
Recent Developments in Combination Chemotherapy for Colorectal and Breast Cancers with Topoisomerase Inhibitors


Abstract
:1. Introduction
2. Combination Therapy
3. TOPO I Inhibitors
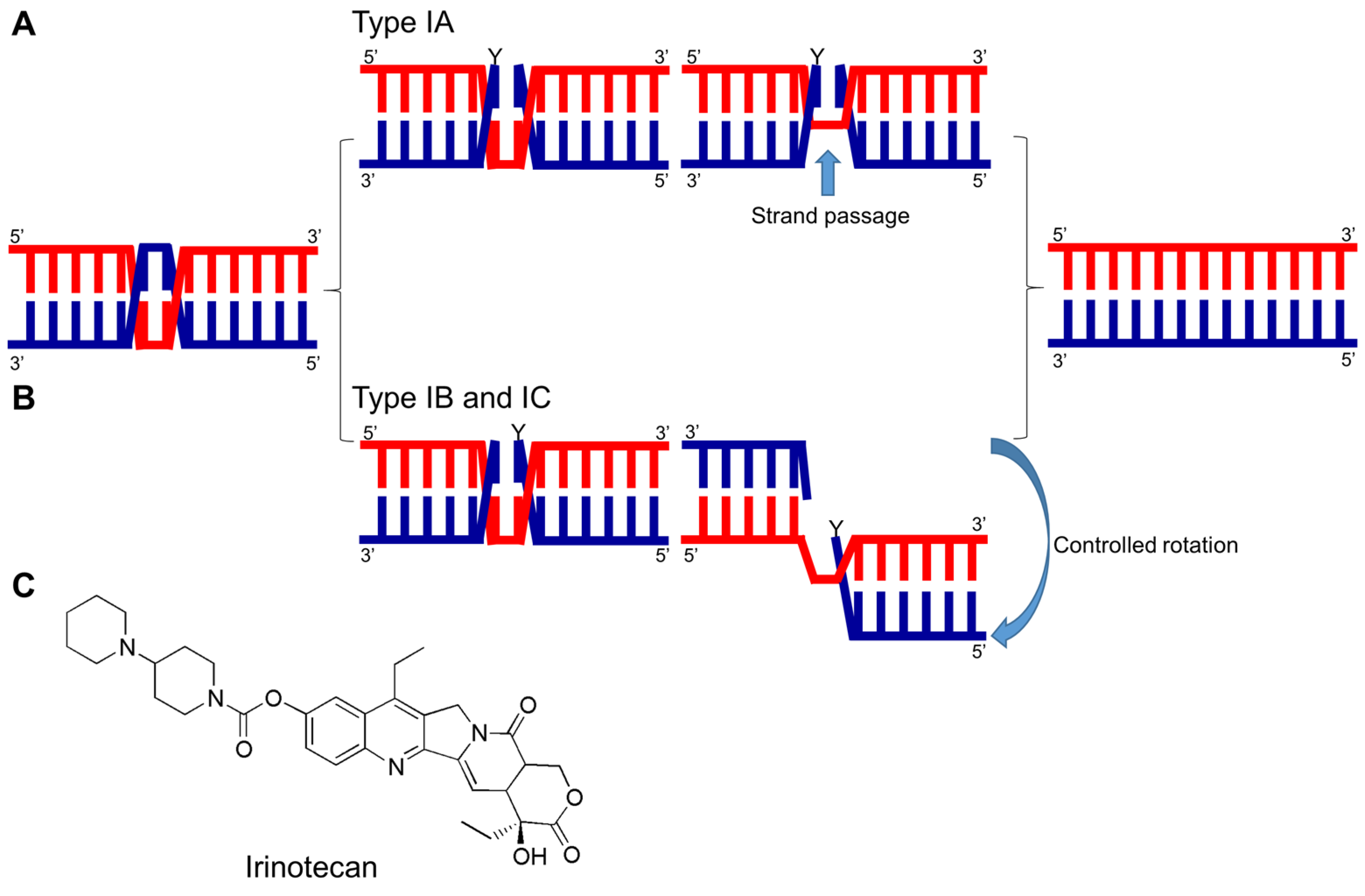
3.1. TOPO I Mechanism and Inhibitors
3.2. Irinotecan Combination Therapy
3.3. Clinical Status of Irinotecan Combination Therapy in CRC
4. TOPO II Inhibitors
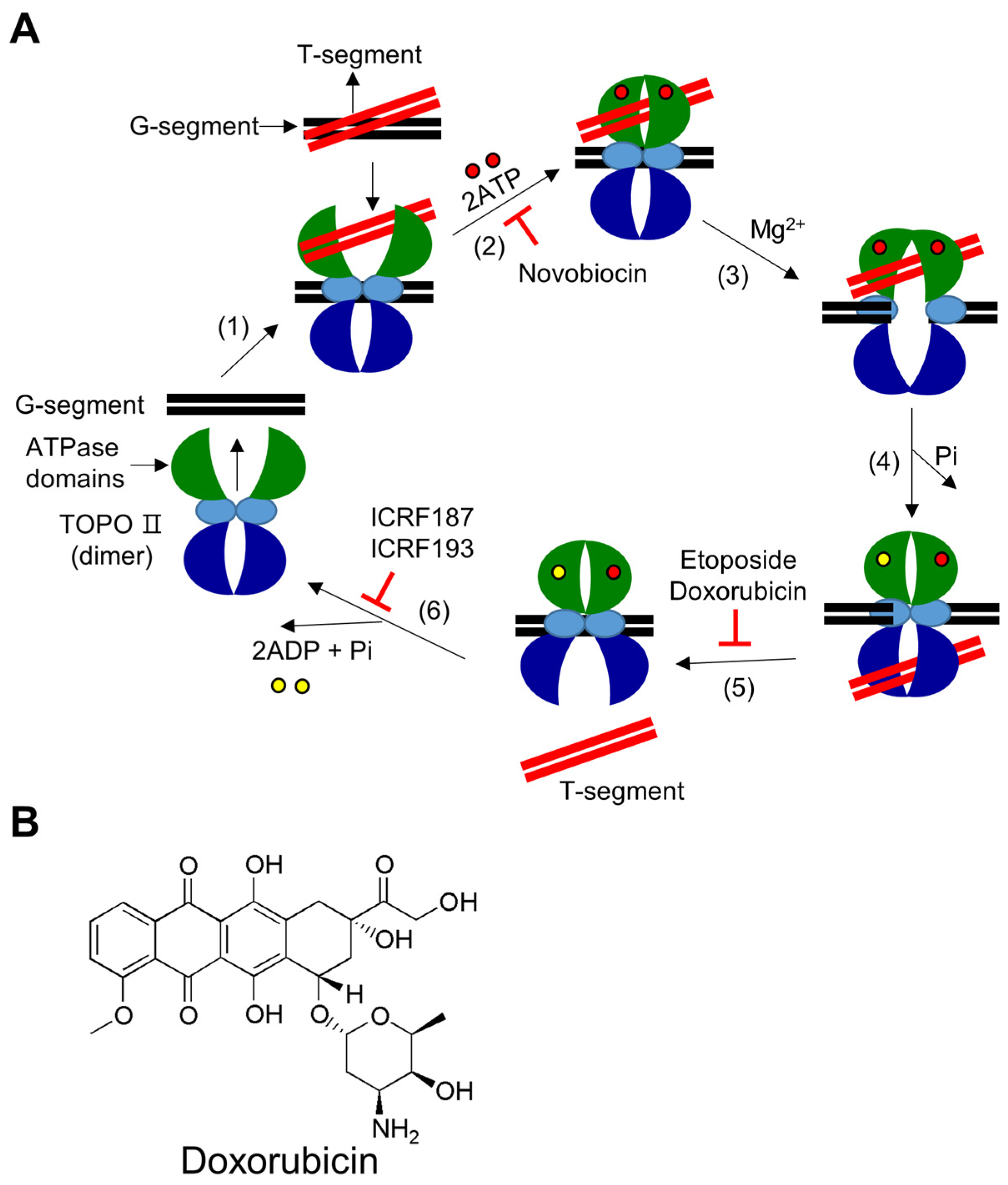
4.1. TOPO II Mechanism and Inhibitors
4.2. Doxorubicin Combination Therapy
4.3. Clinical Status of Doxorubicin Combination Therapy in Breast Cancer
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Liang, X.; Wu, Q.; Luan, S.; Yin, Z.; He, C.; Yin, L.; Zou, Y.; Yuan, Z.; Li, L.; Song, X.; et al. A comprehensive review of topoisomerase inhibitors as anticancer agents in the past decade. Eur. J. Med. Chem. 2019, 171, 129–168. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Singh, V.; Afshan, T.; Tyagi, P.; Varadwaj, P.K.; Sahoo, A.K. Recent development of multi-targeted inhibitors of human topoisomerase II enzyme as potent cancer therapeutics. Int. J. Biol. Macromol. 2023, 226, 473–484. [Google Scholar] [CrossRef] [PubMed]
- Greco, G.; Pellicioni, V.; Cruz-Chamorro, I.; Attisani, G.; Stefanelli, C.; Fimognari, C. Marine-derived compounds targeting topoisomerase II in cancer cells: A review. Mar. Drugs 2022, 20, 674. [Google Scholar] [CrossRef]
- Buzun, K.; Bielawska, A.; Bielawski, K.; Gornowicz, A. DNA topoisomerases as molecular targets for anticancer drugs. J. Enzym. Inhib. Med. Chem. 2020, 35, 1781–1799. [Google Scholar] [CrossRef]
- Bansal, S.; Bajaj, P.; Pandey, S.; Tandon, V. Topoisomerases: Resistance versus sensitivity, how far we can go? Med. Res. Rev. 2017, 37, 404–438. [Google Scholar] [CrossRef] [PubMed]
- Matias-Barrios, V.M.; Dong, X. The implication of topoisomerase II inhibitors in synthetic lethality for cancer therapy. Pharmaceuticals 2023, 16, 94. [Google Scholar] [CrossRef]
- Delgado, J.L.; Hsieh, C.M.; Chan, N.L.; Hiasa, H. Topoisomerases as anticancer targets. Biochem. J. 2018, 475, 373–398. [Google Scholar] [CrossRef]
- Cuya, S.M.; Bjornsti, M.A.; van Waardenburg, R. DNA topoisomerase-targeting chemotherapeutics: What’s new? Cancer Chemother. Pharmacol. 2017, 80, 1–14. [Google Scholar] [CrossRef]
- Wang, W.; Tse-Dinh, Y.C. Recent advances in use of topoisomerase inhibitors in combination cancer therapy. Curr. Top. Med. Chem. 2019, 19, 730–740. [Google Scholar] [CrossRef]
- Bjornsti, M.A.; Kaufmann, S.H. Topoisomerases and cancer chemotherapy: Recent advances and unanswered questions. F1000Research 2019, 8, F10000. [Google Scholar] [CrossRef]
- Hevener, K.; Verstak, T.A.; Lutat, K.E.; Riggsbee, D.L.; Mooney, J.W. Recent developments in topoisomerase-targeted cancer chemotherapy. Acta Pharm. Sin. B 2018, 8, 844–861. [Google Scholar] [CrossRef]
- Felix, C.A. Secondary leukemias induced by topoisomerase-targeted drugs. Biochim. Biophys. Acta 1998, 1400, 233–255. [Google Scholar] [CrossRef] [PubMed]
