
Comprehensive Analysis of the Prognostic Value of Circulating MMP-7 Levels in Urothelial Carcinoma: A Combined Cohort Analysis, Systematic Review, and Meta-Analysis

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Cohorts
2.2. Serum MMP-7 ELISA Analysis
2.3. Meta-Analysis
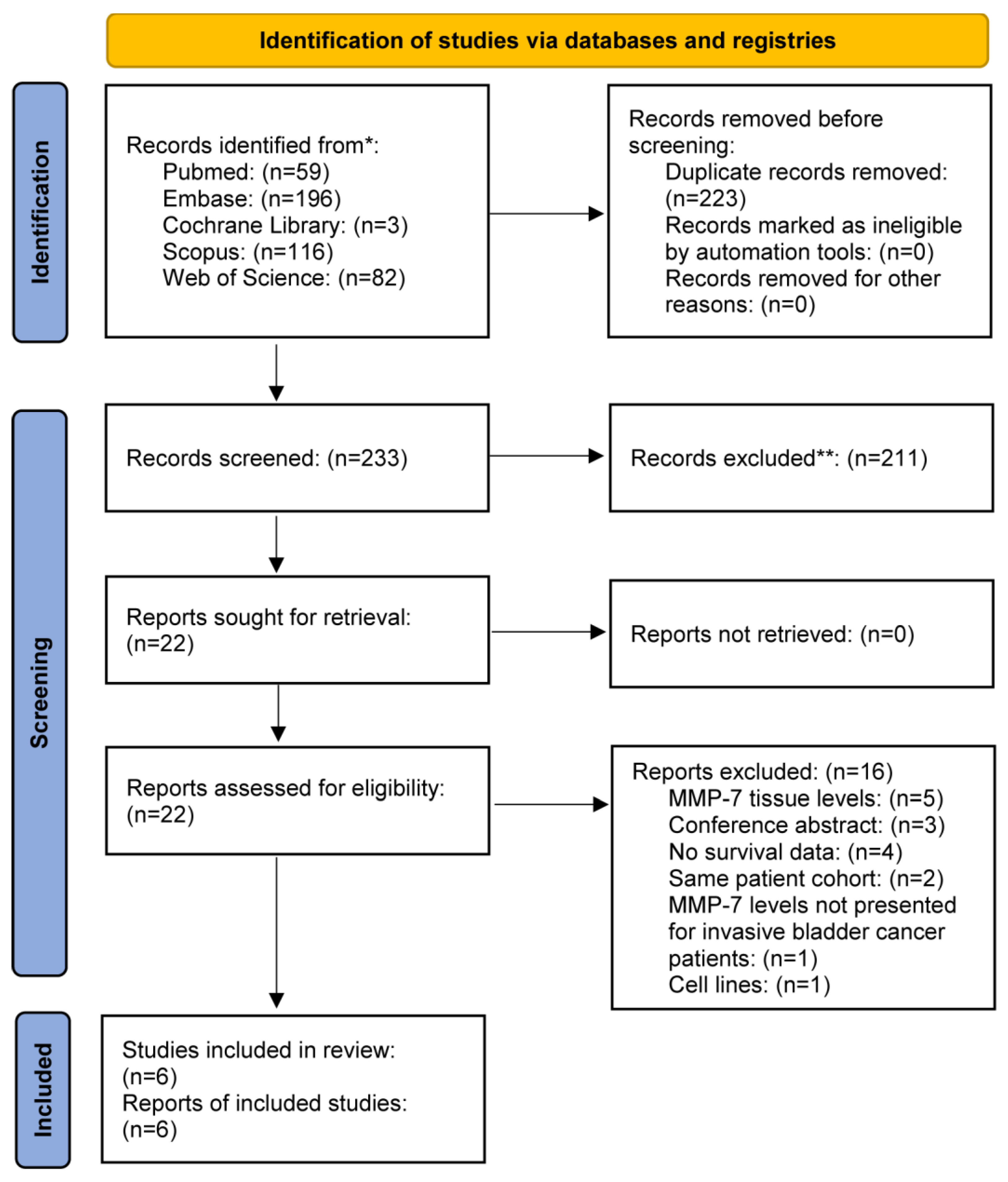
2.3.1. Literature Search
2.3.2. Eligibility Criteria
2.3.3. Data Extraction
2.3.4. Quality Assessment and Evaluation of Evidence
2.3.5. Synthesis Methods
2.3.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.1.1. Present Study Cohort 1
3.1.2. Present Study Cohort 2
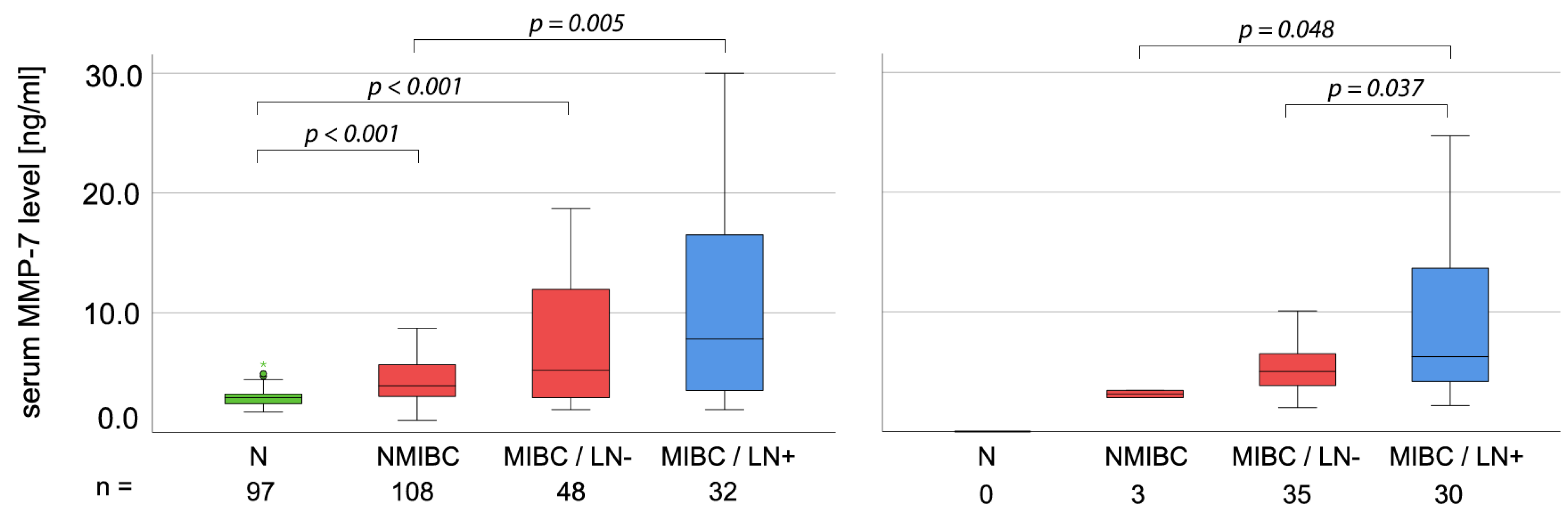
3.2. Correlation of MMP-7 Levels with Clinicopathological Parameters
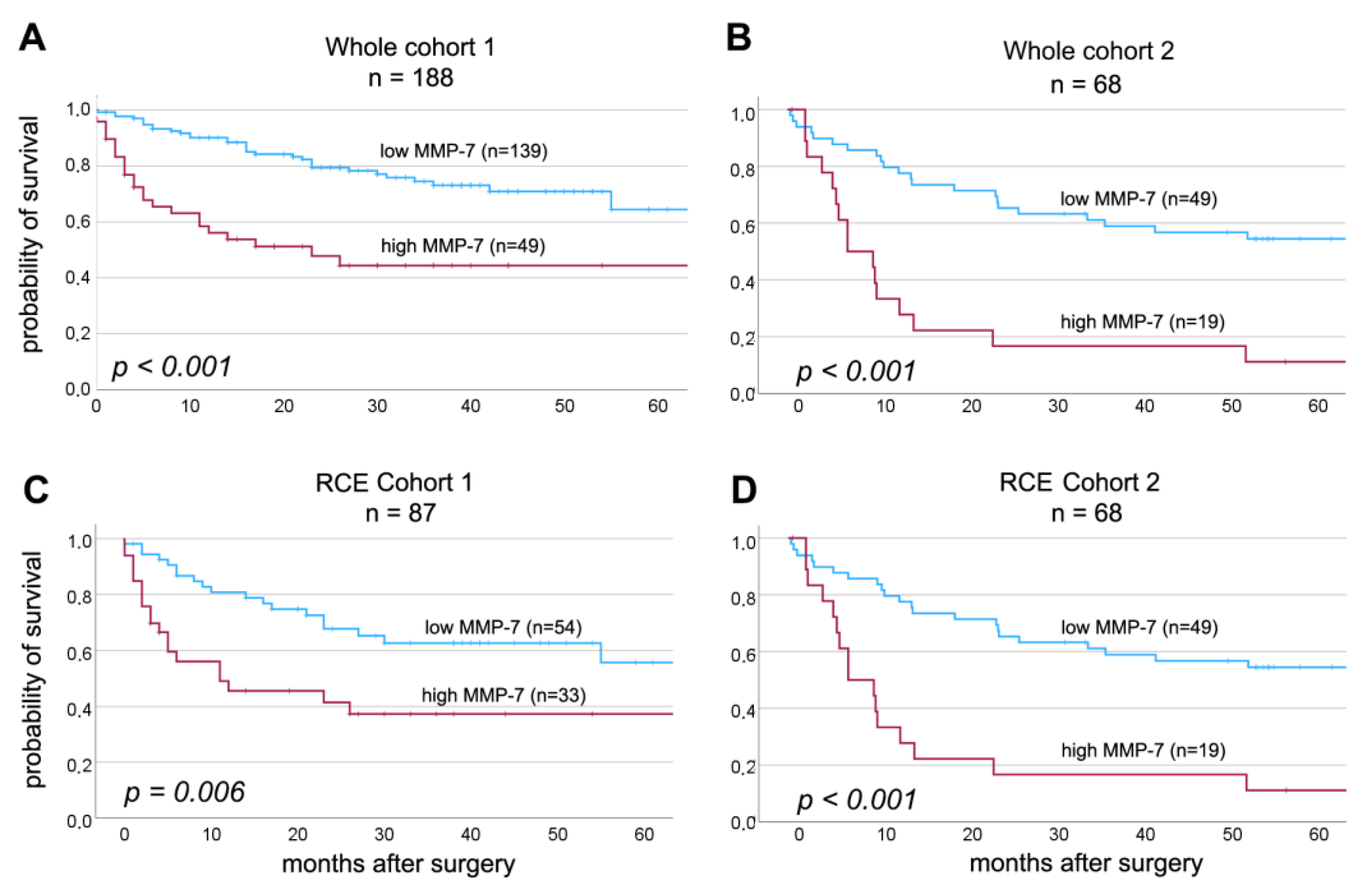
3.3. Correlation of Clinicopathological Parameters and Pretreatment Serum MMP-7 Levels with Patient Prognosis
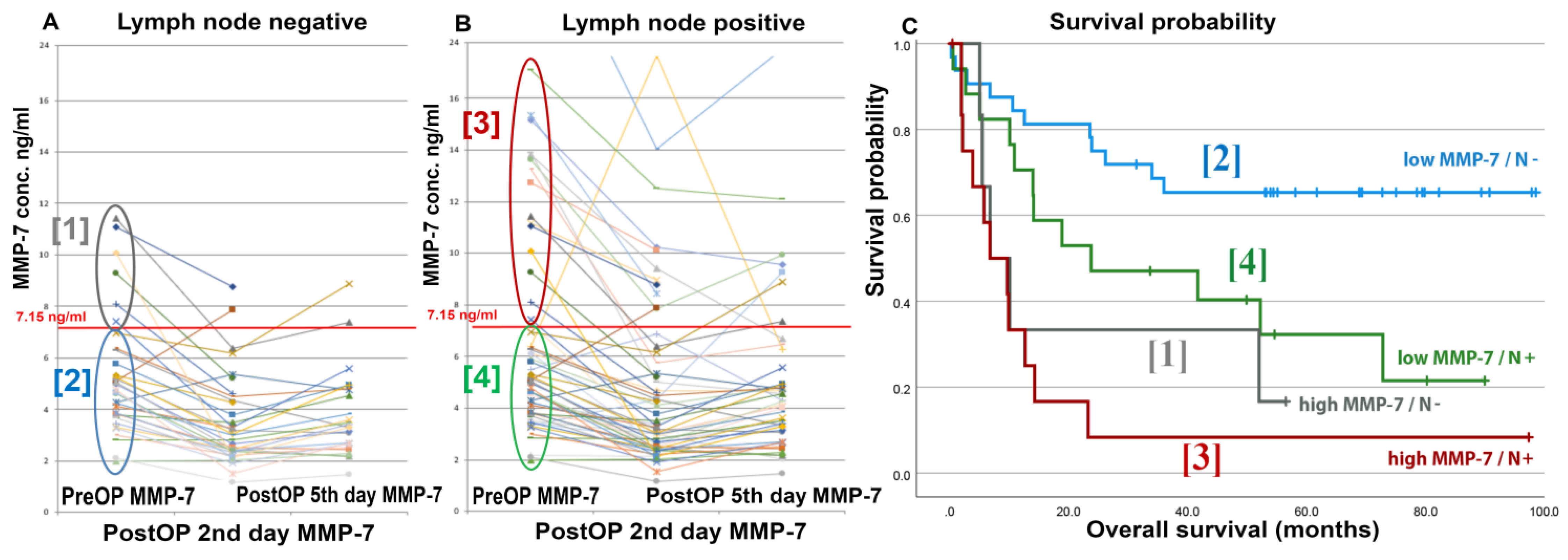
3.4. Correlation of Pretreatment Serum MMP-7 Levels with the Localization of LN Metastases
3.5. Changes of MMP-7 Levels after Radical Cystectomy
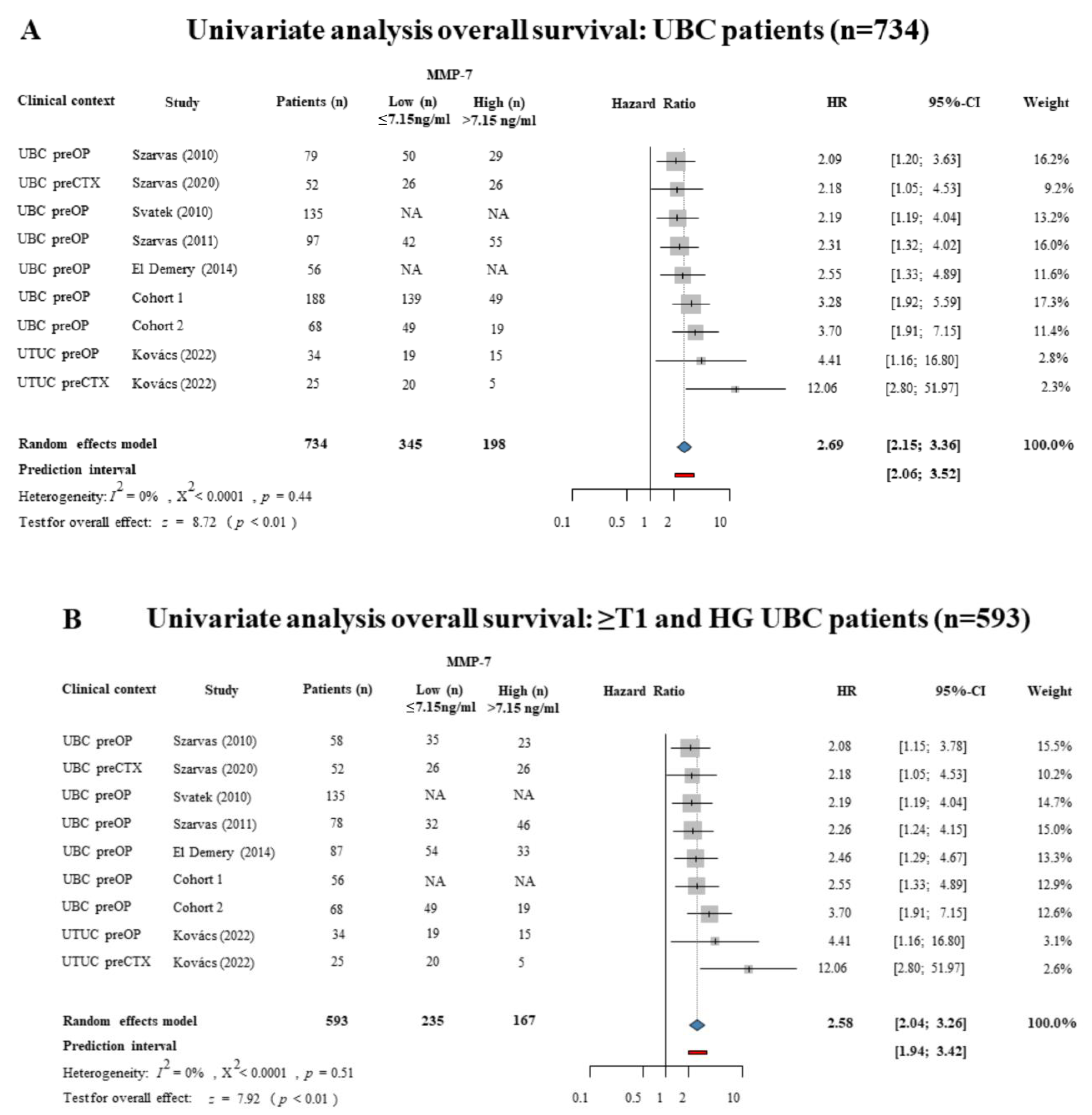
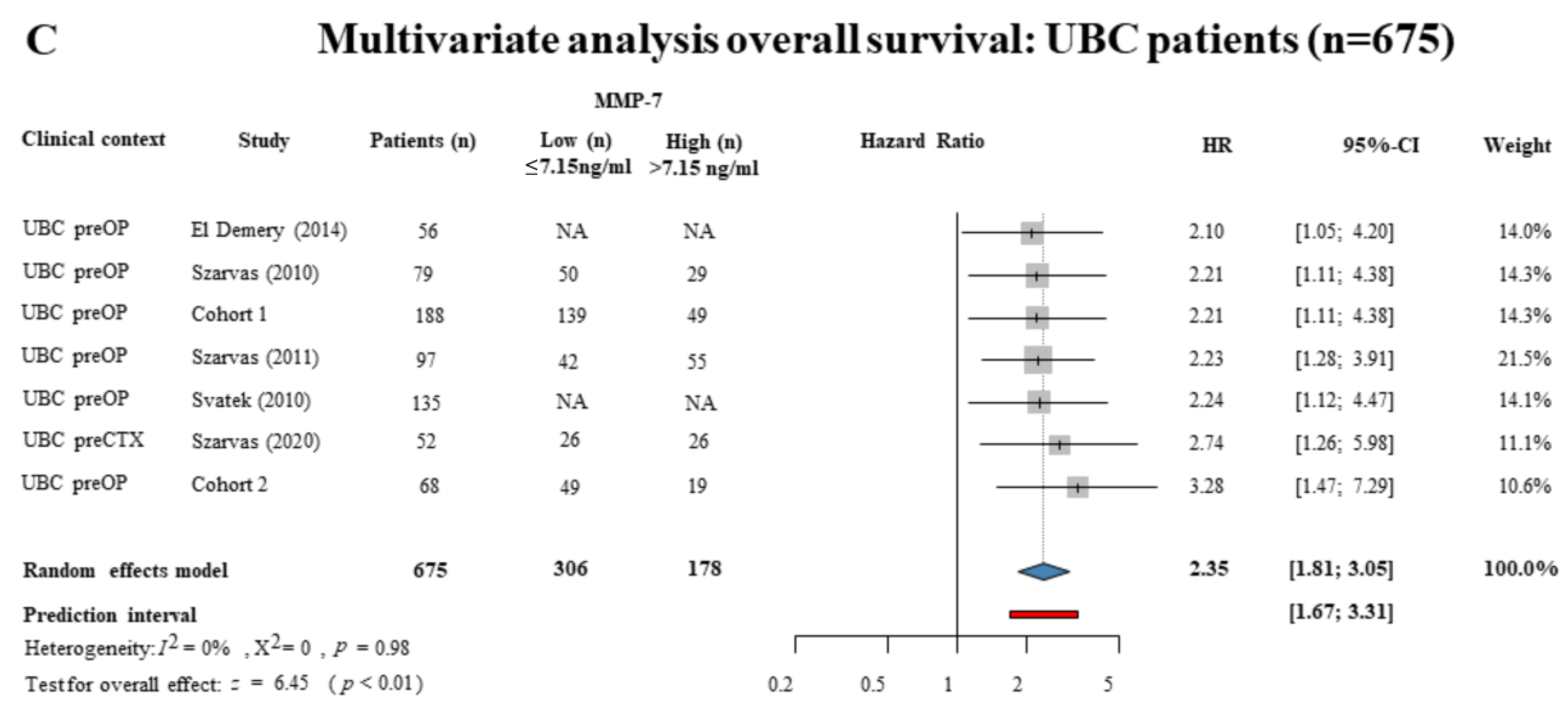
3.6. Meta-Analysis of the Literature
