An Inexpensive and Easy to Use Cervical Range of Motion Measurement Solution Using Inertial Sensors

 ,
,  , ,
, ,
Abstract
:1. Introduction
1.1. The Problem of Spinal Disorders and Neck Pain
1.1.1. Diagnosis of Neck Pain
1.1.2. Treatment of Neck Pain
1.2. Objectives
2. Materials and Methods
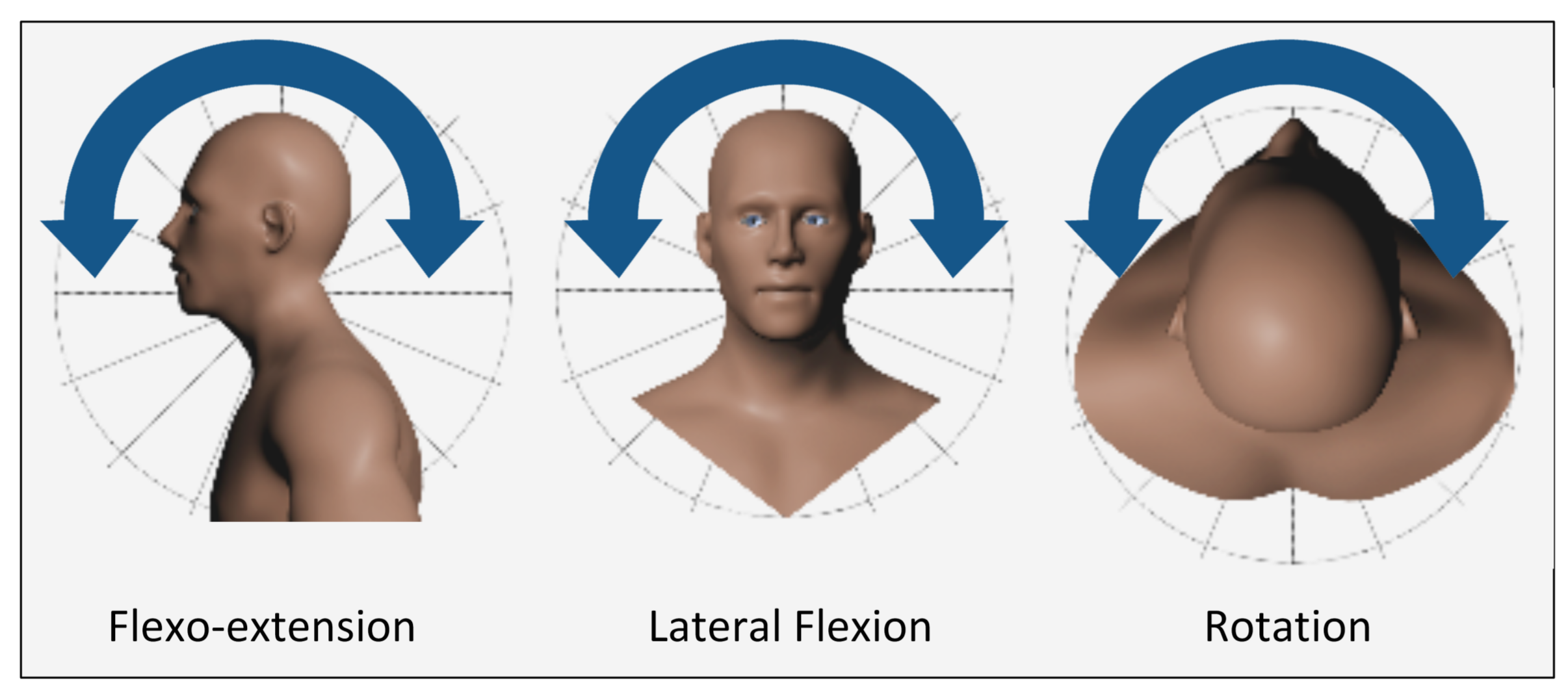
2.1. CROM Measurement
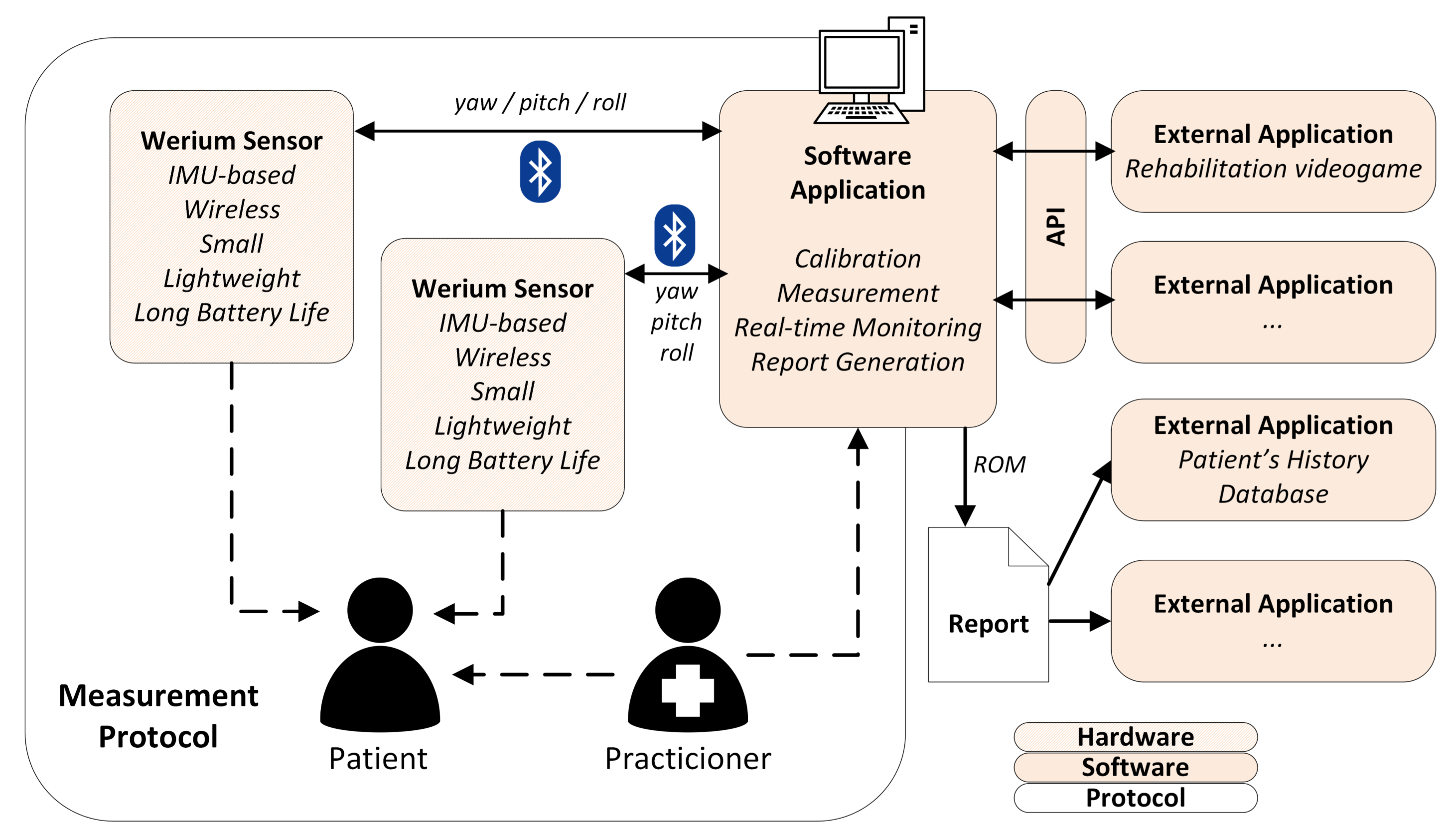
2.2. Proposed Solution
- Complete, out of the box, solution
- High precision, at least as good as the CROM instruments used in the clinical routine
- Easy to use
- Inexpensive
- Suits the needs of clinical practice (it should