- Mistry, A.R.; Felix, C.A.; Whitmarsh, R.J.; Mason, A.; Reiter, A.; Cassinat, B.; Parry, A.; Walz, C.; Wiemels, J.L.; Segal, M.R.; et al. DNA topoisomerase II in therapy-related acute promyelocytic leukemia. N. Engl. J. Med. 2005, 352, 1529–1538. [Google Scholar] [CrossRef] [PubMed]
- Azarova, A.M.; Lyu, Y.L.; Lin, C.P.; Tsai, Y.C.; Lau, J.Y.; Wang, J.C.; Liu, L.F. Roles of DNA topoisomerase II isozymes in chemotherapy and secondary malignancies. Proc. Natl. Acad. Sci. USA 2007, 104, 11014–11019. [Google Scholar] [CrossRef] [PubMed]
- Bayat Mokhtari, R.; Homayouni, T.S.; Baluch, N.; Morgatskaya, E.; Kumar, S.; Das, B.; Yeger, H. Combination therapy in combating cancer. Oncotarget 2017, 8, 38022–38043. [Google Scholar] [CrossRef] [PubMed]
- Nozhat, Z.; Heydarzadeh, S.; Memariani, Z.; Ahmadi, A. Chemoprotective and chemosensitizing effects of apigenin on cancer therapy. Cancer Cell Int. 2021, 21, 574. [Google Scholar] [CrossRef] [PubMed]
- Redondo-Blanco, S.; Fernández, J.; Gutiérrez-Del-Río, I.; Villar, C.J.; Lombó, F. New insights toward colorectal cancer chemotherapy using natural bioactive compounds. Front. Pharmacol. 2017, 8, 109. [Google Scholar] [CrossRef]
- You, F.; Gao, C. Topoisomerase inhibitors and targeted delivery in cancer therapy. Curr. Top. Med. Chem. 2019, 19, 713–729. [Google Scholar] [CrossRef]
- Jain, C.K.; Majumder, H.K.; Roychoudhury, S. Natural compounds as anticancer agents targeting DNA topoisomerases. Curr. Genom. 2017, 18, 75–92. [Google Scholar] [CrossRef]
- Baker, N.M.; Rajan, R.; Mondragón, A. Structural studies of type I topoisomerases. Nucleic Acids Res. 2009, 37, 693–701. [Google Scholar] [CrossRef]
- Talukdar, A.; Kundu, B.; Sarkar, D.; Goon, S.; Mondal, M.A. Topoisomerase I inhibitors: Challenges, progress and the road ahead. Eur. J. Med. Chem. 2022, 236, 114304. [Google Scholar] [CrossRef] [PubMed]
- Capranico, G.; Marinello, J.; Chillemi, G. Type I DNA topoisomerases. J. Med. Chem. 2017, 60, 2169–2192. [Google Scholar] [CrossRef] [PubMed]
- Wall, M.E.; Wani, M.C.; Cook, C.A.; Palmer, K.H.; McPhail, A.T.; Sim, G.A. Plant antitumor agents. I. The isolation and structure of camptothecin, a novel alkaloidal leukemia and tumor inhibitor from camptotheca acuminata. J. Am. Chem. Soc. 1966, 88, 3888–3890. [Google Scholar] [CrossRef]
- Kciuk, M.; Marciniak, B.; Kontek, R. Irinotecan-still an important player in cancer chemotherapy: A comprehensive overview. Int. J. Mol. Sci. 2020, 21, 4919. [Google Scholar] [CrossRef] [PubMed]
- Fujita, K.; Kubota, Y.; Ishida, H.; Sasaki, Y. Irinotecan, a key chemotherapeutic drug for metastatic colorectal cancer. World J. Gastroenterol. 2015, 21, 12234–12248. [Google Scholar] [CrossRef]
- Bailly, C. Irinotecan: 25 years of cancer treatment. Pharmacol. Res. 2019, 148, 104398. [Google Scholar] [CrossRef]
- Capecitabine and Irinotecan in Treating Patients with Locally Advanced, Recurrent, or Metastatic Colorectal Cancer. 2004. Available online: https://ClinicalTrials.gov/show/NCT00022698 (accessed on 17 March 2023).
