
The Concept of Advanced Multi-Sensor Monitoring of Human Stress



Abstract
:1. Introduction
2. Human Stress Phenomena
3. Physiological Variables in Stress Measurement
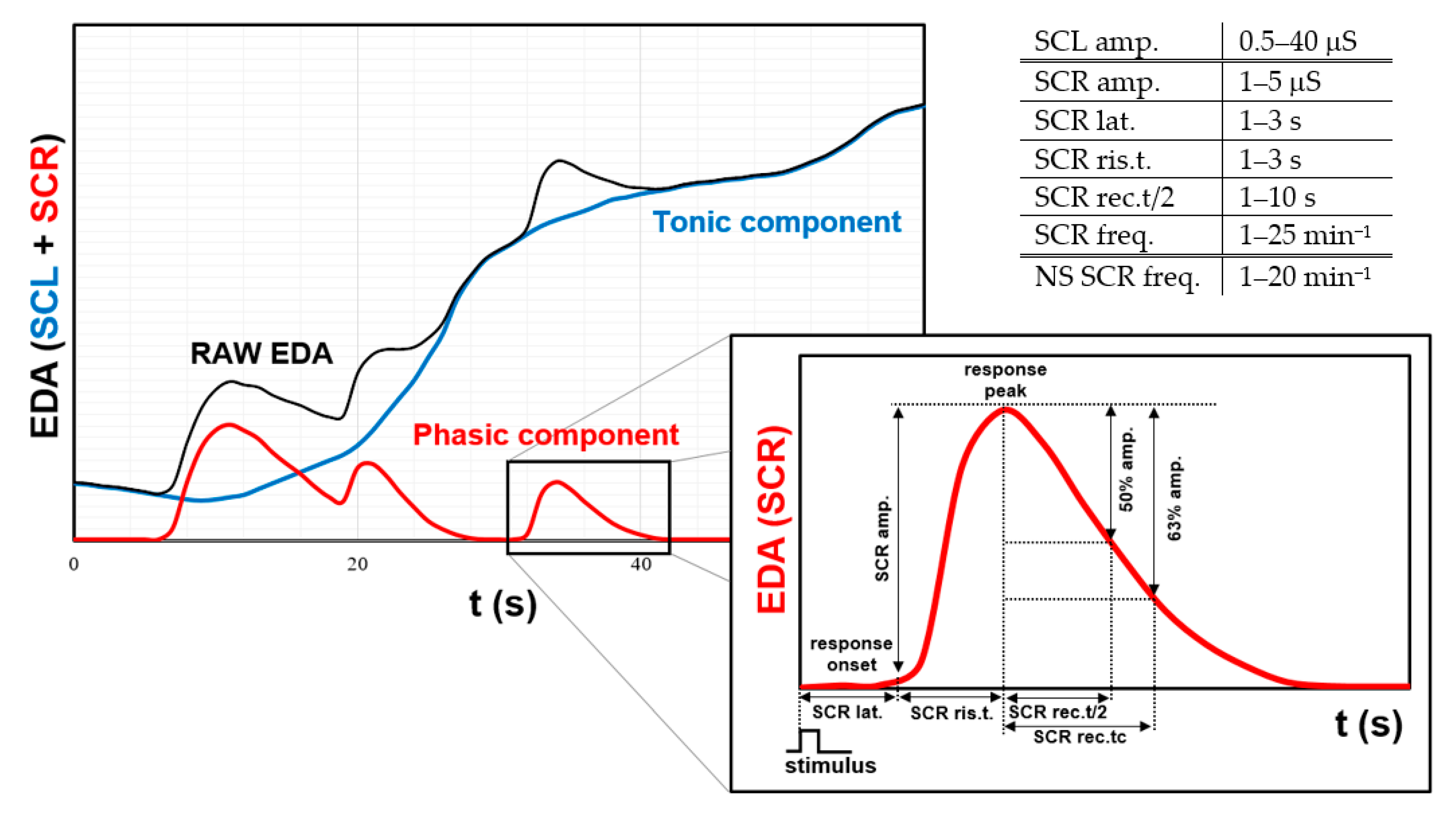
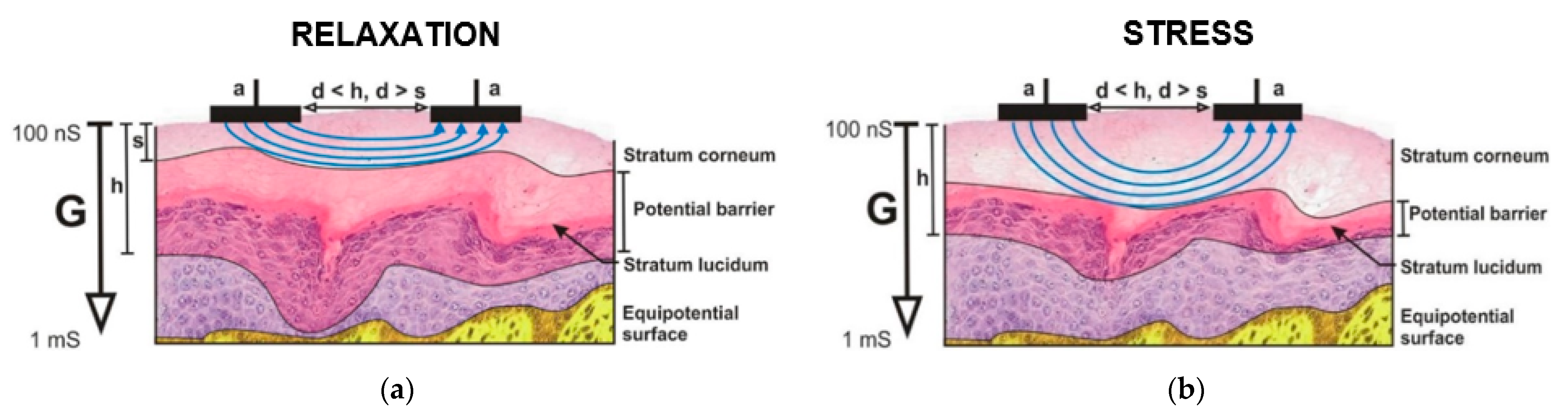
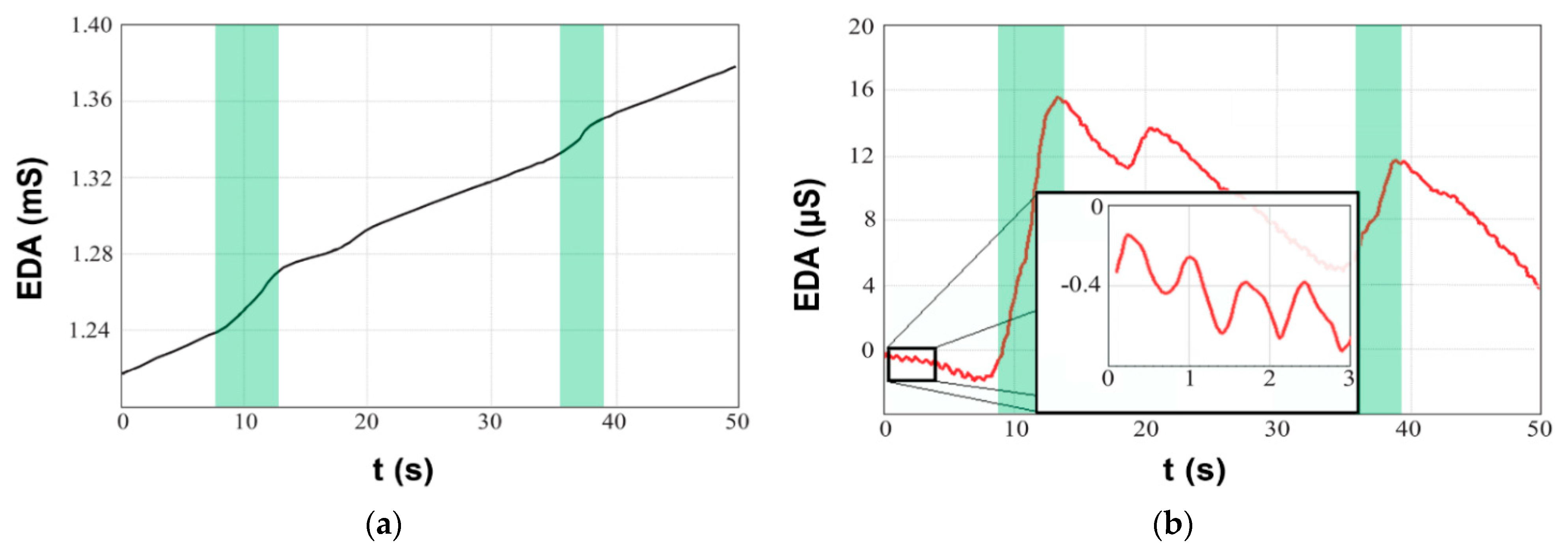
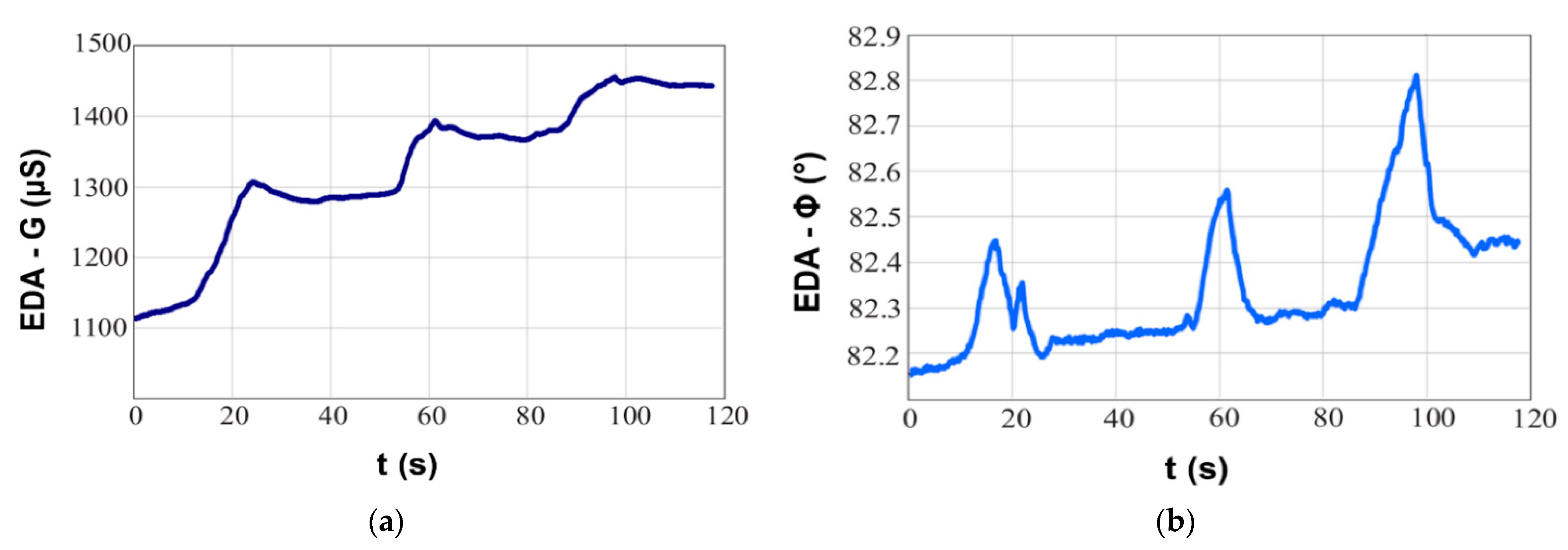
3.1. Electrodermal Activity
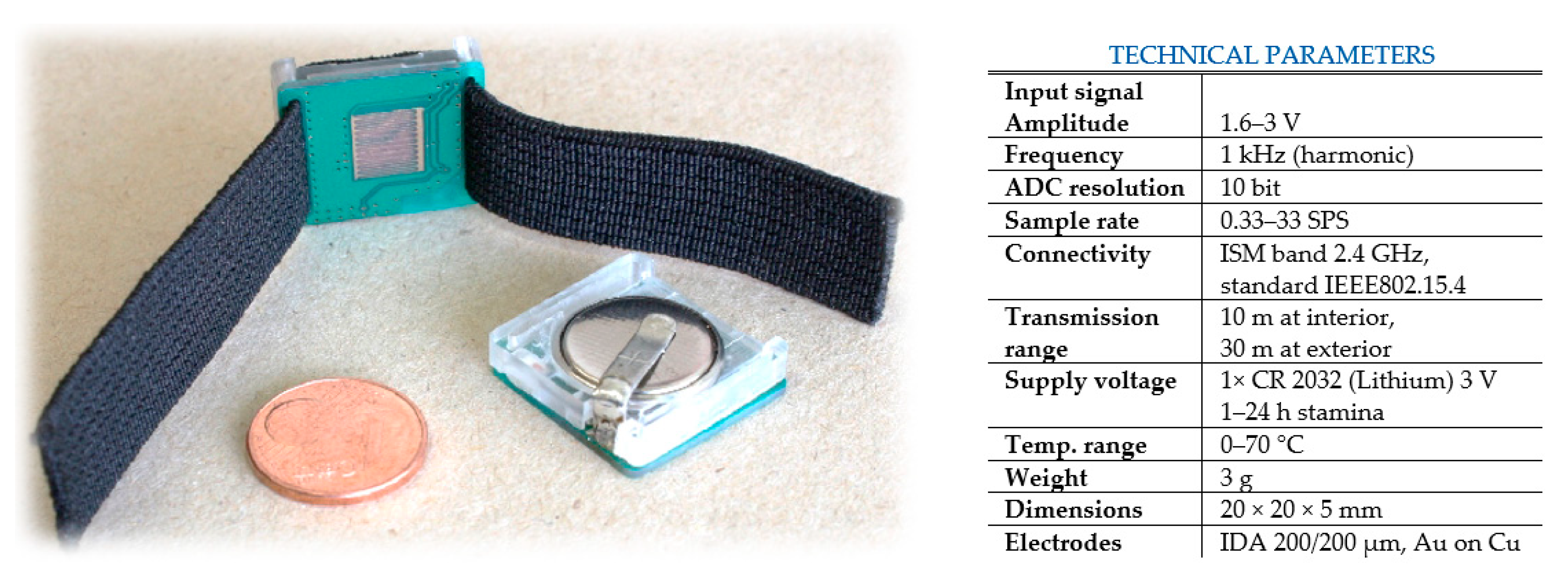
3.1.1. Optimization of EDA Measurements for Wearable Devices
3.1.2. Electrode Motion Artifacts
3.2. Heart Rate, Heart Rate Variability and Electrocardiography
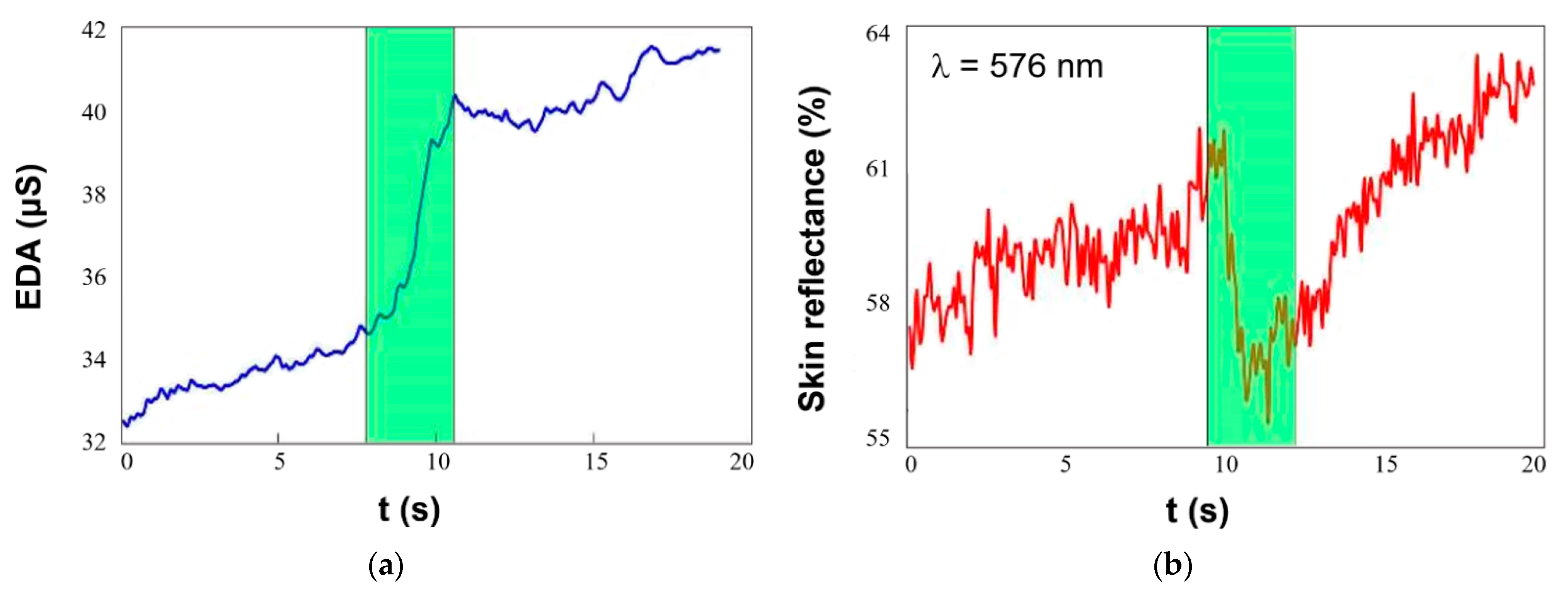
3.3. Circulatory Shock—Temperature and Skin Reflectance
3.4. Respiration
3.5. Blood Pressure
4. Advanced Wearable Stress-Meters
4.1. Multi-Sensor Monitors Overview
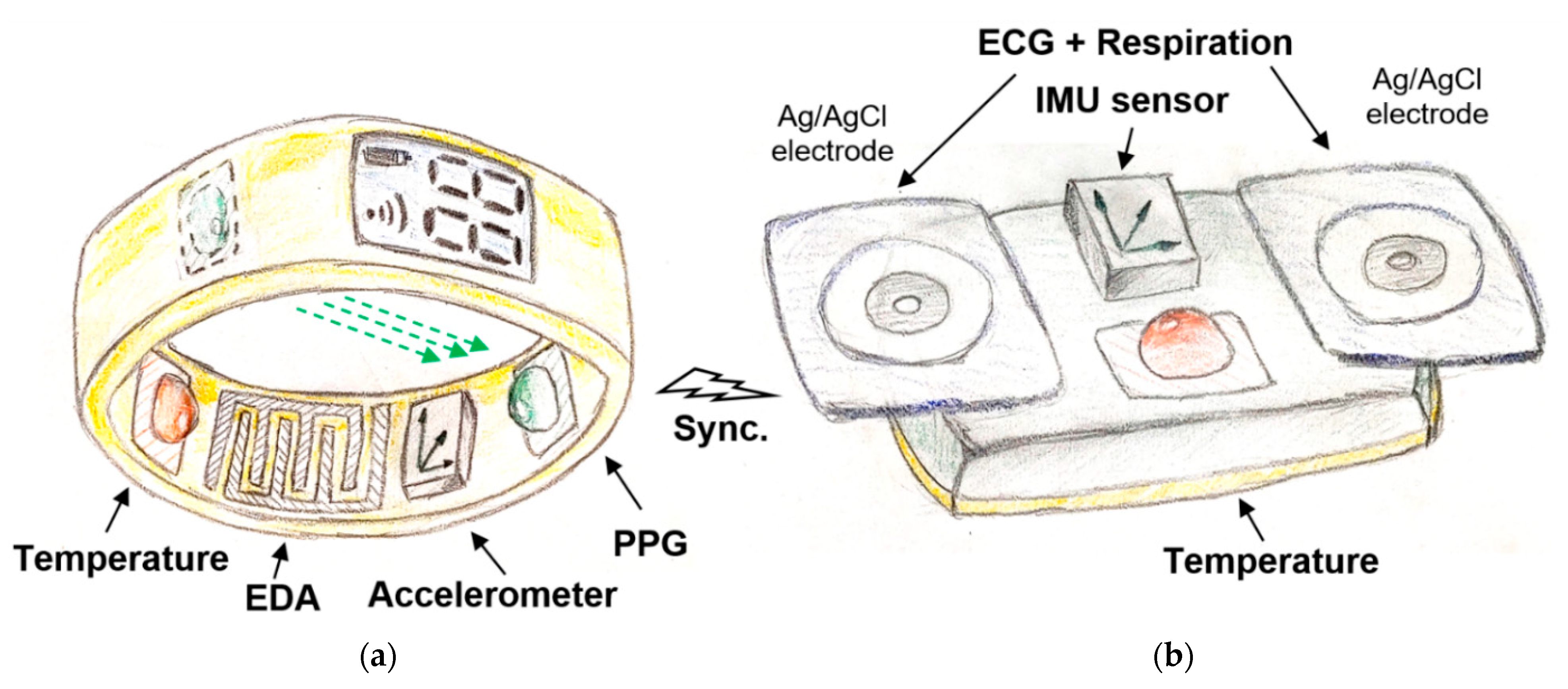
4.2. The Proposed Multi-Sensor Concept
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Bremner, J.D.; Moazzami, K.; Wittbrodt, M.T.; Nye, J.A.; Lima, B.B.; Gillespie, C.F.; Rapaport, M.H.; Pearce, B.D.; Shah, A.J.; Vaccarino, V. Diet, Stress and Mental Health. Nutrients 2020, 12, 2428. [Google Scholar] [CrossRef]
- Bitkina, O.V.; Kim, J.; Park, J.; Park, J.; Kim, H.K. Identifying traffic context using driving stress: A longitudinal preliminary case study. Sensors 2019, 19, 2152. [Google Scholar] [CrossRef] [Green Version]
- Burtscher, J.; Burtscher, M.; Millet, G.P. (Indoor) isolation, stress, and physical inactivity: Vicious circles accelerated by COVID-19? Scand. J. Med. Sci. Sport. 2020, 30, 1544–1545. [Google Scholar] [CrossRef] [PubMed]
- Shiota, S.; Nomura, M. Short-term stress enhances individuals’ adaptive behaviors: A near-infrared spectroscopy study. Neuroreport 2020, 31, 579–582. [Google Scholar] [CrossRef] [PubMed]
- Pakarinen, T.; Pietila, J.; Nieminen, H. Prediction of Self-Perceived Stress and Arousal Based on Electrodermal Activity. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 2191–2195. [Google Scholar]
- Fink, G. Stress: Definition and history. Encycl. Neurosci. 2009, 549–555. [Google Scholar] [CrossRef]
- Cooper, C.L.; Dewe, P. Stress: A Brief History; Blackwell Publishing Ltd.: Oxford, UK, 2008; ISBN 9780470774755. [Google Scholar]
- Robinson, A.M. Let’s talk about stress: History of stress research. Rev. Gen. Psychol. 2018, 22, 334–342. [Google Scholar] [CrossRef]
- Selye, H. The Stress of My Life; McGraw-Hill: New York, NY, USA, 1976; ISBN 9780070562080. [Google Scholar]
- Lupien, S.J.; Juster, R.P.; Raymond, C.; Marin, M.F. The effects of chronic stress on the human brain: From neurotoxicity, to vulnerability, to opportunity. Front. Neuroendocr. 2018, 49, 91–105. [Google Scholar] [CrossRef]
- Lupien, S.J.; Ouellet-Morin, I.; Hupbach, A.; Tu, M.T.; Buss, C.; Walker, D.; Pruessner, J.; McEwen, B.S. Beyond the Stress Concept: Allostatic Load-A Developmental Biological and Cognitive Perspective. Dev. Psychopathol. Second Ed. 2015, 2, 578–628. [Google Scholar]