require less than 10 min (ideally less than 5 min) of complete test time, from setup to report)
- Produces electronic reports with the information that therapists need (CROM in 3 axes)
- Aggregates information from several subjects and multiple measurements from the same subject
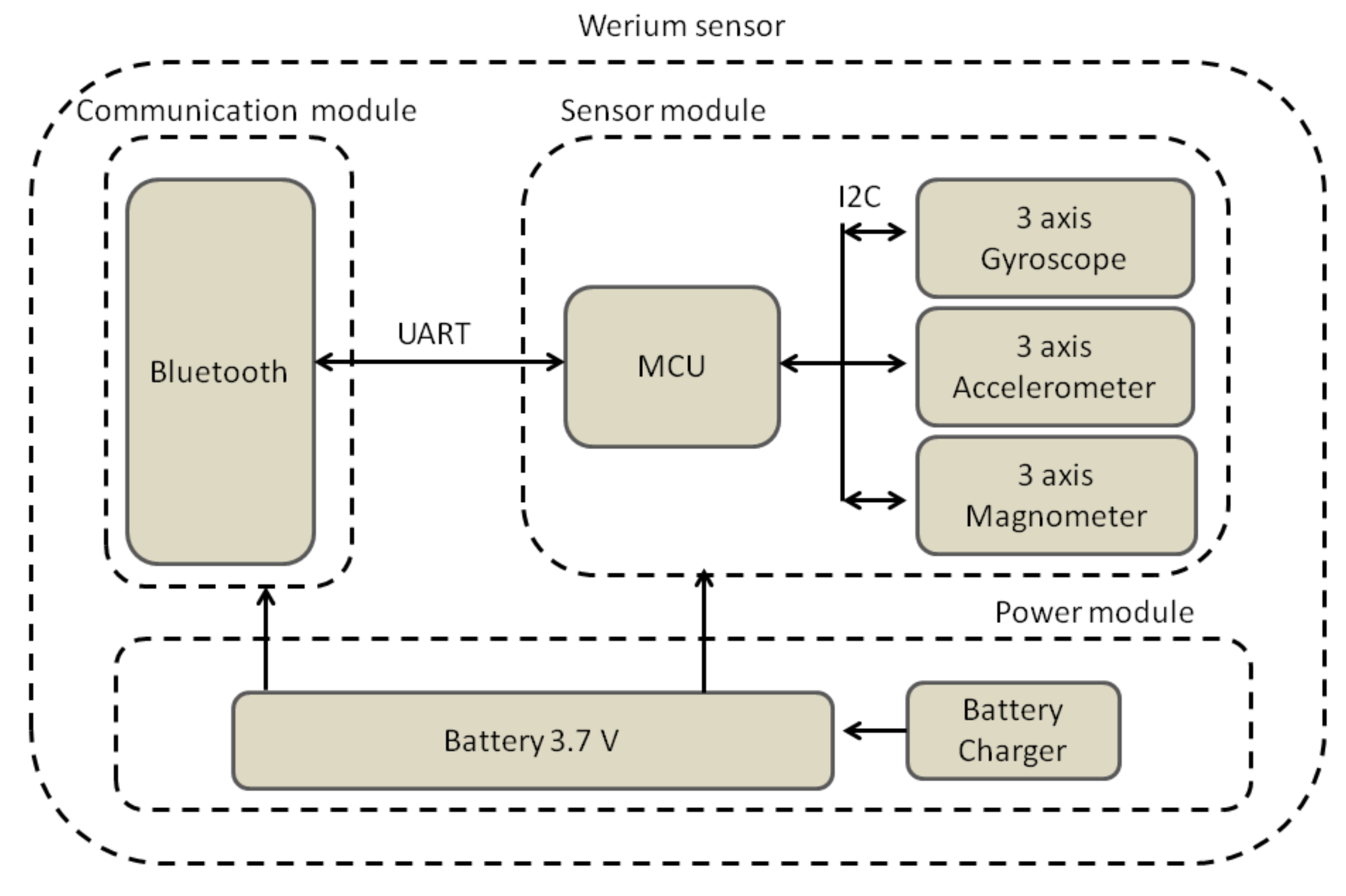
