
Evaluation of Matrix Metalloproteases by Artificial Intelligence Techniques in Negative Biopsies as New Diagnostic Strategy in Prostate Cancer

 , , and
, , and
Abstract
:1. Introduction
2. Results
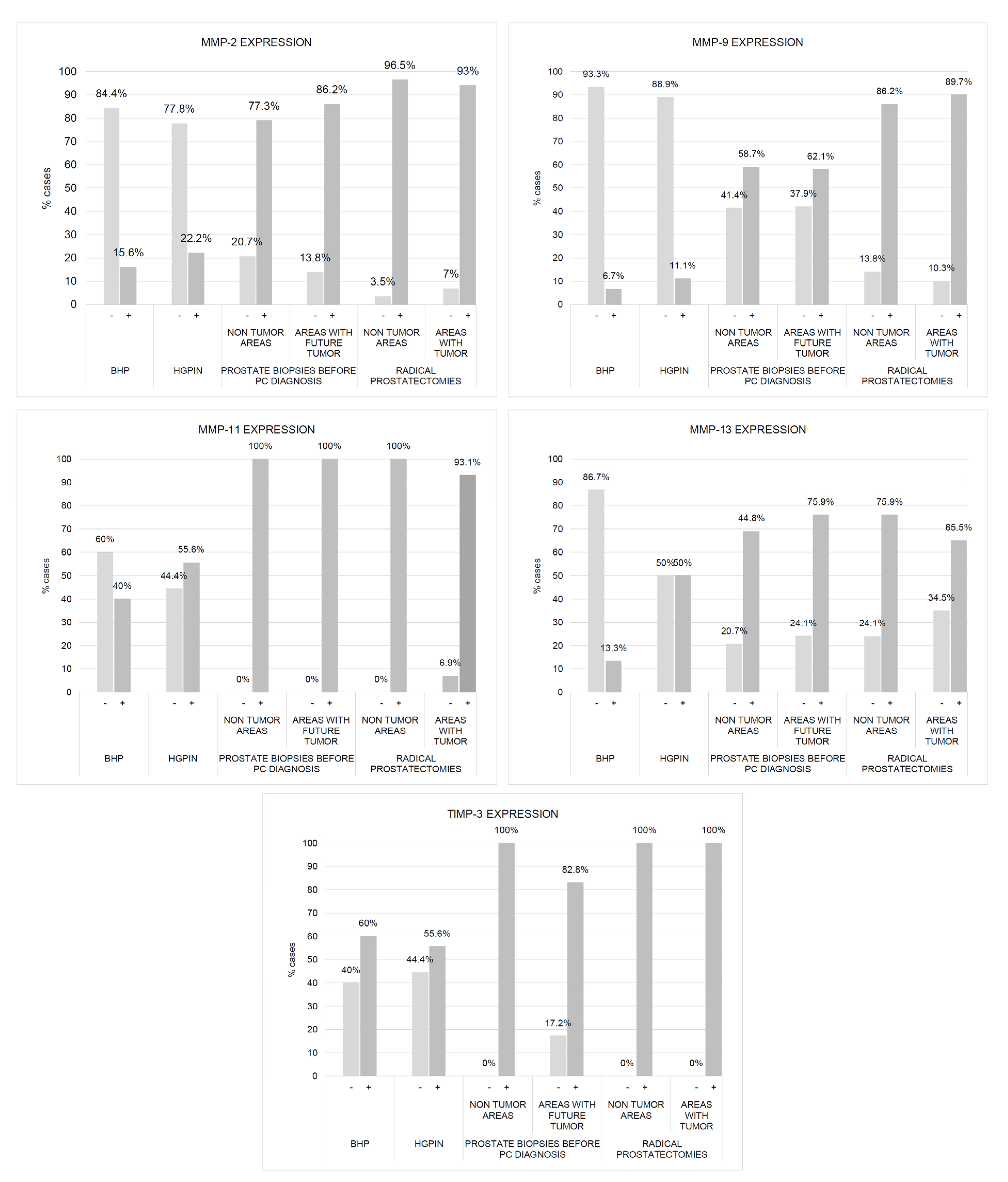
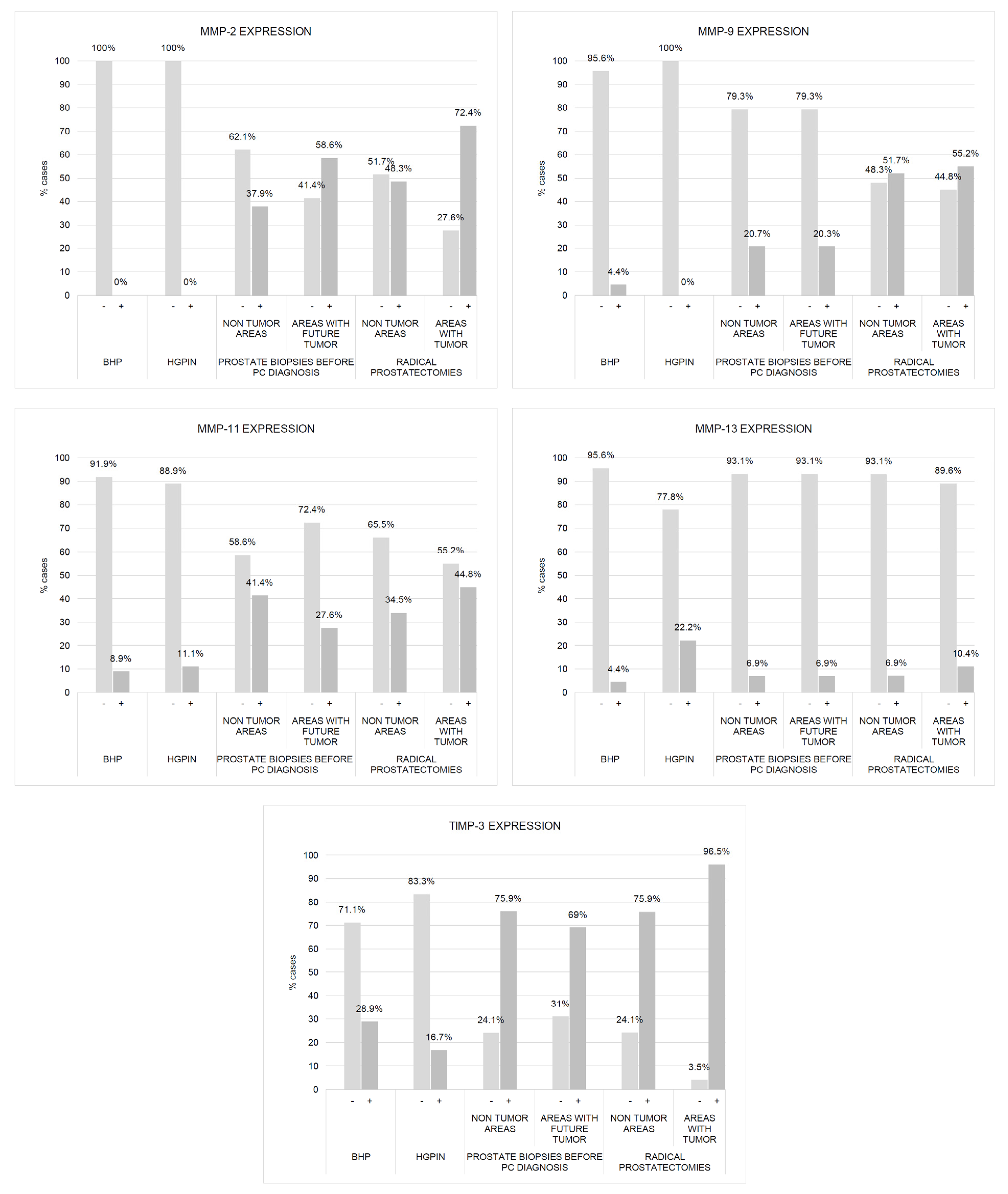
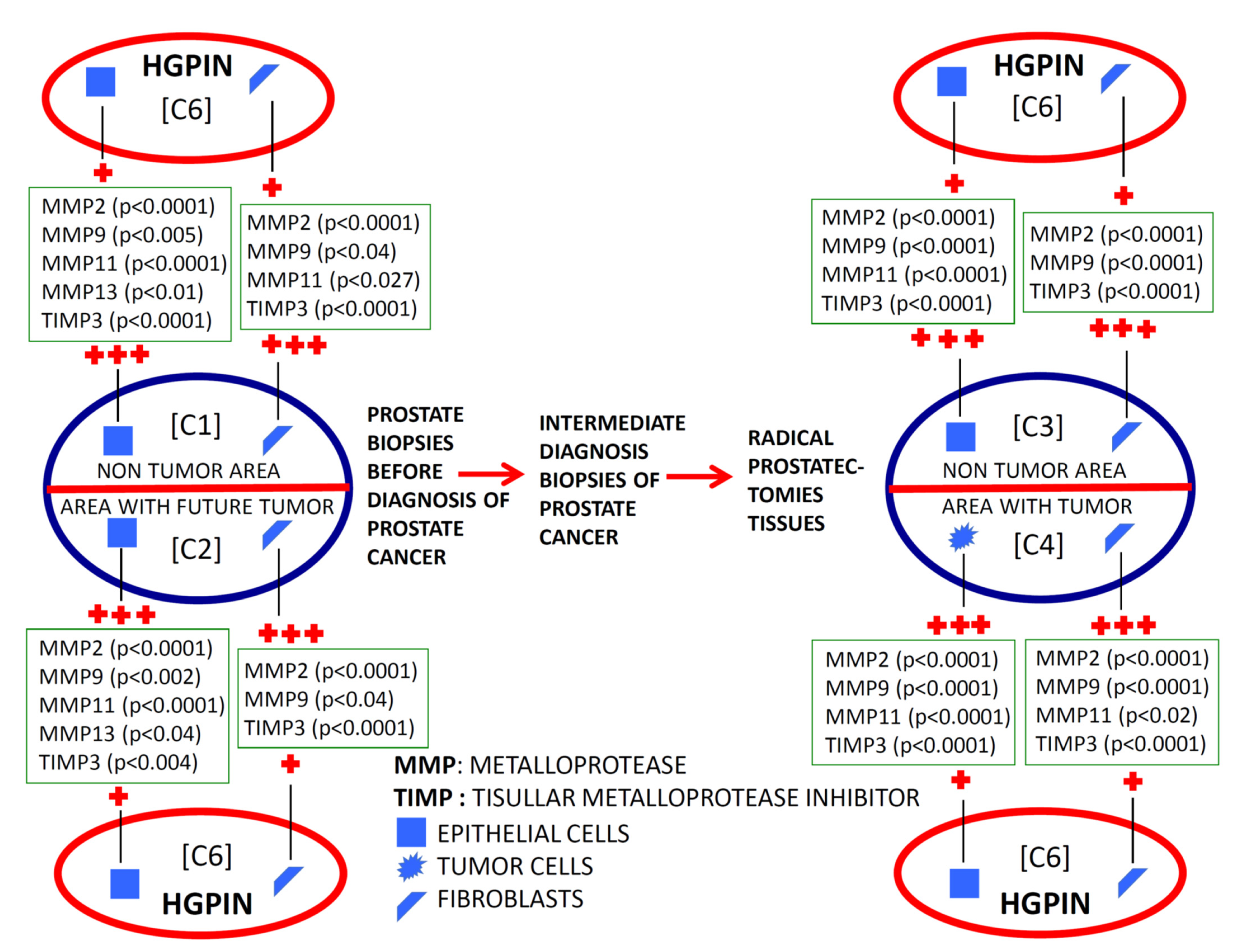