- Meropol, N.J.; Gold, P.J.; Diasio, R.B.; Andria, M.; Dhami, M.; Godfrey, T.; Kovatich, A.J.; Lund, K.A.; Mitchell, E.; Schwarting, R. Thymidine phosphorylase expression is associated with response to capecitabine plus irinotecan in patients with metastatic colorectal cancer. J. Clin. Oncol. 2006, 24, 4069–4077. [Google Scholar] [CrossRef]
- Carlini, L.E.; Meropol, N.J.; Bever, J.; Andria, M.L.; Hill, T.; Gold, P.; Rogatko, A.; Wang, H.; Blanchard, R.L. UGT1A7 and UGT1A9 polymorphisms predict response and toxicity in colorectal cancer patients treated with capecitabine/irinotecan. Clin. Cancer Res. 2005, 11, 1226–1236. [Google Scholar] [CrossRef]
- Research Study of IV Vitamin C in Combination with Irinotecan vs. Irinotecan Alone for Advanced Colorectal Cancer. 2015. Available online: https://ClinicalTrials.gov/show/NCT01550510 (accessed on 17 March 2023).
- A Study of the Combination of Pemetrexed and Irinotecan Every Two Weeks in Metastatic Colorectal Cancer. 2007. Available online: https://ClinicalTrials.gov/show/NCT00191984 (accessed on 17 March 2023).
- Louvet, C.; André, T.; Gamelin, E.; Hebbar, M.; Mabro, M.; Bennamoun, M.; Rassam, H.; de Gramont, A. Phase II study of biweekly pemetrexed plus irinotecan as second-line therapy for metastatic colorectal cancer. J. Oncol. 2010, 2010, 785934. [Google Scholar] [CrossRef]
- ISIS 183750 with Irinotecan for Advanced Solid Tumors or Colorectal Cancer. 2014. Available online: https://ClinicalTrials.gov/show/NCT01675128 (accessed on 17 March 2023).
- Duffy, A.G.; Makarova-Rusher, O.V.; Ulahannan, S.V.; Rahma, O.E.; Fioravanti, S.; Walker, M.; Abdullah, S.; Raffeld, M.; Anderson, V.; Abi-Jaoudeh, N.; et al. Modulation of tumor eIF4E by antisense inhibition: A phase I/II translational clinical trial of ISIS 183750-an antisense oligonucleotide against eIF4E-in combination with irinotecan in solid tumors and irinotecan-refractory colorectal cancer. Int. J. Cancer 2016, 139, 1648–1657. [Google Scholar] [CrossRef] [PubMed]
- Makarova-Rusher, O.V.; Duffy, A.G.; Ulahannan, S.V.; Fioravanti, S.; Walker, M.; Raffeld, M.; Compton, K.; Lee, S.; Tomita, Y.; Trepel, J.B. Phase I/II study of ISIS 183750 in combination with irinotecan for advanced solid tumors or colorectal cancer: Final results. J. Clin. Oncol. 2015, 33, 639. [Google Scholar] [CrossRef]
- A Safety Study of MM-121 with Cetuximab and Irinotecan in Patients with Advanced Cancers. 2013. Available online: https://ClinicalTrials.gov/show/NCT01451632 (accessed on 17 March 2023).
- Cleary, J.M.; McRee, A.J.; O’Neil, B.H.; Sharma, S.; Pearlberg, J.; Manoli, S.; Kubasek, W.L.; Korn, W.M. A phase 1 study of MM-121 (a fully human monoclonal antibody targeting the epidermal growth factor receptor family member ErbB3) in combination with cetuximab and irinotecan in patients with advanced cancers. J. Clin. Oncol. 2014, 32, 3076. [Google Scholar] [CrossRef]
- Phase II Trial of Combination Therapy with Irinotecan, S-1, and Bevacizumab (IRIS/Bev) in Patients with Unresectable or Recurrent Colorectal Cancer. 2010. Available online: https://ClinicalTrials.gov/show/NCT00569790 (accessed on 17 March 2023).
- Komatsu, Y.; Yuki, S.; Sogabe, S.; Fukushima, H.; Nakatsumi, H.; Kobayashi, Y.; Iwanaga, I.; Nakamura, M.; Hatanaka, K.; Miyagishima, T.; et al. Phase II study of combined chemotherapy with irinotecan and S-1 (IRIS) plus bevacizumab in patients with inoperable recurrent or advanced colorectal cancer. Acta Oncol. 2012, 51, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Arq 197 in Combination With Chemotherapy in Patients with Metastatic Colorectal Cancer. 2012. Available online: https://ClinicalTrials.gov/show/NCT01075048 (accessed on 17 March 2023).
- Eng, C.; Hart, L.L.; Severtsev, A.; Gladkov, O.; Mueller, L.; Kopp, M.V.; Vladimirov, V.I.; Langdon, R.M.; Kotiv, B.; Barni, S.; et al. A randomized, placebo-controlled, phase I/II study of tivantinib (ARQ 197) in combination with cetuximab and irinotecan in patients (pts) with KRAS wild-type (WT) metastatic colorectal cancer (CRC) who had received previous front-line systemic therapy. J. Clin. Oncol. 2013, 31, 3508. [Google Scholar] [CrossRef]
- Phase I/II Study of SGI-110 with Irinotecan Versus Regorafenib or TAS-102 in Metastatic Colorectal Cancer. 2019. Available online: https://ClinicalTrials.gov/show/NCT01896856 (accessed on 17 March 2023).
- Sharma, A.; Vatapalli, R.; Abdelfatah, E.; Wyatt McMahon, K.; Kerner, Z.; Guzzetta, A.; Singh, J.; Zahnow, C.; Baylin, S.B.; Yerram, S.; et al. Hypomethylating agents synergize with irinotecan to improve response to chemotherapy in colorectal cancer cells. PLoS ONE 2017, 12, e0176139. [Google Scholar] [CrossRef]
- Cetuximab Combined with Irinotecan in First-Line Therapy for Metastatic Colorectal Cancer (CRYSTAL). 2006. Available online: https://ClinicalTrials.gov/show/NCT00154102 (accessed on 17 March 2023).
- Van Cutsem, E.; Köhne, C.H.; Hitre, E.; Zaluski, J.; Chang Chien, C.R.; Makhson, A.; D’Haens, G.; Pintér, T.; Lim, R.; Bodoky, G.; et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N. Engl. J. Med. 2009, 360, 1408–1417. [Google Scholar] [CrossRef]
- Cutsem, E.V.; Köhne, C.-H.; Láng, I.; Folprecht, G.; Nowacki, M.P.; Cascinu, S.; Shchepotin, I.; Maurel, J.; Cunningham, D.; Tejpar, S.; et al. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: Updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J. Clin. Oncol. 2011, 29, 2011–2019. [Google Scholar] [CrossRef]
- Tejpar, S.; Stintzing, S.; Ciardiello, F.; Tabernero, J.; Van Cutsem, E.; Beier, F.; Esser, R.; Lenz, H.J.; Heinemann, V. Prognostic and predictive relevance of primary tumor location in patients with RAS wild-type metastatic colorectal cancer: Retrospective analyses of the CRYSTAL and FIRE-3 trials. JAMA Oncol. 2017, 3, 194–201. [Google Scholar] [CrossRef]
- Licitra, L.; Störkel, S.; Kerr, K.M.; Van Cutsem, E.; Pirker, R.; Hirsch, F.R.; Vermorken, J.B.; von Heydebreck, A.; Esser, R.; Celik, I.; et al. Predictive value of epidermal growth factor receptor expression for first-line chemotherapy plus cetuximab in patients with head and neck and colorectal cancer: Analysis of data from the EXTREME and CRYSTAL studies. Eur. J. Cancer 2013, 49, 1161–1168. [Google Scholar] [CrossRef]
- Regorafenib+FOLFIRI Versus Placebo+FOLFIRI as 2nd Line Tx in Metastatic Colorectal Cancer. 2016. Available online: https://ClinicalTrials.gov/show/NCT01298570 (accessed on 17 March 2023).
