Window-Modulated Compounding Nakagami Parameter Ratio Approach for Assessing Muscle Perfusion with Contrast-Enhanced Ultrasound Imaging


Abstract
:1. Introduction
2. Materials and Methods
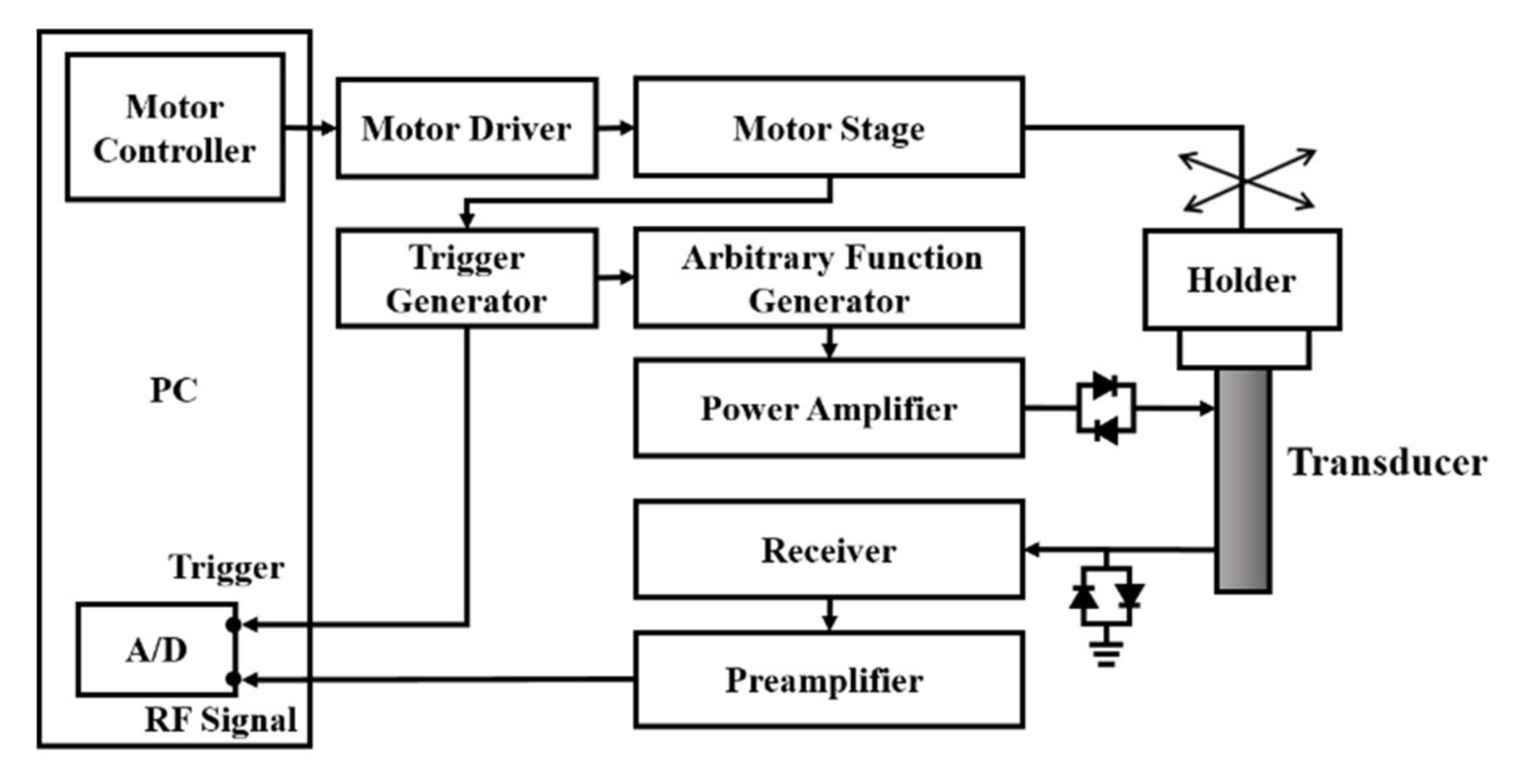
2.1. Ultrasound Imaging System
2.2. Flow Phantom Experiments
2.3. Animal Experiments
2.4. Perfusion Parameters Estimation
3. Results
3.1. Flow Phantom Experiments
3.2. In Vivo Animal Experiments
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Marini, M.; Veicsteinas, A. The exercised skeletal muscle: A review. Eur. J. Transl. Myol. 2010, 20, 105–120. [Google Scholar] [CrossRef]
- Aspelin, P.; Ekberg, O.; Thorsson, O.; Wilhelmsson, M.; Westlin, N. Ultrasound examination of soft tissue injury of the lower limb in athletes. Am. J. Sports Med. 1992, 20, 601–603. [Google Scholar] [CrossRef] [PubMed]
- Draghi, F.; Zacchino, M.; Canepari, M.; Nucci, P.; Alessandrino, F. Muscle injuries: Ultrasound evaluation in the acute phase. J. Med. Ultrasound 2013, 16, 209–214. [Google Scholar] [CrossRef] [Green Version]
- Lovitt, S.; Marden, F.A.; Gundogdu, B.; Ostrowski, M.L. MRI in myopathy. Neurol. Clin. 2004, 22, 509–538. [Google Scholar] [CrossRef]
- Matin, P.; Lang, G.; Carretta, R.; Simon, G. Scintigraphic evaluation of muscle damage following extreme exercise: Concise communication. J. Nucl. 1983, 24, 308–311. [Google Scholar]
- Ament, W.; Lubbers, J.; Rakhorst, G.; Vaalburg, W.; Verkerke, G.J.; Paans, A.M.; Willemsen, A.T. Skeletal muscle perfusion measured by positron emission tomography during exercise. Pflügers Arch. 1998, 436, 653–658. [Google Scholar] [CrossRef]
- Nuutila, P.; Kalliokoski, K. Use of positron emission tomography in the assessment of skeletal muscle and tendon metabolism and perfusion. Scand. J. Med. Sci. Sports 2000, 10, 346–350. [Google Scholar] [CrossRef]
- Garcia, J. MRI in inflammatory myopathies. Skeletal Radiol. 2000, 29, 425–438. [Google Scholar] [CrossRef]
- Lutz, A.M.; Weishaupt, D.; Amann-Vesti, B.R.; Pfammatter, T.; Goepfert, K.; Marincek, B.; Nanz, D. Assessment of skeletal muscle perfusion by contrast medium first-pass magnetic resonance imaging: Technical feasibility and preliminary experience in healthy volunteers. J. Magn. Reson. Imaging 2004, 20, 111–121. [Google Scholar] [CrossRef]
