Wellness Assessment of Alzheimer’s Patients in an Instrumented Health-Care Facility




Abstract
:1. Introduction
1.1. State of the Art
1.1.1. Indoor Localization
1.1.2. Wellness Assessment
- Five factors model of personality [19] (or big five) defines five categories of human behaviour: neuroticism, extraversion, openness to experience, agreeableness, conscientiousness.
- The wheel of wellness model [20] defines five life tasks: spirituality, self-direction, work and leisure, friendship and love.
- Life assessment questionnaire (LAQ) [23] scores wellness with 100 questions on a five-point Likert scale. It provides a measure of the social, spiritual, physical, intellectual, emotional and occupational wellness of the individual.
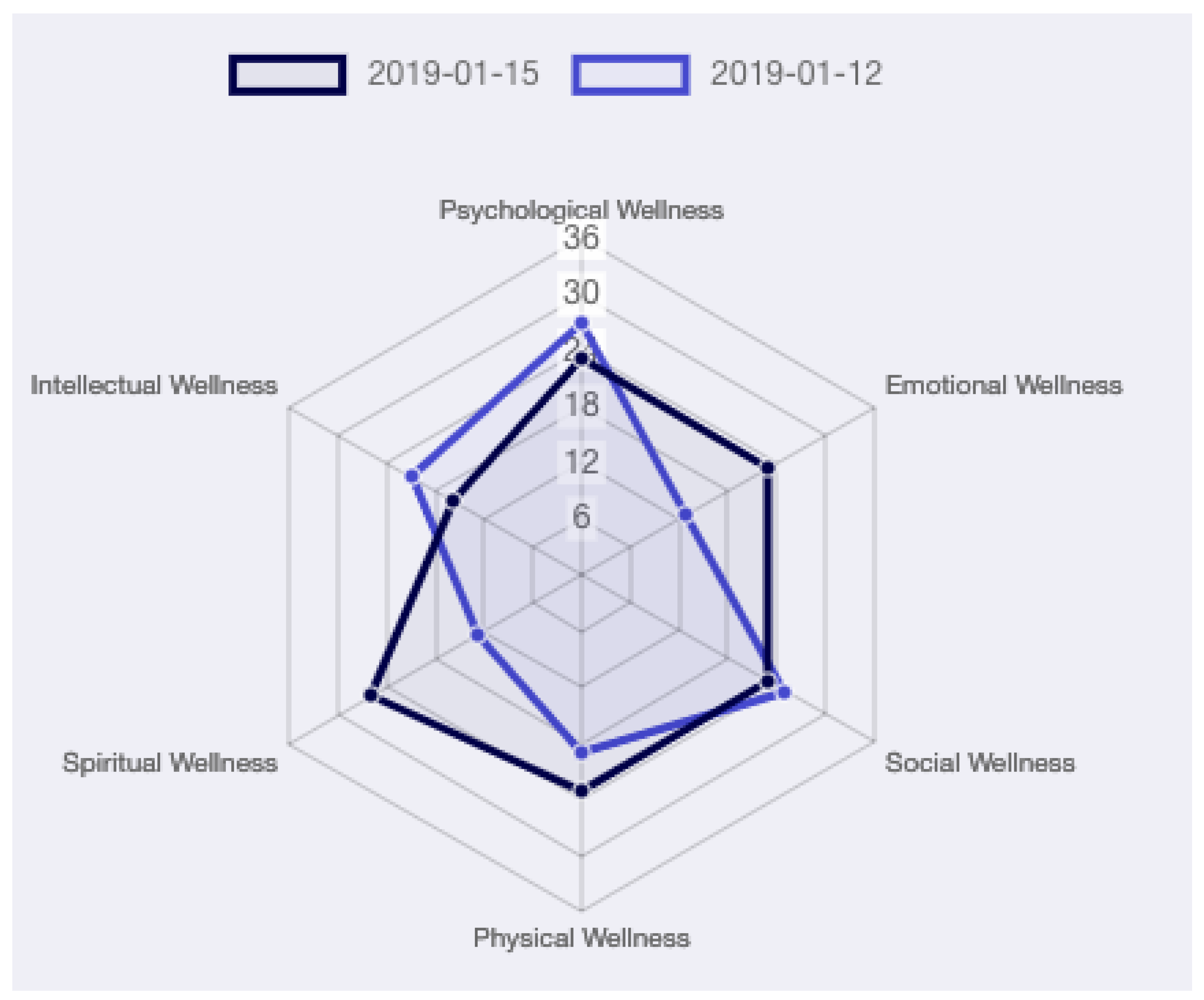
- Perceived wellness survey (PWS) [24] scores wellness with 36 questions on a six-point Likert scale. It provides a measure of the social, emotional, physical, intellectual, spiritual and psychological wellness of the individual.