- Quintanilha, J.C.F.; Geyer, S.; Etheridge, A.S.; Racioppi, A.; Hammond, K.; Crona, D.J.; Peña, C.E.; Jacobson, S.B.; Marmorino, F.; Rossini, D.; et al. KDR genetic predictor of toxicities induced by sorafenib and regorafenib. Pharm. J. 2022, 22, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Schultheis, B.; Folprecht, G.; Kuhlmann, J.; Ehrenberg, R.; Hacker, U.T.; Köhne, C.H.; Kornacker, M.; Boix, O.; Lettieri, J.; Krauss, J.; et al. Regorafenib in combination with FOLFOX or FOLFIRI as first- or second-line treatment of colorectal cancer: Results of a multicenter, phase Ib study. Ann. Oncol. 2013, 24, 1560–1567. [Google Scholar] [CrossRef] [PubMed]
- A Study of ABT-165 plus FOLFIRI vs. Bevacizumab plus FOLFIRI in Subjects with Metastatic Colorectal Cancer Previously Treated with Fluoropyrimidine, Oxaliplatin and Bevacizumab. 2019. Available online: https://ClinicalTrials.gov/show/NCT03368859 (accessed on 17 March 2023).
- Strickler, J.H.; Cubillo, A.; Liang, J.T.; Matrana, M.; Kozloff, M.; Lowe, T.; Blaney, M.; Sahtout, M.; Naumovski, L.; Wainberg, Z.A. Efficacy and safety of dilpacimab (ABT-165) versus bevacizumab plus FOLFIRI in metastatic colorectal cancer: A phase II study. Future Oncol. 2022, 18, 3011–3020. [Google Scholar] [CrossRef] [PubMed]
- Study of Encorafenib + Cetuximab plus or Minus Binimetinib vs. Irinotecan/Cetuximab or Infusional 5-Fluorouracil (5-FU)/Folinic Acid (FA)/Irinotecan (FOLFIRI)/Cetuximab with a Safety Lead-in of Encorafenib + Binimetinib + Cetuximab in Patients with BRAF V600E-Mutant Metastatic Colorectal Cancer. 2019. Available online: https://ClinicalTrials.gov/show/NCT02928224 (accessed on 17 March 2023).
- Stintzing, S.; Seufferlein, T.; Rosé, C.; Reichenbach, F.; Lüftner, D. Encorafenib in combination with cetuximab after systemic therapy in patients with BRAF(V600E) mutant metastatic colorectal cancer: German health technology assessment-driven analyses from the BEACON CRC study. Clin. Color. Cancer 2022, 21, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Kopetz, S.; Grothey, A.; Van Cutsem, E.; Yaeger, R.; Wasan, H.; Yoshino, T.; Desai, J.; Ciardiello, F.; Loupakis, F.; Hong, Y.S.; et al. Quality of life with encorafenib plus cetuximab with or without binimetinib treatment in patients with BRAF V600E-mutant metastatic colorectal cancer: Patient-reported outcomes from BEACON CRC. ESMO Open 2022, 7, 100477. [Google Scholar] [CrossRef]
- Tabernero, J.; Grothey, A.; Van Cutsem, E.; Yaeger, R.; Wasan, H.; Yoshino, T.; Desai, J.; Ciardiello, F.; Loupakis, F.; Hong, Y.S.; et al. Encorafenib plus cetuximab as a new standard of care for previously treated BRAF V600E-mutant metastatic colorectal cancer: Updated survival results and subgroup analyses from the BEACON study. J. Clin. Oncol. 2021, 39, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Kopetz, S.; Grothey, A.; Yaeger, R.; Van Cutsem, E.; Desai, J.; Yoshino, T.; Wasan, H.; Ciardiello, F.; Loupakis, F.; Hong, Y.S.; et al. Encorafenib, binimetinib, and cetuximab in BRAF V600E-mutated colorectal cancer. N. Engl. J. Med. 2019, 381, 1632–1643. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Huijberts, S.; Grothey, A.; Yaeger, R.; Cuyle, P.J.; Elez, E.; Fakih, M.; Montagut, C.; Peeters, M.; Yoshino, T.; et al. Binimetinib, encorafenib, and cetuximab triplet therapy for patients with BRAF V600E-mutant metastatic colorectal cancer: Safety lead-in results from the phase III BEACON colorectal cancer study. J. Clin. Oncol. 2019, 37, 1460–1469. [Google Scholar] [CrossRef]
- A Study of Napabucasin (BBI-608) in Combination with FOLFIRI in Adult Patients with Previously Treated Metastatic Colorectal Cancer. 2020. Available online: https://ClinicalTrials.gov/show/NCT02753127 (accessed on 17 March 2023).
- FOLFIRI and Panitumumab in Treating Patients with RAS and BRAF Wild-Type Metastatic Colorectal Cancer. 2017. Available online: https://ClinicalTrials.gov/show/NCT02508077 (accessed on 17 March 2023).
- A Study in Second Line Metastatic Colorectal Cancer. 2014. Available online: https://ClinicalTrials.gov/show/NCT01183780 (accessed on 17 March 2023).
- Tabernero, J.; Yoshino, T.; Cohn, A.L.; Obermannova, R.; Bodoky, G.; Garcia-Carbonero, R.; Ciuleanu, T.E.; Portnoy, D.C.; Van Cutsem, E.; Grothey, A.; et al. Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine (RAISE): A randomised, double-blind, multicentre, phase 3 study. Lancet Oncol. 2015, 16, 499–508. [Google Scholar] [CrossRef]
- Obermannová, R.; Van Cutsem, E.; Yoshino, T.; Bodoky, G.; Prausová, J.; Garcia-Carbonero, R.; Ciuleanu, T.; Garcia Alfonso, P.; Portnoy, D.; Cohn, A.; et al. Subgroup analysis in RAISE: A randomized, double-blind phase III study of irinotecan, folinic acid, and 5-fluorouracil (FOLFIRI) plus ramucirumab or placebo in patients with metastatic colorectal carcinoma progression. Ann. Oncol. 2016, 27, 2082–2090. [Google Scholar] [CrossRef]
- Tabernero, J.; Hozak, R.R.; Yoshino, T.; Cohn, A.L.; Obermannova, R.; Bodoky, G.; Garcia-Carbonero, R.; Ciuleanu, T.E.; Portnoy, D.C.; Prausová, J.; et al. Analysis of angiogenesis biomarkers for ramucirumab efficacy in patients with metastatic colorectal cancer from RAISE, a global, randomized, double-blind, phase III study. Ann. Oncol. 2018, 29, 602–609. [Google Scholar] [CrossRef]
- Grothey, A.; Yoshino, T.; Bodoky, G.; Ciuleanu, T.; Garcia-Carbonero, R.; García-Alfonso, P.; Van Cutsem, E.; Muro, K.; Mytelka, D.S.; Li, L.; et al. Association of baseline absolute neutrophil counts and survival in patients with metastatic colorectal cancer treated with second-line antiangiogenic therapies: Exploratory analyses of the RAISE trial and validation in an electronic medical record data set. ESMO Open 2018, 3, e000347. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, T.; Portnoy, D.C.; Obermannová, R.; Bodoky, G.; Prausová, J.; Garcia-Carbonero, R.; Ciuleanu, T.; García-Alfonso, P.; Cohn, A.L.; Van Cutsem, E.; et al. Biomarker analysis beyond angiogenesis: RAS/RAF mutation status, tumour sidedness, and second-line ramucirumab efficacy in patients with metastatic colorectal carcinoma from RAISE-a global phase III study. Ann. Oncol. 2019, 30, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.H.; Hopkins, A.M.; Rowland, A.; Yuen, H.Y.; Karapetis, C.S.; Sorich, M.J. Effect of early adverse events on survival outcomes of patients with metastatic colorectal cancer treated with ramucirumab. Target. Oncol. 2019, 14, 743–748. [Google Scholar] [CrossRef]
- Taniguchi, H.; Yoshino, T.; Yamaguchi, K.; Yamazaki, K.; Nixon, A.B.; Tabernero, J.; Van Cutsem, E.; Robling, K.R.; Abada, P.B.; Hozak, R.R.; et al. Clinical development and evaluation of a VEGF-D assay in plasma from patients with metastatic colorectal cancer in the RAISE study. Curr. Med. Res. Opin. 2021, 37, 1769–1778. [Google Scholar] [CrossRef] [PubMed]
- Sequential and Concurrent FOLFOXIRI/Bevacizumab Regimens versus FOLFOX/Bevacizumab in First-Line Metastatic Colorectal Cancer. 2016. Available online: https://ClinicalTrials.gov/show/NCT01765582 (accessed on 17 March 2023).