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kiss, B.; Burkhard, F.C.; Thalmann, G.N. Open radical cystectomy: Still the gold standard for muscle invasive bladder cancer. World J. Urol. 2016, 34, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.P.; Skinner, D.G. Radical cystectomy for invasive bladder cancer: Long-term results of a standard procedure. World J. Urol. 2006, 24, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Bochner, B.H.; Montie, J.E.; Lee, C.T. Follow-up strategies and management of recurrence in urologic oncology bladder cancer: Invasive bladder cancer. Urol. Clin. N. Am. 2003, 30, 777–789. [Google Scholar] [CrossRef] [PubMed]
- Hautmann, R.E.; de Petriconi, R.C.; Pfeiffer, C.; Volkmer, B.G. Radical cystectomy for urothelial carcinoma of the bladder without neoadjuvant or adjuvant therapy: Long-term results in 1100 patients. Eur. Urol. 2012, 61, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.P.; Lieskovsky, G.; Cote, R.; Groshen, S.; Feng, A.C.; Boyd, S.; Skinner, E.; Bochner, B.; Thangathurai, D.; Mikhail, M.; et al. Radical cystectomy in the treatment of invasive bladder cancer: Long-term results in 1,054 patients. J. Clin. Oncol. 2001, 19, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Horn, T.; Zahel, T.; Adt, N.; Schmid, S.C.; Heck, M.M.; Thalgott, M.K.; Hatzichristodoulou, G.; Haller, B.; Autenrieth, M.; Kubler, H.R.; et al. Evaluation of Computed Tomography for Lymph Node Staging in Bladder Cancer Prior to Radical Cystectomy. Urol. Int. 2016, 96, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Tarin, T.V.; Power, N.E.; Ehdaie, B.; Sfakianos, J.P.; Silberstein, J.L.; Savage, C.J.; Sjoberg, D.; Dalbagni, G.; Bochner, B.H. Lymph node-positive bladder cancer treated with radical cystectomy and lymphadenectomy: Effect of the level of node positivity. Eur. Urol. 2012, 61, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.B.; Ulhoi, B.P.; Jensen, K.M. Extended versus limited lymph node dissection in radical cystectomy: Impact on recurrence pattern and survival. Int. J. Urol. 2012, 19, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Abol-Enein, H.; Tilki, D.; Mosbah, A.; El-Baz, M.; Shokeir, A.; Nabeeh, A.; Ghoneim, M.A. Does the extent of lymphadenectomy in radical cystectomy for bladder cancer influence disease-free survival? A prospective single-center study. Eur. Urol. 2011, 60, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Gschwend, J.E.; Heck, M.M.; Lehmann, J.; Rubben, H.; Albers, P.; Wolff, J.M.; Frohneberg, D.; de