- Soreq, H.; Friedman, A.; Kaufer, D. (Eds.) Stress—From Molecules to Behavior; Wiley: Hoboken, NJ, USA, 2009; ISBN 9783527323746. [Google Scholar]
- Rohleder, N. Stress and inflammation—The need to address the gap in the transition between acute and chronic stress effects. Psychoneuroendocrinology 2019, 105, 164–171. [Google Scholar] [CrossRef]
- Gabrys, R.L.; Howell, J.W.; Cebulski, S.F.; Anismana, H.; Matheson, K. Acute stressor effects on cognitive flexibility: Mediating role of stressor appraisals and cortisol. Stress 2019, 22, 182–189. [Google Scholar] [CrossRef]
- Nicolaides, N.C.; Kyratzi, E.; Lamprokostopoulou, A.; Chrousos, G.P.; Charmandari, E. Stress, the stress system and the role of glucocorticoids. Neuroimmunomodulation 2014, 22, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, S.S.; Kemeny, M.E. Acute stressors and cortisol responses: A theoretical integration and synthesis of laboratory research. Psychol. Bull. 2004, 130, 355–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dayas, C.V.; Buller, K.M.; Crane, J.W.; Xu, Y.; Day, T.A. Stressor categorization: Acute physical and psychological stressors elicit distinctive recruitment patterns in the amygdala and in medullary noradrenergic cell groups. Eur. J. Neurosci. 2001, 14, 1143–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, F.; Nilsson, M.; Jones, K. Acute and Chronic Stress-Induced Disturbances of Microglial Plasticity, Phenotype and Function. Curr. Drug Targets 2013, 14, 1262–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawyers, C.; Sheerin, C.; Eastman, M.; Burchett, J.; Howell, P.; Neigh, G.; Amstadter, A.B.; Hettema, J.; Roberson-Nay, R. Genetic and environmental influences on cortisol reactivity to a psychosocial stressor in adolescents and young adults. Psychoneuroendocrinology 2021, 127, 105195. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Asnaani, A.; Vonk, I.J.J.; Sawyer, A.T.; Fang, A. The efficacy of CBT: A review of meta-analyses. Cogn. Ther. Res. 2012, 36, 427–440. [Google Scholar] [CrossRef] [Green Version]
- Qin, H.Y.; Cheng, C.W.; Tang, X.D.; Bian, Z.X. Impact of psychological stress on irritable bowel syndrome. World J. Gastroenterol. 2014, 20, 14126–14131. [Google Scholar] [CrossRef]
- Ray, A.; Gulati, K.; Rai, N. Stress, Anxiety, and Immunomodulation: A Pharmacological Analysis, 1st ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2017; Volume 103. [Google Scholar]
- Zong, Y.; Zhu, S.; Zhang, S.; Zheng, G.; Wiley, J.W.; Hong, S. Chronic stress and intestinal permeability: Lubiprostone regulates glucocorticoid receptor-mediated changes in colon epithelial tight junction proteins, barrier function, and visceral pain in the rodent and human. Neurogastroenterol. Motil. 2019, 31, e13477. [Google Scholar] [CrossRef]
- Zefferino, R.; Di Gioia, S.; Conese, M. Molecular links between endocrine, nervous and immune system during chronic stress. Brain Behav. 2020, 1, e01960. [Google Scholar]
