An Augmented Reality System Using Improved-Iterative Closest Point Algorithm for On-Patient Medical Image Visualization



Abstract
:1. Introduction
2. Method
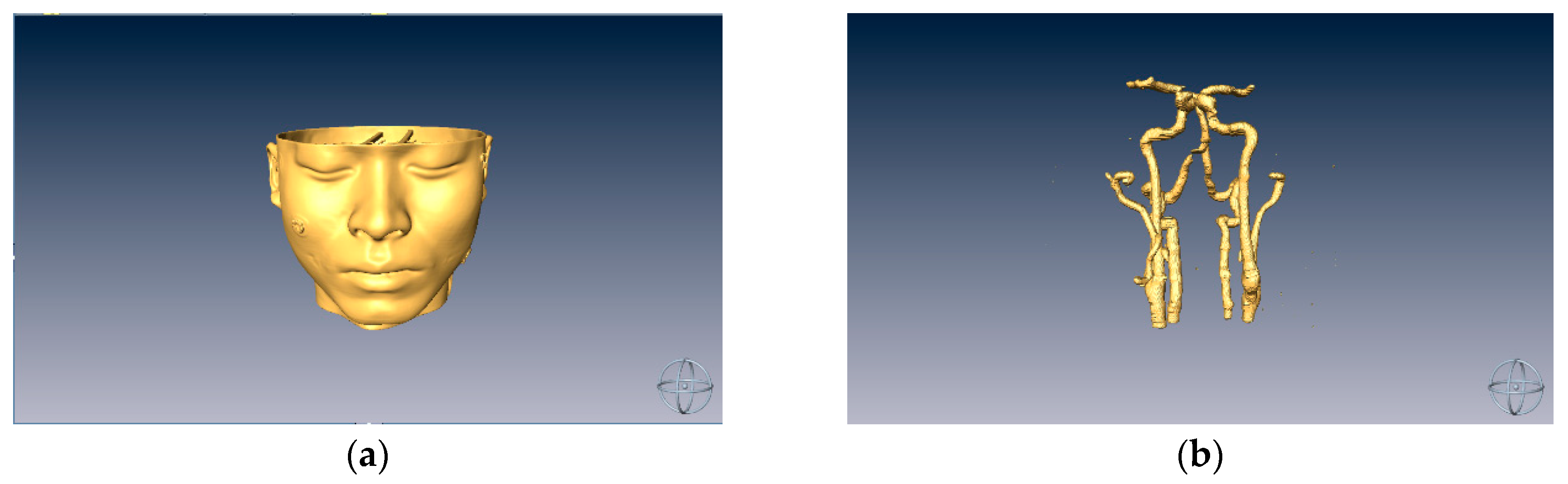
2.1. Modeling from Medical Images
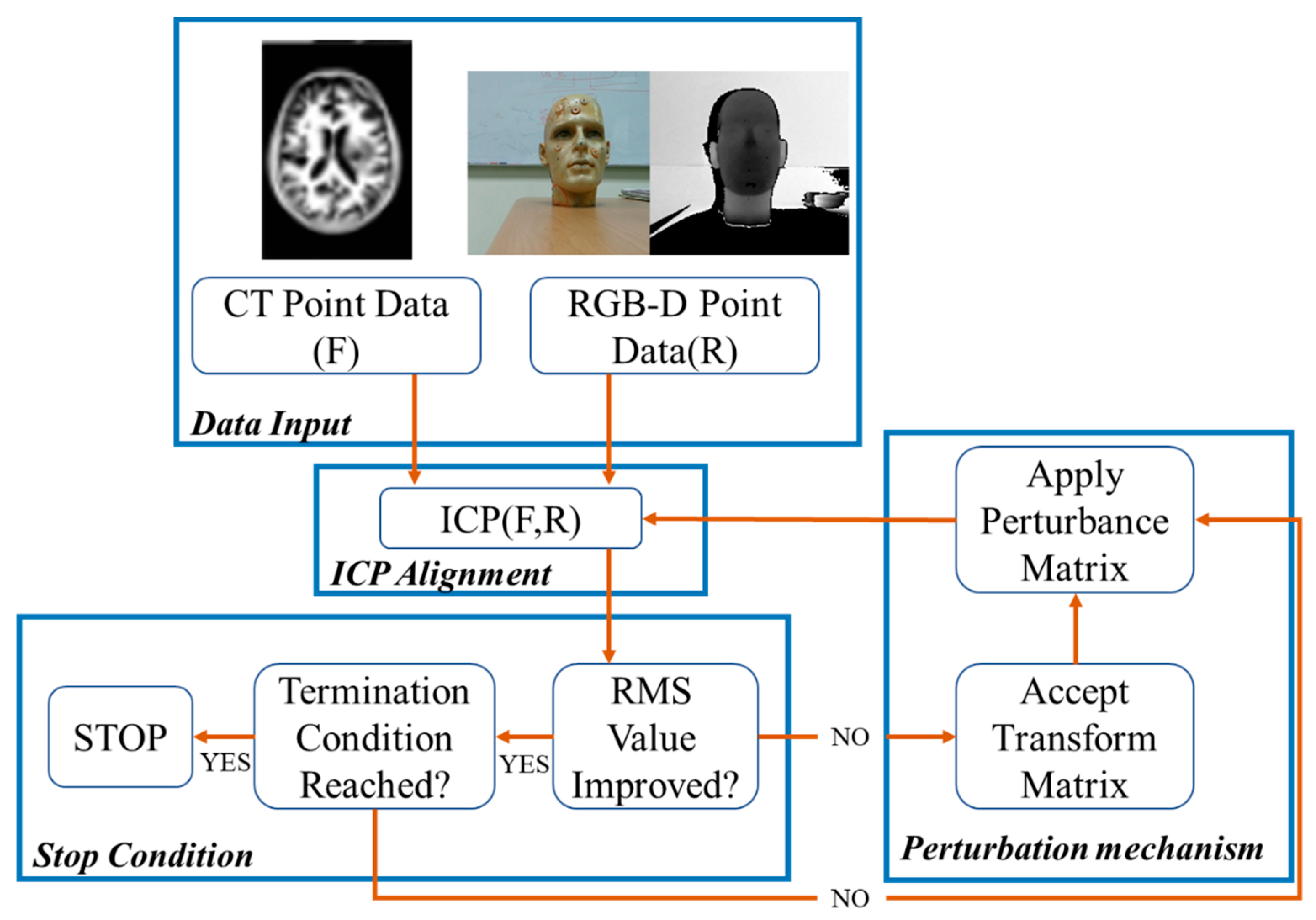
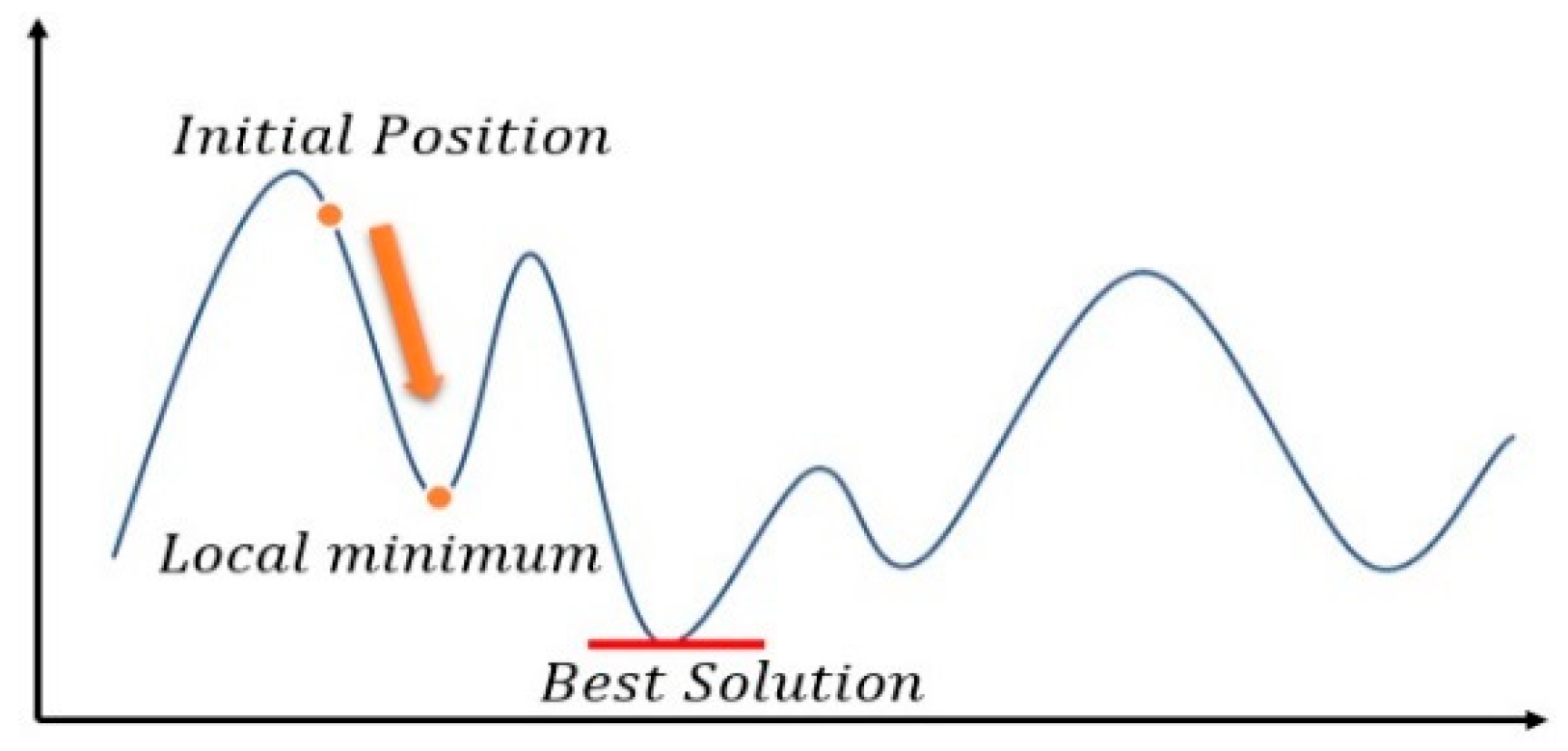
