
A Case–Control Study of the Effects of Chronic Low Back Pain in Spatiotemporal Gait Parameters

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
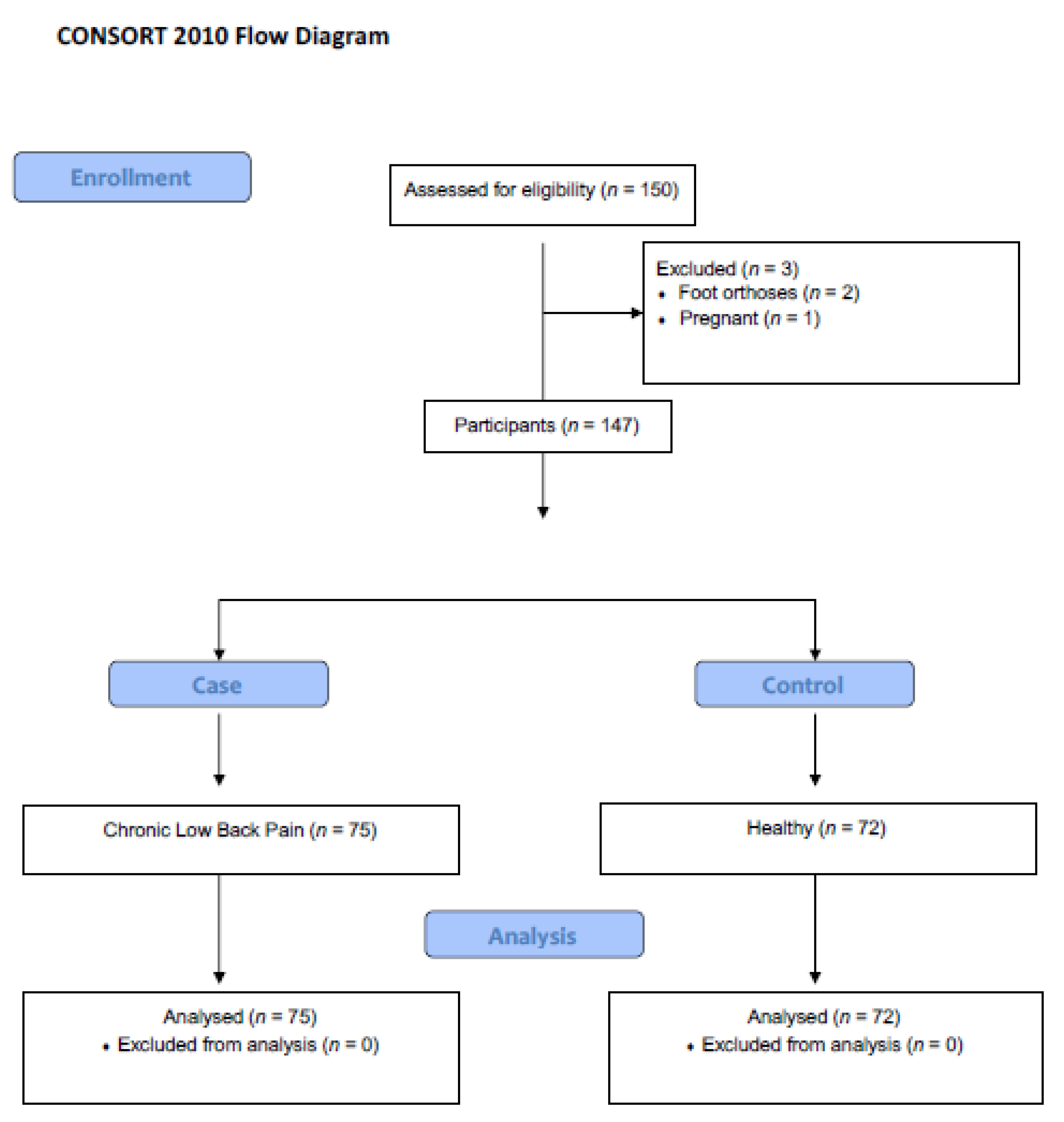
2.1. Trial Design
2.2. Participants
2.3. Inclusion Criteria
2.4. Exclusion Criteria
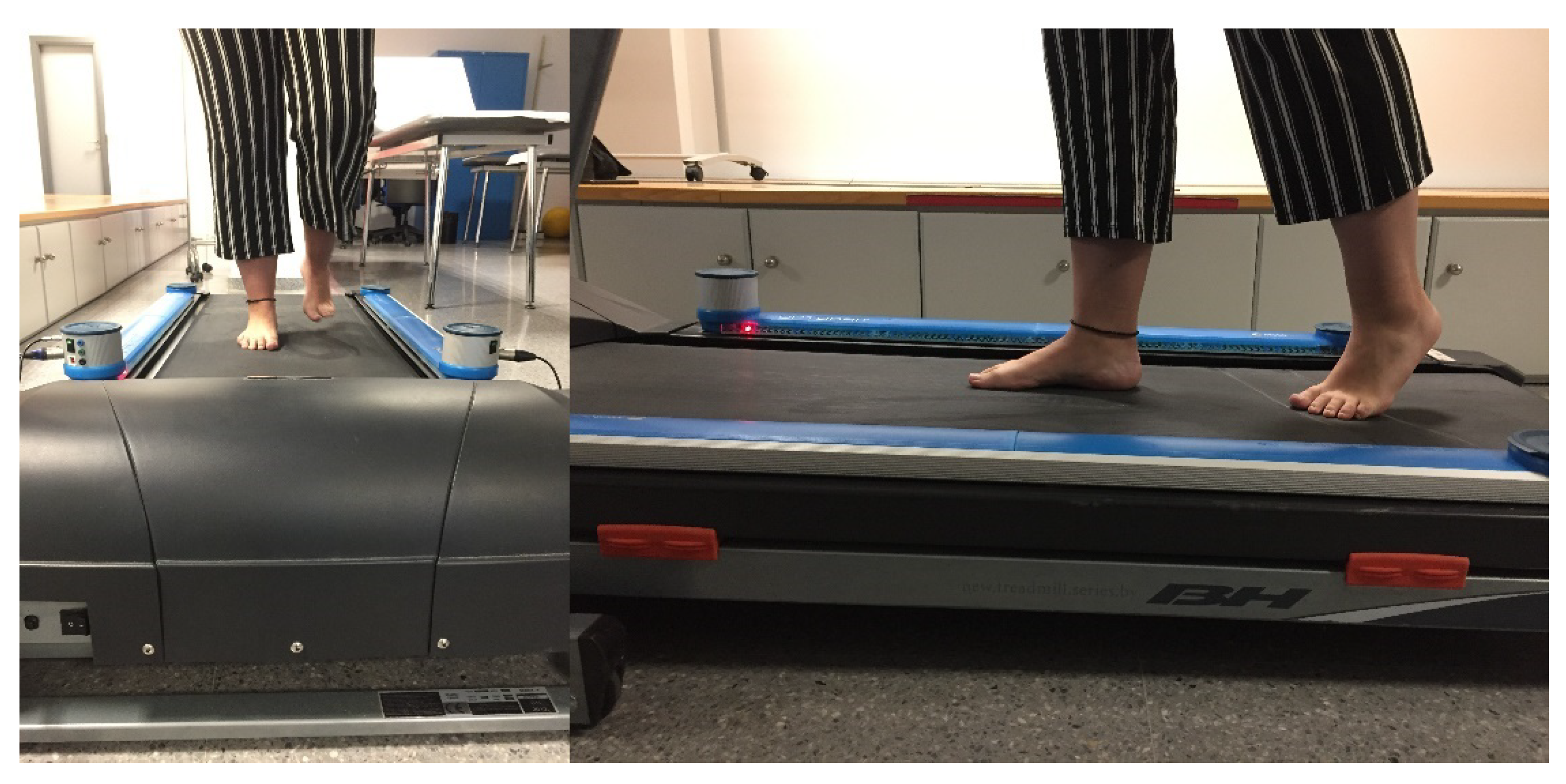
2.5. Procedures
2.6. Ethical Statements
2.7. Statistical Analysis
3. Results
3.1. Description of the Total Sample and by Groups
3.2. Statistical Analysis
4. Discussion
5. Conclusions
5.1. Study Limitations
5.2. Practical Implications of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hartvigsen, J.; Hancock, M.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- Demirel, A.; Onan, D.; Oz, M.; Ozel Aslıyuce, Y.; Ulger, O. Moderate disability has negative effect on spatiotem-poral parameters in patients with chronic low back pain. Gait Posture 2020, 79, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Lee, M.; Song, C.; Lee, K.; Shin, D. Agreement between the spatio-temporal gait parameters from treadmill-based photoelectric cell and the instrumented treadmill system in healthy young adults and stroke patients. Med. Sci. Monit. 2014, 20, 1210–1219. [Google Scholar] [CrossRef] [Green Version]
- Hirase, T.; Okubo, Y.; Sturnieks, D.L.; Lord, S.R. Pain Is Associated with Poor Balance in Community-Dwelling Older Adults: A Systematic Review and Meta-analysis. J. Am. Med. Dir. Assoc. 2020, 21, 597–603.e8. [Google Scholar] [CrossRef]
- Requelo-Rodríguez, I.; Castro-Méndez, A.; Jiménez-Cebrián, A.; González-Elena, M.; Palomo-Toucedo, I.; Pabón-Carrasco, M. Assessment of Selected Spatio-Temporal Gait Parameters on Subjects with Pronated Foot Posture on the Basis of Measurements Using OptoGait. A Case-Control Study. Sensors 2021, 21, 2805. [Google Scholar] [CrossRef] [PubMed]