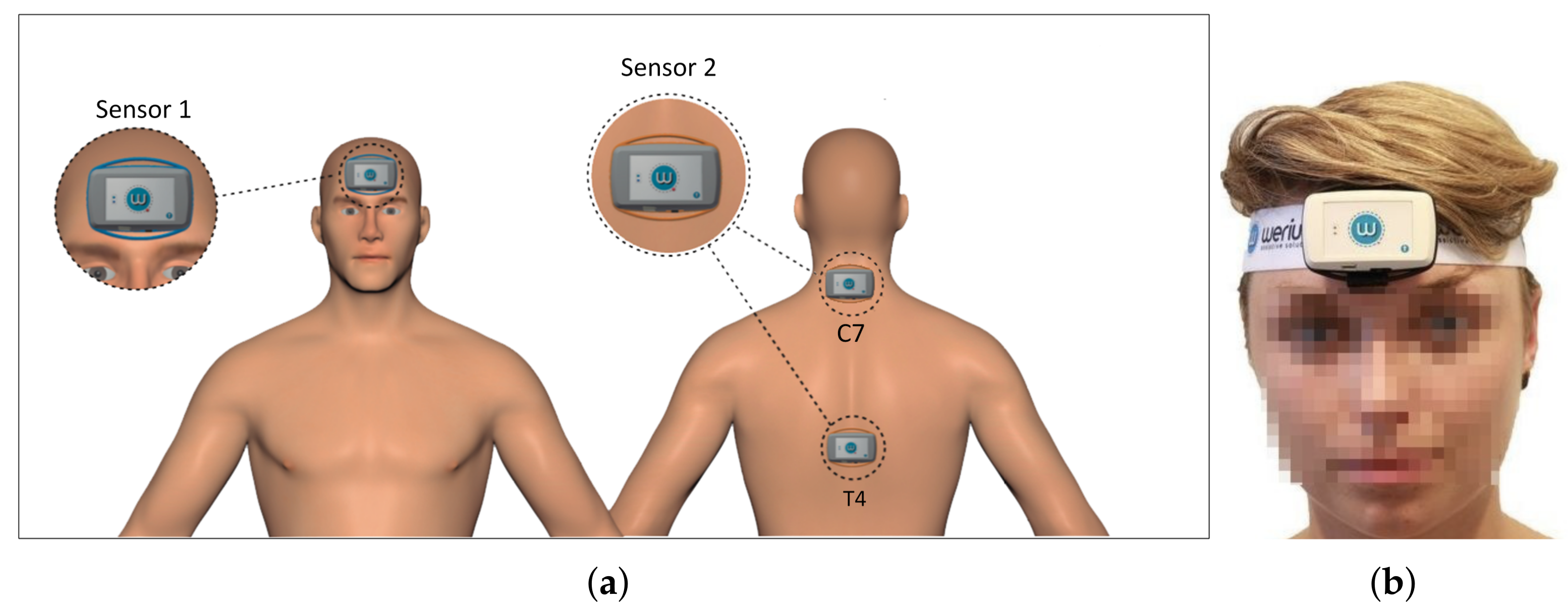
2.3. Sensors
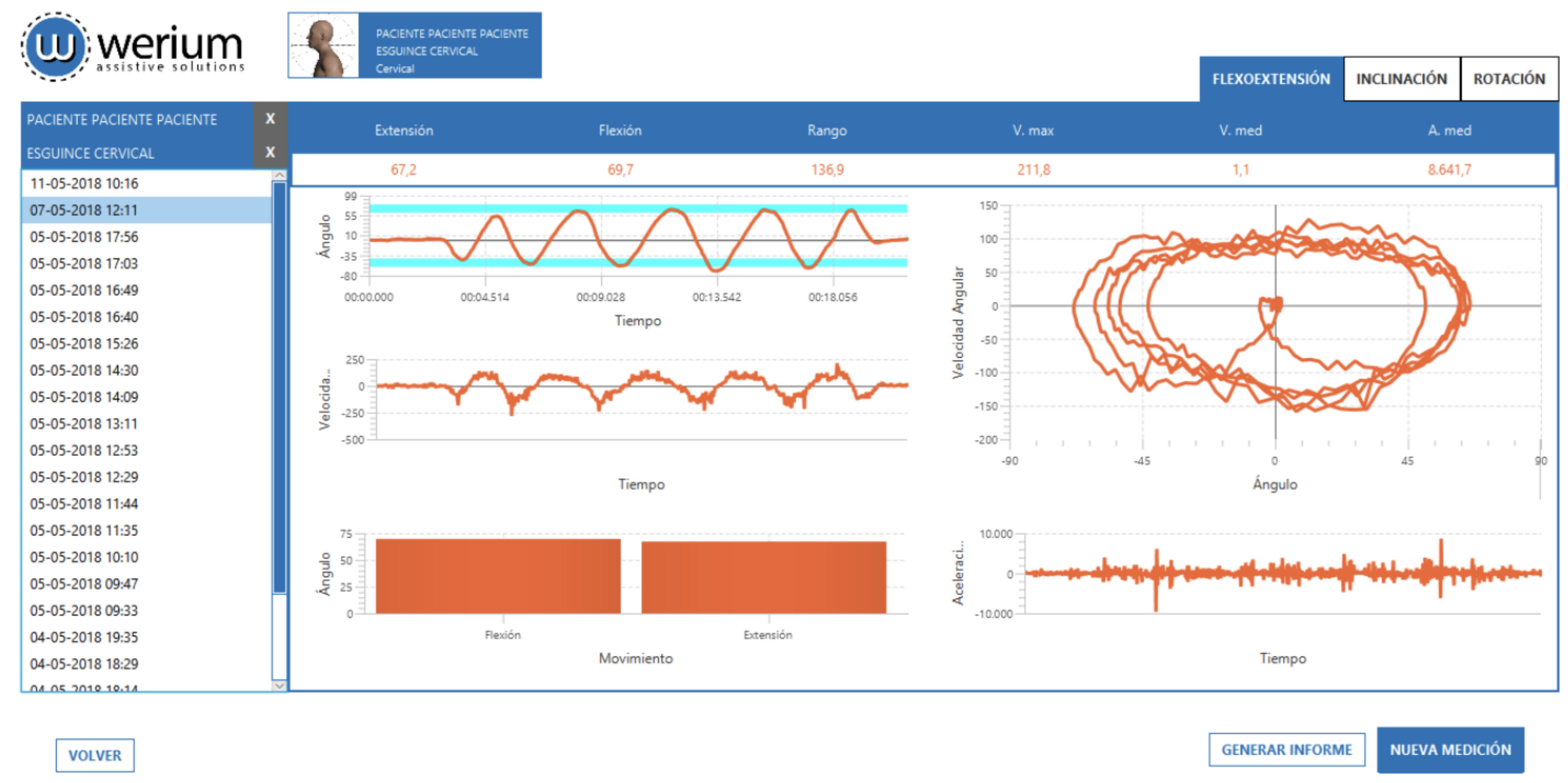
2.4. Software Application
2.5. Protocol Definition and Sensor Validation
- Three consecutive flexion-extension movements, starting from the neutral position and moving to the maximum flexion position first.
