1. Introduction
The post stroke gait disturbance is one of the major complications that requires a long-term rehabilitation and limits the patient’s activities of daily living [
1]. The improved gait function is an important factor in returning to social life and thus is an essential goal of rehabilitation therapy [
2]. While 60% to 80% of stroke patients regain their independent ambulation function, many exhibit hemiparetic gait pattern for the rest of their lives due to unilateral neuromuscular weakness leading to gait asymmetry [
2,
3,
4]. The critical consequences of the impaired walking ability after a stroke include a reduction in gait speed, shorter step and stride lengths, and an increased fall risk [
5,
6]. These residual deficits are mainly caused by muscle weakness and imbalance, decreased weight support on the affected side, and asymmetrical intralimb coordination [
7,
8]. For the patients with these deviations to regain walking abilities, clinical treatments commonly rely on traditional rehabilitation approaches such as neuromuscular re-education, lower limb strength training, and balance training for weight shifting and gait pattern training. While the patients and healthcare providers strive to seek for more effective gait therapy methods, there are not many long-term remedies or set devices for facilitating these treatment options in clinical settings.
With fast growing advances in technology, various forms of wearable measuring-recording devices and sensors have been developed for the health care system. For gait rehabilitation, force sensitive resistor sensors (FSR) are one of the most commonly used sensor types for analyzing gait pattern or plantar pressure, but is known to have the disadvantage of being deformed in time as a response to repetitive force applied. Another drawback of the FSR sensor is the need to be constantly calibrated (good for approximately 100 uses) and its inability to distinguish between load changes in respect to the weight bearing level difference generated during walking [
9,
10]. Another popular type considered for gait biofeedback sensors is piezoelectric material, which has a high impedance, low noise, and susceptibility to electrical interference. However, its weakness is having a limited pressure range and non-linearity in repeated signal output [
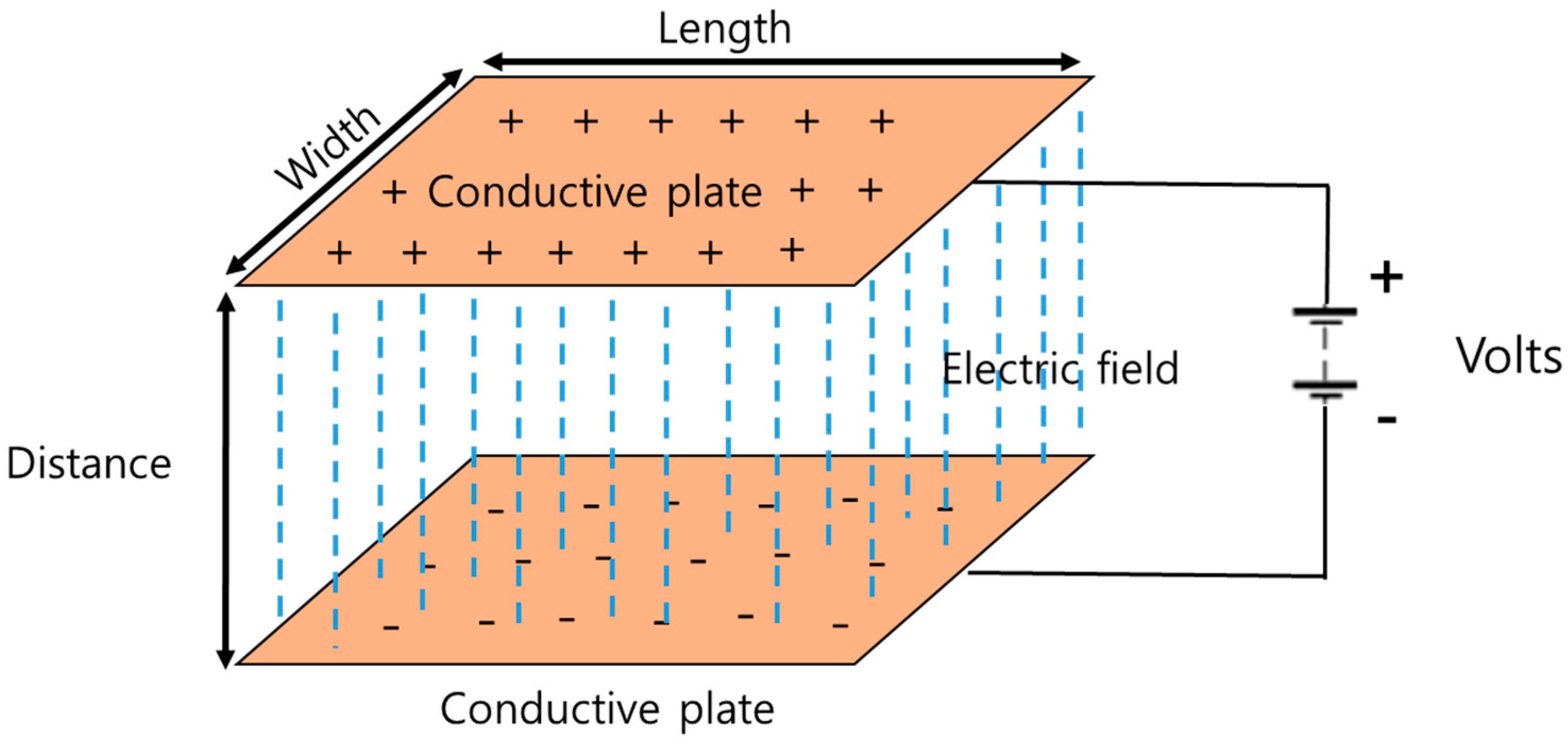
9]. According to a study by Aqueveque et al. (2018), capacitive sensors can be used for developing an in-shoe device that measures plantar pressure [
9]. A capacitive sensor basically consists of two conductive plates that are separated by dielectric material. Modifying the distance between the conductive plates generates a variation of the capacitance and this change in capacitive value can be interpreted as plantar pressure change [
9]. This study developed a capacitive insole sensor to analyze plantar pressure and with the aim to provide real-time feedback on the patients’ gait rehabilitation processes.
