
Age-Related Pathology in Corticobasal Degeneration



Abstract
:1. Introduction
2. Case Presentation
2.1. Results
2.1.1. Clinical Phenotypes
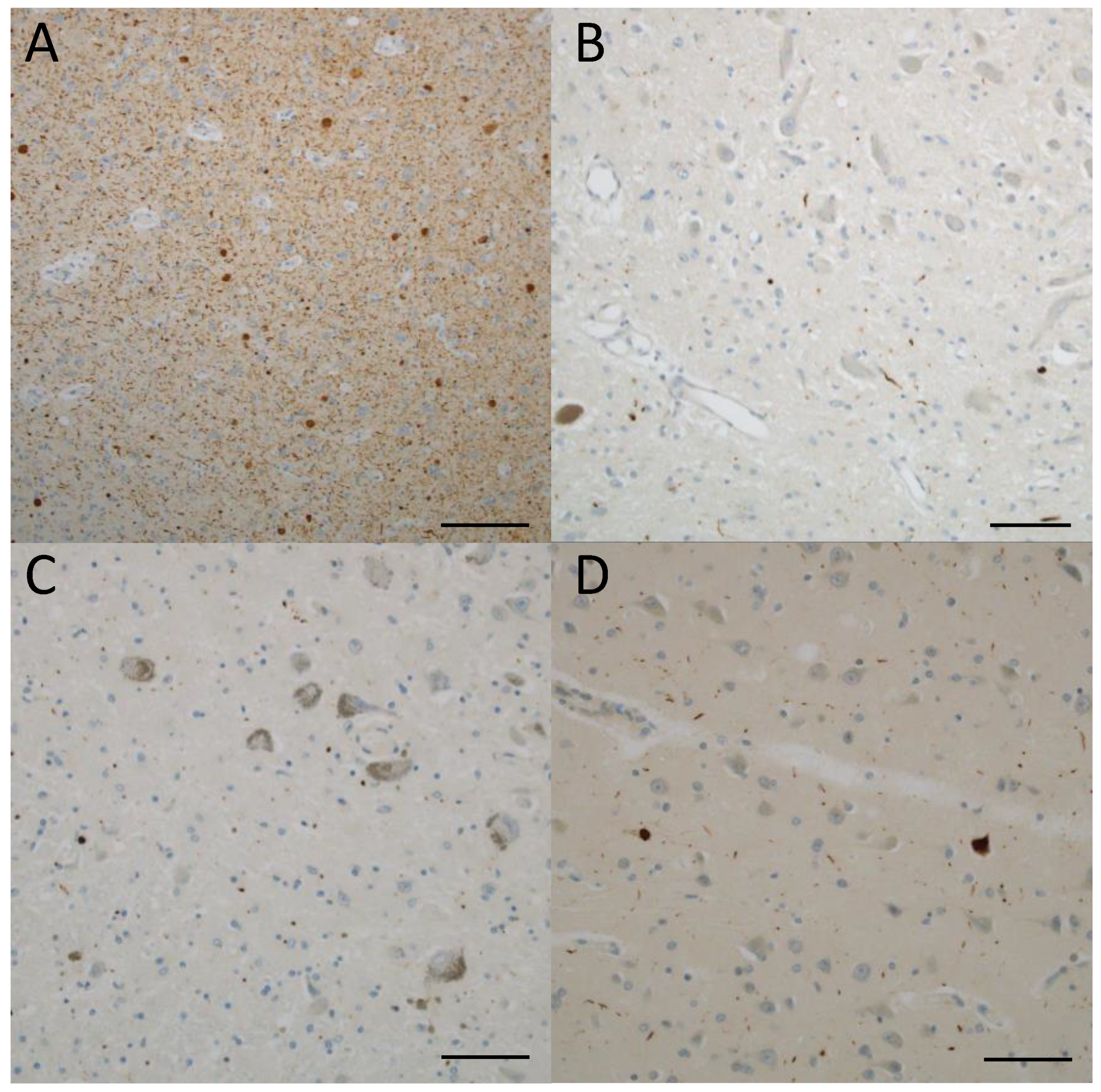
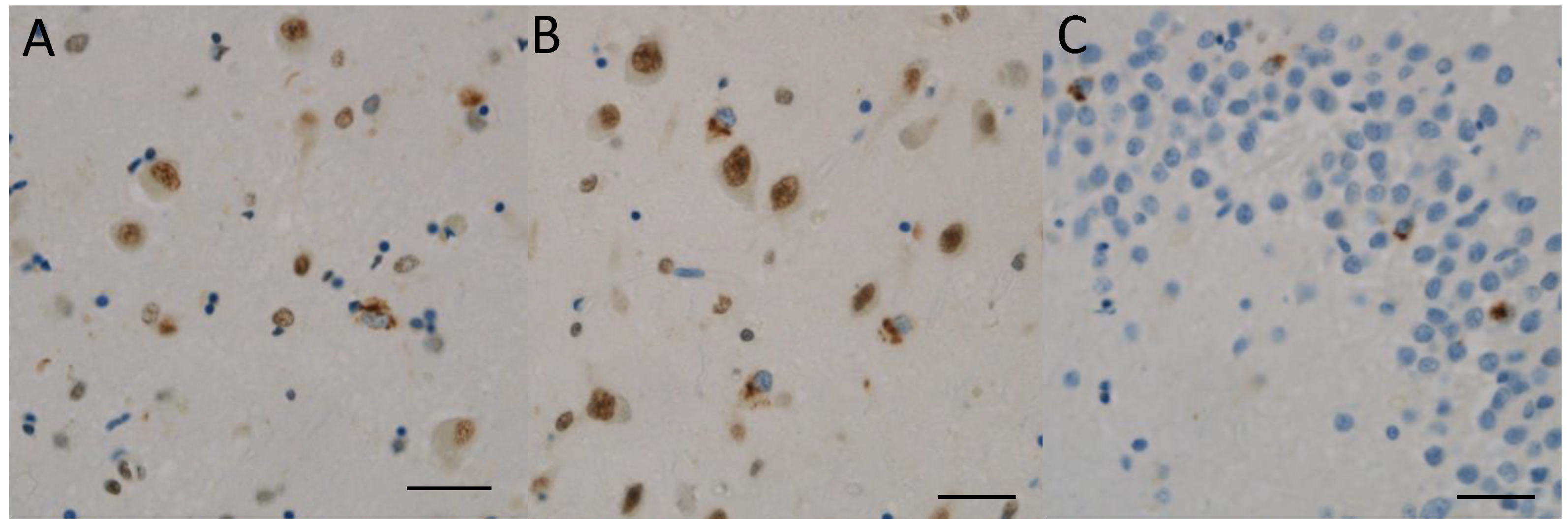
2.1.2. Pathological Phenotypes
2.1.3. Argyrophilic Grain Disease
2.1.4. Alzheimer Disease-Related Neurofibrillary Pathology and Amyloid β (Aβ)-Plaque Pathology
2.1.5. Lewy Body Pathology
2.1.6. Limbic-Predominant and Age-Related TDP-43 Encephalopathy (LATE)
2.2. Materials and Methods
2.2.1. Subjects
2.2.2. Tissue Preparation and Immunohistochemical Procedures
2.2.3. Neuropathological Assessment
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jellinger, K.A.; Attems, J. Challenges of multimorbidity of the aging brain: A critical update. J. Neural Transm. 2015, 122, 505–521. [Google Scholar] [CrossRef]
- Ferrer, I. The unique neuropathological vulnerability of the human brain to aging. Ageing Res. Rev. 2023, 87, 101916. [Google Scholar]
- Hogervorst, E.; Bandelow, S.; Combrinck, M.; Irani, S.R.; Smith, A.D. The validity and reliability of 6 sets of clinical criteria to classify Alzheimer’s disease and vascular dementia in cases confirmed post-mortem: Added value of a decision tree approach. Dement. Geriatr. Cogn. Disord. 2003, 16, 170–180. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, G.G.; Ferrer, I.; Grinberg, L.T.; Irina Alafuzoff, I.; Attems, J.; Herbert Budka, H.; Cairns, N.J.; Crary, J.F.; Duyckaerts, C.; Ghetti, B.; et al. Aging-related tau astrogliopathy (ARTAG): Harmonized evaluation strategy. Acta Neuropathol. 2016, 131, 87–102. [Google Scholar] [CrossRef]
- Nelson, P.T.; Dickson, D.W.; Trojanowski, J.Q.; Jack, C.R.; Boyle, P.A.; Arfanakis, K.; Rademakers, R.; Alafuzoff, I.; Attems, J.; Brayne, C.; et al. Limbic-predominant age-related TDP-43 encephalopathy (LATE): Consensus working group report. Brain 2019, 142, 1503–1527. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; Braak, E. Argyrophilic grains: Charateristic pathology of cerebral cortex in cases of adult onset dementia without Alzheimer changes. Neurosci. Lett. 1987, 76, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; Braak, E. Cortical and subcortical argyrophilic grains characterize a disease associated with adult onset dementia. Neuropathol. Appl. Neurobiol. 1989, 15, 13–15. [Google Scholar] [CrossRef] [PubMed]