- Optimal living profile (OPL) [25] scores wellness with 135 questions on a five-point Likert scale. It provides a measure of the social, emotional, physical, intellectual, spiritual and environmental wellness of the individual.
- Wellness evaluation of life inventory (WEL) [26,27]. The latest version of this survey is the the WEL-S, it scores wellness with 120 questions on a five-point Likert scale. The 5F-WEL instead uses 91 items; among them, 17 are experimental items, on a five-point Likert scale. Finally, the 4F-WEL is an additional extension of the 5F-WEL that scores cognitive-emotional, relational, physical and spiritual wellness.
- Wellness inventory (WI) [28] scores wellness with 120 questions on a five-point Likert scale. It provides a measure of multiple dimensions such as self-responsibility and love, breathing, moving, sensing, thinking, eating, feeling, communication, playing and working, sex, finding meaning, and transcending.
- TestWell [29] scores wellness with 100 questions on a five-point Likert scale. It provides a measure of the social, emotional, physical, intellectual, spiritual and occupational wellness of the individual.
- The Barthel index [32] is currently used in hospitals to evaluate the self-care ability and mobility of patients. Its measure considers 10 basic ADLs to generate a score of independence. The environment greatly influence the final score.
- The Katz index [31] is used to assess the individual ability of performing ADLs independently. An overall performance on six basic ADLs is the result of the instrument.
- The MACTAR patient preference disability questionnaire [33] is used to assess the ability of the patients to perform five specific activities.