- Lansing, J.E.; Ellingson, L.D.; DeShaw, K.J.; Cruz-Maldonado, G.; Hurt, T.R.; Meyer, J.D. A qualitative analysis of barriers and facilitators to reducing sedentary time in adults with chronic low back pain. BMC Public Health 2021, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Schega, L.; Kaps, B.; Broscheid, K.-C.; Bielitzki, R.; Behrens, M.; Meiler, K.; Drange, S.; Franke, J. Effects of a multimodal exercise intervention on physical and cognitive functions in patients with chronic low back pain (MultiMove): Study protocol for a randomized controlled trial. BMC Geriatr. 2021, 21, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Maranesi, E.; Riccardi, G.R.; Lattanzio, F.; Di Rosa, M.; Luzi, R.; Casoni, E.; Rinaldi, N.; Baldoni, R.; Di Donna, V.; Bevilacqua, R. Randomised controlled trial assessing the effect of a technology-assisted gait and balance training on mobility in older people after hip fracture: Study protocol. BMJ Open 2020, 10, e035508. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Jiménez, E.M.; Losa-Iglesias, M.E.; Díaz-Velázquez, J.I.; Becerro-De-Bengoa-Vallejo, R.; Palomo-López, P.; Calvo-Lobo, C.; López-López, D.; Rodríguez-Sanz, D. Acute Effects of Intermittent Versus Continuous Bilateral Ankle Plantar Flexor Static Stretching on Postural Sway and Plantar Pressures: A Randomized Clinical Trial. J. Clin. Med. 2019, 8, 52. [Google Scholar] [CrossRef] [Green Version]
- Bricot, B. La Reprogrammation Posturale Globale (Global Postural Reprogramming), 2nd ed.; Sauramps Medical: Montpellier, France, 2020; pp. 108–145. [Google Scholar]
- Iacob, S.; Chisnoiu, A.; Buduru, S.; Berar, A.; Fluerasu, M.; Iacob, I.; Objelean, A.; Studnicska, W.; Viman, L. Plantar Pressure Variations Induced by Experimental Malocclusion—A Pilot Case Series Study. Healthcare 2021, 9, 599. [Google Scholar] [CrossRef]