- Cremolini, C.; Antoniotti, C.; Stein, A.; Bendell, J.; Gruenberger, T.; Rossini, D.; Masi, G.; Ongaro, E.; Hurwitz, H.; Falcone, A.; et al. Individual patient data meta-analysis of FOLFOXIRI plus bevacizumab versus doublets plus bevacizumab as initial therapy of unresectable metastatic colorectal cancer. J. Clin. Oncol. 2020, 38, 3314–3324. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, H.I.; Tan, B.R.; Reeves, J.A.; Xiong, H.; Somer, B.; Lenz, H.J.; Hochster, H.S.; Scappaticci, F.; Palma, J.F.; Price, R.; et al. Phase II randomized trial of sequential or concurrent FOLFOXIRI-bevacizumab versus FOLFOX-bevacizumab for metastatic colorectal cancer (STEAM). Oncologist 2019, 24, 921–932. [Google Scholar] [CrossRef] [PubMed]
- FOLFOXIRI plus Panitumumab Patients with Metastatic KRAS Wild-Type Colorectal Cancer with Liver Metastases Only. 2014. Available online: https://ClinicalTrials.gov/show/NCT01226719 (accessed on 17 March 2023).
- Bendell, J.C.; Zakari, A.; Peyton, J.D.; Boccia, R.; Moskowitz, M.; Gian, V.; Lipman, A.; Waterhouse, D.; LoCicero, R.; Earwood, C.; et al. A phase II study of FOLFOXIRI plus panitumumab followed by evaluation for resection in patients with metastatic KRAS wild-type colorectal cancer with liver metastases only. Oncologist 2016, 21, 279–280. [Google Scholar] [CrossRef]
- Kang, Y.J.; Jang, J.Y.; Kwon, Y.H.; Lee, J.H.; Lee, S.; Park, Y.; Jung, Y.S.; Im, E.; Moon, H.R.; Chung, H.Y.; et al. MHY2245, a sirtuin inhibitor, induces cell cycle arrest and apoptosis in HCT116 human colorectal cancer cells. Int. J. Mol. Sci. 2022, 23, 1590. [Google Scholar] [CrossRef]
- Choi, Y.J.; Choi, C.Y.; Rhie, S.J.; Shin, S. Safety assessment on serious adverse events of targeted therapeutic agents prescribed for RAS wild-type metastatic colorectal cancer: Systematic review and network meta-analysis. Int. J. Environ. Res. Public Health 2022, 19, 9196. [Google Scholar] [CrossRef]
- Ridouane, Y.; Lopes, G.; Ku, G.; Masud, H.; Haaland, B. Targeted first-line therapies for advanced colorectal cancer: A Bayesian meta-analysis. Oncotarget 2017, 8, 66458–66466. [Google Scholar] [CrossRef] [PubMed]
- Turkes, F.; Chau, I. Ramucirumab and its use in the treatment of hepatocellular carcinoma. Future Oncol. 2019, 15, 979–988. [Google Scholar] [CrossRef]
- Dolatkhah, R.; Dastgiri, S.; Eftekhar Sadat, A.T.; Farassati, F.; Nezamdoust, M.; Somi, M.H. Impact of RAS/RAF mutations on clinical and prognostic outcomes in metastatic colorectal cancer. Bioimpacts 2021, 11, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Okoro, C.O.; Fatoki, T.H. A mini review of novel topoisomerase II inhibitors as future anticancer agents. Int. J. Mol. Sci. 2023, 24, 2532. [Google Scholar] [CrossRef]
- Lee, J.H.; Berger, J.M. Cell Cycle-Dependent Control and Roles of DNA Topoisomerase II. Genes 2019, 10, 859. [Google Scholar] [CrossRef]
- Matias-Barrios, V.M.; Radaeva, M.; Song, Y.; Alperstein, Z.; Lee, A.R.; Schmitt, V.; Lee, J.; Ban, F.; Xie, N.; Qi, J.; et al. Discovery of new catalytic topoisomerase II inhibitors for anticancer therapeutics. Front. Oncol. 2021, 10, 633142. [Google Scholar] [CrossRef] [PubMed]
- Vann, K.R.; Oviatt, A.A.; Osheroff, N. Topoisomerase II poisons: Converting essential enzymes into molecular scissors. Biochemistry 2021, 60, 1630–1641. [Google Scholar] [CrossRef]
- Can, M.M.; Shawuti, S.; Kalindemirtas, F.D.; Erdemir, G.; Kuruca, D.S.; Kaneko, S.; Aktas, Z.; Oncul, O. Anticancer drug doxorubicin (DOX) loading performance of functionalized polyaniline (PANI) surface with active carbon. J. Mater. Sci. 2023, 58, 4726–4738. [Google Scholar] [CrossRef]
- Roychoudhury, S.; Kumar, A.; Bhatkar, D.; Sharma, N.K. Molecular avenues in targeted doxorubicin cancer therapy. Future Oncol. 2020, 16, 687–700. [Google Scholar] [CrossRef]
- Argenziano, M.; Gigliotti, C.L.; Clemente, N.; Boggio, E.; Ferrara, B.; Trotta, F.; Pizzimenti, S.; Barrera, G.; Boldorini, R.; Bessone, F.; et al. Improvement in the anti-tumor efficacy of doxorubicin nanosponges in in vitro and in mice bearing breast tumor models. Cancers 2020, 12, 162. [Google Scholar] [CrossRef]
- Tran, Q.H.; Hoang, D.H.; Song, M.; Choe, W.; Kang, I.; Kim, S.S.; Ha, J. Melatonin and doxorubicin synergistically enhance apoptosis via autophagy-dependent reduction of AMPKα1 transcription in human breast cancer cells. Exp. Mol. Med. 2021, 53, 1413–1422. [Google Scholar] [CrossRef] [PubMed]
- Baxi, S.M.; Beall, R.; Yang, J.; Mackey, T.K. A multidisciplinary review of the policy, intellectual property rights, and international trade environment for access and affordability to essential cancer medications. Global. Health 2019, 15, 57. [Google Scholar] [CrossRef] [PubMed]
- Rawat, P.S.; Jaiswal, A.; Khurana, A.; Bhatti, J.S.; Navik, U. Doxorubicin-induced cardiotoxicity: An update on the molecular mechanism and novel therapeutic strategies for effective management. Biomed. Pharmacother. 2021, 139, 111708. [Google Scholar] [CrossRef]
- Fujii, T.; Le Du, F.; Xiao, L.; Kogawa, T.; Barcenas, C.H.; Alvarez, R.H.; Valero, V.; Shen, Y.; Ueno, N.T. Effectiveness of an adjuvant chemotherapy regimen for early-stage breast cancer: A systematic review and network meta-analysis. JAMA Oncol. 2015, 1, 1311–1318. [Google Scholar] [CrossRef] [PubMed]
- López-Miranda, E.; Pérez-García, J.M.; Di Cosimo, S.; Brain, E.; Ravnik, M.; Escrivá-de-Romaní, S.; Vidal, M.; Gligorov, J.; Borštnar, S.; Calabuig, L.; et al. Trastuzumab emtansine plus non-pegylated liposomal doxorubicin in HER2-positive metastatic breast cancer (thelma): A single-arm, multicenter, phase Ib trial. Cancers 2020, 12, 3509. [Google Scholar] [CrossRef] [PubMed]
- Medina, E.A.G.; Caballero, B.B.; Miguel, K.L.; Gutiérrez, Z.A.; Fernández, B.M.; Tul, L.E.A.; Rodríguez, L.E.M.; Guerrero, O.V.; Varela, I.G.S.; Bernardo, M.C.C.; et al. Neoadjuvant trastuzumab and pertuzumab in combination with standard chemotherapy for HER2-positive early breast cancer: Real-world practice in Cuba. Cancer Treat. Res. Commun. 2023, 34, 100670. [Google Scholar] [CrossRef] [PubMed]
- Cisplatin vs. Doxorubicin/Cyclophosphamide in BrCa. 2019. Available online: https://ClinicalTrials.gov/show/NCT01670500 (accessed on 17 March 2023).
