IoT/Sensor-Based Infrastructures Promoting a Sense of Home, Independent Living, Comfort and Wellness

 ,
,  ,
,
Abstract
:1. Introduction
1.1. Introduction to Study Problem
1.2. Conceptualizing the Study Problem and Underpinning Theory
1.3. Paper Overview
2. Materials and Methods
2.1. Research Objectives
2.2. Overview of Studies
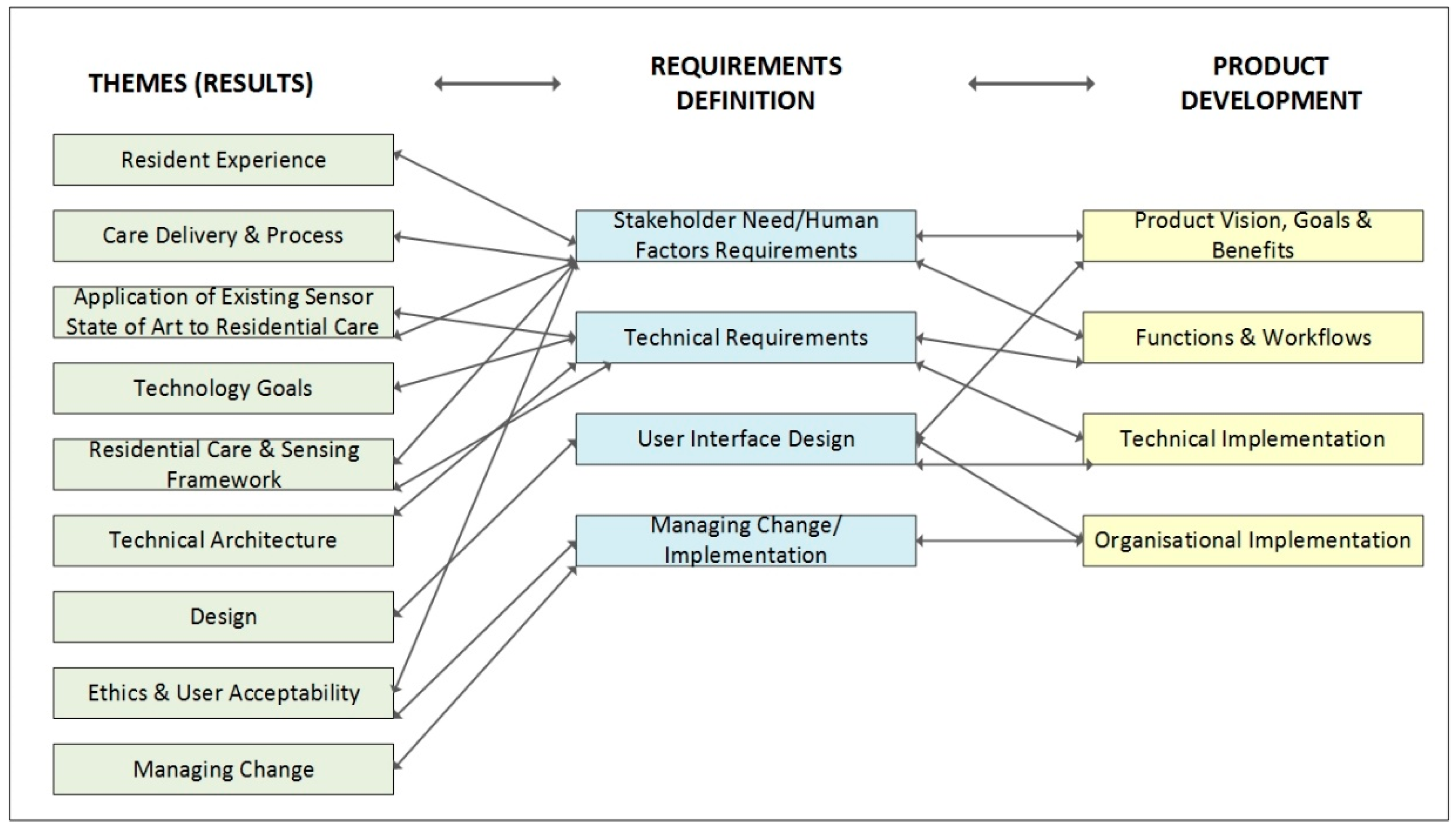
2.3. Stakeholder Evaluation Approach and Innovation
2.4. Study 1a
2.5. Study 1b
2.6. Study 2
- Literature review/market scan in relation to customer needs, technology trends and available technology.
- Evaluation of the current state of the art in relation to sensor kits and IoT architectures.
- Evaluation of prospective customer requirements, including technical and integration requirements (i.e., tender documentation).
- Specification of the preliminary product vision, benefits and end user requirements.
- Analysis of wellness management concepts, resident and caregiver user requirements (outputs of Study 1).
- Definition of stakeholder requirements (outputs of study 1).
- Specification of technical architecture.
- Translating of requirements into user stories (outputs of study 1).
- Prototyping and design, including an analysis of user interface design prototypes for residents and caregivers as emerged in human factors research (outputs of study 1).
- Software development.
- Software testing.
- Product demonstration and evaluation.
2.7. Study 3
3. Results
3.1. Overview of Findings
3.2. Resident Experience
- Other residents are domiciled there.
- Much of the environment is shared with others (for example, corridors, communal/social spaces, eating areas and outdoor areas).
- Care is provided by formal caregivers who ‘work’ at the residential home.
3.3. Wellness Management and Care Delivery
- Change to any one factor/specific pillar will influence the others
- Change to any one factor/specific pillar might be enough to initiate response/call to action
- Individual differences should be considered
- If there a reason for change, then this should impact on the care response (i.e., monitor or take action)
3.4. Residential Care and Sensing Framework
- State of resident (health and wellness).
- State of environment (i.e., resident’s room and other areas and associated implications for state of person and/or activity).
- State of care delivery (i.e., medications taken, Activities of Daily Living (ADL) support, level of care contact, if report due).
3.5. High-Level Technology Goals
3.6. Ethics and User Acceptability
3.7. Application of Existing Sensors ‘State of the Art’
3.8. Design and Wellness Indicator
3.9. Technical Architecture
3.10. Managing Change
