
Bio-Photonic Detection and Quantitative Evaluation Method for the Progression of Dental Caries Using Optical Frequency-Domain Imaging Method



Abstract
:1. Introduction
2. Materials and Methods
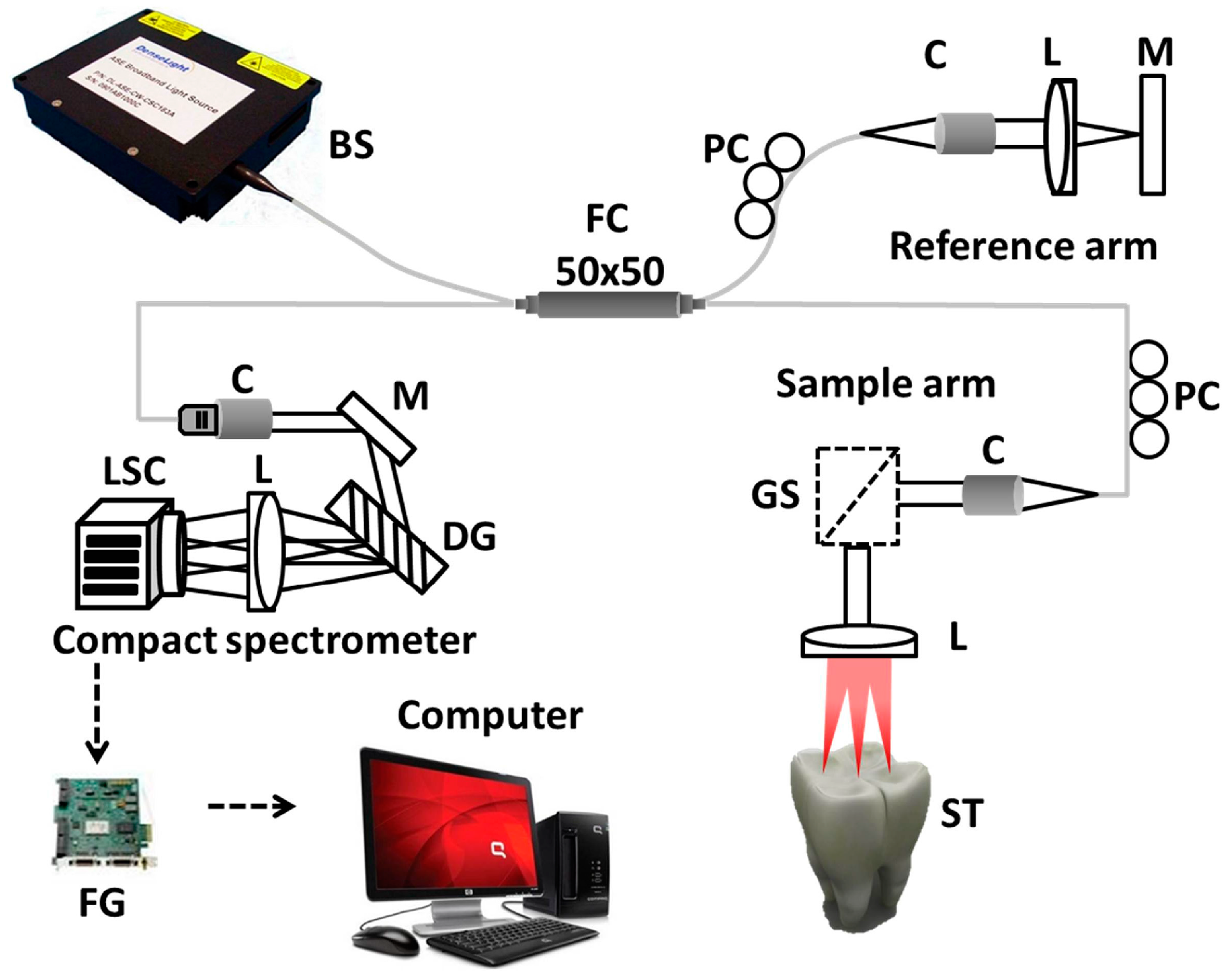
2.1. Optical Frequency Domain Imaging (OFDI) Technique
2.2. Specimen Preparation
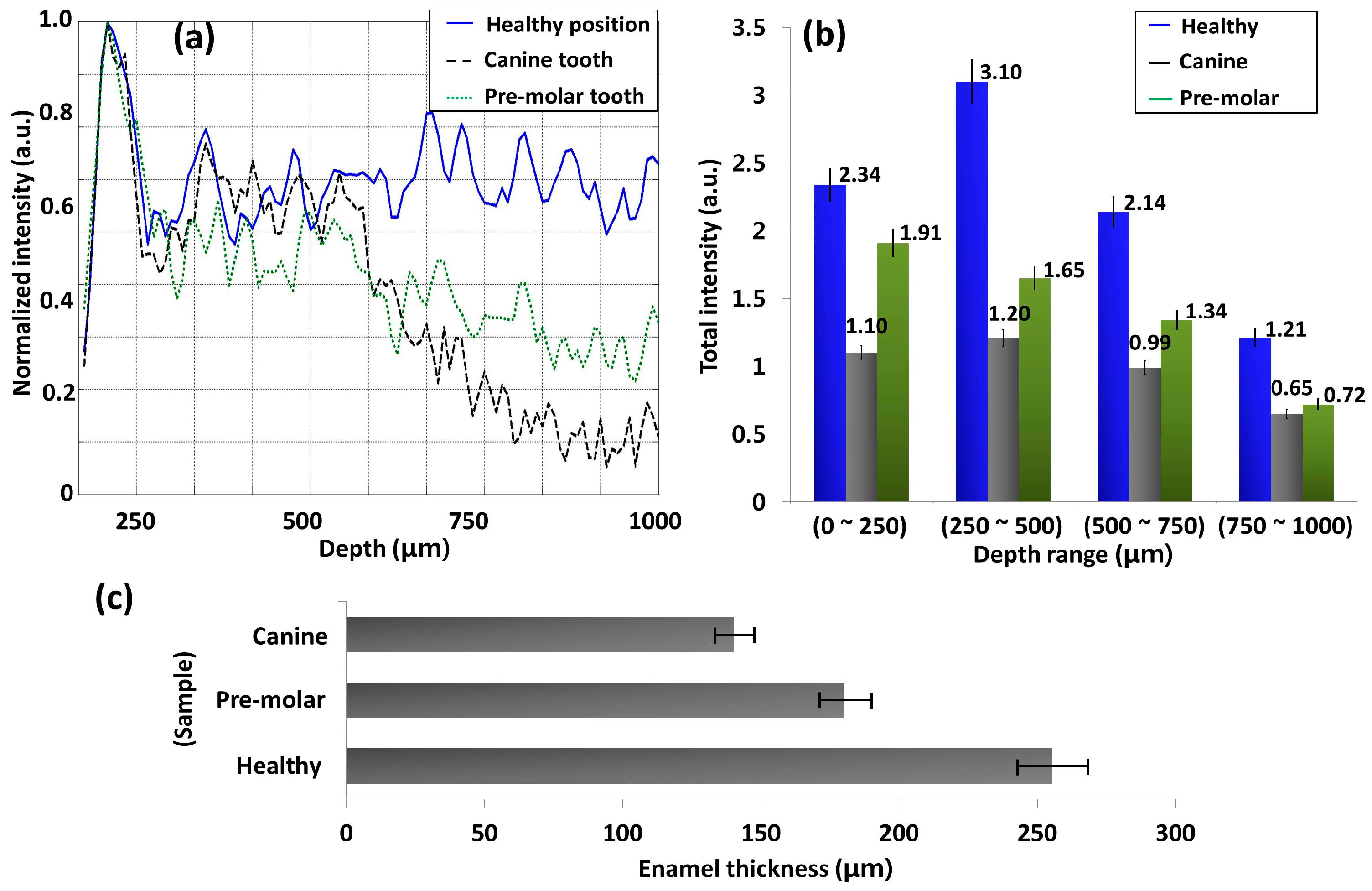
2.3. Intensity Fluctuation Analysis
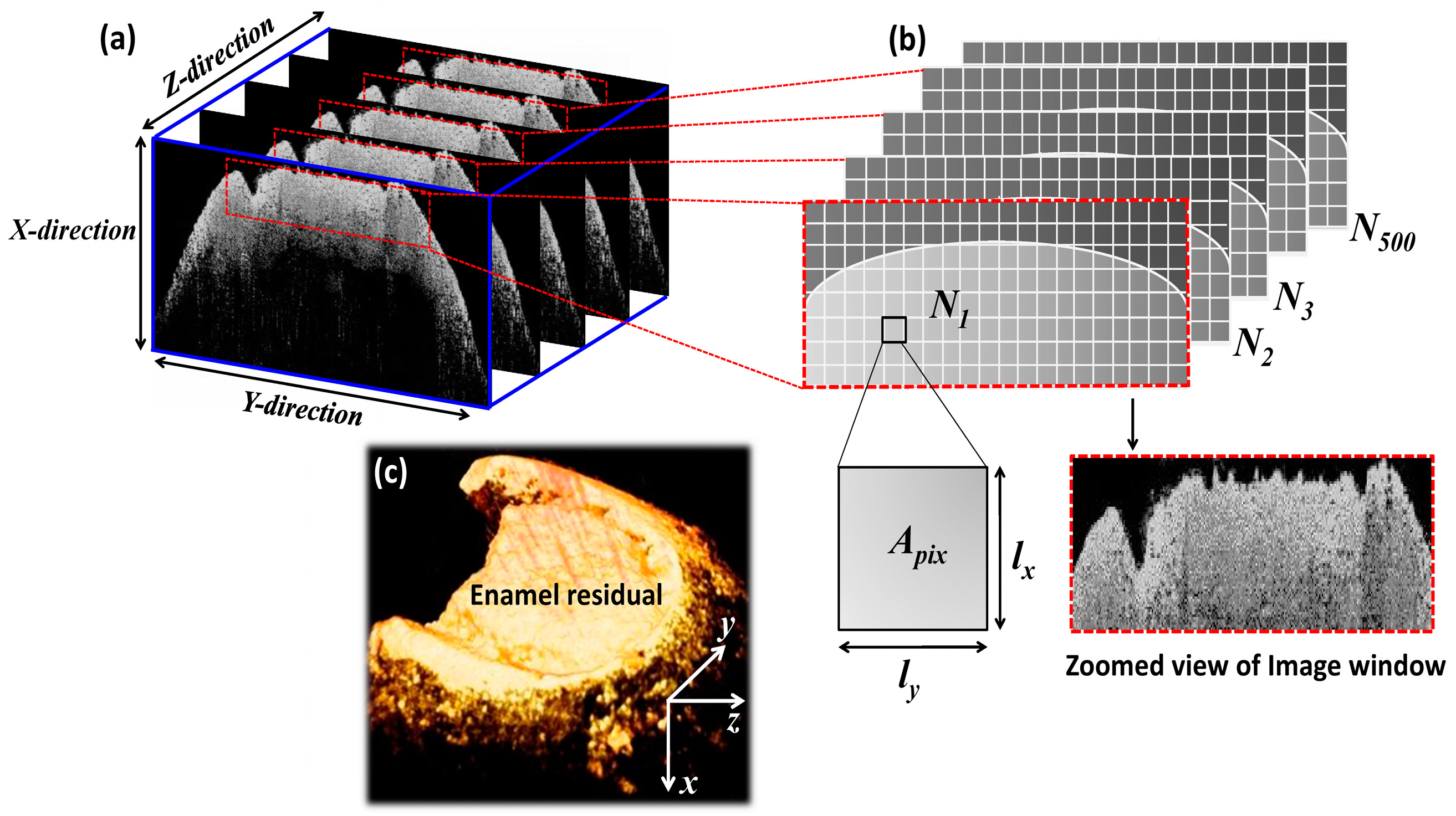
2.4. Volumetric Analysis
3. Results and Discussion
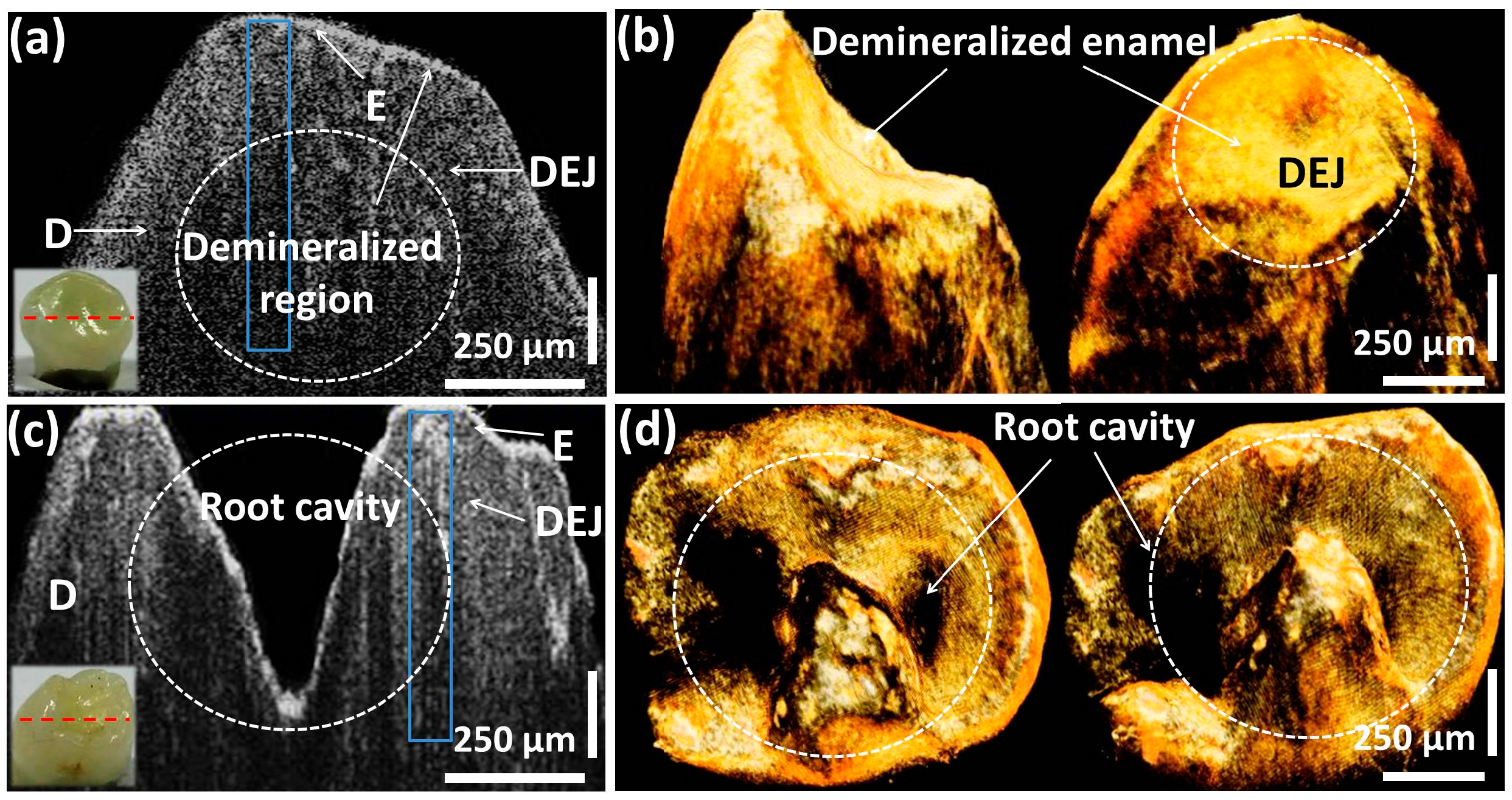
3.1. Morphological Analysis of Dental Caries along with Quantitative Evaluations
3.2. Volumetric Evaluation Technique to Identify Initial Caries
3.3. Structural Comparison between OCT and Conventional Methods
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- Fejerskov, O. Changing paradigms in concepts on dental caries: Consequences for oral health care. Caries Res. 2004, 38, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Dove, S.B.; McDavid, W. A comparison of conventional intra-oral radiography and computer imaging techniques for the detection of proximal surface dental caries. Dentomaxillofac. Radiol. 