- Three consecutive lateral flexion movements, starting from the neutral position and moving to the maximum right lateral flexion position first.
- Three consecutive rotations, starting from the neutral position and moving to the maximum right rotation position first.
2.5.1. Participants
2.5.2. Measurements
2.5.3. Data Analysis
3. Results
3.1. Sensor Validation Results
3.2. Software Application Usability
3.3. Mass Production and Certification
4. Discussion
4.1. Reliability
4.2. Validity
4.3. Half vs. Full Movements
4.4. Sensor Placement for CROM
4.5. Future Work
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hoy, D.; March, L.; Woolf, A.; Blyth, F.; Brooks, P.; Smith, E.; Vos, T.; Jan, B.; Blore, J.; Murray, C.; et al. The global burden of neck pain: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1309–1315. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Hoy, D.; Protani, M.; De, R.; Buchbinder, R. The epidemiology of neck pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.P. Epidemiology, diagnosis, and treatment of neck pain. Mayo Clin. Proc. 2015, 90, 284–299. [Google Scholar] [CrossRef] [PubMed]
- Hogg-Johnson, S.; Van Der Velde, G.; Carroll, L.J.; Holm, L.W.; Cassidy, J.D.; Guzman, J.; Côté, P.; Haldeman, S.; Ammendolia, C.; Carragee, E.; et al. The burden and determinants of neck pain in the general population. Eur. Spine J. 2008, 17, 39–51. [Google Scholar] [CrossRef]
- Quinlan, K.P.; Annest, J.L.; Myers, B.; Ryan, G.; Hill, H. Neck strains and sprains among motor vehicle occupants—United States, 2000. Accid. Anal. Prev. 2004, 36, 21–27. [Google Scholar] [CrossRef]
- Haldeman, S.; Kopansky-Giles, D.; Hurwitz, E.L.; Hoy, D.; Erwin, W.M.; Dagenais, S.; Kawchuk, G.; Strömqvist, B.; Walsh, N. Advancements in the management of spine disorders. Best Pract. Res. Clin. Rheumatol. 2012, 26, 263–280. [Google Scholar] [CrossRef] [PubMed]
- Vassilaki, M.; Hurwitz, E.L. Insights in public health: Perspectives on pain in the low back and neck: Global burden, epidemiology, and management. Hawai’i J. Med. Public Health 2014, 73, 122. [Google Scholar]
- Martin, B.I.; Deyo, R.A.; Mirza, S.K.; Turner, J.A.; Comstock, B.A.; Hollingworth, W.; Sullivan, S.D. Expenditures and health status among adults with back and neck problems. JAMA 2008, 299, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Côté, P.; Cassidy, J.D.; Carroll, L.J.; Kristman, V. The annual incidence and course of neck pain in the general population: A population-based cohort study. Pain 2004, 112, 267–273. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Rehabilitation 2030: A Call for Action; Meeting Report; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Acar, M.; Bewsher, S. Design concepts for an integrated whiplash mitigating head restraint and seat. Int. J. Crashworthiness 2016, 21, 386–395. [Google Scholar] [CrossRef] [Green Version]
- Cagnie, B.; Cools, A.; De Loose, V.; Cambier, D.; Danneels, L. Reliability and normative database of the Zebris cervical range-of-motion system in healthy controls with preliminary validation in a group of patients with neck pain. J. Manip. Physiol. Ther. 2007, 30, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Dall’Alba, P.T.; Sterling, M.M.; Treleaven, J.M.; Edwards, S.L.; Jull, G.A. Cervical range of motion discriminates between asymptomatic persons and those with whiplash. Spine 2001, 26, 2090–2094. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.; Gross, A.; D’Sylva, J.; Burnie, S.J.; Goldsmith, C.H.; Graham, N.; Haines, T.; Brønfort, G.; Hoving, J.L. Manual therapy and exercise for neck pain: A systematic review. Manu. Ther. 2010, 15, 334–354. [Google Scholar] [CrossRef] [PubMed]
