Feasibility of a Sensor-Based Gait Event Detection Algorithm for Triggering Functional Electrical Stimulation during Robot-Assisted Gait Training


Abstract
:1. Introduction
2. Materials and Methods
- Real-time gait detection from an easy-to-use system setup
- Arbitrary sensor alignment
- Functional electrical stimulation during robot-assisted gait training
- Despite introducing new technologies, keeping the additional time expenditure for the therapist on a low level
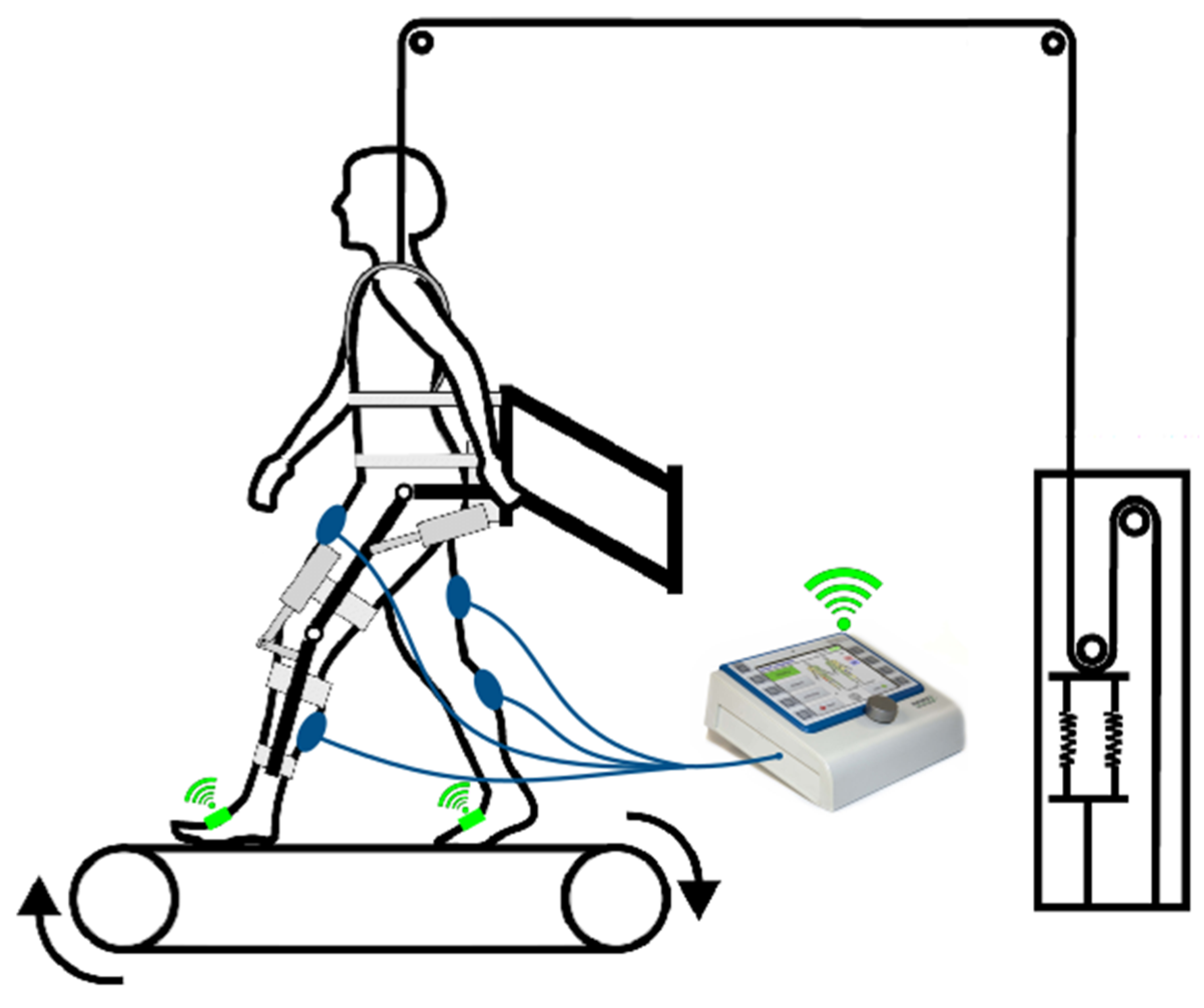
2.1. Robot-Assisted Gait Trainer
2.2. Electrical Stimulator
2.3. Inertial Measurement Unit
2.4. Automatic Real-Time Gait Detection Algorithm
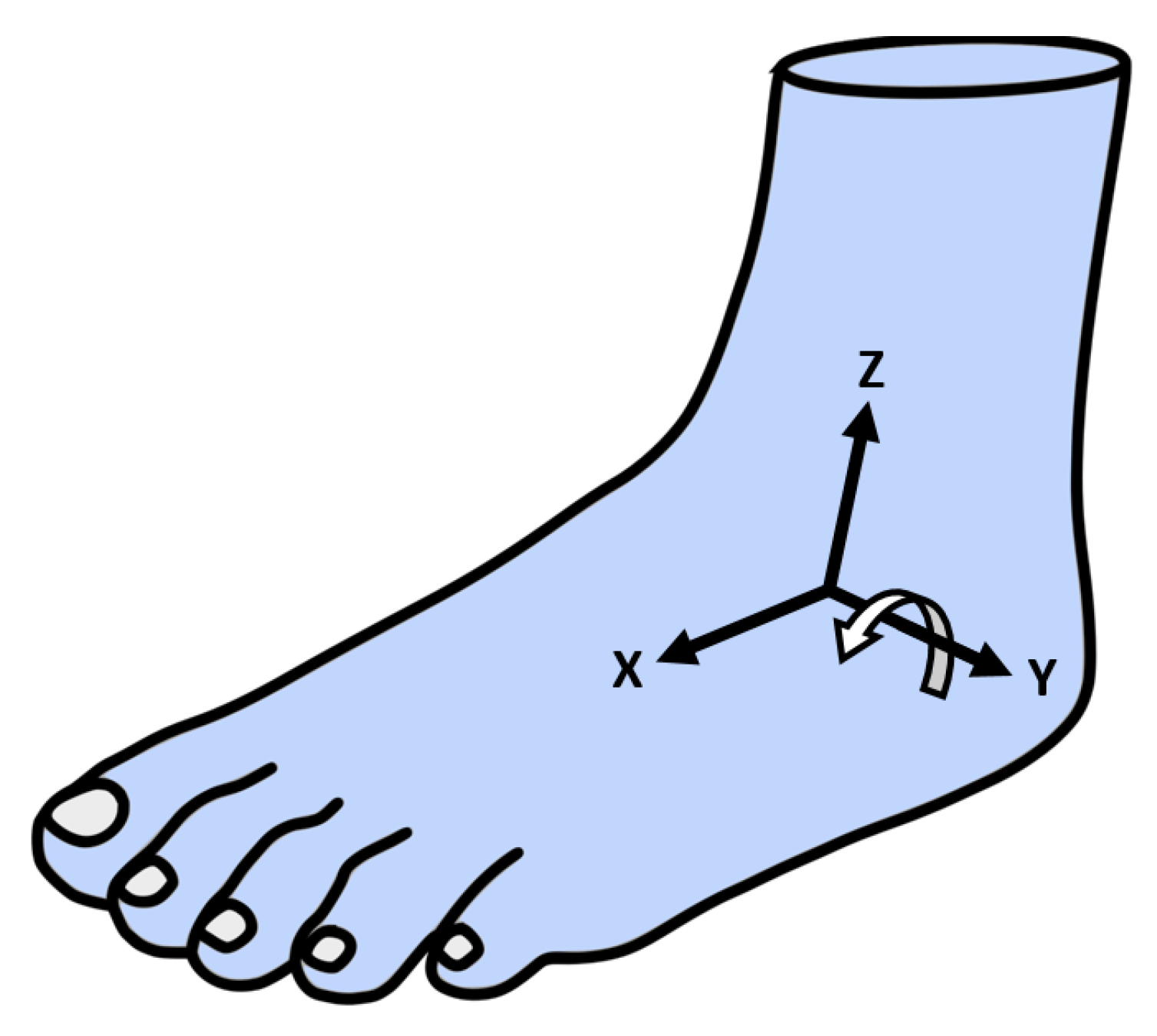
2.4.1. Arbitrary Sensor Alignment Algorithm
- Tightly attaching the sensor to the foot and overlapping the two coordinate systems manually.
- Calculating the current orientation of the sensor for each data point using an arbitrary sensor alignment algorithm.