Geeter, P.; Heidenreich, A.; Kalble, T.; et al. Extended Versus Limited Lymph Node Dissection in Bladder Cancer Patients Undergoing Radical Cystectomy: Survival Results from a Prospective, Randomized Trial. Eur. Urol. 2019, 75, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Lerner, S.P.; Tangen, C.M.; Svatek, R.S.; Koppie, T.M.; Alva, A.; La Rosa, F.G.; Pal, S.K.; Daneshmand, S.; Dinney, C.P.N.; Kibel, A.S.; et al. A Phase Iii Surgical Trial to Evaluate the Benefit of a Standard Versus an Extended Pelvic Lymphadenectomy Performed at Time of Radical Cystectomy for Muscle Invasive Urothelial Cancer: Swog S1011 (Nct #01224665). J. Urol. 2015, 193, E807. [Google Scholar] [CrossRef]
- Simone, G.; Papalia, R.; Ferriero, M.; Guaglianone, S.; Castelli, E.; Collura, D.; Muto, G.; Gallucci, M. Stage-specific impact of extended versus standard pelvic lymph node dissection in radical cystectomy. Int. J. Urol. 2013, 20, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Dhar, N.B.; Klein, E.A.; Reuther, A.M.; Thalmann, G.N.; Madersbacher, S.; Studer, U.E. Outcome after radical cystectomy with limited or extended pelvic lymph node