- Strike, P.C.; Steptoe, A. Psychosocial factors in the development of coronary artery disease. Prog. Cardiovasc. Dis. 2004, 46, 337–347. [Google Scholar] [CrossRef]
- Yao, B.C.; Meng, L.B.; Hao, M.L.; Zhang, Y.M.; Gong, T.; Guo, Z.G. Chronic stress: A critical risk factor for atherosclerosis. J. Int. Med. Res. 2019, 47, 1429–1440. [Google Scholar] [CrossRef]
- Fleshner, M. Physical activity and stress resistance: Sympathetic nervous system adaptations prevent stress-induced immunosuppression. Exerc. Sport Sci. Rev. 2005, 33, 120–126. [Google Scholar] [CrossRef]
- Cooper, C.L.; Williams, S.; Sloan, S.J. Occupational Stress Indicator Management Guide; Windsor NFER-Nelson: Berkshire, UK, 1988. [Google Scholar]
- Ironson, G. Work, job stress, and health. Front. Ind. Organ. Psychol. 1992, 5, 33–69. [Google Scholar]
- Sauter, S.L.; Murphy, L.R. Organizational Risk Factors for Job Stress; American Psychological Association: Washington, DC, USA, 1995; ISBN 1-557-98297. [Google Scholar]
- Landy, F.; Quick, J.C.; Kasl, S. Work, stress, and well-being. Int. J. Stress Manag. 1994, 1, 33–73. [Google Scholar] [CrossRef]
- Stanton, J.M.; Balzer, W.K.; Smith, P.C.; Parra, L.F.; Ironson, G. A general measure of work stress: The stress in general scale. Educ. Psychol. Meas. 2001, 61, 866–888. [Google Scholar] [CrossRef]
- Spijkerman, M.P.J.; Pots, W.T.M.; Bohlmeijer, E.T. Effectiveness of online mindfulness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clin. Psychol. Rev. 2016, 45, 102–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, L.; Xiao, J.F.; Agarwal, N.; Duex, J.E.; Theodorescu, D. Advances in bladder cancer biology and therapy. Nat. Rev. Cancer 2020, 21, 104–121. [Google Scholar] [CrossRef] [PubMed]
- Adamson, M.M.; Phillips, A.; Seenivasan, S.; Martinez, J.; Grewal, H.; Kang, X.; Coetzee, J.; Luttenbacher, I.; Jester, A.; Harris, O.A.; et al. International prevalence and correlates of psychological stress during the global COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9248. [Google Scholar] [CrossRef] [PubMed]
- The American Institute of Stress. Available online: https://www.stress.org/ (accessed on 4 May 2021).
- Stress Statistics. Available online: https://www.therecoveryvillage.com/mental-health/stress/related/stress-statistics/ (accessed on 4 May 2021).
- Here’s Why Workplace Stress Is Costing Employers $300 Billion a Year. Available online: https://www.businessinsider.com/how-stress-at-work-is-costing-employers-300-billion-a-year-2016-6 (accessed on 4 May 2021).
- Stress in America. Available online: https://www.apa.org/news/press/releases/stress/2020/report-october (accessed on 4 May 2021).
- Great Britain and Stress. Available online: https://www.forthwithlife.co.uk/blog/great-britain-and-stress/ (accessed on 4 May 2021).
- American Psychological Association. Available online: https://www.apa.org/news/press/releases/stress/2020/sia-mental-health-crisis.pdf (accessed on 4 May 2021).