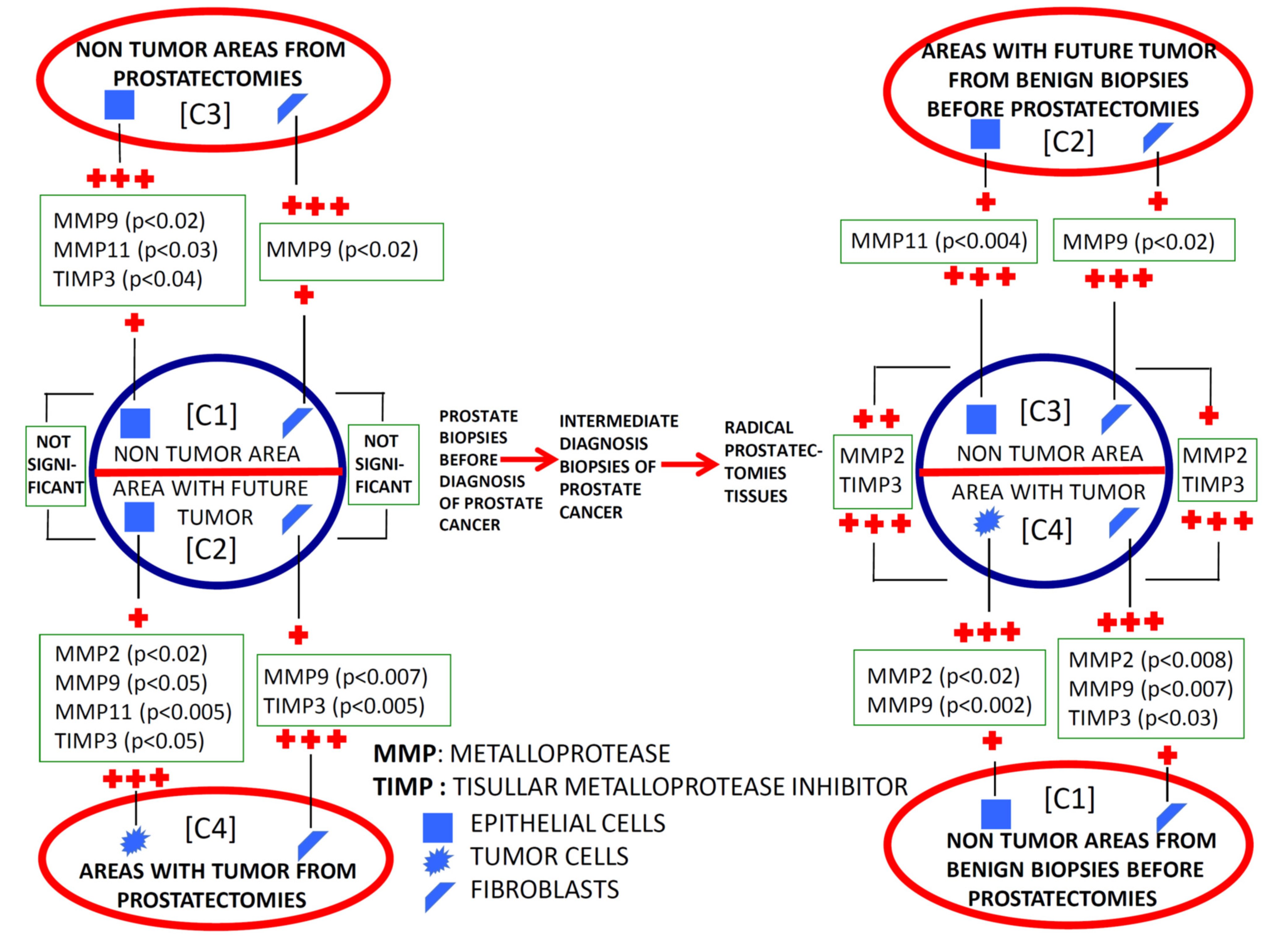
2.1. Comparative Study of the Expression of Factors among Different Benign Tissues Accuracy
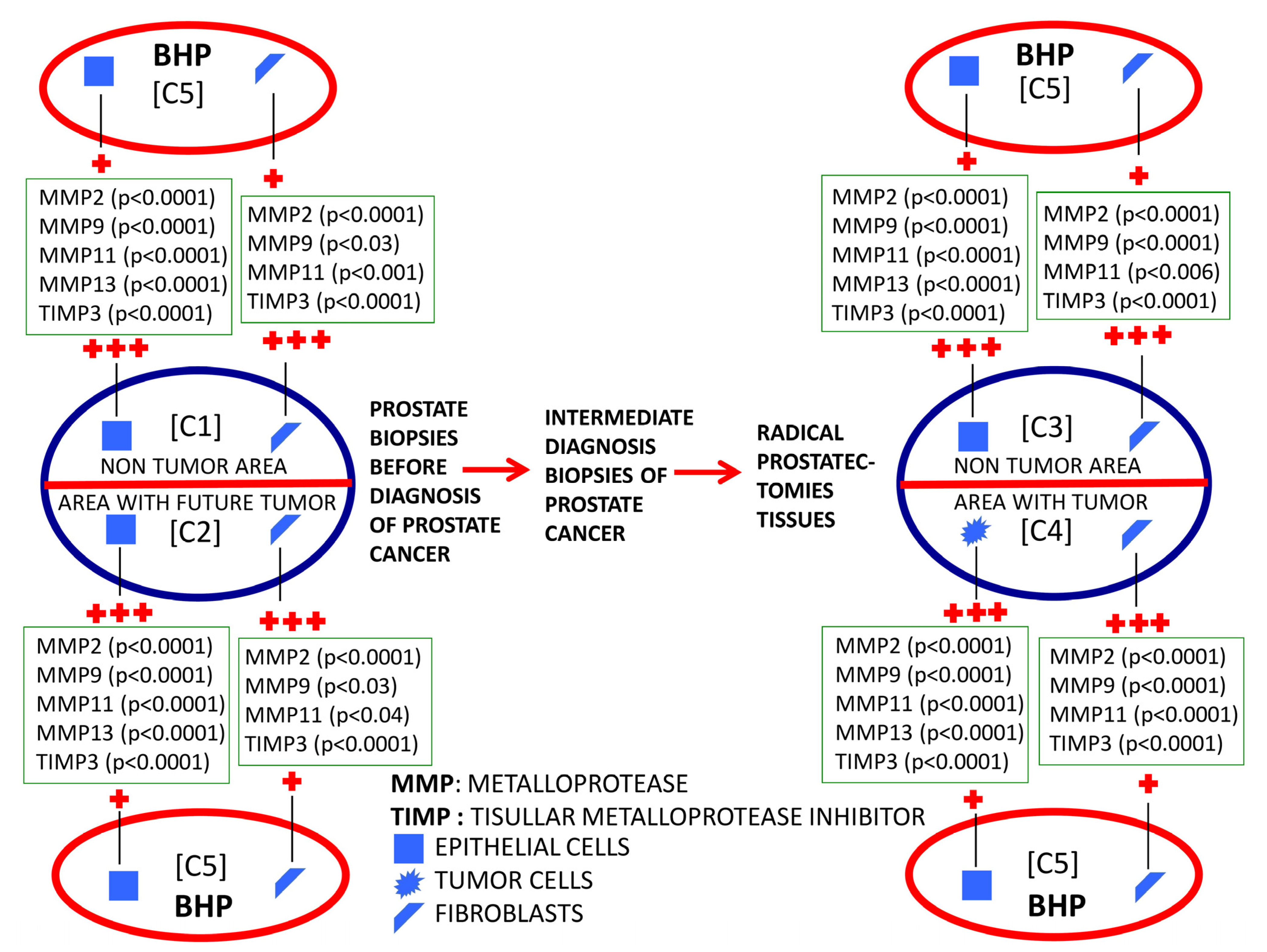
2.2. Evolutionary Changes in Paired Prostate Tissues from Benign Tissues to Cancer Diagnosis
3. Discussion
4. Materials and Methods