- The health assessment questionnaire [34] is used to assess the ability of patients to perform ADLs. It considers 20 items to describe eight basic ADLs.
- The modified health assessment questionnaire [35] is an alteration of the Health Assessment Questionnaire. It considers just 8 items (12 less than HAQ) to score the patient ability of performing ADLs.
- The PF-10 [36] is used to examine the physical ability of an individual through 10 items. It is a subset of the MOS 36-Item Short-Form Health Survey (SF-36): an instrument designed by the same authors to assess the health status of patients in a clinical settings.
- The functional independence measure [37] is used to estimate the level of autonomy in performing 18 basic ADLs. It is designed for adults who are independent in most functional activities.
1.2. Contributions and Paper Organization
1.3. Case Study
2. Materials and Methods
2.1. Coarse Grained Localization System
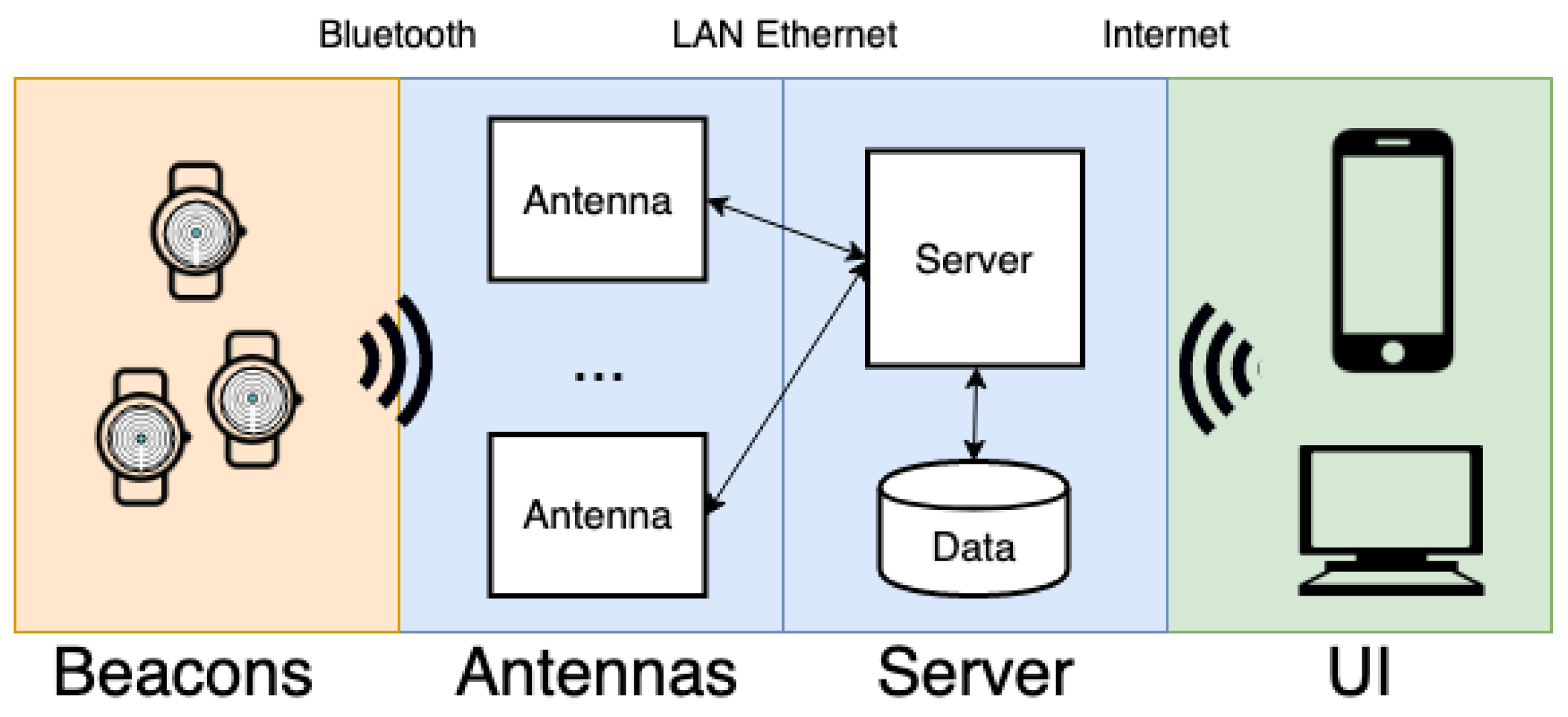
2.1.1. Architecture
2.1.2. Localization Algorithm
| Symbol | Description |
| Bracelet of person i | |
| List of RSSI values of received from all antennas at time t | |
| Candidate position of at time t | |
| Selected position of at time t | |
| Likelihood that the is in at time t | |
| Initialization value of likelihood for each | |
| Constant value added or removed to the likelihood | |
| Likelihood threshold: under this level, wall crossing is allowed |
| Algorithm 1 Localization algorithm. |
|
|
2.1.3. System Notifications
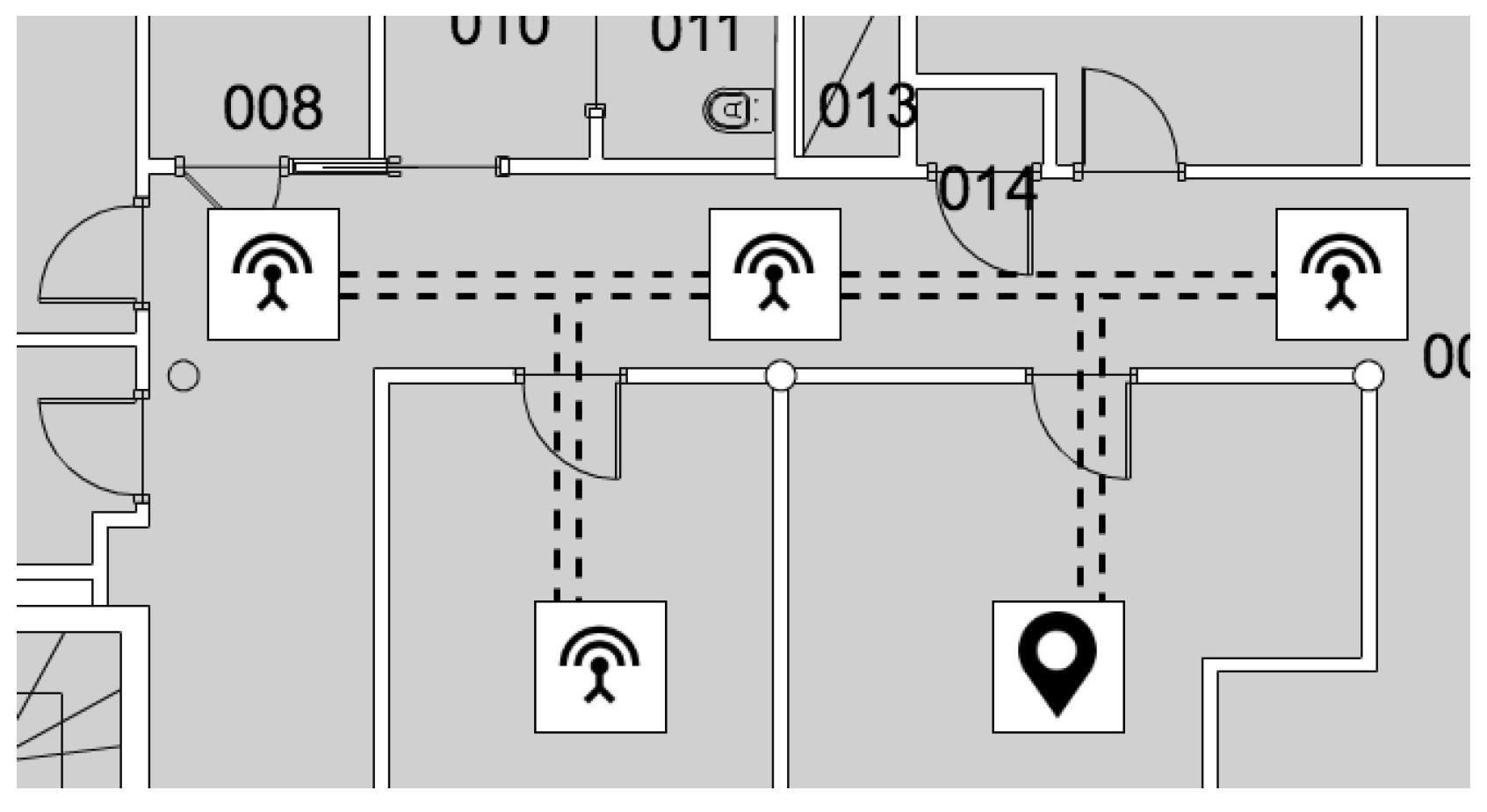
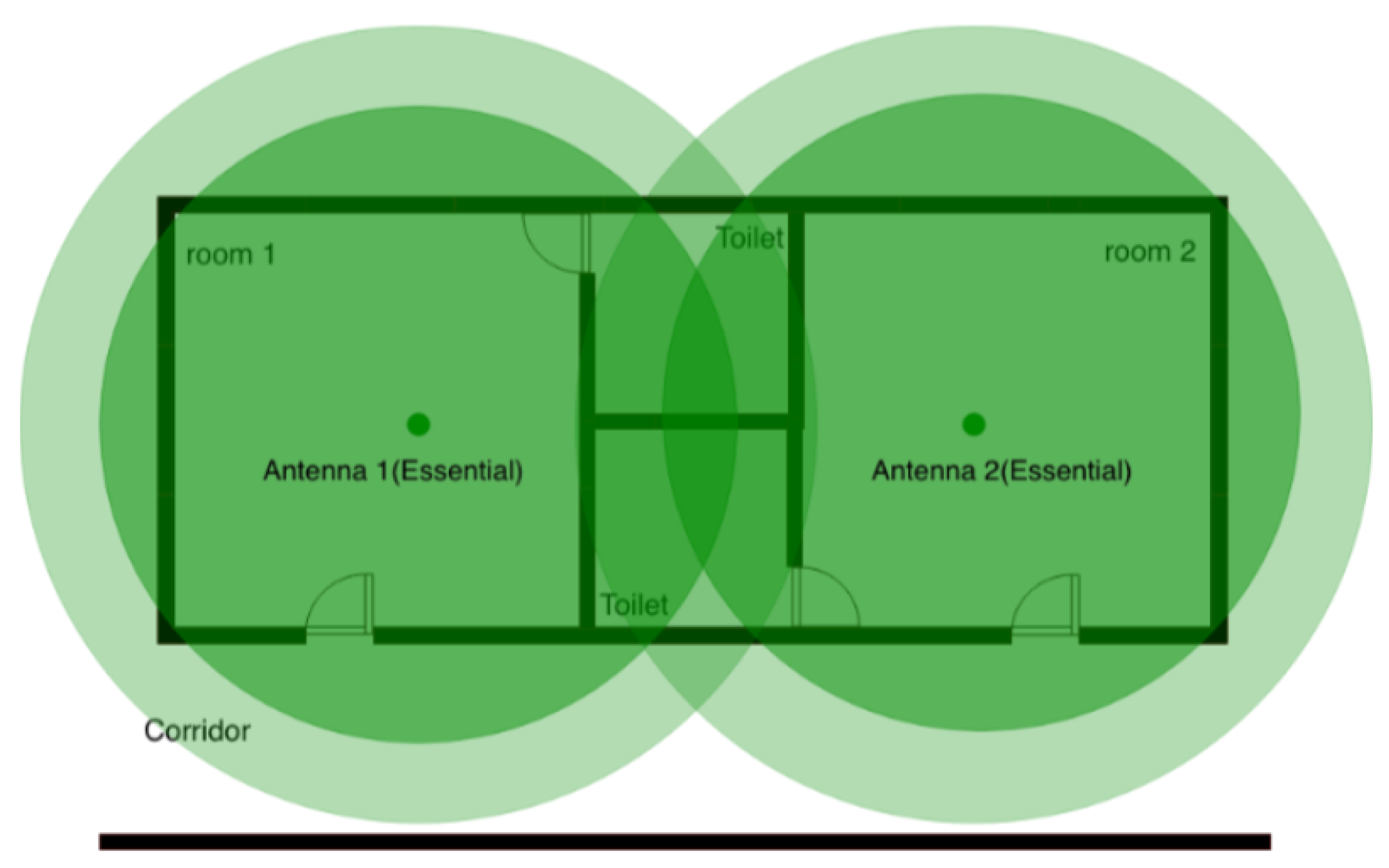
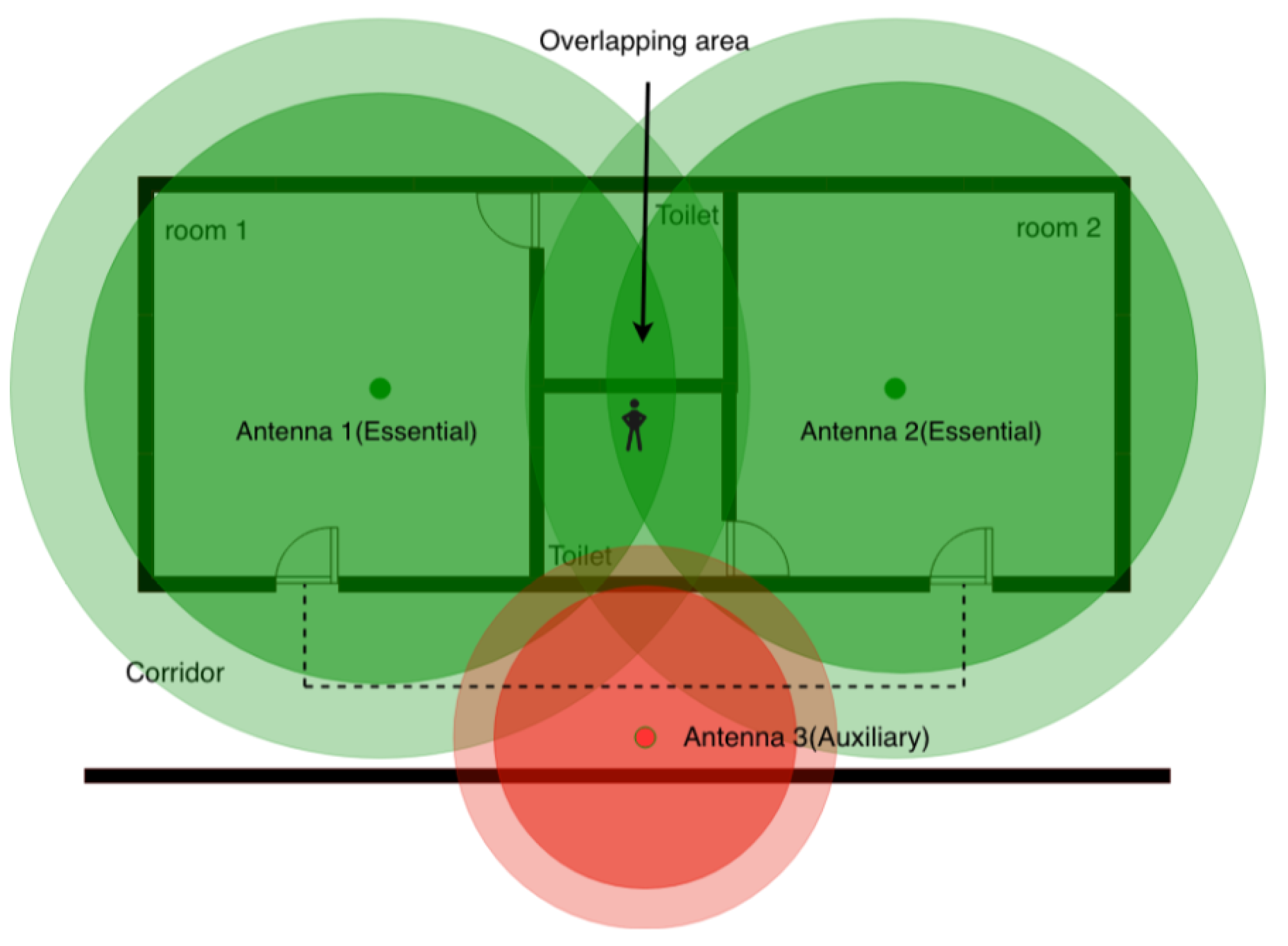
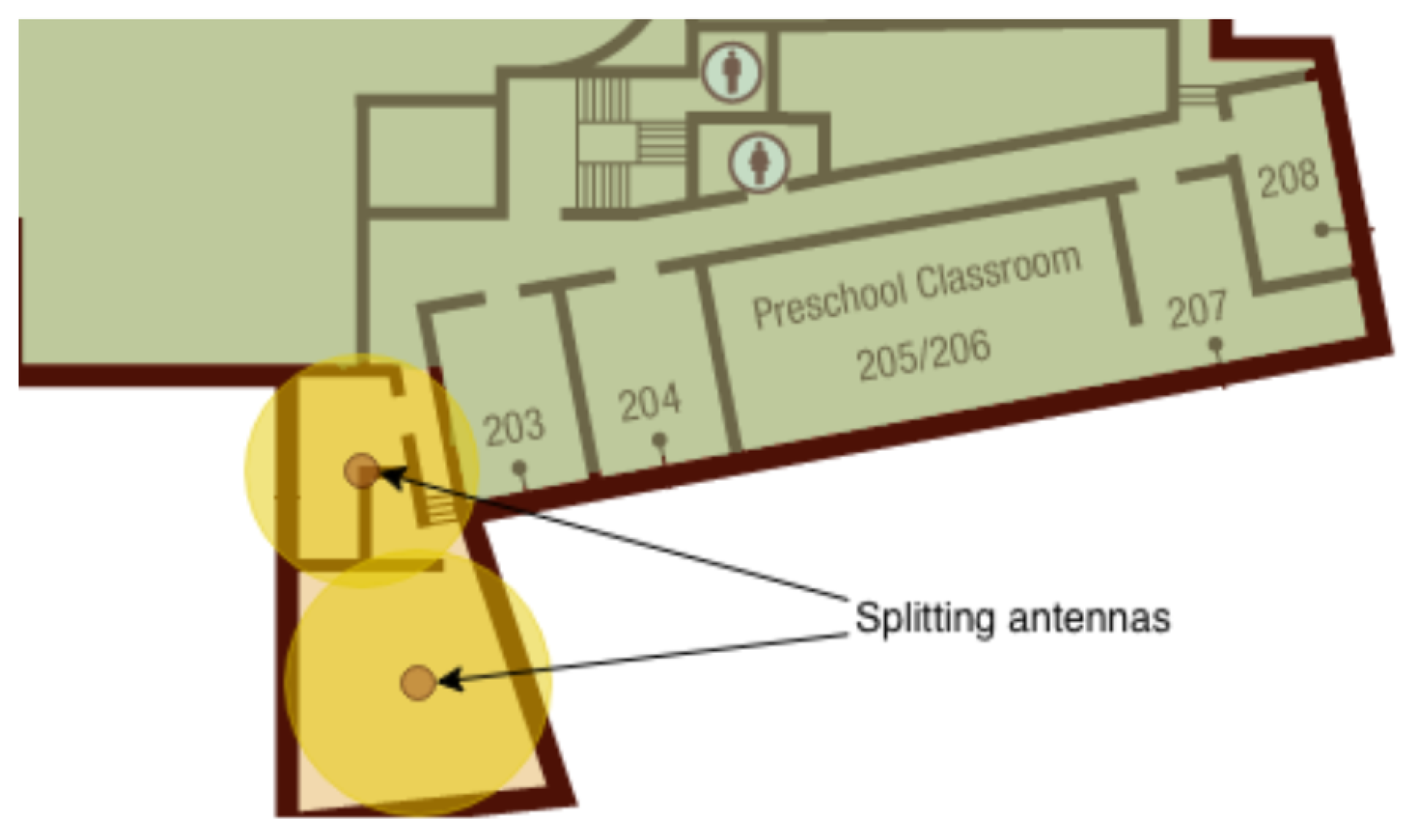
2.1.4. Antenna Positioning
2.2. Wellness Assessment
2.2.1. Physical Activity
2.2.2. Social Activity
2.2.3. Psychological Activity
2.3. System Implementation