1992, 21, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Fercher, A.F. Optical coherence tomography. J. Biomed. Opt. 1996, 1, 157–173. [Google Scholar] [CrossRef] [PubMed]
- Ding, Z.; Ren, H.; Zhao, Y.; Nelson, J.S.; Chen, Z. High-resolution optical coherence tomography over a large depth range with an axicon lens. Opt. Lett. 2002, 27, 243–245. [Google Scholar] [CrossRef] [PubMed]
- Boppart, S.A.; Herrmann, J.; Pitris, C.; Stamper, D.L.; Brezinski, M.E.; Fujimoto, J.G. High-resolution optical coherence tomography-guided laser ablation of surgical tissue. J. Surg. Res. 1999, 82, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Nassif, N.; Cense, B.; Park, B.; Pierce, M.; Yun, S.; Bouma, B.; Tearney, G.; Chen, T.; de Boer, J. In vivo high-resolution video-rate spectral-domain optical coherence tomography of the human retina and optic nerve. Opt. Express 2004, 12, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Wijesinghe, R.E.; Park, K.; Kim, P.; Oh, J.; Kim, S.-W.; Kim, K.; Kim, B.-M.; Jeon, M.; Kim, J. Optically deviated focusing method based high-speed sd-oct for in vivo retinal clinical applications. Opt. Rev. 2016, 23, 307–315. [Google Scholar] [CrossRef]
- Welzel, J. Optical coherence tomography in dermatology: A review. Skin Res. Technol. 2001, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Cho, N.H.; Lee, J.W.; Cho, J.-H.; Kim, J.; Jang, J.H.; Jung, W. Evaluation of the usefulness of three-dimensional optical coherence tomography in a guinea pig model of endolymphatic hydrops induced by surgical obliteration of the endolymphatic duct. J. Biomed. Opt. 2015, 20, 036009. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, K.; Wijesinghe, R.E.; Jeon, D.; Lee, S.H.; Jeon, M.; Jang, J.H. Decalcification using ethylenediaminetetraacetic acid for clear microstructure imaging of cochlea through optical coherence tomography. J. Biomed. Opt. 2016, 21, 081204. [Google Scholar] [CrossRef] [PubMed]
