1. Introduction
Wearable biomedical technology has become ubiquitous in recent years, sparking a new research field in the area of IoT for healthcare applications [
1]. Electronic miniaturization and advances in smart materials have allowed devices to be attached to the surface of the human body for measurement of physiological parameters, while consuming little amount of power and/or harvesting the energy from the body environment itself. Examples of such devices include glucose meters, biopotential monitors, motion trackers, odor sensors and UV detectors. The requirement for causing minimum discomfort and embarrassment to the user is guiding the design of the so-called
wearables so as to be conformal with the body shape, in the form of flexible adhesive patches or incorporated into pieces of clothing and accessories. Many of these devices are already on the market in part to satisfy consumers’ appetite for cutting-edge technology, but also to expand the research from the clinical environment to the comfort of home, workplace or sports venue [
2].
Continuous monitoring of physiological variables is still largely limited to clinical environments and/or specialized laboratories that typically use bulky medical equipment certified for human trials. Such equipment requires galvanically-isolated power and data communication lines for the embedded electronics, as well as wiring connections to the recording spots over the body surface. Measurement of more than one signal modality involves recruiting additional equipment to detect the different signals simultaneously. Therefore, wearable device design must couple, in one end, with the acquisition of signals originated from different transduction mechanisms and, in the other end, employ low-power and low data-rate transfer protocols, like the Bluetooth Low Energy (BLE) for untethered applications that are battery-powered. Much like the case of the present study, where we committed ourselves to measure several signals related with the performance of physical exercise, including the assessment of cardiovascular, motion and sweat parameters, inside a small-form device developed for the head segment.
Body motion detection has been the target of a large portion of wearable technology developed in the past years, employing innovative ways to integrate accelerometers, gyroscopes and/or magnetometers into different body segments/joints and also taking into account the surrounding environment where the detection is performed [
3]. In order to provide motion detection, we opted to include an accelerometer in the proposed device as the information originated by head acceleration can help complement the information derived from cardiovascular and sweat monitoring, by distinguishing if a sudden change in the latter parameters is related to exercise, as targeted by this study, or rather resulting from some pathological condition leading to movement restrictions, such as fever experienced during a systematic inflammatory response of the body. Regarding cardiovascular monitoring, measurement of the electrical activity of the heart has long been the preferential method to estimate heart rate (HR) and heart rate variability (HRV), useful to detect early signs of potential heart attack, arrhythmias and myocardial infection [
4,
5]. For exercise in particular, control of the individual effort by monitoring HR and HRV more accurately and frequently is important not only to avoid body injuries due to inadequate intensive strains but also to prevent sudden death, as the vast majority of exercises practiced in sport involve a short increase in the risk of heart attack. Modern ECG monitors limit the number of body leads in order to reduce dimensions and power consumption, acquiring the electrical signal preferentially over the chest and/or body limbs. In this study, we opted to acquire the ECG around the ears by using a single bipolar lead, hence preventing any wiring connections over the limbs (and chest) that can disturb exercise’s performance. In the interface with the skin, novel ECG electrodes are also been developed to withstand higher temperatures, humidity levels and water immersion, occurring in some sport modalities. Moreover, special adhesives made of nanomaterials and epidermal electronics have been shown to produce less skin irritation, inasmuch like the E-textiles employed in the present study as an alternative to the traditional wet electrodes [
6].
