A Multidomain Approach to Assessing the Convergent and Concurrent Validity of a Mobile Application When Compared to Conventional Methods of Determining Body Composition



Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Measurements with Conventional Methods and LeanScreen
- Neck: inferior to the laryngeal prominence
- Waist: most narrow portion between the xiphoid process and umbilicus
- Umbilicus: directly in line with the umbilicus
- Hips: at the widest point and across the most prominent portion of the buttocks
- Left Humerus: midway between the left acromion and olecranon processes
- Right Humerus: midway between the right acromion and olecranon processes
- Left Femur: midway between the left inguinal crease and proximal border of the patella
- Right Femur: midway between the right inguinal crease and proximal border of the patella
2.3. LeanScreen Methods
2.4. Data Analysis
3. Results
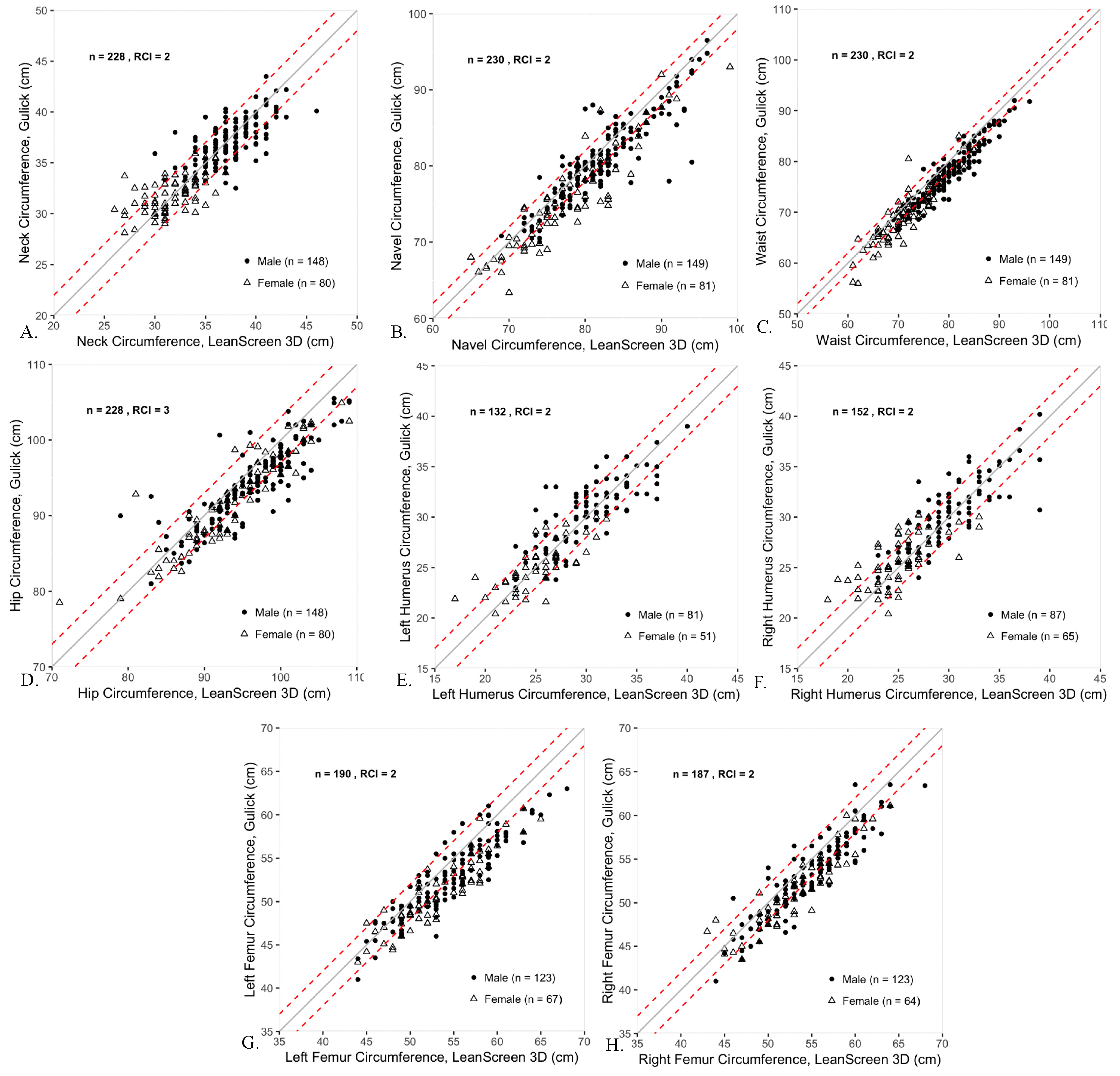
3.1. Body Circumferences
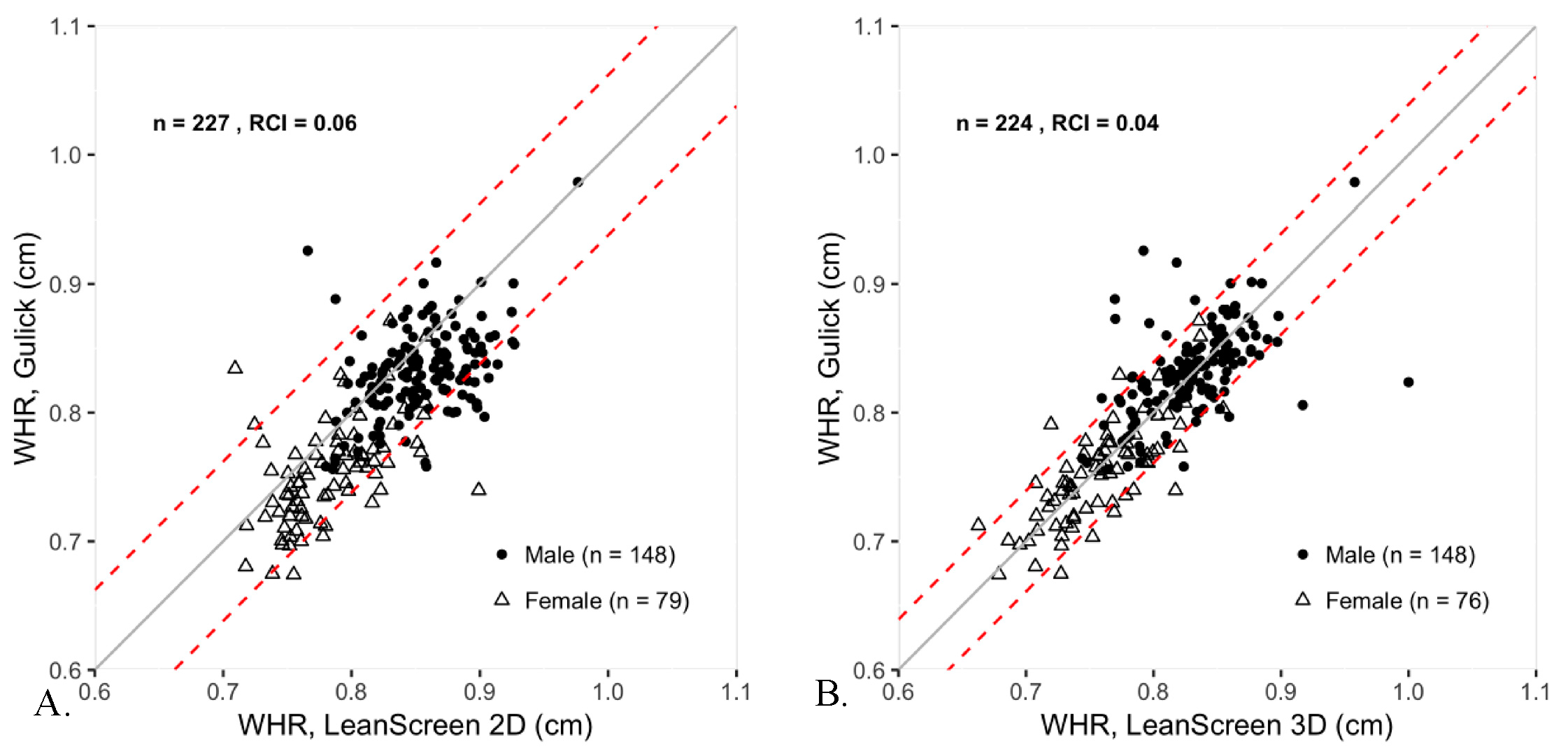
3.2. Waist-To-Hip Ratio
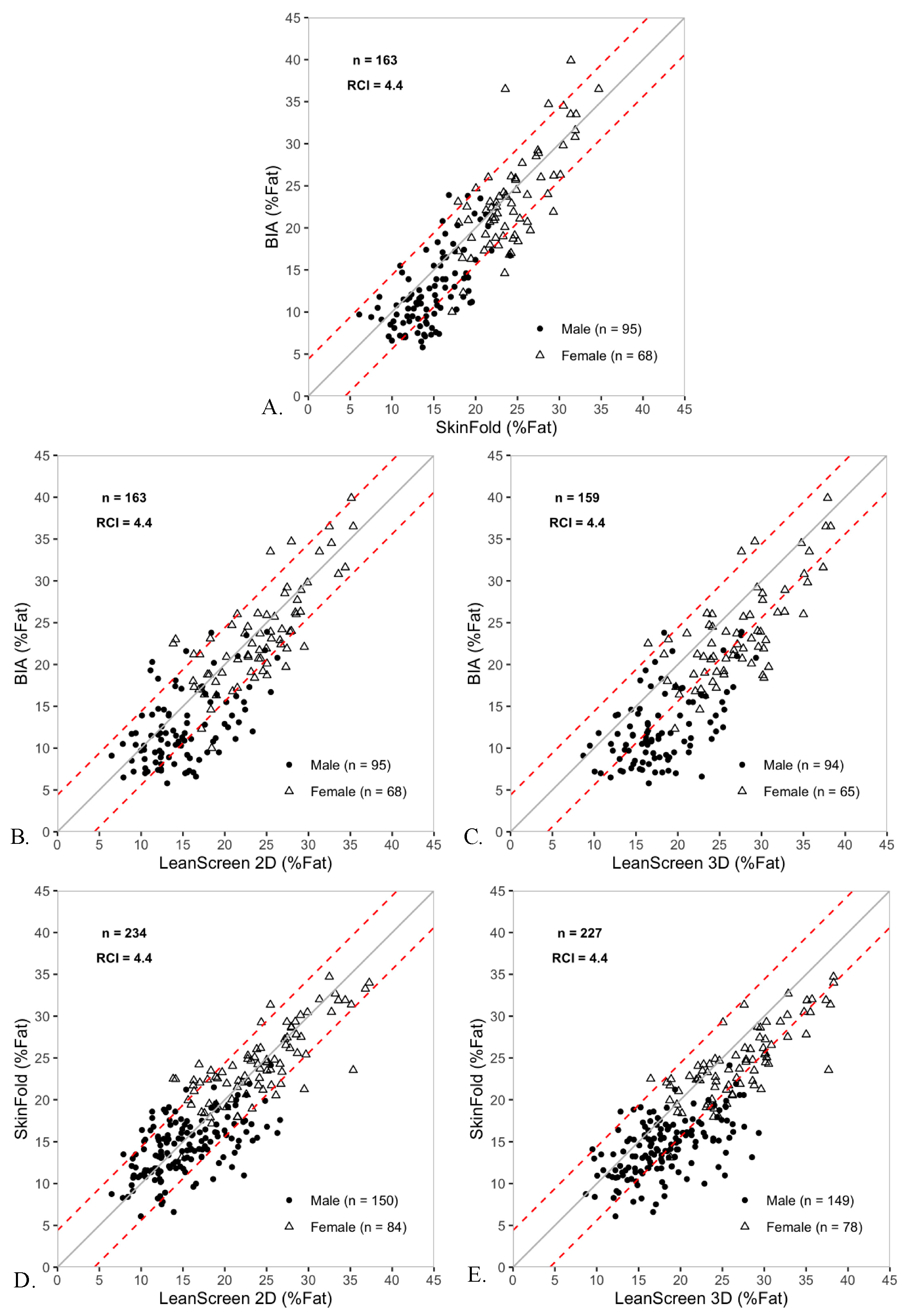
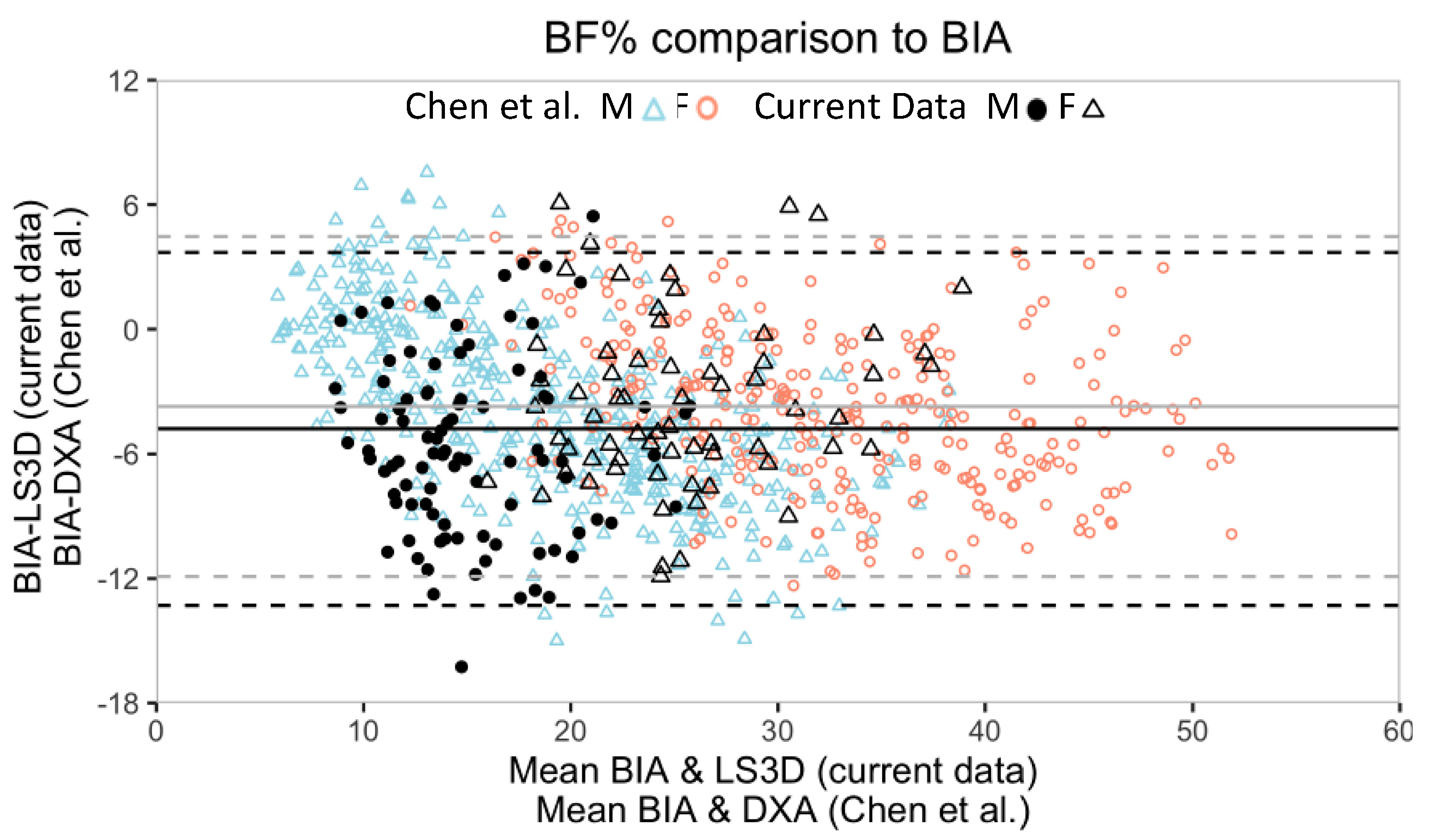
3.3. Body Fat Percentage
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Burke, G.L.; Bertoni, A.G.; Shea, S.; Tracy, R.; Watson, K.E.; Blumenthal, R.S.; Chung, H.; Carnethon, M.R. The impact of obesity on cardiovascular disease risk factors and subclinical vascular disease. Arch Intern. Med. 2008, 168, 928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golay, A.; Ybarra, J. Link between obesity and type 2 diabetes. Best Pract. Res. Clin. Endocrinol. Metab. 2005, 19, 649–663. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; De Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart disease and stroke statistics—2017 update: A report from the american heart association. Circulation 2017, 135. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Kruszon-Moran, D.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Trends in obesity among adults in the united states, 2005 to 2014. JAMA 2016, 315, 2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coppetti, T.; Brauchlin, A.; Müggler, S.; Attinger-Toller, A.; Templin, C.; Schönrath, F.; Hellermann, J.; Lüscher, T.F.; Biaggi, P.; Wyss, C.A. Accuracy of smartphone apps for heart rate measurement. Eur. J. Prev. Cardiol. 2017, 24, 1287–1293. [Google Scholar] [CrossRef]
- Yan, B.P.; Chan, C.K.; Li, C.K.; To, O.T.; Lai, W.H.; Tse, G.; Poh, Y.C.; Poh, M.Z. Resting and postexercise heart rate detection from fingertip and facial photoplethysmography using a smartphone camera: A validation study. JMIR mHealth uHealth 2017, 5, e33. [Google Scholar] [CrossRef]
- Brinkløv, C.F.; Thorsen, I.K.; Karstoft, K.; Brøns, C.; Valentiner, L.; Langberg, H.; Vaag, A.A.; Nielsen, J.S.; Pedersen, B.K.; Ried-Larsen, M. Criterion validity and reliability of a smartphone delivered sub-maximal fitness test for people with type 2 diabetes. BMC Sports Sci. Med. Rehabil. 2016, 8, 31. [Google Scholar] [CrossRef] [Green Version]