dissection. J. Urol. 2008, 179, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Liao, H.Y.; Da, C.M.; Liao, B.; Zhang, H.H. Roles of matrix metalloproteinase-7 (MMP-7) in cancer. Clin. Biochem. 2021, 92, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Szarvas, T.; Becker, M.; vom Dorp, F.; Gethmann, C.; Tötsch, M.; Bánkfalvi, A.; Schmid, K.W.; Romics, I.; Rübben, H.; Ergün, S. Matrix metalloproteinase-7 as a marker of metastasis and predictor of poor survival in bladder cancer. Cancer Sci. 2010, 101, 1300–1308. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Svatek, R.S.; Shah, J.B.; Xing, J.; Chang, D.; Lin, J.; McConkey, D.J.; Wu, X.; Dinney, C.P. A multiplexed, particle-based flow cytometric assay identified plasma matrix metalloproteinase-7 to be associated with cancer-related death among patients with bladder cancer. Cancer 2010, 116, 4513–4519. [Google Scholar] [CrossRef] [PubMed]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Cote, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis with R: A Hands-On Guide; Chapman & Hall/CRC Press: Boca Raton, FL, USA; London, UK, 2021; ISBN 978-0-367-61007-4. Available online: http://dmetar.protectlab.org (accessed on 11 November 2022).