- Jin, J.; Gao, B.; Yang, S.; Zhao, B.; Luo, L.; Woo, W.L. Attention-Block Deep Learning Based Features Fusion in Wearable Social Sensor for Mental Wellbeing Evaluations. IEEE Access 2020, 8, 89258–89268. [Google Scholar] [CrossRef]
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and health: Psychological, behavioral, and biological determinants. Annu. Rev. Clin. Psychol. 2005, 1, 607–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhabhar, F.S. The short-term stress response—Mother nature’s mechanism for enhancing protection and performance under conditions of threat, challenge, and opportunity. Front. Neuroendocr. 2018, 49, 175–192. [Google Scholar] [CrossRef] [PubMed]
- Larrosa, P.N.F.; Ojea, A.; Ojea, I.; Molina, V.A.; Zorrilla-Zubilete, M.A.; Delorenzi, A. Retrieval under stress decreases the long-term expression of a human declarative memory via reconsolidation. Neurobiol. Learn. Mem. 2017, 142, 135–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joëls, M. Corticosteroids and the brain. J. Endocrinol. 2018, 238, R121–R130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savage, B.M.; Lujan, H.L.; Thipparthi, R.R.; DiCarlo, S.E. Humor, laughter, learning, and health! A brief review. Adv. Physiol. Educ. 2017, 41, 341–347. [Google Scholar] [CrossRef] [Green Version]
- Jung, Y.H.; Jang, J.H.; Lee, D.; Choi, Y.; Choi, S.H.; Kang, D.H. Relationships Between Catecholamine Levels and Stress or Intelligence. Neurochem. Res. 2019, 44, 1192–1200. [Google Scholar] [CrossRef]
- Wickramasuriya, D.S.; Qi, C.; Faghih, R.T. A State-Space Approach for Detecting Stress from Electrodermal Activity. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; IEEE: Piscataway, NJ, USA, 2018; Volume 2018, pp. 3562–3567. [Google Scholar]
- Weissman, D.G.; Mendes, W.B. Correlation of sympathetic and parasympathetic nervous system activity during rest and acute stress tasks. Int. J. Psychophysiol. 2021, 162, 60–68. [Google Scholar] [CrossRef]
- Miyazaki, Y.; Ikei, H.; Song, C. Forest medicine research in Japan. Nihon Eiseigaku Zasshi 2014, 69, 122–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kudielka, B.M.; Wüst, S. Human models in acute and chronic stress: Assessing determinants of individual hypothalamuspituitaryadrenal axis activity and reactivity. Stress 2010, 13, 1–14. [Google Scholar] [CrossRef]
- De Looff, P.C.; Cornet, L.J.M.; Embregts, P.J.C.M.; Nijman, H.L.I.; Didden, H.C.M. Associations of sympathetic and parasympathetic activity in job stress and burnout: A systematic review. PLoS ONE 2018, 13, e0205741. [Google Scholar] [CrossRef] [PubMed]
- Nagai, Y.; Critchley, H.D.; Featherstone, E.; Trimble, M.R.; Dolan, R.J. Activity in ventromedial prefrontal cortex covaries with sympathetic skin conductance level: A physiological account of a “default mode” of brain function. Neuroimage 2004, 22, 243–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, S.; Gianaros, P.J.; Manuck, S.B. A Stage Model of Stress and Disease. Perspect. Psychol. Sci. 2016, 11, 456–463. [Google Scholar] [CrossRef]
- Van Puyvelde, M.; Neyt, X.; McGlone, F.; Pattyn, N. Voice stress analysis: A new framework for voice and effort in human performance. Front. Psychol. 2018, 9, 1–25. [Google Scholar] [CrossRef]
- Partila, P.; Tovarek, J.; Rozhon, J.; Jalowiczor, J. Human stress detection from the speech in danger situation. In Mobile Multimedia/Image Processing, Security, and Applications 2019; Agaian, S.S., DelMarco, S.P., Asari, V.K., Eds.; SPIE: Bellingham, WA, USA, 2019; p. 31. [Google Scholar]
- Tomba, K.; Dumoulin, J.; Mugellini, E.; Khaled, O.A.; Hawila, S. Stress detection through speech analysis. In Proceedings of the ICETE 2018—15th International Joint Conference on e-Business and Telecommunications, Porto, Portugal, 26–28 July 2018; Volume 1, pp. 394–398. [Google Scholar]
- Dhole, N.P.; Kale, S.N. Stress Detection in Speech Signal Using Machine Learning and AI. In Machine Learning and Information Processing; Springer: Singapore, 2020; pp. 11–26. [Google Scholar]
- Kurniawan, H.; Maslov, A.V.; Pechenizkiy, M. Stress detection from speech and Galvanic Skin Response signals. In Proceedings of the 26th IEEE International Symposium on Computer-Based Medical Systems, Porto, Portugal, 20–22 June 2013; IEEE: Piscataway, NJ, USA, 2013; pp. 209–214. [Google Scholar]
- Jiang, L.; Gao, B.; Gu, J.; Chen, Y.; Gao, Z.; Ma, X.; Kendrick, K.M.; Woo, W.L. Wearable Long-Term Social Sensing for Mental Wellbeing. IEEE Sens. J. 2019, 19, 8532–8542. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Gao, B.; Jiang, L.; Jin, J.; Gao, Z.; Ma, X.; Woo, W.L. IoT Structured Long-Term Wearable Social Sensing for Mental Wellbeing. IEEE Internet Things J. 2019, 6, 3652–3662. [Google Scholar] [CrossRef]
- Sevil, M.; Rashid, M.; Hajizadeh, I.; Askari, M.R.; Hobbs, N.; Brandt, R.; Park, M.; Quinn, L.; Cinar, A. Discrimination of simultaneous psychological and physical stressors using wristband biosignals. Comput. Methods Programs Biomed. 2021, 199, 105898. [Google Scholar] [CrossRef]
- Lamb, D.H. On the distinction between physical and psychological stressors. Motiv. Emot. 1979, 3, 51–61. [Google Scholar] [CrossRef]
- Matos, T.M.; De Souza-Talarico, J.N. How stress mediators can cumulatively contribute to Alzheimer’s disease An allostatic load approach. Dement. Neuropsychol. 2019, 13, 11–21. [Google Scholar] [CrossRef]
- Juster, R.-P.; Vencill, J.A.; Johnson, P.J. Impact of Stress and Strain on Current LGBT Health Disparities. In Trauma, Resilience, and Health Promotion in LGBT Patients; Springer International Publishing: Cham, Switzerland, 2017; pp. 35–48. ISBN 9783319545097. [Google Scholar]
- Giakoumis, D.; Tzovaras, D.; Hassapis, G. Subject-dependent biosignal features for increased accuracy in psychological stress detection. Int. J. Hum. Comput. Stud. 2013, 71, 425–439. [Google Scholar] [CrossRef]
- Nasiri Khoozani, E.; Hadzic, M. Designing the human stress ontology: A formal framework to capture and represent knowledge about human stress. Aust. Psychol. 2010, 45, 258–273. [Google Scholar] [CrossRef]
- Holmes, T.H.; Rahe, R.H. The social readjustment rating scale. J. Psychosom. Res. 1967, 11, 213–218. [Google Scholar] [CrossRef]
- Vavrinský, E.; Stopjaková, V.; Březina, I.; Tvarožek, V.; Majer, L.; Soláriková, P. Electro-optical monitoring of human cognitive processes. In Proceedings of the 2008 International Conference on Advanced Semiconductor Devices and Microsystems, Smolenice, Slovakia, 12–16 October 2008; pp. 279–282. [Google Scholar]
- Anusha, A.S.; Sukumaran, P.; Sarveswaran, V.; Surees Kumar, S.; Shyam, A.; Akl, T.J.; Preejith, S.P.; Sivaprakasam, M. Electrodermal Activity Based Pre-surgery Stress Detection Using a Wrist Wearable. IEEE J. Biomed. Health Inform. 2020, 24, 92–100. [Google Scholar]
- Majer, L.; Stopjaková, V.; Vavrinský, E. Wireless measurement system for non-invasive biomedical monitoring of psycho-physiological processes. J. Electr. Eng. 2009, 60, 57–68. [Google Scholar]
- Sheraton, M.; Deo, N.; Dutt, T.; Surani, S.; Hall-Flavin, D.; Kashyap, R. Psychological effects of the COVID 19 pandemic on healthcare workers globally: A systematic review. Psychiatry Res. 2020, 292, 113360. [Google Scholar] [CrossRef] [PubMed]
- Nappo, N. Job stress and interpersonal relationships cross country evidence from the EU15: A correlation analysis. BMC Public Health 2020, 20, 1143. [Google Scholar] [CrossRef] [PubMed]
- Martinsen, Ø.G.; Pabst, O.; Tronstad, C.; Grimnes, S. Sources of error in AC measurement of skin conductance. J. Electr. Bioimpedance 2019, 6, 49–53. [Google Scholar] [CrossRef] [Green Version]
- Zheng, D.; Chernyshov, G.; Kunze, K. Electrodermal activity sensing using smart eyewear. In Proceedings of the UbiComp/ISWC ’19—2019 ACM International Joint Conference on Pervasive and Ubiquitous Computing and Proceedings of the 2019 ACM International Symposium on Wearable Computers, London, UK, 9–13 September 2019; pp. 653–656. [Google Scholar]
- Poh, M.Z.; Swenson, N.C.; Picard, R.W. A wearable sensor for unobtrusive, long-term assessment of electrodermal activity. IEEE Trans. Biomed. Eng. 2010, 57, 1243–1252. [Google Scholar]
- Zontone, P.; Affanni, A.; Bernardini, R.; Del Linz, L.; Piras, A.; Rinaldo, R. Stress evaluation in simulated autonomous and manual driving through the analysis of skin potential response and electrocardiogram signals. Sensors 2020, 20, 2494. [Google Scholar] [CrossRef]
- Peternel, K.; Pogačnik, M.; Tavčar, R.; Kos, A. A presence-based context-aware chronic stress recognition system. Sensors 2012, 12, 15888–15906. [Google Scholar] [CrossRef]
- Kim, H.; Kwon, S.; Kwon, Y.T.; Yeo, W.H. Soft wireless bioelectronics and differential electrodermal activity for home sleep monitoring. Sensors 2021, 21, 354. [Google Scholar] [CrossRef]
- Posada-Quintero, H.F.; Chon, K.H. Innovations in Electrodermal Activity Data Collection and Signal Processing: A Systematic Review. Sensors 2020, 20, 479. [Google Scholar] [CrossRef] [Green Version]
- Caborni, C.; Regalia, G.; Onorati, F.; Picard, R.W. Clinical evaluation of the Embrace smart watch detection capability of generalized tonic-clonic seizures recorded at the ankles. In Proceedings of the American Epilepsy Society Annual Meeting, Baltimore, MD, USA, 6–10 December 2019. [Google Scholar]
- Posada-Quintero, H.F.; Florian, J.P.; Orjuela-Cañón, A.D.; Chon, K.H. Electrodermal activity is sensitive to cognitive stress under water. Front. Physiol. 2018, 8, 1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Du, S. Psychological stress level detection based on electrodermal activity. Behav. Brain Res. 2018, 341, 50–53. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Yuan, F.H.; Chen, T.; Huang, Q.; Wang, Y.; Liu, Z.G. ER stress-mediated cell damage contributes to the release of EDA+ fibronectin from hepatocytes in nonalcoholic fatty liver disease. J. Huazhong Univ. Sci. Technol. Med. Sci. 2017, 37, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Gigi, A.; Papirovitz, M. Association of anxiety awareness with risk factors of cognitive decline in MCI. Brain Sci. 2021, 11, 135. [Google Scholar] [CrossRef]
- Andreassi, J.L. Psychophysiology: Human Behavior & Physiological Response, 5th ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2007; ISBN 0-805849505. [Google Scholar]
- Braithwaite, J.J.J.; Derrick, D.; Watson, G.; Jones, R.; Rowe, M.; Watson, D.; Robert, J.; Mickey, R. A Guide for Analysing Electrodermal Activity (EDA) & Skin Conductance Responses (SCRs) for Psychological Experiments; BIOPAC Systems, Inc.: Goleta, CA, USA, 2013; pp. 1–42. [Google Scholar]