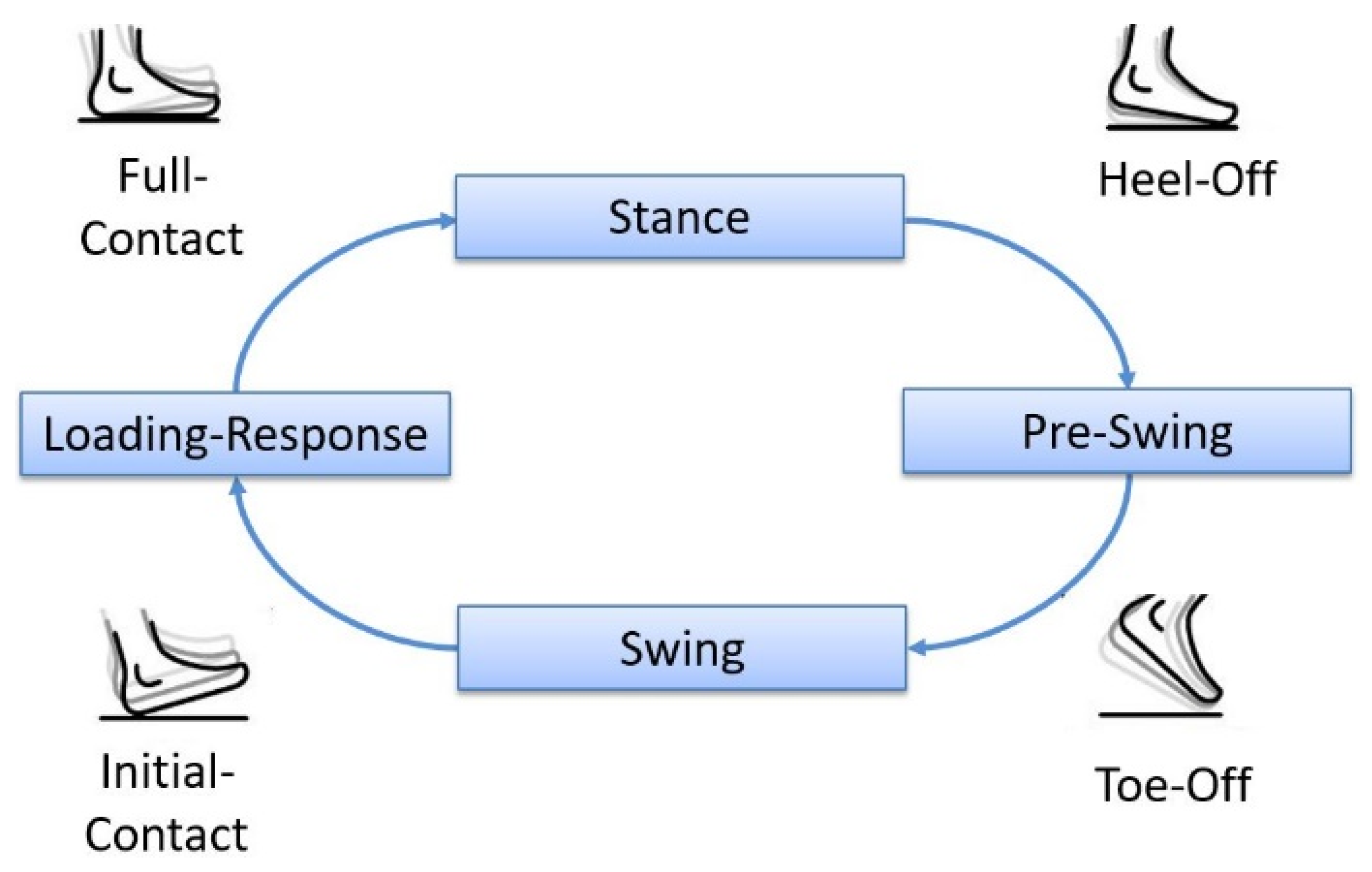
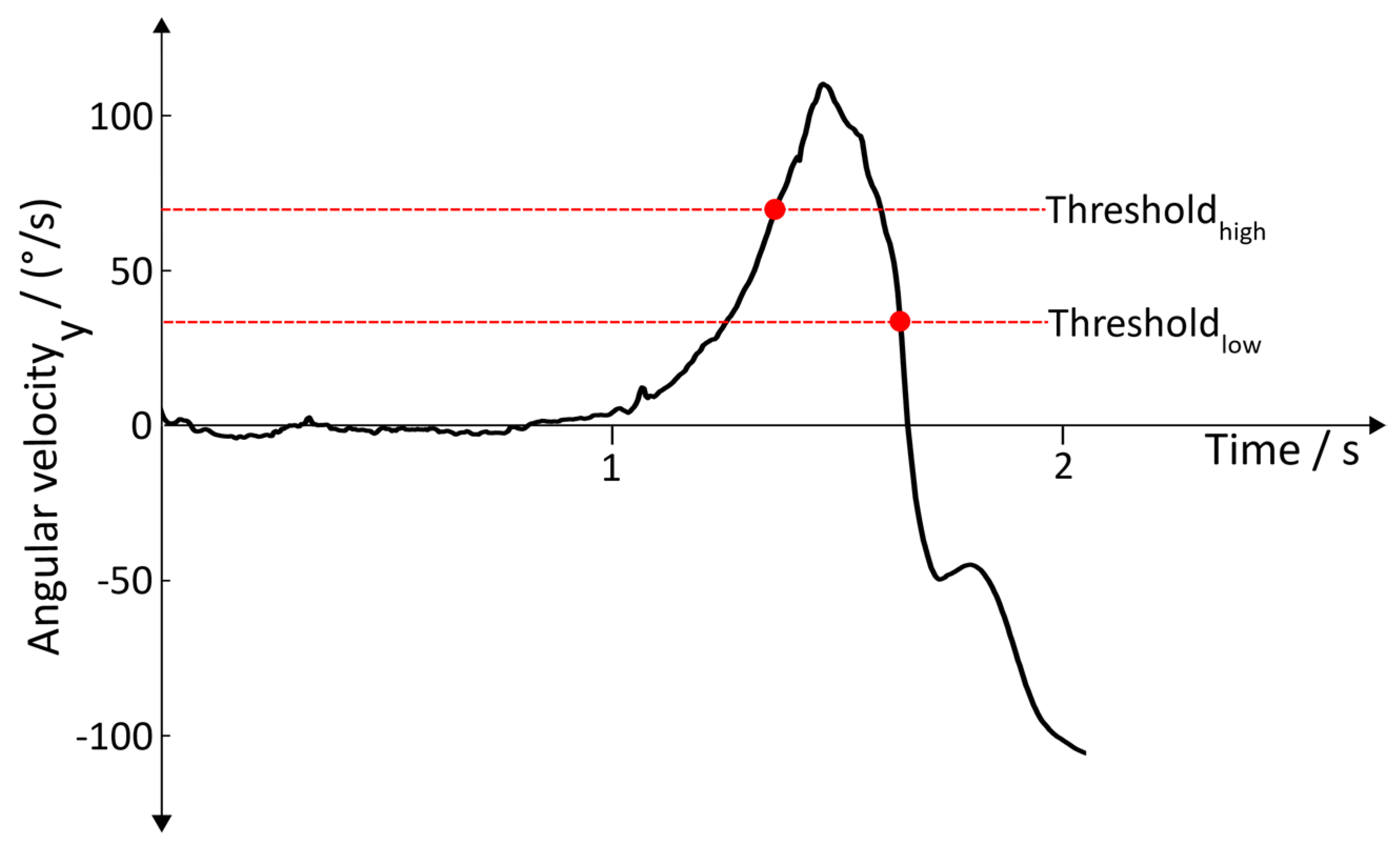
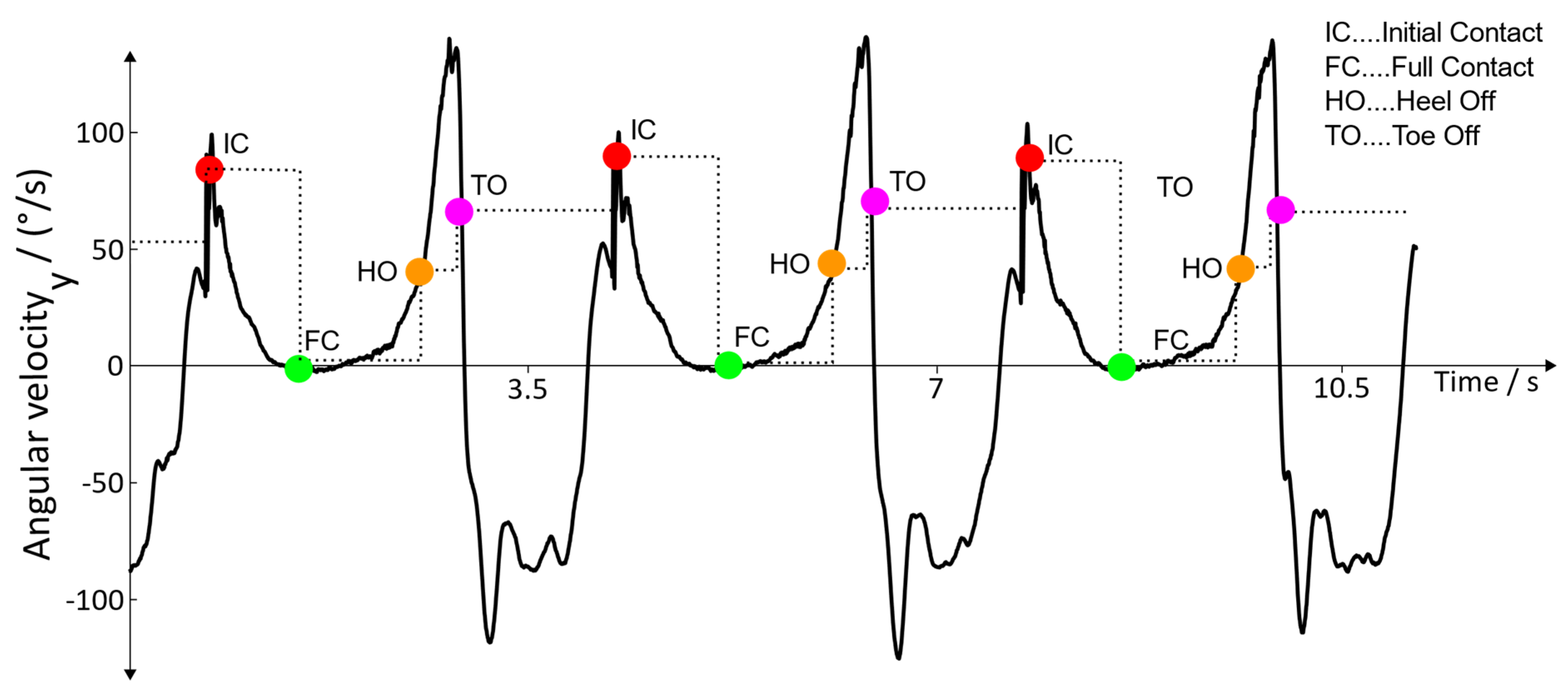
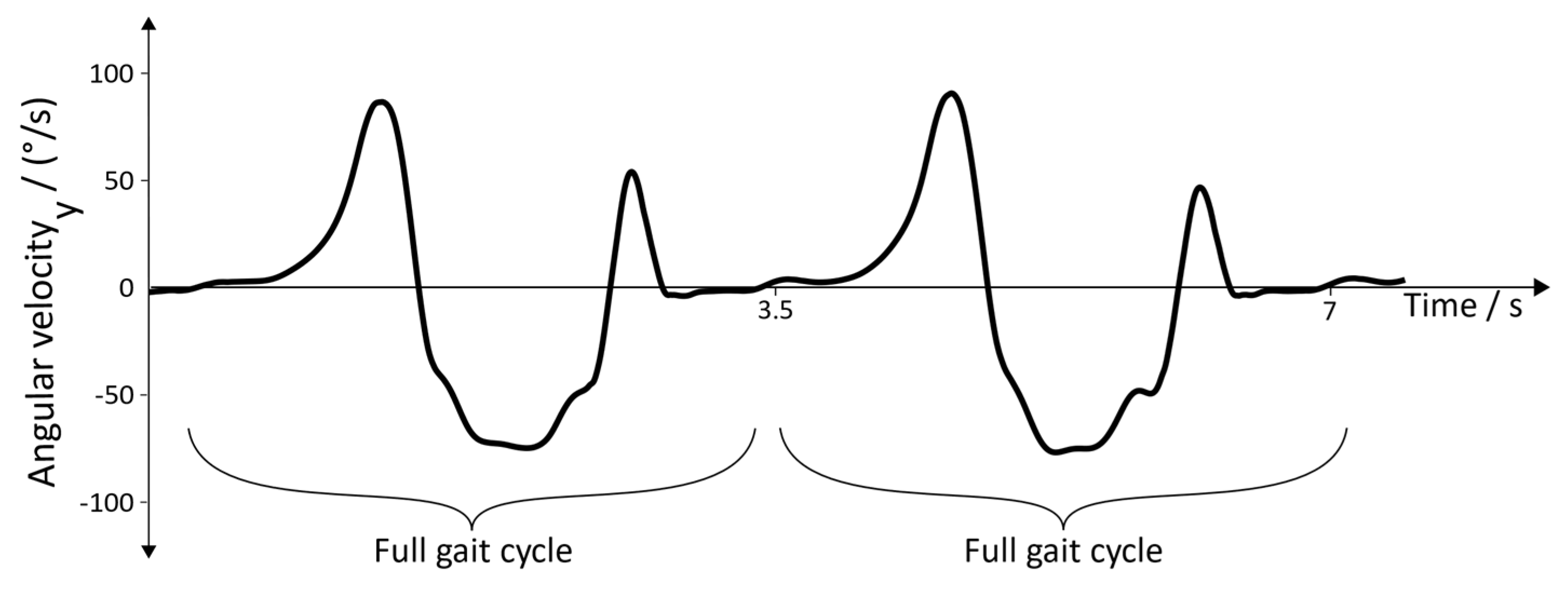
2.4.2. Gait Event Detection
2.4.3. Error Handling
2.4.4. Threshold Adaption
2.4.5. Robot-Assisted Gait Trainer Adaption
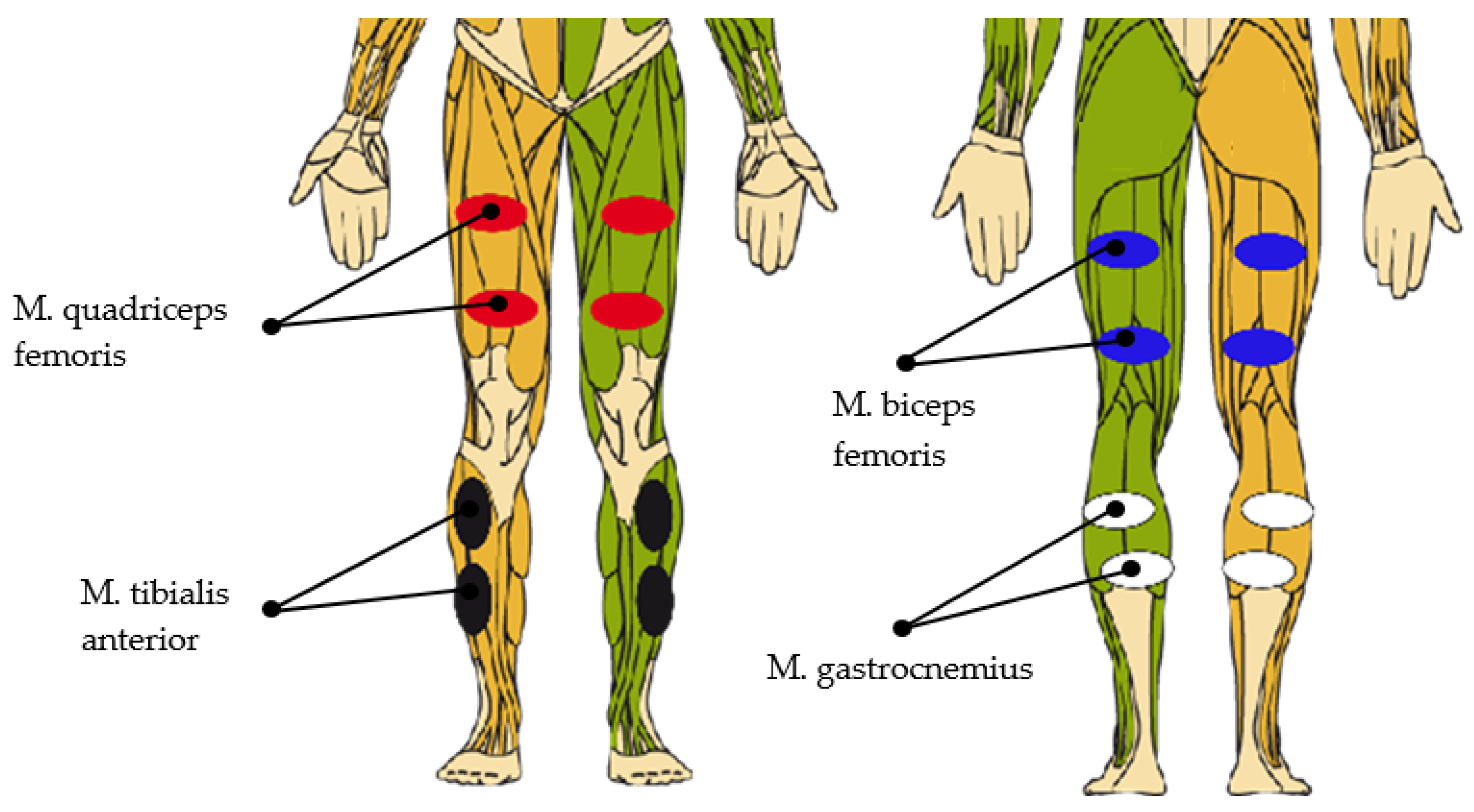
2.5. Functional Electrical Stimulation
3. Results
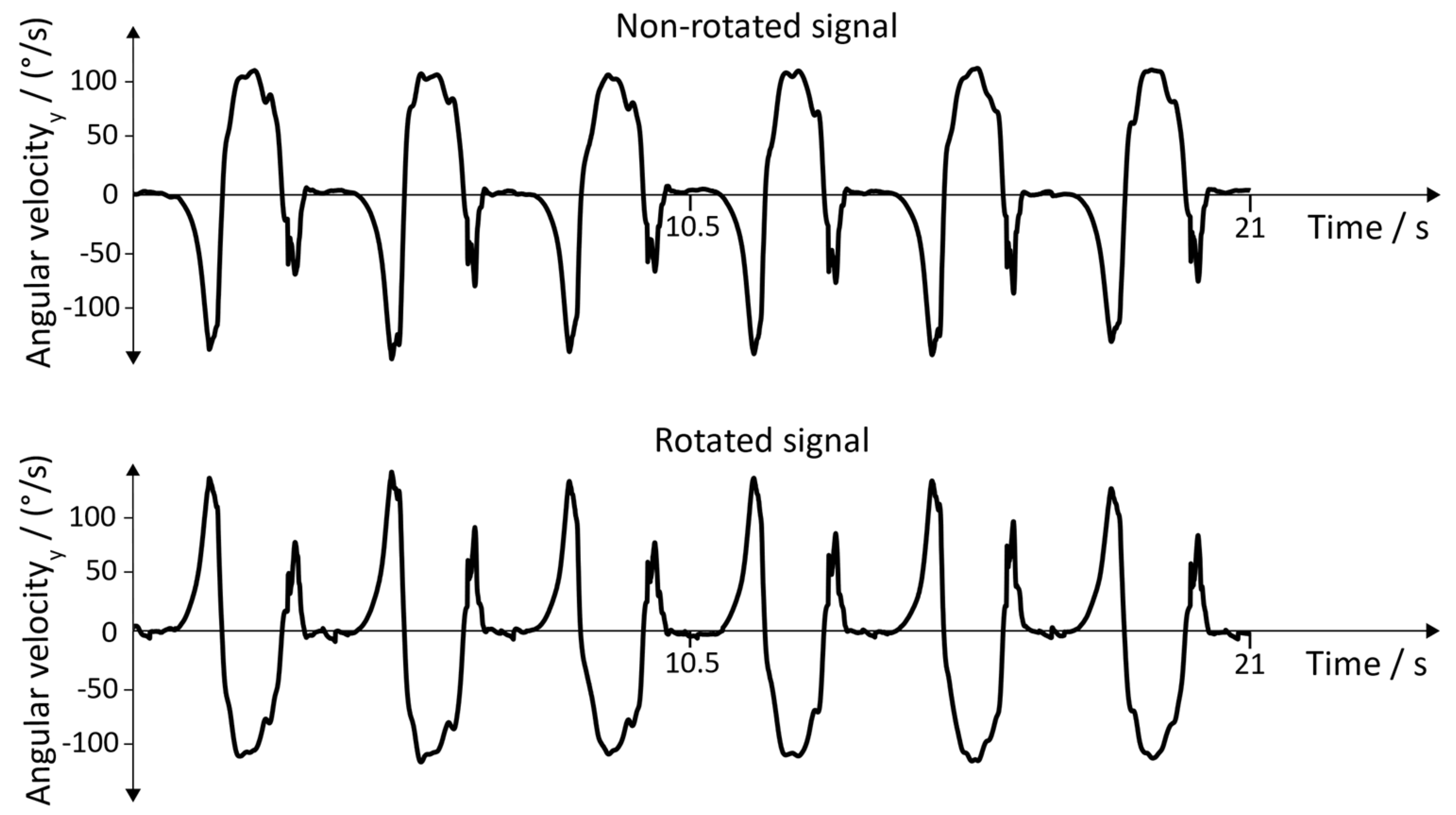
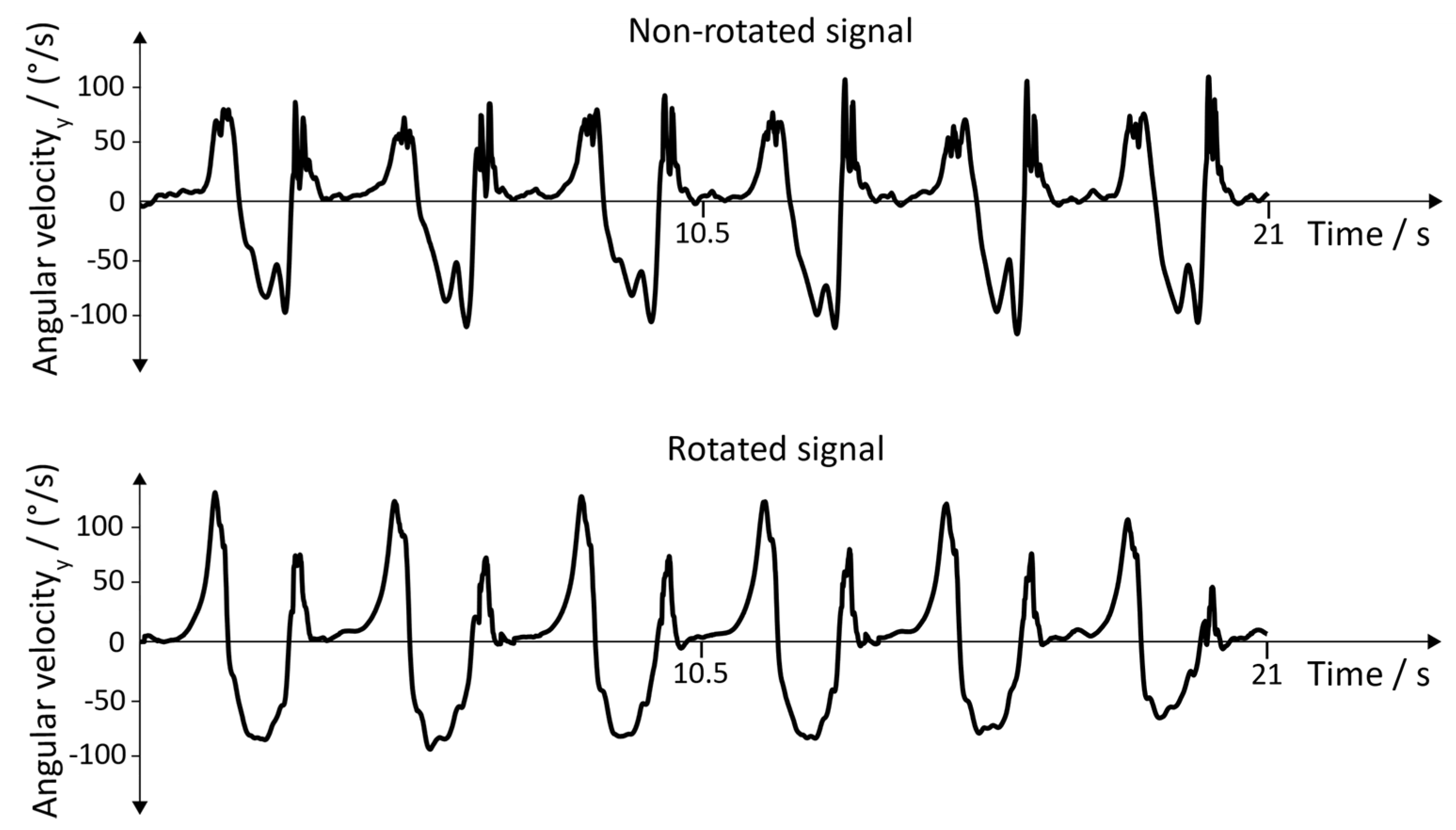
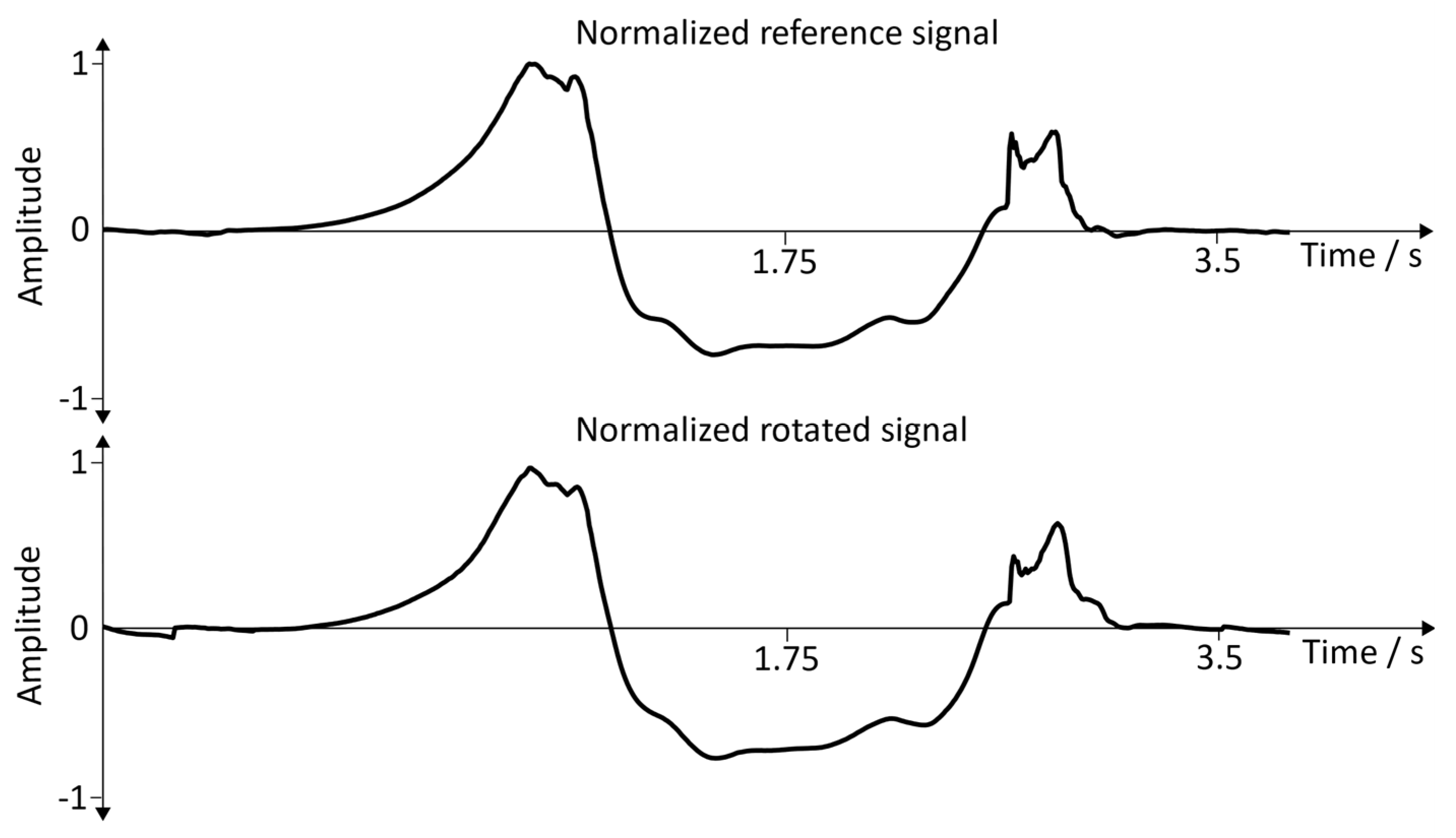
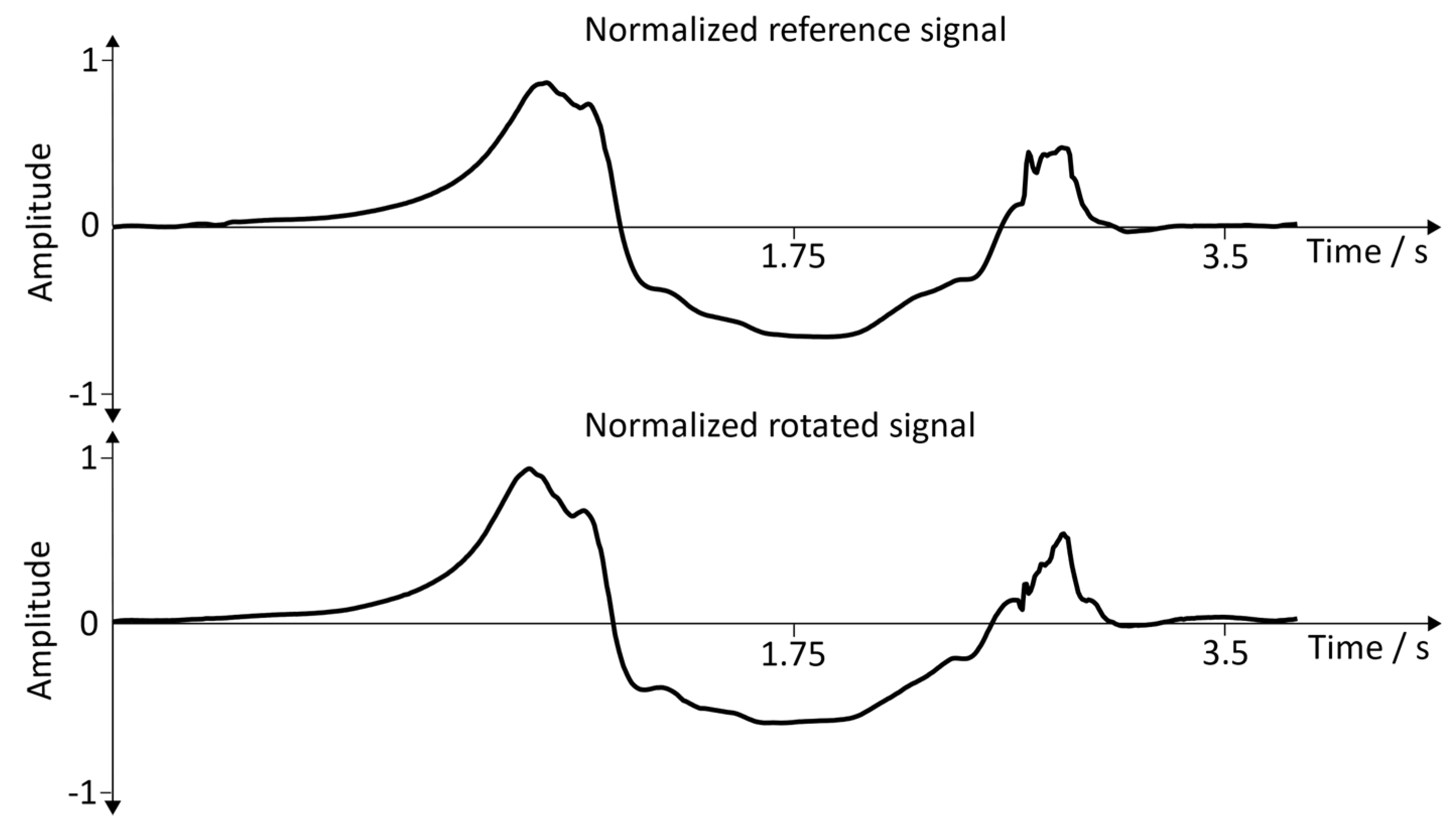
3.1. Arbitrary Sensor Alignment
- Well-defined shape of the angular velocity of the (pitch), as depicted in Figure 11
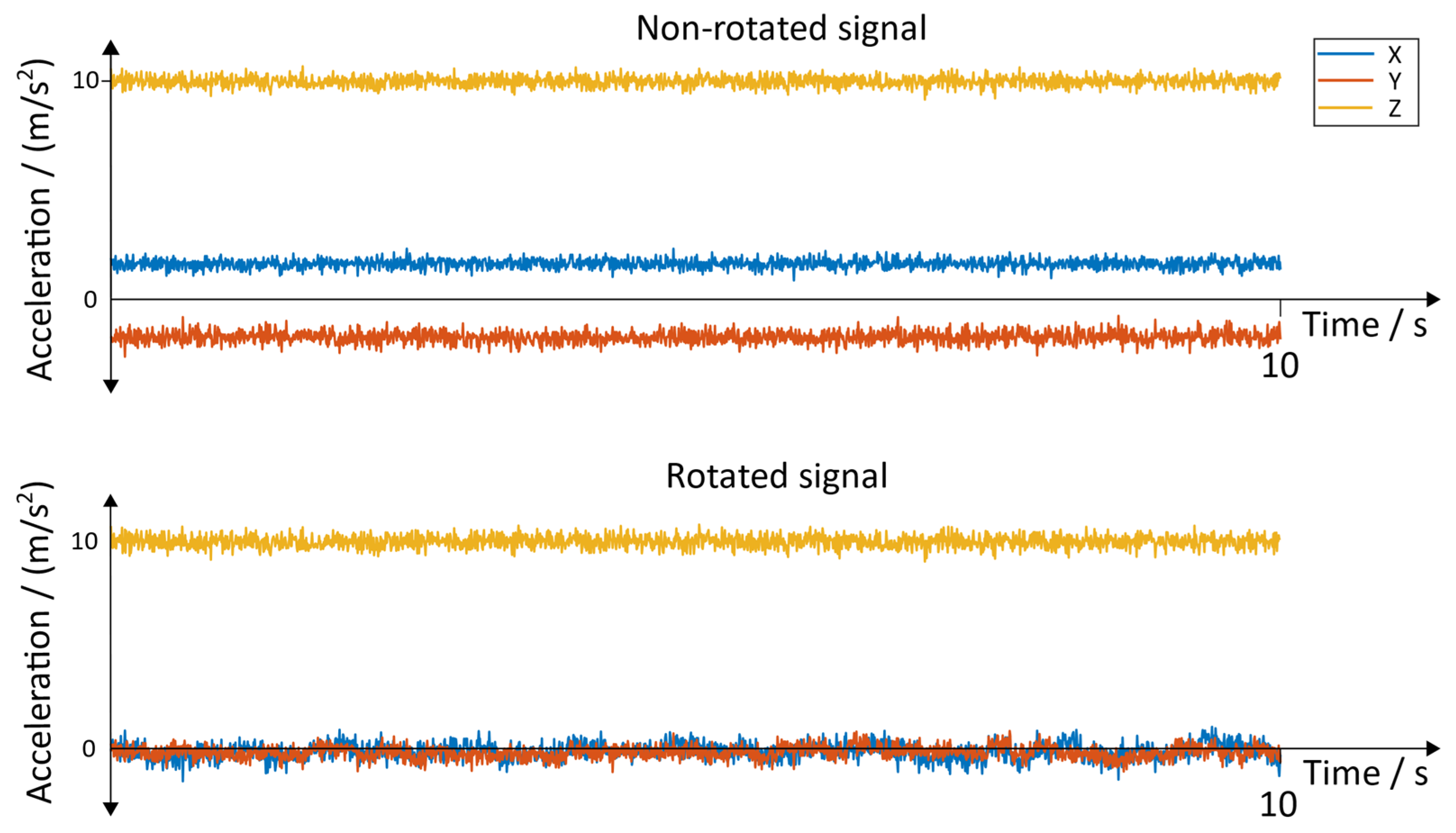
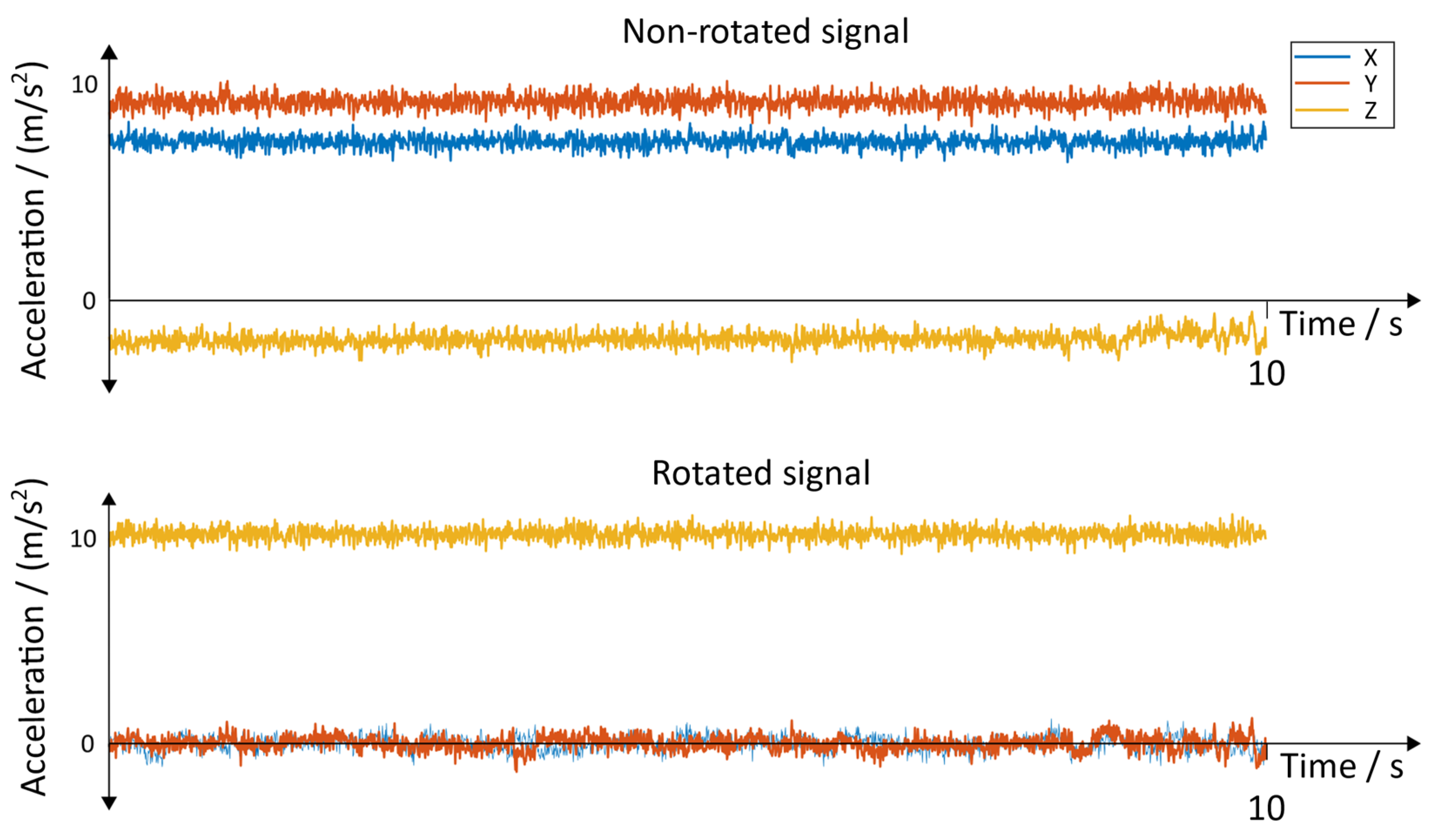
- Acceleration in the at rest must be around ‒9.81 m/s2, which is caused by the gravitational field
- Acceleration in the and at rest must be in a low band around zero
- Removing of the offset by subtracting the mean value of the signal
- Normalization of the amplitude with the following calculation (written as MATLAB code):
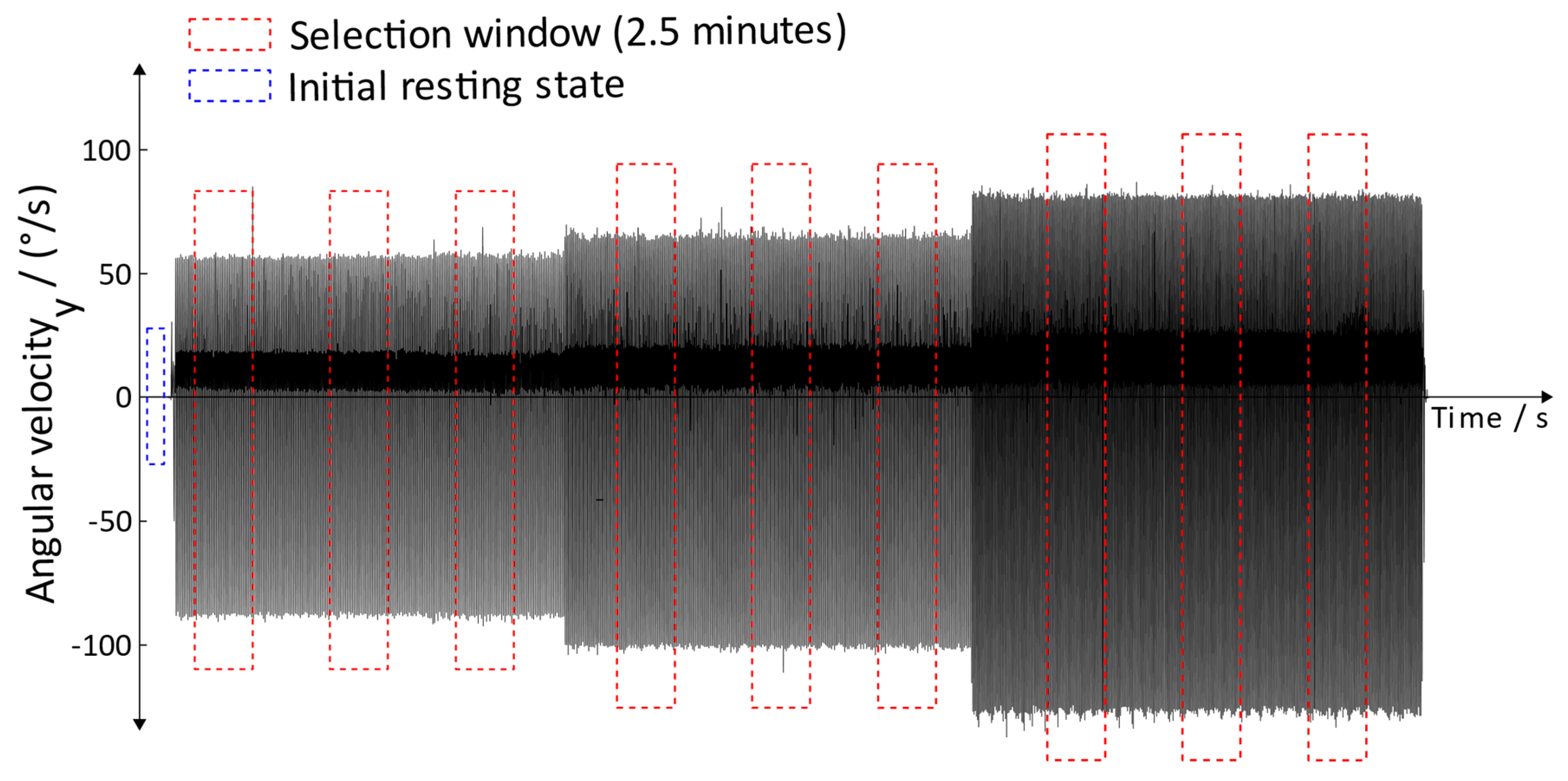
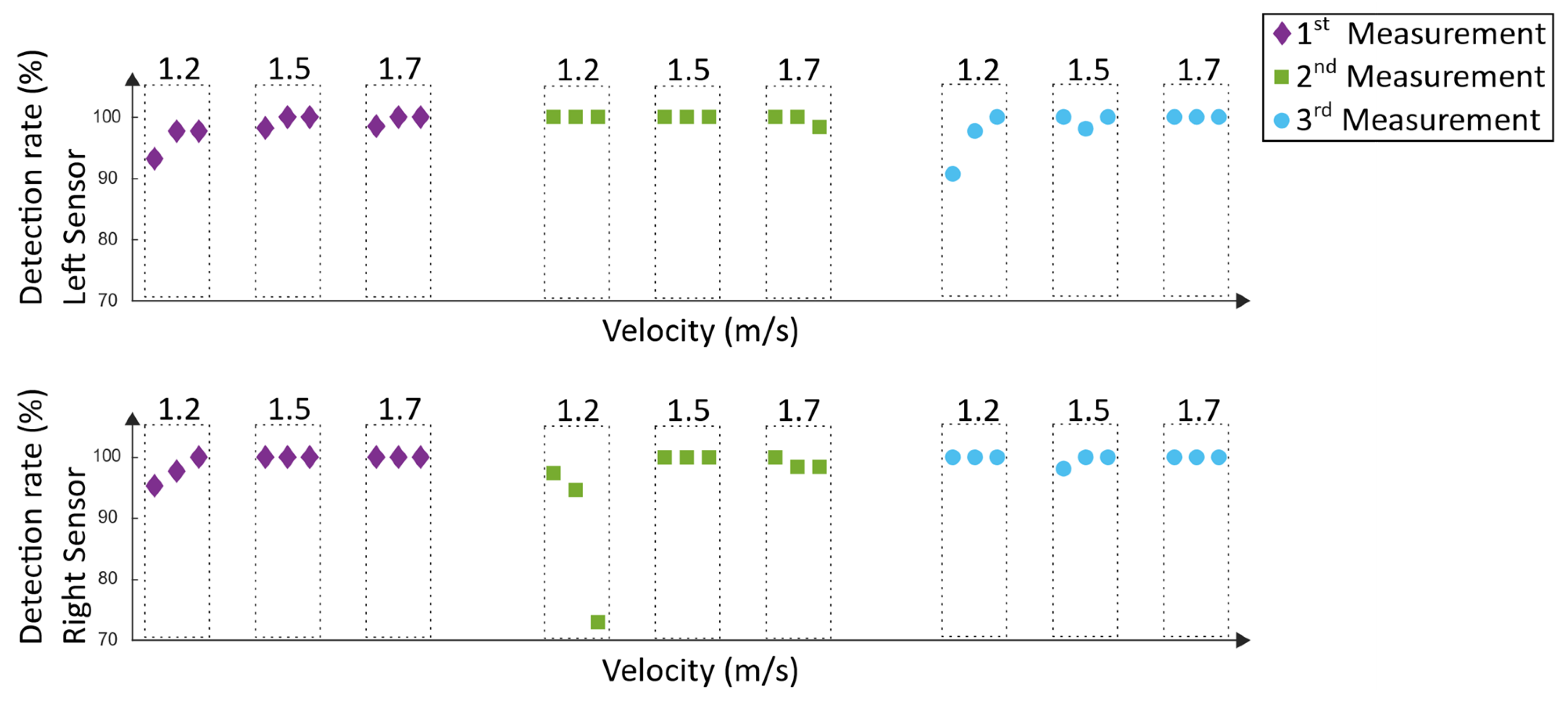
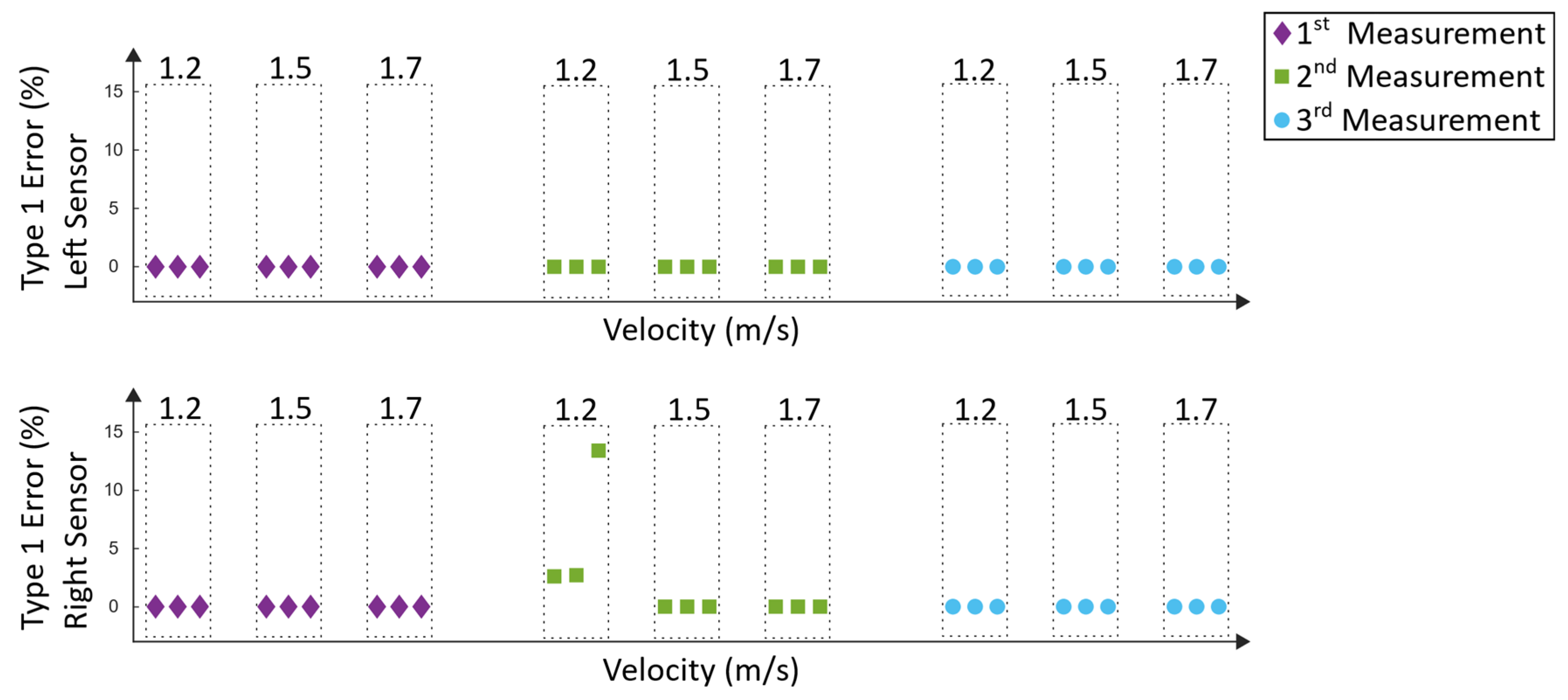
3.2. Lokomat Measurements
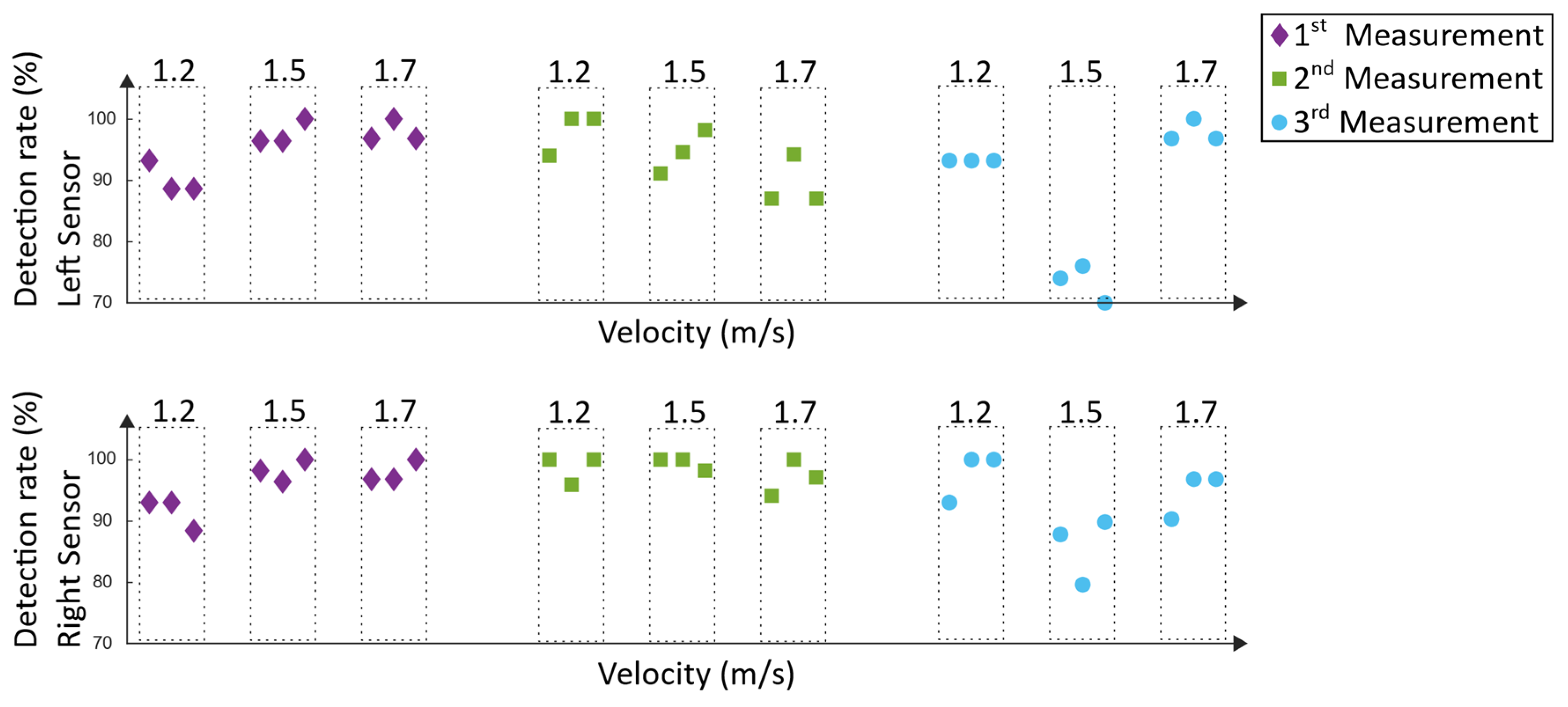
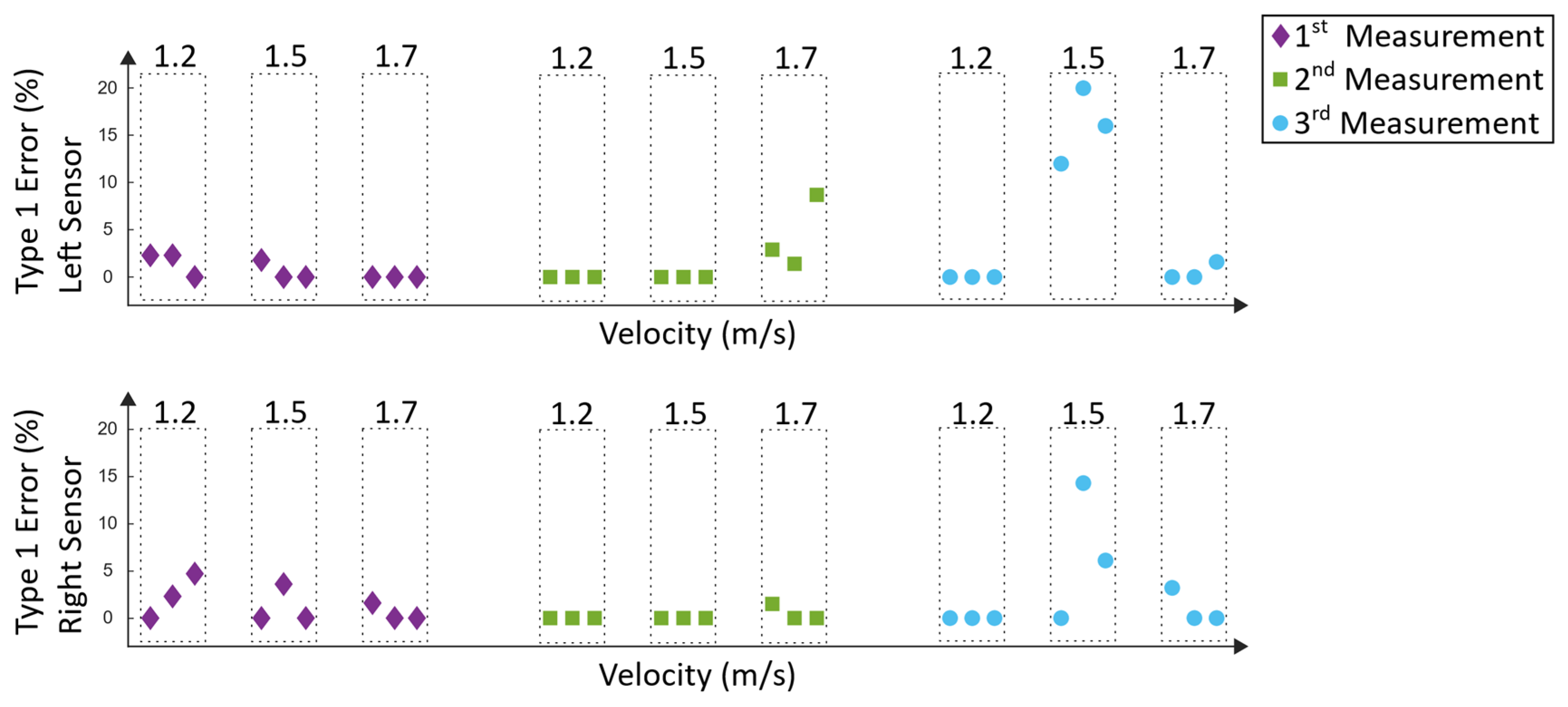
3.3. Lyra Measurements
4. Discussion
4.1. Arbitrary Sensor Alignment
4.2. Lokomat Measurements