- Togo, T.; Sahara, N.; Yen, S.H.; Cookson, N.; Ishizawa, T.; Hutton, M.; De Silva, R.; Lees, A.; Dickson, D.W. Argyrophilic grain disease is a sporadic 4-repeat tauopathy. J. Neuropathol. Exp. Neurol. 2002, 61, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Tatsumi, S.; Mimuro, M.; Iwasaki, Y.; Takahashi, R.; Kakita, A.; Takahashi, H.; Yoshida, M. Argyrophilic grains are reliable disease-specific features of corticobasal degeneration. J. Neuropathol. Exp. Neurol. 2014, 73, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Yokota, O.; Miki, T.; Ikeda, C.; Nagao, S.; Takenoshita, S.; Ishizu, H.; Haraguchi, T.; Kuroda, S.; Terada, S.; Yamada, N. Symposium: Comorbid pathologies of neurodegenerative disease Neuropathological comorbidity associated with argyrophilic grain disease. Neuropathology 2018, 38, 82–97. [Google Scholar] [CrossRef]
- Hauw, J.J.; Daniel, S.E.; Dickson, D.; Horoupianm, D.S.; Jellinger, K.; Lantos, P.L.; McKee, A.; Tabaton, M.; Litvan, I. Preliminary NINDS neuropathologic criteria for Steele-Richardson-Olszewski syndrome (progressive supranuclear palsy). Neurology 1994, 44, 2015–2019. [Google Scholar] [CrossRef]
- Roemer, S.F.; Grinberg, L.T.; Crary, J.F.; Seeley, W.W.; McKee, A.C.; Kovacs, G.G.; Beach, T.G.; Duyckaerts, C.; Ferrer, I.A.; Gelpi, E.; et al. Rainwater charitable foundation criteria for the neuropathologic diagnosis of progressive supranuclear palsy. Acta Neuropathol. 2022, 144, 603–614. [Google Scholar] [CrossRef] [PubMed]
- Santpere, G.; Ferre, I. Delineation of early changes in cases with progressive supranuclear palsy-like pathology. Astrocytes in striatum are primary targets of tau phosphorylation and GFAP oxidation. Brain Pathol. 2009, 19, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, C.; Yokota, O.; Nagao, S.; Ishizu, H.; Oshima, E.; Hasegawa, M.; Okahisa, Y.; Terada, S.; Yamada, N. The relationship between development of neuronal and astrocytic tau pathologies in subcortical nuclei and progression of argyrophilic grain disease. Brain Pathol. 2016, 26, 488–505. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, K.; Akiyama, H.; Kondo, H.; Haga, C.; Tanno, E.; Tokuda, T.; Ikeda, S. Thorn-shaped asatrocytes: Possibly secondarily induced tau-positive glial fibrillary tangles. Acta Neuropathol. 1995, 90, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.; Ghebremedhin, E.; Tredici, K.D.; Rüb, U.; Braak, H. High prevalence of thorn-shaped astrocytes in the aged human medial temporal lobe. Neurobiol. Aging 2004, 25, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, G.G.; Robinson, J.L.; Xie, S.X.; Lee, E.B.; Grossman, M.; Wolk, D.A.; Irwin, D.J.; Weintraub, D.; Kim, C.F.; Schuck, T.; et al. Evaluating the patterns of aging-related tau astrogliopathy unravels novel insights into brain aging and neurodegenerative disease. J. Neuropathol. Exp. Neurol. 2017, 76, 270–288. [Google Scholar] [CrossRef] [PubMed]