4. Emerging Concept
4.1. Overview of Sensing Solution
4.2. Resident Profile and Resident Record
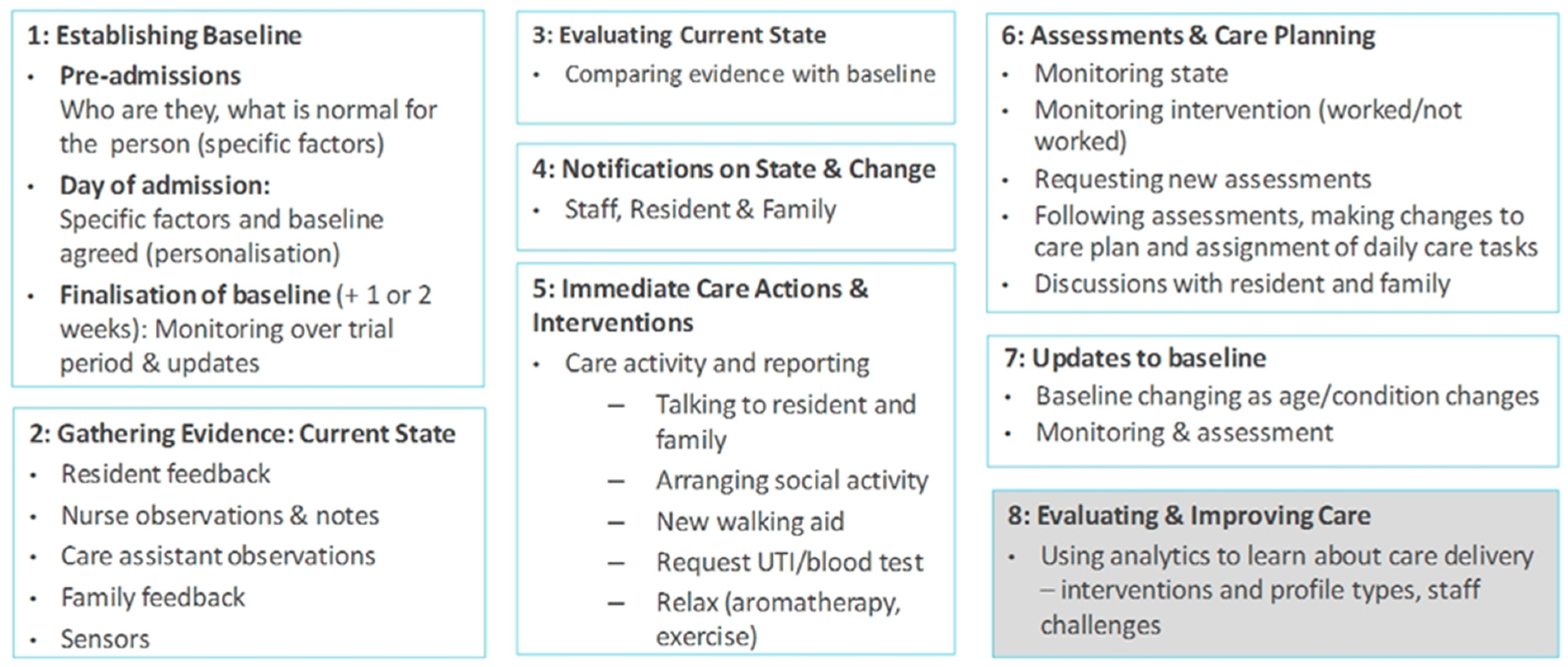
4.3. Process Flow for Monitoring/Managing (1) Resident Wellness, (2) Resident Environment and (3) Care Delivery
- In relation to (1) resident wellness: A wellness report is completed by the resident using the tablet solution (specifically, the resident reports on sleep and mood problems);
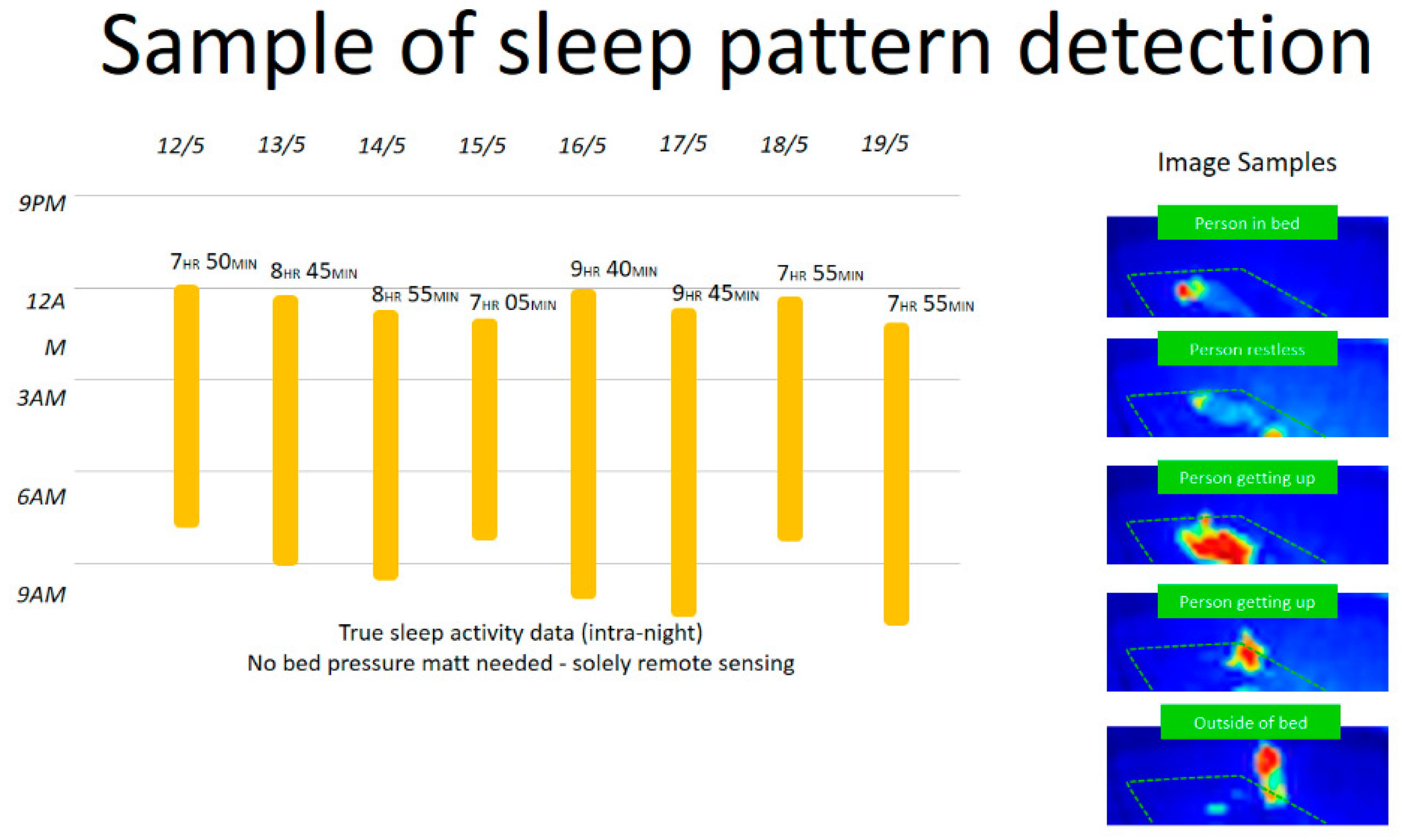
- In relation to (2) resident’s environment: The resident’s bed sensor indicates certain changes to sleep patterns (i.e., out of bed more often and less sleep time);
- In relation to (3) care activity: The caregiver reports on resident rounding using the tablet solution—noting that the resident is fatigued, and that their mood has worsened;
- In relation to (2) resident environment: The room temperature in the room is lowered, and the speakers are set up to play calming music close to the resident’s sleep time;
- In relation to (3) care activity: The nurse prescribes daily physical and social activity to address sleep feedback from the resident, nurses and sensors, and mood feedback from self-reports and nurse observations. The nurse continuously monitors feedback from (1) and (2), to see if the resident’s sleep has improved and if there is an improvement in mood. This involves checking data in the nurse tablet pertaining to sensors and resident reports, along with an in-person conversation with the resident and/or their family. Depending on the outcome, there may need to be further assessments, and potentially a change in health baseline. This would trigger a new care plan, and revisions to daily care tasks and associated reporting of daily care.
4.4. Wellness Indicator
- Predictive risk management—flag wellness problems so they can be addressed early;
- Staff briefing and handover in relation to resident wellness—daily summaries;
- Resident/staff communication and care delivery;
- Resident self-management of health (i.e., awareness of state).
5. Technology Overview
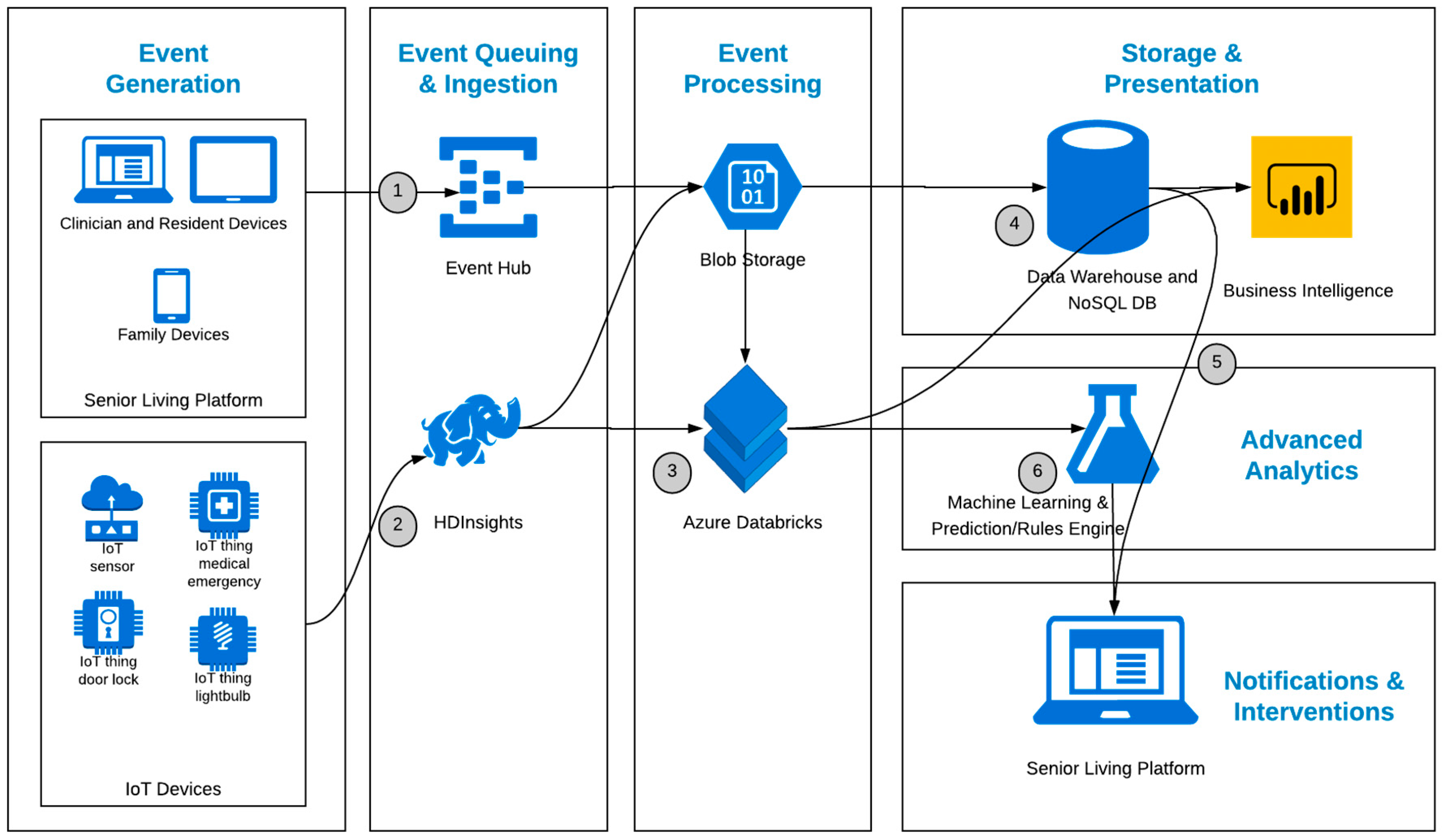
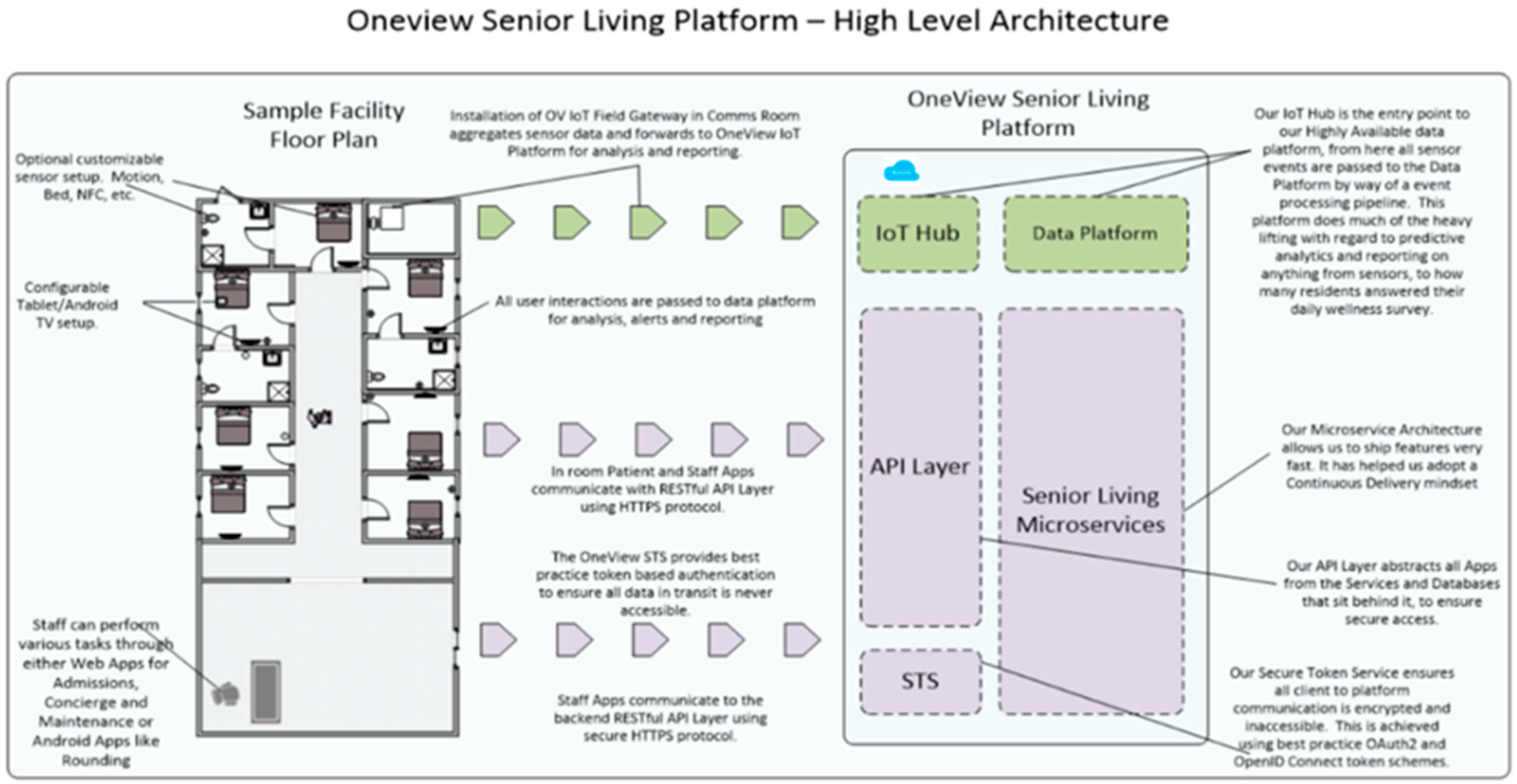
5.1. Overview of the Technical Architecture and Data Platform
- (1)
- The resident and clinician devices access the senior living platform via apps on the tablets and desktop machines, which generate events that are processed by the senior living platform to perform operational functions, but also passed to the data platform event hub for reporting and analytics.
- (2)
- The IoT sensor data is sent either aggregated or raw to the IoT hub and then HDInsights (Hadoop), which is another entry point into the data platform.