- Hartvigsen, J.; Morsø, L.; Bendix, T.; Manniche, C. Supervised and non-supervised Nordic walking in the treatment of chronic low back pain: A single blind randomized clinical trial. BMC Musculoskelet. Disord. 2010, 11, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rum, L.; Brasiliano, P.; Vannozzi, G.; Laudani, L.; Macaluso, A. Non-specific chronic low back pain elicits kinematic and neuromuscular changes in walking and gait termination. Gait Posture 2021, 84, 238–244. [Google Scholar] [CrossRef]
- Koch, C.; Hänsel, F. Chronic Non-specific Low Back Pain and Motor Control during Gait. Front. Psychol. 2018, 9, 2236. [Google Scholar] [CrossRef] [PubMed]
- Barzilay, Y.; Segal, G.; Lotan, R.; Regev, G.; Beer, Y.; Lonner, B.S.; Mor, A.; Elbaz, A. Patients with chronic non-specific low back pain who reported reduction in pain and improvement in function also demonstrated an improvement in gait pattern. Eur. Spine J. 2015, 25, 2761–2766. [Google Scholar] [CrossRef]
- Bijur, P.; Silver, W.; Gallagher, E. Reliability of the visual analog scale for measurement of acute pain. Acad. Emerg. Med. 2001, 8, 1153–1157. [Google Scholar] [CrossRef]
- Chapman, J.R.; Norvell, D.C.; Hermsmeyer, J.T.; Bransford, R.J.; Devine, J.; McGirt, M.J.; Lee, M.J. Evaluating Common Outcomes for Measuring Treatment Success for Chronic Low Back Pain. Spine 2011, 36, S54–S68. [Google Scholar] [CrossRef]
- Declaración de Helsinki de la AMM. Principios Éticos para las Investigaciones Médicas en seres Humanos. Asamblea General de la AMM, Fortaleza, Brasil, Octubre de 2013. Available online: https://www.wma.net/es/policies-post/declaracion-de-helsinki-de-la-amm-principios-eticos-para-las-investigaciones-medicas-en-seres-humanos/ (accessed on 25 December 2020).