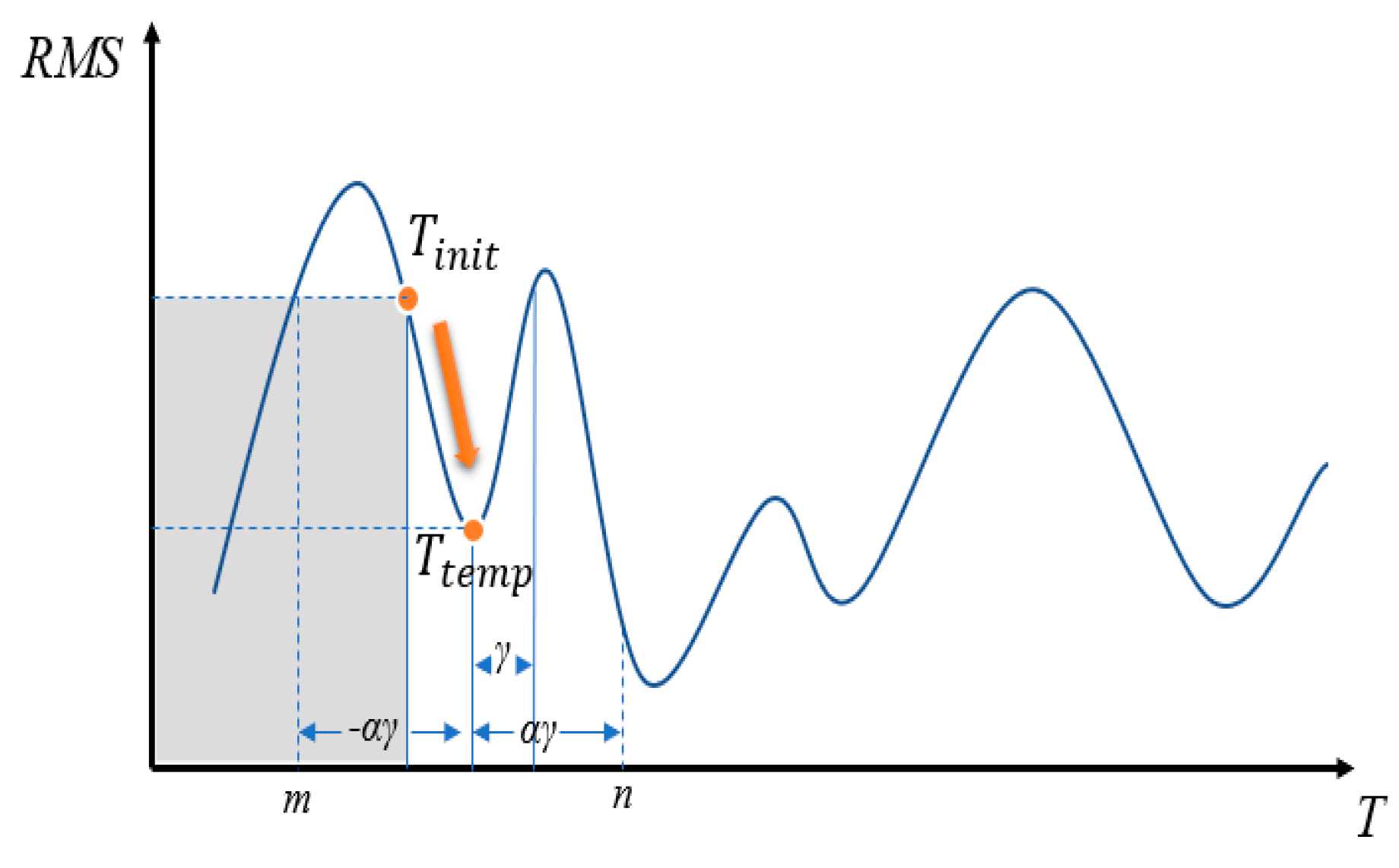
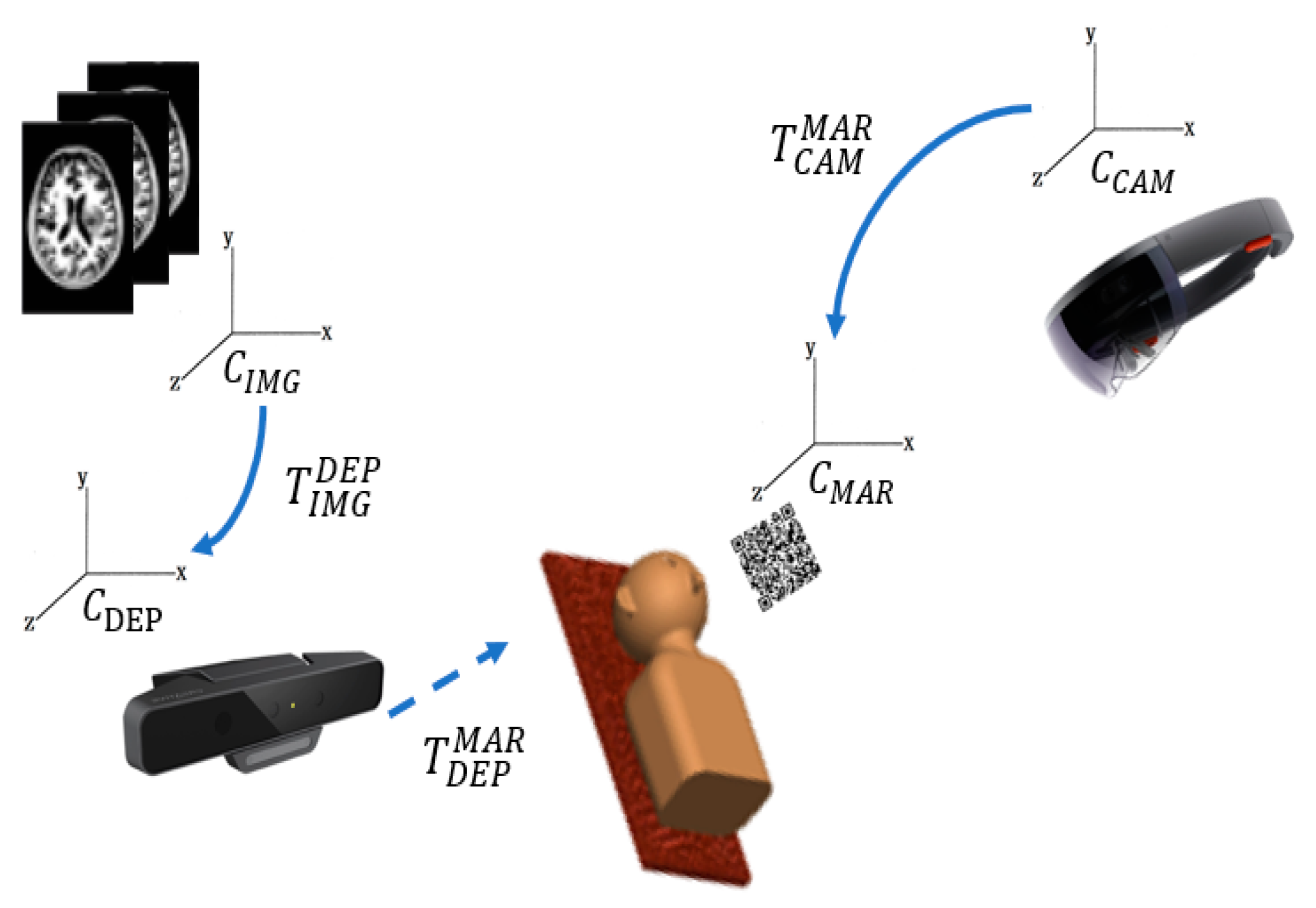
2.2. Surface Data Alignment
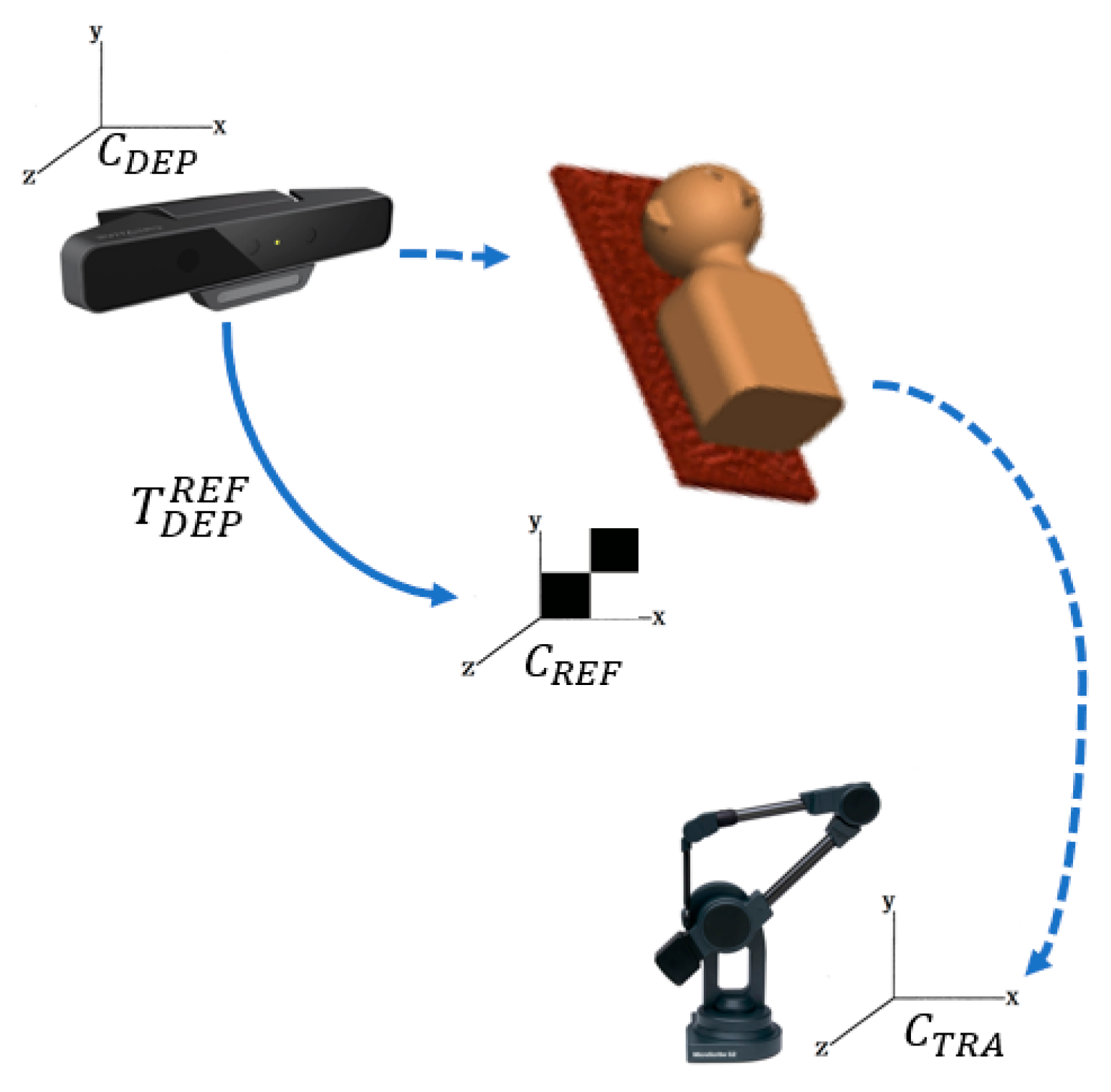
2.3. Detection of the Marker Board
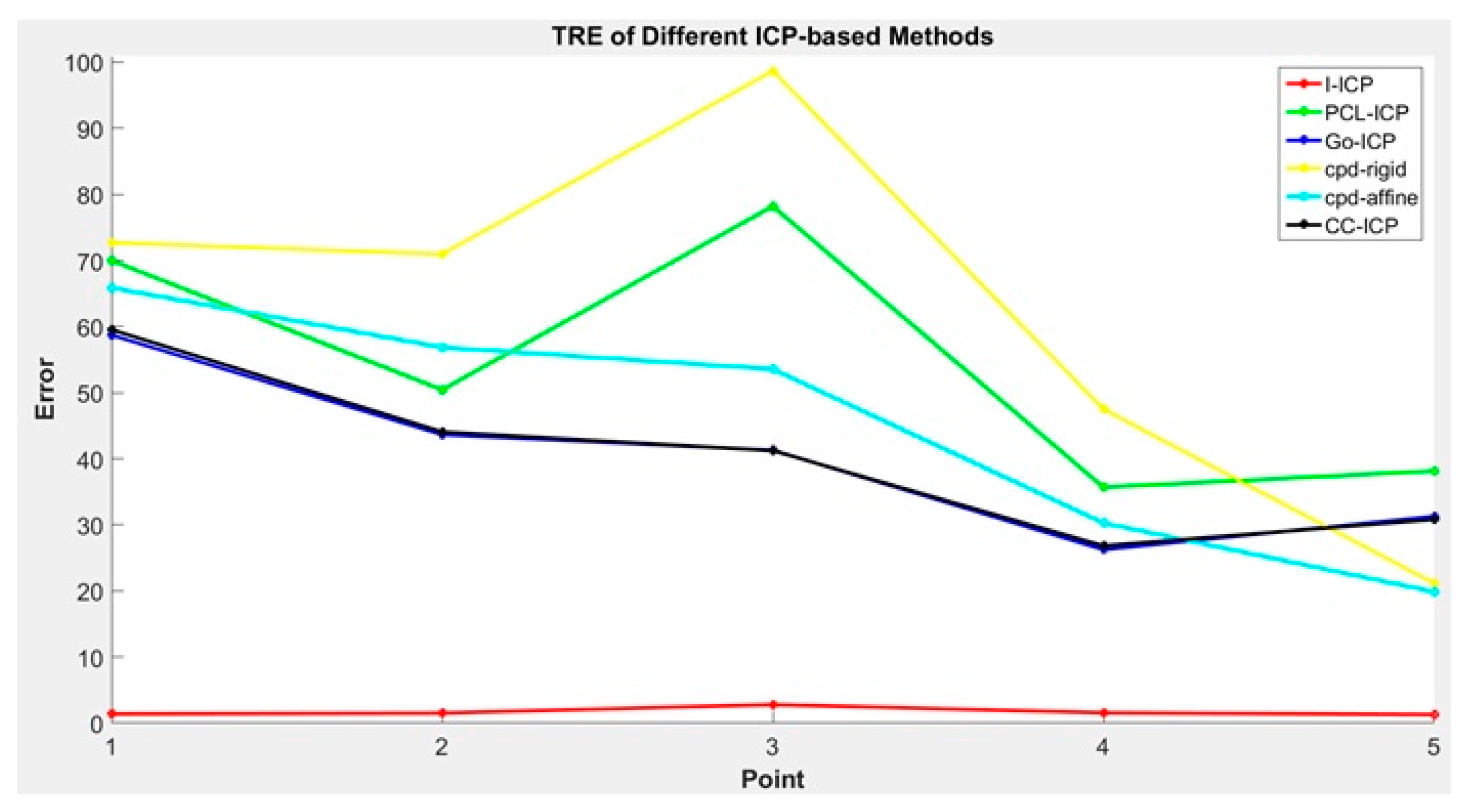
3. Experimental Results
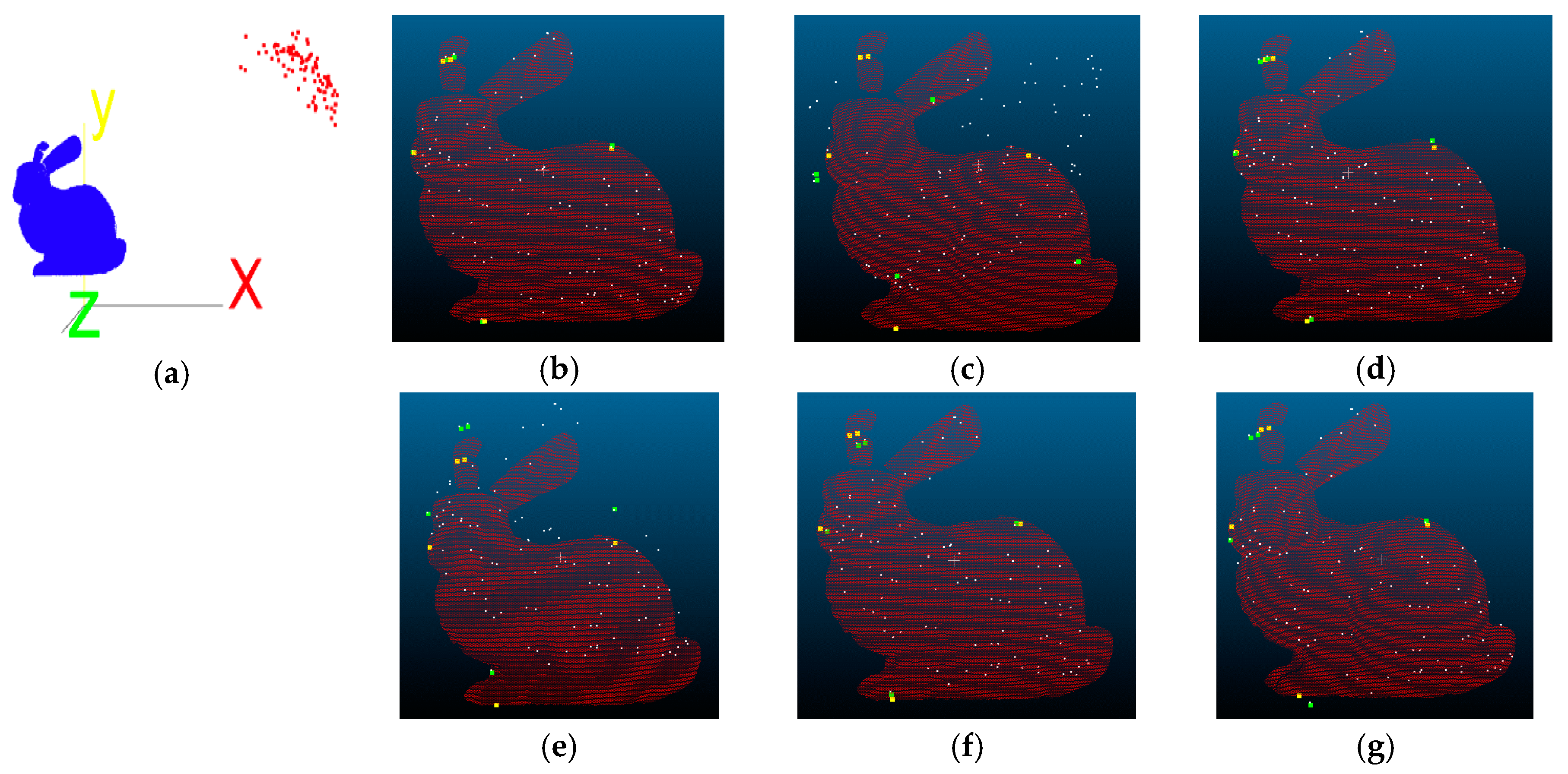