Sweat monitoring is another modality gaining much attention lately in wearable technology, which has application in the detection of early signs of skin dehydration and imbalances in the internal body fluids produced by intensive physical activities or some autonomic dysfunctions, such as hyperhidrosis and diabetes. Laboratory methods for measuring sweat are vast and include Miner’s method [
7], “wash-down” techniques [
8], Parafilm patches [
9] and impedance [
10]. From all these methods, only impedance can be performed for extended periods of time outside laboratorial settings. However, impedance involves complex circuitry for
wearables and it is neither completely immune to movement artifacts nor electrode placement. In this paper, we reduce the complexity in electronics by allowing a single excitation frequency in the lower spectrum (1 kHz) where the conductivity effects dominate within the biological tissues, introducing also a new matrix made of electrodes to cover the tissues under analysis more uniformly. Such strategy avoids the problem related to electrode placement, while providing an area for sweat spreading (and dissipation), slowing down the process of channel saturation. In opposition to the approaches that use water vapor flow measurements [
11] and humidity sensors printed on textiles [
12], our solution employs a smaller and removable detection matrix, which minimizes the disturbance in the microclimate close to the skin where the sweat glands are located. Sweat also contains electrolytes that can be further analyzed such as pH and lactate for assessment of the athletes’ performance or personal wellbeing [
13]. pH is the analyte detected by means of a voltammeter transduction mechanism [
14], wherein the concentration of protons in solution increases the voltage potential around an active electrode in reference to a bias level. The active pH electrode can be deposited using different techniques such as screen printing [
15,
16,
17], dip casting, electrochemical deposition [
18] and tailored according to the requirements using, in some cases, gold modified hydrogen ionosphere and plasticized PVC or graphene-polyurethane composites [
