NurseNet: Monitoring Elderly Levels of Activity with a Piezoelectric Floor

Abstract
:1. Introduction
1.1. General Introduction
1.2. Related Work
1.2.1. Gait Sensing
1.2.2. Gait Analysis
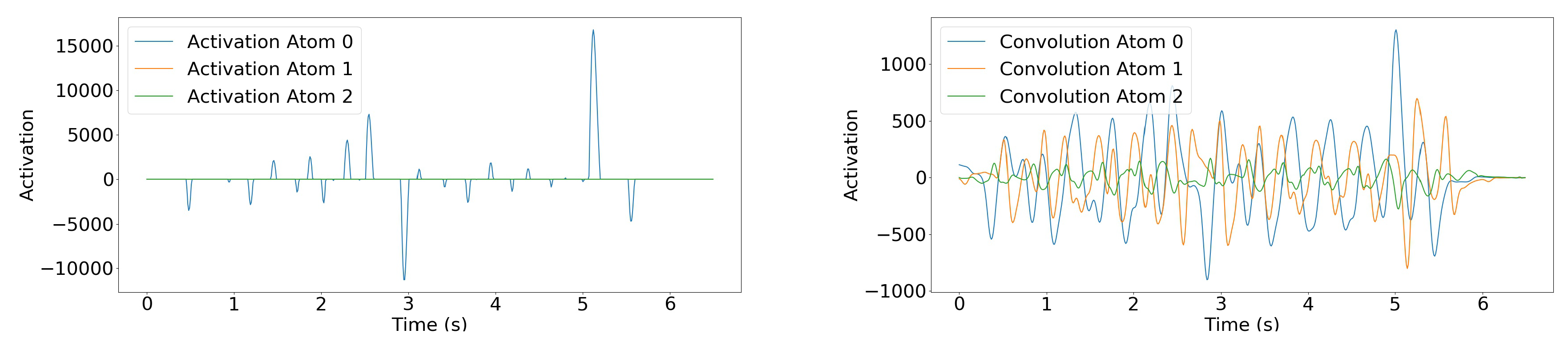
1.2.3. Sparse Coding and Dictionary Learning
1.2.4. Signal Processing with Deep Learning
2. Materials and Methods
2.1. NurseNet Hardware
2.1.1. The Piezoelectric Principle
2.1.2. The NurseNet Unit
2.2. The NurseNet Algorithm
2.2.1. General Classifier
- One 1D convolutional layer with 32 filters of size 60, with a stride of 10, followed by a BatchNorm layer, with the activation function hyperbolic tangent (tanh).
- One 1D convolutional layer with 16 filters of size 1, with a stride of 1, followed by a BatchNorm layer, with the activation function tanh.
- One 1D convolutional layer with 8 filters of size 1, with a stride of 1, followed by a BatchNorm layer, with the activation function tanh.
- One 1D convolutional layer with 1 filter of size 5, with a stride of 1, with the activation function Rectified Linear Unit (ReLU) [58]. It was followed by a Maxpool layer of size 5.
- One fully-connected layer, with an output of dimension 64, with activation function ReLU.
- One fully-connected layer, with an output of dimension 16, with activation function ReLU.
- One fully-connected layer, with an output of dimension 1, with activation function sigmoid.