- Schoeppe, S.; Alley, S.; Van Lippevelde, W.; Bray, N.A.; Williams, S.L.; Duncan, M.J.; Vandelanotte, C. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 127. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Kang, J.-H.; Kim, O.; Choi, M.; Oh, M.; Nam, J.; Sung, E. Interventions for preventing childhood obesity with smartphones and wearable device: A protocol for a non-randomized controlled trial. Int. J. Environ. Res. Public Health 2017, 14, 184. [Google Scholar] [CrossRef] [Green Version]
- Scott, B.K.; Miller, G.T.; Fonda, S.J.; Yeaw, R.E.; Gaudaen, J.C.; Pavliscsak, H.H.; Quinn, M.T.; Pamplin, J.C. Advanced digital health technologies for COVID-19 and future emergencies. Telemed. e-Health 2020. [Google Scholar] [CrossRef]
- Sust, P.P.; Solans, O.; Fajardo, J.C.; Peralta, M.M.; Rodenas, P.; Gabaldà, J.; Eroles, L.G.; Comella, A.; Muñoz, C.V.; Ribes, J.S.; et al. Turning the crisis into an opportunity: Digital health strategies deployed during the COVID-19 outbreak. JMIR Public Health Surveill. 2020, 22, e19106. [Google Scholar] [CrossRef] [PubMed]
- Inkster, B.; O’Brien, R.; Selby, E.; Joshi, S.; Subramanian, V.; Kadaba, M.; Schroeder, K.; Godson, S.; Comley, K.; Vollmer, S.J.; et al. Digital health management during and beyond the COVID-19 pandemic: Opportunities, barriers, and recommendations (Preprint). JMIR Ment. Health 2020, 7, e19246. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.S.; Asch, D.A.; Volpp, K.G. Wearable devices as facilitators, not drivers, of health behavior change. JAMA 2015, 313, 459. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Bian, J.; Leavitt, T.; Vincent, H.K.; Vander Zalm, L.; Teurlings, T.L.; Smith, M.D.; Modave, F. Assessing the quality of mobile exercise apps based on the american college of sports medicine guidelines: A reliable and valid scoring instrument. J. Med. Internet Res. 2017, 19, e67. [Google Scholar] [CrossRef]