2.4. Data Collection
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Department of Economic and Social Affairs, United Nations. World Population Ageing 2017; Technical report; United Nations: San Francisco, CA, USA, 2017. [Google Scholar]
- Benetazzo, F.; Ferracuti, F.; Freddi, A.; Giantomassi, A.; Iarlori, S.; Longhi, S.; Monteriù, A.; Ortenzi, D. AAL technologies for independent life of elderly people. In Ambient Assisted Living; Springer: Basel, Switzerland, 2015; pp. 329–343. [Google Scholar]
- Niemeijer, A.R.; Frederiks, B.J.; Depla, M.F.; Legemaate, J.; Eefsting, J.A.; Hertogh, C.M. The ideal application of surveillance technology in residential care for people with dementia. J. Med. Ethics 2011, 37, 303–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doshi-Velez, F.; Li, W.; Battat, Y.; Charrow, B.; Curthis, D.; Park, J.G.; Hemachandra, S.; Velez, J.; Walsh, C.; Fredette, D.; et al. Improving safety and operational efficiency in residential care settings with WiFi-based localization. J. Am. Med. Dir. Assoc. 2012, 13, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Farid, Z.; Nordin, R.; Ismail, M. Recent advances in wireless indoor localization techniques and system. J. Netw. Comput. Appl. 2013, 2013, 185138. [Google Scholar] [CrossRef]
- Tariq, Z.B.; Cheema, D.M.; Kamran, M.Z.; Naqvi, I.H. Non-GPS Positioning Systems: A Survey. ACM Comput. Surv. (CSUR) 2017, 50, 57. [Google Scholar] [CrossRef]
- Stojanović, D.; Stojanović, N. Indoor localization and tracking: Methods, technologies and research challenges. Facta Universitatis Ser. Autom. Control Robot. 2014, 13, 57–72. [Google Scholar]