- Akkaya, N.; Kansu, Ö.; Kansu, H.; Çağirankaya, L.; Arslan, U. Comparing the accuracy of panoramic and intraoral radiography in the diagnosis of proximal caries. Dentomaxillofac. Radiol. 2014. [CrossRef] [PubMed]
- Seneadza, V.; Koob, A.; Kaltschmitt, J.; Staehle, H.; Duwenhoegger, J.; Eickholz, P. Digital enhancement of radiographs for assessment of interproximal dental caries. Dentomaxillofac. Radiol. 2014. [CrossRef] [PubMed]
- Featherstone, J.; Ten Cate, J.; Shariati, M.; Arends, J. Comparison of artificial caries-like lesions by quantitative microradiography and microhardness profiles. Caries Res. 1983, 17, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Bühler, C.M.; Ngaotheppitak, P.; Fried, D. Imaging of occlusal dental caries (decay) with near-ir light at 1310-nm. Opt. Express 2005, 13, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, N.J.; Iijima, Y.; Shen, P.; Yuan, Y.; Walker, G.D.; Reynolds, C.; MacRae, C.M.; Wilson, N.C.; Adams, G.G.; Reynolds, E.C. Comparative study of the measurement of enamel demineralization and remineralization using transverse microradiography and electron probe microanalysis. Microsc. Microanal. 2014, 20, 937–945. [Google Scholar] [CrossRef] [PubMed]
- Fried, D.; Xie, J.; Shafi, S.; Featherstone, J.D.; Breunig, T.M.; Le, C. Imaging caries lesions and lesion progression with polarization sensitive optical coherence tomography. J. Biomed. Opt. 2002, 7, 618–627. [Google Scholar] [CrossRef] [PubMed]
- Ishibashi, K.; Ozawa, N.; Tagami, J.; Sumi, Y. Swept-source optical coherence tomography as a new tool to evaluate defects of resin-based composite restorations. J. Dent. 2011, 39, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, A.; Dichtl, S.; Hitzenberger, C.; Sattmann, H.; Robl, B.; Moritz, A.; Fercher, A.; Sperr, W. Polarization–sensitive optical coherence tomography of dental structures. Caries Res. 1999, 34, 59–69. [Google Scholar] [CrossRef]
- Huynh, G.D.; Darling, C.L.; Fried, D. Changes in the optical properties of dental enamel at 1310 nm after demineralization. In Proceedings of the Biomedical Optics 2004, San Jose, CA, USA, 28 May 2004; pp. 118–124.