- Jo, E.; Lewis, K.; Directo, D.; Kim, M.J.; Dolezal, B.A. Validation of biofeedback wearables for photoplethysmographic heart rate tracking. Sport Sci. Med. 2016, 15, 540–547. [Google Scholar]
- Lee, J.; Finkelstein, J. Consumer sleep tracking devices: A critical review. Stud. Health Technol. Inf. 2015, 210, 458–460. [Google Scholar]
- Shieh, C.; Knisely, M.R.; Clark, D.; Carpenter, J.S. Self-weighing in weight management interventions: A systematic review of literature. Obes. Res. Clin. Pract. 2016, 10, 493–519. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; Klem MLou Sereika, S.M.; Danford, C.A.; Ewing, L.J.; Burke, L.E. Self-weighing in weight management: A systematic literature review. Obesity 2015, 23, 256–265. [Google Scholar] [CrossRef]
- Banack, H.R.; Wactawski-Wende, J.; Hovey, K.M.; Stokes, A. Is BMI a valid measure of obesity in postmenopausal women? Menopause 2018, 25, 307–313. [Google Scholar] [CrossRef]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Thomas, R.J.; Collazo-Clavell, M.L.; Korinek, J.E.; Allison, T.G.; Batsis, J.A.; Sert-Kuniyoshi, F.H.; Lopez-Jimenez, F. Accuracy of body mass index in diagnosing obesity in the adult general population. Int. J. Obes. 2008, 32, 959–966. [Google Scholar] [CrossRef] [Green Version]
- Wickramasinghe, V.P.; Cleghorn, G.J.; Edmiston, K.A.; Murphy, A.J.; Abbott, R.A.; Davies, P.S.W. Validity of BMI as a measure of obesity in Australian white Caucasian and Australian Sri Lankan children. Ann. Hum. Biol. 2005, 32, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.; Wang, Z.; Heshka, S.; Heo, M.; Faith, M.S.; Heymsfield, S.B. Waist circumference and obesity-associated risk factors among whites in the third national health and nutrition examination survey: Clinical action thresholds. Am. J. Clin. Nutr. 2002, 76, 743. [Google Scholar] [CrossRef] [PubMed]
- Dalton, M.; Cameron, A.J.; Zimmet, P.Z.; Shaw, J.E.; Jolley, D.; Dunstan, D.W.; Welborn, T.A.; AusDiab Steering Committee. Waist circumference, waist-hip ratio and body mass index and their correlation with cardiovascular disease risk factors in Australian adults. J. Intern. Med. 2003, 254, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Q.; Dong, S.-Y.; Sun, X.-N.; Xie, J.; Cui, Y. Percent body fat is a better predictor of cardiovascular risk factors than body mass index. Braz. J. Med. Biol. Res. 2012, 45, 591–600. [Google Scholar] [CrossRef]
- Lee, S.Y.; Gallagher, D. Assessment methods in human body composition. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 566–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boland, D.M.; Neufeld, E.V.; Ruddell, J.; Dolezal, B.A.; Cooper, C.B. Inter- and intra-rater agreement of static posture analysis using a mobile application. J. Phys. Ther. Sci. 2016, 28, 3398–3402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macdonald, E.Z.; Vehrs, P.R.; Fellingham, G.W.; Eggett, D.; George, J.D.; Hager, R. Validity and reliability of assessing body composition using a mobile application. Med. Sci. Sports Exerc. 2017, 49, 2593–2599. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Wolters Kluwer/Lippincott Williams & Wilkins Health: Philadelphia, PA, USA, 2014. [Google Scholar]