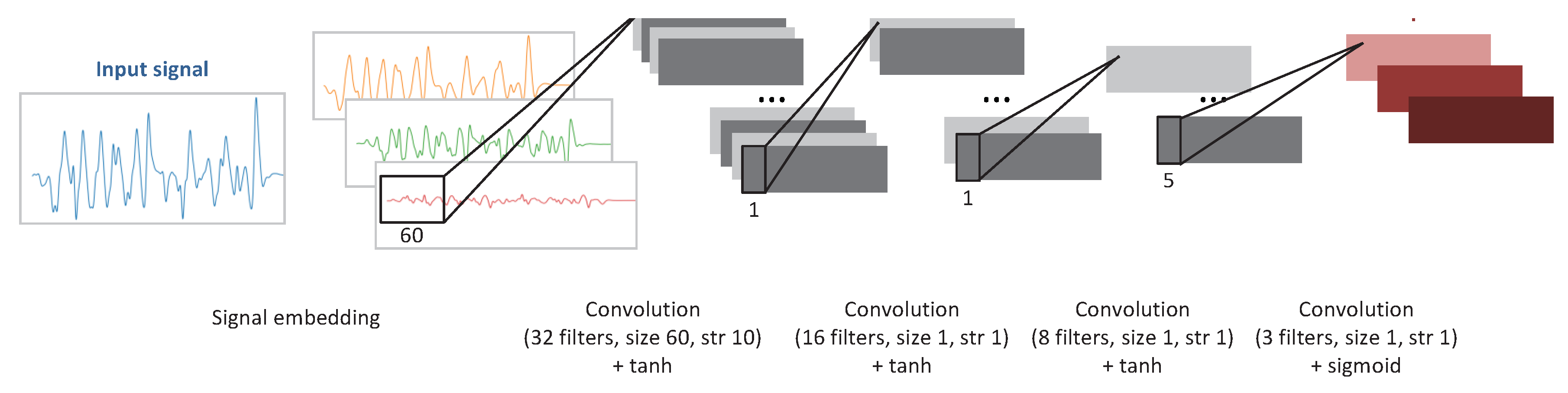
2.2.2. Data Embedding
- Each channel was filtered with a low-pass Butterworth filter with a 10-Hz cutoff frequency, fifth order, and zero lag. This step aimed to limit the amount of electronic noise present in the signal, as the 10-Hz cutoff frequency is the reference in gait-related signals [66].
- The linear trend of each channel was removed using a least squares model.
- Each channel whose signal maximum amplitude was small was then set to zero, as the channel was assumed to only account for noise.
- The resulting signal was obtained as the sum of all the channels:
2.2.3. Pre Training Weights with Step Detection
- One 1D convolutional layer with 32 filters of size 60, with a stride of 10, followed by a BatchNorm layer, with the activation function hyperbolic tangent (tanh).
- One 1D convolutional layer with 16 filters of size 1, with a stride of 1, followed by a BatchNorm layer, with the activation function tanh.
- One 1D convolutional layer with 8 filters of size 1, with a stride of 1, followed by a BatchNorm layer, with the activation function tanh.
- One 1D convolutional layer with 3 filters of size 1, with a stride of 1, with the activation function sigmoid.
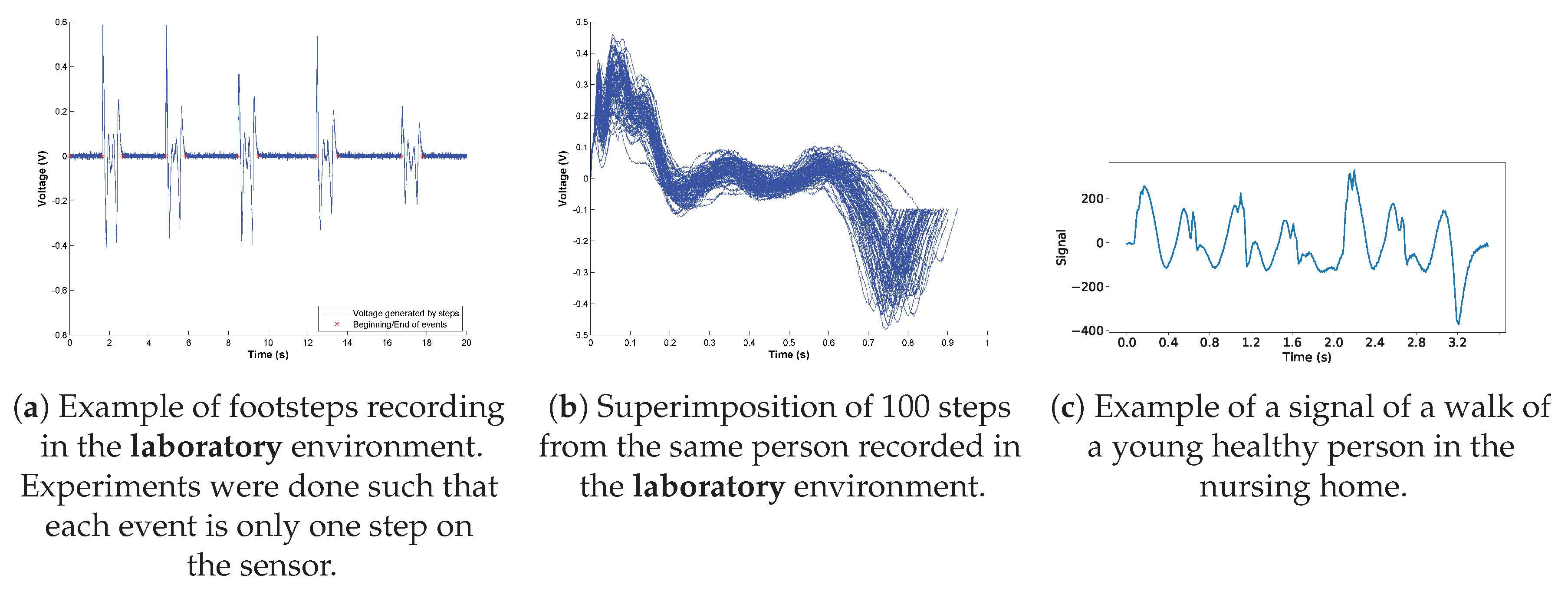
2.3. Data Collection
3. Results
3.1. Performance Evaluation
3.2. Ablation Analysis
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| NurseNet | Non-invasive Unit Recognition System for the Elderly Network |
| SPN | Step Proposal Network |
| RPN | Region Proposal Network |
| CNN | Convolutional Neural Network |
| CDL | Convolutional Dictionary Learning |
| RF | Random Forest |
References
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Vellas, B.; Van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.; Doehner, W.; Evans, J.; et al. Frailty consensus: A call to action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Vellas, B. Implementing frailty screening, assessment, and sustained intervention: The experience of the Gérontopôle. J. Nutr. Health Aging 2015, 19, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Fried, T.R.; Mor, V. Frailty and hospitalization of long-term stay nursing home residents. J. Am. Geriatr. Soc. 1997, 45, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Avorn, J.; Langer, E. Induced disability in nursing home patients: A controlled trial. J. Am. Geriatr. Soc. 1982, 30, 397–400. [Google Scholar] [CrossRef] [PubMed]
- Fiatarone, M.A.; O’Neill, E.F.; Ryan, N.D.; Clements, K.M.; Solares, G.R.; Nelson, M.E.; Roberts, S.B.; Kehayias, J.J.; Lipsitz, L.A.; Evans, W.J. Exercise training and nutritional supplementation for physical frailty in very elderly people. N. Engl. J. Med. 1994, 330, 1769–1775. [Google Scholar] [CrossRef] [PubMed]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef]