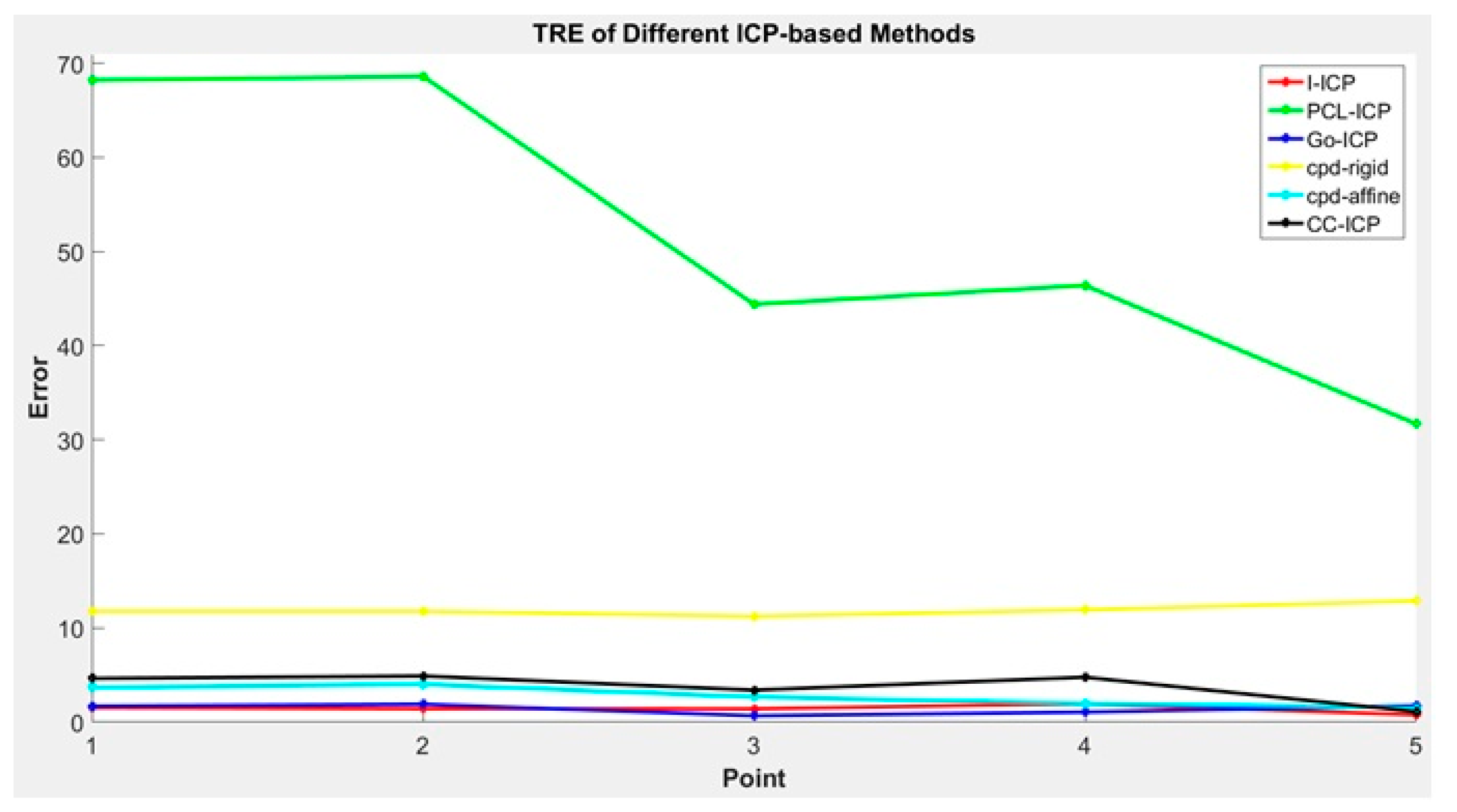
3.1. Alignment Tests Using a Non-Medical Dataset
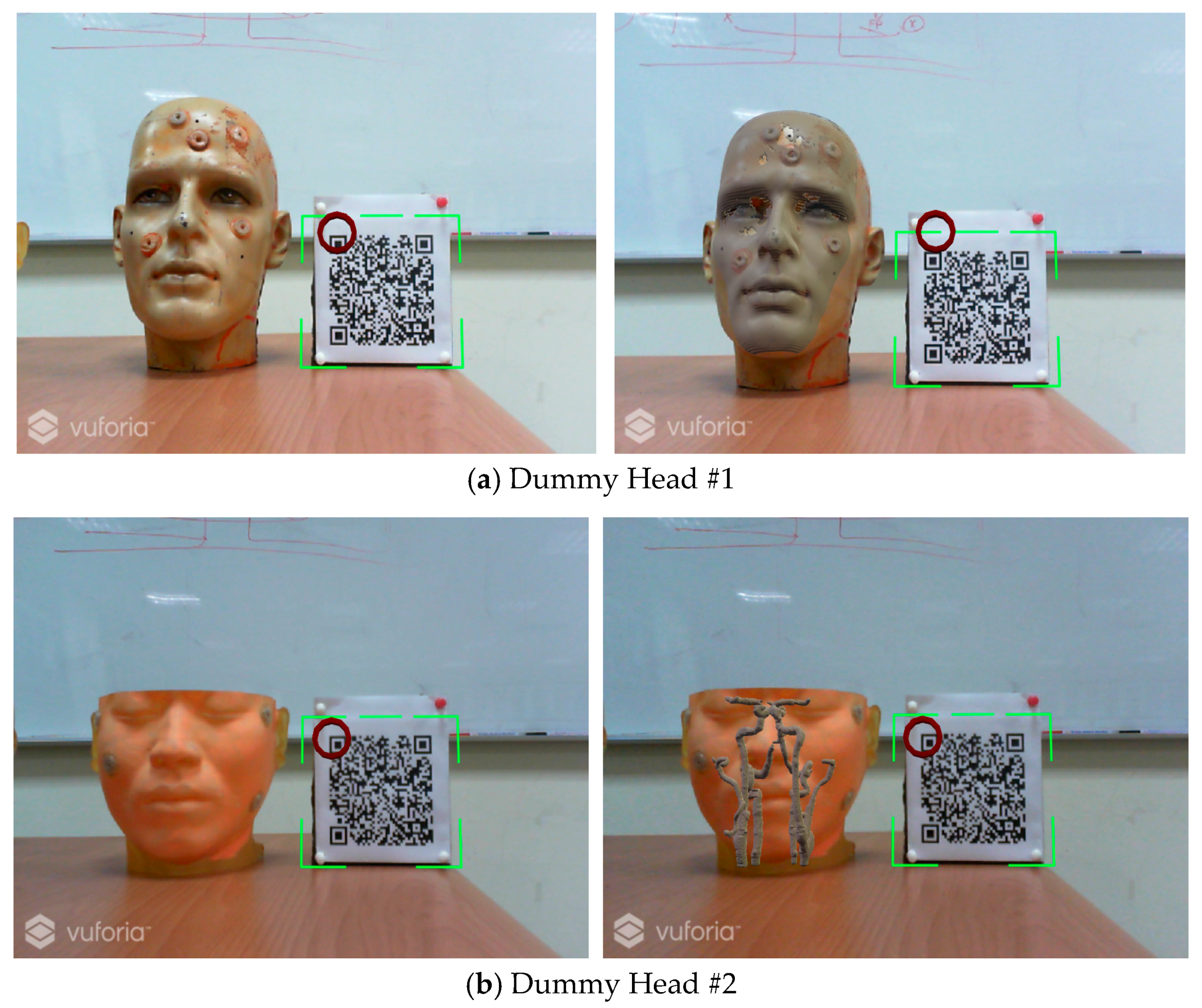
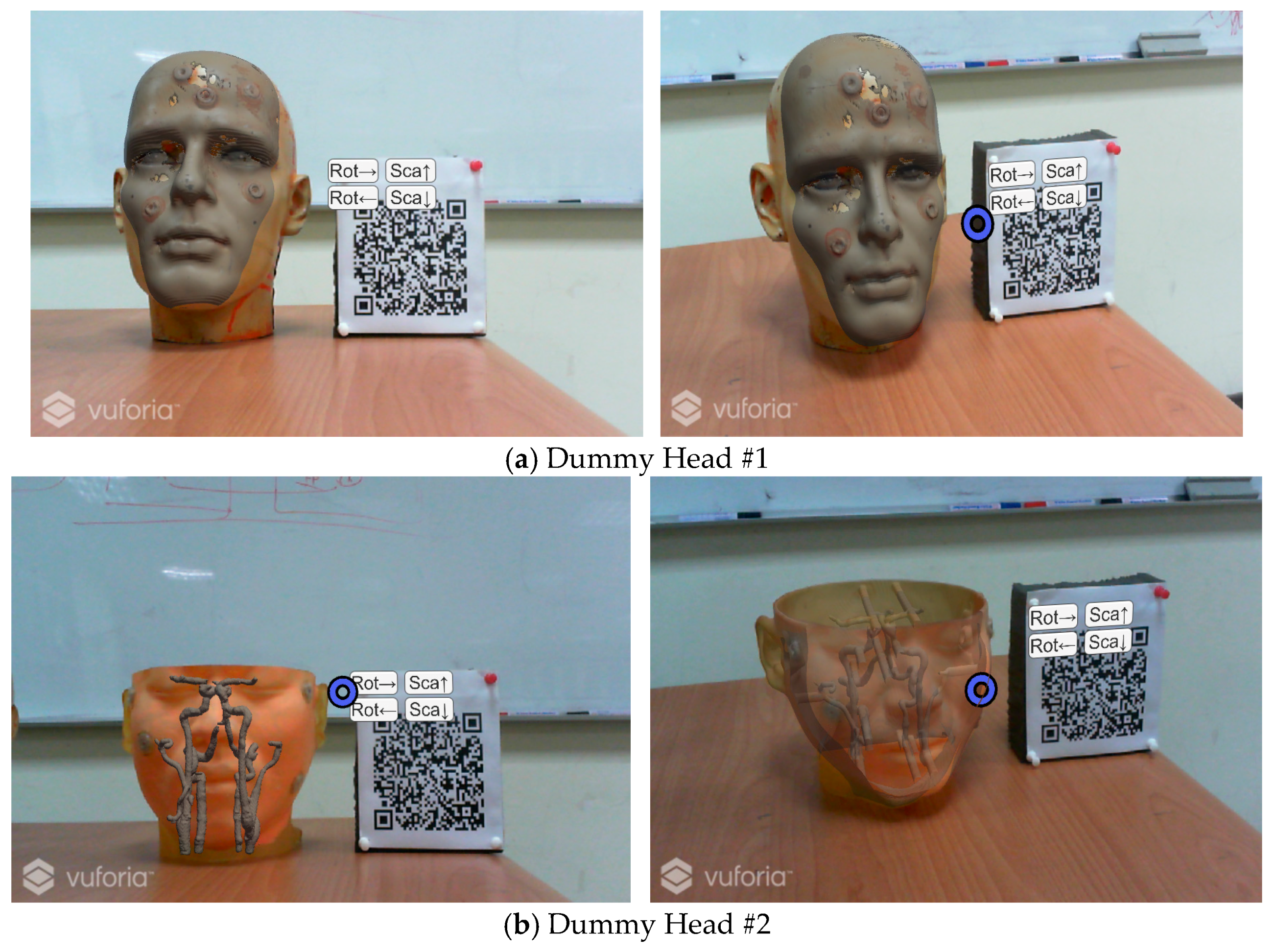
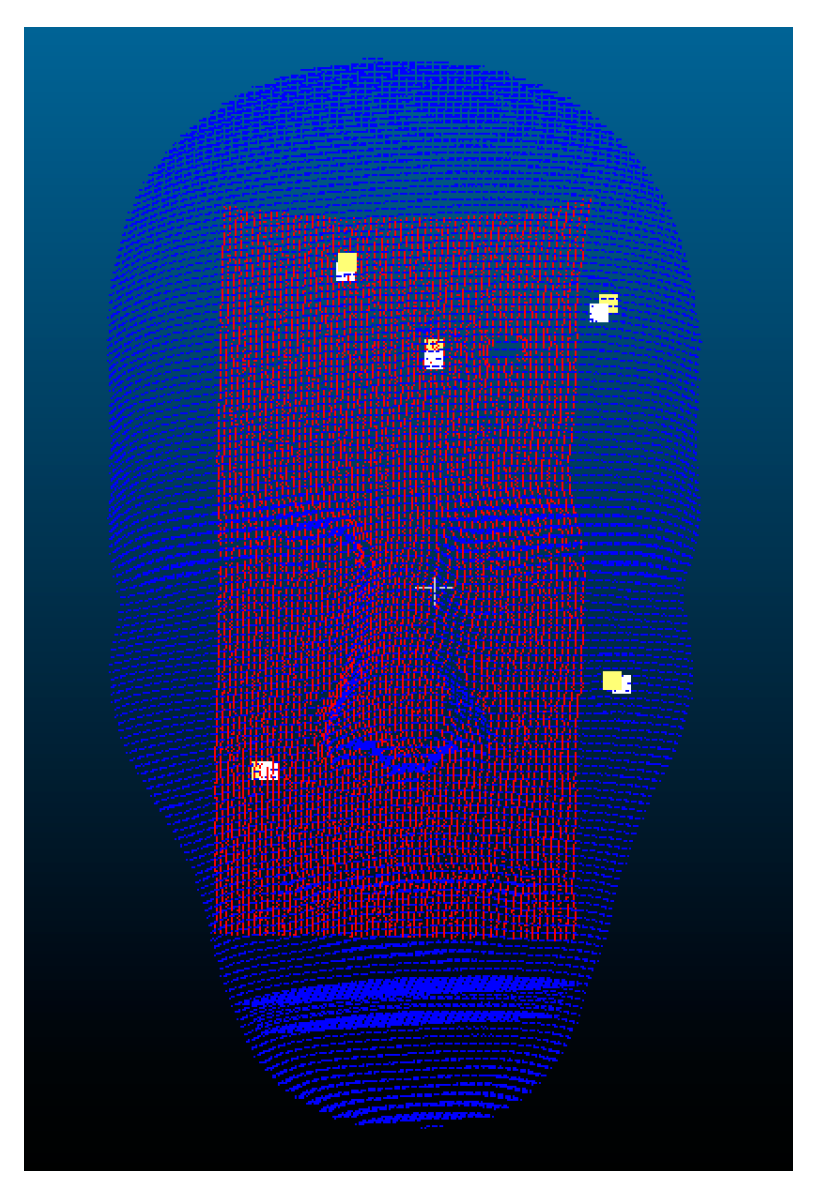
3.2. Dummy Head Alignment Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kundu, S.N.; Muhammad, N.; Sattar, F. Using the augmented reality sandbox for advanced learning in geoscience education. In Proceedings of the 2017 IEEE 6th International Conference on Teaching, Assessment, and Learning for Engineering (TALE), Hong Kong, China, 12–14 December 2018; pp. 13–17. [Google Scholar]
- Ashfaq, Q.; Sirshar, M. Emerging trends in augmented reality games. Computing, Mathematics and Engineering Technologies. In Proceedings of the 2018 International Conference on Computing, Mathematics and Engineering Technologies (iCoMET), Sukkur, Pakistan, 3–4 March 2018; pp. 1–7. [Google Scholar]
- Hamacher, A.; Kim, S.J.; Cho, S.T.; Pardeshi, S.; Lee, S.H.; Eun, S.J.; Whangbo, T.K. Application of Virtual, Augmented, and Mixed Reality to Urology. Int. Neurourol. J. 2016, 20, 172–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virtual Reality. Available online: https://www.wareable.com/vr/how-does-vr-work-explained (accessed on 16 February 2018).