19]. The typically high impedance of the electrode must be matched in the recording electronics by an ultra-low input bias current amplifier in order to reduce measurement errors introduced by the multiplication of the bias current of the amplifier by the electrode’s impedance, masking the potential generated by the protons in solution (around 56 mV/ unit pH). By its turn, lactate is recorded amperometrically by immobilizing lactate enzyme inside a sensing membrane and careful tailoring of the sensing layers to prevent unwanted interferences from other molecules in solution [
20]. Lactate is then ionized and flows accordingly to the electric field imposed between a counter and reference electrodes, being detected through a working electrode that transforms this ionic flow into electrical current. Within this study, we deposited pH and lactate sensors over gold-platted electrodes located on a removable ear support, which contains also the electrodes for impedance and ECG. An additional membrane protects the chemical sensors from movement interferences, which constitutes a novelty when compared to the laboratory platforms found in the aforementioned literature, yet porous enough to allow sweat to flow. For the case of intense exercise leading to a faster saturation of the measurement channels, the ear support can easily be detached from the main circuitry board, washed and new sensors deposited again, assuring the reuse of the proposed technology.
From all the exposed above and in summary, in this paper we propose an ear-worn device to measure cardiovascular and sweat parameters during exercise with BLE connectivity. Unlike the approach followed by the authors of [
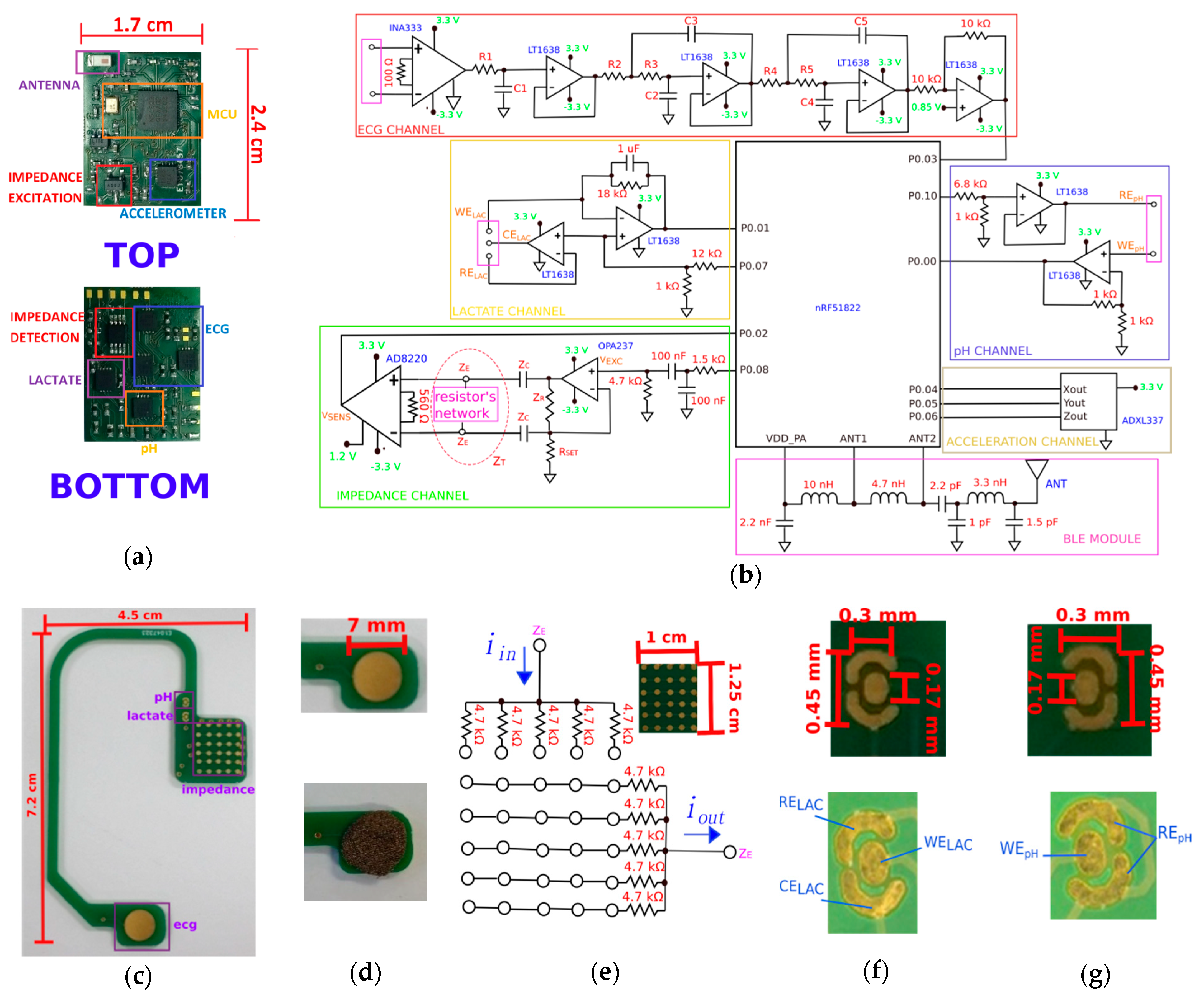
21], the proposed device records bipolar ECG signals around the ears, whereas sweat rate is estimated by the impedance method. Recording of pH and lactate levels as well as head motion complements the specifications of the device, especially designed as an unobtrusive earpiece shown in
Figure 1. Its location has been selected to facilitate access to the sweat accumulating in the upper part of the cheek (zygomatic arch) in the left side of the head, while the detection of the ECG signal occurs over the sternocleidomastoid muscle, hence avoiding the surrounding (non-conductive) bone areas. Our approach is to integrate multimodal sensing into a single device by making use of discrete
off-the-shelf components. Another approaches use either large commercial chipsets or
system-on-chip design into a custom-made smaller chip, which can integrate many functions and sensing capabilities by reconfiguring the basic analogue front-end blocks involved in the measurement of bio-potential, impedance and/or chemical analytes [