- Weber, M.A.; Krix, M.; Delorme, S. Quantitative evaluation of muscle perfusion with CEUS and with MR. Eur. Radiol. 2007, 17, 2663–2674. [Google Scholar] [CrossRef] [PubMed]
- Peetrons, P. Ultrasound of muscles. Eur. Radiol. 2002, 12, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-H.; Hsieh, M.-Y.; Su, F.-C.; Wang, S.-H. Assessment of the kinetic trajectory of the median nerve in the wrist by high-frequency ultrasound. Sensors 2014, 14, 7738–7752. [Google Scholar] [CrossRef] [PubMed]
- Krix, M.; Weber, M.A.; Krakowski-Roosen, H.; Huttner, H.B.; Delorme, S.; Kauczor, H.U.; Hildebrandt, W. Assessment of skeletal muscle perfusion using contrast-enhanced ultrasonography. J. Med. Ultrasound 2005, 24, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Huang, C.C.; Wang, S.H. Quantitative assessments of burn degree by high-frequency ultrasonic backscattering and statistical model. Phys. Med. Biol. 2011, 56, 757–773. [Google Scholar] [CrossRef]
- Maruvada, S.; Shung, K.K.; Wang, S.-H. High-frequency backscatter and attenuation measurements of porcine erythrocyte suspensions between 30–90 MHz. Ultrasound Med. Biol. 2002, 28, 1081–1088. [Google Scholar] [CrossRef]
- Shung, K.K. Diagnostic Ultrasound: Imaging and Blood Flow Measurements; CRC Press: Boca Raton, FL, USA, 2006. [Google Scholar]
- Cosgrove, D. Ultrasound contrast agents: An overview. Eur. J. Radiol. 2006, 60, 324–330. [Google Scholar] [CrossRef]
- Sboros, V. Response of contrast agents to ultrasound. Adv. Drug. Deliv. Rev. 2008, 60, 1117–1136. [Google Scholar] [CrossRef]
- Huang, C.C.; Lin, Y.H.; Wang, S.H. The Effect of Kinetic Properties on Statistical Variations of Ultrasound Signals Backscattered from Flowing Blood. Jpn. J. Appl. Phys. 2009, 48, 027002. [Google Scholar] [CrossRef]
- Kaul, S. Myocardial contrast echocardiography: A 25-year retrospective. Circulation 2008, 118, 291–308. [Google Scholar] [CrossRef] [Green Version]
- Siracusano, S.; Bertolotto, M.; Ciciliato, S.; Valentino, M.; Liguori, G.; Visalli, F. The current role of contrast-enhanced ultrasound (CEUS) imaging in the evaluation of renal pathology. World J. Urol. 2011, 29, 633. [Google Scholar] [CrossRef]