- Traub, J.; Sielhorst, T.; Heining, S.; Navab, N. Advanced Display and Visualization Concepts for Image Guided Surgery. J. Disp. Technol. 2008, 4, 483–490. [Google Scholar] [CrossRef]
- Kersten-Oertel, M.; Gerard, I.J.; Drouin, S.; Mok, K.; Sirhan, D.; Sinclair, D.S.; Collins, D.L. Augmented Reality for Specific Neurovascular Tasks; Springer: Cham, Switzerland, 2015. [Google Scholar]
- Deng, W.; Li, F.; Wang, M.; Song, Z. Multi-mode navigation in image-guided neurosurgery using a wireless tablet PC. Austral. Phys. Eng. Sci. Med. 2014, 37, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Macedo, M.C.F.; Apolinário, A.L.; Souza, A.C.S.; Giraldi, G.A. A Semi-Automatic Markerless Augmented Reality Approach for On-Patient Volumetric Medical Data Visualization. In Proceedings of the 2014 XVI Symposium on Virtual and Augmented Reality, Piata Salvador, Brazil, 12–15 May 2014; pp. 63–70. [Google Scholar]
- Hu, L.; Wang, M.; Song, Z. A Convenient Method of Video See-Through Augmented Reality Based on Image-Guided Surgery System. In Proceedings of the Internet Computing for Engineering and Science (ICICSE), Shanghai, China, 20–22 December 2013; pp. 100–103. [Google Scholar]
- Larrarte, E.; Alban, A. Virtual markers in virtual laparoscopy surgery. In Proceedings of the Signal Processing, Images and Artificial Vision, Bucaramanga, Colombia, 31 August–2 September 2016; pp. 1–6. [Google Scholar]
- HoloLens Mixed Reality Surgery: Holographic Augmented Mixed Reality Navigation. Available online: https://www.youtube.com/watch?v=qLGD570I1OE/ (accessed on 27 November 2017).
- Holographic Assisted Spine Surgery with Hololens. Available online: https://www.youtube.com/watch?v=zC5097mA9f4/ (accessed on 27 November 2017).
- Xie, T.; Islam, M.M.; Lumsden, A.B.; Kakadiaris, I.A. Holographic iRay: Exploring Augmentation for Medical Applications. In Proceedings of the 2017 IEEE International Symposium on Mixed and Augmented Reality Adjunct Proceedings, Nantes, France, 9–13 October 2017; pp. 220–222. [Google Scholar]
- Besl, P.J.; McKay, N.D. A method for registration of 3-D shapes. Int. Soc. Opt. Photonics 1992, 14, 239–256. [Google Scholar] [CrossRef]
- Zhang, Z. Iterative point matching for registration of free-form curves and surfaces. Int. J. Comput. Vis. 1994, 13, 119–152. [Google Scholar] [CrossRef] [Green Version]
- Lu, S.; Lin, X.; Han, X. Virtual-Real Registration of Augmented Reality Technology Used in the Cerebral Surgery Lesion Localization. In Proceedings of the Instrumentation and Measurement, Computer, Communication and Control, Qinhuangdao, China, 18–20 September 2015; pp. 620–625. [Google Scholar]
- Penney, G.P.; Edwards, P.J.; King, A.P.; Blackall, J.M.; Batchelor, P.G.; Hawkes, D.J. A Stochastic Iterative Closest Point Algorithm (stochastICP). In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Berlin/Heidelberg, Germany, 2001; pp. 762–769. [Google Scholar]
- Myronenko, A.; Song, X. Point Set Registration Coherent Point Drift. IEEE Trans. Pattern Anal. Mach. Intell. 2010, 32, 2262–2275. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Li, H.; Campbell, D.; Jia, Y. Go-ICP: A Globally Optimal Solution to 3D ICP Point-Set Registration. IEEE Trans. Pattern Anal. Mach. Intell. 2015, 38, 2241–2254. [Google Scholar] [CrossRef] [PubMed]
- OpenCV. Available online: https://opencv.org/ (accessed on 1 October 2016).
- PCL-Point Cloud Library. Available online: http://docs.pointclouds.org/trunk/group__registration.html/ (accessed on 16 June 2017).
- Glocker, B.; Shotton, J.; Criminisi, A.; Izadi, S. Real-Time RGB-D Camera Relocalization via Randomized Ferns for Keyframe Encoding. IEEE Trans. Vis. Comput. Gr. 2014, 21, 571–583. [Google Scholar] [CrossRef] [PubMed]
- PCL-Point Cloud Library. Available online: http://pointclouds.org/ (accessed on 16 June 2017).
- Lehiani, Y.; Maidi, M.; Preda, M.; Ghorbel, F. Object identification and tracking for steady registration in mobile augmented reality. In Proceedings of the IEEE International Conference on Signal and Image Processing Applications, Kuala Lumpur, Malaysia, 19–21 October 2016; pp. 54–59. [Google Scholar]
- Li, F.; Stoddart, D.; Hitchens, C. Method to automatically register scattered point clouds based on principal pose estimation. Opt. Eng. 2017, 56. [Google Scholar] [CrossRef]
- Chetverikov, D.; Stepanov, D.; Krsek, P. Robust Euclidean alignment of 3D point sets: The trimmed iterative closest point algorithm. Image Vis. Comput. Comp. 2005, 23, 299–309. [Google Scholar] [CrossRef]
- Vuforia. Available online: https://developer.vuforia.com/ (accessed on 13 September 2017).
- ARToolkit. Available online: https://www.artoolkit.org/ (accessed on 8 March 2017).
- Hololens. Coordinate. Available online: https://docs.microsoft.com/en-us/windows/mixed-reality/coordinate-systems (accessed on 3 October 2017).
- Hololens. Available online: https://www.microsoft.com/en-us/hololens/ (accessed on 31 August 2017).
- Hololens. Spatial Mapping. Available online: https://docs.microsoft.com/zh-tw/windows/mixed-reality/spatial-mapping/ (accessed on 5 December 2017).
- Izadi, S.; Kim, D.; Hilliges, O.; Molyneaux, D.; Newcombe, R.; Kohli, P.; Shotton, J.; Hodges, S.; Freeman, D.; Davison, A.; et al. KinectFusion: Real-time 3D reconstruction and interaction using a moving depth camera. In Proceedings of the 2011 24th Annual ACM Symposium on User Interface Software and Technology, Santa Barbara, CA, USA, 16–19 October 2011; pp. 5559–5568. [Google Scholar]
- Newcombe, R.A.; Izadi, S.; Hilliges, O.; Molyneaux, D.; Kim, D.; Davison, A.J.; Kohi, P.; Shotton, J.; Hodges, S.; Fitzgibbon, A. KinectFusion: Real-time dense surface mapping and tracking. Mixed and Augmented Reality. In Proceedings of the 2011 10th IEEE International Symposium on Mixed and Augmented Reality, Basel, Switzerland, 26–29 October 2012; pp. 127–136. [Google Scholar]
- Unity. Available online: https://unity3d.com/ (accessed on 31 August 2017).
- Stanford Bunny. Available online: http://graphics.stanford.edu/data/3Dscanrep/ (accessed on 11 January 2018).
- CloudCompare. Available online: http://www.cloudcompare.org/ (accessed on 24 August 2017).
- Hololens. Gestures. Available online: https://developer.microsoft.com/en-us/windows/mixed-reality/gestures/ (accessed on 5 September 2017).
- MicroScribe G2X Digitizer. Available online: http://www.3d-microscribe.com/G2%20Page.htm/ (accessed on 11 April 2017).