- Rebeiz, J.J.; Kolodny, E.H.; Richardson, E.P., Jr. Corticodentatonigral degeneration with neuronal achromasia. Arch. Neurol. 1968, 18, 20–33. [Google Scholar] [CrossRef]
- Gibb, W.R.; Luthert, P.J.; Marsden, C.D. Corticobasal degeneration. Brain 1989, 112, 1171–1192. [Google Scholar] [CrossRef]
- Dickson, D.W.; Bergeron, C.; Chin, S.S.; Duyckaerts, C.; Horoupian, D.; Ikeda, K.; Jellinger, K.; Lantos, P.L.; Lippa, C.F.; Mirra, S.S.; et al. Office of rare diseases neuropathologic criteria for courticobasal degeneration. J. Neuropathol. Exp. Neurol. 2002, 61, 935–946. [Google Scholar] [CrossRef]
- Rebeiz, J.J.; Kolodny, E.H.; Richardson, E.P., Jr. Corticodentatonigral degeneration with neuronal achromasia: A progressive disorder of late adult life. Trans. Am. Neurol. Assoc. 1967, 92, 23–26. [Google Scholar]
- Tolnay, M.; Probst, A. Ballooned neurons expressing alpha B-crystallin as a constant feature of the amygdala in argyrophilic grain disease. Neurosci. Lett. 1998, 246, 165–168. [Google Scholar] [CrossRef]
- Fujino, Y.; DeLucia, M.W.; Daviest, P.; Dickson, D.W. Ballooned neurons in the limbic lobe are associated with Alzheimer type pathology and lack diagnostic specificity. Neuropathol. Appl. Neurobiol. 2004, 30, 676–682. [Google Scholar] [CrossRef]
- Mathew, R.; Bak, T.H.; Hodges, J.R. Diagnostic criteria for corticobasal syndorome: A comparative study. J. Neurol. Neurosurg. Psychiatry 2012, 83, 405–410. [Google Scholar] [CrossRef]
- Feany, M.B.; Dickson, D.W. Widespread cytoskeletal pathology characterizes corticobasal degeneration. Am. J. Pathol. 1995, 146, 1388–1396. [Google Scholar] [PubMed]
- Braak, H.; Braak, E.; Ohm, T.; Bohl, J. Silver impregranion of Alzneimer’s neurofibrillary changes counterstained for basophilic and lipofuscin pigment. Stain Technol. 1988, 63, 197–200. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.J.; Litvan, I.; Lang, A.E.; Bak, T.H.; Bhatia, K.P.; Borroni, B.; Boxer, A.L.; Dickson, D.W.; Grossman, M.; Hallett, M.; et al. Criteria for the diagnosis of corticobasal degeneration. Neurology 2013, 80, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M. Symposium: Definition and differentials-How to distinguish disease-specific changes on microscopy Astrocytic incusions in progressive supranuclear palsy and corticobasal degeneration. Neuropathology 2014, 34, 555–570. [Google Scholar] [CrossRef] [PubMed]