22,
23]. However, this latter approach has several disadvantages including longer design-to-production times and the inability to measure all modalities in simultaneous, besides requiring logical signals and reference clocks to select the desirable configuration, filter tuning and control that adds extra modulation noise originating from external complex digital circuitry. Moreover, multiplexing of input signals to meet the requirements of reconfigurable electronics is never a good option as it degrades the input impedance of the first amplifier on the electronic chain as seen directly by the source of the input signals, which must remain as higher as possible for detection of tiny bio-potential signals and/or pH level, as performed in this study.
4. Discussion
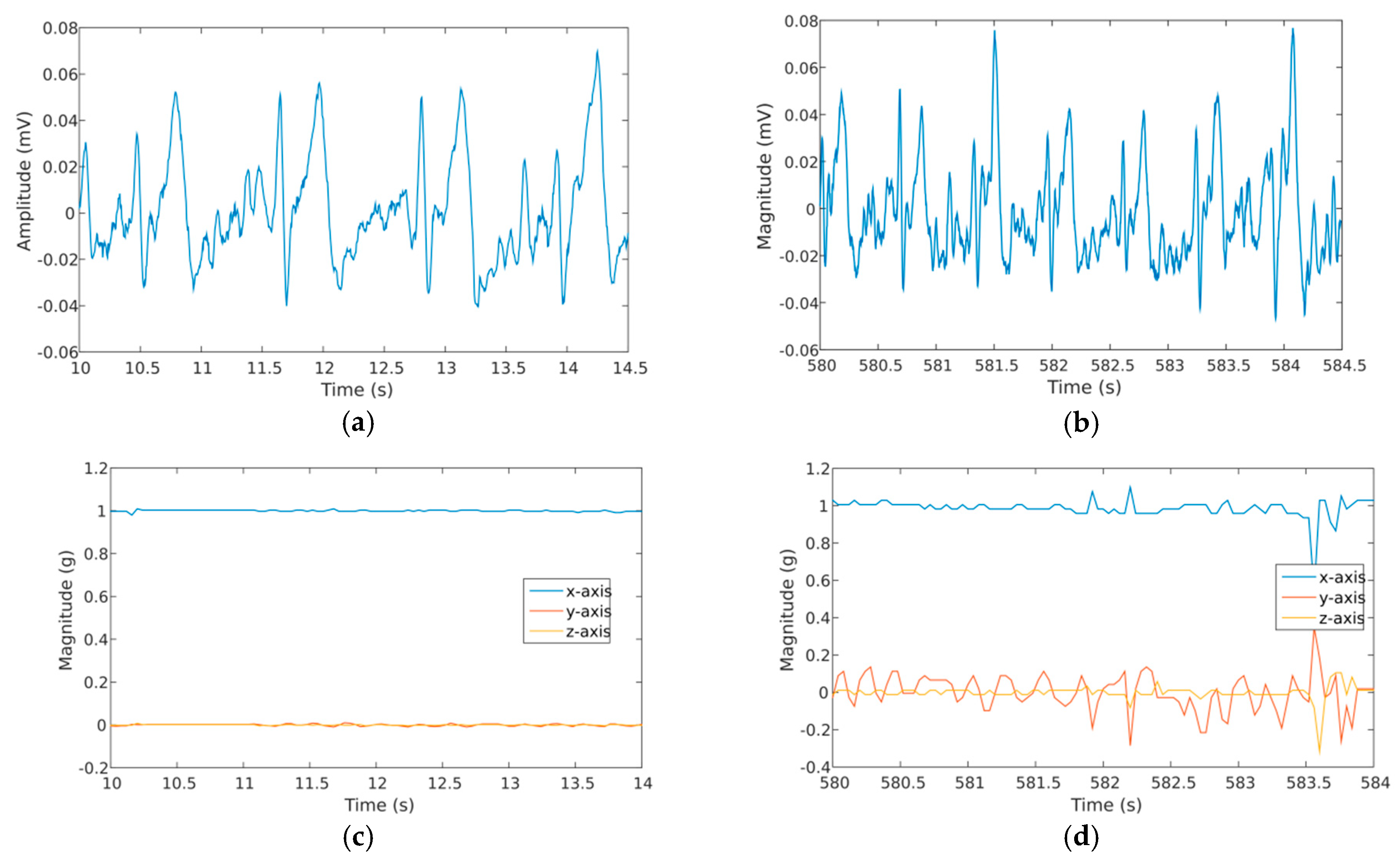
The results obtained for the ECG channel have shown signals with higher SNR value for the chest lead, followed by the shoulder/leg, wrist and ear region, after amplification. The SNR levels obtained after amplification (INA333) are still relative small, which is reflected by the presence of a large amount of noise in the spectrum, especially from the 50 Hz power-grid (
Figure 3c). Subsequent analogue and digital filtering has elevated the SNR to allow digitalization of the ECGs with moderate QRS definition, enough to estimate the heart beat even at the level of the ears, but with complete absence of the P-wave as experienced already by the authors of [
21]. The measuring equipment employed to calculate SNR in this study also introduced additional noise and measurement errors to the values, though it was the only method available to access the target pins directly over the electronics. Moreover, defining the frequency components that belong exclusively to ECG events from those arising from other sources (including noise) is not a trivial process, if commercial and calibrated ECG recording equipment is not available for comparison. In any case, from
Figure 3b, one can see that the signals acquired in the chest have the highest amplitudes and ears the lowest of all. This is further corroborated by the simulation model in
Figure 3a, where the electric dipole propagates with higher intensity along the chest area, followed by the propagation into the limbs and finally to the head segment.
