Blood Pressure Estimation from Photoplethysmogram Using a Spectro-Temporal Deep Neural Network



Abstract
:1. Introduction
1.1. PPG Background
1.2. PTT Approach to BP Estimation
1.3. PPG-Only Approach to BP Estimation
1.4. Our Research in the Context of Related Work
- Using a large, precisely specified subset of the MIMIC III database with available IDs and the corresponding code for obtaining it, and
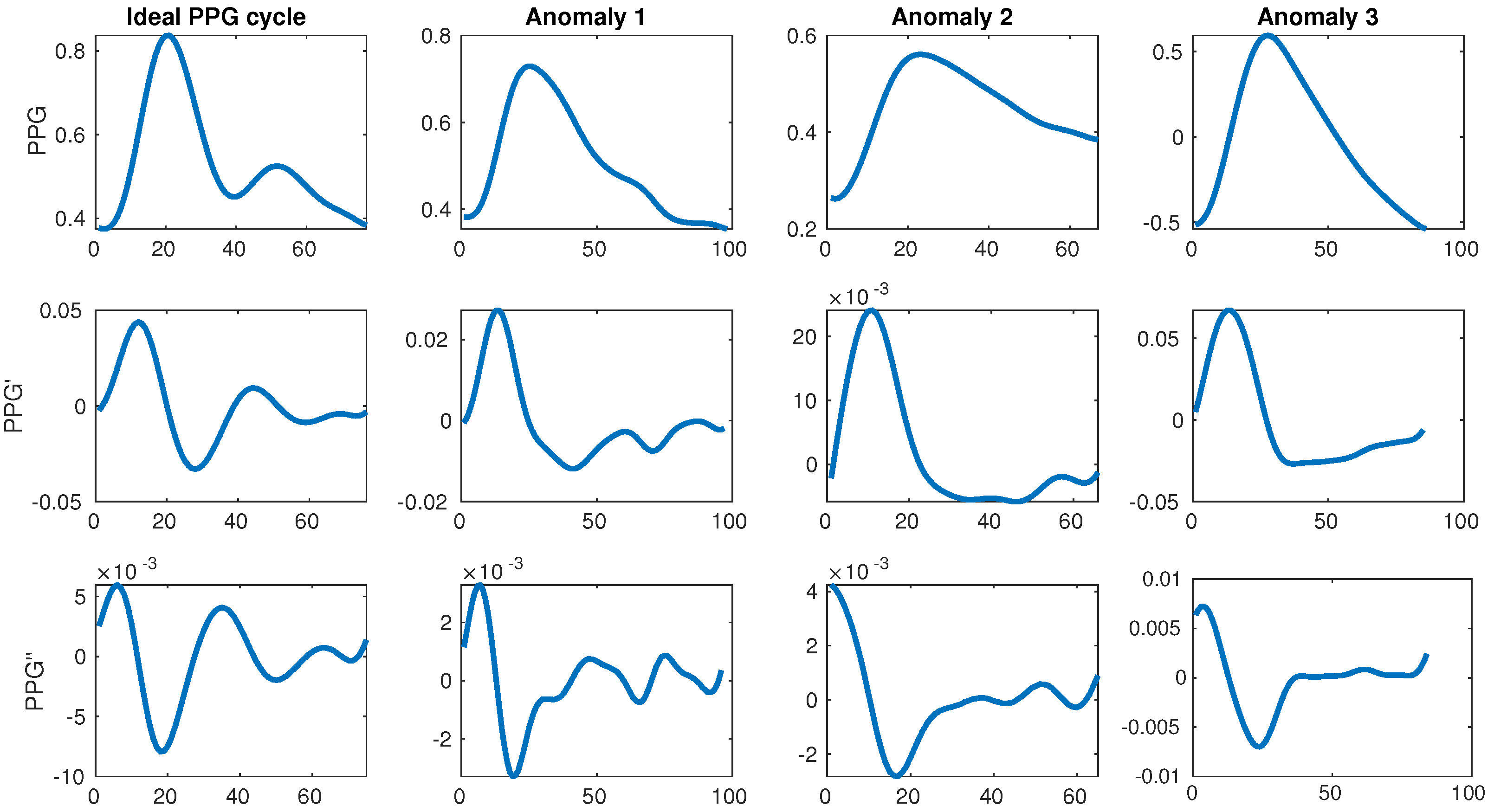
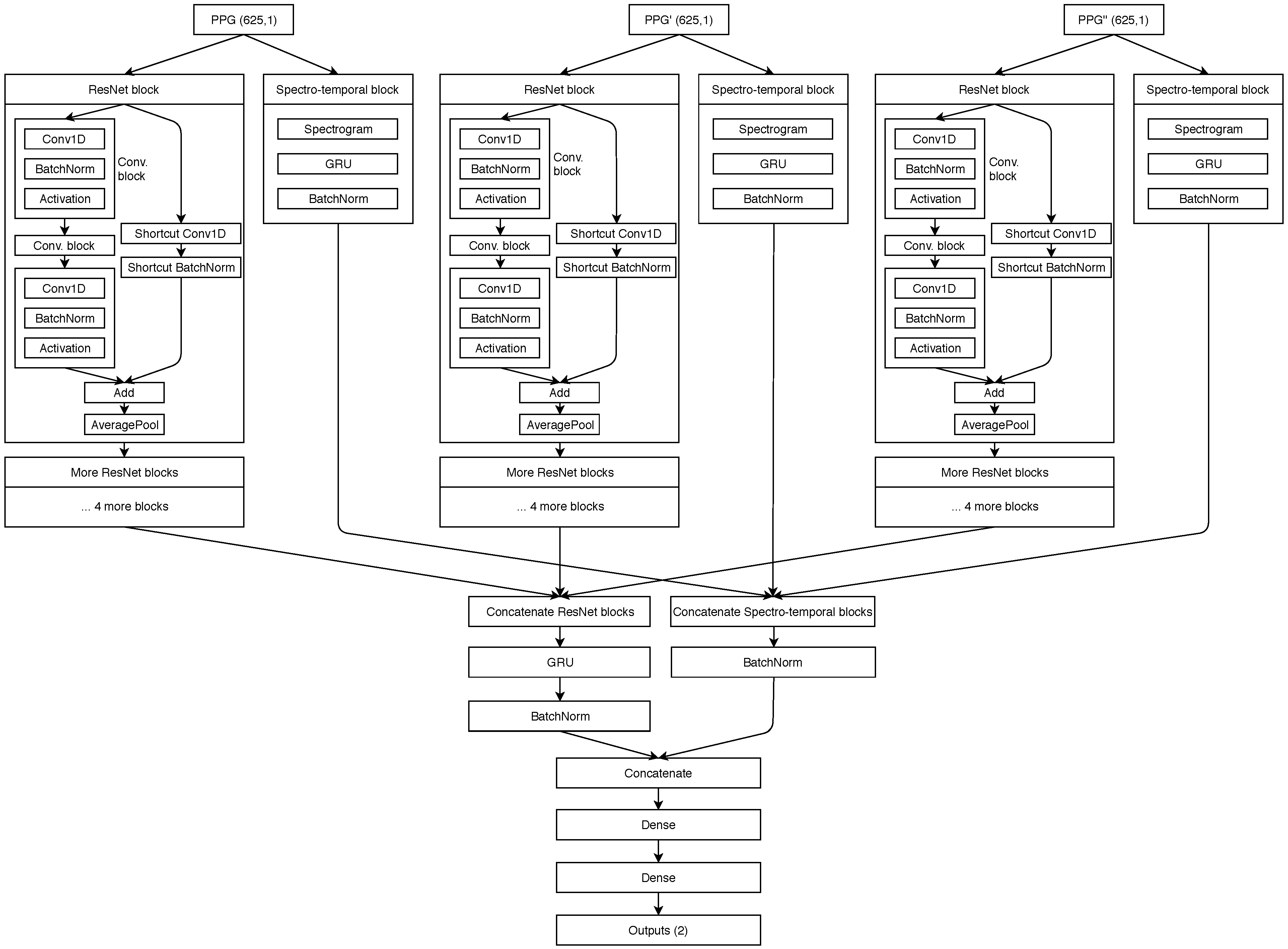
- Directly using the PPG and its derivatives waveforms as input into a novel spectro-temporal residual neural network, which successfully modelled the relationship between PPG and BP. Our proposed neural network architecture is, to our knowledge, the most sophisticated in this field to date, as it takes into account both temporal and frequency information contained in the PPG waveform and its derivatives. The architectural details are described in the later sections and the code for the models is made available.
