
The Use of Synthetic IMU Signals in the Training of Deep Learning Models Significantly Improves the Accuracy of Joint Kinematic Predictions


Abstract
:1. Introduction
2. Materials and Methods
2.1. IMU Measurement and Simulation Workflow Overview
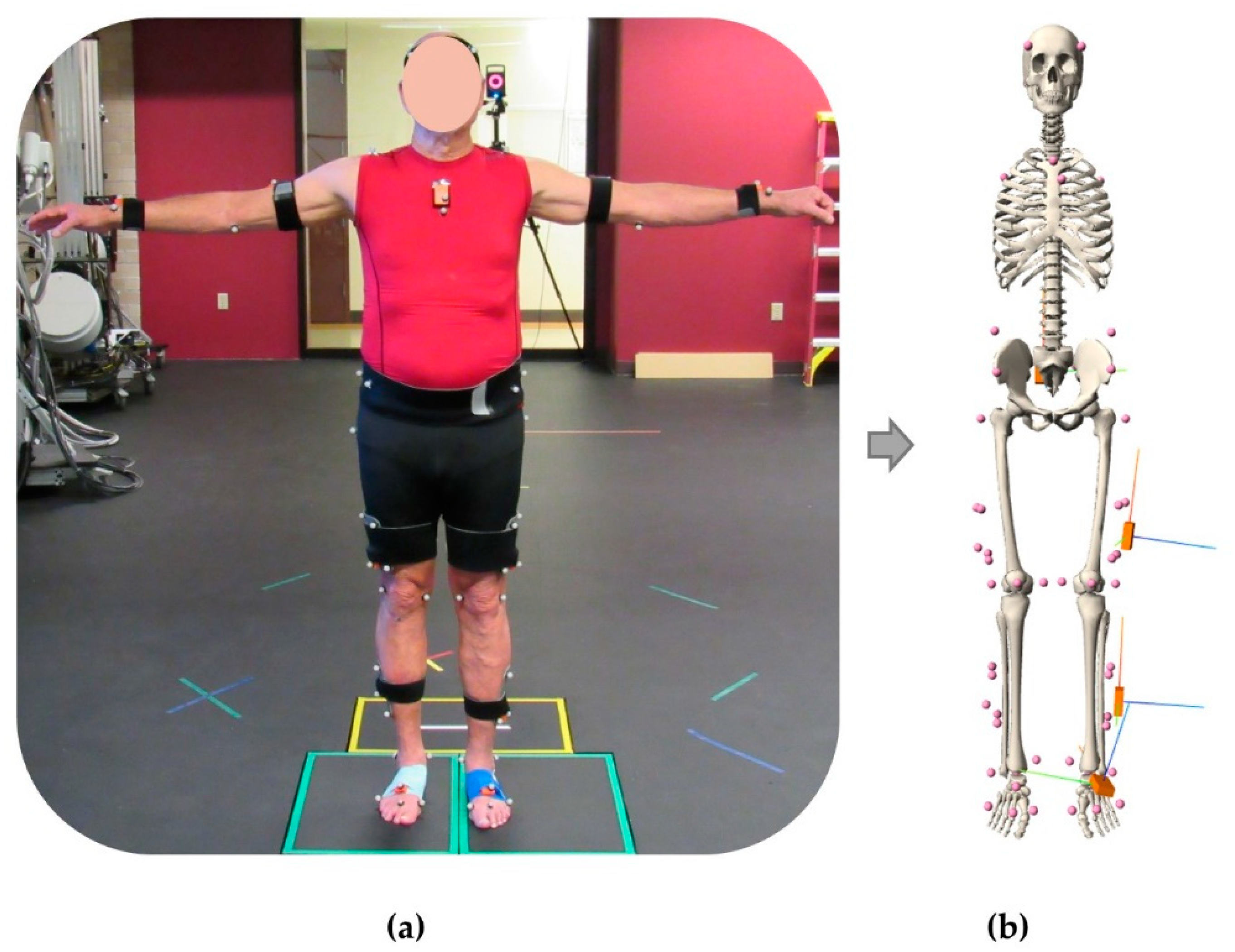