- (3)
- The IoT and event data is processed in two key ways:
- Run against rules-based logic to assist with operational decisions in the senior living applications
- Processed and stored in a data warehouse for reporting and heavy computation analytics
- (4)
- The data platform is hosted in Azure, so Azure tools are the default choice when technically feasible and not cost-prohibitive. Azure options for handling the above scenarios include:
- Azure HDInsight for the IoT data processing [80];
- Azure Databricks for combining the IoT data and application event data, cleaning it, and applying machine learning techniques [81];
- Stream analytics for real-time analysis and pattern recognition of IoT and event data [82];
- Logic Apps for rule-based triggers back into the senior living platform [83]
- (5)
- The data from any of these sources can be returned as actionable information to relevant users, in an easy to understand form, allowing for the enhanced provision of care by giving the care user access to this information at the point of care.
- (6)
- Machine learning algorithms deployed in a prediction engine can leverage the historical data in the multiple storage sources to train their models and make decisions against the real-time data flowing in.
- (7)
- These decisions are what drive the “smart” capabilities of the system as outlined in the Sensor Kit and Sensor Profiles section.
5.2. Data Analytics
5.3. Implementation of Internet of Things (IoT) Environments
5.4. Technical Architecture and Data Security
5.5. Technical Architecture and Enterprise-Level Scalability
- Event sourcing;
- Automatic horizontal scalability;
- Couchbase Server Read Model, Couchbase Sync Gateway and Couchbase Lite;
- Cloud availability;
- Network disruption on site.
- Zone redundancy storage (ZRS) ensuring that all data stored on disk in our cloud is distributed across multiple zones in a region.
- For SQL database read models, Azure SQL databases inbuilt functionality is used.
- The Azure load balancer is geo redundant within zone.
- Each node behind the load balancer sits inside a scale-set that ensures nodes are distributed across multiple availability zones.
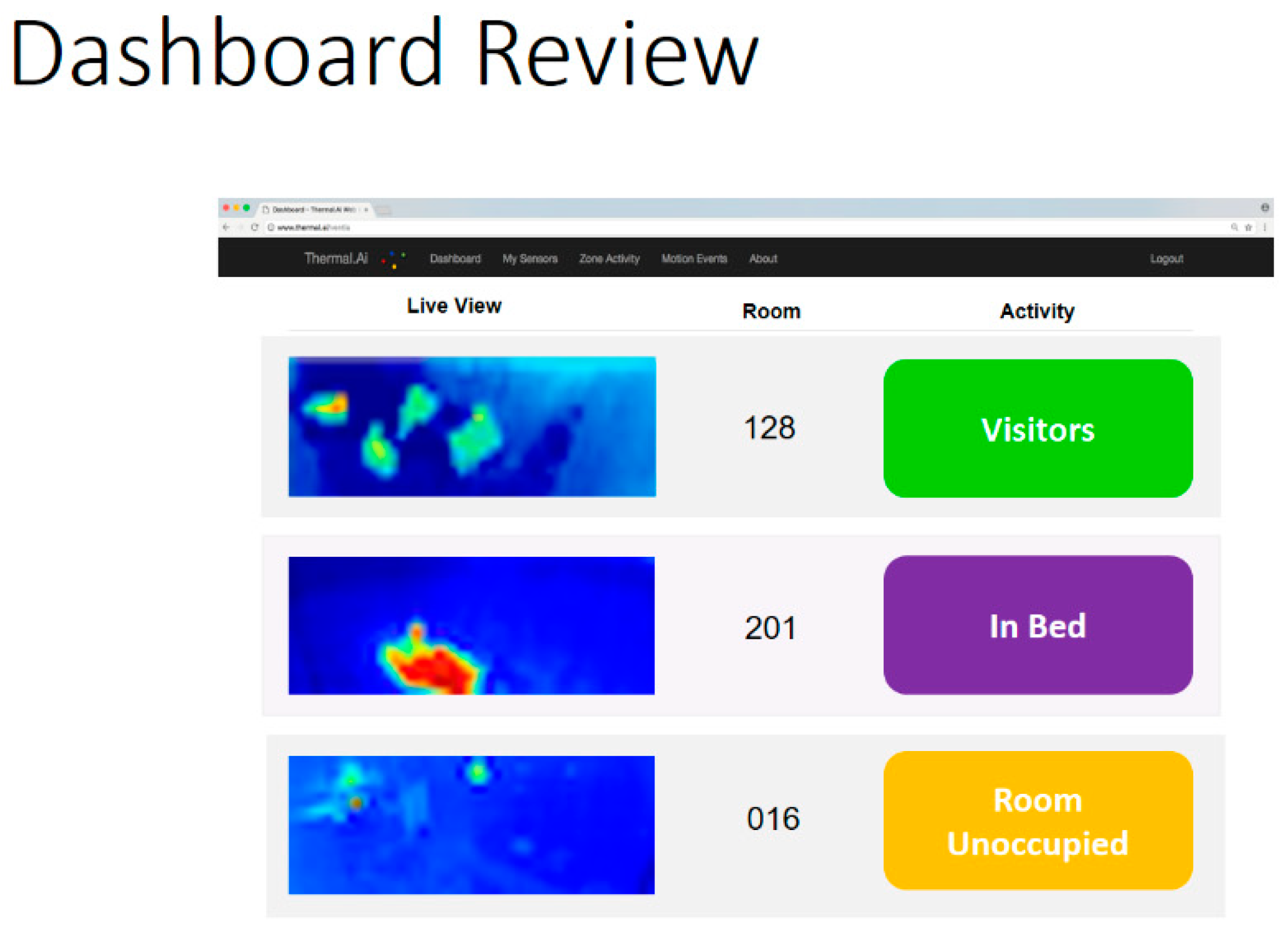
5.6. Sensor Kit and Sensor Profiles
5.7. Customer Implementation and Sensors
- In bed
- Out of bed
- In bathroom
- Falls
- Multiple persons
- Intruder
6. Discussion
6.1. Structuring Device/Frame of Reference—Three Levels
- The state of the resident considering the three wellness pillars, with a key emphasis on social participation (including the resident’s relationship with caregivers, other residents and family members).