The assessment of gait rehabilitation is usually made using clinical scales, but many of the neuromuscular disabilities are still being evaluated manually with analog scales [
11,
12,
13,
14,
15]. Thus, it is difficult to verify the accuracy in measurement methods, and both the intra- and inter-personal evaluation results have low reliability. A practical device that can quantitatively analyze the characteristics of hemiparetic gait pre and post rehabilitation is substantially needed. A recent study by Ngueleu et al. (2019) stated that, although using pressure-sensing insoles for identification of the step count is a promising approach in gait analysis, the accuracy of the activity monitors in step counting remains limited and that there appears to be no consensus for optimal positioning and the number of sensors for insoles [
10].
In stroke rehabilitation, the basic gait analysis parameters include the plantar pressure distribution, the step count, the stride time, velocity (or gait speed), the center of pressure (CoP), the coefficient of variation (CV) and the phase coordination index (PCI) [
16,
17,
18,
19,
20,
21,
22,
23]. Among these indices, plantar pressure and PCI have shown to be relatively more sensitive measures in analyzing the bilateral coordination or asymmetry of locomotion and balance, which are meaningful variables [
16,
17,
24,
25]. According to previous studies, the wearable gait analysis system [
26], such as with insole pressure sensors, can analyze gait parameters including gait velocity, cadence, stride length, step length, stride time, single limb support and stance (coordination function) by analyzing pressure between the foot plantar surface and the shoe insole. Therefore, this study developed an insole-type wearable pressure sensor.
In several other previous studies, the insole-type pressure sensor and smart shoes were developed for gait analysis and smart phone applications enabled real-time monitoring of the activities being carried out [
27,
28]. However, these devices are expensive, and the bio-signals collected and analyzed were reported to be not as accurate for use in clinical research [
29]. To solve the cost-related problem of the sensors, researchers tried to apply pressure sensors for a gait analysis system, but they were found to be short-lived, making them still expensive for both users and researchers. Based on these advantages, researchers are conducting studies on an insole type textile pressure sensor considering the properties of conductive textile that is user friendly and inexpensive [
30,
31,
32,
33,
34]. However, studies on the clinical application of the wearable textile insole sensor are scarce.
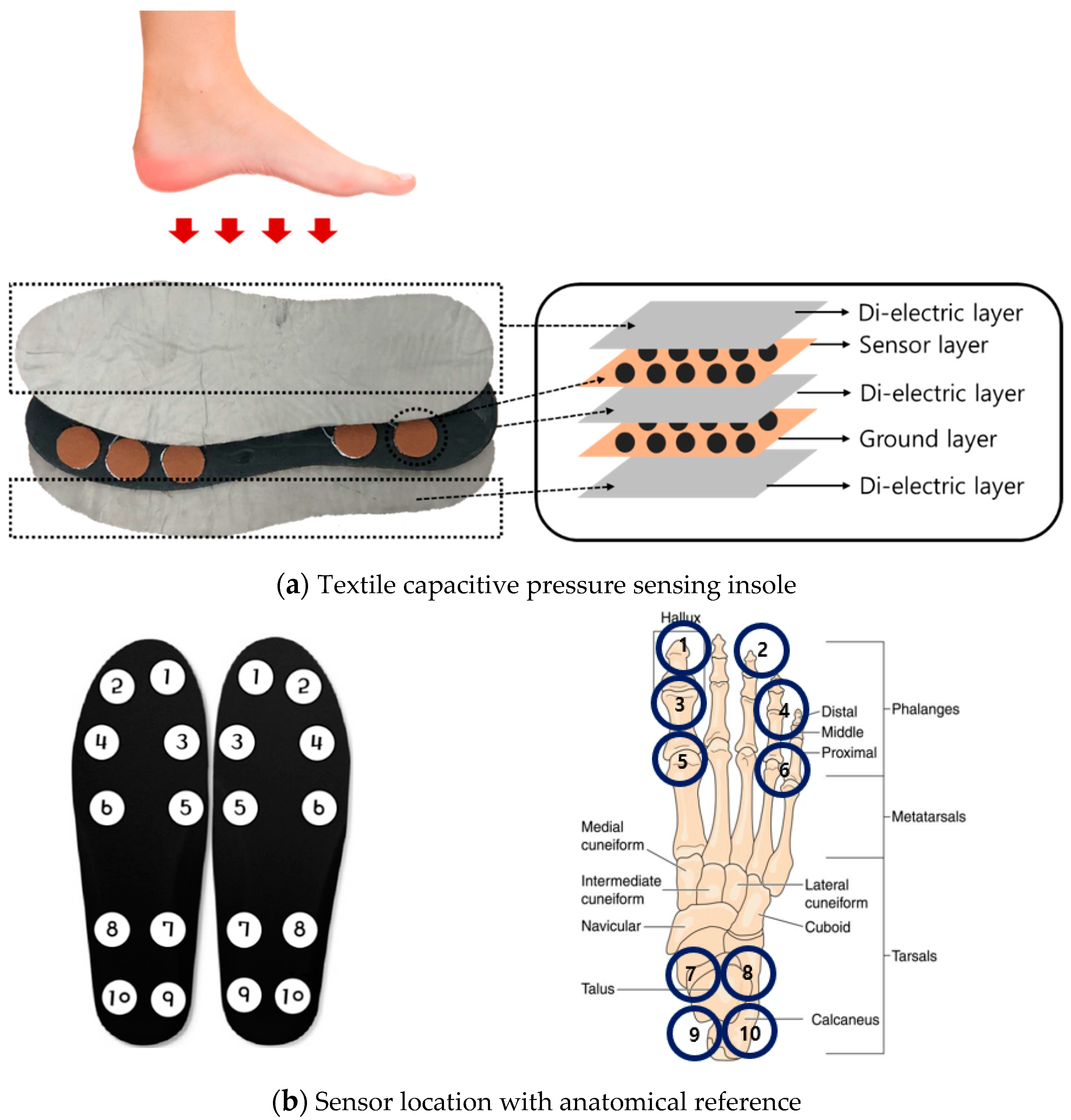
Therefore, this study developed a wearable textile capacitive pressure-sensing insole to test its feasibility in analyzing hemiparetic gait patterns and distinguishing its characteristics from normal gait.
