Energy-Based Metrics for Arthroscopic Skills Assessment


 ,
, 
Abstract
:1. Introduction
1.1. Skills Assessment in Minimally Invasive Surgery
1.2. Objectives
2. Methods
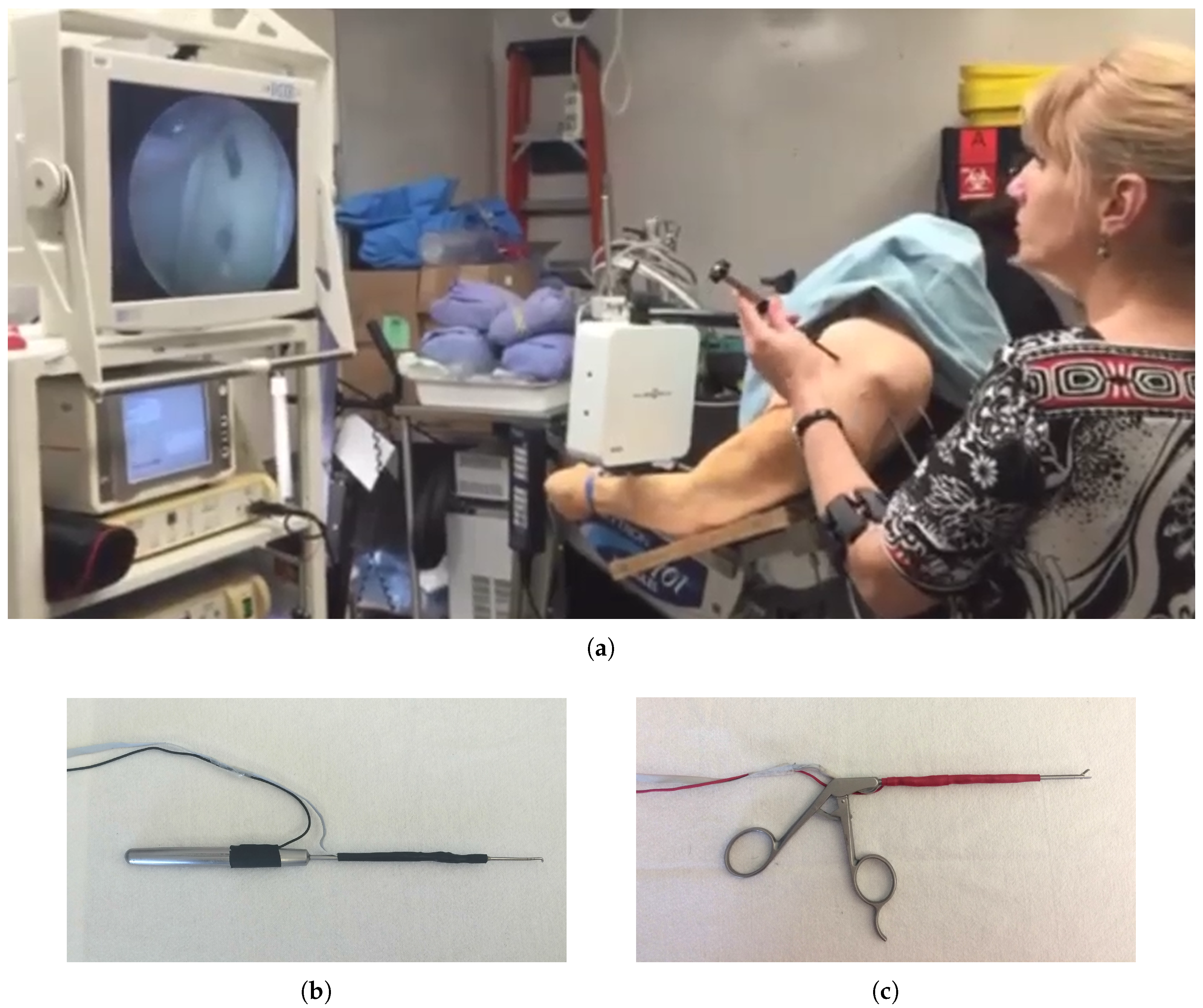
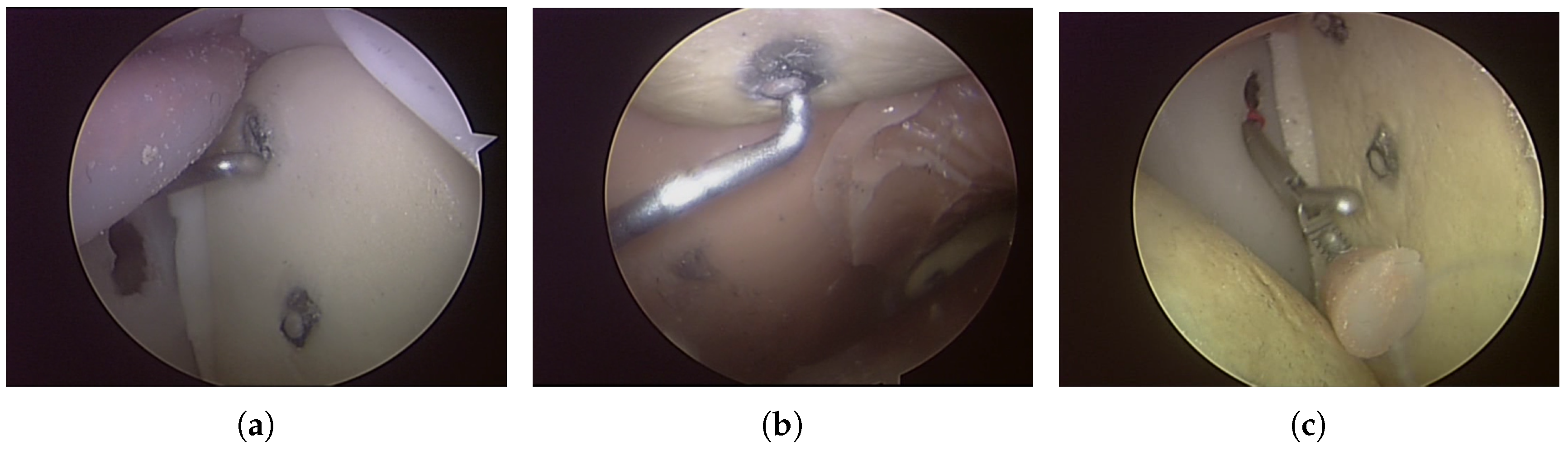
2.1. Experimental Design
2.2. Metrics
2.3. Trainee Classification
2.4. Validation
2.4.1. Leave-One-Subject-Out Cross-Validation
2.4.2. Computation Time
3. Results
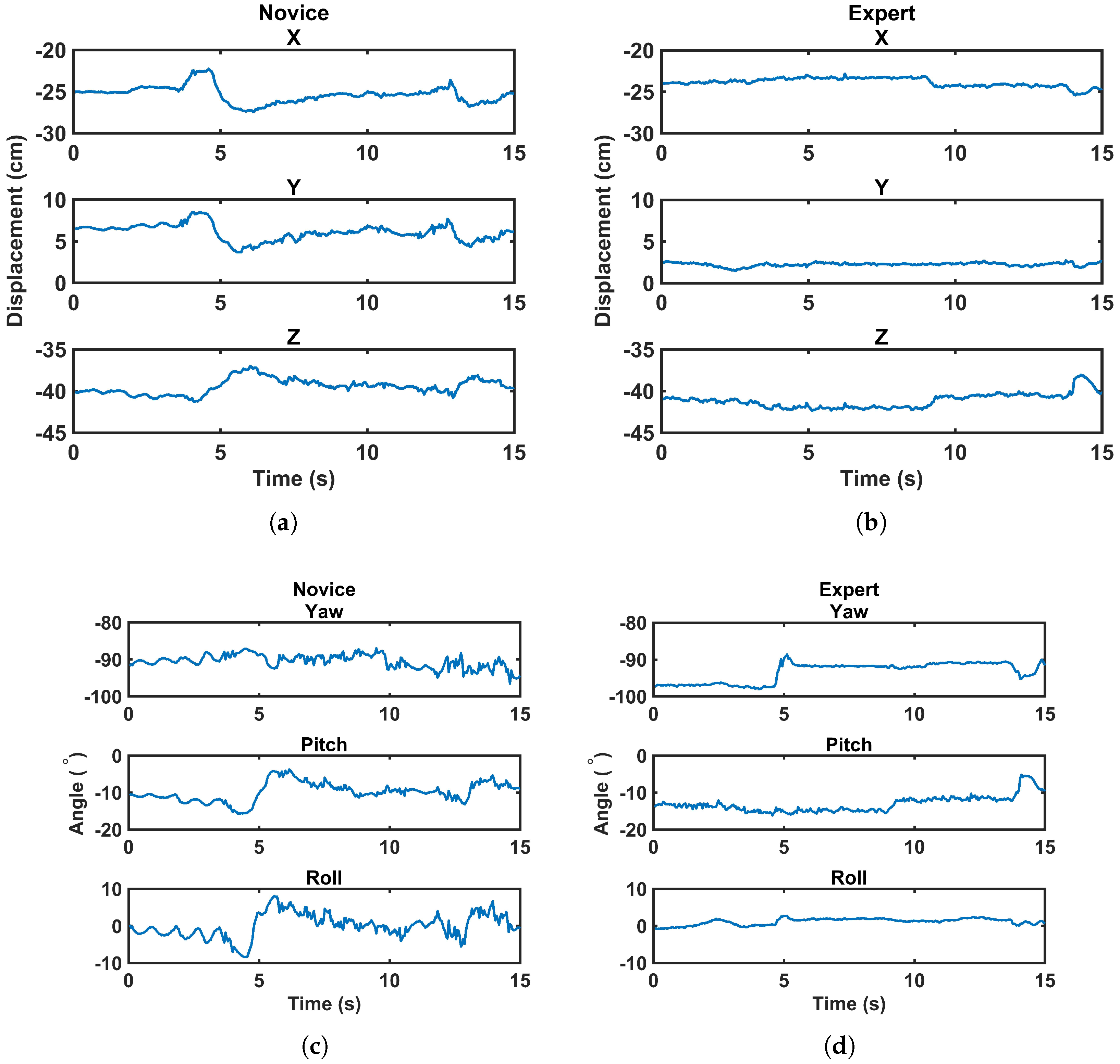
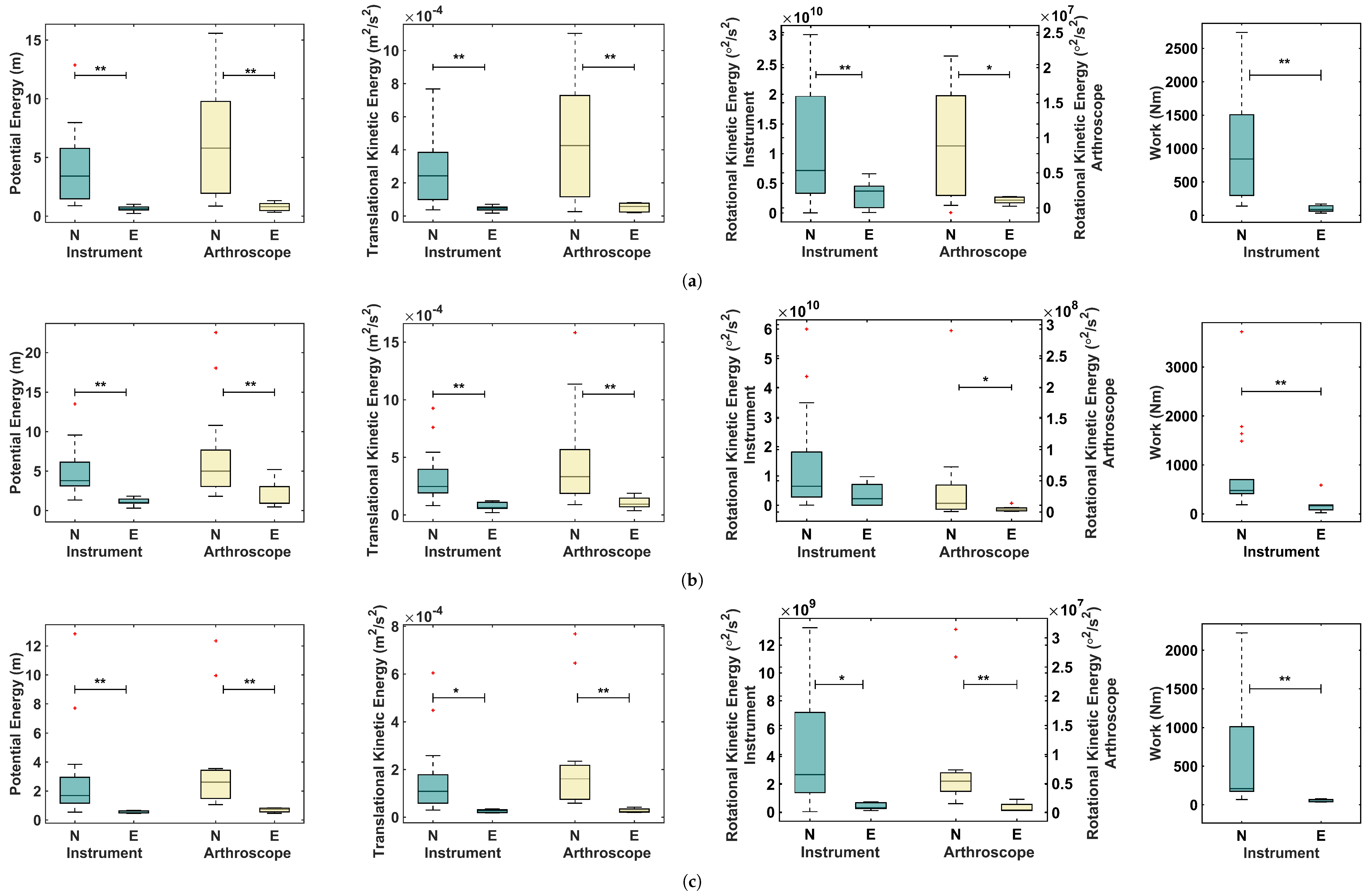
3.1. Energy-Based Metrics and Normalized Energy-Based Metrics
3.2. Validation
4. Discussion
4.1. Normalized Energy-Based Metrics
4.2. Instrument, Arthroscope, or Both?
4.3. Classifiers
4.4. Tasks
5. Conclusions and Future Work
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Roberts, P.G.; Guyver, P.; Baldwin, M.; Akhtar, K.; Alvand, A.; Price, A.J.; Rees, J.L. Validation of the updated ArthroS simulator: Face and construct validity of a passive haptic virtual reality simulator with novel performance metrics. Knee Surg. Sports Traumatol. Arthrosc. 