- Světlák, M.; Bob, P.; Roman, R.; Ježek, S.; Damborská, A.; Chládek, J.; Shaw, D.J.; Kukleta, M. Stress-induced alterations of left-right electrodermal activity coupling indexed by pointwise transinformation. Physiol. Res. 2013, 62, 711–719. [Google Scholar] [CrossRef]
- Tronstad, C.; Staal, O.M.; Saelid, S.; Martinsen, O.G. Model- based filtering for artifact and noise suppression with state estimation for electrodermal activity measurements in real time. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 2750–2753. [Google Scholar]
- Affanni, A.; Chiorboli, G.; Minen, D. Motion artifact removal in stress sensors used in driver in motion simulators. In Proceedings of the 2016 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Benevento, Italy, 15–18 May 2016. [Google Scholar]
- Figner, B.; Murphy, R.O. Using skin conductance in judgment and decision making research. In A Handbook of Process Tracing Methods for Decision Research: A Critical Review and User’s Guide; Schulte-Mecklenbeck, M., Kühberger, A., Ranyard, R., Eds.; Psychology Press: East Sussex, UK, 2011; pp. 163–184. [Google Scholar]
- Dawson, M.E.; Schell, A.M.; Filion, D.L. The electrodermal system. In Handbook of Psychophysiology (Cambridge Handbooks in Psychology; Cambridge University Press: Cambridge, UK, 2016; pp. 217–243. [Google Scholar]
- Grimnes, S.; Jabbari, A.; Martinsen, Ø.G.; Tronstad, C. Electrodermal activity by DC potential and AC conductance measured simultaneously at the same skin site. Skin Res. Technol. 2011, 17, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Affanni, A.; Chiorboli, G. Design and characterization of a real-time, wearable, endosomatic electrodermal system. Meas. J. Int. Meas. Confed. 2015, 75, 111–121. [Google Scholar] [CrossRef]
- Greco, A.; Lanata, A.; Citi, L.; Vanello, N.; Valenza, G.; Scilingo, E.P. Skin admittance measurement for emotion recognition: A study over frequency sweep. Electronics 2016, 5, 46. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.; Sun, S. A systematic exploration of deep neural networks for EDA-based emotion recognition. Information 2020, 11, 212. [Google Scholar] [CrossRef] [Green Version]
- Kelsey, M.; Palumbo, R.V.; Urbaneja, A.; Akcakaya, M.; Huang, J.; Kleckner, I.R.; Barrett, L.F.; Quigley, K.S.; Sejdic, E.; Goodwin, M.S. Artifact detection in electrodermal activity using sparse recovery. In Compressive Sensing VI: From Diverse Modalities to Big Data Analytics. International Society for Optics and Photonics; SPIE: Bellingham, WA, USA, 2017; Volume 10211, p. 102110D. [Google Scholar]
- Dawson, M.E.; Schell, A.M.; Filion, D.L. The Electrodermal System. In Handbook of Psychophysiology; Cambridge University Press: Boston, MA, USA, 1993; pp. 217–243. [Google Scholar]
- Silva Moreira, P.; Chaves, P.; Dias, R.; Dias, N.; Almeida, P.R. Validation of Wireless Sensors for Psychophysiological Studies. Sensors 2019, 19, 4824. [Google Scholar] [CrossRef] [Green Version]
- Benedek, M.; Kaernbach, C. A continuous measure of phasic electrodermal activity. J. Neurosci. Methods 2010, 190, 80–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, D.P.; Bai, O.; Gorgey, A.S.; Fox, J.; Lovegreen, W.T.; Burkhardt, B.W.; Atri, R.; Marquez, J.S.; Li, Q.; Fei, D.Y. Electroencephalogram-based brain-computer interface and lower-limb prosthesis control: A case study. Front. Neurol. 2017, 8, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowles, D.C.; Christie, M.J.; Edelberg, R.; GRINGS, W.W.; Lykken, D.T.; Venables, P.H. Publication recommendations for electrodermal measurements. Psychophysiology 2012, 49, 1017–1034. [Google Scholar] [CrossRef] [PubMed]
- Leiner, D.; Fahr, A.; Früh, H. EDA Positive Change: A Simple Algorithm for Electrodermal Activity to Measure General Audience Arousal During Media Exposure. Commun. Methods Meas. 2012, 6, 237–250. [Google Scholar] [CrossRef]
- Al Machot, F.; Elmachot, A.; Ali, M.; Al Machot, E.; Kyamakya, K. A deep-learning model for subject-independent human emotion recognition using electrodermal activity sensors. Sensors 2019, 19, 1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddad, P.A.; Servati, A.; Soltanian, S.; Ko, F.; Servati, P. Breathable dry silver/silver chloride electronic textile electrodes for electrodermal activity monitoring. Biosensors 2018, 8, 79. [Google Scholar] [CrossRef] [Green Version]
- Litscher, G.; Litscher, D.; Ofner, M.; Gaischek, I.; Malliga, D.-E. RegentK and Physiotherapy—Electrodermal Mapping. Medicines 2014, 1, 22–31. [Google Scholar] [CrossRef] [Green Version]
- Affanni, A. Wireless Sensors System for Stress Detection by Means of ECG and EDA Acquisition. Sensors 2020, 20, 2026. [Google Scholar] [CrossRef] [Green Version]
- Laborde, S.; Mosley, E.; Thayer, J.F. Heart rate variability and cardiac vagal tone in psychophysiological research—Recommendations for experiment planning, data analysis, and data reporting. Front. Psychol. 2017, 8, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weis, M.; Danilla, T.; Matay, L.; Hrkút, P.; Kákoš, J. Noninvasive Biomedical Sensor s on the Biology—Interface of Human Skin. In Proceedings of the 7th International IMECO TC-13 Conference on Measurement in Clinical Medicine: Model Based Biomeasurement, Stará Lesná, Slovakia, 6–9 September 1995; pp. 89–91. [Google Scholar]
- Ivanic, R.; Novotny, I.; Rehacek, V.; Tvarozek, V.; Weis, M. Thin film non-symmetric microelectrode array for impedance monitoring of human skin. Thin Solid Film. 2003, 433, 332–336. [Google Scholar] [CrossRef]
- Matsui, T.; Amagai, M. Dissecting the formation, structure and barrier function of the stratum corneum. Int. Immunol. 2015, 27, 269–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osseiran, S.; Cruz, J.D.; Jeong, S.; Wang, H.; Fthenakis, C.; Evans, C.L. Characterizing stratum corneum structure, barrier function, and chemical content of human skin with coherent Raman scattering imaging. Biomed. Opt. Express 2018, 9, 6425. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Lyga, J. Brain-skin connection: Stress, inflammation and skin aging. Inflamm. Allergy Drug Targets 2014, 13, 177–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altemus, M.; Rao, B.; Dhabhar, F.S.; Ding, W.; Granstein, R.D. Stress-induced changes in skin barrier function in healthy women. J. Investig. Dermatol. 2001, 117, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Vavrinsky, E.; Stopjakova, V.; Brezina, I.; Majer, L.; Solarikova, P.; Tvarozek, V. Electro-Optical Monitoring and Analysis of Human Cognitive Processes. In Semiconductor Technologies; InTech: London, UK, 2010; pp. 465–490. ISBN 978-953-307-080-3. [Google Scholar]
- Shukla, J.; Barreda-Ángeles, M.; Oliver, J.; Puig, D. Efficient wavelet-based artifact removal for electrodermal activity in real-world applications. Biomed. Signal Process. Control 2018, 42, 45–52. [Google Scholar] [CrossRef]
- Zdimalova, M.; Roznovjak, R.; Weismann, P.; El Falougy, H.; Kubikova, E. Use of graph algorithms in the processing and analysis of images with focus on the biomedical data. Bratisl. Med. J. 2017, 118, 485–490. [Google Scholar] [CrossRef]
- Zhang, Y.; Haghdan, M.; Xu, K.S. Unsupervised motion artifact detection in wrist-measured electrodermal activity data. In Proceedings of the 2017 ACM International Symposium on Wearable Computers, Maui, HI, USA, 11–15 September 2017; pp. 54–57. [Google Scholar]
- Chen, W.; Jaques, N.; Taylor, S.; Sano, A.; Fedor, S.; Picard, R.W. Wavelet-based motion artifact removal for electrodermal activity. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; IEEE: Piscataway, NJ, USA, 2015; Volume 176, pp. 6223–6226. [Google Scholar]
- Westeyn, T.; Presti, P.; Starner, T. ActionGSR: A combination galvanic skin response-accelerometer for physiological measurements in active environments. In Proceedings of the 2006 10th IEEE International Symposium on Wearable Computers, Montreux, Switzerland, 11–14 October 2006; pp. 129–130. [Google Scholar]
- Kenneally, G.; De, A.; Koditschek, D.E. Design Principles for a Family of Direct-Drive Legged Robots. IEEE Robot. Autom. Lett. 2016, 1, 900–907. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Chung, H.; Kim, J.W.; Lee, J. Motion Artifact Identification and Removal from Wearable Reflectance Photoplethysmography Using Piezoelectric Transducer. IEEE Sens. J. 2019, 19, 3861–3870. [Google Scholar] [CrossRef]
- Passler, S.; Müller, N.; Senner, V. In-Ear Pulse Rate Measurement: A Valid Alternative to Heart Rate Derived from Electrocardiography? Sensors 2019, 19, 3641. [Google Scholar] [CrossRef] [Green Version]
- Ernst, G. Heart-Rate Variability—More than Heart Beats? Front. Public Health 2017, 5, 240. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhoja, R.; Guttman, O.T.; Fox, A.A.; Melikman, E.; Kosemund, M.; Gingrich, K.J. Psychophysiological Stress Indicators of Heart Rate Variability and Electrodermal Activity with Application in Healthcare Simulation Research. Simul. Healthc. J. Soc. Simul. Healthc. 2020, 15, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.; Sundaram, S.; Kadish, A.H.; Goldberger, J.J. Autonomic effects on the spectral analysis of heart rate variability after exercise. Am. J. Physiol. Heart Circ. Physiol. 2009, 297, 1421–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schubert, C.; Lambertz, M.; Nelesen, R.A.; Bardwell, W.; Choi, J.B.; Dimsdale, J.E. Effects of stress on heart rate complexity-A comparison between short-term and chronic stress. Biol. Psychol. 2009, 80, 325–332. [Google Scholar] [CrossRef] [Green Version]
- Von Rosenberg, W.; Chanwimalueang, T.; Adjei, T.; Jaffer, U.; Goverdovsky, V.; Mandic, D.P. Resolving Ambiguities in the LF/HF Ratio: LF-HF Scatter Plots for the Categorization of Mental and Physical Stress from HRV. Front. Physiol. 2017, 8, 360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, S.-Y.; Lee, M.; Park, H.; Youn, I. Stress Resilience Measurement with Heart-Rate Variability During Mental And Physical Stress. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 5290–5293. [Google Scholar]
- Janet, M.T.; Cassio, L.; Richard, M.G. Chronic Stress and the Heart. JAMA 2007, 298, 8724. [Google Scholar]
- Kim, H.G.; Cheon, E.J.; Bai, D.S.; Lee, Y.H.; Koo, B.H. Stress and heart rate variability: A meta-analysis and review of the literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef] [Green Version]
- Baevsky, R.M.; Chernikova, A.G. Heart rate variability analysis: Physiological foundations and main methods. Cardiometry 2017, 66–76. [Google Scholar] [CrossRef] [Green Version]
- HRV in Evaluating ANS Function. Available online: https://www.kubios.com/hrv-ans-function/ (accessed on 2 May 2021).