- Bouchard, K.; Ramezani, R.; Naeim, A. Features based proximity localization with Bluetooth emitters. In Proceedings of the 2016 IEEE 7th Annual Ubiquitous Computing, Electronics & Mobile Communication Conference (UEMCON), New York, NY, USA, 20–22 October 2016; pp. 1–5. [Google Scholar]
- Honkavirta, V.; Perala, T.; Ali-Loytty, S.; Piché, R. A comparative survey of WLAN location fingerprinting methods. In Proceedings of the 2009 IEEE 6th workshop on positioning, navigation and communication, Hannover, Germany, 19–19 March 2009; pp. 243–251. [Google Scholar]
- Yang, Z.; Liu, Y. Quality of trilateration: Confidence-based iterative localization. IEEE Trans. Parallel Distrib. Syst. 2009, 21, 631–640. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. On happiness and human potentials: A review of research on hedonic and eudaimonic well-being. Annu. Rev. Psy. 2001, 52, 141–166. [Google Scholar] [CrossRef] [PubMed]
- Pinto, S.; Fumincelli, L.; Mazzo, A.; Caldeira, S.; Martins, J.C. Comfort, well-being and quality of life: Discussion of the differences and similarities among the concepts. Porto Biomed. J. 2017, 2, 6–12. [Google Scholar] [CrossRef]
- Roscoe, L.J. Wellness: A review of theory and measurement for counselors. J. Couns. Dev. 2009, 87, 216–226. [Google Scholar] [CrossRef]
- Organization, W.H. Constitution of the World Health Organization; World Health Organization: Geneva, Switzerland, 1995. [Google Scholar]
- Cella, D.F. Quality of life: concepts and definition. JPSM 1994, 9, 186–192. [Google Scholar] [CrossRef]
- Felce, D.; Perry, J. Quality of life: Its definition and measurement. Res. Dev. Disabil. 1995, 16, 51–74. [Google Scholar] [CrossRef]
- Torrance, G.W. Utility approach to measuring health-related quality of life. J. Chron. Dis. 1987, 40, 593–600. [Google Scholar] [CrossRef]