2016, 25, 616–625. [Google Scholar] [CrossRef] [PubMed]
- Reiley, C.E.; Lin, H.C.; Yuh, D.D.; Hager, G.D. Review of methods for objective surgical skill evaluation. Surg. Endosc. 2011, 25, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Hoyle, A.C.; Whelton, C.; Umaar, R.; Funk, L. Validation of a global rating scale for shoulder arthroscopy: A pilot study. Shoulder Elb. 2012, 4, 16–21. [Google Scholar] [CrossRef]
- Tashiro, Y.; Miura, H.; Nakanishi, Y.; Okazaki, K.; Iwamoto, Y. Evaluation of skills in arthroscopic training based on trajectory and force data. Clin. Orthop. Relat. Res. 2009, 467, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Martin, K.D.; Belmont, P.J.; Schoenfeld, A.J.; Todd, M.; Cameron, K.L.; Owens, B.D. Arthroscopic basic task performance in shoulder simulator model correlates with similar task performance in cadavers. J. Bone Joint Surg. 2011, 93. [Google Scholar] [CrossRef] [PubMed]
- Escoto, A.; Le Ber, F.; Trejos, A.L.; Naish, M.D.; Patel, R.V.; LeBel, M.E. A knee arthroscopy simulator: Design and validation. In Proceedings of the 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 5715–5718. [Google Scholar]
- Oropesa, I.; Sánchez-González, P.; Lamata, P.; Chmarra, M.K.; Pagador, J.B.; Sánchez-Margallo, J.A.; Sánchez-Margallo, F.M.; Gómez, E.J. Methods and tools for objective assessment of psychomotor skills in laparoscopic surgery. J. Surg. Res. 2011, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escoto, A.; Trejos, A.L.; Naish, M.D.; Patel, R.V.; LeBel, M.E. Force sensing-based simulator for arthroscopic skills assessment in orthopaedic knee surgery. In Medicine Meets Virtual Reality; IOS Press: Amsterdam, The Netherlands, 2012; pp. 129–135. [Google Scholar]