2. Materials and Methods
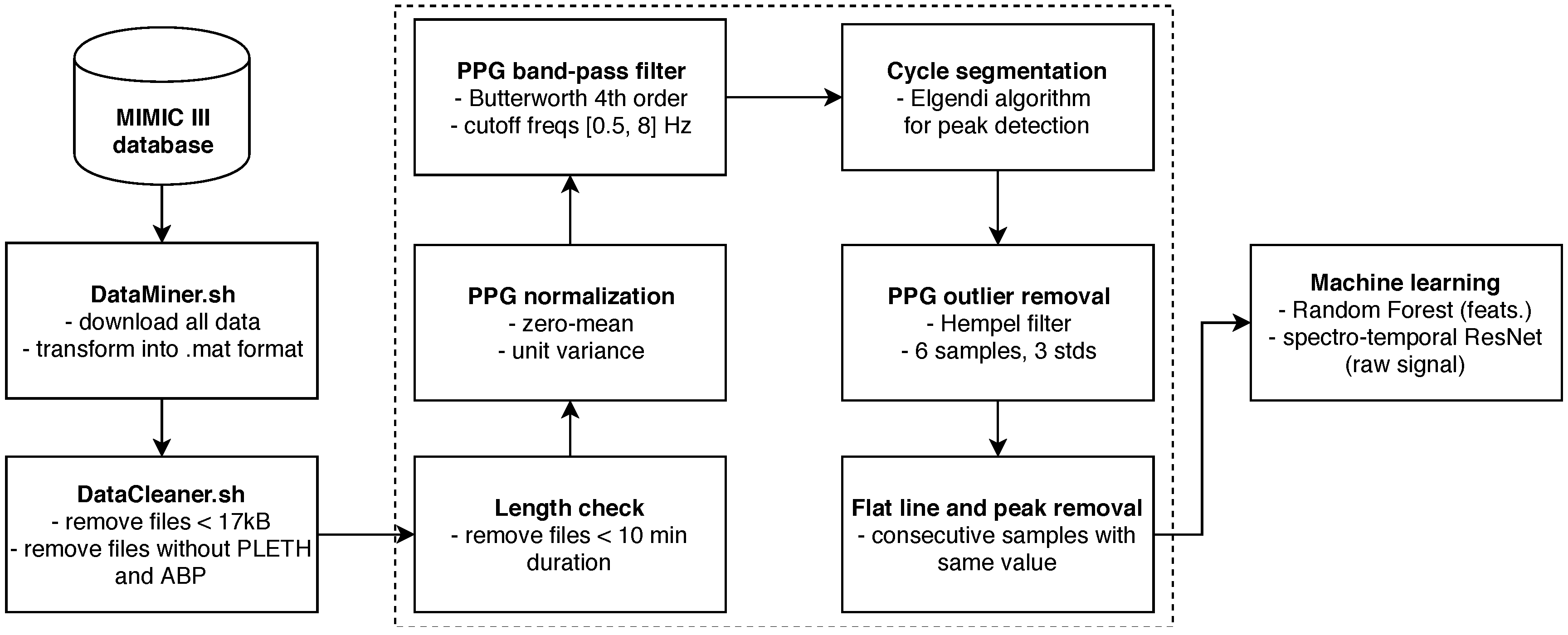
2.1. Obtaining and Cleaning Raw Data
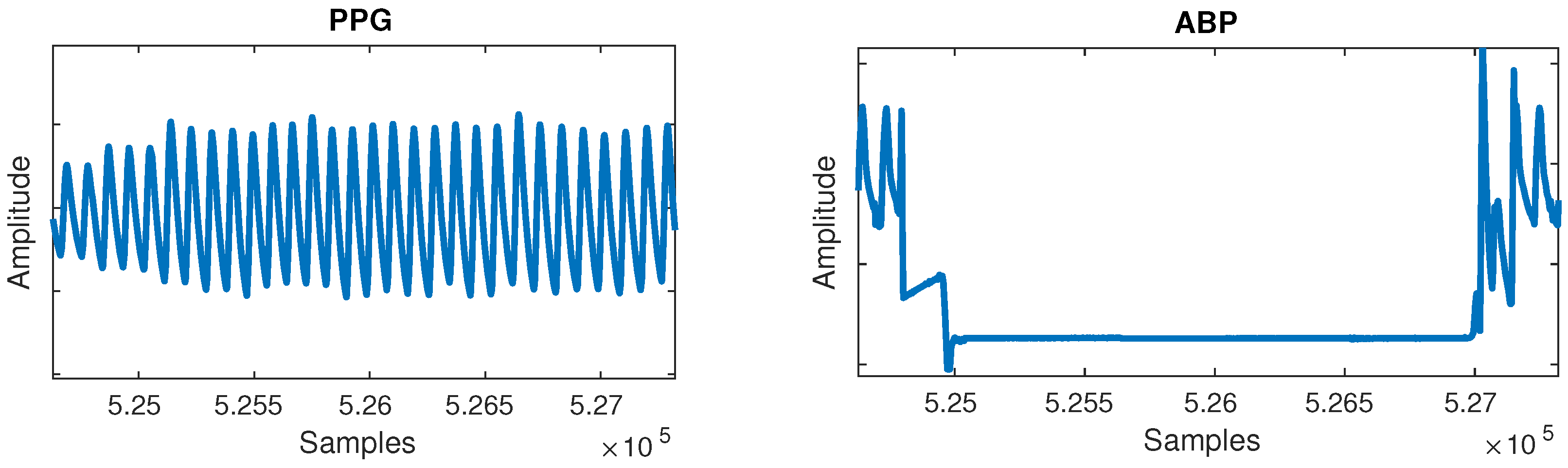
- Flat lines: Flat lines sometimes appeared for long periods of time between normal cycles in both PPG and ABP, as shown in Figure 2. A flat line was detected when three or more consecutive signal samples did not change their value. Such flat lines could be observed in several separate segments of the signal and we postulate they were caused by a periodic sensor anomaly or detachment of sensor. Such areas were useless and were thus cut out from the waveforms.