- The state of the resident’s living environment (i.e., room and use of space in residential care facility), and how it is experienced by the resident.
- The state of care delivery (i.e., whether the person has received care/assistance in accordance with their care plan and associated assessments).
6.2. Residents and Care Staff
6.3. Care Culture and Ethos
6.4. Wellness Reporting and Care Delivery
6.5. Ageing, Identity and Technology
6.6. Societal Values
6.7. Relationship Centered Care, Technology and Transforming Societal Values
6.8. Research Status and Next Steps
6.9. Study Limits and Areas for Further Thinking
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Overview of Study 1a Research Phases & Activities

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phase | Research Phase/Activity | Stakeholders | No of Participants | Personae | Prototype |
|---|---|---|---|---|---|
| 1 | Literature analysis | N/A | N/A | N/A | N/A |
| 2 | Preliminary Definition of Approach, concept, high level requirements and personae | Internal stakeholders | N = 3 | Personae 1 | N/A |
| 3 | Needs/Requirements Elicitation (interviews and observations with stakeholders) | Internal and External stakeholders | Internal: N = 9 External: N = 38 | N/A | N/A |
| 4 | Needs/Requirements Elicitation (observations) | External Stakeholders | N/A | N/A | N/A |
| 5 | Needs/Requirements Analysis: Elaboration of concept and philosophy and specification of detailed requirements and personae | Internal stakeholders | N = 2 | Personae 2 | N/A |
| 6 | Production of Initial Prototype | Internal stakeholders | N = 2 | N/A | Prototype V 1 |
| 7 | Co-design and Evaluation, Phase 1 | External stakeholders | N = 6 | N/A | Prototype V 1 and V 2 |
| 8 | Co-design and Evaluation, Phase 2 | External stakeholders | N = 5 | N/A | Prototype V 2 and V 3 |
| 9 | Needs/Requirements Elicitation (Residential Home Study) | External stakeholders | N = 5 | Personae 3 | Prototype V 3 and V4 |
| 10 | Co-design and Evaluation, Phase 3 | External stakeholders | N = 5 | N/A | Prototype V 4 and V5 |
| 11 | Co-design and Evaluation, Phase 4 | External stakeholders | N = 5 | N/A | Prototype V 5 and V6 |
| 12 | Co-design and Evaluation, Phase 5 | External stakeholders | N = 5 | N/A | Prototype V 6 and V7 |
| 13 | Final Specification and Design | N/A | N/A | Final Personae | Prototype V 8 |
| Internal stakeholders = members of project team External stakeholders = older persons, nurses, family members, dementia experts, residential home managers/owners and gerontologists | |||||
Appendix B. Overview of Study 1a Methods
| Method | Description |
|---|---|
| Literature Review | The literature view focused on providing a qualitative summary of existing evidence pertaining to successful ageing, wellbeing, care approaches, stakeholder need, technology requirements and ethical issues. Relevant theoretical literature pertaining to successful ageing, wellbeing and care approaches was reviewed. Policy documentation and research studies pertaining to the advancement of assisted living technologies were also examined. Furthermore, an analysis of the existing competitor offering was undertaken. Lastly, the researcher reviewed requirements documentation provided by three prospective customers. |
| Needs/Requirements Elicitation (interviews) | Semi-structured interviews were conducted in person either at the participants home or their workplace. Four separate interview guides were developed to support interviews with (1) older adults, (2) family members, (3) nurses/care staff and, (4) ageing experts and volunteers. Specific interview questions linked to key research questions and relevant themes emanating from the literature review. In each case, the participant was posed questions pertaining to their own experience and needs, and that of other stakeholders. Overall, 47 interviews were conducted with external (N = 38) and internal (N = 9) stakeholders. In terms of interview duration, 25 long interviews (approx. average duration 2 h) and 22 short interviews (approx. average duration 0.5 h) were undertaken. In all cases, the researcher took written notes. There was no audio or video recording. In terms of participant breakdown, external stakeholders included 11 older adults (mean age mean age 79.36 years), 7 family members, 5 experts in ageing/dementia, 1 ICT expert, 4 nurses, 5 representatives spanning two ‘care for the elderly’ day services, 3 representatives from a post-acute care service, and 2 representatives from a residential home. |
| Needs/Requirements Elicitation (observations) | Preliminary observations were undertaken taken at two day hospitals and one residential home. A short walk around was undertaken at one day hospital (approximate time: 0.5 h). The researcher was accompanied by the assistant director of nursing. A detailed walk-around was undertaken at a second day hospital (1 day). Here the researcher was accompanied by the nursing manager, along with other staff (dietician, case manager and pharmacist). The researcher observed several settings—case rooms, occupational therapy room, service user interviews and assessments and service user social activities/interaction in the common room. Furthermore, the researcher received a walk-through of relevant technologies used by different staff, to document case work. A third observation was undertaken at a residential home (approx. time 2 h). Here, the researcher visited indoor and outdoor social spaces, dining rooms, activity rooms and resident rooms accompanied by the residential home owner. In all cases, the researcher collected artefacts from the settings including paper forms and information leaflets. In relation to the second day hospital, the researcher took screenshots of the technologies used by the different roles, and schedule/workload information presented on nurse whiteboards. |
| Needs/Requirements Analysis: Elaboration of concept and philosophy and specification of detailed requirements and personae | Following the interviews/observations, the researcher’s notes were transcribed. Data analysis focused on understanding/defining the lived experience of older adults, care approaches and specific stakeholder technology requirements. A thematic analysis of field research findings was undertaken. The thematic analysis was initially driven by the research question and associated theory (i.e., not inductive). In support of this, a preliminary coding/data frame with high level nodes was defined. An initial review of sample manuscripts across different stakeholders was undertaken. Following this, the coding frame was refined, and sub-nodes were identified (i.e., link to emergent themes). |
| Production of Initial Prototype | Stakeholder personae and scenarios were used to (1) support problem solving around stakeholder requirements and (2) the user interface design of prototypes. Early stage prototypes were developed using the wire framing tool Balsamiq. The primary focus was on the resident solution. Three different prototypes linking to three high level resident contexts were defined: (a) resident is considering moving to residential home, (b) resident is in the admissions process and (c) resident is domicile in residential home. The specification of (c) involved the parallel definition of complementary prototypes for other stakeholders. This includes prototypes for nurses, care assistants and family members. The initial prototype was reviewed by members of the project team (internal stakeholders, N = 2), in advance of the co-design activities. |