- Blair, S.N.; Kohl, H.W.; Gordon, N.F.; Paffenbarger, R.S., Jr. How much physical activity is good for health? Annu. Rev. Public Health 1992, 13, 99–126. [Google Scholar] [CrossRef]
- Mukhopadhyay, S.C. Wearable sensors for human activity monitoring: A review. IEEE Sens. J. 2014, 15, 1321–1330. [Google Scholar] [CrossRef]
- Serra, R.; Knittel, D.; Di Croce, P.; Peres, R. Activity recognition with smart polymer floor sensor: Application to human footstep recognition. IEEE Sens. J. 2016, 16, 5757–5775. [Google Scholar] [CrossRef]
- Cucchiara, R.; Prati, A.; Vezzani, R.; Emilia, R. A multi-camera vision system for fall detection and alarm generation. Expert Syst. 2007, 24, 334–345. [Google Scholar] [CrossRef]
- Zhuang, X.; Huang, J.; Potamianos, G.; Hasegawa-Johnson, M. Acoustic fall detection using Gaussian mixture models and GMM supervectors. In Proceedings of the 2009 IEEE International Conference on Acoustics, Speech and Signal Processing, Taipei, Taiwan, 19–24 April 2009; pp. 69–72. [Google Scholar]
- Jonghee, H.; Hyo Sun, J.; Beom Suk, J.; Kwang Suk, P. Gait detection from three dimensional acceleration signals of ankles for the patients with Parkinson’s disease. In Proceedings of the IEEE The International Special Topic Conference on Information Technology in Biomedicine, Ioannina, Epirus, Greece, 26 October 2006. [Google Scholar]
- Bourke, A.; O’Brien, J.; Lyons, G. Evaluation of a threshold-based tri-axial accelerometer fall detection algorithm. Gait Posture 2007, 26, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, E.L.; Mahoney, D.F. Acceptance of wearable technology by people with Alzheimer’s disease: Issues and accommodations. Am. J. Alzheimer’s Dis. Other Dementias 2010, 25, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Taborri, J.; Palermo, E.; Rossi, S.; Cappa, P. Gait partitioning methods: A systematic review. Sensors 2016, 16, 66. [Google Scholar] [CrossRef] [PubMed]
- Muro-De-La-Herran, A.; Garcia-Zapirain, B.; Mendez-Zorrilla, A. Gait analysis methods: An overview of wearable and non-wearable systems, highlighting clinical applications. Sensors 2014, 14, 3362–3394. [Google Scholar] [CrossRef] [PubMed]
- Ao, B.; Wang, Y.; Liu, H.; Li, D.; Song, L.; Li, J. Context Impacts in Accelerometer-Based Walk Detection and Step Counting. Sensors 2018, 18, 3604. [Google Scholar] [CrossRef]
- Derawi, M.O. Accelerometer-based gait analysis, a survey. In Proceedings of the Nor Informasjonssikkerhetskonferanse NISK 2010, Gjovik, Norway, 23–24 November 2010. [Google Scholar]
- Wang, W.; Liu, A.X.; Shahzad, M. Gait recognition using wifi signals. In Proceedings of the 2016 ACM International Joint Conference on Pervasive and Ubiquitous Computing, Heidelberg, Germany, 12–16 September 2016; pp. 363–373. [Google Scholar]