- Cahill, L.; Lee, A.M.; Pahlevaninezhad, H.; Ng, S.; MacAulay, C.E.; Poh, C.; Lane, P. Passive endoscopic polarization sensitive optical coherence tomography with completely fiber based optical components. In Proceedings of the SPIE BiOS, San Francisco, CA, USA, 2 March 2015; p. 930413.
- Jones, R.S.; Staninec, M.; Fried, D. Imaging artificial caries under composite sealants and restorations. J. Biomed. Opt. 2004, 9, 1297–1304. [Google Scholar] [CrossRef] [PubMed]
- Popescu, D.P.; Sowa, M.G.; Hewko, M.D. Assessment of early demineralization in teeth using the signal attenuation in optical coherence tomography images. J. Biomed. Opt. 2008, 13, 054053. [Google Scholar] [CrossRef] [PubMed]
- Shimada, Y.; Sadr, A.; Burrow, M.F.; Tagami, J.; Ozawa, N.; Sumi, Y. Validation of swept-source optical coherence tomography (ss-oct) for the diagnosis of occlusal caries. J. Dent. 2010, 38, 655–665. [Google Scholar] [CrossRef] [PubMed]
- Cara, A.C.; Zezell, D.M.; Ana, P.A.; Maldonado, E.P.; Freitas, A.Z. Evaluation of two quantitative analysis methods of optical coherence tomography for detection of enamel demineralization and comparison with microhardness. Lasers Surg. Med. 2014, 46, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.-S.; Ho, Y.-C.; Lee, S.-Y.; Chuang, C.-C.; Tsai, J.-C.; Lin, K.-F.; Sun, C.-W. Dental optical coherence tomography. Sensors 2013, 13, 8928–8949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keane, P.A.; Ruiz-Garcia, H.; Sadda, S.R. Clinical applications of long-wavelength (1000-nm) optical coherence tomography. Ophthalmic Surg. Lasers Imaging Retin. 2011, 42, S67–S74. [Google Scholar] [CrossRef] [PubMed]
- Jeon, M.; Kim, J.; Jung, U.; Lee, C.; Jung, W.; Boppart, S.A. Full-range k-domain linearization in spectral-domain optical coherence tomography. Appl. Opt. 2011, 50, 1158–1163. [Google Scholar] [CrossRef] [PubMed]
- Jung, U.-S.; Cho, N.-H.; Kim, S.-H.; Jeong, H.-S.; Kim, J.-H.; Ahn, Y.-C. Simple spectral calibration method and its application using an index array for swept source optical coherence tomography. J. Opt. Soc. Korea 2011, 15, 386–393. [Google Scholar] [CrossRef]
- Lee, C.; Lee, S.-Y.; Kim, J.-Y.; Jung, H.-Y.; Kim, J. Optical sensing method for screening disease in melon seeds by using optical coherence tomography. Sensors 2011, 11, 9467–9477. [Google Scholar] [CrossRef] [PubMed]
- Wijesinghe, R.E.; Lee, S.-Y.; Kim, P.; Jung, H.-Y.; Jeon, M.; Kim, J. Optical inspection and morphological analysis of diospyros kaki plant leaves for the detection of circular leaf spot disease. Sensors 2016, 16, 1282. [Google Scholar] [CrossRef] [PubMed]
- Shellis, R. Relationship between human enamel structure and the formation of caries-like lesions in vitro. Arch. Oral Biol. 1984, 29, 975–981. [Google Scholar] [CrossRef]
- Silverstone, L.; Poole, D. The effect of saliva and calcifying solutions upon the histological appearance of enamel caries. Caries Res. 1968, 2, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, K.; Kuzmina, I.; Bjørndal, L.; Thylstrup, A. Relationship between external and histologic features of progressive stages of caries in the occlusal fossa. Caries Res. 1995, 29, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Go, E.-J.; Jung, H.-S.; Kim, E.-S.; Jung, I.-Y.; Lee, S.-J. Histology of dental pulp healing after tooth replantation in rats. J. Korean Acad. Conserv. Dent. 2010, 35, 273–284. [Google Scholar] [CrossRef]