4.3. Lyra Measurements
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Iosa, M.; Morone, G.; Fusco, A.; Bragoni, M.; Coiro, P.; Multari, M.; Venturiero, V.; de Angelis, D.; Pratesi, L.; Paolucci, S. Seven Capital Devices for the Future of Stroke Rehabilitation. Stroke Res. Treat. 2012, 2012, 187965. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Thomas, S.; Werner, C.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2017, 5. [Google Scholar] [CrossRef]
- Hidler, J.M.; Wall, A.E. Alterations in muscle activation patterns during robotic-assisted walking. Clin. Biomech. (BristolAvon) 2005, 20, 184–193. [Google Scholar] [CrossRef]
- Hesse, S. Lokomotionstherapie: Ein Praxisorientierter Überblick; Hippocampus: Bad Honnef, Germany, 2007. [Google Scholar]
- Functional Electrical Stimulation (FES) for Stroke Rehabilitation; Tong, R.K.-Y. (Ed.) John WIley & Sons Inc.: Hoboken, NJ, USA, 2006. [Google Scholar]
- Springer, S.; Khamis, S. Effects of functional electrical stimulation on gait in people with multiple sclerosis—A systematic review. Mult. Scler. Relat. Disord. 2017, 13, 4–12. [Google Scholar] [CrossRef]
- Sharif, F.; Ghulam, S.; Malik, A.N.; Saeed, Q. Effectiveness of Functional Electrical Stimulation (FES) versus Conventional Electrical Stimulation in Gait Rehabilitation of Patients with Stroke. J. Coll. Physicians Surg. Pak. JCPSP 2017, 27, 703–706. [Google Scholar]