- Jiang, H.; Cai, C.; Ma, X.; Yang, Y.; Liu, J. Smart home based on WiFi sensing: A survey. IEEE Access 2018, 6, 13317–13325. [Google Scholar] [CrossRef]
- Pan, S.; Yu, T.; Mirshekari, M.; Fagert, J.; Bonde, A.; Mengshoel, O.J.; Noh, H.Y.; Zhang, P. Footprintid: Indoor pedestrian identification through ambient structural vibration sensing. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2017, 1, 89. [Google Scholar] [CrossRef]
- Fagert, J.; Mirshekari, M.; Pan, S.; Zhang, P.; Noh, H.Y. Characterizing left-right gait balance using footstep-induced structural vibrations. In Sensors and Smart Structures Technologies for Civil, Mechanical, and Aerospace Systems 2017; International Society for Optics and Photonics: Bellingham, WA, USA, 2017; Volume 10168, p. 1016819. [Google Scholar]
- Yun, J.; Woo, W.; Ryu, J. User identification using user’s walking pattern over the ubiFloorII. In Computational Intelligence and Security; Springer: Berlin/Heidelberg, Germany, 2005; pp. 949–956. [Google Scholar]
- Suutala, J.; Fujinami, K.; Röning, J. Gaussian process person identifier based on simple floor sensors. In Smart Sensing and Context; Springer: Berlin/Heidelberg, Germany, 2008; pp. 55–68. [Google Scholar]
- Rimminen, H.; Lindström, J.; Sepponen, R. Positioning accuracy and multi-target separation with a human tracking system using near field imaging. Int. J. Smart Sens. Intell. Syst. 2009, 2, 156–175. [Google Scholar] [CrossRef]
- Henry, R.; Matti, L.; Raimo, S. Human tracking using near field imaging. In Proceedings of the 2008 Second International Conference on Pervasive Computing Technologies for Healthcare, Tampere, Finland, 30 January–1 February 2008; pp. 148–151. [Google Scholar]
- Valtonen, M.; Maentausta, J.; Vanhala, J. Tiletrack: Capacitive human tracking using floor tiles. In Proceedings of the 2009 IEEE International Conference on Pervasive Computing And Communications, Galveston, TX, USA, 9–13 March 2009; pp. 1–10. [Google Scholar]
- Tanaka, O.; Ryu, T.; Hayashida, A.; Moshnyaga, V.G.; Hashimoto, K. A smart carpet design for monitoring people with dementia. In Progress in Systems Engineering; Springer: Cham, Switzerland, 2015; pp. 653–659. [Google Scholar]
- Suutala, J.; Röning, J. Methods for person identification on a pressure-sensitive floor: Experiments with multiple classifiers and reject option. Inf. Fusion 2008, 9, 21–40. [Google Scholar] [CrossRef]
- Rodríguez, R.V.; Lewis, R.P.; Mason, J.S.; Evans, N.W. Footstep recognition for a smart home environment. Int. J. Smart Home 2008, 2, 95–110. [Google Scholar]