- O’Connor, D.P.; Bray, M.S.; McFarlin, B.K.; Sailors, M.H.; Ellis, K.J.; Jackson, A.S. Generalized equations for estimating DXA percent fat of diverse young women and men. Med. Sci. Sports Exerc. 2010, 42, 1959–1965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidson, L.E.; Wang, J.; Thornton, J.C.; Kaleem, Z.; Silva-Palacios, F.; Pierson, R.N.; Heymsfield, S.B.; Gallagher, D. Predicting fat percent by skinfolds in racial groups. Med. Sci. Sports Exerc. 2011, 43, 542–549. [Google Scholar] [CrossRef] [Green Version]
- Heyward, V. ASEP methods recommendation: Body composition assessment. J. Exerc. Physiol. Online 2001, 4, 1–12. [Google Scholar]
- Carlson, K.D.; Herdman, A.O. Understanding the impact of convergent validity on research results. Organ. Res. Methods 2012, 15, 17–32. [Google Scholar] [CrossRef]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2009. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding bland altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Stolarova, M.; Wolf, C.; Rinker, T.; Brielmann, A. How to assess and compare inter-rater reliability, agreement and correlation of ratings: An exemplary analysis of mother-father and parent-teacher expressive vocabulary rating pairs. Front. Psychol. 2014, 5, 509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revelle, W.R. psych: Procedures for Personality and Psychological Research. Published Online. 2017. Available online: https://www.scholars.northwestern.edu/en/publications/psych-procedures-for-personality-and-psychological-research (accessed on 6 September 2020).