- Gross, A.; Paquin, J.; Dupont, G.; Blanchette, S.; Lalonde, P.; Cristie, T.; Graham, N.; Kay, T.; Burnie, S.; Gelley, G.; et al. Exercises for mechanical neck disorders: A Cochrane review update. Manu. Ther. 2016, 24, 25–45. [Google Scholar] [CrossRef] [PubMed]
- Blanpied, P.R.; Gross, A.R.; Elliott, J.M.; Devaney, L.L.; Clewley, D.; Walton, D.M.; Sparks, C.; Robertson, E.K.; Altman, R.D.; Beattie, P.; et al. Neck pain: Revision 2017: Clinical practice guidelines linked to the international classification of functioning, disability and health from the orthopaedic section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2017, 47, A1–A83. [Google Scholar] [CrossRef] [PubMed]
- Lluch, E.; Schomacher, J.; Gizzi, L.; Petzke, F.; Seegar, D.; Falla, D. Immediate effects of active cranio-cervical flexion exercise versus passive mobilisation of the upper cervical spine on pain and performance on the cranio-cervical flexion test. Manu. Ther. 2014, 19, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Childs, J.D.; Cleland, J.A.; Elliott, J.M.; Teyhen, D.S.; Wainner, R.S.; Whitman, J.M.; Sopky, B.J.; Godges, J.J.; Flynn, T.W.; Delitto, A.; et al. Neck pain: Clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic Section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2008, 38, A1–A34. [Google Scholar] [CrossRef] [PubMed]
- Teasell, R.W.; McClure, J.A.; Walton, D.; Pretty, J.; Salter, K.; Meyer, M.; Sequeira, K.; Death, B. A research synthesis of therapeutic interventions for whiplash-associated disorder: Part 1—Overview and summary. Pain Res. Manag. 2010, 15, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Hole, D.; Cook, J.; Bolton, J. Reliability and concurrent validity of two instruments for measuring cervical range of motion: Effects of age and gender. Manu. Ther. 1995, 1, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Petersen, C.; Johnson, R.; Schuit, D. Reliability of cervical range of motion using the OSI CA 6000 spine motion analyser on asymptomatic and symptomatic subjects. Manu. Ther. 2000, 5, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Mayer, T.; Brady, S.; Bovasso, E.; Pope, P.; Gatchel, R.J. Noninvasive measurement of cervical tri-planar motion in normal subjects. Spine 1993, 18, 2191–2195. [Google Scholar] [CrossRef] [PubMed]
- Rheault, W.; Albright, B.; Byers, C.; Franta, M.; Johnson, A.; Skowronek, M.; Dougherty, J. Intertester reliability of the cervical range of motion device. J. Orthop. Sports Phys. Ther. 1992, 15, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Capuano-Pucci, D.; Rheault, W.; Aukai, J.; Bracke, M.; Day, R.; Pastrick, M. Intratester and intertester reliability of the cervical range of motion device. Arch. Phys. Med. Rehabil. 1991, 72, 338–340. [Google Scholar] [PubMed]
- Williams, M.A.; McCarthy, C.J.; Chorti, A.; Cooke, M.W.; Gates, S. A systematic review of reliability and validity studies of methods for measuring active andPassive cervical range of motion. J. Manip. Physiol. Ther. 2010, 33, 138–155. [Google Scholar] [CrossRef] [PubMed]
- Tousignant, M.; Smeesters, C.; Breton, A.M.; Breton, É.; Corriveau, H. Criterion validity study of the cervical range of motion (CROM) device for rotational range of motion on healthy adults. J. Orthop. Sports Phys. Ther. 2006, 36, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Lantz, C.A.; Chen, J.; Buch, D. Clinical validity and stability of active and passive cervical range of motion with regard to total and unilateral uniplanar motion. Spine 1999, 24, 1082–1089. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.P.; Bandy, W.D. Intrarater reliability of CROM measurement of cervical spine active range of motion in persons with and without neck pain. J. Orthop. Sports Phys. Ther. 2008, 38, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Audette, I.; Dumas, J.P.; Côté, J.N.; De Serres, S.J. Validity and between-day reliability of the cervical range of motion (CROM) device. J. Orthop. Sports Phys. Ther. 2010, 40, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Prushansky, T.; Deryi, O.; Jabarreen, B. Reproducibility and validity of digital inclinometry for measuring cervical range of motion in normal subjects. Physiother. Res. Int. 2010, 15, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Alqhtani, R.S.; Jones, M.D.; Theobald, P.S.; Williams, J.M. Reliability of an accelerometer-based system for quantifying multiregional spinal range of motion. J. Manip. Physiol. Ther. 2015, 38, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Iosa, M.; Picerno, P.; Paolucci, S.; Morone, G. Wearable inertial sensors for human movement analysis. Expert Rev. Med. Devices 2016, 13, 641–659. [Google Scholar] [CrossRef] [PubMed]
- Theobald, P.S.; Jones, M.D.; Williams, J.M. Do inertial sensors represent a viable method to reliably measure cervical spine range of motion? Manu. Ther. 2012, 17, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Raya, R.; Rocon, E.; Gallego, J.A.; Ceres, R.; Pons, J.L. A robust kalman algorithm to facilitate human-computer interaction for people with cerebral palsy, using a new interface based on inertial sensors. Sensors 2012, 12, 3049–3067. [Google Scholar] [CrossRef] [PubMed]
- Raya, R.; Roa, J.; Rocon, E.; Ceres, R.; Pons, J. Wearable inertial mouse for children with physical and cognitive impairments. Sens. Actuators A Phys. 2010, 162, 248–259. [Google Scholar] [CrossRef]
- Premerlani, W.; Bizard, P. Direction Cosine Matrix IMU: Theory. Available online: https://owenson.me/build-your-own-quadcopter-autopilot/DCMDraft2.pdf (accessed on 7 August 2018).
- International Organization for Standardization. Ergonomic Requirements for Office Work with Visual Display Terminals (VDTs)—Part 9: Requirements for Non-Keyboard Input Devices (ISO 9241-9); International Organization for Standardization: Geneva, Switzerland, 2002. [Google Scholar]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Una Solución de Vanguardia con ICOT. Available online: http://www.grupoicot.es/2017/03/15/werium-pro-motion-capture-en-canarias-7/ (accessed on 22 May 2018).
- Ferrario, V.F.; Sforza, C.; Serrao, G.; Grassi, G.; Mossi, E. Active range of motion of the head and cervical spine: A three-dimensional investigation in healthy young adults. J. Orthop. Res. 2002, 20, 122–129. [Google Scholar] [CrossRef]
- Schmidt, J.; Berg, D.R.; Ploeg, H.L.; Ploeg, L. Precision, repeatability and accuracy of Optotrak® optical motion tracking systems. Int. J. Exp. Comput. Biomech. 2009, 1, 114–127. [Google Scholar] [CrossRef]
- Lohse, K.; Shirzad, N.; Verster, A.; Hodges, N.; Van der Loos, H.M. Video games and rehabilitation: Using design principles to enhance engagement in physical therapy. J. Neurol. Phys. Ther. 2013, 37, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Flores, E.; Tobon, G.; Cavallaro, E.; Cavallaro, F.I.; Perry, J.C.; Keller, T. Improving patient motivation in game development for motor deficit rehabilitation. In Proceedings of the 2008 International Conference on Advances in Computer Entertainment Technology, Yokohama, Japan, 3–5 December 2008; pp. 381–384. [Google Scholar]
- Meijer, H.A.; Graafland, M.; Goslings, J.C.; Schijven, M.P. A systematic review on the effect of serious games and wearable technology used in rehabilitation of patients with traumatic bone and soft tissue injuries. Arch. Phys. Med. Rehabil. 2017. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Set 1 (Mean ± SD) | Set 2 (Mean ± SD) | ICC | 95% CI for ICC | Mean Difference between Sets | Difference between Means | |