- Martin, R.; Sadowsky, C.; Obst, K.; Meyer, B.; McDonald, J. Functional electrical stimulation in spinal cord injury: From theory to practice. Top. Spinal Cord Inj. Rehabil. 2012, 18, 28–33. [Google Scholar] [CrossRef]
- del-Ama, A.J.; Gil-Agudo, A.; Pons, J.L.; Moreno, J.C. Hybrid FES-robot cooperative control of ambulatory gait rehabilitation exoskeleton. J. Neuroeng. Rehabil. 2014, 11, 27. [Google Scholar] [CrossRef]
- Bruni, M.F.; Melegari, C.; De Cola, M.C.; Bramanti, A.; Bramanti, P.; Calabrò, R.S. What does best evidence tell us about robotic gait rehabilitation in stroke patients: A systematic review and meta-analysis. J. Clin. Neurosci. 2018, 48, 11–17. [Google Scholar] [CrossRef]
- Dohring, M.E.; Daly, J.J. Automatic synchronization of functional electrical stimulation and robotic assisted treadmill training. IEEE Trans. Neural Syst. Rehabil. Eng. 2008, 16, 310–313. [Google Scholar] [CrossRef]
- McCabe, J.P. Feasibility of combining gait robot and multichannel functional electrical stimulation with intramuscular electrodes. JRRD 2008, 45, 997–1006. [Google Scholar] [CrossRef]
- Laursen, C.B.; Nielsen, J.F.; Andersen, O.K.; Spaich, E.G. Feasibility of Using Lokomat Combined with Functional Electrical Stimulation for the Rehabilitation of Foot Drop. Eur. J. Transl. Myol. 2016, 26, 6221. [Google Scholar] [CrossRef]