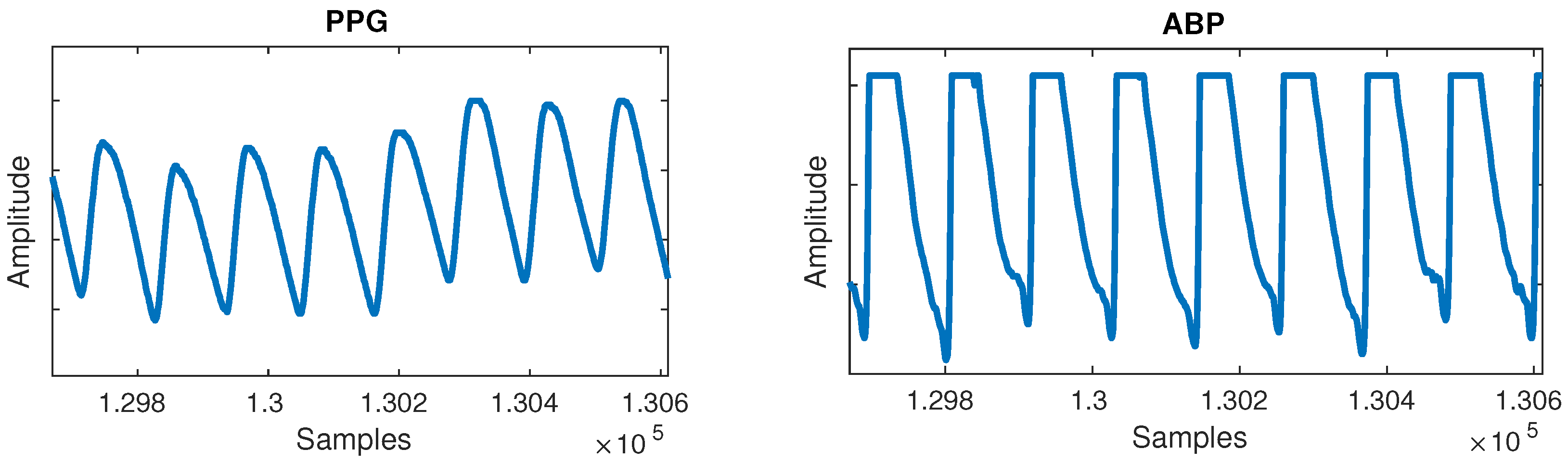
- Flat peaks: Similarly, it was common for the ABP waveforms to have flat peaks with top parts missing, as shown in Figure 3. After the PPG was segmented into cycles, peaks were similarly detected by checking if three or more consecutive samples had the same value within a given cycle. The cause was again unknown, but could most likely be attributed to a sensor issue. The peak of the ABP is vital, as its value is the SBP, which is the ground truth needed for machine learning.