- Lehnert, B. BlandAltmanLeh: Plots (Slightly Extended) Bland-Altman Plots Version 0.3.1 from CRAN. Available online: https://rdrr.io/cran/BlandAltmanLeh/ (accessed on 6 September 2020).
- Chen, K.T.; Chen, Y.Y.; Wang, C.W.; Chuang, C.L.; Chiang, L.M.; Lai, C.L.; Lu, H.K.; Dwyer, G.B.; Chao, S.P.; Shih, M.K.; et al. Comparison of standing posture bioelectrical impedance analysis with DXA for body composition in a large, healthy Chinese population. PLoS ONE 2016, 11, e0160105. [Google Scholar] [CrossRef]
- Marx, R.; Porcari, J.P.; Doberstein, S.; Mikat, R.; Ryskey, A.; Foster, C. Ability of the leanscreen app to accurately assess body composition. Comp. Exerc. Physiol. 2017, 13, 59–66. [Google Scholar] [CrossRef]
- Dolezal, B.A.; Lau, M.J.; Abrazado, M.; Storer, T.W.; Cooper, C.B. Validity of two commercial grade bioelectrical impedance analyzers for measurement of body fat percentage. J. Exerc. Physiol. Online 2013, 16, 74–83. [Google Scholar]
- Choudhary, P.K.; Nagaraja, H.N. Measuring agreement in method comparison studies—a review. Adv. Rank. Sel. Mult. Comp. Reliab. 2007, 2802, 215–244. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Body Composition Measure | Conventional Methods | LeanScreen Methods |
|---|---|---|
| Body Circumferences | Gulick tape | LeanScreen 3D (LS3D) |
| Waist-To-Hip Ratio (WHR) | Gulick tape | LeanScreen 2D (LS2D) LeanScreen 3D (LS3D) |
| Body Fat Percentage (BF%) | SkinfoldsBioelectrical Impedance (BIA) | LeanScreen 2D (LS2D) LeanScreen 3D (LS3D) |
| Body Circumference Locations | Convergent Validity | Concurrent Validity | ||||
|---|---|---|---|---|---|---|
| Pearson Coefficient r [95% CI] | Bias [95% CI] | 95% Limits of Agreement | Individual % Agreement ** | |||
| Male | Female | Total | ||||
| Neck (cm) | 0.85 [0.80, 0.88] | 0 [−1, 1] | (−4, 4) | 74 (4) | 78 (5) | 75 (3) |
| Umbilicus (cm) | 0.91 [0.89, 0.93] | 2 [1, 3] * | (−4, 8) | 62 (4) | 51 (6) | 58 (3) |
| Waist (cm) | 0.96 [0.94, 0.97] | 2 [−6, 6] | (−2, 6) | 46 (4) | 46 (6) | 46 (3) |
| Hip (cm) | 0.89 [0.86, 0.91] | 2 [1, 3] * | (−4, 8) | 69 (4) | 70 (5) | 69 (3) |
| Left Humerus (cm) | 0.85 [0.80, 0.89] | 0 [−1, 1] | (−4, 4) | 62 (5) | 76 (6) | 67 (4) |
| Right Humerus (cm) | 0.85 [0.80, 0.89] | 0 [−1, 1] | (−4, 4) | 67 (5) | 69 (6) | 68 (4) |
| Left Femur (cm) | 0.90 [0.87, 0.92] | 2 [1, 3] * | (−2, 6) | 53 (5) | 42 (6) | 49 (4) |
| Right Femur (cm) | 0.92 [0.89, 0.94] | 2 [1, 3] * | (−2, 5) | 56 (4) | 50 (6) | 54 (4) |
| Waist-to-Hip Ratio Measurements | Convergent Validity | Concurrent Validity | ||||