- Mimuro, M.; Yoshida, M. Chameleons and mimics: Progressive supranuclear palsy and corticobasal degeneration. Neuropathology 2020, 40, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; Alafuzov, I.; Arzberger, T.; Kretzschmar, H.; Tredici, K.D. Staging of Alzheimer disease-associated neurofibrillary pathology using paraffin sections and immunocytochemistry. Acta Neuropathol. 2006, 112, 389–404. [Google Scholar] [CrossRef]
- Thal, D.R.; Rüb, U.; Orantes, M.; Braak, H. Phases of A-deposition in the human brain and its relevance for the development of AD. Neurology 2002, 58, 1791–1800. [Google Scholar] [CrossRef]
- Montine, T.J.; Phelps, C.H.; Beach, T.G.; Bigio, E.H.; Cairns, N.J.; Dickson, D.W.; Duyckaerts, C.; Frosch, M.P.; Masliah, E.; Mirra, S.S.; et al. National institute on Aging—Alzheimer’s association guidelines for the neuropathologic assessment of Alzheimer’s disease: A practical approach. Acta Neuropathol. 2012, 123, 1–11. [Google Scholar] [CrossRef]
- Saito, Y.; Ruberu, N.N.; Sawabe, M.; Arai, T.; Kazama, H.; Hosoi, T.; Yamanouchi, H.; Murayama, S. Lewy body-related a-Synucleinopathy in aging. J. Neuropathol. Exp. Neurol. 2004, 63, 742–749. [Google Scholar] [CrossRef] [PubMed]
- McKeith, I.G.; Boeve, B.F.; Dickson, D.W.; Halliday, G.; Taylor, J.P.; Weintraub, D.; Aarsland, D.; Galvin, J.; Attems, J.; Ballard, C.G.; et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB consortium. Neurology 2017, 89, 88–100. [Google Scholar] [CrossRef]
- Love, S.; Chalmers, K.; Ince, P.; Esiri, M.; Attems, J.; Jellinger, K.; Yamada, M.; McCarron, M.; Minett, T.; Matthews, F.; et al. Development, appraisal, validation and implementation of a consensus protocol for the assessment of cerebral amyloid angiopathy in post-mortem brain tissue. Am. J. Neurodegener. Dis. 2014, 3, 19–32. [Google Scholar]
- Rahimi, J.; Kovacs, G.G. Prevalence of mixed pathologies in the aging brain. Alzheimer Res. Ther. 2014, 6, 82. [Google Scholar] [CrossRef]
- Kovacs, G.G.; Milenkovic, I.; Wöhrer, A.; Höftberger, R.; Gelpi, E.; Haberler, C.; Hönigschnabl, S.; Reiner-Concin, A.; Heinzl, H.; Jungwirth, S.; et al. Non-Alzheimer neurodegenerative pathologies and their combinations are more frequent than commonly believed in the elderly brain: A community-based autopsy series. Acta Neuropathol. 2013, 126, 365–384. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.S.; Yu, L.; Trojanowski, J.Q.; Chen, E.Y.; Boyle, P.A.; Bennett, D.A.; Schneider, J.A. TDP-43 pathology, cognitive decline, and dementia in old age. JAMA Neurol. 2013, 70, 1418–1424. [Google Scholar] [CrossRef]