- Puangmali, P.; Althoefer, K.; Seneviratne, L.D.; Murphy, D.; Dasgupta, P. State-of-the-art in force and tactile sensing for minimally invasive surgery. IEEE Sens. J. 2008, 8, 371–381. [Google Scholar] [CrossRef]
- Cutler, N.; Balicki, M.; Finkelstein, M.; Wang, J.; Gehlbach, P.; McGready, J.; Iordachita, I.; Taylor, R.; Handa, J.T. Auditory force feedback substitution improves surgical precision during simulated ophthalmic surgery. Investig. Ophthalmol. Vis. Sci. 2013, 54, 1316–1324. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, E.R. The Psychology of Learning; Harper: Oxford, UK, 1952. [Google Scholar]
- Elliott, D.; Grierson, L.E.; Hayes, S.J.; Lyons, J. Action representations in perception, motor control and learning: implications for medical education. Med. Educ. 2011, 45, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Elliott, D.; Hansen, S.; Mendoza, J.; Tremblay, L. Learning to optimize speed, accuracy, and energy expenditure: a framework for understanding speed-accuracy relations in goal-directed aiming. J. Mot. Behav. 2004, 36, 339–351. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, F.; Sinigaglia, S.; Megali, G.; Pietrabissa, A.; Dario, P.; Mosca, F.; Cuschieri, A. Biomechanics–machine learning system for surgical gesture analysis and development of technologies for minimal access surgery. Surg. Innov. 2014, 21, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Poursartip, B.; LeBel, M.E.; Patel, R.V.; Naish, M.D.; Trejos, A.L. Energy-based metrics for laparoscopic skills assessment. In Proceedings of the 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 2648–2651. [Google Scholar]
- Poursartip, B.; LeBel, M.E.; Patel, R.V.; Naish, M.D.; Trejos, A.L. Analysis of energy-based metrics for laparoscopic skills assessment. Accepted for publication in the IEEE Transactions on Biomedical Engineering 2017. Available online: http://ieeexplore.ieee.org/document/7932145 (accessed on 19 May 2017).