- Guyatt, G.H. Measurement of health-related quality of life in heart failure. J. Am. Coll. Cardiol. 1993, 22, A185–A191. [Google Scholar] [CrossRef] [Green Version]
- Costa, P.T., Jr.; McCrae, R.R. The five-factor model of personality and its relevance to personality disorders. For. Chron. 1992, 6, 343–359. [Google Scholar] [CrossRef]
- Myers, J.E.; Sweeney, T.J.; Witmer, J.M. The wheel of wellness counseling for wellness: A holistic model for treatment planning. J. Couns. Dev. 2000, 78, 251–266. [Google Scholar] [CrossRef]
- Myers, J.E.; Sweeney, T.J. The indivisible self: An evidence-based model of wellness. J. Ind. Psychol. 2004, 60, 234–244. [Google Scholar]
- Adler, A. Understanding Human Nature (Psychology Revivals); Routledge Publishing: London, UK, 2013. [Google Scholar]
- Institute, N.W. Life Style Assessment Questionnaire, 2nd ed.; National Wellness Institute: Stevens Point, WI, USA, 1983. [Google Scholar]
- Adams, T.; Bezner, J.; Steinhardt, M. The conceptualization and measurement of perceived wellness: Integrating balance across and within dimensions. Am.J. Health Promot. 1997, 11, 208–218. [Google Scholar] [CrossRef]
- Renger, R.F.; Midyett, S.J.; Mas, S.; Francisco, G.; Erin, T.D.; McDermott, H.M.; Papenfuss, R.L.; Eichling, P.S.; Baker, D.H.; Johnson, K.A.; et al. Optimal Living Profile: An inventory to assess health and wellness. Am. J. Health. Behav. 2000, 24, 403–412. [Google Scholar] [CrossRef]
- Myers, J.E.; Witmer, J.M.; Sweeney, T.J. Manual for the Wellness Evaluation of Lifestyle; Mind Garden: Palo Alto, CA, USA, 2004. [Google Scholar]
- Myers, J.E.; Sweeney, T.J. Manual for the Five Factor Wellness Inventory; Mind Garden: Palo Alto, CA, USA, 2004. [Google Scholar]
- Travis, J.W. Wellness Index: A Self-Assessment of Health and Vitality; Springer Science & Business: Berlin, Germany, 2004. [Google Scholar]