- Miki, T.; Yokota, O.; Haraguchi, T.; Ishizu, H.; Hasegawa, M.; Ishihara, T.; Ueno, S.; Takanoshita, S.; Terada, S.; Yamada, N. Factors associated with development and distribution of granular/fuzzy astrocytes in neurodegenerative diseases. Brain Pathol. 2020, 30, 811–830. [Google Scholar] [CrossRef]
- Kovacs, G.G.; Xie, S.X.; Robinson, J.L.; Lee, E.B.; Smith, D.H.; Schuck, T.; Lee, V.M.Y.; Trojanowski, J.Q. Sequential stages and distribution patterns of aging-related tau astrogliopathy (ARTAG) in the human brain. Acta Neuropathol. Commun. 2018, 6, 50. [Google Scholar] [CrossRef] [PubMed]
- Josephs, K.A.; Mandrekar, J.N.; Dickson, D.W. The relationship between histopathological features of progressive supranuclear palsy and disease duration. Park. Relat. Disord. 2006, 12, 109–112. [Google Scholar] [CrossRef]
- Mimuro, M.; Yoshida, M.; Kuzuhara, S.; Kokubo, Y. Symposium; Comorbid pathologies of neurodegenerative diseases Amyotrophic lateral sclerosis and parkinsonism-dementia complex of the Hohara focus of the Kii peninsula: A multiple proteinopathy? Neuropathology 2018, 38, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.L.; Lee, E.B.; Xie, S.X.; Rennert, L.; Suh, E.R.; Bredenberg, C.; Caswell, C.; Deerlin, V.M.V.; Yan, N.; Yousef, A.; et al. Neurodegenerative disease concomitant proteinopathies are prevalent, age-related and APOE4-associated. Brain 2018, 141, 2181–2193. [Google Scholar] [CrossRef] [PubMed]
- Borghammer, P.; Horsager, J.; Andersen, K.; Van Den Berge, N.; Raunio, A.; Murayama, S.; Parkkinen, L.; Myllykangas, L. Neuropathological evidence of body-first vs. brain-first Lewy body disease. Neurobiol. Dis. 2021, 161, 105557. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; Tredici, K.D.; Rub, U.; de Vos, R.A.I.; Steur, E.N.H.J.; Braak, E. Staging of brain patahology related to sporadic Parkinson’s disease. Neurobiol. Aging 2003, 24, 197–211. [Google Scholar] [CrossRef]
- Raunio, A.; Kaivola, K.; Tuimala, J.; Kero, M.; Oinas, M.; Polvikoski, T.; Paetau, A.; Tienari, P.J.; Myllykangas, L. Lewy-related pathology exhibits two anatomically and genetically distinct progression patterns: A population-based study of Finns aged 85. Acta Neuropathol. 2019, 138, 771–782. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Case | Sex | Age of Death | Clinical Duration, Years | Clinical Phenotype a | Brain Weight | Pathological Phenotype b | Thal’s Amyloid Phase | Braak’s NFT Stage | CERAD Neuritic Plaque Score | Love’s CAA Score | Saito’s AGD Stage | Lewy Body Pathology Classification | LATE Stage |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 60 | 7 | PSPS | 1145 | PSP-like | 0 | II | 0 | 0 | II | 0 | 0 |