- Sacco, I.d.C.N.; Amadio, A.C. A study of biomechanical parameters in gait analysis and sensitive cronaxie of diabetic neuropathic patients. Clin. Biomech. 2000, 15, 196–202. [Google Scholar] [CrossRef]
- Dockstader, S.L.; Berg, M.J.; Tekalp, A.M. Stochastic kinematic modeling and feature extraction for gait analysis. IEEE Trans. Image Process. 2003, 12, 962–976. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Liu, W.; Ma, H.; Fu, H. Siamese neural network based gait recognition for human identification. In Proceedings of the 2016 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Shanghai, China, 20–25 March 2016; pp. 2832–2836. [Google Scholar]
- González, R.C.; López, A.M.; Rodriguez-Uría, J.; Álvarez, D.; Alvarez, J.C. Real-time gait event detection for normal subjects from lower trunk accelerations. Gait Posture 2010, 31, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Ying, H.; Silex, C.; Schnitzer, A.; Leonhardt, S.; Schiek, M. Automatic step detection in the accelerometer signal. In Proceedings of the 4th International Workshop on Wearable and Implantable Body Sensor Networks (BSN 2007), Aachen, Germany, 26–28 March 2007; pp. 80–85. [Google Scholar]
- Bae, J.; Tomizuka, M. Gait phase analysis based on a Hidden Markov Model. Mechatronics 2011, 21, 961–970. [Google Scholar] [CrossRef]
- Brajdic, A.; Harle, R. Walk detection and step counting on unconstrained smartphones. In Proceedings of the 2013 ACM International Joint Conference on Pervasive and Ubiquitous Computing, Zurich, Switzerland, 8–12 September 2013; pp. 225–234. [Google Scholar]
- Barralon, P.; Vuillerme, N.; Noury, N. Walk detection with a kinematic sensor: Frequency and wavelet comparison. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 1711–1714. [Google Scholar]
- Zhang, Y.; Ogunbona, P.O.; Li, W.; Munro, B.; Wallace, G.G. Pathological gait detection of parkinson’s disease using sparse representation. In Proceedings of the 2013 International Conference on Digital Image Computing: Techniques and Applications (DICTA), Hobart, Australia, 26–28 November 2013; pp. 1–8. [Google Scholar]
- Li, M.; Tian, S.; Sun, L.; Chen, X. Gait Analysis for Post-Stroke Hemiparetic Patient by Multi-Features Fusion Method. Sensors 2019, 19, 1737. [Google Scholar] [CrossRef] [PubMed]
- Mairal, J.; Ponce, J.; Sapiro, G.; Zisserman, A.; Bach, F.R. Supervised dictionary learning. In Advances in Neural Information Processing Systems; Curran Associates, Inc.: Red Hook, NY, USA, 2009; pp. 1033–1040. [Google Scholar]
- Huang, K.; Aviyente, S. Sparse representation for signal classification. In Advances in Neural Information Processing Systems; MIT Press: Cambridge, MA, USA, 2007; pp. 609–616. [Google Scholar]