- Ahmidi, N.; Poddar, P.; Jones, J.D.; Vedula, S.S.; Ishii, L.; Hager, G.D.; Ishii, M. Automated objective surgical skill assessment in the operating room from unstructured tool motion in septoplasty. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 981–991. [Google Scholar] [CrossRef] [PubMed]
- Horeman, T.; Dankelman, J.; Jansen, F.W.; van den Dobbelsteen, J.J. Assessment of laparoscopic skills based on force and motion parameters. IEEE Trans. Biomed. Eng. 2014, 61, 805–813. [Google Scholar] [CrossRef] [PubMed]
- Chmarra, M.K.; Klein, S.; de Winter, J.C.; Jansen, F.W.; Dankelman, J. Objective classification of residents based on their psychomotor laparoscopic skills. Surg. Endosc. 2010, 24, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Richstone, L.; Schwartz, M.J.; Seideman, C.; Cadeddu, J.; Marshall, S.; Kavoussi, L.R. Eye metrics as an objective assessment of surgical skill. Ann. Surg. 2010, 252, 177–182. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.C. Development of a Physical Shoulder Simulator for the Training of Basic Arthroscopic Skills. Master’s Thesis, Biomedical Engineering Program, Western University, London, ON, Canada, 2015. [Google Scholar]
- Bishop, C. Pattern Recognition and Machine Learning (Information Science and Statistics), 2nd ed.; Springer: New York, NY, USA, 2007. [Google Scholar]
- Xu, S.; Chen, L. A novel approach for determining the optimal number of hidden layer neurons for FNN’s and its application in data mining. In Proceedings of the 5th International Conference on Information Technology and Applications (ICITA), Cairns, Queensland, Australia, 23–26 June 2008; pp. 683–686. [Google Scholar]
- Reiley, C.E.; Hager, G.D. Decomposition of robotic surgical tasks: An analysis of subtasks and their correlation to skill. In M2CAI Workshop; MICCAI: London, UK, 2009. [Google Scholar]
- Despinoy, F.; Bouget, D.; Forestier, G.; Penet, C.; Zemiti, N.; Poignet, P.; Jannin, P. Unsupervised trajectory segmentation for surgical gesture recognition in robotic training. IEEE Trans. Biomed. Eng. 2016, 63, 1280–1291. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Jog, A.; Malpani, A.; Vagvolgyi, B.; Yuh, D.; Nguyen, H.; Hager, G.; Chen, C.C.G. Assessing system operation skills in robotic surgery trainees. Int. J. Med. Robot. Comput. Assist. Surg. 2012, 8, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Poursartip, B.; McCracken, L.; Escoto, A.; Patel, R.; LeBel, M.; Trejos, A.; Naish, M. Development and evaluation of a sensorized shoulder simulator. In Proceedings of the 30th Canadian Conference of the IEEE Electrical and Computer Engineering (CCECE), Windsor, ON, Canada, 1–3 May 2017. [Google Scholar]