| Co-design and Evaluation Phase 1 | The first phase of co-design/evaluation occurred after the analysis of field research and the specification of the initial prototypes (prototypes 1). The evaluation focused on eliciting stakeholder feedback regarding the high-level product concept for the resident application, and a subset of the other stakeholder solutions (for example, nursing staff, families, pre-admissions and admissions). External stakeholders included older adults (N = 4) and nurses (N = 2). In advance of viewing the prototypes, participants reviewed a short Microsoft power-point presentation which provided a background to the research and preliminary findings, a summary of the different applications and functions, and an example persona. The review/co-design of prototypes then commenced. The initial prototypes were demonstrated to stakeholders using a laptop computer. Participants were invited to review prototypes based on (1) their own experience and need, and (2) on the imagined situation of Frank (persona). Feedback pertaining to user need, user expectations, user acceptability and issues related to ethics and privacy was elicited. |
| Co-design and Evaluation Phase 2 | The second phase of co-design involved the same procedure as phase 1. However, the second phase of co-design focused on the resident and nurse applications only. The prototypes demonstrate basic level functionality on the tablet (i.e., touch interaction). The focus here was on (1) eliciting more specific usability feedback (i.e., task workflows, interaction style, nomenclature and iconography) and (2) following up on certain key human factors issues (for example, reduction in human contact). Participants included older adults (N = 3) and nurses (N = 2). |
| Co-design and Evaluation Phase 3 | The third phase of co-design involved the same procedure as phase 1. However, this phase focused on the nurse applications only. Five nurses provided feedback about specific nursing workflows—pertaining to reviewing the overall resident status, assessing care needs for specific residents, reporting on daily care and monitoring wellness interventions. |
| Co-design and Evaluation Phase 4 | The fourth phase of co-design involved the same procedure as phase 1. This phase focused on refining the concepts, processes/workflows and specific user interface (UI) design for both the resident and nursing applications. |
| Co-design and Evaluation Phase 5 | The fifth phase of co-design involved the same procedure as previous phases. However, this phase focused on the nurse applications only. The primary focus was on (a) evaluating those functions which pertain to resident wellness (for example, reporting on resident status and activity, ensuring meaningful interactions with the resident, evaluating resident changes and making a case for new assessments/care plan updates), and (b) exploring how best to manage issues around reduction in human contact/optimizing human contact in care delivery. Five nurses provided feedback pertaining to specific nursing workflows. |
Appendix C. Three Pillars and Factors to be Monitored
| Pillar | Factor | Time-Period | Changes to |
|---|---|---|---|
| Biological | Mobility | 24 h | Level of Mobility |
| Activities of Daily Living (ADL) Support | Week | ADL Support/Dressing ADL Support/Feeding ADL Support/Toileting ADL Support/Hygiene | |
| Night Sleep | 24 h | Not sleeping as normally do • Sleep (Bed Exists) • Sleep time | |
| Fatigue and Day Sleep | 24 h | Sleep routine during the day (being in bed during day or level of sleep during day) | |
| Eating and Drinking | 24 h | What eating How much eating How much drinking Refusing food/drink Issues with swallow | |
| Toileting | 24 h | Changes to elimination/typical patterns (constipated etc.) | |
| Pain | 4 h | Level of pain Comfort being dressed/showered | |
| Pressure Sores | 24 h | Change in pressure sore status? New pressure sore? | |
| Body Temperature | 2 h | ||
| Basic level Physical activity | Several days | Leaving bed/sitting out in chair Leaving room | |
| Physical Exercise | Several days | Taking walks outside Engagement in exercise activities | |
| Wandering | Several days | ||
| Falls | Week | No of falls | |
| Nurse Bell Requests | 24 h | ||
| Psychological | Mood | Several days | Difference in mood |
| Cognitive | Several days | Sad, Anxious, Depressed | |
| General Behavior | Several days | Difference in | |
| Dementia Specific Behavior | Several days | Awareness | |
| Nurse Bell Requests | 24 h | Understanding instructions | |
| Engagement: Hobbies and Interests | Several days | Memory (person, place, time) | |
| Engagement in Education | Several days | Difference in | |
| Engagement in Self-Management Activities | Several days | Level of stress, confusion, agitation | |
| Social | Personality/Level of Social Engagement | Several days | Normally outgoing and talk to people—but change? |
| Time in Room | Several days | Change in typical social patterns—not leaving room, spending more time alone than normal | |
| Club Events and Hobbies | Several days | Not responding to RSVPs Not attending/following normal patterns of attendance for club events | |
| Family Visits | Several days | Not having visits, refusing visits, cancelling visits | |
| Travel Outside | Several days | Not leaving facility—irrespective of whether out hours permissible | |
| Engagement: Communication with Staff | Several days | Changes in communication level Changes in communication style |
Appendix D. Examples of Wellness Communications
| Resident Behavior/Activity | Resident to Care Assistant | Nurse to Resident | Resident to Daughter |
| Resident Fidgeting Resident spitting out food Resident Wandering Resident ringing call bell 7 times in 3 h | I’m not feeling well? When is Jane (daughter) coming to visit? What can I do today? Can I leave? I want to leave! | Hi, how are you feeling today? How is the pain? How did you sleep? Are you not hungry? Stroking resident’s arm and eliciting response | Is it you Jane (daughter)? The pain in my side is getting worse I can’t eat this dinner Where am I? Can I leave? I want to leave! |
| Resident’s Daughter to Nurse | Between Staff Nurses and Care Assistants | Residents Nurse to Daughter | Room/Environment |
| Mum seems in more pain It’s hard to tell whether mum is doing any better—what do you think? Mum seems off/not herself/not doing activities—could there be something wrong? Is mum falling more these days? Mums seems to be angry and doesn’t want to talk—what should I do? | How is Zena—any improvements? I’m having problems with room 10 Can you ask the Dr to have a look at Zena when he arrives? I need two people for room 10! Have we checked Zena for a Urinary Tract Infection (UTI)? I think we need to look at Zena’s care plan again. | Zena fell yesterday—her mobility is getting worse We think Zena might have a UTI and are doing some tests? We need to change Zena’s care plan Zena’s needs more care/help | Room/doors open |
Appendix E. Overview of Solutions for Different Stakeholders
| # | Process | Actor | Application and Device | Description |
|---|---|---|---|---|
| 1 | Preadmissions | Sales Representative | Pre-admission app (website) | Resident and/or loved one provides background information about the resident—social and personal profile, health status, prior assessments and ability. |
| 2 | Admissions | Admissions Co-coordinator | Admissions App (Desktop Computer and Tablet) | The admissions application is used to complete the resident profile picture, at the time of admissions. Prior information provided at the preadmissions stage is prepopulated in the system. The admissions user interface is conceptualized in terms of a series of steps to promote familiarization for both residents and care staff, and reassurance for residents and family members. |