- Aharon, M.; Elad, M.; Bruckstein, A. rmk-SVD: An algorithm for designing overcomplete dictionaries for sparse representation. IEEE Trans. Signal Process. 2006, 54, 4311–4322. [Google Scholar] [CrossRef]
- Mairal, J.; Bach, F.; Ponce, J.; Sapiro, G. Online learning for matrix factorization and sparse coding. J. Mach. Learn. Res. 2010, 11, 19–60. [Google Scholar]
- Garcia-Cardona, C.; Wohlberg, B. Convolutional dictionary learning: A comparative review and new algorithms. IEEE Trans. Comput. Imaging 2018, 4, 366–381. [Google Scholar] [CrossRef]
- Poschadel, N.; Moghaddamnia, S.; Alcaraz, J.C.; Steinbach, M.; Peissig, J. A dictionary learning based approach for gait classification. In Proceedings of the 2017 22nd International Conference on Digital Signal Processing (DSP), London, UK, 23–25 August 2017; pp. 1–4. [Google Scholar]
- Ouyang, W.; Wang, X.; Zeng, X.; Qiu, S.; Luo, P.; Tian, Y.; Li, H.; Yang, S.; Wang, Z.; Loy, C.C.; et al. Deepid-net: Deformable deep convolutional neural networks for object detection. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 2403–2412. [Google Scholar]
- Cai, Z.; Fan, Q.; Feris, R.S.; Vasconcelos, N. A unified multi-scale deep convolutional neural network for fast object detection. In Proceedings of the EUropean Conference on Computer Vision, Amsterdam, The Netherlands, 8–16 October 2016; pp. 354–370. [Google Scholar]
- Li, G.; Yu, Y. Deep contrast learning for salient object detection. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 478–487. [Google Scholar]
- Ren, S.; He, K.; Girshick, R.; Sun, J. Faster r-cnn: Towards real-time object detection with region proposal networks. In Advances in Neural Information Processing Systems; Curran Associates, Inc.: Red Hook, NY, USA, 2015; pp. 91–99. [Google Scholar]
- Redmon, J.; Divvala, S.; Girshick, R.; Farhadi, A. You only look once: Unified, real-time object detection. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 779–788. [Google Scholar]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436. [Google Scholar] [CrossRef]
- Suder, K.; Drepper, F.R.; Schiek, M.; Abel, H.H. One-dimensional, nonlinear determinism characterizes heart rate pattern during paced respiration. Am. J. Physiol. Heart Circ. Physiol. 1998, 275, H1092–H1102. [Google Scholar] [CrossRef]
- Rubin, J.; Parvaneh, S.; Rahman, A.; Conroy, B.; Babaeizadeh, S. Densely connected convolutional networks and signal quality analysis to detect atrial fibrillation using short single-lead ECG recordings. In Proceedings of the 2017 Computing in Cardiology (CinC), Rennes, France, 24–27 September 2017; pp. 1–4. [Google Scholar]
- Kiranyaz, S.; Ince, T.; Gabbouj, M. Real-time patient-specific ECG classification by 1-D convolutional neural networks. IEEE Trans. Biomed. Eng. 2015, 63, 664–675. [Google Scholar] [CrossRef] [PubMed]