- Tung, N.; Arun, B.; Hacker, M.R.; Hofstatter, E.; Toppmeyer, D.L.; Isakoff, S.J.; Borges, V.; Legare, R.D.; Isaacs, C.; Wolff, A.C.; et al. TBCRC 031: Randomized phase II study of neoadjuvant cisplatin versus doxorubicin-cyclophosphamide in germline BRCA carriers with HER2-negative breast cancer (the INFORM trial). J. Clin. Oncol. 2020, 38, 1539–1548. [Google Scholar] [CrossRef]
- Tung, N.; Hacker, M.R.; Garber, J.E. Reply to S. Takamizawa et al. J. Clin. Oncol. 2020, 38, 2700–2701. [Google Scholar] [CrossRef]
- Takamizawa, S.; Ishiki, H.; Shimoi, T.; Shimizu, M.; Satomi, E. Neoadjuvant cisplatin in BRCA carriers with HER2-negative breast cancer. J. Clin. Oncol. 2020, 38, 2699–2700. [Google Scholar] [CrossRef]
- A Phase 2 Study of Eribulin Followed by AC as Preoperative Therapy for HER2-Negative Inflammatory Breast Cancer. 2021. Available online: https://ClinicalTrials.gov/show/NCT02623972 (accessed on 17 March 2023).
- Combination Chemotherapy and Bevacizumab in Treating Women with HER2/Neu-Negative Stage II or Stage III Breast Cancer. 2014. Available online: https://ClinicalTrials.gov/show/NCT00679029 (accessed on 17 March 2023).
- Tipifarnib and Combination Chemotherapy in Treating Patients with Stage II or Stage III Breast Cancer. 2013. Available online: https://ClinicalTrials.gov/show/NCT00470301 (accessed on 17 March 2023).
- Andreopoulou, E.; Vigoda, I.S.; Valero, V.; Hershman, D.L.; Raptis, G.; Vahdat, L.T.; Han, H.S.; Wright, J.J.; Pellegrino, C.M.; Cristofanilli, M.; et al. Phase I-II study of the farnesyl transferase inhibitor tipifarnib plus sequential weekly paclitaxel and doxorubicin-cyclophosphamide in HER2/neu-negative inflammatory carcinoma and non-inflammatory estrogen receptor-positive breast carcinoma. Breast Cancer Res. Treat. 2013, 141, 429–435. [Google Scholar] [CrossRef]
- Docetaxel in Breast Cancer. 2008. Available online: https://ClinicalTrials.gov/show/NCT00312208 (accessed on 17 March 2023).
- Mackey, J.R.; Pieńkowski, T.; Crown, J.; Sadeghi, S.; Martin, M.; Chan, A.; Saleh, M.; Sehdev, S.; Provencher, L.; Semiglazov, V.; et al. Long-term outcomes after adjuvant treatment of sequential versus combination docetaxel with doxorubicin and cyclophosphamide in node-positive breast cancer: BCIRG-005 randomized trial. Ann. Oncol. 2016, 27, 1041–1047. [Google Scholar] [CrossRef] [PubMed]
- Press, M.F.; Sauter, G.; Buyse, M.; Fourmanoir, H.; Quinaux, E.; Tsao-Wei, D.D.; Eiermann, W.; Robert, N.; Pienkowski, T.; Crown, J.; et al. HER2 gene amplification testing by fluorescent in situ hybridization (FISH): Comparison of the ASCO-college of American pathologists guidelines with FISH scores used for enrollment in breast cancer international research group clinical trials. J. Clin. Oncol. 2016, 34, 3518–3528. [Google Scholar] [CrossRef] [PubMed]
- A Randomized Trial of Ixempra versus Taxol in Adjuvant Therapy of Triple Negative Breast Cancer. 2015. Available online: https://ClinicalTrials.gov/show/NCT00789581 (accessed on 17 March 2023).
- Yardley, D.A.; Arrowsmith, E.R.; Daniel, B.R.; Eakle, J.; Brufsky, A.; Drosick, D.R.; Kudrik, F.; Bosserman, L.D.; Keaton, M.R.; Goble, S.A.; et al. TITAN: Phase III study of doxorubicin/cyclophosphamide followed by ixabepilone or paclitaxel in early-stage triple-negative breast cancer. Breast Cancer Res. Treat. 2017, 164, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Combination Chemotherapy with or Without Colony-Stimulating Factors in Treating Women with Breast Cancer. 2014. Available online: https://ClinicalTrials.gov/show/NCT00014222 (accessed on 17 March 2023).
- Combination Chemotherapy with or without Trastuzumab in Treating Women with Breast Cancer. 2014. Available online: https://ClinicalTrials.gov/show/NCT00021255 (accessed on 17 March 2023).
- Stern, H.M.; Gardner, H.; Burzykowski, T.; Elatre, W.; O’Brien, C.; Lackner, M.R.; Pestano, G.A.; Santiago, A.; Villalobos, I.; Eiermann, W.; et al. PTEN loss is associated with worse outcome in HER2-amplified breast cancer patients but is not associated with trastuzumab resistance. Clin. Cancer. Res. 2015, 21, 2065–2074. [Google Scholar] [CrossRef]
- Press, M.F.; Sauter, G.; Buyse, M.; Bernstein, L.; Guzman, R.; Santiago, A.; Villalobos, I.E.; Eiermann, W.; Pienkowski, T.; Martin, M.; et al. Alteration of topoisomerase II-alpha gene in human breast cancer: Association with responsiveness to anthracycline-based chemotherapy. J. Clin. Oncol. 2011, 29, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Perez, E.A.; Press, M.F.; Dueck, A.C.; Jenkins, R.B.; Kim, C.; Chen, B.; Villalobos, I.; Paik, S.; Buyse, M.; Wiktor, A.E.; et al. Immunohistochemistry and fluorescence in situ hybridization assessment of HER2 in clinical trials of adjuvant therapy for breast cancer (NCCTG N9831, BCIRG 006, and BCIRG 005). Breast Cancer Res. Treat. 2013, 138, 99–108. [Google Scholar] [CrossRef]
- Au, H.J.; Eiermann, W.; Robert, N.J.; Pienkowski, T.; Crown, J.; Martin, M.; Pawlicki, M.; Chan, A.; Mackey, J.; Glaspy, J.; et al. Health-related quality of life with adjuvant docetaxel- and trastuzumab-based regimens in patients with node-positive and high-risk node-negative, HER2-positive early breast cancer: Results from the BCIRG 006 Study. Oncologist 2013, 18, 812–818. [Google Scholar] [CrossRef]
- Slamon, D.; Eiermann, W.; Robert, N.; Pienkowski, T.; Martin, M.; Press, M.; Mackey, J.; Glaspy, J.; Chan, A.; Pawlicki, M.; et al. Adjuvant trastuzumab in HER2-positive breast cancer. N. Engl. J. Med. 2011, 365, 1273–1283. [Google Scholar] [CrossRef]
- Docetaxel in Node Positive Adjuvant Breast Cancer. 2010. Available online: https://ClinicalTrials.gov/show/NCT00688740 (accessed on 17 March 2023).