4.1. Patients
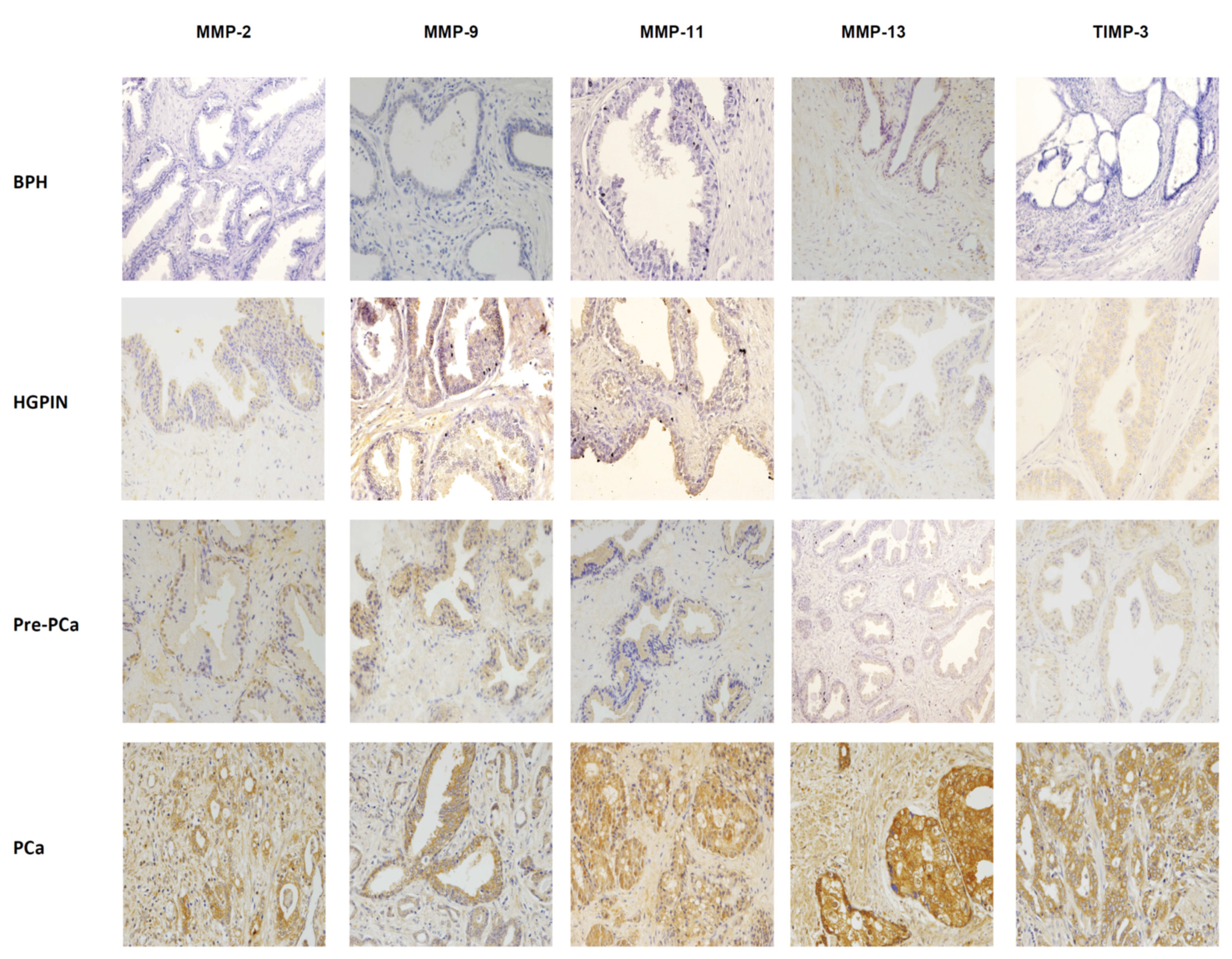
4.2. Immunohistochemical Analysis
4.3. Description of Data Sets
- (a)
- Training dataset: the data were used to train the algorithm to obtain the relevant and coherent knowledge and information capable of discriminating the input breaking down data (MMP-2, -9, -11, -13, and TIMP-3 expression);
- (b)
- Test dataset: the data were used to determine whether the behavior and knowledge provided by the intelligent system are adequate, through the corresponding evaluation by the degree of success or accuracy, and thus verify the effectiveness of the said algorithm.