| 2 | M | 61 | 3 | CBS | 1250 | typical | 1 | I | 0 | 0 | I | 0 | 0 |
| 3 | F | 62 | 8 | PSPS | 990 | PSP-like | 1 | II | 0 | 1 | I | 0 | 0 |
| 4 | F | 62 | 10 | naPPA | 870 | typical | 3 | II | 0 | 0 | II | 0 | 0 |
| 5 | F | 67 | 6 | FBS | 975 | typical | 0 | I | 0 | 0 | I | 0 | 0 |
| 6 | F | 67 | 8 | PSPS | 985 | PSP-like | 2 | I | B | 2 | II | 0 | 2 |
| 7 | M | 68 | 4 | PSPS | 1350 | typical | 1 | I | 0 | 1 | II | 0 | 0 |
| 8 | M | 68 | 8 | PSPS | 1200 | PSP-like | 0 | I | 0 | 1 | I | Brainstem | 1 |
| 9 | M | 68 | 3 | PSPS | 1270 | BG | 0 | II | A | 0 | I | 0 | 1 |
| 10 | M | 69 | 10 | PSPS | 1015 | PSP-like | 0 | I | 0 | 0 | II | 0 | 1 |
| 11 | F | 70 | 11 | FBS | 770 | typical | 2 | IV | A | 0 | III | 0 | 0 |
| 12 | M | 70 | 8 | unclassified | 1135 | typical | 4 | II | B | 2 | I | Amygdala | 0 |
| 13 | M | 70 | 4 | unclassified | 1161 | PSP-like | 0 | II | 0 | 0 | II | 0 | 0 |
| 14 | F | 71 | 8 | PSPS | 1020 | PSP-like | 2 | II | 0 | 1 | II | 0 | 0 |
| 15 | M | 73 | 6 | CBS | 1200 | typical | 1 | III | 0 | 1 | I | 0 | 0 |
| 16 | F | 74 | 10 | PSPS | 1000 | PSP-like | 0 | III | 0 | 0 | I | 0 | 0 |
| 17 | M | 76 | 7 | unclassified | 1120 | typical | 0 | II | 0 | 0 | I | Limbic | 0 |
| 18 | M | 77 | 5 | PSPS | 1190 | typical | 1 | II | 0 | 0 | II | 0 | 0 |
| 19 | F | 81 | 11 | CBS | 1060 | typical | 1 | I | 0 | 1 | III | 0 | 2 |
| 20 | F | 83 | 6 | CBS | 955 | typical | 0 | III | 0 | 1 | I | 0 | 0 |
| 21 | M | 86 | 6 | unclassified | 1025 | typical | 2 | I | B | 0 | III | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mimuro, M.; Iwasaki, Y. Age-Related Pathology in Corticobasal Degeneration. Int. J. Mol. Sci. 2024, 25, 2740. https://doi.org/10.3390/ijms25052740
Mimuro M, Iwasaki Y. Age-Related Pathology in Corticobasal Degeneration. International Journal of Molecular Sciences. 2024; 25(5):2740. https://doi.org/10.3390/ijms25052740
Chicago/Turabian StyleMimuro, Maya, and Yasushi Iwasaki. 2024. "Age-Related Pathology in Corticobasal Degeneration" International Journal of Molecular Sciences 25, no. 5: 2740. https://doi.org/10.3390/ijms25052740
APA StyleMimuro, M., & Iwasaki, Y. (2024). Age-Related Pathology in Corticobasal Degeneration. International Journal of Molecular Sciences, 25(5), 2740. https://doi.org/10.3390/ijms25052740