- Sahoo, T.K.; Mahapatra, A.; Ruban, N. Stress Index Calculation and Analysis based on Heart Rate Variability of ECG Signal with Arrhythmia. In Proceedings of the 2019 Innovations in Power and Advanced Computing Technologies (i-PACT), Vellore, India, 22–23 March 2019; pp. 1–7. [Google Scholar]
- O’Neal, W.T.; Hammadah, M.; Sandesara, P.B.; Almuwaqqat, Z.; Samman-Tahhan, A.; Gafeer, M.M.; Abdelhadi, N.; Wilmot, K.; Al Mheid, I.; Bremner, D.J.; et al. The association between acute mental stress and abnormal left atrial electrophysiology. J. Cardiovasc. Electrophysiol. 2017, 28, 1151–1157. [Google Scholar] [CrossRef]
- Elsayed, Y.M.H. An electrocardiographic anxiety- induced quadrigeminy and re-assurance. Egypt. J. Crit. Care Med. 2018, 6, 21–23. [Google Scholar] [CrossRef]
- Lampert, R. ECG signatures of psychological stress. J. Electrocardiol. 2015, 48, 1000–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Napp, L.C.; Bauersachs, J. Takotsubo syndrome: Between evidence, myths, and misunderstandings. Herz 2020, 45, 252–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vavrinsky, E.; Subjak, J.; Donoval, M.; Wagner, A.; Zavodnik, T.; Svobodova, H. Application of Modern Multi-Sensor Holter in Diagnosis and Treatment. Sensors 2020, 20, 2663. [Google Scholar] [CrossRef] [PubMed]
- Vinkers, C.H.; Penning, R.; Hellhammer, J.; Verster, J.C.; Klaessens, J.H.G.M.; Olivier, B.; Kalkman, C.J. The effect of stress on core and peripheral body temperature in humans. Stress 2013, 16, 520–530. [Google Scholar] [CrossRef]
- Greaney, J.L.; Kenney, W.L.; Alexander, L.M. Sympathetic regulation during thermal stress in human aging and disease. Auton. Neurosci. 2016, 196, 81–90. [Google Scholar] [CrossRef] [Green Version]
- Oka, T. Stress-Induced Hyperthermia and Hypothermia, 1st ed.; Elsevier B.V.: Amsterdam, The Netherlands, 2018; Volume 157, ISBN 9780444640741. [Google Scholar]
- Cho, D.; Ham, J.; Oh, J.; Park, J.; Kim, S.; Lee, N.K.; Lee, B. Detection of stress levels from biosignals measured in virtual reality environments using a kernel-based extreme learning machine. Sensors 2017, 17, 2435. [Google Scholar] [CrossRef]
- Lin, H.P.; Lin, H.Y.; Lin, W.L.; Huang, A.C.W. Effects of stress, depression, and their interaction on heart rate, skin conductance, finger temperature, and respiratory rate: Sympathetic-parasympathetic hypothesis of stress and depression. J. Clin. Psychol. 2011, 67, 1080–1091. [Google Scholar] [CrossRef]
- Vila, G.; Godin, C.; Sakri, O.; Labyt, E.; Vidal, A.; Charbonnier, S.; Ollander, S.; Campagne, A. Real-time monitoring of passenger’s psychological stress. Future Internet 2019, 11, 102. [Google Scholar] [CrossRef] [Green Version]
- Zhai, J.; Barreto, A. Stress detection in computer users through non-invasive monitoring of physiological signals. Biomed. Sci. Instrum. 2006, 42, 495–500. [Google Scholar]
- Herborn, K.A.; Graves, J.L.; Jerem, P.; Evans, N.P.; Nager, R.; McCafferty, D.J.; McKeegan, D.E.F. Skin temperature reveals the intensity of acute stress. Physiol. Behav. 2015, 152, 225–230. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Abbod, M.; Shieh, J.S. Pain and stress detection using wearable sensors and devices—A review. Sensors 2021, 21, 1030. [Google Scholar] [CrossRef]
- Oka, T. Psychogenic fever: How psychological stress affects body temperature in the clinical population. Temperature 2015, 2, 368–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkawaz, M.H.; Mohamad, D.; Saba, T.; Basori, A.H.; Rehman, A. The Correlation Between Blood Oxygenation Effects and Human Emotion Towards Facial Skin Colour of Virtual Human. 3D Res. 2015, 6, 1–16. [Google Scholar] [CrossRef]
- Ziegler, M.G.; Ruiz-Ramon, P.; Shapiro, M.H. Abnormal stress responses in patients with diseases affecting the sympathetic nervous system. Psychosom. Med. 1993, 55, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Marazziti, D.; Di Muro, A.; Castrogiovanni, P. Psychological stress and body temperature changes in humans. Physiol. Behav. 1992, 52, 393–395. [Google Scholar] [CrossRef]
- Vincent, J.; De Backer, D. Circulatory Shock. N. Engl. J. Med. 2013, 369, 1726–1734. [Google Scholar] [CrossRef] [Green Version]
- Valdés, A.A. Measurement of Acute Psychological Stress; Universitat Autònoma de Barcelona: Barcelona, Spain, 2017. [Google Scholar]
- Tvarozek, V.; Reznicek, Z.; Jakubec, A.; Novotny, I. Asymmetric ratio sensors of nonelectric quantities. In Proceedings of the 2002 23rd International Conference on Microelectronics. Proceedings (Cat. No.02TH8595), Nis, Yugoslavia, 12–15 May 2002; IEEE: Piscataway, NJ, USA, 2002; Volume 1, pp. 219–222. [Google Scholar]
- Tsai, H.Y.; Huang, K.C.; Chang, H.C.; Yeh, J.L.A.; Chang, C.H. A noncontact skin oxygen-saturation imaging system for measuring human tissue oxygen saturation. IEEE Trans. Instrum. Meas. 2014, 63, 2620–2631. [Google Scholar] [CrossRef]
- Nitzan, M.; Romem, A.; Koppel, R. Pulse oximetry: Fundamentals and technology update. Med. Devices Evid. Res. 2014, 7, 231–239. [Google Scholar] [CrossRef]
- Torp, K.D.; Modi, P.; Simon, L.V. Pulse Oximetry. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470348/ (accessed on 2 May 2021).