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S.; Poole, C.; Schlesselman, J.J.; Egger, M.; Strobe Initiative. Strengthening the Reporting of Observational studies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Migueles, J.; Cadenas-Sanchez, C.; Alcantara, J.; Leal-Martín, J.; Mañas, A.; Ara, I.; Glynn, N.; Shiroma, E. Calibration and Cross-Validation of Accelerometer Cut-Points to Classify Sedentary Time and Physical Activity from Hip and Non-Dominant and Dominant Wrists in Older Adults. Sensors 2021, 21, 3326. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.; Zheng, H.; Wang, H.; Newell, D. Assessment of gait patterns of chronic low back pain patients: A smart mobile phone based approach. In Proceedings of the 2015 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Washington, DC, USA, 9–12 November 2015; pp. 1016–1023. [Google Scholar]
- Jaén-Carrillo, D.; García-Pinillos, F.; Cartón-Llorente, A.; Almenar-Arasanz, A.J.; Bustillo-Pelayo, J.A.; Roche-Seruendo, L. Test–retest reliability of the OptoGait system for the analysis of spatiotemporal running gait parameters and lower body stiffness in healthy adults. Proc. Inst. Mech. Eng. Part P J. Sports Eng. Technol. 2020, 234, 154–161. [Google Scholar] [CrossRef]
- User Manual. Microgate, Bolzano, Italia OptoGait. Available online: http://www.optogait.com/OptoGaitPortal/Media/Manuals/Manual-ES.PDF (accessed on 12 February 2021).
- Simoni, L.; Scarton, A.; Macchi, C.; Gori, F.; Pasquini, G.; Pogliaghi, S. Quantitative and Qualitative Running Gait Analysis through an Innovative Video-Based Approach. Sensors 2021, 21, 2977. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Hollman, J.H.; McDade, E.M.; Petersen, R.C. Normative spatiotemporal gait parameters in older adults. Gait Posture 2011, 34, 111–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henchoz, Y.; Soldini, N.; Peyrot, N.; Malatesta, D. Energetics and mechanics of walking in patients with chronic low back pain and healthy matched controls. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 115, 2433–2443. [Google Scholar] [CrossRef]
- Koremans, F.; Chen, X.; Das, A.; Diwan, A. Changes in Back Pain Scores after Bariatric Surgery in Obese Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 1443. [Google Scholar] [CrossRef] [PubMed]
- Maki, B.E. Gait Changes in Older Adults: Predictors of Falls or Indicators of Fear? J. Am. Geriatr. Soc. 1997, 45, 313–320. [Google Scholar] [CrossRef]
- Muchna, A.; Najafi, B.; Wendel, C.S.; Schwenk, M.; Armstrong, D.G.; Mohler, J. Foot Problems in Older Adults. J. Am. Podiatr. Med. Assoc. 2018, 108, 126–139. [Google Scholar] [CrossRef] [Green Version]
- Castro-Méndez, A.; Munuera, P.V.; Albornoz-Cabello, M. The short-term effect of custom-made foot orthoses in subjects with excessive foot pronation and lower back pain. Prosthetics Orthot. Int. 2013, 37, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Menz, H.; Alyssa, B.; Riskowski, J.; Howard, J.; Hannan, T. Foot posture, foot function and low back pain: The Framingham foot study. Rheumatology 2013, 53, 2275–2282. [Google Scholar] [CrossRef] [Green Version]