- Schwesig, R.; Kauert, R.; Wust, S.; Becker, S.; Leuchte, S. Reliability of the novel gait analysis system RehaWatch. Biomed. Tech. Biomed. Eng. 2010, 55, 109–115. (In Germany) [Google Scholar] [CrossRef] [PubMed]
- Donath, L.; Faude, O.; Lichtenstein, E.; Nüesch, C.; Mündermann, A. Validity and reliability of a portable gait analysis system for measuring spatiotemporal gait characteristics: Comparison to an instrumented treadmill. J. Neuroeng. Rehabil. 2016, 13, 6. [Google Scholar] [CrossRef]
- Mariani, B.; Hoskovec, C.; Rochat, S.; Büla, C.; Penders, J.; Aminian, K. 3D gait assessment in young and elderly subjects using foot-worn inertial sensors. J. Biomech. 2010, 43, 2999–3006. [Google Scholar] [CrossRef] [PubMed]
- Mariani, B.; Rouhani, H.; Crevoisier, X.; Aminian, K. Quantitative estimation of foot-flat and stance phase of gait using foot-worn inertial sensors. Gait Posture 2013, 37, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Dundar, U.; Toktas, H.; Solak, O.; Ulasli, A.M.; Eroglu, S. A comparative study of conventional physiotherapy versus robotic training combined with physiotherapy in patients with stroke. Top. Stroke Rehabil. 2014, 21, 453–461. [Google Scholar] [CrossRef]
- Banz, R.; Riener, R.; Lünenburger, L.; Bolliger, M. Assessment of walking performance in robot-assisted gait training: A novel approach based on empirical data. In Proceedings of the 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 1977–1980. [Google Scholar]