- Duerschmied, D.; Olson, L.; Olschewski, M.; Rossknecht, A.; Freund, G.; Bode, C.; Hehrlein, C. Contrast ultrasound perfusion imaging of lower extremities in peripheral arterial disease: A novel diagnostic method. Eur. Heart J. 2006, 27, 310–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duerschmied, D.; Maletzki, P.; Freund, G.; Olschewski, M.; Seufert, J.; Bode, C.; Hehrlein, C. Analysis of muscle microcirculation in advanced diabetes mellitus by contrast enhanced ultrasound. Diabetes Res. Clin. Pract. 2008, 81, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.N.; Cotter, J.D.; Lucas, S.J.; Hill, B.G.; van Rij, A.M. Reliability of contrast-enhanced ultrasound for the assessment of muscle perfusion in health and peripheral arterial disease. Ultrasound Med. Biol. 2015, 41, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Hotfiel, T.; Heiss, R.; Swoboda, B.; Kellermann, M.; Gelse, K.; Grim, C.; Strobel, D.; Wildner, D. Contrast-enhanced ultrasound as a new investigative tool in diagnostic imaging of muscle injuries—A pilot study evaluating conventional ultrasound, CEUS, and findings in MRI. Clin. J. Sport Med. 2018, 28, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Krix, M.; Krakowski-Roosen, H.; Kauczor, H.U.; Delorme, S.; Weber, M.A. Real-time contrast-enhanced ultrasound for the assessment of perfusion dynamics in skeletal muscle. Ultrasound Med. Biol. 2009, 35, 1587–1595. [Google Scholar] [CrossRef]
- Song, Y.; Li, Y.; Wang, P.J.; Gao, Y. Contrast-enhanced ultrasonography of skeletal muscles for type 2 diabetes mellitus patients with microvascular complications. Int. J. Clin. Exp. Med. 2014, 7, 573–579. [Google Scholar]
- Forsberg, F.; Merton, D.; Liu, J.; Needleman, L.; Goldberg, B. Clinical applications of ultrasound contrast agents. Ultrasonics 1998, 36, 695–701. [Google Scholar] [CrossRef]
- Tao, Q.; Wang, Y.; Fish, P.; Wang, W.; Cardoso, J. The wall signal removal in Doppler ultrasound systems based on recursive PCA. Ultrasound Med. Biol. 2004, 30, 369–379. [Google Scholar] [CrossRef]
- Tsui, P.-H.; Wang, S.-H. The effect of transducer characteristics on the estimation of Nakagami parameter as a function of scatterer concentration. Ultrasound Med. Biol. 2004, 30, 1345–1353. [Google Scholar] [CrossRef]
- Tsui, P.H.; Chang, C.C. Imaging local scatterer concentrations by the Nakagami statistical model. Ultrasound Med. Biol. 2007, 33, 608–619. [Google Scholar] [CrossRef]