2.2. Classical Machine Learning
2.3. Deep Learning
2.3.1. Neural Network Architecture and Hyperparameters
2.4. Experimental Setup
3. Results
4. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ABP | arterial blood pressure |
| ANN | artificial neural network |
| BP | blood pressure |
| CV | cross validation |
| CVDs | cardiovascular diseases |
| DBP | diastolic blood pressure |
| ECG | electrocardiogram |
| FFT | fast fourier transform |
| GDPR | general data protection regulation |
| HR | heart rate |
| LED | light-emmiting diode |
| LOSO | leave one subject out |
| LSTM | long short-term memory |
| MAE | mean absolute error |
| ME | mean error |
| PPG | photoplethysmogram |
| PPG’ | 1st derivative of photoplethysmogram |
| PPG” | 2nd derivative of photoplethysmogram |
| PPT | pulse transit time |
| PSD | power spectral densitiy |
| PWV | pulse wawe velocity |
| RNN | recurrent neural networks |
| SBP | systolic blood pressure |
| WHO | World Health Organisation |
References
- Handler, J. The Importance of Accurate Blood Pressure Measurement. Perm. J. 2009, 13, 51–54. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Top 10 Causes of Death. Available online: http://www.who.int/mediacentre/factsheets/fs310/en/ (accessed on 18 April 2019).
- Levy, D.; Larson, M.G.; Vasan, R.S.; Kannel, W.B.; Ho, K.L. The progression from hypertension to congestive heart failure. JAMA 1996, 275, 1557–1562. [Google Scholar] [CrossRef] [PubMed]
- Frese, E.M.; Sadowsky, H.S. Blood Pressure Measurement Guidelines for Physical Therapists. Cardiopulmanory Phys. Ther. J. 2011, 22, 5–12. [Google Scholar] [CrossRef]
- He, X.; Goubran, R.A.; Liu, X.P. Evaluation of the correlation between blood pressure and pulse transit time. In Proceedings of the 2013 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Gatineau, QC, Canada, 4–5 May 2013; pp. 17–20. [Google Scholar] [CrossRef]
- World Health Organization. mHealth: New Horizons for Health through Mobile Technologies; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Allen, J. Photoplethysmography and its application in clinical physiological measurement. Physiol. Meas. 2007, 28, R1. [Google Scholar] [CrossRef] [PubMed]
- Shelley, K.; Shelley, S. Pulse oximeter waveform: Photoelectric plethysmography. In Clinical Monitoring; Lake, C., Hines, R., Blitt, C., Eds.; WB Saunders Company: Philadelphia, PA, USA, 2001; pp. 420–428. [Google Scholar]
- Bramwell, J.C.; Hill, A.V. The velocity of pulse wave in man. Proc. R. Soc. London. Ser. B Contain. Pap. Biol. Character 1922, 93, 298–306. [Google Scholar] [CrossRef] [Green Version]
- Geddes, L.A.; Voelz, M.H.; Babbs, C.F.; Bourl, J.D.; Tacker, W.A. Pulse transit time as an indicator of arterial blood pressure. Psychophysiology 1981, 18, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.E.; Pollard, T.J.; Shen, L.; Li-wei, H.L.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Celi, L.A.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, K.W.; Hung, K.; Zhang, Y.T. Noninvasive and cuffless measurements of blood pressure for telemedicine. In Proceedings of the 23rd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Istanbul, Turkey, 25–28 October 2001; pp. 3592–3593. [Google Scholar]