- Mackey, J.R.; Martin, M.; Pienkowski, T.; Rolski, J.; Guastalla, J.P.; Sami, A.; Glaspy, J.; Juhos, E.; Wardley, A.; Fornander, T.; et al. Adjuvant docetaxel, doxorubicin, and cyclophosphamide in node-positive breast cancer: 10-year follow-up of the phase 3 randomised BCIRG 001 trial. Lancet Oncol. 2013, 14, 72–80. [Google Scholar] [CrossRef]
- Martin, M.; Pienkowski, T.; Mackey, J.; Pawlicki, M.; Guastalla, J.P.; Weaver, C.; Tomiak, E.; Al-Tweigeri, T.; Chap, L.; Juhos, E.; et al. Adjuvant docetaxel for node-positive breast cancer. N. Engl. J. Med. 2005, 352, 2302–2313. [Google Scholar] [CrossRef]
- Neoadjuvant Study of Sequential Eribulin followed by FAC Compared to Sequential Paclitaxel followed by FEC in Early Stage Breast Cancer not Overexpressing HER-2. 2020. Available online: https://ClinicalTrials.gov/show/NCT01593020 (accessed on 17 March 2023).
- Lim, B.; Song, J.; Ibrahim, N.K.; Koenig, K.B.; Chavez-MacGregor, M.; Ensor, J.E., Jr.; Gomez, J.S.; Krishnamurthy, S.; Caudle, A.S.; Shaitelman, S.F.; et al. A randomized phase II study of sequential eribulin versus paclitaxel followed by FAC/FEC as neoadjuvant therapy in patients with operable HER2-negative breast cancer. Oncologist 2021, 26, e230–e240. [Google Scholar] [CrossRef] [PubMed]
- Comparison of Two Combination Chemotherapy Regimens in Treating Women with Breast Cancer. 2014. Available online: https://ClinicalTrials.gov/show/NCT00087178 (accessed on 17 March 2023).
- Taxotere and Adriamycin/Cytoxan (AC) Validation in Breast Cancer Patients. 2016. Available online: https://ClinicalTrials.gov/show/NCT00206518 (accessed on 17 March 2023).
- TAC Versus TC for Adjuvant Breast Cancer. 2015. Available online: https://ClinicalTrials.gov/show/NCT00493870 (accessed on 17 March 2023).
- Blum, J.L.; Flynn, P.J.; Yothers, G.; Asmar, L.; Geyer, C.E., Jr.; Jacobs, S.A.; Robert, N.J.; Hopkins, J.O.; O’Shaughnessy, J.A.; Dang, C.T.; et al. Anthracyclines in early breast cancer: The ABC trials-USOR 06-090, NSABP B-46-I/USOR 07132, and NSABP B-49 (NRG Oncology). J. Clin. Oncol. 2017, 35, 2647–2655. [Google Scholar] [CrossRef] [PubMed]
- Combination Chemotherapy in Treating Women Who Have Undergone Surgery for Node-Positive Breast Cancer. 2012. Available online: https://ClinicalTrials.gov/show/NCT00093795 (accessed on 17 March 2023).
- Swain, S.M.; Tang, G.; Geyer, C.E., Jr.; Rastogi, P.; Atkins, J.N.; Donnellan, P.P.; Fehrenbacher, L.; Azar, C.A.; Robidoux, A.; Polikoff, J.A.; et al. Definitive results of a phase III adjuvant trial comparing three chemotherapy regimens in women with operable, node-positive breast cancer: The NSABP B-38 trial. J. Clin. Oncol. 2013, 31, 3197–3204. [Google Scholar] [CrossRef] [PubMed]
- Safety and Efficacy of Trastuzumab as Part of Breast Cancer Treatment Regimen. 2021. Available online: https://ClinicalTrials.gov/show/NCT02419742 (accessed on 17 March 2023).
- A Study to Evaluate the Efficacy and Safety of Atezolizumab or Placebo in Combination with Neoadjuvant Doxorubicin + Cyclophosphamide followed by Paclitaxel + Trastuzumab + Pertuzumab in Early Her2-Positive Breast Cancer. 2021. Available online: https://ClinicalTrials.gov/show/NCT03726879 (accessed on 17 March 2023).
- Huober, J.; Barrios, C.H.; Niikura, N.; Jarząb, M.; Chang, Y.C.; Huggins-Puhalla, S.L.; Pedrini, J.; Zhukova, L.; Graupner, V.; Eiger, D.; et al. Atezolizumab with neoadjuvant anti-human epidermal growth factor receptor 2 therapy and chemotherapy in human epidermal growth factor receptor 2-positive early breast cancer: Primary results of the randomized phase III IMpassion050 trial. J. Clin. Oncol. 2022, 40, 2946–2956. [Google Scholar] [CrossRef] [PubMed]
- Waks, A.G.; Winer, E.P. Breast cancer treatment: A review. JAMA 2019, 321, 288–300. [Google Scholar] [CrossRef]
- Portnow, L.H.; Kochkodan-Self, J.M.; Maduram, A.; Barrios, M.; Onken, A.M.; Hong, X.; Mittendorf, E.A.; Giess, C.S.; Chikarmane, S.A. Multimodality imaging review of HER2-positive breast cancer and response to neoadjuvant chemotherapy. Radiographics 2023, 43, e220103. [Google Scholar] [CrossRef]
- Suppan, C.; Balic, M. Current standards and future outlooks in metastatic Her2-positive breast cancer. Breast Care 2023, 18, 69–75. [Google Scholar] [CrossRef]
- Vega Cano, K.S.; Marmolejo Castañeda, D.H.; Escrivá-de-Romaní, S.; Saura, C. Systemic therapy for HER2-positive metastatic breast cancer: Current and future trends. Cancers 2022, 15, 51. [Google Scholar] [CrossRef]
- Peliçário Vargas, B.; Sari, M.H.M.; Ferreira, L.M. Trastuzumab in breast cancer treatment: The era of biosimilars. Anticancer Agents Med. Chem. 2022, 22, 2507–2516. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Drugs | Target Cancer | Purpose of Study | Clinical Trials Status | Clinical Trials Identifier | Refs. |
|---|---|---|---|---|---|
| Capecitabine, Irinotecan | CRC | A study on the combined effect of capecitabine and irinotecan | Phase 2 | NCT00022698 | [28,29,30] |
| Ascorbic acid, Irinotecan | Stage IV CRC | Phase I/II study of ascorbic acid infusion versus irinotecan monotherapy combined with irinotecan treatment in patients with relapsed or advanced CRC who have failed at least one treatment regimen with a fluorouracil-based regimen | Phase 1 Phase 2 | NCT01550510 | [31] |
| Pemetrexed, Irinotecan | Metastatic CRC | To determine the efficacy and safety of the combination of pemetrexed and irinotecan | Phase 2 | NCT00191984 | [32,33] |
| ISIS 183750, Irinotecan | Colorectal neoplasms Colorectal carcinoma Colorectal tumors | Testing the safety and efficacy of irinotecan against ISIS 183750 and advanced solid or CRC | Phase 1 Phase 2 | NCT01675128 | [34,35,36] |
| MM-121, Irinotecan, Cetuximab | CRC | To evaluate the safety and tolerability of escalating doses of MM-121 + cetuximab and MM-121 + cetuximab + irinotecan combinations | Phase 1 | NCT01451632 | [37,38] |
| S-1, Irinotecan, Bevacizumab | CRC | To determine if it is safe to treat unresectable or recurrent colorectal cancer | Phase 2 | NCT00569790 | [39,40] |
| Tivantinib, Cetuximab, Irinotecan | Metastatic CRC | ARQ 197 or placebo plus irinotecan and cetuximab, defines the recommended dose for phase 2 | Phase 1 Phase 2 | NCT01075048 | [41,42] |
| Guadecitabine (SGI-110), Regorafenib, Lonsurf (TAS-102), Irinotecan | Previously treated metastatic CRC | Enrollment in phase 1 study of SGI-110 combined with irinotecan and after the MTD was determined, patients were enrolled in a 2:1 randomized phase 2 study of SGI-110 and irinotecan versus standard-of-care regorafenib or TAS-102 | Phase 1 Phase 2 | NCT01896856 | [43,44] |
| Cetuximab, FOLFIRI | EGFR expressing metastatic CRC | To investigate the effect of cetuximab in combination with chemotherapy (FOLFIRI) compared to the same chemotherapy for patient EGF receptors | Phase 3 | NCT00154102 | [45,46,47,48,49] |