4. Discussion
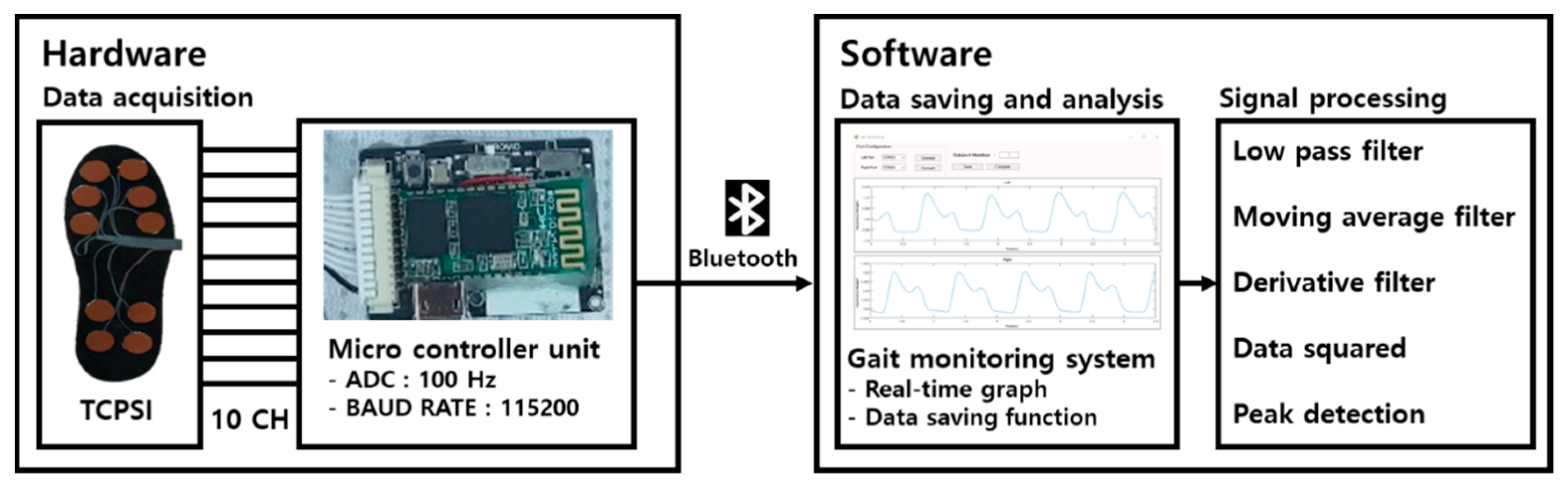
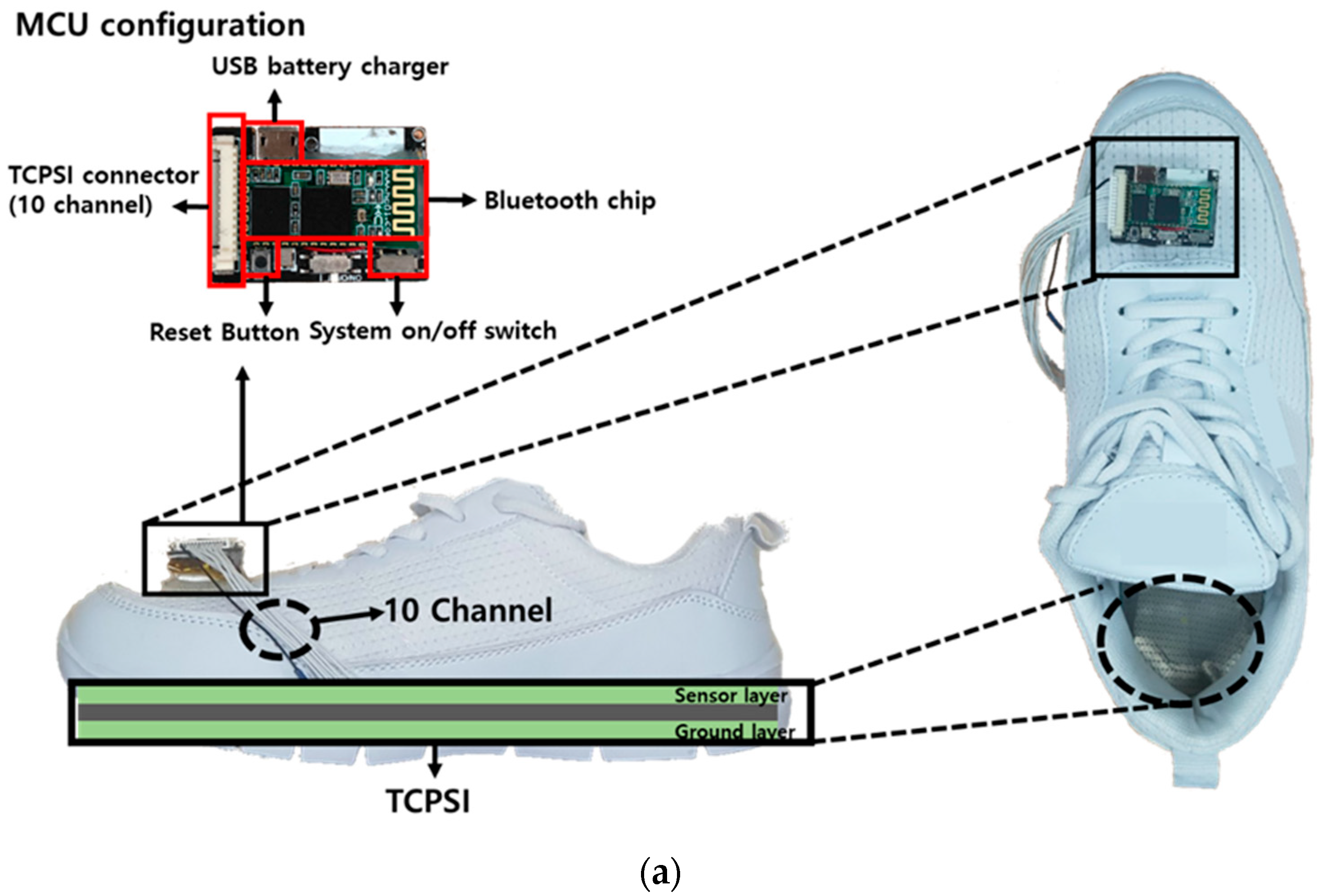
With the aim of producing a practical and reliable device to quantitatively analyze the human gait, a 10-channeled TCPSI and a real-time monitoring system were developed and applied in this study for hemiparetic gait pattern analysis in comparison with healthy adults. The results of this study showed that our sensor is capable of detecting and distinguishing the differences in plantar pressure (PPD), the step count, the stride time, the coefficient of variation, and the phase coordination index (PCI) between paretic and healthy limbs. These parameters were selected for analysis, because a stroke survivors’ gait abnormality is characterized by a pronounced gait asymmetry [
25], decreased gait speed and stance phase, shorter stride length, and prolonged swing phase of the paretic limb [
39]. These gait abnormalities along with muscle imbalance and weakness leads to a high risk of falls [
40,
41].
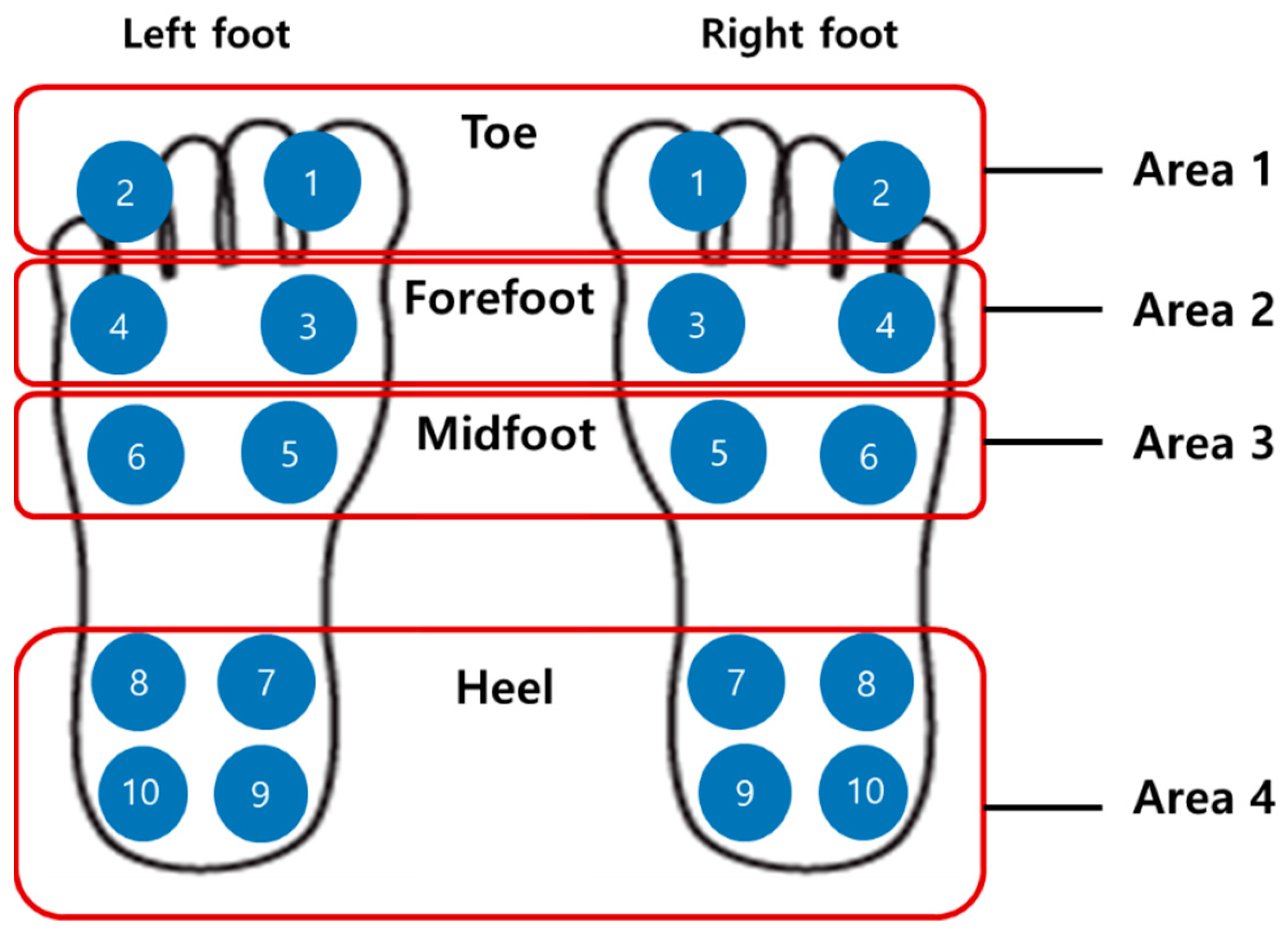
In this study, the subjects with hemiparesis showed the highest PPD in the toe area where the sensor numbers 1 and 2 were located (right hemi: 13.43%, left hemi: 28.27%). The closer to 0% the PPD is, the less the differential pressure of the feet, which means that the feet are well balanced [