Regarding impedance, the excitation signal generated by the device yielded a THD value of −20.46 dB (
Figure 4a). This relative low value for THD is a consequence of filtering the square signal produced by the MCU with 1st-order filters only. This drawback was compensated by performing impedance calibrations using resistors and solutions with stable resistance values in the frequency domain, instead of relying directly on the result given by Equation (4). As the frequency of excitation is relatively slow (1 kHz), the conductivity effects on the materials being tested prevail over permittivity and the dispersion effects. Conductivity effects are more frequency-independent and their influence can be understood by applying a simplified version of the Ohm’s law. Within this regard, the loss in impedance magnitude is proportional to the decay induced by the influence of signal harmonics over the fundamental, whose real impedance value for materials and tissues can then be recovered by calibration. From the calibration graph in
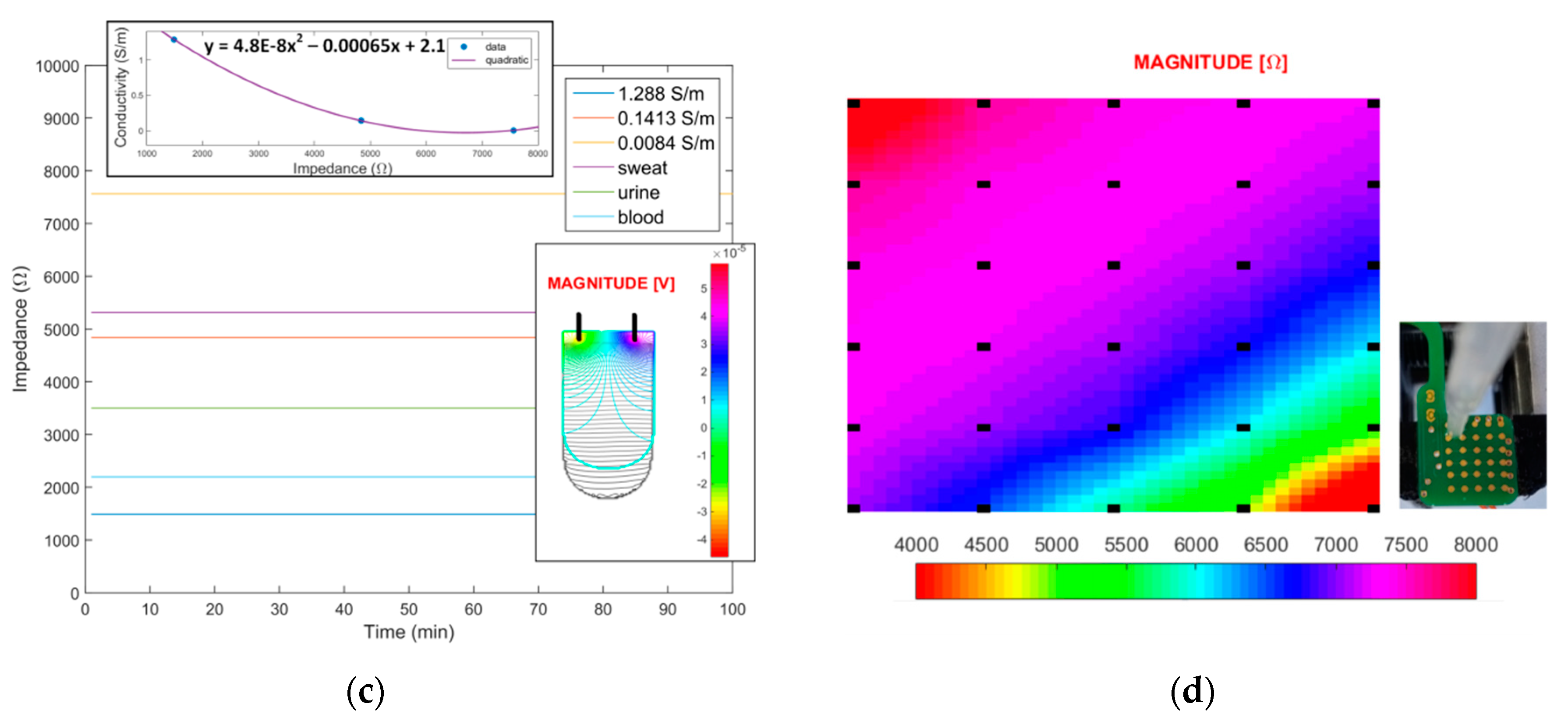
Figure 4b, it can be seen that the device responds to a range between 1 kΩ and 8 kΩ, with a step resolution close to 10 Ω, a value obtained by considering the resolution of the acquisition channel (10-bit) and the interval of impedance values measured. The 10 Ω resistor produces a voltage of 20 μV, which is already above the noise level of the differential amplifier employed in the acquisition channel (14 nV/√Hz) within a 1 kHz bandwidth (14 μV). By its turn, measurement of the impedance value for solutions with different conductivities has allowed to obtain a fitting curve employed latter to detect the true conductivity level of some body fluids, independently of the geometry of the electrodes and sample container (
Figure 4c). Conductivity levels measured by this method were 0.9 S/m for blood, 0.08 S/m for sweat and 0.4 S/m for urine. Compared with literature reference (
Table A1,
Appendix A), these values are higher by almost a value of 0.2 S/m (blood and urine only), though the experimental conditions were not the same between the current experiment and literature. For the simulation model in
Figure 4b, the isocurrent lines for the resistor cross its entire extension, yielding potential lines symmetrically distributed between the recording electrodes, whereas in
Figure 4c, some of the current lines escape from the top of the solution and their contribution to the voltage level detected is not accounted for, a fact that might explain the aforementioned discrepancies in conductivity.