| Regorafenib, FOLFIRI | CRC metastatic | Comparison of PFS between regorafenib + FOLFIRI chemotherapy and placebo + FOLFIR in mCRC patients previously treated with FOLFOX therapy | Phase 2 | NCT01298570 | [50,51,52] |
| ABT-165, Bevacizumab, FOLFIRI | Previously treated metastatic adenocarcinoma of the colon or rectum | Study evaluating efficacy and tolerability of ABT-165 + FOLFIRI compared to bevacizumab + FOLFIRI | Phase 2 | NCT03368859 | [53,54] |
| Encorafenib, Binimetinib, Cetuximab, FOLFIRI | BRAF V600E-mutant metastatic CRC | To evaluate encorafenib plus cetuximab plus or minus binimetinib versus choosing either irinotecan/cetuximab or FOLFIRI/cetuximab as control in patients with BRAFV600E mCRC | Phase 3 | NCT02928224 | [55,56,57,58,59,60] |
| Napabucasin, Bevacizumab, FOLFIRI | CRC | Trial of cancer stem cell pathway inhibitor napabucacin plus standard biweekly FOLFIRI versus standard biweekly FOLFIRI | Phase 3 | NCT02753127 | [61] |
| FOLFIRI, Panitumumab | Recurrent colorectal carcinoma Stage IVA CRC Stage IVB CRC | A study on how well FOLFIRI works in combination with panitumumab in the treatment of CRC patients | Phase 2 | NCT02508077 | [62] |
| Ramucirumab, FOLFIRI | CRC | Comparing overall survival of participants with metastatic CRC treated with ramucirumab plus FOLFIRI or placebo plus FOLFIRI | Phase 3 | NCT01183780 | [63,64,65,66,67,68,69,70] |
| Bevacizumab, FOLFOXIRI | Colorectal neoplasms | Efficacy and safety evaluation of FOLFOXIRI/bevacizumab regimen (concurrent and sequential) versus FOLFOX/bevacizumab | Phase 2 | NCT01765582 | [71,72,73] |
| Panitumumab, FOLFOXIRI | CRC | A plan to determine the ORR of the combination of FOLFOXIRI and panitumumab | Phase 2 | NCT01226719 | [74,75] |
| Drugs | Target Cancer | Purpose of Study | Clinical Trials Status | Clinical Trials Identifier | Refs. |
|---|---|---|---|---|---|
| Cisplatin, AC | Breast cancer | To evaluate cisplatin, a chemotherapy drug that has been shown to be active in the treatment of breast cancer and women with BRCA mutations | Phase 2 | NCT01670500 | [94,95,96,97] |
| Eribulin, AC | Inflammatory breast cancer HER2-negative carcinoma of breast | Studying a drug called eribulin combined with standard therapy as a possible preoperative treatment for HER2-negative inflammatory breast cancer | Phase 2 | NCT02623972 | [98] |
| Bevacizumab, Paclitaxel, Gemcitabine hydrochloride, Pegfilgrastim, AC | HER2-negative breast cancer Stage II breast cancer Stage IIIA breast cancer Stage IIIB breast cancer Stage IIIC breast cancer | To investigate the efficacy and side effects of adding bevacizumab to the chemotherapy regimen in the treatment of stage 2 or 3 HER2-neu negative breast cancer in women | Phase 2 | NCT00679029 | [99] |
| AC, Paclitaxel, Tipifarnib | Breast cancer Male breast cancer | To study the side effects and optimal dose of tipifarnib when given with combination chemotherapy and how effective it is in treating patients with stage 2 or 3 breast cancer | Phase 1 Phase 2 | NCT00470301 | [100,101] |
| AC-T (Docetaxel) | Breast cancer | Comparison of disease-free survival after TAC versus AC-T in HER2-neu negative breast cancer patients who are eligible for surgery | Phase 3 | NCT00312208 | [102,103,104] |
| AC-T (Paclitaxel), Ixabepilone | Breast cancer | Comparison of patients receiving AC and ixabepilone and patients receiving AC and weekly paclitaxel | Phase 3 | NCT00789581 | [105,106] |
| AC-T (Paclitaxel), Epoetin alfa, Filgrastim, Epirubicin hydrochloride, Fluorouracil | Breast cancer | Comparing the effectiveness of chemotherapy with or without epoetin alfa for the treatment of women who have undergone surgery for stage I, II, or III breast cancer | Phase 3 | NCT00014222 | [107] |
| AC-T (Docetaxel), Trastuzumab, Carboplatin | Breast neoplasms | Comparing the treatment outcomes of women with HER2-positive breast cancer who had positive lymph nodes or high-risk negative lymph nodes and were treated with adjuvant therapy including doxorubicin, cyclophosphamide, and docetaxel, with or without trastuzumab, versus those who received trastuzumab, docetaxel, and carboplatin | Phase 3 | NCT00021255 | [104,108,109,110,111,112,113] |
| FAC, Docetaxel | Breast cancer | Comparison of disease-free survival rates after TAC combination therapy and FAC combination therapy | Phase 3 | NCT00688740 | [114,115,116] |
| FAC, Paclitaxel, Eribulin, Epirubicin | Breast cancer | To find out if and how well eribulin given in combination with standard chemotherapy can treat early-stage breast cancer compared to paclitaxel given in combination with standard chemotherapy | Phase 2 | NCT01593020 | [117,118] |
| Doxorubicin, FEC | Breast cancer | Two combination chemotherapy regimens were studied to compare how effective they were in treating women who had surgery for breast cancer that had not spread to the lymph nodes | Phase 3 | NCT00087178 | [119] |
| TAC | Breast cancer | To see if we can find out if taxotere and/or adriamycin/cytoxan can make tumors smaller | Phase 2 | NCT00206518 | [120] |
| TAC | Breast cancer | To find out what effect (good or bad) TC or TAC has on early-stage HER2- breast cancer | Phase 3 | NCT00493870 | [121,122] |
| TAC, Paclitaxel, Gemcitabine | Breast cancer | Studying three different combination chemotherapy regimens and comparing how effective they are in treating women who have had surgery for node-positive breast cancer | Phase 3 | NCT00093795 | [123,124] |
| AC-TH, Carboplatin | Breast cancer | To evaluate the safety of trastuzumab for the treatment of HER2-positive nodule-positive or high-risk nodule-negative | Phase 4 | NCT02419742 | [125] |
| AC-THP, Atezolizumab, Trastuzumab emtansine | Breast cancer | To evaluate the efficacy and safety of atezolizumab compared with placebo when given in combination with neoadjuvant dose-dense doxorubicin + cyclophosphamide followed by paclitaxel + trastuzumab + pertuzumab in patients with early HER2-positive breast cancer | Phase 3 | NCT03726879 | [126,127] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, J.Y.; Kim, D.; Kim, N.D. Recent Developments in Combination Chemotherapy for Colorectal and Breast Cancers with Topoisomerase Inhibitors. Int. J. Mol. Sci. 2023, 24, 8457. https://doi.org/10.3390/ijms24098457
Jang JY, Kim D, Kim ND. Recent Developments in Combination Chemotherapy for Colorectal and Breast Cancers with Topoisomerase Inhibitors. International Journal of Molecular Sciences. 2023; 24(9):8457. https://doi.org/10.3390/ijms24098457
Chicago/Turabian StyleJang, Jung Yoon, Donghwan Kim, and Nam Deuk Kim. 2023. "Recent Developments in Combination Chemotherapy for Colorectal and Breast Cancers with Topoisomerase Inhibitors" International Journal of Molecular Sciences 24, no. 9: 8457. https://doi.org/10.3390/ijms24098457
APA StyleJang, J. Y., Kim, D., & Kim, N. D. (2023). Recent Developments in Combination Chemotherapy for Colorectal and Breast Cancers with Topoisomerase Inhibitors. International Journal of Molecular Sciences, 24(9), 8457. https://doi.org/10.3390/ijms24098457