- Serra, R. Développement et Caractérisation d’un Système de sol Piézoélectrique Intelligent. Application à la Détection des Chutes. Ph.D. Thesis, Université de Strasbourg, Strasbourg, France, 2017. [Google Scholar]
- Nair, V.; Hinton, G.E. Rectified linear units improve restricted boltzmann machines. In Proceedings of the 27th International Conference on Machine Learning (ICML-10), Haifa, Israel, 21–24 June 2010; pp. 807–814. [Google Scholar]
- Yosinski, J.; Clune, J.; Bengio, Y.; Lipson, H. How transferable are features in deep neural networks? In Advances in Neural Information Processing Systems; Curran Associates, Inc.: Red Hook, NY, USA, 2014; pp. 3320–3328. [Google Scholar]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Nesterov, Y. A method for unconstrained convex minimization problem with the rate of convergence O (1/k^ 2). Doklady AN USSR 1983, 269, 543–547. [Google Scholar]
- Prechelt, L. Early stopping-but when? In Neural Networks: Tricks of the Trade; Springer: Berlin/Heidelberg, Germany, 1998; pp. 55–69. [Google Scholar]
- Rubinstein, R.; Zibulevsky, M.; Elad, M. Double sparsity: Learning sparse dictionaries for sparse signal approximation. IEEE Trans. Signal Process. 2009, 58, 1553–1564. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. In Advances in Neural Information Processing Systems; Curran Associates, Inc.: Red Hook, NY, USA, 2012; pp. 1097–1105. [Google Scholar]
- Pal, K.K.; Sudeep, K. Preprocessing for image classification by convolutional neural networks. In Proceedings of the 2016 IEEE International Conference on Recent Trends in Electronics, Information & Communication Technology (RTEICT), Bangalore, India, 20–21 May 2016; pp. 1778–1781. [Google Scholar]
- Antonsson, E.K.; Mann, R.W. The frequency content of gait. J. Biomech. 1985, 18, 39–47. [Google Scholar] [CrossRef]
- Um, T.T.; Pfister, F.M.J.; Pichler, D.; Endo, S.; Lang, M.; Hirche, S.; Fietzek, U.; Kulić, D. Data augmentation of wearable sensor data for Parkinson’s disease monitoring using convolutional neural networks. arXiv 2017, arXiv:1706.00527. [Google Scholar]
- Minvielle, L.; Atiq, M.; Serra, R.; Mougeot, M.; Vayatis, N. Fall detection using smart floor sensor and supervised learning. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Seogwipo, Korea, 11–15 July 2017; pp. 3445–3448. [Google Scholar]
- Robinson, J.L.; Smidt, G.L. Quantitative gait evaluation in the clinic. Phys. Ther. 1981, 61, 351–353. [Google Scholar] [CrossRef]
- Gabell, A.; Nayak, U. The effect of age on variability in gait. J. Gerontol. 1984, 39, 662–666. [Google Scholar] [CrossRef]
- Garcia-Cardona, C.; Wohlberg, B. Subproblem coupling in convolutional dictionary learning. In Proceedings of the 2017 IEEE International Conference on Image Processing (ICIP), Beijing, China, 17–20 September 2017; pp. 1697–1701. [Google Scholar]
