GPIbα | TGCCAGATCTCACGGTGAAC | AACGAGTGCTCACATCCTGAT |
| GPV | CCACTTGCTTTACATCCATGCA | GGAAGAACAAATGAGACTGTGACA |
| GPIX | AACAACAGCCTTCAGTCCGT | CAGAGGCGCAGATAGGTGAG |
| B2M | AGTATGCCTGCCGTGTGAAC | GCAAGCAAGCAGAATTTGGA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klaeske, K.; Brade, A.; Eifert, S.; Jawad, K.; Saeed, D.; Haunschild, J.; Sieg, F.; Borger, M.A.; Dieterlen, M.-T. The Glycoprotein (GP)Ib-IX-V Complex on Platelets: GPIbα Protein Expression Is Reduced in HeartMate 3 Patients with Bleeding Complications within the First 3 Months. Int. J. Mol. Sci. 2023, 24, 5639. https://doi.org/10.3390/ijms24065639
Klaeske K, Brade A, Eifert S, Jawad K, Saeed D, Haunschild J, Sieg F, Borger MA, Dieterlen M-T. The Glycoprotein (GP)Ib-IX-V Complex on Platelets: GPIbα Protein Expression Is Reduced in HeartMate 3 Patients with Bleeding Complications within the First 3 Months. International Journal of Molecular Sciences. 2023; 24(6):5639. https://doi.org/10.3390/ijms24065639
Chicago/Turabian StyleKlaeske, Kristin, Anneke Brade, Sandra Eifert, Khalil Jawad, Diyar Saeed, Josephina Haunschild, Franz Sieg, Michael A. Borger, and Maja-Theresa Dieterlen. 2023. "The Glycoprotein (GP)Ib-IX-V Complex on Platelets: GPIbα Protein Expression Is Reduced in HeartMate 3 Patients with Bleeding Complications within the First 3 Months" International Journal of Molecular Sciences 24, no. 6: 5639. https://doi.org/10.3390/ijms24065639
APA StyleKlaeske, K., Brade, A., Eifert, S., Jawad, K., Saeed, D., Haunschild, J., Sieg, F., Borger, M. A., & Dieterlen, M. -T. (2023). The Glycoprotein (GP)Ib-IX-V Complex on Platelets: GPIbα Protein Expression Is Reduced in HeartMate 3 Patients with Bleeding Complications within the First 3 Months. International Journal of Molecular Sciences, 24(6), 5639. https://doi.org/10.3390/ijms24065639