4.4. Data Analysis and Intelligent Algorithms: Description and Evaluation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Ramos, M.; Escolar Pujolar, A. The mortality of prostate cancer in Andalusia. Contributions to mass screening. Actas Urol. Esp. 2005, 29, 41–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barry, M.J. Screening for prostate cancer—The controversy that refuses to die. N. Engl. J. Med. 2009, 360, 1351–1354. [Google Scholar] [CrossRef] [PubMed]
- Kvale, R.; Moller, B.; Wahlqvist, R.; Fossa, S.D.; Berner, A.; Busch, C.; Kyrdalen, A.E.; Svindland, A.; Viset, T.; Halvorsen, O.J. Concordance between Gleason scores of needle biopsies and radical prostatectomy specimens: A population-based study. BJU Int. 2009, 103, 1647–1654. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Escrig, J.L.; McCracken, S.R.; Greene, D. Beyond diagnosis: Evolving prostate biopsy in the era of focal therapy. Prostate Cancer 2011, 2011, 386207. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.M.; Rais-Bahrami, S.; Truong, H.; Stamatakis, L.; Vourganti, S.; Nix, J.; Hoang, A.N.; Walton-Diaz, A.; Shuch, B.; Weintraub, M.; et al. Magnetic resonance imaging/ultrasound-fusion biopsy significantly upgrades prostate cancer versus systematic 12-core transrectal ultrasound biopsy. Eur. Urol. 2013, 64, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Keetch, D.W.; Catalona, W.J.; Smith, D.S. Serial prostatic biopsies in men with persistently elevated serum prostate specific antigen values. J. Urol. 1994, 151, 1571–1574. [Google Scholar] [CrossRef]
- van de Ven, W.J.; Barentsz, J.O. Prostate cancer: MRI/US-guided biopsy—A viable alternative to TRUS-guidance. Nat. Rev. Urol. 2013, 10, 559–560. [Google Scholar] [CrossRef]
- Klein, E.A. Prostate cancer: MR-TRUS fusion biopsy—Defining a new standard. Nat. Rev. Clin. Oncol. 2015, 12, 253–254. [Google Scholar] [CrossRef]
- Nassiri, N.; Natarajan, S.; Margolis, D.J.; Marks, L.S. Targeted Prostate Biopsy: Lessons Learned Midst the Evolution of a Disruptive Technology. Urology 2015, 86, 432–438. [Google Scholar] [CrossRef] [Green Version]
- Mendhiratta, N.; Rosenkrantz, A.B.; Meng, X.; Wysock, J.S.; Fenstermaker, M.; Huang, R.; Deng, F.M.; Melamed, J.; Zhou, M.; Huang, W.C.; et al. Magnetic Resonance Imaging-Ultrasound Fusion Targeted Prostate Biopsy in a Consecutive Cohort of Men with No Previous Biopsy: Reduction of over Detection through Improved Risk Stratification. J. Urol. 2015, 194, 1601–1606. [Google Scholar] [CrossRef] [PubMed]
- Hoeks, C.M.; Schouten, M.G.; Bomers, J.G.; Hoogendoorn, S.P.; Hulsbergen-van de Kaa, C.A.; Hambrock, T.; Vergunst, H.; Sedelaar, J.P.; Futterer, J.J.; Barentsz, J.O. Three-Tesla magnetic resonance-guided prostate biopsy in men with increased prostate-specific antigen and repeated, negative, random, systematic, transrectal ultrasound biopsies: Detection of clinically significant prostate cancers. Eur. Urol. 2012, 62, 902–909. [Google Scholar] [CrossRef]
- Nelson, A.R.; Fingleton, B.; Rothenberg, M.L.; Matrisian, L.M. Matrix metalloproteinases: Biologic activity and clinical implications. J. Clin. Oncol. 2000, 18, 1135–1149. [Google Scholar] [CrossRef]
- Eiró, N.; Fernandez-Garcia, B.; Gonzalez, L.; Vizoso, F. Clinical Relevance of Matrix Metalloproteases and their Inhibitors in Breast Cancer. J. Carcinogene Mutagene 2013, S13, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Wurtz, S.O.; Schrohl, A.S.; Sorensen, N.M.; Lademann, U.; Christensen, I.J.; Mouridsen, H.; Brunner, N. Tissue inhibitor of metalloproteinases-1 in breast cancer. Endocr. Relat. Cancer 2005, 12, 215–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brehmer, B.; Biesterfeld, S.; Jakse, G. Expression of matrix metalloproteinases (MMP-2 and -9) and their inhibitors (TIMP-1 and -2) in prostate cancer tissue. Prostate Cancer Prostatic Dis. 2003, 6, 217–222. [Google Scholar] [CrossRef] [Green Version]
- Morgia, G.; Falsaperla, M.; Malaponte, G.; Madonia, M.; Indelicato, M.; Travali, S.; Mazzarino, M.C. Matrix metalloproteinases as diagnostic (MMP-13) and prognostic (MMP-2, MMP-9) markers of prostate cancer. Urol. Res. 2005, 33, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Riddick, A.C.; Shukla, C.J.; Pennington, C.J.; Bass, R.; Nuttall, R.K.; Hogan, A.; Sethia, K.K.; Ellis, V.; Collins, A.T.; Maitland, N.J.; et al. Identification of degradome components associated with prostate cancer progression by expression analysis of human prostatic tissues. Br. J. Cancer 2005, 92, 2171–2180. [Google Scholar] [CrossRef] [Green Version]