17]. Sanghan et al. (2015) reported that the PPD of hemiparetic patients was 3 times higher than that of the healthy group [
17]. Normally in healthy subjects, the heel contacts first, followed by the midfoot, the forefoot, and then toe pressure. However, since hemiplegic patients do not pressurize the paralyzed feet properly when walking, it may have showed higher pressure in the toe area and in general compared to the healthy adult group. This result was congruent with the results in Perry’s research (1992) [
39]. Based on this, our proposed sensor was confirmed that it can detect the dynamic pressure difference of the two feet and be analyzed. In gait analysis, plantar pressure distribution is an important parameter for evaluating the balancing capability in terms of weight-shifting, balance strategies, and a risk of falls.
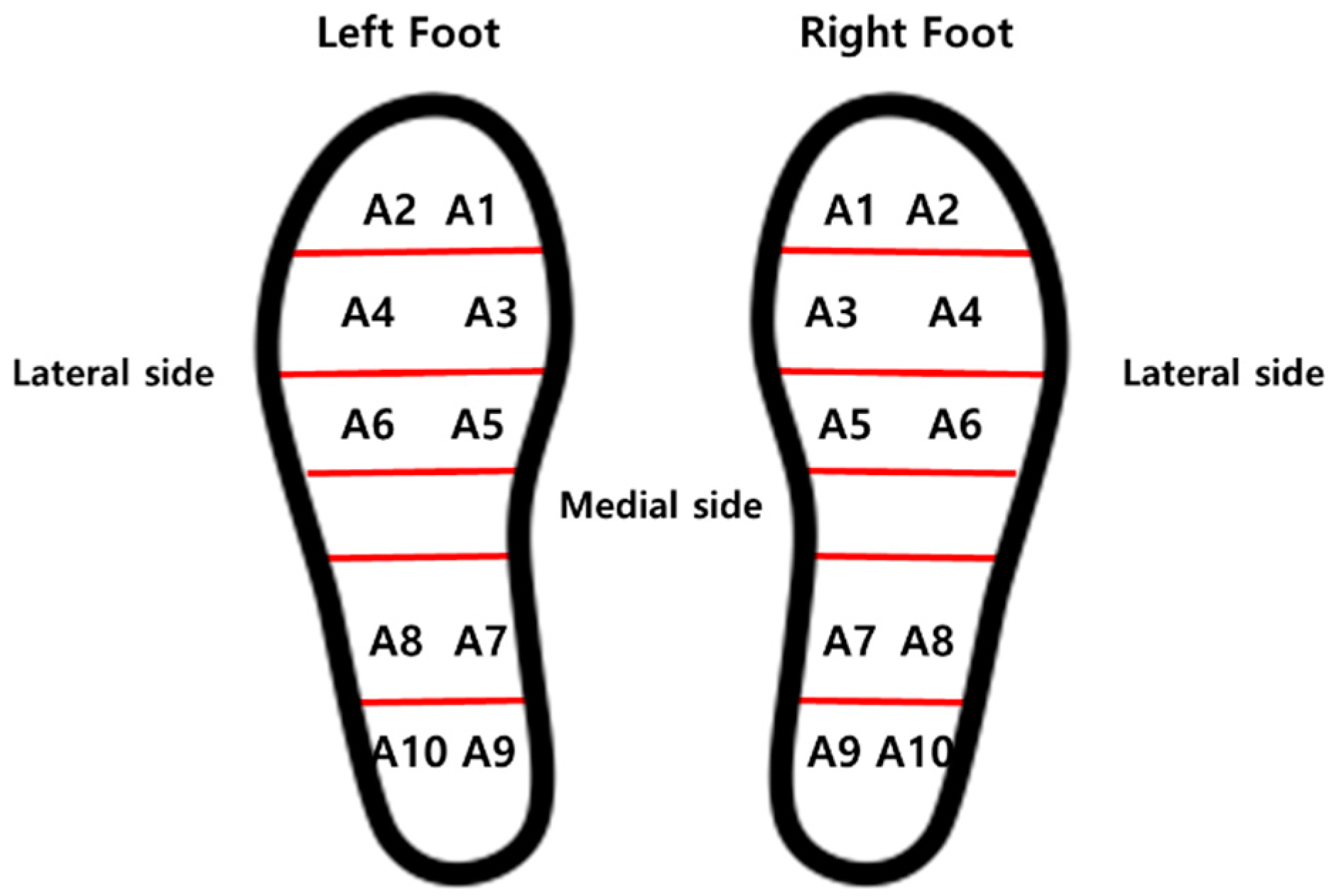
The plantar pressure distribution comparison analysis showed that the plantar pressure moves towards the lateral side of the affected foot in hemiparetic patients. This phenomenon occurs as a form of compensation to avoid falling. The patients shift their bodyweight towards the unaffected side for more secured stability [