- Yun, S.; Tearney, G.; de Boer, J.; Iftimia, N.; Bouma, B. High-speed optical frequency-domain imaging. Opt. Express 2003, 11, 2953–2963. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| System Parameters | Specification |
|---|---|
| Central Wavelength | 1310 nm |
| Spectral bandwidth | 135 nm |
| Axial resolution air/tissue | 6 μm/3.61 μm |
| Transverse resolution | 25 μm |
| Maximum imaging width | 8 mm |
| Maximum imaging depth | >6 mm |
| Optical power variation | ±5% |
| Experimented Volunteer | Tooth Classification | Inspection Category |
|---|---|---|
| 11-year-old male | Molar tooth | Healthy |
| 11-year-old female | Molar tooth | Partially demineralized |
| 10-year-old male | Molar tooth | Carious |
| 11-year-old male | Canine tooth | Partially demineralized |
| 12-year-old female | Pre-molar tooth | Partially demineralized |
| Specimen Category | Enamel Thickness (μm) | Total Intensity Fluctuation in Each Depth Range (a.u.) | |||
|---|---|---|---|---|---|
| 0–250 μm | 250–500 μm | 500–750 μm | 750–1000 μm | ||
| Healthy molar | 255.45 ± 15.03 | 2.34 ± 0.2 | 3.10 ± 0.2 | 2.14 ± 0.2 | 1.21 ± 0.2 |
| Dem. molar | 150.30 ± 10.02 | 2.09 ± 0.2 | 2.21 ± 0.2 | 1.24 ± 0.2 | 0.77 ± 0.1 |
| Carious molar | 100.20 ± 6.68 | 1.24 ± 0.1 | 0.74 ± 0.05 | 0.41 ± 0.02 | 0.11 ± 0.01 |
| Dem. canine | 140.28 ± 9.35 | 1.10 ± 0.1 | 1.21 ± 0.1 | 0.99 ± 0.1 | 0.65 ± 0.1 |
| Dem. premolar | 180.36 ± 12.02 | 1.91 ± 0.1 | 1.65 ± 0.1 | 1.34 ± 0.1 | 0.72 ± 0.05 |
| Tooth Specimen | Total Number of 2D OCT Images | Total Number of Enamel Residual Pixels | Enamel Residual Volume (mm3) |
|---|---|---|---|
| Healthy molar tooth | 500 | 2.13 × 107 | 28.72 |
| Part.dem. molar | 500 | 1.31 × 107 | 17.70 |
| Carious molar | 500 | 0.91 × 107 | 12.26 |
| Part.dem. canine | 500 | 1.28 × 107 | 17.20 |
| Part.dem. pre-molar | 500 | 1.42 × 107 | 19.15 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wijesinghe, R.E.; Cho, N.H.; Park, K.; Jeon, M.; Kim, J. Bio-Photonic Detection and Quantitative Evaluation Method for the Progression of Dental Caries Using Optical Frequency-Domain Imaging Method. Sensors 2016, 16, 2076. https://doi.org/10.3390/s16122076
Wijesinghe RE, Cho NH, Park K, Jeon M, Kim J. Bio-Photonic Detection and Quantitative Evaluation Method for the Progression of Dental Caries Using Optical Frequency-Domain Imaging Method. Sensors. 2016; 16(12):2076. https://doi.org/10.3390/s16122076
Chicago/Turabian StyleWijesinghe, Ruchire Eranga, Nam Hyun Cho, Kibeom Park, Mansik Jeon, and Jeehyun Kim. 2016. "Bio-Photonic Detection and Quantitative Evaluation Method for the Progression of Dental Caries Using Optical Frequency-Domain Imaging Method" Sensors 16, no. 12: 2076. https://doi.org/10.3390/s16122076
APA StyleWijesinghe, R. E., Cho, N. H., Park, K., Jeon, M., & Kim, J. (2016). Bio-Photonic Detection and Quantitative Evaluation Method for the Progression of Dental Caries Using Optical Frequency-Domain Imaging Method. Sensors, 16(12), 2076. https://doi.org/10.3390/s16122076