- Stevens Point. TestWell, a Wellness Inventory; National Wellness Institute: Stevens Point, WI, USA, 1992. [Google Scholar]
- Ni, Q.; García Hernando, A.; de la Cruz, I. The elderly’s independent living in smart homes: A characterization of activities and sensing infrastructure survey to facilitate services development. Sensors 2015, 15, 11312–11362. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of Illness in the Aged: The Index of ADL: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Mahoney, R. Barthel index (BI). Md. St. Med. J. 1965, 14, 56–61. [Google Scholar]
- Tugwell, P.; Bombardier, C.; Buchanan, W.; Goldsmith, C.; Grace, E.; Hanna, B. The Mactar Patient Preference Disability Questionnaire–an individualized functional priority approach for assessing improvement in physical disability in clinical trials in rheumatoid arthritis. J. Rheumatol. 1987, 14, 446–451. [Google Scholar] [PubMed]
- Fries, J.F.; Spitz, P.; Kraines, R.G.; Holman, H.R. Measurement of patient outcome in arthritis. Arthritis Rheum. 1980, 23, 137–145. [Google Scholar] [CrossRef]
- Pincus, T.; Summey, J.A.; Soraci, S.A., Jr.; Wallston, K.A.; Hummon, N.P. Assessment of patient satisfaction in activities of daily living using a modified Stanford Health Assessment Questionnaire. Arthritis Rheum. 1983, 26, 1346–1353. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Keith, R.A. The functional independence measure: a new tool for rehabilitation. Adv. Clin. Rehabil. 1987, 2, 6–18. [Google Scholar]
- Umphred, D. Neurological Rehabilitation, 6th ed.; Elsevier Health: London, UK, 2012. [Google Scholar]
- Il Paese Ritrovato Project. Cooperativa la meridiana. Available online: http://www.cooplameridiana.it/il-paese-ritrovato/ (accessed on 19 July 2019).