- Anaya, F.; Thangavel, P.; Yu, H. Hybrid FES–robotic gait rehabilitation technologies: A review on mechanical design, actuation, and control strategies. Int. J. Intell. Robot Appl. 2018, 2, 1–28. [Google Scholar] [CrossRef]
- Cheng, P.Y.; Lai, P.Y. Comparison of Exoskeleton Robots and End-Effector Robots on Training Methods and Gait Biomechanics. In Lecture Notes in Computer Science, Intelligent Robotics and Applications; Springer: Berlin/Heidelberg, Germany, 2013; pp. 258–266. [Google Scholar]
- De Sousa, A.C.C.; Valtin, M.; Bó, A.P.L.; Schauer, T. Automatic Detection of Stimulation Artifacts to Isolate Volitional from Evoked EMG Activity. IFAC Pap. 2018, 51, 282–287. [Google Scholar] [CrossRef]
- Neumann, D.A.; Rowan, E.E. Kinesiology of the Musculoskeletal System: Foundations for Physical Rehabilitation; Mosby: St. Louis, MO, USA, 2008. [Google Scholar]
- Seel, T.; Landgraf, L.; de Escobar, V.C.; Schauer, T. Online Gait Phase Detection with Automatic Adaption to Gait Velocity Changes Using Accelerometers and Gyroscopes. Biomed. Technik. Biomed. Eng. 2014, 59 (Suppl. 1), s758–s909. [Google Scholar]
- Perry, J. Gait Analysis: Normal and Pathological Function; Slack: Thorofare, NJ, USA, 1992. [Google Scholar]
- Teufl, W.; Lorenz, M.; Miezal, M.; Taetz, B.; Fröhlich, M.; Bleser, G. Towards Inertial Sensor Based Mobile Gait Analysis: Event-Detection and Spatio-Temporal Parameters. Sensors 2019, 19, 38. [Google Scholar] [CrossRef]