| 3 | Assessments and Care Planning | Nurse | Assessments App (Desktop Computer) | This records resident assessments information—comprising general wellness, nutrition, activities of daily living and functional ability, cognitive, behavioural etc |
| 4 | Daily Care | Resident | Resident App (Tablet) | The resident solution is customized in relation to resident need and ability. The resident can select from a series of functions—based on need/interest. Residents with mid to late stage Dementia—are not expected to interact directly with tablet system (require assistance). |
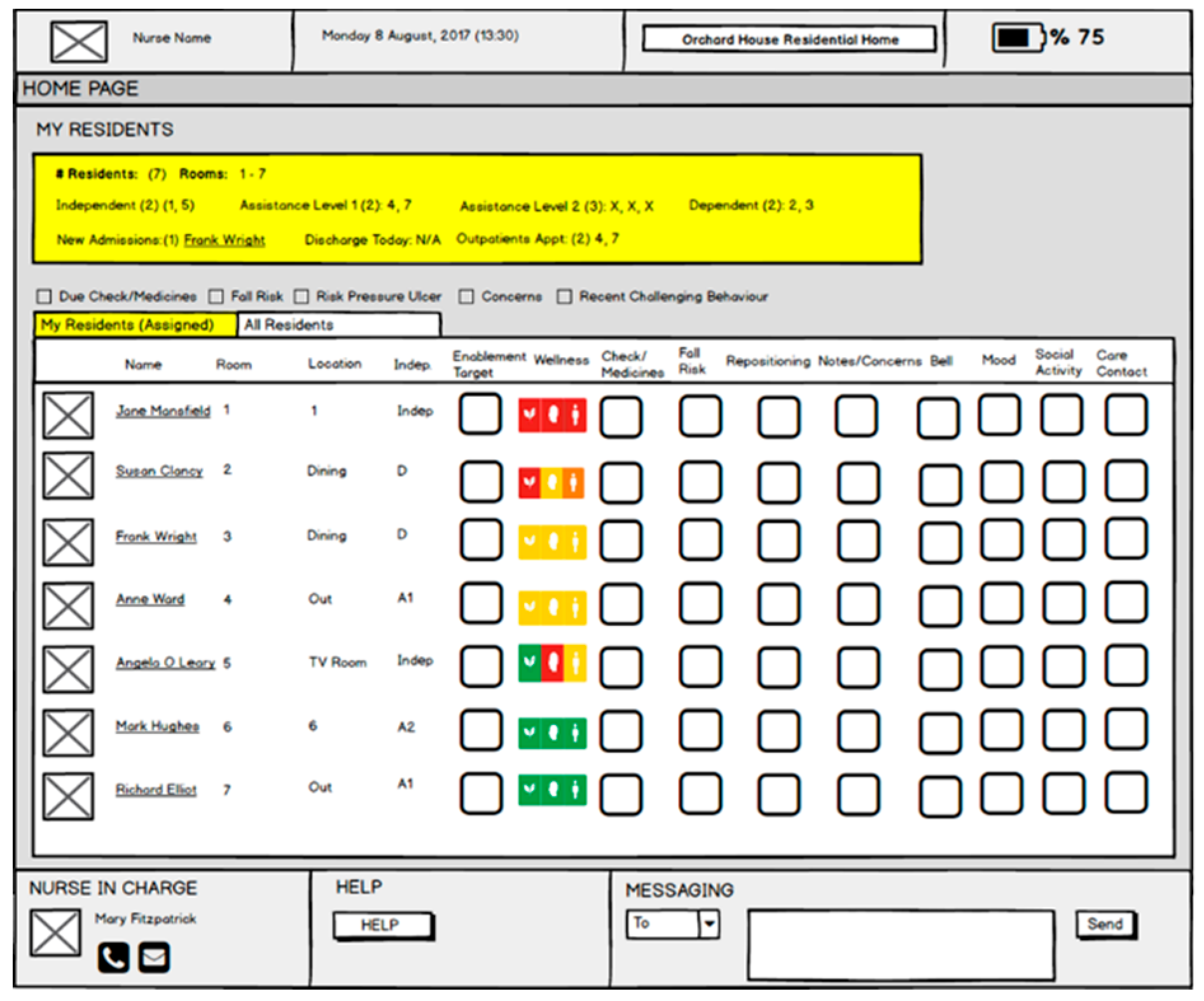
| Nurse | Nurse Rounding App (Tablet) | The nursing solution promotes meaningful interaction with the resident, based on a real time picture of the resident’s state, and background information about who the resident is and what matters to them. This application is also used to record rounding information—structured from biopsychosocial perspective. | ||
| Care Assistant | Caregiver App (Tablet) | This care assistant application enables reporting on ADL and caregiving tasks—it also provides access to information about the resident—personal history, what matters. | ||
| Nurse Manager | Care Console (Desktop Computer) | Supports queries/data analytics in relation to resident wellness, assessments, activity and so forth. Also provides real-time information about the resident. | ||
| Family | Family App (phone, web) | This allows the family member to view relevant real time and historical information about their loved one. Used also to upload content/information etc. | ||
| 5 | Maintenance | Maintenance | Maintenance Managements (Desktop and Tablet) | This application is used to process and manage maintenance requests from residents and staff. |
| 6 | Resident Activities and Entertainment | Entertainment Coordinator | Event Managements (Desktop) | Manage resident social activities and events. |
| 7 | Concierge | Concierge Manager | Concierge (Desktop) | Manage resident requests (i.e., travel, room maintenance etc). |
Appendix F. Study 3, Customer 1—Sensor Technology Implementation
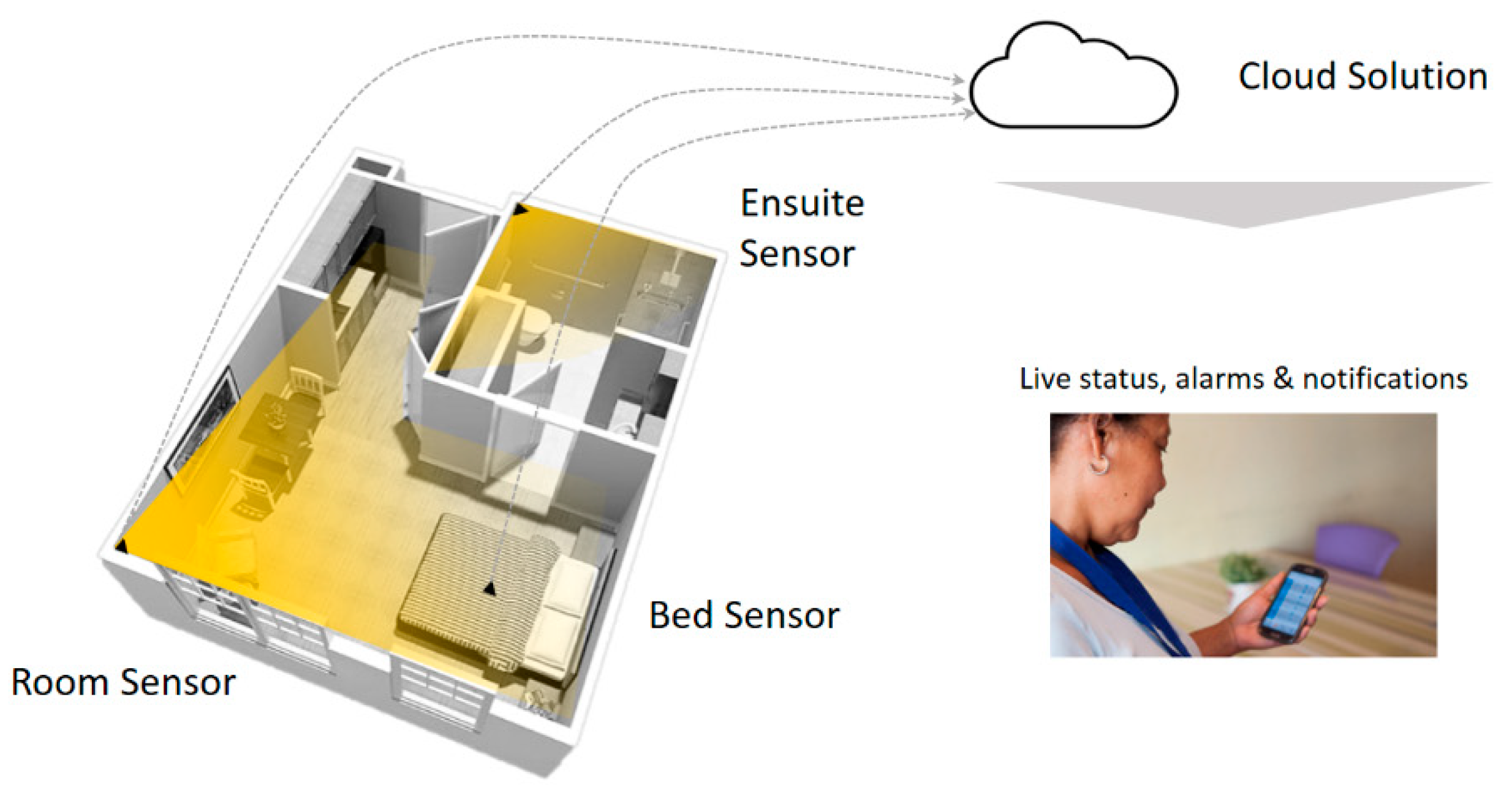
| Room Sensor | Bed Sensor | Ensuite Sensor |
|---|---|---|
 |  |  |
| Complete room view for activity/wellbeing tracking and fall detection Mounted onto Corner of Room 5V DC 2.0A Max input via Micro USB Data transmission via Wi-fi or LAN | In-bed detection and advanced sleeping pattern analytics Mounted onto Ceiling 5V DC 2.0A Max input via Micro USB Data transmission via Wi-fi or LAN | Complete room view for activity tracking and fall detection Mounted onto ceiling 5V DC 2.0A Max input via Micro USB Data transmission via Wi-fi or LAN |
References
- Aarts, E.; Encarnao, J. True Visions: The Emergence of Ambient Intelligence, 1st ed.; Springer: New York, NY, USA, 2008. [Google Scholar]
- Sadri, F. Ambient intelligence: A survey. ACM Comput. Surv. 2011, 43, 36–66. [Google Scholar] [CrossRef]
- Cook, D.J.; Augusto, J.C.; Jakkula, V.R. Ambient intelligence: Technologies, applications, and opportunities. Pervasive Mob. Comput. 2009, 5, 277–298. [Google Scholar] [CrossRef] [Green Version]
- Ageing Well in the Digital World. Available online: www.aal-europe.eu (accessed on 18 December 2018).
- Rashidi, P.; Mihailidis, A. A survey on ambient-assisted living tools for older adults. IEEE J. Biomed. Health Inf. 2013, 17, 579–590. [Google Scholar] [CrossRef]
- Nolin, J.; Olson, N. The internet of things and convenience. Internet Res. 2016, 26, 360–376. [Google Scholar] [CrossRef]
- Dupuy, L.; Consel, C.; Sauzéon, H. Self determination based design to achieve acceptance of assisted living technologies for older adults. Comput. Hum. Behav. 2016, 65, 508–521. [Google Scholar] [CrossRef]
- Chen, K.; Chan, A.H.S. A review of technology acceptance by older adults. Gerontechnology 2011, 10, 1–12. [Google Scholar] [CrossRef]
- Lee, Y.; Lee, J.; Hwang, Y. Relating motivation to information and communication technology acceptance: Self-determination theory perspective. Comput. Hum. Behav. 2015, 51, 418–428. [Google Scholar] [CrossRef]
- Conklin, J. Dialogue Mapping: Building Shared Understanding of Wicked Problems; Wiley: Bognor Regis, UK, 2005. [Google Scholar]
- Morris, Z.S.; Wooding, S.; Grant, J. The answer is 17 years, what is the question: Understanding time lags in translational research. J. R. Soc. Med. 2011, 104, 510–520. [Google Scholar] [CrossRef]
- Hignett, S.; Jones, E.L.; Miller, D.; Wolf, L.; Modi, C.; Shahzad, M.W.; Buckle, P.; Banerjee, J.; Catchpole, K. Human factors and ergonomics and quality improvement science: Integrating approaches for safety in healthcare. BMJ Qual. Saf. 2015, 24, 250–254. [Google Scholar] [CrossRef] [PubMed]
- American Association of Retired Persons. Aging in Place: A State Survey of Livability Policies and Practices; A research Report by the National Conference of State Legislatures and the AARP Public Policy Institute; AARP Public Policy Institute: Washington, DC, USA, 2011. [Google Scholar]
- Milligan, C. There’s No Place Like Home: Place and Care in an Ageing Society, 1st ed.; Ashgate: Farnham, UK, 2009. [Google Scholar]
- Rabiee, P. Exploring the relationships between choice and independence: Experiences of disabled and older people. Br. J. Soc. Work 2013, 43, 872–888. [Google Scholar] [CrossRef]
- Baldwin, N.; Harris, J.; Kelly, D. Institutionalisation: Why blame the institution? Ageing Soc. 1993, 13, 69–81. [Google Scholar] [CrossRef]
- Health Dimensions Group. Top Trends in Aging Services: Healthcare Insights and Outlooks 2018. Available online: https://www.beckershospitalreview.com/hospital-management-administration/top-trends-in-aging-services-healthcare-insights-and-outlooks-2018.html (accessed on 18 December 2018).
- Kane, R.A. Definition, measurement, and correlates of quality of life in nursing homes: Toward a reasonable practice, research, and policy agenda. Gerontologist 2003, 43, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Forbes-Thompson, S.; Gessert, C.E. Nursing homes and suffering: Part of the problem or part of the solution? J. Appl. Gerontol. 2006, 25, 234–252. [Google Scholar] [CrossRef]
- Public Health Well. Regulation and Quality Improvement Authority: Staffing Guidance for Nursing Homes. Available online: http://publichealthwell.ie/search-results/staffing-guidance-nursing-homes?source=relatedblock&content=resource&member=572160&catalogue=none&collection=none&tokens_complete=true (accessed on 18 December 2018).
- Cocco, E.; Gatti, M.; de Mendonça Lima, C.A.; Camus, V. A comparative study of stress and burnout among staff caregivers in nursing homes and acute geriatric wards. Int. J. Geriatr. Psychiatry 2003, 18, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Wallace, J.E.; Lemaire, J.B.; Ghali, W.A. Physician wellness: A missing quality indicator. Lancet 2009, 374, 1714–1721. [Google Scholar] [CrossRef]
- Bužgová, R.; Ivanová, K. Violation of ethical principles in institutional care for older people. Nurs. Ethics 2011, 18, 64–78. [Google Scholar] [CrossRef] [PubMed]
- McDonald, L.; Beaulieu, M.; Harbison, J.; Hirst, S.; Lowenstein, A.; Podnieks, E.; Wahl, J. Institutional abuse of older adults: What we know, what we need to know. J. Elder Abuse Negl. 2012, 24, 138–160. [Google Scholar] [CrossRef] [PubMed]
- Cahill, J.; Power, D.; Mackey, G.; McLoughlin, S. New technologies supporting professionalism, patient experience and patient centered care. In Proceedings of the Annual Conference of the Irish Ergonomics Society, Dublin, Ireland, 31 May 2018; pp. 1–6. [Google Scholar]
- Madden, D. Building a Culture of Patient Safety: Report of the Commission on Patient Safety and Quality Assurance; Department of Health: Dublin, Ireland, 2008.