- Tsui, P.H.; Yeh, C.K.; Chang, C.C. Microvascular Flow Estimation by Microbubble-Assisted Nakagami Imaging. Ultrasound Med. Biol. 2009, 35, 653–671. [Google Scholar] [CrossRef]
- Gu, X.; Wei, M.; Zong, Y.; Jiang, H.; Wan, M. Flow quantification with nakagami parametric imaging for suppressing contrast microbubbles attenuation. Ultrasound Med. Biol. 2013, 39, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Shankar, P.M. Ultrasonic tissue characterization using a generalized Nakagami model. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2001, 48, 1716–1720. [Google Scholar] [CrossRef] [PubMed]
- Tsui, P.-H.; Ma, H.-Y.; Zhou, Z.; Ho, M.-C.; Lee, Y.-H. Window-modulated compounding Nakagami imaging for ultrasound tissue characterization. Ultrasonics 2014, 54, 1448–1459. [Google Scholar] [CrossRef]
- Krix, M.; Kiessling, F.; Farhan, N.; Schmidt, K.; Hoffend, J.; Delorme, S. A multivessel model describing replenishment kinetics of ultrasound contrast agent for quantification of tissue perfusion. Ultrasound Med. Biol. 2003, 29, 1421–1430. [Google Scholar] [CrossRef]
- Everitt, B.S.; Skrondal, A. The Cambridge Dictionary of Statistics, 4th ed.; Cambridge University Press: Cambridge, UK, 2010. [Google Scholar]
- Tsui, P.-H.; Wang, S.-H.; Huang, C.-C.; Chiu, C.-Y. Quantitative Analysis of Noise Influence on the Detection of Scatterer Concentration by Nakagami Parameter. J. Med. Biol. Eng. 2005, 25, 45–51. [Google Scholar]
- Sassaroli, E.; Hynynen, K. Resonance frequency of microbubbles in small blood vessels: A numerical study. Phys. Med. Biol. 2005, 50, 5293–5305. [Google Scholar] [CrossRef]
- Dave, J.K.; Halldorsdottir, V.G.; Eisenbrey, J.R.; Liu, J.B.; McDonald, M.E.; Dickie, K.; Leung, C.; Forsberg, F. Noninvasive Estimation of Dynamic Pressures In Vitro and In Vivo Using the Subharmonic Response From Microbubbles. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2011, 58, 2056–2066. [Google Scholar] [CrossRef]
- Chen, Q.; Zagzebski, J.; Wilson, T.; Stiles, T. Pressure-dependent attenuation in ultrasound contrast agents. Ultrasound Med. Biol. 2002, 28, 1041–1051. [Google Scholar] [CrossRef]