|---|---|---|---|---|---|---|
| Pearson Coefficient r [95% CI] | Bias [95% CI] | 95% Limits of Agreement | Individual % Agreement ** | |||
| Male | Female | Total | ||||
| Gulick and LeanScreen 2D | 0.73 [0.66, 0.78] | 0.02 [0.01, 0.03] * | (−0.05, 0.10) | 86.5 (2.8) | 82.3 (4.3) | 85.0 (2.4) |
| Gulick and LeanScreen 3D | 0.81 [0.75, 0.85] | 0.00 [−0.01, 0.01] | (−0.06, 0.06) | 87.8 (2.7) | 85.5 (4.0) | 87.1 (2.2) |
| BF% Measurements | Convergent Validity | Concurrent Validity | ||||
|---|---|---|---|---|---|---|
| Pearson Coefficient r [95% CI] | Bias [95% CI] | (95% LoA) | Individual % Agreement (SD) ** | |||
| Male | Female | Overall | ||||
| BIA and Skinfolds | 0.86 [0.82, 0.90] | 1.7 [1.1, 2.3] * | (−5.7, 9.0) | 65.3 (4.9) | 72.1 (5.4) | 68.1 (3.7) |
| BIA and LeanScreen2D | 0.82 [0.77, 0.87] | 1.8 [1.2, 2.4] * | (−6.5, 10.1) | 58.9 (5.0) | 75.0 (5.3) | 65.6 (3.7) |
| Skinfolds and LeanScreen2D | 0.83 [0.78, 0.86] | 0.5 [0.0, 1.0] | (−6.8, 7.8) | 74.7 (3.6) | 82.1 (4.2) | 77.4 (2.7) |
| BIA and LeanScreen3D | 0.82 [0.76, 0.86] | 4.8 [4.1, 5.5] * | (−3.7, 13.3) | 38.3 (5.0) | 47.7 (6.2) | 42.1 (3.9) |
| Skinfolds and LeanScreen3D | 0.82 [0.77, 0.86] | 3.4 [2.9, 3.9] * | (−4.1, 10.8) | 57.7 (4.0) | 69.2 (5.2) | 61.7 (3.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neufeld, E.V.; Seltzer, R.A.; Sazzad, T.; Dolezal, B.A. A Multidomain Approach to Assessing the Convergent and Concurrent Validity of a Mobile Application When Compared to Conventional Methods of Determining Body Composition. Sensors 2020, 20, 6165. https://doi.org/10.3390/s20216165
Neufeld EV, Seltzer RA, Sazzad T, Dolezal BA. A Multidomain Approach to Assessing the Convergent and Concurrent Validity of a Mobile Application When Compared to Conventional Methods of Determining Body Composition. Sensors. 2020; 20(21):6165. https://doi.org/10.3390/s20216165
Chicago/Turabian StyleNeufeld, Eric V., Ryan A. Seltzer, Tasnim Sazzad, and Brett A. Dolezal. 2020. "A Multidomain Approach to Assessing the Convergent and Concurrent Validity of a Mobile Application When Compared to Conventional Methods of Determining Body Composition" Sensors 20, no. 21: 6165. https://doi.org/10.3390/s20216165
APA StyleNeufeld, E. V., Seltzer, R. A., Sazzad, T., & Dolezal, B. A. (2020). A Multidomain Approach to Assessing the Convergent and Concurrent Validity of a Mobile Application When Compared to Conventional Methods of Determining Body Composition. Sensors, 20(21), 6165. https://doi.org/10.3390/s20216165