- Kachuee, M.; Kiani, M.M.; Mohammadzade, H.; Shabany, M. Cuffless blood pressure estimation algorithms for continuous health-care monitoring. IEEE Trans. Biomed. Eng. 2017, 64, 859–869. [Google Scholar] [CrossRef] [PubMed]
- Su, P.; Ding, X.R.; Zhang, Y.T.; Liu, J.; Miao, F.; Zhao, N. Long-term blood pressure prediction with deep recurrent neural networks. In Proceedings of the 2018 IEEE EMBS International Conference on Biomedical & Health Informatics (BHI), Las Vegas, NV, USA, 4–7 March 2018; pp. 323–328. [Google Scholar] [CrossRef]
- Gesche, H.; Grosskurth, D.; Küchler, G.; Patzak, A. Continuous blood pressure measurement by using the pulse transit time: Comparison to a cuff-based method. Eur. J. Appl. Physiol. 2012, 112, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Mukkamala, R.; Hahn, J.O.; Inan, O.T.; Mestha, L.K.; Kim, C.S.; Töreyin, H.; Kyal, S. Toward ubiquitous blood pressure monitoring via pulse transit time: Theory and practice. IEEE Trans. Biomed. Eng. 2015, 62, 1879–1901. [Google Scholar] [CrossRef] [PubMed]
- Teng, X.F.; Zhang, Y.T. Continuous and noninvasive estimation of arterial blood pressure using a photoplethysmographic approach. In Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Cancun, Mexico, 17–21 September 2003; pp. 3153–3156. [Google Scholar]
- Kurylyak, Y.; Lamonaca, F.; Grimaldi, D. A Neural Network-based method for continuous blood pressure estimation from a PPG signal. In Proceedings of the 2013 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Minneapolis, MN, USA, 6–9 May 2013; pp. 280–283. [Google Scholar] [CrossRef]
- Xing, X.; Sun, M. Optical blood pressure estimation with photoplethysmography and FFT-based neural networks. Biomed. Opt. Express 2016, 7, 3007–3020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gotlibovych, I.; Crawford, S.; Goyal, D.; Liu, J.; Kerem, Y.; Benaron, D.; Yilmaz, D.; Marcus, G.; Li, Y. End-to-end deep learning from raw sensor data: Atrial fibrillation detection using wearables. KDD Deep Learning Day 2018. arXiv 2018, arXiv:1807.10707. [Google Scholar]
- Baker, M. Is there a reproducibility crisis? A Nature survey lifts the lid on how researchers view the’crisis rocking science and what they think will help. Nature 2016, 533, 452–455. [Google Scholar] [CrossRef] [PubMed]
- Yousef, Q.; Reaz, M.B.I.; Ali, M.A.M. The analysis of PPG morphology: Investigating the effects of aging on arterial compliance. Meas. Sci. Rev. 2012, 12, 266–271. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a New Research Resource for Complex Physiologic Signals. Circulation 2000, 101, e215–e220. [Google Scholar] [CrossRef]
- The MathWorks, Inc. Outlier Removal Using Hampel Identifier. Available online: https://www.mathworks.com/help/signal/ref/hampel.html (accessed on 29 April 2019).