- May, J.M.; Phillips, J.P.; Fitchat, T.; Ramaswamy, S.; Snidvongs, S.; Kyriacou, P.A. A novel photoplethysmography sensor for vital signs monitoring from the human trachea. Biosensors 2019, 9, 119. [Google Scholar] [CrossRef] [Green Version]
- Miyake, S.; Wada-Takahashi, S.; Honda, H.; Takahashi, S.S.; Sasaguri, K.; Sato, S.; Lee, M.C. Il Stress and chewing affect blood flow and oxygen levels in the rat brain. Arch. Oral Biol. 2012, 57, 1491–1497. [Google Scholar] [CrossRef]
- Crestani, C.C. Emotional stress and cardiovascular complications in animal models: A review of the influence of stress type. Front. Physiol. 2016, 7, 251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Standl, T.; Annecke, T.; Cascorbi, I.; Heller, A.R.; Sabashnikov, A.; Teske, W. Nomenklatur, Definition und Differenzierung der Schockformen. Dtsch. Arztebl. Int. 2018, 115, 757–767. [Google Scholar]
- Yoo, T.K.; Lee, J.Y.; Sung, K.C.; Oh, S.S.; Song, Y.S.; Lee, S.J.; Ko, K.J. Stress-induced cardiomyopathy presenting as shock. J. Cardiovasc. Ultrasound 2016, 24, 79–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernando, A.; Lázaro, J.; Gil, E.; Arza, A.; Garzón, J.M.; López-Antón, R.; De La Camara, C.; Laguna, P.; Aguiló, J.; Bailón, R. Inclusion of Respiratory Frequency Information in Heart Rate Variability Analysis for Stress Assessment. IEEE J. Biomed. Health Inform. 2016, 20, 1016–1025. [Google Scholar] [CrossRef]
- Masaoka, Y.; Homma, I. Anxiety and respiratory patterns: Their relationship during mental stress and physical load. Int. J. Psychophysiol. 1997, 27, 153–159. [Google Scholar] [CrossRef]
- Kato, A.; Takahashi, K.; Homma, I. Relationships between trait and respiratory parameters during quiet breathing in normal subjects. J. Physiol. Sci. 2018, 68, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Widjaja, D.; Orini, M.; Vlemincx, E.; Van Huffel, S. Cardiorespiratory dynamic response to mental stress: A multivariate time-frequency analysis. Comput. Math. Methods Med. 2013, 2013, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Tipton, M.J.; Harper, A.; Paton, J.F.R.; Costello, J.T. The human ventilatory response to stress: Rate or depth? J. Physiol. 2017, 595, 5729–5752. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S. Protective and damaging effects of stress mediators: Central role of the brain. Dialogues Clin. Neurosci. 2006, 8, 367–381. [Google Scholar]
- Spruill, T. Chronic Psychological Stress and Hypertension. Curr. Hypertens. Rep. 2013, 12, 10–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulkarni, S.; O’Farrell, I.; Erasi, M.; Kochar, M.S. Stress and hypertension. WMJ 1998, 97, 34–38. [Google Scholar] [PubMed]
- Hosanee, M.; Chan, G.; Welykholowa, K.; Cooper, R.; Kyriacou, P.A.; Zheng, D.; Allen, J.; Abbott, D.; Menon, C.; Lovell, N.H.; et al. Cuffless Single-Site Photoplethysmography for Blood Pressure Monitoring. J. Clin. Med. 2020, 9, 723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, G.-R.; Jung, D.-K.; Kim, G.-R.; Shin, B.-J. The Development of Integrated Sensor System for Measuring Simultaneously ECG, PPG and PPW. J. Korea Acad. Coop. Soc. 2009, 10, 992–999. [Google Scholar]
- Yoon, Y.; Cho, J.H.; Yoon, G. Non-constrained blood pressure monitoring using ECG and PPG for personal healthcare. J. Med. Syst. 2009, 33, 261–266. [Google Scholar] [CrossRef]
- Liu, W.; Fang, X.; Chen, Q.; Li, Y.; Li, T. Reliability analysis of an integrated device of ECG, PPG and pressure pulse wave for cardiovascular disease. Microelectron. Reliab. 2018, 87, 183–187. [Google Scholar] [CrossRef]
- Shin, W.; Cha, Y.D.; Yoon, G. ECG/PPG integer signal processing for a ubiquitous health monitoring system. J. Med. Syst. 2010, 34, 891–898. [Google Scholar] [CrossRef]
- Vavrinsky, E.; Solarikova, P.; Stopjakova, V.; Tvarozek, V.; Brezi, I. Implementation of Microsensor Interface for Biomonitoring of Human Cognitive Processes. In Biomedical Engineering, Trends in Electronics, Communications and Software; IntechOpen: London, UK, 2011. [Google Scholar]
- Ren, P.; Barreto, A.; Huang, J.; Gao, Y.; Ortega, F.R.; Adjouadi, M. Off-line and on-line stress detection through processing of the pupil diameter signal. Ann. Biomed. Eng. 2014, 42, 162–176. [Google Scholar] [CrossRef]
- De Santos Sierra, A.; Sánchez Ávila, C.; Guerra Casanova, J.; Bailador Del Pozo, G. A stress-detection system based on physiological signals and fuzzy logic. IEEE Trans. Ind. Electron. 2011, 58, 4857–4865. [Google Scholar] [CrossRef] [Green Version]
- van den Broek, E.L. Affective Signal Processing (ASP): Unraveling the mystery of emotions, by Egon, L. van den Broek. J. Ambient Intell. Smart Environ. 2012, 4, 67–69. [Google Scholar]
- Lee, J.; Yoo, S.K. Design of user-customized negative emotion classifier based on feature selection using physiological signal sensors. Sensors 2018, 18, 4253. [Google Scholar] [CrossRef] [Green Version]
- Pinto, G.; Carvalho, J.M.; Barros, F.; Soares, S.C.; Pinho, A.J.; Brás, S. Multimodal emotion evaluation: A physiological model for cost-effective emotion classification. Sensors 2020, 20, 3515. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Lee, T.; Yang, T.; Yoon, C.; Kim, S.P. Detection of drivers’ anxiety invoked by driving situations using multimodal biosignals. Processes 2020, 8, 155. [Google Scholar] [CrossRef] [Green Version]
- Posada-Quintero, H.F.; Bolkhovsky, J.B. Machine learning models for the identification of cognitive tasks using autonomic reactions from heart rate variability and electrodermal activity. Behav. Sci. 2019, 9, 45. [Google Scholar] [CrossRef] [Green Version]
- Jimenez-Molina, A.; Retamal, C.; Lira, H. Using psychophysiological sensors to assess mental workload during web browsing. Sensors 2018, 18, 458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hui, T.K.L.; Sherratt, R.S. Coverage of emotion recognition for common wearable biosensors. Biosensors 2018, 8, 30. [Google Scholar]
- Whoop. Available online: https://www.whoop.com/ (accessed on 4 May 2021).
- Garmin. Available online: www.garmin.com (accessed on 4 May 2021).
- Galaxy Watch Active2. Available online: https://www.samsung.com/uk/watches/galaxy-watch-active/galaxy-watch-active2-44mm-pink-sm-r820nzdabtu/ (accessed on 4 May 2021).
- Apple Watch. Available online: www.apple.com (accessed on 4 May 2021).
- Fossil. Available online: https://www.fossil.com/en-us/smartwatches/learn-more/sport/ (accessed on 4 May 2021).
- Fitbit. Available online: https://www.fitbit.com/global/us/technology/stress (accessed on 4 May 2021).
- Fitbit Smartwatches. Available online: https://www.fitbit.com/global/us/products/smartwatches/sense (accessed on 4 May 2021).
- Scanwatch. Available online: https://www.withings.com/us/en/scanwatch (accessed on 4 May 2021).
- Martin, N.; Mathieu, N.; Pallamin, N.; Ragot, M.; Diverrez, J.-M. Virtual reality sickness detection: An approach based on physiological signals and machine learning. In Proceedings of the 2020 IEEE International Symposium on Mixed and Augmented Reality (ISMAR), Porto de Galinhas, Brazil, 9–13 November 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 387–399. [Google Scholar]
- Romaniszyn-Kania, P.; Pollak, A.; Danch-Wierzchowska, M.; Kania, D.; Myśliwiec, A.P.; Piętka, E.; Mitas, A.W. Hybrid system of emotion evaluation in physiotherapeutic procedures. Sensors 2020, 20, 6343. [Google Scholar] [CrossRef] [PubMed]
- Empatica. Available online: www.empatica.com (accessed on 2 May 2021).
- SIMBAND. Available online: https://www.simband.io/documentation/simband-documentation/ (accessed on 4 May 2021).
- Ouraring HERITAGE—SILVER. Available online: https://ouraring.com/product/heritage-silver/step1 (accessed on 4 May 2021).
- Zephyranywhere. Available online: https://www.zephyranywhere.com/system/components (accessed on 4 May 2021).
- QARDIO. Available online: https://www.getqardio.com/qardiocore-wearable-ecg-ekg-monitor-iphone/ (accessed on 4 May 2021).
- Philips: Wearable Biosensor. Available online: https://www.usa.philips.com/healthcare/product/HC989803196871/wearable-biosensor-wireless-remote-sensing-device?origin=2_us_en_5370367_Skimlinks_12056403_mixedtype_cj&utm_medium=affiliate&utm_campaign=partnerize&utm_content=Skimlinks&utm_term=12056403&cjevent=b941764894ae11eb803d01a80a180511 (accessed on 5 May 2021).
- Mindtecstore NeuroSky-Brainwave. Available online: https://www.mindtecstore.com/NeuroSky-Brainwave-Starter-Kit-EEG-Headset?gclid=Cj0KCQjw1a6EBhC0ARIsAOiTkrGGtBquNJ_OGnNpF0hgOT57wQwlwr7-q3OV0AirSC1pHbV9dJNBc9QaAhF2EALw_wcB (accessed on 4 May 2021).
- Muse-2. Available online: https://choosemuse.com/muse-2/ (accessed on 4 May 2021).
- Flowtime. Available online: https://www.kickstarter.com/projects/987756376/flowtime-biosensing-meditation-headband (accessed on 4 May 2021).
- Spirehealth. Available online: www.spirehealth.com (accessed on 4 May 2021).