- Semaan, M.; Jovenin, N.; Birembaut, P.; Menard, J.; Staerman, F. Prognostic value of stromal immunolabelling by MMP-2, MT1-MMP and TIMP-2 in clinically localized prostate cancer. Prog. Urol. 2005, 15, 250–254. [Google Scholar]
- Cardillo, M.R.; Di Silverio, F.; Gentile, V. Quantitative immunohistochemical and in situ hybridization analysis of metalloproteinases in prostate cancer. Anticancer Res. 2006, 26, 973–982. [Google Scholar]
- Escaff, S.; Fernandez, J.M.; Gonzalez, L.O.; Suarez, A.; Gonzalez-Reyes, S.; Gonzalez, J.M.; Vizoso, F.J. Study of matrix metalloproteinases and their inhibitors in prostate cancer. Br. J. Cancer 2010, 102, 922–929. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Gomez, J.; Escaf, S.; Gonzalez, L.O.; Suarez, A.; Gonzalez-Reyes, S.; Gonzalez, J.; Miranda, O.; Vizoso, F. Relationship between metalloprotease expression in tumour and stromal cells and aggressive behaviour in prostate carcinoma: Simultaneous high-throughput study of multiple metalloproteases and their inhibitors using tissue array analysis of radical prostatectomy samples. Scand. J. Urol. Nephrol. 2011, 45, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Escaff, S.; Fernandez, J.M.; Gonzalez, L.O.; Suarez, A.; Gonzalez-Reyes, S.; Gonzalez, J.M.; Vizoso, F.J. Collagenase-3 expression by tumor cells and gelatinase B expression by stromal fibroblast-like cells are associated with biochemical recurrence after radical prostatectomy in patients with prostate cancer. World J. Urol. 2011, 29, 657–663. [Google Scholar] [CrossRef]
- Cao, J.; Chiarelli, C.; Kozarekar, P.; Adler, H.L. Membrane type 1-matrix metalloproteinase promotes human prostate cancer invasion and metastasis. Thromb. Haemost. 2005, 93, 770–778. [Google Scholar] [CrossRef] [PubMed]
- Nabha, S.M.; Bonfil, R.D.; Yamamoto, H.A.; Belizi, A.; Wiesner, C.; Dong, Z.; Cher, M.L. Host matrix metalloproteinase-9 contributes to tumor vascularization without affecting tumor growth in a model of prostate cancer bone metastasis. Clin. Exp. Metastasis 2006, 23, 335–344. [Google Scholar] [CrossRef]
- Pulukuri, S.M.; Rao, J.S. Matrix metalloproteinase-1 promotes prostate tumor growth and metastasis. Int. J. Oncol. 2008, 32, 757–765. [Google Scholar] [PubMed] [Green Version]
- Trudel, D.; Fradet, Y.; Meyer, F.; Harel, F.; Tetu, B. Significance of MMP-2 expression in prostate cancer: An immunohistochemical study. Cancer Res. 2003, 63, 8511–8515. [Google Scholar]
- Escaff, S.; Fernandez, J.M.; Gonzalez, L.O.; Suarez, A.; Gonzalez-Reyes, S.; Gonzalez, J.M.; Vizoso, F.J. Comparative study of stromal metalloproteases expression in patients with benign hyperplasia and prostate cancer. J. Cancer Res. Clin. Oncol. 2011, 137, 551–555. [Google Scholar] [CrossRef]
- Gonzalez, L.O.; Eiro, N.; Fraile, M.; Beridze, N.; Escaf, A.R.; Escaf, S.; Fernandez-Gomez, J.M.; Vizoso, F.J. Prostate Cancer Tumor Stroma: Responsibility in Tumor Biology, Diagnosis and Treatment. Cancers 2022, 14, 4412. [Google Scholar] [CrossRef]
- Bettendorf, O.; Schmidt, H.; Staebler, A.; Grobholz, R.; Heinecke, A.; Boecker, W.; Hertle, L.; Semjonow, A. Chromosomal imbalances, loss of heterozygosity, and immunohistochemical expression of TP53, RB1, and PTEN in intraductal cancer, intraepithelial neoplasia, and invasive adenocarcinoma of the prostate. Genes Chromosomes Cancer 2008, 47, 565–572. [Google Scholar] [CrossRef]
- Epstein, J.I. Precursor lesions to prostatic adenocarcinoma. Virchows Arch. 2009, 454, 1–16. [Google Scholar] [CrossRef]
- Ayala, A.G.; Ro, J.Y. Prostatic intraepithelial neoplasia: Recent advances. Arch. Pathol. Lab. Med. 2007, 131, 1257–1266. [Google Scholar] [CrossRef] [PubMed]
- Barron, D.A.; Rowley, D.R. The reactive stroma microenvironment and prostate cancer progression. Endocr. Relat. Cancer 2012, 19, R187–R204. [Google Scholar] [CrossRef] [Green Version]
- Franco, O.E.; Hayward, S.W. Targeting the tumor stroma as a novel therapeutic approach for prostate cancer. Adv. Pharmacol. 2012, 65, 267–313. [Google Scholar] [CrossRef] [PubMed]
- Eiro, N.; Fernandez-Gomez, J.; Sacristan, R.; Fernandez-Garcia, B.; Lobo, B.; Gonzalez-Suarez, J.; Quintas, A.; Escaf, S.; Vizoso, F.J. Stromal factors involved in human prostate cancer development, progression and castration resistance. J. Cancer Res. Clin. Oncol. 2017, 143, 351–359. [Google Scholar] [CrossRef]