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- IntHout, J.; Ioannidis, J.P.; Rovers, M.M.; Goeman, J.J. Plea for routinely presenting prediction intervals in meta-analysis. BMJ Open 2016, 6, e010247. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W.; Cheung, M.W. Outlier and influence diagnostics for meta-analysis. Res. Synth. Methods 2010, 1, 112–125. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, V., Austria. 2022. Available online: https://www.R-project.org (accessed on 11 November 2022).
- Schwarzer, G. Meta-Analysis in R. In Systematic Reviews in Health Research: Meta-Analysis in Context; John Wiley & Sons: Hoboken, NJ, USA, 2022; pp. 510–534. [Google Scholar]
- Szarvas, T.; Jäger, T.; Becker, M.; Tschirdewahn, S.; Niedworok, C.; Kovalszky, I.; Rübben, H.; Ergün, S.; vom Dorp, F. Validation of circulating MMP-7 level as an independent prognostic marker of poor survival in urinary bladder cancer. Pathol. Oncol. Res. 2011, 17, 325–332. [Google Scholar] [CrossRef]
- El Demery, M.; Demirdjian-Sarkissian, G.; Thezenas, S.; Jacot, W.; Laghzali, Y.; Darbouret, B.; Culine, S.; Rebillard, X.; Lamy, P.J. Serum Matrix Metalloproteinase-7 is an independent prognostic biomarker in advanced bladder cancer. Clin. Transl. Med. 2014, 3, 31. [Google Scholar] [CrossRef] [PubMed]
- Szarvas, T.; Hoffmann, M.J.; Olah, C.; Szekely, E.; Kiss, A.; Hess, J.; Tschirdewahn, S.; Hadaschik, B.; Grotheer, V.; Nyirady, P.; et al. MMP-7 Serum and Tissue Levels Are Associated with Poor Survival in Platinum-Treated Bladder Cancer Patients. Diagnostics 2020, 11, 48. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, P.T.; Mayer, T.; Csizmarik, A.; Varadi, M.; Olah, C.; Szeles, A.; Tschirdewahn, S.; Krafft, U.; Hadaschik, B.; Nyirady, P.; et al. Elevated Pre-Treatment Serum MMP-7 Levels Are Associated with the Presence of Metastasis and Poor Survival in Upper Tract Urothelial Carcinoma. Biomedicines 2022, 10, 698. [Google Scholar] [CrossRef] [PubMed]
- Benoit, T.; Keller, E.X.; Wolfsgruber, P.; Hermanns, T.; Günthart, M.; Banzola, I.; Sulser, T.; Provenzano, M.; Poyet, C. High VEGF-D and Low MMP-2 Serum Levels Predict Nodal-Positive Disease in Invasive Bladder Cancer. Med. Sci. Monit. 2015, 21, 2266–2274. [Google Scholar] [CrossRef]
- Bryan, R.T.; Gordon, N.S.; Abbotts, B.; Zeegers, M.P.; Cheng, K.K.; James, N.D.; Ward, D.G. Multiplex screening of 422 candidate serum biomarkers in bladder cancer patients identifies syndecan-1 and macrophage colony-stimulating factor 1 as prognostic indicators. Transl. Cancer Res. 2017, 6, S657–S665. [Google Scholar] [CrossRef]
- Vargo-Gogola, T.; Crawford, H.C.; Fingleton, B.; Matrisian, L.M. Identification of novel matrix metalloproteinase-7 (matrilysin) cleavage sites in murine and human Fas ligand. Arch. Biochem. Biophys. 2002, 408, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Ii, M.; Yamamoto, H.; Adachi, Y.; Maruyama, Y.; Shinomura, Y. Role of matrix metalloproteinase-7 (matrilysin) in human cancer invasion, apoptosis, growth, and angiogenesis. Exp. Biol. Med. 2006, 231, 20–27. [Google Scholar] [CrossRef]
- Szarvas, T.; vom Dorp, F.; Ergün, S.; Rübben, H. Matrix metalloproteinases and their clinical relevance in urinary bladder cancer. Nat. Rev. Urol. 2011, 8, 241–254. [Google Scholar] [CrossRef] [PubMed]