- Müller, P.; Seel, T.; Schauer, T. Experimental Evaluation of a Novel Inertial Sensor Based Realtime Gait Phase Detection Algorithm. In Proceedings of the 6th European Conference on Technically Assisted Rehabilitation—TAR, Berlin, Germany, 12–13 March 2015. [Google Scholar]
- Backus, D.; Tefertiller, C. Incorporating Manual and Robotic Locomotor Training into Clinical Practice: Suggestions for Clinical Decision Making. Top. Spinal Cord Inj. Rehabil. 2008, 14, 23–38. [Google Scholar] [CrossRef]


























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Muscle | Start (% of Gait Cycle) | Stop (% of Gait Cycle) |
|---|---|---|
| M. quadriceps femoris (left) | 90 | 16 |
| M. quadriceps femoris (right) | 40 | 66 |
| M. biceps femoris (left) | 80 | 12 |
| M. biceps femoris (right) | 30 | 62 |
| M. tibialis anterior (left) | 56 | 12 |
| M. tibialis anterior (right) | 6 | 62 |
| M. gastrocnemius (left) | 10 | 50 |
| M. gastrocnemius (right) | 60 | 100 |
| Number of Gait Cycles | Sensor Position | Mean | Standard Deviation |
|---|---|---|---|
| 20 | Inside the foot | 0.988 | 0.012 |
| 20 | Dorsum of the foot | 0.990 | 0.006 |
| Number of Resting Phases | Sensor Position | Axis | Mean (m/s2) | Standard Deviation (m/s2) |
|---|---|---|---|---|