- Jones, J.L.; Glynn, P.; Walker, R.A. Expression of MMP-2 and MMP-9, their inhibitors, and the activator MT1-MMP in primary breast carcinomas. J. Pathol. 1999, 189, 161–168. [Google Scholar] [CrossRef]
- Egeblad, M.; Werb, Z. New functions for the matrix metalloproteinases in cancer progression. Nat. Rev. Cancer 2002, 2, 161–174. [Google Scholar] [CrossRef]
- Pei, D.; Weiss, S.J. Furin-dependent intracellular activation of the human stromelysin-3 zymogen. Nature 1995, 375, 244–247. [Google Scholar] [CrossRef] [Green Version]
- Peruzzi, D.; Mori, F.; Conforti, A.; Lazzaro, D.; De Rinaldis, E.; Ciliberto, G.; La Monica, N.; Aurisicchio, L. MMP11: A novel target antigen for cancer immunotherapy. Clin. Cancer Res. 2009, 15, 4104–4113. [Google Scholar] [CrossRef] [Green Version]
- Brasse, D.; Mathelin, C.; Leroux, K.; Chenard, M.P.; Blaise, S.; Stoll, I.; Tomasetto, C.; Rio, M.C. Matrix metalloproteinase 11/stromelysin-3 exerts both activator and repressor functions during the hematogenous metastatic process in mice. Int. J. Cancer 2010, 127, 1347–1355. [Google Scholar] [CrossRef]
- Boulay, A.; Masson, R.; Chenard, M.P.; El Fahime, M.; Cassard, L.; Bellocq, J.P.; Sautes-Fridman, C.; Basset, P.; Rio, M.C. High cancer cell death in syngeneic tumors developed in host mice deficient for the stromelysin-3 matrix metalloproteinase. Cancer Res. 2001, 61, 2189–2193. [Google Scholar]
- Jiang, Y.; Goldberg, I.D.; Shi, Y.E. Complex roles of tissue inhibitors of metalloproteinases in cancer. Oncogene 2002, 21, 2245–2252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palacios, A.M.; Sánchez, L.; Couso, I. Diagnosis of dyslexia with low quality data with genetic fuzzy systems. Int. J. Approx. Reason. 2010, 51, 993–1009. [Google Scholar] [CrossRef] [Green Version]
- Palaniappan, S.; Awang, R. Intelligent heart disease prediction system using data mining techniques. In Proceedings of the 2008 IEEE/ACS International Conference on Computer Systems and Applications, Doha, Qatar, 31 March–4 April 2008; pp. 108–115. [Google Scholar]
- Kourou, K.; Exarchos, T.P.; Exarchos, K.P.; Karamouzis, M.V.; Fotiadis, D.I. Machine learning applications in cancer prognosis and prediction. Comput. Struct. Biotechnol. J. 2015, 13, 8–17. [Google Scholar] [CrossRef] [Green Version]
- Bottaci, L.; Drew, P.J.; Hartley, J.E.; Hadfield, M.B.; Farouk, R.; Lee, P.W.; Macintyre, I.M.; Duthie, G.S.; Monson, J.R. Artificial neural networks applied to outcome prediction for colorectal cancer patients in separate institutions. Lancet 1997, 350, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, A.N.; Kambhampati, C.; Monson, J.R.; Drew, P.J. Artificial intelligence in medicine. Ann. R Coll. Surg. Engl. 2004, 86, 334–338. [Google Scholar] [CrossRef] [Green Version]
- Hamet, P.; Tremblay, J. Artificial intelligence in medicine. Metabolism 2017, 69S, S36–S40. [Google Scholar] [CrossRef] [PubMed]
- Doyle, S.; Madabhushi, A.; Feldman, M.; Tomaszeweski, J. A boosting cascade for automated detection of prostate cancer from digitized histology. Med. Image Comput. Comput. Assist. Interv. 2006, 9, 504–511. [Google Scholar] [CrossRef] [Green Version]
- Cruz, J.A.; Wishart, D.S. Applications of machine learning in cancer prediction and prognosis. Cancer Inform. 2007, 2, 59–77. [Google Scholar] [CrossRef]
- Hosseini, R.; Khezri, R.; Mazinani, M. A Fuzzy Rule-based Expert System for the Prognosis of the Risk of Development of the Breast Cancer. Int. J. Eng. 2014, 27, 1557–1564. [Google Scholar]
- Chiu, P.K.; Shen, X.; Wang, G.; Ho, C.L.; Leung, C.H.; Ng, C.F.; Choi, K.S.; Teoh, J.Y. Enhancement of prostate cancer diagnosis by machine learning techniques: An algorithm development and validation study. Prostate Cancer Prostatic Dis. 2021, 25, 672–676. [Google Scholar] [CrossRef]
- Flemming, I.; Cooper, J.; Henson, D.; Hutte, R.; Kennedy, B.; Murphy, G.; O’Sullivan, B.; Sobin, L.; Yarbro, J. American Joint Committee on Cancer Manual for Staging of Cancer; Lippincott-Raven: Philadelphia, PA, USA, 1997. [Google Scholar]
- Fernandez-Garcia, B.; Eiro, N.; Miranda, M.A.; Cid, S.; Gonzalez, L.O.; Dominguez, F.; Vizoso, F.J. Prognostic significance of inflammatory factors expression by stroma from breast carcinomas. Carcinogenesis 2016, 37, 768–776. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, L.O.; Gonzalez-Reyes, S.; Marin, L.; Gonzalez, L.; Gonzalez, J.M.; Lamelas, M.L.; Merino, A.M.; Rodriguez, E.; Pidal, I.; del Casar, J.M.; et al. Comparative analysis and clinical value of the expression of metalloproteases and their inhibitors by intratumour stromal mononuclear inflammatory cells and those at the invasive front of breast carcinomas. Histopathology 2010, 57, 862–876. [Google Scholar] [CrossRef]