- Boyd, S.; Parikh, N.; Chu, E.; Peleato, B.; Eckstein, J. Distributed optimization and statistical learning via the alternating direction method of multipliers. Found. Trends Mach. Learn. 2011, 3, 1–122. [Google Scholar] [CrossRef]
- Wohlberg, B. SPORCO: A Python package for standard and convolutional sparse representations. In Proceedings of the 15th Python in Science Conference, Austin, TX, USA, 11–17 July 2016; pp. 1–8. [Google Scholar]
- Holden, M.K.; Gill, K.M.; Magliozzi, M.R.; Nathan, J.; Piehl-Baker, L. Clinical gait assessment in the neurologically impaired: Reliability and meaningfulness. Phys. Ther. 1984, 64, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Rifkin, R.M. Everything Old Is New Again: A Fresh Look at Historical Approaches in Machine Learning. Ph.D. Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 2002. [Google Scholar]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Event | Number of Instances |
|---|---|
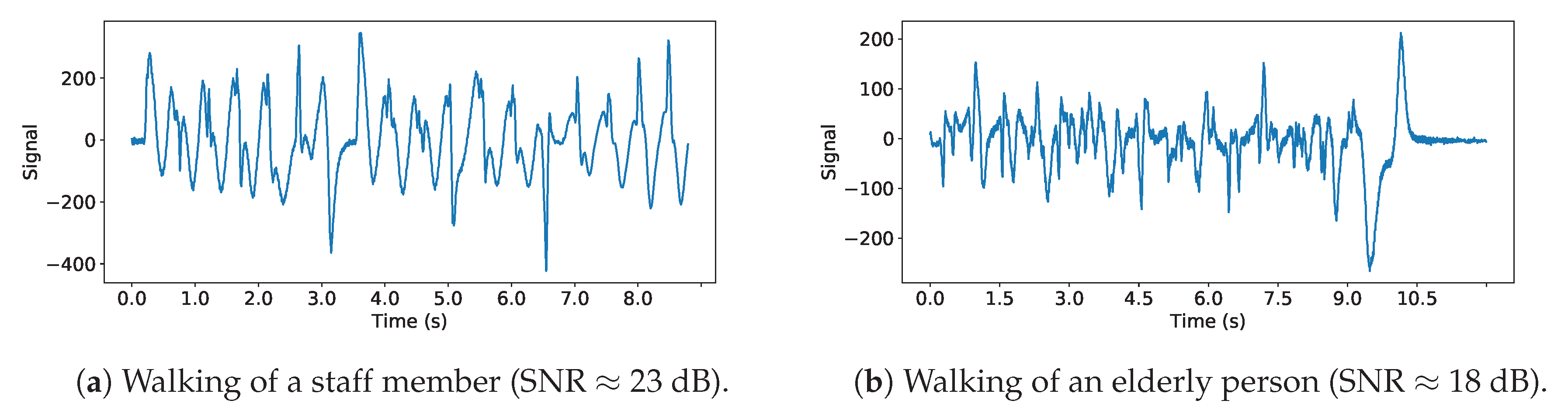
| Walking, 1 person, staff | 42 |
| Walking, 1 person, elderly | 16 |
| Walking, >1 person | 11 |
| Wheelchair | 9 |
| Wheelchair pushed by another | 5 |
| Walking with a cart | 5 |
| Other events | 5 |
| Label | Staff | Elderly |
|---|---|---|
| Single Walk | 40 | 18 |
| Multiple Walks | 8 | 3 |
| Other | 7 | 17 |
| Staff | Elderly | ||||||
|---|---|---|---|---|---|---|---|
| Single Walk | Multiple Walks | Other | Single Walk | Multiple Walks | Other | ||
| Test | Classified Staff | 13 | 3 | 1 | 2 | 0 | 0 |
| Classified Elderly | 0 | 0 | 1 | 4 | 1 | 6 | |
| All | Classified Staff | 40 | 7 | 5 | 4 | 1 | 1 |
| Classified Elderly | 0 | 1 | 2 | 14 | 2 | 16 | |
| Test | Classified Staff | 12 | 2 | 1 | 1 | 0 | 0 |
| Classified Elderly | 1 | 1 | 1 | 5 | 1 | 6 | |
| All | Classified Staff | 39 | 3 | 3 | 1 | 0 | 1 |
| Classified Elderly | 1 | 5 | 4 | 17 | 3 | 16 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minvielle, L.; Audiffren, J. NurseNet: Monitoring Elderly Levels of Activity with a Piezoelectric Floor. Sensors 2019, 19, 3851. https://doi.org/10.3390/s19183851
Minvielle L, Audiffren J. NurseNet: Monitoring Elderly Levels of Activity with a Piezoelectric Floor. Sensors. 2019; 19(18):3851. https://doi.org/10.3390/s19183851
Chicago/Turabian StyleMinvielle, Ludovic, and Julien Audiffren. 2019. "NurseNet: Monitoring Elderly Levels of Activity with a Piezoelectric Floor" Sensors 19, no. 18: 3851. https://doi.org/10.3390/s19183851
APA StyleMinvielle, L., & Audiffren, J. (2019). NurseNet: Monitoring Elderly Levels of Activity with a Piezoelectric Floor. Sensors, 19(18), 3851. https://doi.org/10.3390/s19183851