- Mohino-Herranz, I.; Gil-Pita, R.; Rosa-Zurera, M.; Seoane, F. Activity recognition using wearable physiological measurements: Selection of features from a comprehensive literature study. Sensors 2019, 19, 5524. [Google Scholar] [CrossRef] [Green Version]
- Slavich, G.M.; Taylor, S.; Picard, R.W. Stress measurement using speech: Recent advancements, validation issues, and ethical and privacy considerations. Stress 2019, 22, 408–413. [Google Scholar] [CrossRef] [Green Version]
- Seshadri, D.R.; Li, R.T.; Voos, J.E.; Rowbottom, J.R.; Alfes, C.M.; Zorman, C.A.; Drummond, C.K. Wearable sensors for monitoring the physiological and biochemical profile of the athlete. NPJ Digit. Med. 2019, 2, 72. [Google Scholar] [CrossRef] [Green Version]
- Zhang, T.; El Ali, A.; Wang, C.; Hanjalic, A.; Cesar, P. Corrnet: Fine-grained emotion recognition for video watching using wearable physiological sensors. Sensors 2021, 21, 52. [Google Scholar] [CrossRef] [PubMed]
- Bizzego, A.; Gabrieli, G.; Furlanello, C.; Esposito, G. Comparison of wearable and clinical devices for acquisition of peripheral nervous system signals. Sensors 2020, 20, 6778. [Google Scholar] [CrossRef] [PubMed]
- Can, Y.S.; Iles-Smith, H.; Chalabianloo, N.; Ekiz, D.; Fernández-Álvarez, J.; Repetto, C.; Riva, G.; Ersoy, C. How to Relax in Stressful Situations: A Smart Stress Reduction System. Healthcare 2020, 8, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Can, Y.S.; Chalabianloo, N.; Ekiz, D.; Ersoy, C. Continuous stress detection using wearable sensors in real life: Algorithmic programming contest case study. Sensors 2019, 19, 1849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhury, A.K.; Tjondronegoro, D.; Chandran, V.; Zhang, J.; Trost, S.G. Prediction of relative physical activity intensity using multimodal sensing of physiological data. Sensors 2019, 19, 4509. [Google Scholar] [CrossRef] [Green Version]
- Zangróniz, R.; Martínez-Rodrigo, A.; Pastor, J.M.; López, M.T.; Fernández-Caballero, A. Electrodermal activity sensor for classification of calm/distress condition. Sensors 2017, 17, 2324. [Google Scholar] [CrossRef] [Green Version]
- Seoane, F.; Mohino-Herranz, I.; Ferreira, J.; Alvarez, L.; Buendia, R.; Ayllón, D.; Llerena, C.; Gil-Pita, R. Wearable biomedical measurement systems for assessment of mental stress of combatants in real time. Sensors 2014, 14, 7120–7141. [Google Scholar] [CrossRef] [Green Version]
- Betti, S.; Lova, R.M.; Rovini, E.; Acerbi, G.; Santarelli, L.; Cabiati, M.; Del Ry, S.; Cavallo, F. Evaluation of an integrated system of wearable physiological sensors for stress monitoring in working environments by using biological markers. IEEE Trans. Biomed. Eng. 2018, 65, 1748–1758. [Google Scholar]
- Pourmohammadi, S.; Maleki, A. Stress detection using ECG and EMG signals: A comprehensive study. Comput. Methods Programs Biomed. 2020, 193, 105482. [Google Scholar] [CrossRef]
- Muaremi, A.; Arnrich, B.; Tröster, G. Towards Measuring Stress with Smartphones and Wearable Devices During Workday and Sleep. Bionanoscience 2013, 3, 172–183. [Google Scholar] [CrossRef] [Green Version]
- Nakajima, M.; Lemieux, A.M.; Fiecas, M.; Chatterjee, S.; Sarker, H.; Saleheen, N.; Ertin, E.; Kumar, S.; al’Absi, M. Using novel mobile sensors to assess stress and smoking lapse. Int. J. Psychophysiol. 2020, 158, 411–418. [Google Scholar] [CrossRef]
- Peake, J.M.; Kerr, G.; Sullivan, J.P. A critical review of consumer wearables, mobile applications, and equipment for providing biofeedback, monitoring stress, and sleep in physically active populations. Front. Physiol. 2018, 9, 743. [Google Scholar] [CrossRef] [PubMed]
- Mohr, D.C.; Zhang, M.; Schueller, S.M. Personal Sensing: Understanding Mental Health Using Ubiquitous Sensors and Machine Learning. Annu. Rev. Clin. Psychol. 2017, 13, 23–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Ceja, E.; Riegler, M.; Nordgreen, T.; Jakobsen, P.; Oedegaard, K.J.; Tørresen, J. Mental health monitoring with multimodal sensing and machine learning: A survey. Pervasive Mob. Comput. 2018, 51, 1–26. [Google Scholar] [CrossRef]
- TrendMedic. Available online: https://www.trendmedic.de/en/wellue-o2-ring-oxygen-monitor (accessed on 4 May 2021).
- Texas Instruments. Available online: https://www.ti.com/product/ADS1292R (accessed on 4 May 2021).
- Asgarian, F.; Najafi, K. Time synchronization in a network of bluetooth low energy beacons. In Proceedings of the SIGCOMM Posters and Demos, Los Angeles, CA, USA, 22–24 August 2017; pp. 119–120. [Google Scholar]
- Di Rienzo, M.; Rizzo, G.; Işilay, Z.M.; Lombardi, P. SeisMote: A Multi-Sensor Wireless Platform for Cardiovascular Monitoring in Laboratory, Daily Life, and Telemedicine. Sensors 2020, 20, 680. [Google Scholar] [CrossRef] [Green Version]
- Stopjakova, V.; Kovac, M.; Potocny, M. On-chip energy harvesting for implantable medical devices. Radioengineering 2020, 29, 269–284. [Google Scholar] [CrossRef]
- Nagy, G.; Arbet, D.; Stopjakova, V.; Kovac, M. Novel CMOS bulk-driven charge pump for ultra low input voltage. Radioengineering 2016, 25, 321–331. [Google Scholar] [CrossRef]
- Ouraring. Available online: www.ouraring.com/ (accessed on 4 May 2021).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Garmin Vivoactive 4 [190] |
| Sensors: PPG 1, accelerometer, gyroscope, compass, barometer, thermometer, microphone, ambient light, GPS, GLONASS, Galileo |
| Physiology variables: HR, spO2, stress 2, respiration 2 (meditation), sleep and activity tracking, body battery energy |
| Connectivity: Bluetooth, Wi-Fi, NFC, ANT+, Waterproof: 5 ATM; Form: Watch |
| Samsung Galaxy Watch Active 2 [191] |
| Sensors: PPG 1, ECG 3, accelerometer, gyroscope, compass, barometer, microphone, ambient light, GPS, GLONASS, Galileo, Beidou |
| Physiology variables: ECG 3, HR, BP 3, stress 2 (meditation), sleep and activity monitoring |
| Connectivity: Bluetooth, Wi-Fi, NFC; Waterproof: 5 ATM; Form: watch |
| Google Fossil Gen 5 [193] |
| Sensors: PPG 1, accelerometer, gyroscope, compass, barometer, microphone, ambient light, GPS |
| Physiology variables: HR, stress 2 (meditation), sleep and activity monitoring |
| Connectivity: Bluetooth, Wi-Fi, NFC; Waterproof: 3 ATM; Form: watch |
| Apple Watch 6 [192] |
| Sensors: PPG 1, ECG 3, accelerometer, gyroscope, compass, barometer, microphone, ambient light, GPS, GLONASS, Galileo |
| Physiology variables: ECG 3, HR, spO2, sleep and activity monitoring |
| Connectivity: Bluetooth, Wi-Fi, NFC; Waterproof: 5 ATM; Form: watch |
| Withings Scanwatch [196] |
| Sensors: PPG 1, ECG 3, accelerometer, gyroscope, compass, barometer, ambient light |
| Physiology variables: ECG 3, HR, spO2 (medical grade), sleep and activity tracking |
| Connectivity: Bluetooth Low Energy, USB; Waterproof: 5 ATM; Form: watch |
| Fitbit Sense [195] |
| Sensors: PPG 1, ECG 3, EDA 3, thermometer, accelerometer, gyroscope, barometer, microphone, ambient light, GPS, GLONASS |
| Physiology variables: ECG 3, HR, spO2, peripheral temperature, stress (meditation), sleep and activity monitoring |
| Connectivity: Bluetooth Low Energy, Wi-Fi, NFC; Waterproof: 5 ATM; Form: watch |
| Samsung Simband [200] |
| Sensors: PPG 1, ECG 3, EDA, bioimpedance, thermometer, accelerometer |
| Physiology variables: ECG 3, HR, EDA, bioimpedance (blood flow), peripheral temperature, activity tracking |
| Connectivity: Bluetooth, USB; Form: watch |
| Empatica Embrace 2 [199] |
| Sensors: EDA, temperature, accelerometer, gyroscope |
| Physiology variables: EDA (clinical grade), peripheral temperature, stress, sleep and activity tracking |
| Connectivity: Bluetooth Low Energy; Waterproof: 0.1 ATM; Form: wristband |
| Empatica E4 [199] |
| Sensors: PPG 1, EDA, infrared temperature, accelerometer, event maker |
| Physiology variables: HR, spO2, EDA, peripheral temperature, activity tracking |
| Connectivity: Bluetooth Low Energy, USB 2.0, Raw data analysis; Waterproof: 0.1 ATM; Form: wristband |
| Zephyr Bioharness 3 [202] |
| Sensors: HR, RR, accelerometer |
| Physiology variables: HR, RR, activity monitoring |
| Connectivity: Bluetooth Low Energy; Form: chest-belt |
| Quardiocore [203] |
| Sensors: ECG, skin temperature, accelerometer, gyroscope, compass |
| Physiology variables: ECG, HR, RR, body core temperature, activity tracking |
| Connectivity: Bluetooth 4.0; Form: chest-belt |
| Philips Wearable biosensor [204] |
| Sensors: ECG, skin temperature, accelerometer |
| Physiology variables: ECG, HR, RR, body core temperature, activity tracking |
| Connectivity: Bluetooth; Form: chest-belt |
| Oura health ring [232] |
| Sensors: PPG 4, accelerometer, gyroscope, NTC thermometer |
| Physiology variables: HR, RR 2, peripheral temperature, stress (meditation), sleep and activity tracking |
| Connectivity: Bluetooth Low Energy; Waterproof: 10 ATM; Form: ring |
| Neurosky MindWave [205] |
| Sensors: EEG |
| Physiology variables: EEG |
| Connectivity: Bluetooth/Bluetooth Low Energy dual mode; Form: headband |
| Muse 2 EEG [206] |
| Sensors: EEG, PPG 1, accelerometer, gyroscope |
| Physiology variables: EEG (emotions), HR, stress (meditation) and activity tracking |
| Connectivity: Bluetooth 4.2, USB; Form: headband |
| Flowtime EEG [207] |
| Sensors: EEG, PPG 1 |
| Physiology variables: EEG, HR, stress tracking (active/neutral/calm) |
| Connectivity: Bluetooth; Form: headband |
| Spire Health Tag [208] |
| Sensors: PPG 1, accelerometer |
| Physiology variables: HR, RR 2, stress (calm/focus/tension), sleep and activity tracking |
| Connectivity: Bluetooth; Form: adhered to clothes; Washer and dryer proof |
| Multi-sensor concept |
| Sensors: ECG, PPG 4, respiration, EDA (IDA microelectrodes), 2× infrared temperature, 2× accelerometer, gyroscope, compass |
| Physiology variables: ECG, HR, spO2, EDA, respiration, peripheral and body core temperature (heat gradient), BP (derived from ECG and PPG), stress, sleep and activity monitoring |
| Connectivity: Bluetooth Low Energy, USB; Form: ring and chest-belt |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vavrinsky, E.; Stopjakova, V.; Kopani, M.; Kosnacova, H. The Concept of Advanced Multi-Sensor Monitoring of Human Stress. Sensors 2021, 21, 3499. https://doi.org/10.3390/s21103499
Vavrinsky E, Stopjakova V, Kopani M, Kosnacova H. The Concept of Advanced Multi-Sensor Monitoring of Human Stress. Sensors. 2021; 21(10):3499. https://doi.org/10.3390/s21103499
Chicago/Turabian StyleVavrinsky, Erik, Viera Stopjakova, Martin Kopani, and Helena Kosnacova. 2021. "The Concept of Advanced Multi-Sensor Monitoring of Human Stress" Sensors 21, no. 10: 3499. https://doi.org/10.3390/s21103499
APA StyleVavrinsky, E., Stopjakova, V., Kopani, M., & Kosnacova, H. (2021). The Concept of Advanced Multi-Sensor Monitoring of Human Stress. Sensors, 21(10), 3499. https://doi.org/10.3390/s21103499