42]. The plantar dynamics of the involved leg exhibited a transfer of initial contact from the hind to the forefoot, increased lateral plantar support, limited roll-over, and reduced or absent push-off at a terminal stance. There was a tendency for heel support to disappear on the paretic side with reduced functional abilities.
Field et al. (2013) reported that the patients with a stroke reduce daily stepping activities by 27% compared to a healthy adult [
43]. This was also found in our study results. The step count of hemiparetic patients was higher than that of healthy adults.
The average stride time difference between the right and left foot of left hemiparesis was 0.14 ± 0.04 s (
Table 4), those of the right hemiparesis was 0.11 ± 0.04 s, and of the bilateral hemiparesis was 0.04 ± 0.04 s, respectively (
Table 5 and
Table 6). The temporal aspects of hemiplegic gait are characterized by increased stride times [
44]. Hemiplegic patients usually have reduced joint excursion and insufficient forward propulsion, which may lead to an asymmetrical and unstable walking pattern [
5]. Since the single support time of the affected limb is significantly shorter than that of the unaffected limb, the unaffected limb’s step length is shorter than the affected limb’s step length [
4,
6]. Likely, the stride time of the affected foot was longer than the unaffected side in our study.
As presented in
Table 6, the time difference in the average stride time in healthy adults was 0.02 ± 0.01 s and the average stride time difference was three times lower than the hemiparetic patients. Mackenzie et al. (2006) and Sartini et al. (2010) reported that the stride time was related to falling and an abnormal gait pattern causes a risk of falls [
45,
46]. The elderly who have experienced falls are associated with a decrease in walking speed, stepping and an increase in step symmetry [
47]. Our proposed sensor system can also detect and decrease the risk of falls by real-time gait monitoring.
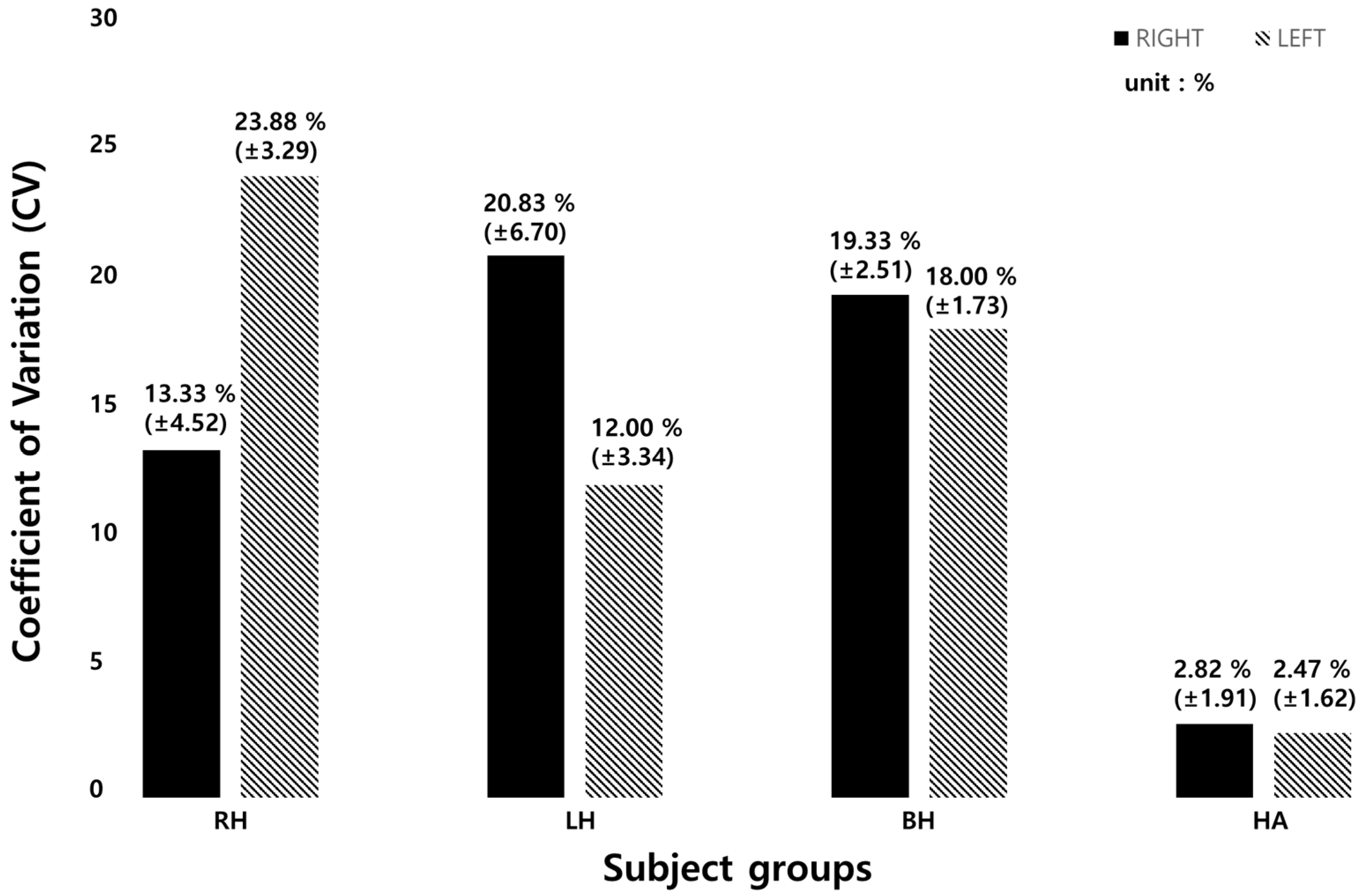
The CV is used to compare the magnitude of the change regardless of the data dimension. In this study, because the step length and the stride time may be different depending on the subject and the degree of the disease, the CV was calculated and the change amount was examined. The CV of stride time with heathy adults was 5 times higher than hemiparetic patients as shown in
Table 8 and
Figure 9. This means that hemiparetic patients cannot walk with a constant gait speed and thus walk irregularly. It was confirmed that our sensor can analyze various gait parameters.
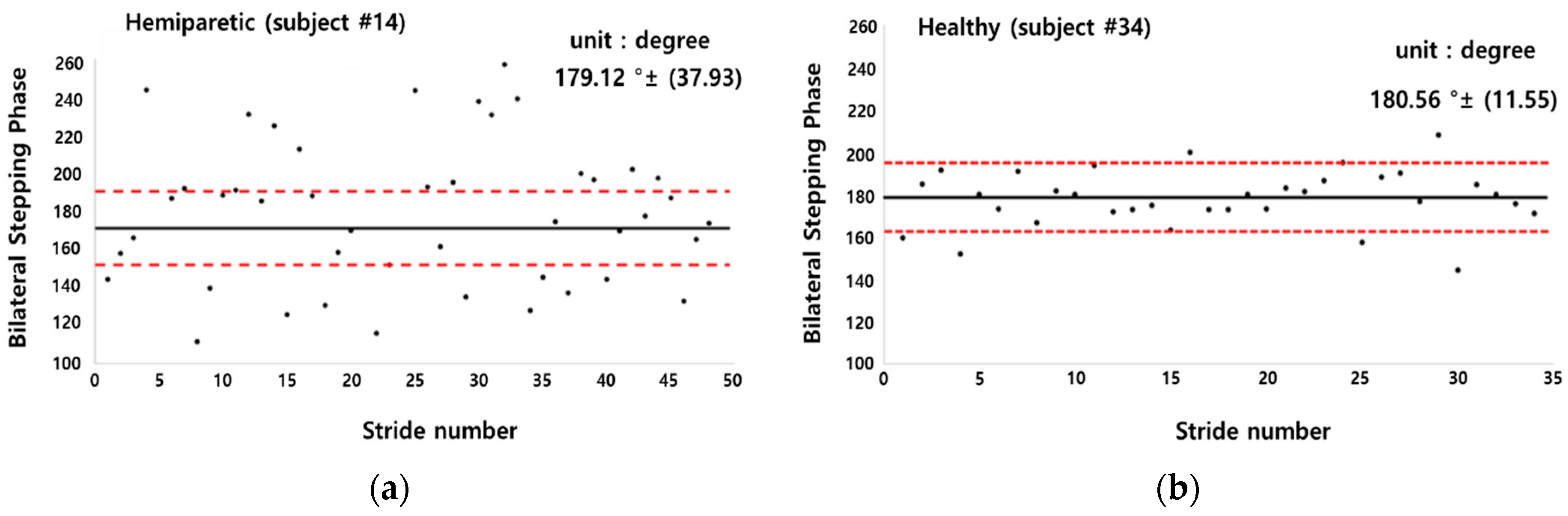