| 20 | Inside the foot | xaxis | −0.142 | 0.197 |
| 20 | Inside the foot | yaxis | 0.108 | 0.246 |
| 20 | Inside the foot | zaxis | 9.944 | 0.110 |
| 20 | Dorsum of the foot | xaxis | −0.514 | 0.273 |
| 20 | Dorsum of the foot | yaxis | 0.200 | 0.323 |
| 20 | Dorsum of the foot | zaxis | 10.028 | 0.126 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schicketmueller, A.; Rose, G.; Hofmann, M. Feasibility of a Sensor-Based Gait Event Detection Algorithm for Triggering Functional Electrical Stimulation during Robot-Assisted Gait Training. Sensors 2019, 19, 4804. https://doi.org/10.3390/s19214804
Schicketmueller A, Rose G, Hofmann M. Feasibility of a Sensor-Based Gait Event Detection Algorithm for Triggering Functional Electrical Stimulation during Robot-Assisted Gait Training. Sensors. 2019; 19(21):4804. https://doi.org/10.3390/s19214804
Chicago/Turabian StyleSchicketmueller, Andreas, Georg Rose, and Marc Hofmann. 2019. "Feasibility of a Sensor-Based Gait Event Detection Algorithm for Triggering Functional Electrical Stimulation during Robot-Assisted Gait Training" Sensors 19, no. 21: 4804. https://doi.org/10.3390/s19214804
APA StyleSchicketmueller, A., Rose, G., & Hofmann, M. (2019). Feasibility of a Sensor-Based Gait Event Detection Algorithm for Triggering Functional Electrical Stimulation during Robot-Assisted Gait Training. Sensors, 19(21), 4804. https://doi.org/10.3390/s19214804