|---|---|---|---|---|---|---|
| Flexion | 49.54° ± 12.24° | 47.82° ± 10.08° | 0.87 | 0.71–0.94 | 6.10° | 1.73° |
| Extension | 47.81° ± 14.14° | 47.27° ± 13.24° | 0.93 | 0.84–0.97 | 5.47° | 0.54° |
| Right Lateral Flexion | 33.32° ± 6.51° | 34.93° ± 6.75° | 0.87 | 0.70–0.94 | 3.36° | 1.62° |
| Left Lateral Flexion | 35.37° ± 8.18° | 35.16° ± 9.71° | 0.96 | 0.90–0.98 | 2.85° | 0.21° |
| Right Rotation | 63.55° ± 10.73° | 63.5° ± 9.73° | 0.91 | 0.81–0.96 | 4.75° | 0.06° |
| Left Rotation | 68.64° ± 11.63° | 69.47° ± 12.33° | 0.91 | 0.80–0.96 | 5.27° | 0.83° |
| Set 1 (Mean ± SD) | Set 2 (Mean ± SD) | ICC | 95% CI for ICC | Mean Difference between Sets | Difference between Means | |
|---|---|---|---|---|---|---|
| Flexion | 56.92° ± 11.57° | 56.14 ± 11.10 | 0.90 | 0.77–0.95 | 5.23° | 0.78 |
| Extension | 60.53° ± 16.62° | 61.25° ± 14.77° | 0.92 | 0.82–0.96 | 6.65° | 0.72 |
| Right Lateral Flexion | 38.1° ± 7.26° | 37.05° ± 7.69° | 0.88 | 0.74–0.95 | 3.6° | 1.05° |
| Left Lateral Flexion | 38.01° ± 8.29° | 40.14° ± 9.00° | 0.70 | 0.36–0.86 | 5.15° | 2.13° |
| Right Rotation | 71.24° ± 10.56° | 73.84° ± 11.60° | 0.91 | 0.79–0.96 | 4.98 | 2.6 |
| Left Rotation | 75.38 ± 10.17 | 74.2° ± 10.70 | 0.92 | 0.82–0.96 | 4.59 | 1.18 |
| Set 1 (Mean ± SD) | Set 2 (Mean ± SD) | ICC | 95% CI for ICC | Mean Difference between Sets | Difference between Means | |
|---|---|---|---|---|---|---|
| Flexion-Extension | 97.37° ± 21.16° | 95.10° ± 20.43° | 0.97 | 0.93–0.99 | 5.33° | 2.27° |
| Lateral Flexion | 68.70° ± 13.18° | 70.10° ± 14.49° | 0.95 | 0.89–0.98 | 4.80° | 1.40° |
| Rotation | 132.20° ± 20.43° | 132.98° ± 19.20° | 0.98 | 0.95–0.99 | 4.53° | 0.78° |
| Set 1 (Mean ± SD) | Set 2 (Mean ± SD) | ICC | 95% CI for ICC | Mean Difference between Sets | Difference between Means | |
|---|---|---|---|---|---|---|
| Flexion-Extension | 117.46° ± 23.26° | 117.40° ± 19.95° | 0.97 | 0.93–0.97 | 5.14° | 0.06° |
| Lateral Flexion | 76.12° ± 14.40° | 77.20° ± 13.81° | 0.90 | 0.78–0.95 | 5.70° | 1.08° |
| Rotation | 146.62° ± 17.74° | 148.05° ± 20.37° | 0.96 | 0.90–0.98 | 5.62° | 1.43° |
| Cervical Movement | Mean ± SD | Range |
|---|---|---|
| Flexion | 46.1° ± 10.8° | 26–77° |
| Extension | 48.8° ± 14.9° | 25–83° |
| Right Lateral Flexion | 32.4° ± 8.0° | 10–51° |
| Left Lateral Flexion | 33.6° ± 7.3° | 10–52° |
| Right Rotation | 55.1° ± 8.9° | 25–78° |
| Left Rotation | 57.1° ± 10.3° | 28–86° |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raya, R.; Garcia-Carmona, R.; Sanchez, C.; Urendes, E.; Ramirez, O.; Martin, A.; Otero, A. An Inexpensive and Easy to Use Cervical Range of Motion Measurement Solution Using Inertial Sensors. Sensors 2018, 18, 2582. https://doi.org/10.3390/s18082582
Raya R, Garcia-Carmona R, Sanchez C, Urendes E, Ramirez O, Martin A, Otero A. An Inexpensive and Easy to Use Cervical Range of Motion Measurement Solution Using Inertial Sensors. Sensors. 2018; 18(8):2582. https://doi.org/10.3390/s18082582
Chicago/Turabian StyleRaya, Rafael, Rodrigo Garcia-Carmona, Cristina Sanchez, Eloy Urendes, Oscar Ramirez, Alvaro Martin, and Abraham Otero. 2018. "An Inexpensive and Easy to Use Cervical Range of Motion Measurement Solution Using Inertial Sensors" Sensors 18, no. 8: 2582. https://doi.org/10.3390/s18082582
APA StyleRaya, R., Garcia-Carmona, R., Sanchez, C., Urendes, E., Ramirez, O., Martin, A., & Otero, A. (2018). An Inexpensive and Easy to Use Cervical Range of Motion Measurement Solution Using Inertial Sensors. Sensors, 18(8), 2582. https://doi.org/10.3390/s18082582