- Bodwell, J.A.; Mahurin, R.K.; Waddle, S.; Price, R.; Cramer, S.C. Age and features of movement influence motor overflow. J. Am. Geriatr. Soc. 2003, 51, 1735–1739. [Google Scholar] [CrossRef] [PubMed]
- Addamo, P.K.; Farrow, M.; Bradshaw, J.L.; Georgiou-Karistianis, N. Relative or absolute? Implications and consequences of the measures adopted to investigate motor overflow. J. Mot. Behav. 2011, 43, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Horeman, T.; Tuijthof, G.; Wulms, P.; Kerkhoffs, G.; Gerards, R.; Karahan, M. A Force Measurement System for Training of Arthroscopic Tissue Manipulation Skills on Cadaveric Specimen. J. Med. Devices 2016, 10, 044508. [Google Scholar] [CrossRef]
- Trejos, A.L.; Patel, R.V.; Malthaner, R.A.; Schlachta, C.M. Development of force-based metrics for skills assessment in minimally invasive surgery. Surg. Endosc. 2014, 28, 2106–2119. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Task | Instrument | Arthroscope | Instrument and Athroscope | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Novices | Experts | Total | Novices | Experts | Total | Novices | Experts | Total | |
| 1 | 16 | 4 | 20 | 15 | 5 | 20 | 14 | 4 | 18 |
| 2 | 18 | 5 | 23 | 17 | 6 | 23 | 15 | 5 | 20 |
| 3 | 16 | 4 | 20 | 12 | 4 | 16 | 12 | 4 | 16 |
| Task 1 | Task 2 | Task 3 | ||||||
|---|---|---|---|---|---|---|---|---|
| Metric | Level | Mean ± SD | p value | Mean ± SD | p value | Mean ± SD | p value | |
| Instrument | Novice | 5.87 ± 4.47 | 0.001 | 5.15 ± 3.26 | <0.001 | 5.22 ± 5.55 | 0.002 | |
| Expert | 0.88 ± 0.44 | 1.18 ± 0.60 | 1.10 ± 0.17 | |||||
| Novice | 6.24 ± 4.65 | <0.001 † | 5.92 ± 4.12 | 0.001 | 6.92 ± 6.98 | 0.022 | ||
| Expert | 1.07 ± 0.51 | 1.37 ± 0.74 | 1.84 ± 1.29 | |||||
| Novice | 145.35 ± 127.06 | 0.014 † | 8.05 ± 10.15 | 0.199 * | 5.10 ± 3.33 | 0.003 † | ||
| Expert | 50.56 ± 29.24 | 2.41 ± 2.65 | 1.95 ± 0.78 | |||||
| Novice | 29.43 ± 22.71 | <0.001 † | 9.92 ± 10.16 | 0.007 | 7.64 ± 7.89 | 0.001 | ||
| Expert | 3.49 ± 1.32 | 2.68 ± 2.52 | 0.53 ± 0.21 | |||||
| Arthroscope | Novice | 11.89 ± 9.35 | 0.001 † | 7.07 ± 6.10 | 0.024 | 8.34 ± 8.02 | 0.001 | |
| Expert | 1.59 ± 0.79 | 2.34 ± 1.93 | 2.23 ± 1.56 | |||||
| Novice | 10.72 ± 8.74 | 0.011 | 6.44 ± 5.47 | 0.002 | 8.38 ± 8.56 | 0.001 | ||
| Expert | 1.40 ± 0.77 | 1.58 ± 0.79 | 1.84 ± 1.88 | |||||