- Yazdani, S.; Dizji, E.; Alizadeh, F.; Hassanlouei, H. Effect of chronic idiopathic low back pain on the kinetic gait characteristics in different foot masks. J. Biomech. 2018, 79, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Cambron, J.A.; Duarte, M.; Dexheimer, J.; Solecki, T. Shoe Orthotics for the Treatment of Chronic Low Back Pain: A Randomized Controlled Pilot Study. J. Manip. Physiol. Ther. 2011, 34, 254–260. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sample n = 147 | Group | |||
|---|---|---|---|---|
| Case n = 75 | Control n = 72 | p-Value | ||
| Gender Male | 75 (51.0%) | 45 (60.0%) | 30 (40.0%) | p = 0.007 a |
| Gender Female | 72 (49.0%) | 29 (40.27%) | 43 (59.72%) | p = 0.007 a |
| BMI | 24.00 (2.80) | 25.25 (3.61) | 22.02 (4.15) | p = 0001 b |
| Sample n = 147 | Group | |||
|---|---|---|---|---|
| Case n = 75 | Control n = 72 | p-Value | ||
| Right foot stride length, cm | 60.50 (3.00) | 60.70 (2.80) | 60.40 (4.15) | p = 0.901 |
| Left foot stride length, cm | 60.10 (4.40) | 60.30 (6.50) | 59.90 (2.70) | p = 0.438 |
| Ground contact time: | ||||
| Right foot sec | 0.54 (0.03) | 0.54 (0.03) | 0.54 (0.09) | p = 0.332 |
| Step % | 70.50 (6.70) | 65.00 (9.30) | 71.10 (1.40) | p = 0.001 |
| Left foot sec | 0.54 (0.03) | 0.54 (0.06) | 0.55 (0.06) | p = 0.101 |
| Step % | 70.10 (7.60) | 66.00 (10.47) | 70.80 (1.00) | p = 0.001 |
| Difference stride% | 0.10 (3.30) | −0.70 (3.40) | −0.93 (3.00) | p = 0.001 |
| Difference contact% | −0.70 (1.50) | −0.70 (2.10) | −0.60 (1.10) | p = 0.050 |
| Gait cycle sec | 1.10 (0.05) | 1.09 (0.06) | 1.11 (0.06) | p = 0.867 |
| Gait cadence spm | 107.90 (9.40) | 107.03 (8.70) | 110.90 (8.80) | p = 0.013 |
| Total Stride length cm Speed, Km/h | 119.90 (6.20) 4.33 (0.74) | 122.50 (8.45) 4.21 (0.82) | 119.50 (3.30) 4.38 (0.92) | p = 0.036 p = 0.043 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castro-Méndez, A.; Requelo-Rodríguez, I.; Pabón-Carrasco, M.; González-Elena, M.L.; Ponce-Blandón, J.A.; Palomo-Toucedo, I.C. A Case–Control Study of the Effects of Chronic Low Back Pain in Spatiotemporal Gait Parameters. Sensors 2021, 21, 5247. https://doi.org/10.3390/s21155247
Castro-Méndez A, Requelo-Rodríguez I, Pabón-Carrasco M, González-Elena ML, Ponce-Blandón JA, Palomo-Toucedo IC. A Case–Control Study of the Effects of Chronic Low Back Pain in Spatiotemporal Gait Parameters. Sensors. 2021; 21(15):5247. https://doi.org/10.3390/s21155247
Chicago/Turabian StyleCastro-Méndez, Aurora, Inmaculada Requelo-Rodríguez, Manuel Pabón-Carrasco, María Luisa González-Elena, José Antonio Ponce-Blandón, and Inmaculada Concepción Palomo-Toucedo. 2021. "A Case–Control Study of the Effects of Chronic Low Back Pain in Spatiotemporal Gait Parameters" Sensors 21, no. 15: 5247. https://doi.org/10.3390/s21155247
APA StyleCastro-Méndez, A., Requelo-Rodríguez, I., Pabón-Carrasco, M., González-Elena, M. L., Ponce-Blandón, J. A., & Palomo-Toucedo, I. C. (2021). A Case–Control Study of the Effects of Chronic Low Back Pain in Spatiotemporal Gait Parameters. Sensors, 21(15), 5247. https://doi.org/10.3390/s21155247