- Sboros, V.; MacDonald, C.A.; Pye, S.D.; Moran, C.M.; Gomatam, J.; McDicken, W.N. The dependence of ultrasound contrast agents backscatter on acoustic pressure: Theory versus experiment. Ultrasonics 2002, 40, 579–583. [Google Scholar] [CrossRef]
- Ho, M.-C.; Lin, J.-J.; Shu, Y.-C.; Chen, C.-N.; Chang, K.-J.; Chang, C.-C.; Tsui, P.-H. Using ultrasound Nakagami imaging to assess liver fibrosis in rats. Ultrasonics 2012, 52, 215–222. [Google Scholar] [CrossRef] [PubMed]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Center frequency | 7.3 MHz |
| −6 dB bandwidth | 3.2 MHz |
| f-number | 2.8 |
| Depth of focus | 53.3 mm |
| Aperture size | 19 mm |
| Perfusion Parameter | Descriptions |
|---|---|
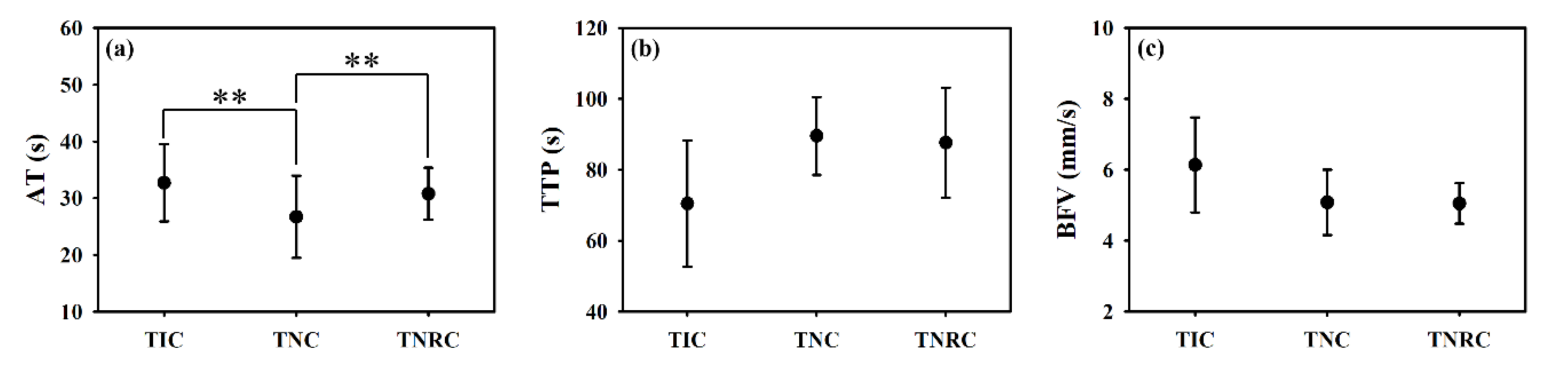
| Arrival time (AT) | Time at the arrival of UCAs |
| Peak value (MAX) | Peak value of the perfusion curve corresponding to the flow-in UCAs |
| Time-to-peak (TTP) | Interval between AT and the time of MAX |
| Blood flow velocity (BFV) | Mean blood flow velocity within the duration of UCAs perfusion |
| Area under perfusion curve (AUC) | Area under the curve of UCAs perfusion |
| Method | TIC | TNC | TNRC | |
|---|---|---|---|---|
| Parameter | ||||
| AT | 19.27% | 53.78% | 10.07% | |
| TTP | 25.20% | 12.29% | 17.12% | |
| MAX | 33.33% | 11.11% | 26.08% | |
| BFV | 19.59% | 14.93% | 9.24% | |
| AUC | 24.04% | 8.62% | 17.48% | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, H.-C.; Wang, S.-H. Window-Modulated Compounding Nakagami Parameter Ratio Approach for Assessing Muscle Perfusion with Contrast-Enhanced Ultrasound Imaging. Sensors 2020, 20, 3584. https://doi.org/10.3390/s20123584
Lin H-C, Wang S-H. Window-Modulated Compounding Nakagami Parameter Ratio Approach for Assessing Muscle Perfusion with Contrast-Enhanced Ultrasound Imaging. Sensors. 2020; 20(12):3584. https://doi.org/10.3390/s20123584
Chicago/Turabian StyleLin, Huang-Chen, and Shyh-Hau Wang. 2020. "Window-Modulated Compounding Nakagami Parameter Ratio Approach for Assessing Muscle Perfusion with Contrast-Enhanced Ultrasound Imaging" Sensors 20, no. 12: 3584. https://doi.org/10.3390/s20123584
APA StyleLin, H.-C., & Wang, S.-H. (2020). Window-Modulated Compounding Nakagami Parameter Ratio Approach for Assessing Muscle Perfusion with Contrast-Enhanced Ultrasound Imaging. Sensors, 20(12), 3584. https://doi.org/10.3390/s20123584