For the chemical sensors, a sensitivity level of 53 mV/pH was measured for the fabricated pH sensor (
Figure 5a), which declines to a level of 50 mV/pH with the electronic device (
Figure 5c). The bias current at the input terminal of the non-inverting amplifier can be responsible for this decline as well as the circuit board traces connecting the pH sensor to the amplifier, introducing further measurement errors. Nevertheless, the device with pH sensor attached was able to distinguish the pH from different solutions by producing proportional voltage levels. By its turn, for lactate, an increasing voltage level was obtained with the concentration of the analyte in solution for both the electrochemical workstation (
Figure 5b) and proposed device (
Figure 5d). For the latter, the sensibility is higher for the lower concentrations of lactate (<20 mM) reflected in the higher voltage difference between signal baselines in
Figure 5d. The complete lactate measurement channel saturates for concentrations close to 20 mM as a consequence of the current amplification level set by device electronics. In the present conditions and attending to the fitting curve obtained, the voltage difference between tested solution (≃20 mM) is 0.25 V, a value that divided by the resistor employed in the transimpedance amplifier (18,000 kΩ) yields a detectable current level of 14 μA or a standardized sensitivity level of 0.8 μA/mM for the sensor.
Finally, in what concerns the physical exercise, the parameters that experience faster changes are heart rate and impedance (
Figure 7), with pH and lactate experiencing an abrupt rise at the middle of the indoors cycling event. Moreover, in the 10 min period allowed for recovery, these parameters do not return to their initial levels, in opposition to ECG, with all subjects going back to pre-exercise HR. By its turn, the impedance level never recovers completely from the decline proportionated by exercise, suggesting that some sort of micro fluidic channel must be included within the matrix to remove more efficiently the sweat during intensive physical activities or replace the ear support by a freshly new one in order to continue monitoring. At the end, the mean variation of the physiological parameters measured among all subjects during the trail are pH = 5.10 ± 1.54, LAC = 5.26 ± 7.50 mM, IMP = 4.59 ± 3.73 kΩ and HR = 85 ± 25.
5. Conclusions
An ear-worn device for cardiovascular and sweat monitoring has been experimentally tested under both laboratory and real exercise conditions. The need to confine the electronics into a small low-powered device has led to some simplifications in terms of circuitry implementation, namely the absence of higher-order filters to increase the THD of the excitation signal (impedance) and cascade amplifiers for the pH and lactate channels. Measurement of the phase for impedance was also not performed in this study as it remains unclear its influence in the course of the biological processes occurring inside tissues. The limitation on the acquisition rate of the internal ADC of the microcontroller (<10 kSPS) prevented the use of higher frequencies for impedance stimulation as well. By its turn, the absence of a driven right leg circuit for ECG had repercussions in the lower SNR values obtained in the first stage of signal amplification. With more robust electronics, we believe that it is still possible to detect all features of the ECG around the ears if higher ADC resolutions are employed (16-bit as commonly employed by front-end components in medical equipment) together with better shielding of device electronics and body segment.
To the best knowledge of the authors, this is the first study that combines the measurement of the cardiovascular performance with sweat parameters that has been fully integrated into a single ear-worn device. Control of the individual effort in physical activities is of paramount importance in sports in order to avoid injuries due to unadjusted intensive strains, a situation that the device can help prevent if overstrain is detected on the levels of the measured signals in real-time.
Finally, as future work, miniaturization of the device in terms of electronics can still be achieved externally by system-on-chip integration for every sensing modality independently or, internally, by means of an implantable device. In this latter scenario, bipolar ECG recordings are no longer feasible and HR estimation must be performed by means of optical measurements, such as pulse plethysmography over the earlobe. A flexible circuit board can also be designed for the ear support to adjust more naturally to the contour of the head and ears, though the capacitive substrates employed in the process may alter the impedance measurements. In the chemistry point-of-view, other analytes can also be detected in sweat by incorporation of new sensors with specialized membranes tailored to detect them. In this scenario, the specificity of each sensor must be individually evaluated against all the chemical species present in the medium, from each lactate is one of the most predominant analytes expelled during exercise.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}