| Novice | 17.23 ± 23.34 | 0.042 | 10.95 ± 19.03 | 0.062 * | 10.46 ± 11.53 | 0.002 | ||
| Expert | 1.56 ± 0.79 | 1.44 ± 1.36 | 1.09 ± 1.10 | |||||
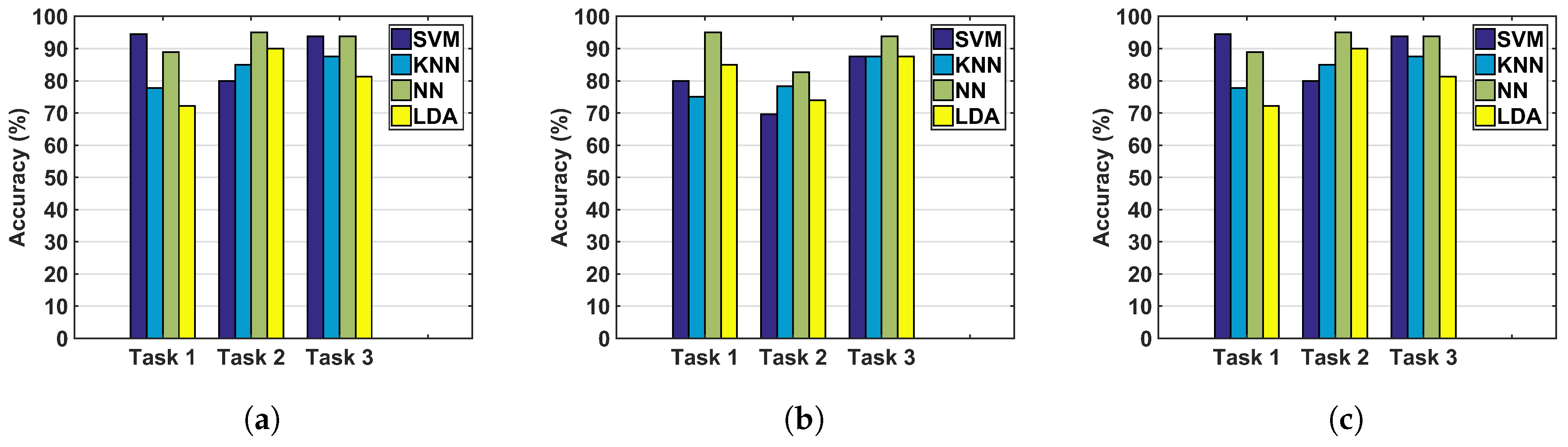
| Task | Classifier | Accuracy | Precision | Recall | F1 score |
|---|---|---|---|---|---|
| 1 | SVM | 94.44 | 80.00 | 100.00 | 88.89 |
| KNN | 77.78 | 50.00 | 75.00 | 60.0 | |
| NN | 88.89 | 75.00 | 75.00 | 75.00 | |
| LDA | 72.22 | 42.85 | 75.00 | 54.55 | |
| 2 | SVM | 80.00 | 57.14 | 80.00 | 66.67 |
| KNN | 85.00 | 75.00 | 60.00 | 66.67 | |
| NN | 95.00 | 100.00 | 80.00 | 88.89 | |
| LDA | 90.00 | 80.00 | 80.00 | 80.00 | |
| 3 | SVM | 93.75 | 80.00 | 100.00 | 88.89 |
| KNN | 87.50 | 66.67 | 100.00 | 80.00 | |
| NN | 93.75 | 80.00 | 100.00 | 88.89 | |
| LDA | 81.25 | 60.00 | 75.00 | 66.67 |
| Task | Classifier | Accuracy | Precision | Recall | F1 score |
|---|---|---|---|---|---|
| 1 | SVM | 66.67 | 25.00 | 25.00 | 25.00 |
| KNN | 61.11 | 0.00 | 0.00 | 0.00 | |
| NN | 83.33 | 66.67 | 50.00 | 57.14 | |
| LDA | 88.89 | 75.00 | 75.00 | 75.00 | |
| 2 | SVM | 80.00 | 66.67 | 40.00 | 50.00 |
| KNN | 75.00 | 50.00 | 20.00 | 28.57 | |
| NN | 95.00 | 100.00 | 80.00 | 88.89 | |
| LDA | 80.00 | 100.00 | 20.00 | 33.33 | |
| 3 | SVM | 81.25 | 60.00 | 75.00 | 66.67 |
| KNN | 87.50 | 75.00 | 75.00 | 75.00 | |
| NN | 93.75 | 100.00 | 75.00 | 85.71 | |
| LDA | 87.50 | 100.00 | 50.00 | 66.67 |
| Classifier | SVM | KNN | NN | LDA |
|---|---|---|---|---|
| Running time (s) (Mean ± SD) | 0.969 ± 0.028 | 0.866 ± 0.039 | 3.290 ± 0.452 | 1.015 ± 0.033 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poursartip, B.; LeBel, M.-E.; McCracken, L.C.; Escoto, A.; Patel, R.V.; Naish, M.D.; Trejos, A.L. Energy-Based Metrics for Arthroscopic Skills Assessment. Sensors 2017, 17, 1808. https://doi.org/10.3390/s17081808
Poursartip B, LeBel M-E, McCracken LC, Escoto A, Patel RV, Naish MD, Trejos AL. Energy-Based Metrics for Arthroscopic Skills Assessment. Sensors. 2017; 17(8):1808. https://doi.org/10.3390/s17081808
Chicago/Turabian StylePoursartip, Behnaz, Marie-Eve LeBel, Laura C. McCracken, Abelardo Escoto, Rajni V. Patel, Michael D. Naish, and Ana Luisa Trejos. 2017. "Energy-Based Metrics for Arthroscopic Skills Assessment" Sensors 17, no. 8: 1808. https://doi.org/10.3390/s17081808
APA StylePoursartip, B., LeBel, M. -E., McCracken, L. C., Escoto, A., Patel, R. V., Naish, M. D., & Trejos, A. L. (2017). Energy-Based Metrics for Arthroscopic Skills Assessment. Sensors, 17(8), 1808. https://doi.org/10.3390/s17081808