- Bolenz, C.; Knauf, D.; John, A.; Erben, P.; Steidler, A.; Schneider, S.W.; Gunes, C.; Gorzelanny, C. Decreased Invasion of Urothelial Carcinoma of the Bladder by Inhibition of Matrix-Metalloproteinase 7. Bladder Cancer 2018, 4, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Gong, T.; Kong, K.V.; Goh, D.; Olivo, M.; Yong, K.T. Sensitive surface enhanced Raman scattering multiplexed detection of matrix metalloproteinase 2 and 7 cancer markers. Biomed. Opt. Express 2015, 6, 2076–2087. [Google Scholar] [CrossRef]
- Rangasamy, L.; Geronimo, B.D.; Ortin, I.; Coderch, C.; Zapico, J.M.; Ramos, A.; de Pascual-Teresa, B. Molecular Imaging Probes Based on Matrix Metalloproteinase Inhibitors (MMPIs). Molecules 2019, 24, 2982. [Google Scholar] [CrossRef]
- Vandenbroucke, R.E.; Libert, C. Is there new hope for therapeutic matrix metalloproteinase inhibition? Nat. Rev. Drug Discov. 2014, 13, 904–927. [Google Scholar] [CrossRef]
- Wang, L.L.; Zhang, B.; Zheng, M.H.; Xie, Y.Z.; Wang, C.J.; Jin, J.Y. Matrix Metalloproteinases (MMPs) in Targeted Drug Delivery: Synthesis of a Potent and Highly Selective Inhibitor against Matrix Metalloproteinase- 7. Curr. Top. Med. Chem. 2020, 20, 2459–2471. [Google Scholar] [CrossRef]
- Laronha, H.; Carpinteiro, I.; Portugal, J.; Azul, A.; Polido, M.; Petrova, K.T.; Salema-Oom, M.; Caldeira, J. Challenges in Matrix Metalloproteinases Inhibition. Biomolecules 2020, 10, 717. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort 1 | Cohort 2 | ||||||
|---|---|---|---|---|---|---|---|
| PreOP Serum MMP-7 cc. | PreOP Serum MMP-7 cc. | ||||||
| Parameters | n | Median (Range) | p | n | Median (Range) | p | |
| Whole UBC cohort | 188 | 4.2 (1.0–75.2) | <0.001 | 68 | 5.21 (1.99–24.71) | - | |
| Non-tumorous control | 97 | 2.9 (1.7–5.7) | - | 0 | - | - | |
| Age | ≤65 | 51 | 3.6 (1.6–75.2) | 0.006 | 28 | 5.26 (1.99–15.34) | 0.866 |
| >65 | 137 | 4.6 (1.9–62.0) | - | 40 | 5.20 (2.09–24.70) | - | |
| Sex | male | 149 | 4.1 (1.6–62.0) | 0.622 | 43 | 4.77 (2.09–24.00) | 0.239 |
| female | 39 | 4.4 (1.0–75.2) | - | 25 | 6.11 (2.09–24.70) | - | |
| Stage | Ta | 81 | 3.9 (1.4–18.2) | - | 0 | - | - |
| Cis | 8 | 3.6 (2.4–2.6) | - | 2 | 3.13 (2.83–3.43) | - | |
| T1 | 19 | 3.9 (1.0–15.9) | - | 1 | 3.62 | - | |
| T2 | 28 | 5.8 (1.9–75.2) | - | 20 | 4.87 (1.99–9.28) | - | |
| T3 | 27 | 4.4 (2.3–26.2) | - | 32 | 6.23 (2.98–24.71) | - | |
| T4 | 25 | 6.2 (1.9–62.0) | - | 13 | 5.91 (2.09–17.09) | - | |
| Non-inv. | (Cis-Ta-T1) | 108 | 3.9 (1.0–18.2) | 0.006 | 3 | 3.43 (2.82–3.62) | 0.030 |
| Invasive | (T2–T4) | 80 | 5.3 (1.9–75.2) | - | 65 | 5.31 (1.99–24.71) | |
| Grade | G1 | 37 | 4.1 (1.9–18.0) | - | 0 | - | - |
| G2 | 93 | 4.4 (1.0–30.0) | - | 9 | 6.11 (2.83–12.73) | - | |
| G3 | 58 | 4.1 (1.9–75.2) | - | 47 | 5.31 (2.09–24.71) | - | |
| Unknown | 0 | - | 12 | - | |||
| Low-grade | (G1–2) | 130 | 4.3 (1.0–30.0) | 0.622 | 9 | 6.11 (2.83–12.73) | 0.973 |
| High-grade | (G3) | 58 | 4.1 (1.9–75.2) | - | 47 | 5.31 (2.09–24.71) | |
| Surgery | TURB | 101 | 3.9 (1.0–18.2) | 0.021 | 0 | - | - |
| RC | 87 | 4.7 (1.9–75.2) | - | 68 | 5.21 (1.99–24.71) | - | |
| Lymph node | N0/Nx | 156 | 4.0 (1.0–75.2) | 0.015 | 38 | 4.87 (1.99–24.00) | 0.021 |
| N+ | 32 | 7.8 (1.9–75.2) | 30 | 6.25 (2.17–24.71) | |||
| Cohort 1 | Cohort 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| OS | OS | ||||||||
| General Data | n | HR | 95% CI | p | n | HR | 95% CI | p | |
| Age | ≤65 | 51 | ref. | 28 | ref. | ||||
| >65 | 137 | 1.727 | 0.892–3.343 | 0.105 | 40 | 1.444 | 0.757–2.756 | 0.265 | |
| Sex | female | 39 | ref. | 43 | ref. | ||||
| male | 149 | 0.660 | 0.369–1.179 | 0.160 | 25 | 0.902 | 0.463–1.758 | 0.762 | |