- Kohn, L.T.; Corrigan, J.M.; Donaldson, M.S. Institute of Medicine. To Err is Human: Building a Safer Health System; National Academy Press: Washington, DC, USA, 2000. [Google Scholar]
- Brennan, T.A.; Gawande, A.; Thomas, E.; Studdert, D. Accidental deaths, saved lives, and improved quality. N. Engl. J. Med. 2005, 353, 1405–1409. [Google Scholar] [CrossRef]
- Dixon-Woods, M.; Pronovost, P.J. Patient safety and the problem of many hands. BMJ Qual. Saf. 2016, 25, 485–488. [Google Scholar] [CrossRef] [Green Version]
- Seeman, T.E.; Charpentier, P.A.; Berkman, L.F.; Tinetti, M.E.; Guralnik, J.M.; Albert, M.; Blazer, D.; Rowe, J.W. Predicting changes in physical performance in a high-functioning elderly cohort: MacArthur studies of successful aging. J. Gerontol. 1994, 49, 97–108. [Google Scholar] [CrossRef]
- Rowe, J.W.; Kahn, R.L. Successful Aging; Pantheon Books: New York, NY, USA, 1998. [Google Scholar]
- Silverstein, M.; Parker, M.G. Leisure activities and quality of life among the oldest old in Sweden. Res. Aging 2002, 24, 528–547. [Google Scholar] [CrossRef]
- Leonard, W.M. Successful aging: An elaboration of social and psychological factors. Int. J. Aging Hum. Dev. 1982, 14, 223–232. [Google Scholar] [CrossRef]
- Cinoğlu, H.; Arıkan, Y. Self, identity and identity formation: From the perspectives of three major theories. Int. J. Hum. Sci. 2012, 9, 1114–1131. [Google Scholar]
- Hewitt, J.P. Dilemmas of the American Self; Temple University Press: Philadelphia, PA, USA, 1989. [Google Scholar]
- Stryker, S. Symbolic Interactionism: A Social Structural Version; Benjamin/Cummings: Menlo Park, CA, USA, 1980. [Google Scholar]
- Brewer, M.B.; Gardner, W. Who is this “We”? Levels of collective identity and self-representations. J. Personal. Soc. Psychol. 1996, 71, 83–93. [Google Scholar] [CrossRef]
- European Commission. European Charter of Rights and Responsibilities of Older People in Need of Long Term Care and Assistance; Publications Office of the European Union: Luxembourg, 2010. [Google Scholar]
- The Alzheimer’s Society of Ireland. Human Rights and Older People in Ireland. Policy Paper. 2013. Available online: https://www.alzheimer.ie/Alzheimer/media/SiteMedia/ImageSlider/Fixed/ASI-HROP-A4-Online-Report.pdf (accessed on 3 January 2019).
- Hillcoat-Nallétamby, S. The meaning of “independence” for older people in different residential settings. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2014, 69, 419–430. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, V.; Neville, S. Personal autonomy for older people living in residential care: An overview. Nurs. Prax. N. Z. 2007, 23, 29–36. [Google Scholar]
- Barnes, M.; Blom, A.; Cox, K. The Social Exclusion of Older People: Evidence from the First Wave of the English Longitudinal Study of Ageing (ELSA): Final Report; Office for the Deputy of Prime Minister: London, UK, 2006.
- Perkins, M.; Ball, M.; Whittington, F.J.; Hollingsworth, C. Relational autonomy in assisted living: A focus on diverse care settings for older adults. J. Aging Stud. 2012, 26, 214–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engel, G. The need for a new medical model: A challenge for biomedical science. Science 1977, 196, 126–129. [Google Scholar] [CrossRef]
- Havelka, M.; Lucanin, J.D.; Lucanin, D. Biopsychosocial model—The integrated approach to health and disease. Coll. Antropol. 2009, 33, 303–310. [Google Scholar] [PubMed]
- Wolf, J.A.; Niederhauser, V.; Marshburn, D.; LaVela, S. Defining patient experience. Patient Exp. J. 2014, 1, 7–19. [Google Scholar]
- Blazek, D.; (Oneview, Dublin, Ireland). Personal communication, 2018.
- Picker Institute. Patient Experience Surveys: The Rationale; Picker Institute Europe: Oxford, UK, 2008. [Google Scholar]
- Department of Health. NHS Patient Experience Framework. 2011. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/215159/dh_132788.pdf. (accessed on 3 January 2018).
- Reframe Health Lab. Patient Engagement Versus the Engaged Patient. Available online: https://www.reframehealthlab.com/patient-engagement-vs-the-engaged-patient/ (accessed on 3 January 2018).
- World Health Organisation. Patient Engagement—Technical Series on Safer Primary Care. Available online: http://apps.who.int/iris/bitstream/handle/10665/252269/9789241511629-eng.pdf;jsessionid=21C6E37403727A9934B94345134DFBFC?sequence=1 (accessed on 3 January 2018).
- Blazek, D. Resident Engagement in Senior Living Communities—What Is It? Available online: https://www.oneviewhealthcare.com/resident-engagement-senior-living-communities/ (accessed on 3 January 2018).
- Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academy Press: Washington, DC, USA, 2001; Volume 6. [Google Scholar]
- Starfield, B. Is patient-centered care the same as person-focused care? Perm. J. 2011, 15, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Kitwood, T. Dementia Reconsidered: The Person Comes First; Open University Press: Buckingham, UK, 1997. [Google Scholar]
- Nolan, M. Relationship-centred care: Towards a new model of rehabilitation. Int. J. Ther. Rehabil. 2002, 9, 472–477. [Google Scholar] [CrossRef]
- Soklaridis, S.; Ravitz, P.; Adler, G.; Nevo, A.; Lieff, S. Relationship-centered care in health: A 20-year scoping review. Patient Exp. J. 2016, 3, 130–145. [Google Scholar]
- Beach, M.C.; Inui, T. Relationship-Cantered Care Research Network. Relationship-centered care: A constructive reframing. J. Gen. Intern. Med. 2006, 21 (Suppl. 1), S3–S8. [Google Scholar] [CrossRef] [PubMed]
- Cahill, J.; McLoughlin, S.; Wetherall, S. The design of new technology supporting wellbeing, independence and social participation for older adults domicile in residential homes and/or assisted living communities. Technologies 2018, 6, 18. [Google Scholar] [CrossRef]
- Cahill, J.; McLoughlin, S.; Wetherall, S. Lived Experience, Stakeholder Evaluation and the Participatory Design of Assisted Living Technology. In Proceedings of the AAATE 2017 Congress, Sheffield, UK, 12–15 September 2017; iOS Press: Amsterdam, The Netherlands. [Google Scholar] [CrossRef]
- Cahill, J.; McLoughlin, S.; Wetherall, S.; Stolberg, M.; O’Connor, M. Addressing Issues of Need, Adaptability, User Acceptability and Ethics in the Participatory Design of New Technology Enabling Wellness, Independence and Dignity for Seniors Living in Residential Homes. In Proceedings of the Third International Conference on Human Aspects of IT for the Aged Population (ITAP 2017), Held as Part of HCI International 2017, Vancouver, BC, Canada, 9–14 July 2017; Springer: Berlin, Germany, 2017. [Google Scholar]
- Wetherall, S. Creating Ambient Care Environments. Oneview Healthcare Internal Report. Unpublished work. 2016. [Google Scholar]
- Cousins, J.B.; Whitmore, E.; Shulha, L. Arguments for a common set of principles for collaborative inquiry in evaluation. Am. J. Eval. 2013, 34, 7–22. [Google Scholar] [CrossRef]
- Van Maanen, J. Tales of the Field: On Writing Ethnography; University of Chicago Press: Chicago, IL, USA, 1988. [Google Scholar]
- Hammersley, M.; Atkinson, P. Ethnography: Principles in Practice, 3rd ed.; Routledge: London, UK, 2007. [Google Scholar]
- Knight, J. Ethnography, Chapter 31. In Encyclopedia of Human Computer Interaction, 2nd ed.; Ghaoui, C., Ed.; Idea Group Publishing: Hershey, PA, USA, 2006. [Google Scholar]
- Lindseth, A.; Norberg, A. A phenomenological hermeneutical method for researching lived experience. Scand. J. Caring Sci. 2004, 18, 145–153. [Google Scholar] [CrossRef] [Green Version]
- Pruitt, J.; Grudin, J. Personas: Practice and Theory. In Proceedings of the 2003 Conference on Designing for User Experiences (DUX ’03), San Francisco, CA, USA, 5–7 June 2003; ACM: New York, NY, USA, 2003; pp. 1–15. [Google Scholar] [CrossRef]
- Carroll, J.M. Scenario-Based Design: Envisioning Work and Technology in System Development; John Wiley and Sons: New York, NY, USA, 1995. [Google Scholar]
- Bødker, S.; Burr, J. The design collaboratorium: A place for usability design. ACM Trans. Comput. Hum. Interact. 2002, 9, 152–169. [Google Scholar] [CrossRef]
- Wenger, E. Communities of Practice: Learning, Meaning, and Identity; Cambridge University Press: Cambridge, UK, 1998. [Google Scholar]
- WMA General Assembly. Declaration of Helsinki; Amended by the 64th WMA General Assembly, Fortaleza, Brazil, 2013; World Medical Association: Ferney-Voltaire, France, 2015. [Google Scholar]
- Schwaber, K. Agile Project Management with Scrum; Microsoft Press: Washington, DC, USA, 2004; ISBN 978-0-7356-1993-7. [Google Scholar]
- Scrum Alliance. What Is Scrum? An Agile Framework for Completing Complex Projects. Available online: https://www.scrumalliance.org/ScrumRedesignDEVSite/media/ScrumAllianceMedia/Public%20Relations_2/What-is-Scrum-Backgrounder-2014.pdf (accessed on 24 February 2016).