- Zhao, Z.; Liu, H. Spectral feature selection for supervised and unsupervised learning. In Proceedings of the 24th International Conference on Machine Learning, Corvalis, OR, USA, 20–24 June 2007; pp. 1151–1157. [Google Scholar]
- Efron, B. Bootstrap methods: Another look at the jackknife. Ann. Stat. 1979, 7, 1–26. [Google Scholar] [CrossRef]
- Hühn, J.; Hüllermeier, E. FURIA: An algorithm for unordered fuzzy rule induction. Data Min. Knowl. Discov. 2009, 19, 293–319. [Google Scholar] [CrossRef] [Green Version]
- Hühn, J.C.; Hüllermeier, E. An Analysis of the FURIA Algorithm for Fuzzy Rule Induction. In Advances in Machine Learning I: Dedicated to the Memory of Professor Ryszard S. Michalski; Koronacki, J., Raś, Z.W., Wierzchoń, S.T., Kacprzyk, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2010; pp. 321–344. [Google Scholar]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Srivastava, D.; Bhambhu, L. Data classification using support vector machine. J. Theor. Appl. Inf. Technol. 2010, 12, 1–7. [Google Scholar]
- Coudray, N.; Ocampo, P.S.; Sakellaropoulos, T.; Narula, N.; Snuderl, M.; Fenyö, D.; Moreira, A.L.; Razavian, N.; Tsirigos, A. Classification and mutation prediction from non–small cell lung cancer histopathology images using deep learning. Nat. Med. 2018, 24, 1559–1567. [Google Scholar] [CrossRef]
- Dreiseitl, S.; Ohno-Machado, L. Logistic regression and artificial neural network classification models: A methodology review. J. Biomed. Inform. 2002, 35, 352–359. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Epithelial Cells | SVM | LR | DeepL | xbgoost | FURIA |
|---|---|---|---|---|---|
| C1 vs. C5 | 97.2% | 95.9% | 71.6% | 95.9% | 97.2% |
| C2 vs. C5 | 95.9% | 91.8% | 78.3% | 93.2% | 96.0% |
| C1 vs. C6 | 95.7% | 93.6% | 72.3% | 95.7% | 97.6% |
| C2 vs. C6 | 93.6% | 87.2% | 61.7% | 82.9% | 98.0% |
| Fibroblasts | SVM | LR | DeepL | xbgoost | FURIA |
|---|---|---|---|---|---|
| C1 vs. C5 | 67.5% | 71.6% | 62.1% | 78.3% | 84.2% |
| C2 vs. C5 | 83.7% | 77.0% | 64.8% | 85.1% | 87.8% |
| C1 vs. C6 | 78.7% | 80.8% | 57.4% | 85.1% | 88.5% |
| C2 vs. C6 | 78.7% | 68.0% | 55.3% | 74.4% | 81.7% |
| Benign prostate biopsy before the diagnosis of PCa Class 1: Zone without future cancer development (C1) Class 2: Zone with future tumor (C2) |
| Positive biopsy: PCa Class 3: Non-tumor area from prostatectomy (C3) Class 4: Tumor area from prostatectomy (C4) |
| Class 5: Benign prostatic hyperplasia (BPH) (C5) |
| Class 6: High-grade prostate intraepithelial neoplasia (HGPIN) (C6) |
| Prediction | |||
|---|---|---|---|
| Positives | Negatives | ||
| True | Positives | VN | FN |
| Negatives | FP | VN | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eiro, N.; Medina, A.; Gonzalez, L.O.; Fraile, M.; Palacios, A.; Escaf, S.; Fernández-Gómez, J.M.; Vizoso, F.J. Evaluation of Matrix Metalloproteases by Artificial Intelligence Techniques in Negative Biopsies as New Diagnostic Strategy in Prostate Cancer. Int. J. Mol. Sci. 2023, 24, 7022. https://doi.org/10.3390/ijms24087022
Eiro N, Medina A, Gonzalez LO, Fraile M, Palacios A, Escaf S, Fernández-Gómez JM, Vizoso FJ. Evaluation of Matrix Metalloproteases by Artificial Intelligence Techniques in Negative Biopsies as New Diagnostic Strategy in Prostate Cancer. International Journal of Molecular Sciences. 2023; 24(8):7022. https://doi.org/10.3390/ijms24087022
Chicago/Turabian StyleEiro, Noemi, Antonio Medina, Luis O. Gonzalez, Maria Fraile, Ana Palacios, Safwan Escaf, Jesús M. Fernández-Gómez, and Francisco J. Vizoso. 2023. "Evaluation of Matrix Metalloproteases by Artificial Intelligence Techniques in Negative Biopsies as New Diagnostic Strategy in Prostate Cancer" International Journal of Molecular Sciences 24, no. 8: 7022. https://doi.org/10.3390/ijms24087022
APA StyleEiro, N., Medina, A., Gonzalez, L. O., Fraile, M., Palacios, A., Escaf, S., Fernández-Gómez, J. M., & Vizoso, F. J. (2023). Evaluation of Matrix Metalloproteases by Artificial Intelligence Techniques in Negative Biopsies as New Diagnostic Strategy in Prostate Cancer. International Journal of Molecular Sciences, 24(8), 7022. https://doi.org/10.3390/ijms24087022