- Dagar, M.; Mishra, N.; Rani, A.; Agarwal, S.; Yadav, J. Performance Comparison of Hampel and Median Filters in Removing Deep Brain Stimulation Artifact. In Innovations in Computational Intelligence: Best Selected Papers of the Third International Conference on REDSET 2016; Springer: Singapore, 2018; pp. 17–28. [Google Scholar]
- Elgendi, M.; Norton, I.; Brearley, M.; Abbott, D.; Schuurmans, D. Systolic peak detection in acceleration photoplethysmograms measured from emergency responders in tropical conditions. PLoS ONE 2013, 8, e76585. [Google Scholar] [CrossRef] [PubMed]
- Slapničar, G.; Luštrek, M.; Marinko, M. Continuous blood pressure estimation from PPG signal. Informatica 2018, 42, 33–42. [Google Scholar]
- Welch, P. The use of fast Fourier transform for the estimation of power spectra: A method based on time averaging over short, modified periodograms. IEEE Trans. Audio Electroacoust. 1967, 15, 70–73. [Google Scholar] [CrossRef] [Green Version]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Patil, O.R.; Gao, Y.; Li, B.; Jin, Z. CamBP: A camera-based, non-contact blood pressure monitor. In Proceedings of the 2017 ACM International Joint Conference on Pervasive and Ubiquitous Computing and Proceedings of the 2017 ACM International Symposium on Wearable Computers, Maui, HI, USA, 11–15 September 2017. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Domain | Features |
|---|---|
| Temporal |
|
| Frequency |
|
| Leave-One-Subject-Out (LOSO) Experiment (5-s Windows of Raw Signal as Instances) | ||
| MAE for SBP [mmHg] | MAE for DBP [mmHg] | |
| Dummy (mean of training) | 19.66 | 10.64 |
| ResNet (raw PPG, no personalization) | 16.39 | 13.41 |
| ResNet (raw PPG, with personalization) | 10.52 | 7.67 |
| ResNet (raw PPG + PPG’ + PPG”, no personalization) | 15.41 | 12.38 |
| ResNet (raw PPG + PPG’ + PPG”, with personalization) | 9.43 | 6.88 |
| LOSO Experiment (Per-Cycle PPG Features as Instances) | ||
| MAE for SBP [mmHg] | MAE for DBP [mmHg] | |
| Dummy (mean of training) | 19.17 | 10.22 |
| Random Forest (features, no personalization) | 18.34 | 13.86 |
| Random Forest (features, with personalization) | 13.62 | 11.73 |
| Author | Data Used | Method Used | Personalization | Error |
|---|---|---|---|---|
| Chan et al. [12] | Unspecified proprietary data | PTT approach, classical ML (linear regression) | Yes | ME of 7.5 for SBP and 4.1 for DBP |
| Su et al. [14] | Proprietary data (84 subjects, 10 min each) | PTT approach, deep learning (long short-term memory (LSTM)) | Unknown | RMSE of 3.73 for SBP and 2.43 for DBP |
| Kachuee et al. [13] | MIMIC II (1000 subjects) | PTT approach, classical ML (AdaBoost) | Optional | MAE of 11.17 for SBP and 5.35 for DBP |
| Teng et al. [17] | Proprietary data (15 subjects, 18 seconds each) | Temporal PPG features, classical ML (linear regression) | Unknown | ME of 0.21 for SBP and 0.02 for DBP |
| Kurylyak et al. [18] | MIMIC (15,000 beats) | Temporal PPG features, deep learning (fully-connected artificial neural network (ANN)) | Unknown | MAE of 3.80 for SBP and 2.21 for DBP |
| Xing et al. [19] | MIMIC II (69 subjects) and proprietary data (23 subjects) | Frequency PPG features, deep learning (fully-connected ANN) | Unknown | RMSE of 0.06 for SBP and 0.01 for DBP |
| Our work | MIMIC III (510 subjects) | Temporal and frequency features of PPG, PPG’ and PPG”, deep learning (spectro-temporal ResNet) | Yes | MAE of 9.43 for SBP and 6.88 for DBP |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Slapničar, G.; Mlakar, N.; Luštrek, M. Blood Pressure Estimation from Photoplethysmogram Using a Spectro-Temporal Deep Neural Network. Sensors 2019, 19, 3420. https://doi.org/10.3390/s19153420
Slapničar G, Mlakar N, Luštrek M. Blood Pressure Estimation from Photoplethysmogram Using a Spectro-Temporal Deep Neural Network. Sensors. 2019; 19(15):3420. https://doi.org/10.3390/s19153420
Chicago/Turabian StyleSlapničar, Gašper, Nejc Mlakar, and Mitja Luštrek. 2019. "Blood Pressure Estimation from Photoplethysmogram Using a Spectro-Temporal Deep Neural Network" Sensors 19, no. 15: 3420. https://doi.org/10.3390/s19153420
APA StyleSlapničar, G., Mlakar, N., & Luštrek, M. (2019). Blood Pressure Estimation from Photoplethysmogram Using a Spectro-Temporal Deep Neural Network. Sensors, 19(15), 3420. https://doi.org/10.3390/s19153420