- Beck, K.; Beedle, M.; Bennekum, A.; Cockburn, A.; Cunningham, W.; Fowler, M.; Grenning, J.; Highsmith, J.; Hunt, A.; Jeffries, R.; et al. Manifesto for Agile Software Development. 2001. Available online: http://www.agilemanifesto.org/ (accessed on 18 December 2018).
- Dynn, C.; Agogino, A.; Eris, O.; Frey, D.; Leifer, L. Engineering design thinking, teaching, and learning. IEEE Eng. Manag. Rev. 2006, 34, 65. [Google Scholar] [CrossRef]
- Avedesian, M. Creating Successful Products, Building Sustainable Businesses. In The Lean Startup; Crown Publishing Group: New York, NY, USA, 2014. [Google Scholar]
- Jones, T.S.; Richey, R.C. Rapid prototyping methodology in action: A developmental study. Educ. Technol. Res. Dev. 2000, 48, 63–80. [Google Scholar] [CrossRef]
- Agile for All. New to Agile—Invest in Good User Stories. Available online: https://agileforall.com/new-to-agile-invest-in-good-user-stories/ (accessed on 18 December 2018).
- HD Insight. Available online: https://docs.microsoft.com/en-us/azure/hdinsight/ (accessed on 7 January 2018).
- What is Azure Databricks. Available online: https://docs.microsoft.com/en-us/azure/azure-databricks/what-is-azure-databricks (accessed on 7 January 2018).
- Introduction to Stream Analytics. Available online: https://docs.microsoft.com/en-us/azure/stream-analytics/stream-analytics-introduction (accessed on 7 January 2018).
- Overview of Logic Apps. Available online: https://docs.microsoft.com/en-us/azure/logic-apps/logic-apps-overview (accessed on 7 January 2018).
- Nait Aicha, A.; Englebienne, G.; van Schooten, K.S.; Pijnappels, M.; Krose, B. Deep learning to predict falls in oder adults based on daily-life trunk accelerometry. Sensors 2018, 18, 1654. [Google Scholar] [CrossRef] [PubMed]
- Open Systems Interconnections (OSI) Models. Available online: https://en.wikipedia.org/wiki/OSI_model. (accessed on 7 January 2018).
- OpenThread. Available online: https://openthread.io (accessed on 7 January 2018).
- Zigbee. Available online: https://en.wikipedia.org/wiki/Zigbee (accessed on 7 January 2018).
- Message Queuing Telemetry Transport (MQTT). Available online: https://en.wikipedia.org/wiki/MQTT (accessed on 7 January 2018).
- Pubsub. Available online: https://cloud.google.com/pubsub (accessed on 7 January 2018).
- Pubsub. Available online: https://www.pubnub.com/solutions/iot (accessed on 7 January 2018).
- What Is KNX: A Brief Introduction. Available online: https://www.knx.org/knx-en/for-professionals/What-is-KNX/A-brief-introduction/index.php (accessed on 7 January 2018).












| # | Theme | Subtheme | 1a | 1b | 2 | 3 |
|---|---|---|---|---|---|---|
| 3.2 | Resident Experience | Concept of home | * | * | * | |
| Residential home | * | * | * | |||
| Comfort | * | * | * | |||
| Resident states | * | * | * | |||
| Identity social participation | * | * | * | * | ||
| 3.3 | Care Delivery | Scope and processes | * | * | * | |
| Wellness communications | * | * | * | |||
| Wellness and stability | * | * | * | |||
| 3.4 | Residential Care and Sensing Framework | * | * | * | * | |
| 3.5 | Technology Goals | * | * | * | * | |
| 3.6 | Ethics and User Acceptability | * | * | * | ||
| 3.7 | Application of Existing Sensor State of the Art to Residential Care | General | * | * | ||
| Sensors and monitoring person/resident | * | * | ||||
| Sensors and monitoring environment | * | * | ||||
| Sensors and monitoring care delivery | * | * | ||||
| 3.8 | Technical Architecture | * | * | |||
| 3.9 | Design | * | * | * | * | |
| 3.10 | Managing Change | * | * | * |
| # | High-Level Technology Goals |
|---|---|
| 1 | Enable holistic care delivery—underpinned by concepts of holistic care—attention to wellness, relationship centered care and professionalism. |
| 2 | Overall, use technology (sensor and tablet kit) to build a resident profile. This includes a picture of the (1) resident and their wellness, (2) how they are living in the environment, and (3) their care, and (4) the relationships between each of these. |
| 3 | Following from (2), to use the technology (tablet and sensor kit), to actively manage and update the resident’s profile, to optimize resident wellness. |
| 4 | Link up information flows arising from the diverse care processes—admission, assessments, care planning, daily care, reporting, adverse events reporting. |
| 5 | Predictive risk management in relation to resident wellness and stability—anticipate state changes and flag need for interventions if required. |
| 6 | Continuously monitor status of care delivery—if missed rounding or medication—and notify care-givers and management as to status. |
| 7 | Flag need for interventions at environmental level (adjust room lighting, temp etc.), and automate action to ensure room settings appropriate to resident preference and/or wellness. |
| 8 | Support staff communication (staff briefing and handover). |
| 9 | Support resident/staff communication and care delivery. |
| 10 | Enable everybody involved in care/report on resident wellness (resident, family, nurse, Dr, care assistant, admin). |
| 11 | Gather data about (1) individual residents, (2) all residents—to improve care planning/quality of care. |
| # | Sensing Framework | Care Processes | Sensors and Smart Room | ||
|---|---|---|---|---|---|
| Admissions | Assessments and Care Planning | Daily Care | |||
| 1 | Resident & resident wellness | Advance initial personal profile Advance preliminary health profile | Following assessments, define a health profile and baseline in relation to key wellness parameters (biological, psychological and social) | Track and report wellness against baseline If significant changes, identify need for reassessments and new care plan (i.e., relationship to 3) | Advance sensor profile for resident linking to (1) Track health/wellness including social and physical activity |
| 2 | Environment | Define resident preferences for room | N/A | N/A | Over time, use sensors to build profile of resident/continuously learn about person and room preferences and relationship between wellness and room settings Make changes to room settings, based on learnings |
| 3 | Care Delivery | Establish preliminary care need linked to health profile (1) | Following assessments, assign a care profile and specific care tasks | Report on care delivery Track receiving care in line with care plan etc | Track human contact/presence of caregiver in room |
| # | Wellness Management |
|---|---|
| 1 | Residents and care assistants reports on wellness and wellness information is available to all (integrated in existing reports, surveys, specific wellness reports). |
| 2 | Includes 1 Also, staff report on actions taken to manage wellness. |
| 3 | Includes 1 and 2 Also, system automates a basic summary wellness evaluation/status (for 3 pillars)—based on analysis of parameters provided by ALL (resident, nurse, care assistant, family). |
| 4 | Includes 1, 2 and 3 Also, system recommends care actions (spanning 3 pillars), which can be accepted, or alternatives proposed—all actions documented by staff using system. |
| 5 | Includes 1, 2, 3 and 4 Also, system requests reports from relevant actors on status of care actions—if successful/improvement in wellbeing. |
| 6 | Includes 1, 2, 3 and 4 Also, system provides intelligence as to care outcomes, requirement for reassessment, other interventions. |
| 7 | Wider reporting and analytics over time for care facility, per issue, per intervention, per patient. |
| # | Change in State | Care Action | Indicator |
|---|---|---|---|
| 1 | No Change | None |  |
| 2 | Minor Change | Monitor |  |
| 3 | Significant Change | Action Required |  |
| 4 | Major Change | Action Required—(Immediate/Urgency) |  |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cahill, J.; Portales, R.; McLoughin, S.; Nagan, N.; Henrichs, B.; Wetherall, S. IoT/Sensor-Based Infrastructures Promoting a Sense of Home, Independent Living, Comfort and Wellness. Sensors 2019, 19, 485. https://doi.org/10.3390/s19030485
Cahill J, Portales R, McLoughin S, Nagan N, Henrichs B, Wetherall S. IoT/Sensor-Based Infrastructures Promoting a Sense of Home, Independent Living, Comfort and Wellness. Sensors. 2019; 19(3):485. https://doi.org/10.3390/s19030485
Chicago/Turabian StyleCahill, Joan, Raul Portales, Sean McLoughin, Nithia Nagan, Braden Henrichs, and Sean Wetherall. 2019. "IoT/Sensor-Based Infrastructures Promoting a Sense of Home, Independent Living, Comfort and Wellness" Sensors 19, no. 3: 485. https://doi.org/10.3390/s19030485
APA StyleCahill, J., Portales, R., McLoughin, S., Nagan, N., Henrichs, B., & Wetherall, S. (2019). IoT/Sensor-Based Infrastructures Promoting a Sense of Home, Independent Living, Comfort and Wellness. Sensors, 19(3), 485. https://doi.org/10.3390/s19030485