- La Meridiana. Cooperativa Sociale La Meridiana. Available online: http://www.cooplameridiana.it (accessed on 19 July 2019).
- Veronese, F.; Masciadri, A.; Comai, S.; Matteucci, M.; Salice, F. Behavior Drift Detection Based on Anomalies Identification in Home Living Quantitative Indicators. Technologies 2018, 6, 16. [Google Scholar] [CrossRef]
- Niemeijer, A.R.; Frederiks, B.J.; Riphagen, I.I.; Legemaate, J.; Eefsting, J.A.; Hertogh, C.M. Ethical and practical concerns of surveillance technologies in residential care for people with dementia or intellectual disabilities: an overview of the literature. Int. Psychogeriatr. 2009, 22, 1129–1142. [Google Scholar] [CrossRef]
- IBeacon. Apple informazioni sui servizi di localizzazione. Available online: https://support.apple.com/en-gb/HT202880 (accessed on 19 July 2019).
- Aman, M.S.; Jiang, H.; Quint, C.; Yelamarthi, K.; Abdelgawad, A. Reliability evaluation of iBeacon for micro-localization. In Proceedings of the 2016 IEEE 7th Annual Ubiquitous Computing, Electronics Mobile Communication Conference (UEMCON), New York, NY, USA, 20–22 October 2016. [Google Scholar]
- Raspberry RaspberryPi 3—Model B. Available online: https://www.raspberrypi.org/products/raspberry-pi-3-model-b/ (accessed on 19 July 2019).
- National Institute of Neurological Disorders and Stroke Brain Basics: Understanding Sleep. Available online: https://www.ninds.nih.gov/Disorders/patient-caregiver-education/understanding-sleep (accessed on 19 July 2019).
- Reed, D.L.; Sacco, W.P. Measuring sleep efficiency: What should the denominator be? J. Clin. Sleep Med. 2016, 12, 263–266. [Google Scholar] [CrossRef]
- Levasseur, M.; Richard, L.; Gauvin, L.; Raymond, É. Inventory and analysis of definitions of social participation found in the aging literature: Proposed taxonomy of social activities. Soc. Sci. Med. 2010, 71, 2141–2149. [Google Scholar] [CrossRef] [Green Version]
- Stewart-Brown, S. Emotional wellbeing and its relation to health: Physical disease may well result from emotional distress. BMJ 1998, 317, 1608–1609. [Google Scholar] [CrossRef] [PubMed]
- Grossi, G.; Lanzarotti, R.; Napoletano, P.; Noceti, N.; Odone, F. Emotional and Social Well-being of Older People: A Review. Pattern Recogn. Lett. 2019. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masciadri, A.; Comai, S.; Salice, F. Wellness Assessment of Alzheimer’s Patients in an Instrumented Health-Care Facility. Sensors 2019, 19, 3658. https://doi.org/10.3390/s19173658
Masciadri A, Comai S, Salice F. Wellness Assessment of Alzheimer’s Patients in an Instrumented Health-Care Facility. Sensors. 2019; 19(17):3658. https://doi.org/10.3390/s19173658
Chicago/Turabian StyleMasciadri, Andrea, Sara Comai, and Fabio Salice. 2019. "Wellness Assessment of Alzheimer’s Patients in an Instrumented Health-Care Facility" Sensors 19, no. 17: 3658. https://doi.org/10.3390/s19173658
APA StyleMasciadri, A., Comai, S., & Salice, F. (2019). Wellness Assessment of Alzheimer’s Patients in an Instrumented Health-Care Facility. Sensors, 19(17), 3658. https://doi.org/10.3390/s19173658