| Stage | NMIBC (Cis-Ta-T1) | 108 | ref. | ref. | |||||
| MIBC (T2–T4) | 80 | 3.705 | 2.093–6.558 | <0.001 | 65 | 2.085 | 0.286–15.206 | 0.469 | |
| Grade | Low-grade (G1–2) | 130 | ref. | 9 | ref. | ||||
| High-grade (G3) | 58 | 2.489 | 1.470–4.212 | 0.001 | 47 | 1.389 | 0.541–3.568 | 0.495 | |
| LN status | N0/Nx | 156 | ref. | 38 | ref. | ||||
| N+ | 32 | 5.523 | 3.213–9.492 | <0.001 | 30 | 2.721 | 1.427–5.189 | 0.002 | |
| PreOP MMP-7 whole cohort | 188 | 68 | |||||||
| ≤7.15 ng/mL | 139 | ref. | 49 | ref. | |||||
| >7.15 ng/mL | 49 | 3.276 | 1.921–5.589 | <0.001 | 19 | 3.699 | 1.913–7.153 | <0.001 | |
| NMIBC (Ta-Cis-T1) | 108 | 3 | |||||||
| ≤7.15 ng/mL | 92 | ref. | 3 | - | |||||
| >7.15 ng/mL | 16 | 2.743 | 0.885–8.502 | 0.080 | 0 | - | - | - | |
| MIBC (T2–T4) | 80 | 65 | |||||||
| ≤7.15 ng/mL | 47 | ref. | 46 | ref. | |||||
| >7.15 ng/mL | 33 | 2.217 | 1.176–4.180 | 0.014 | 19 | 3.623 | 1.860–7.055 | <0.001 | |
| RC | 87 | 68 | |||||||
| ≤7.15 ng/mL | 54 | ref. | 48 | ref. | |||||
| >7.15 ng/mL | 33 | 2.455 | 1.291–4.669 | 0.006 | 19 | 3.699 | 1.913–7.153 | <0.001 | |
| TURB | 101 | 0 | |||||||
| ≤7.15 ng/mL | 85 | ref. | 0 | - | |||||
| >7.15 ng/mL | 16 | 3.085 | 1.090–8.736 | 0.034 | 0 | - | - | - | |
| Cohort 1 | Cohort 2 | ||||||
|---|---|---|---|---|---|---|---|
| OS | OS | ||||||
| General Data | HR | 95% CI | p | HR | 95% CI | p | |
| Stage | ≤T2 vs. >T2 | 4.253 | 1.764–10.252 | 0.001 | 1.272 | 0.493–3.281 | 0.619 |
| Grade | 2 vs. 3 | 1.424 | 0.664–3.054 | 0.364 | 1.256 | 0.484–3.261 | 0.640 |
| Lymph node | neg. vs. pos. | 2.316 | 1.115–4.810 | 0.024 | 1.434 | 0.685–2.999 | 0.339 |
| MMP-7: ≤7.15 vs. >7.15 ng/mL | 2.206 | 1.111–4.380 | 0.024 | 3.279 | 1.475–7.290 | 0.004 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kubik, A.; das Virgens, I.P.A.; Szabó, A.; Váradi, M.; Csizmarik, A.; Keszthelyi, A.; Majoros, A.; Fehérvári, P.; Hegyi, P.; Ács, N.; et al. Comprehensive Analysis of the Prognostic Value of Circulating MMP-7 Levels in Urothelial Carcinoma: A Combined Cohort Analysis, Systematic Review, and Meta-Analysis. Int. J. Mol. Sci. 2023, 24, 7859. https://doi.org/10.3390/ijms24097859
Kubik A, das Virgens IPA, Szabó A, Váradi M, Csizmarik A, Keszthelyi A, Majoros A, Fehérvári P, Hegyi P, Ács N, et al. Comprehensive Analysis of the Prognostic Value of Circulating MMP-7 Levels in Urothelial Carcinoma: A Combined Cohort Analysis, Systematic Review, and Meta-Analysis. International Journal of Molecular Sciences. 2023; 24(9):7859. https://doi.org/10.3390/ijms24097859
Chicago/Turabian StyleKubik, András, Isabel Pinto Amorim das Virgens, Anett Szabó, Melinda Váradi, Anita Csizmarik, Attila Keszthelyi, Attila Majoros, Péter Fehérvári, Péter Hegyi, Nándor Ács, and et al. 2023. "Comprehensive Analysis of the Prognostic Value of Circulating MMP-7 Levels in Urothelial Carcinoma: A Combined Cohort Analysis, Systematic Review, and Meta-Analysis" International Journal of Molecular Sciences 24, no. 9: 7859. https://doi.org/10.3390/ijms24097859
APA StyleKubik, A., das Virgens, I. P. A., Szabó, A., Váradi, M., Csizmarik, A., Keszthelyi, A., Majoros, A., Fehérvári, P., Hegyi, P., Ács, N., Nyirády, P., & Szarvas, T. (2023). Comprehensive Analysis of the Prognostic Value of Circulating MMP-7 Levels in Urothelial Carcinoma: A Combined Cohort Analysis, Systematic Review, and Meta-Analysis. International Journal of Molecular Sciences, 24(9), 7859. https://doi.org/10.3390/ijms24097859