- Rusu, R.B.; Blodow, N.; Beetz, M. Fast Point Feature Histograms (FPFH) for 3D Registration; Robotics and Automation: Kobe, Japan, 2009; pp. 3212–3217. [Google Scholar]
- Shamir, R.R.; Joskowicz, L.; Shoshan, Y. Fiducial Optimization for Minimal Target Registration Error in Image-Guided Neurosurgery. IEEE Trans. Med. Imaging 2011, 31, 725–737. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| I-ICP | PCL-ICP | Go-ICP | CPD-ICP (Rigid) | CPD-ICP (Affine) | CC-ICP | |
|---|---|---|---|---|---|---|
| RMS | 0.0008 | 0.0008 | 0.0007 | 0.0007 | 0.0008 | 0.0003 |
| Run time | 5 s | 75 s | 14 s | 17 s | 20 s | 3 s |
| Method | Axis | Point 1 | Point 2 | Point 3 | Point 4 | Point 5 | Avg. |
|---|---|---|---|---|---|---|---|
| I-ICP | x | 2.02 | 2.23 | −0.27 | −1.05 | 0.38 | 1.19 |
| y | 1.08 | 0.72 | 0.24 | −0.63 | 1.55 | 0.84 | |
| z | −1.51 | −1.34 | −3.73 | −4.22 | 0.38 | 2.23 | |
| PCL-ICP | x | −27.68 | −23.14 | 37.34 | 94.91 | −51.08 | 46.83 |
| y | −47.67 | −49.57 | −58.20 | 37.91 | 26.27 | 43.92 | |
| z | 129.26 | 133.14 | 37.60 | −6.40 | −17.72 | 64.82 | |
| Go-ICP | x | −2.79 | −2.55 | −0.57 | 2.01 | −0.99 | 1.78 |
| y | −0.43 | −0.90 | −0.59 | 0.82 | 3.82 | 1.31 | |
| z | 1.87 | 2.26 | 0.87 | −0.36 | −0.40 | 1.15 | |
| CPD-ICP (rigid) | x | 1.65 | 1.84 | −1.42 | −2.85 | −0.68 | 1.69 |
| y | 19.60 | 19.25 | 19.85 | 19.16 | 20.66 | 19.70 | |
| z | 14.07 | 14.23 | 12.47 | 13.76 | 17.29 | 14.36 | |
| CPD-ICP (affine) | x | 4.14 | 4.56 | 3.52 | −0.51 | −2.46 | 3.04 |
| y | −4.79 | −5.14 | −1.32 | 2.43 | 0.33 | 2.80 | |
| z | 2.14 | 2.35 | −3.19 | −3.03 | 1.73 | 2.49 | |
| CC-ICP | x | −5.99 | −5.73 | −0.57 | 6.65 | −0.47 | 3.88 |
| y | −3.40 | −4.03 | −6.97 | −5.15 | 2.37 | 4.38 | |
| z | 4.55 | 4.96 | 2.67 | −2.54 | −0.48 | 3.04 |
| Registration Method | Axis | Point 1 | Point 2 | Point 3 | Point 4 | Point 5 | Avg. | Time |
|---|---|---|---|---|---|---|---|---|
| I-ICP | x | 2.09 | 0.93 | −4.71 | 3.26 | −2.18 | 2.63 | 7 s |
| y | −1.68 | −2.89 | −2.84 | 0.25 | −0.03 | 1.54 | ||
| z | −0.37 | 0.73 | −0.83 | 1.19 | 1.69 | 0.96 | ||
| PCL-ICP | x | 23.57 | 15.34 | 6.01 | −2.03 | 1.40 | 9.67 | 234 s |
| y | −160.44 | −125.27 | −146.21 | 14.27 | 53.77 | 99.99 | ||
| z | 25.97 | −10.69 | −82.38 | −90.77 | 59.30 | 53.82 | ||
| Go-ICP | x | 43.25 | 42.40 | 18.98 | −13.59 | −2.27 | 24.10 | 176 s |
| y | −126.17 | −85.92 | −100.18 | 55.79 | 77.92 | 89.20 | ||
| z | 6.80 | 2.60 | 4.73 | −9.32 | −13.68 | 7.43 | ||
| CPD-ICP (rigid) | x | 22.37 | 16.68 | 7.12 | 6.84 | 10.16 | 12.63 | 180 s |
| y | −176.52 | −140.46 | −161.69 | −1.51 | 37.43 | 103.5 | ||
| z | −19.17 | −55.71 | −127.24 | −134.20 | 15.87 | 70.44 | ||
| CPD-ICP (affine) | x | 15.53 | 12.78 | −1.19 | −14.25 | −10.57 | 10.86 | 200 s |
| y | −151.02 | −125.56 | −114.06 | 43.91 | 40.88 | 95.09 | ||
| z | −31.05 | −32.24 | −45.41 | −32.71 | −8.13 | 29.91 | ||
| CC-ICP | x | 42.87 | 41.81 | 17.72 | −14.50 | −1.79 | 23.74 | 12 s |
| y | −126.21 | −85.64 | −99.05 | 56.67 | 77.03 | 88.92 | ||
| z | 9.50 | 4.77 | 6.86 | −9.30 | −13.65 | 8.81 |
| Registration Method | Axis | Point 1 | Point 2 | Point 3 | Point 4 | Point 5 | Avg. | Time |
|---|---|---|---|---|---|---|---|---|
| I-ICP | x | 3.04 | 2.13 | −3.08 | 3.71 | −1.31 | 2.65 | 8 s |
| y | −1.09 | −2.33 | −2.36 | 0.78 | 0.68 | 1.45 | ||
| z | 1.62 | 2.49 | 0.95 | 1.78 | 2.15 | 1.80 | ||
| PCL-ICP | x | 4.07 | 2.92 | −2.37 | 5.23 | −0.88 | 3.09 | 138 s |
| y | −0.19 | −1.43 | −1.26 | 1.50 | 0.97 | 1.07 | ||
| z | −0.16 | 0.99 | −0.44 | 1.54 | 1.75 | 0.98 | ||
| CC-ICP | x | −3.90 | −4.69 | −9.75 | −1.38 | −8.03 | 5.55 | 36 s |
| y | 1.81 | 0.47 | 0.57 | 3.47 | 3.20 | 1.90 | ||
| z | 0.50 | 1.53 | 0.05 | 1.34 | 1.58 | 1.00 | ||
| Go-ICP | x | −10.71 | −10.31 | −15.13 | −3.46 | −10.83 | 10.0 | 720 s |
| y | −3.15 | −4.19 | −3.13 | 0.62 | −1.27 | 2.47 | ||
| z | 2.07 | 3.27 | 1.34 | 3.14 | 4.05 | 2.77 | ||
| CPD-ICP (rigid) | x | 6.19 | 5.09 | −0.10 | 7.51 | 1.19 | 4.02 | 840 s |
| y | −2.50 | −3.80 | −3.72 | −0.97 | −1.30 | 2.46 | ||
| z | −10.98 | −9.90 | −11.36 | −9.69 | −9.44 | 10.2 | ||
| CPD-ICP (affine) | x | 3.58 | 2.46 | −3.04 | 4.23 | −1.68 | 3.00 | 6 s |
| y | −0.74 | −1.85 | −2.14 | 1.08 | 1.28 | 1.42 | ||
| z | 1.28 | 1.83 | −0.72 | 0.88 | 3.43 | 1.63 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, M.-L.; Chien, J.-C.; Wu, C.-T.; Lee, J.-D. An Augmented Reality System Using Improved-Iterative Closest Point Algorithm for On-Patient Medical Image Visualization. Sensors 2018, 18, 2505. https://doi.org/10.3390/s18082505
Wu M-L, Chien J-C, Wu C-T, Lee J-D. An Augmented Reality System Using Improved-Iterative Closest Point Algorithm for On-Patient Medical Image Visualization. Sensors. 2018; 18(8):2505. https://doi.org/10.3390/s18082505
Chicago/Turabian StyleWu, Ming-Long, Jong-Chih Chien, Chieh-Tsai Wu, and Jiann-Der Lee. 2018. "An Augmented Reality System Using Improved-Iterative Closest Point Algorithm for On-Patient Medical Image Visualization" Sensors 18, no. 8: 2505. https://doi.org/10.3390/s18082505
APA StyleWu, M. -L., Chien, J. -C., Wu, C. -T., & Lee, J. -D. (2018). An Augmented Reality System Using Improved-Iterative Closest Point Algorithm for On-Patient Medical Image Visualization. Sensors, 18(8), 2505. https://doi.org/10.3390/s18082505