This study performed the PCI comparison between hemiparetic patients and healthy adults because hemiparetic gait is characterized by mild to severe asymmetric patterns. Hemiparetic patients have increased stance phase and double support duration. In addition, the stride length and step length decrease, and the paralyzed side has longer step [
48]. The PCI is an indicator for evaluating the balance of a pair of feet. A value closer to 0% refers to a higher balance between the two feet [
23,
24,
25,
48]. The PCI was originally developed to evaluate the asymmetry during walking and many studies evaluated the gait asymmetry of patients with Parkinson’s disease and a stroke [
23,
24,
25,
48]. In the previous studies evaluating gait asymmetry in patients with stroke patients [
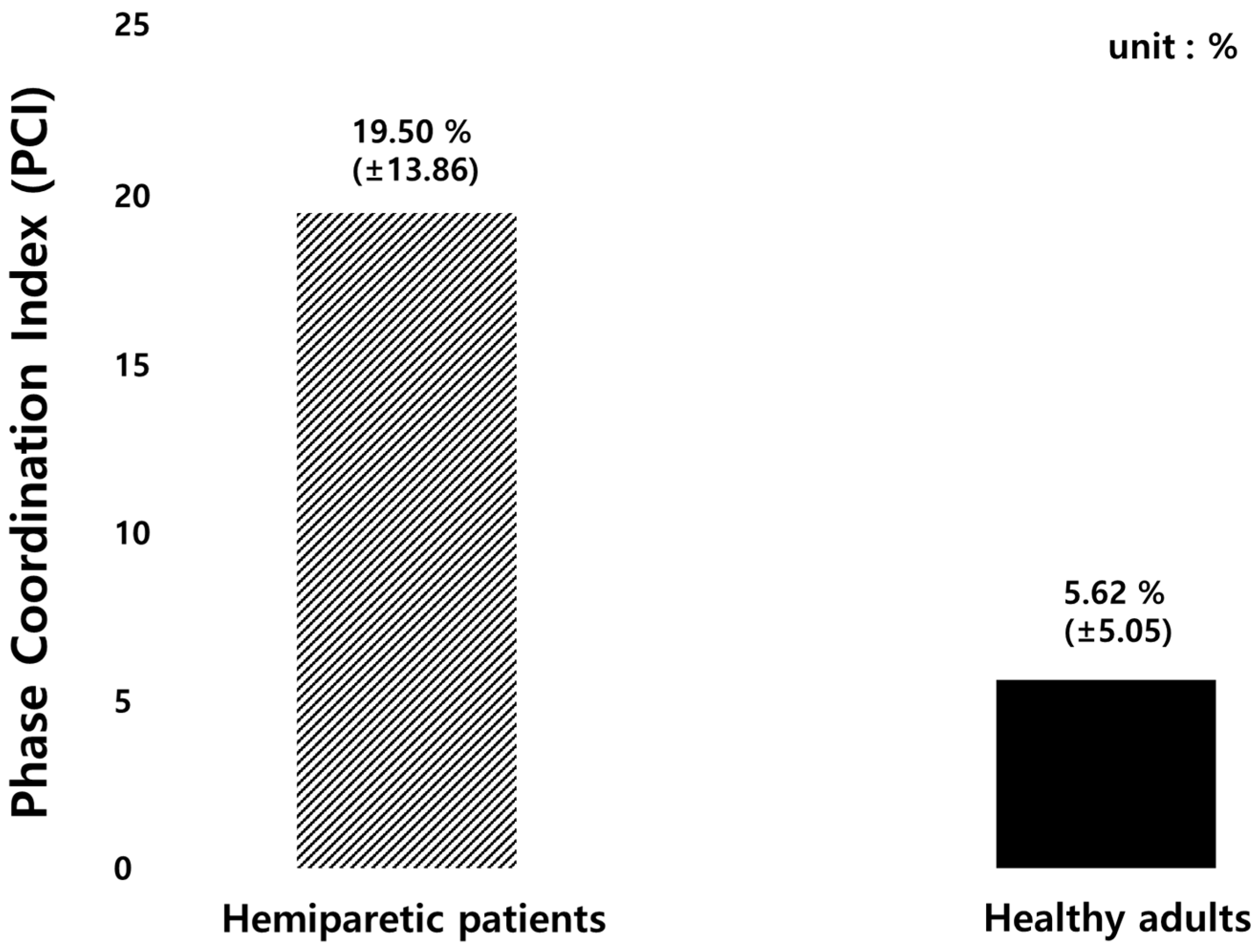
48], the PCI value of stroke patients was 19.5% ± 2.3% and that of healthy subjects was 6.2% ± 1.0%. The PCI value was approximately 3 times higher in the patient group than in the healthy group.
In this study, the PCI value of stroke patients was 19.5% ± 13.9% and that of healthy subjects was 5.6% ± 5.1%, showing similar results to the previous studies as summarized in
Table 7. Our results showed a higher standard deviation of the PCI value than that of previous studies. This may be because the age range of the subjects participating in this study was larger (63.3 ± 8.6 yrs.) The ages of the subjects (number 2, 6, 8, 10, and 14) were 65, 63, 63, 60, and 68, respectively, and were diagnosed with hemiparesis. The PCI values of the five subjects were 4.07%, 4.00%, 4.64%, 0.98%, 4.03%, respectively, which seemed to be similar to those of healthy adults. According to the previous studies, aging is associated with decreased stride time, velocity, step length during gait. Slowed walking speed leads to larger gait variability [
37]. Other previous studies explored age-related changes by analyzing gait speed and PCI values, and found out that the average gait speed decreases and the PCI value increases every decade from the age of 70 years [
49,
50,
51].
Study limitations: Generalizing the results of this study may be difficult because the number of subjects was small. In our previous study [
35], a soft-material-based pressure insole and its performance feasibility test for performing a clinical experiment was developed and analyzed. The study results showed that our pressure insole sensor was confirmed to have a high correlation with F-scan (R
2 0.90,
p < 0.05). Therefore, the sensor performance analysis was not repeated in this study.




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