2.2. Experimental Data Collection
2.3. Musculoskeletal Modeling and IMU Simulation
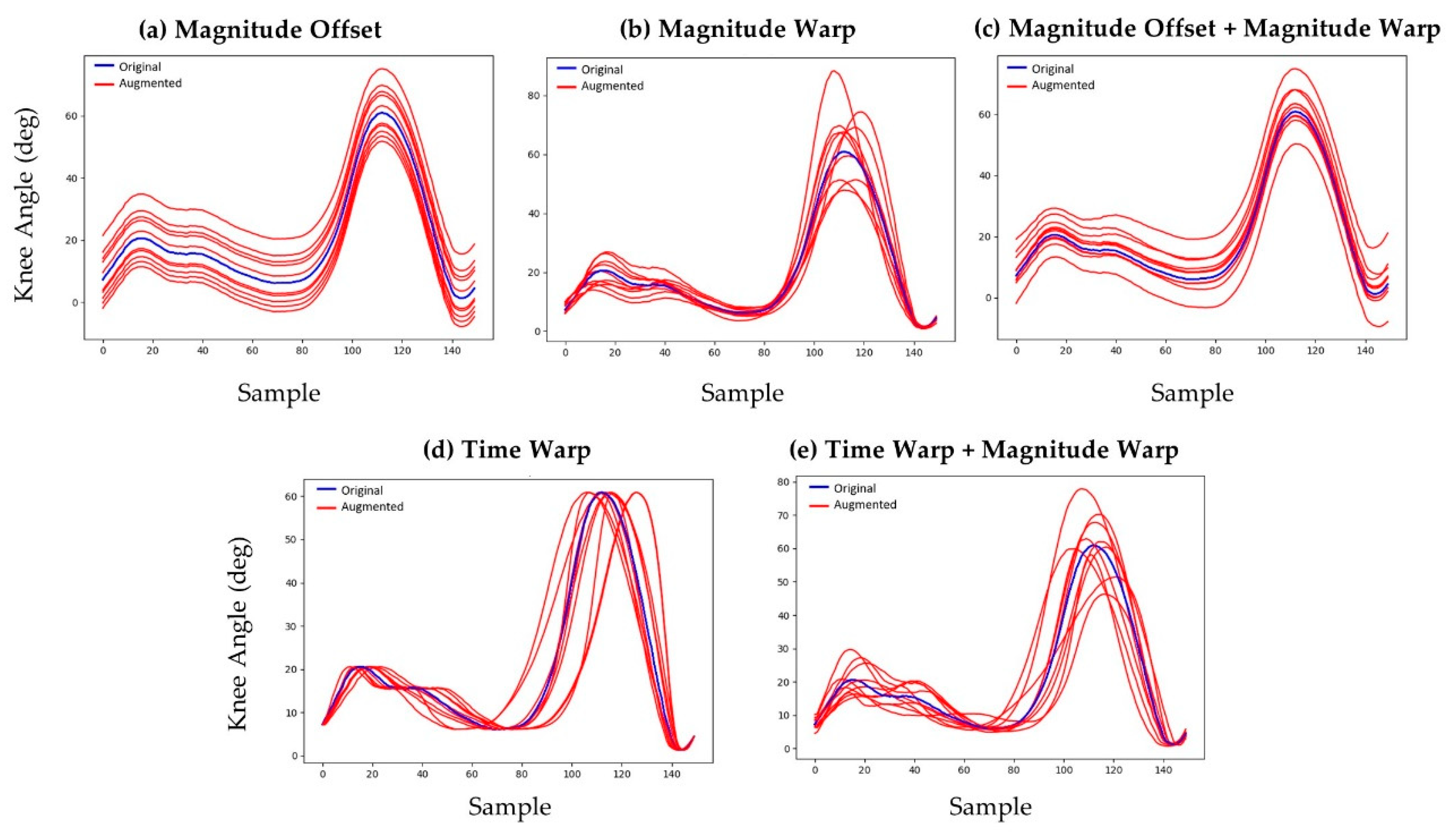
2.4. Kinematic Augmentation and Synthetic IMU Data Generation
2.5. Neural Network Model Architecture, Tuning, Training, and Evaluation
3. Results
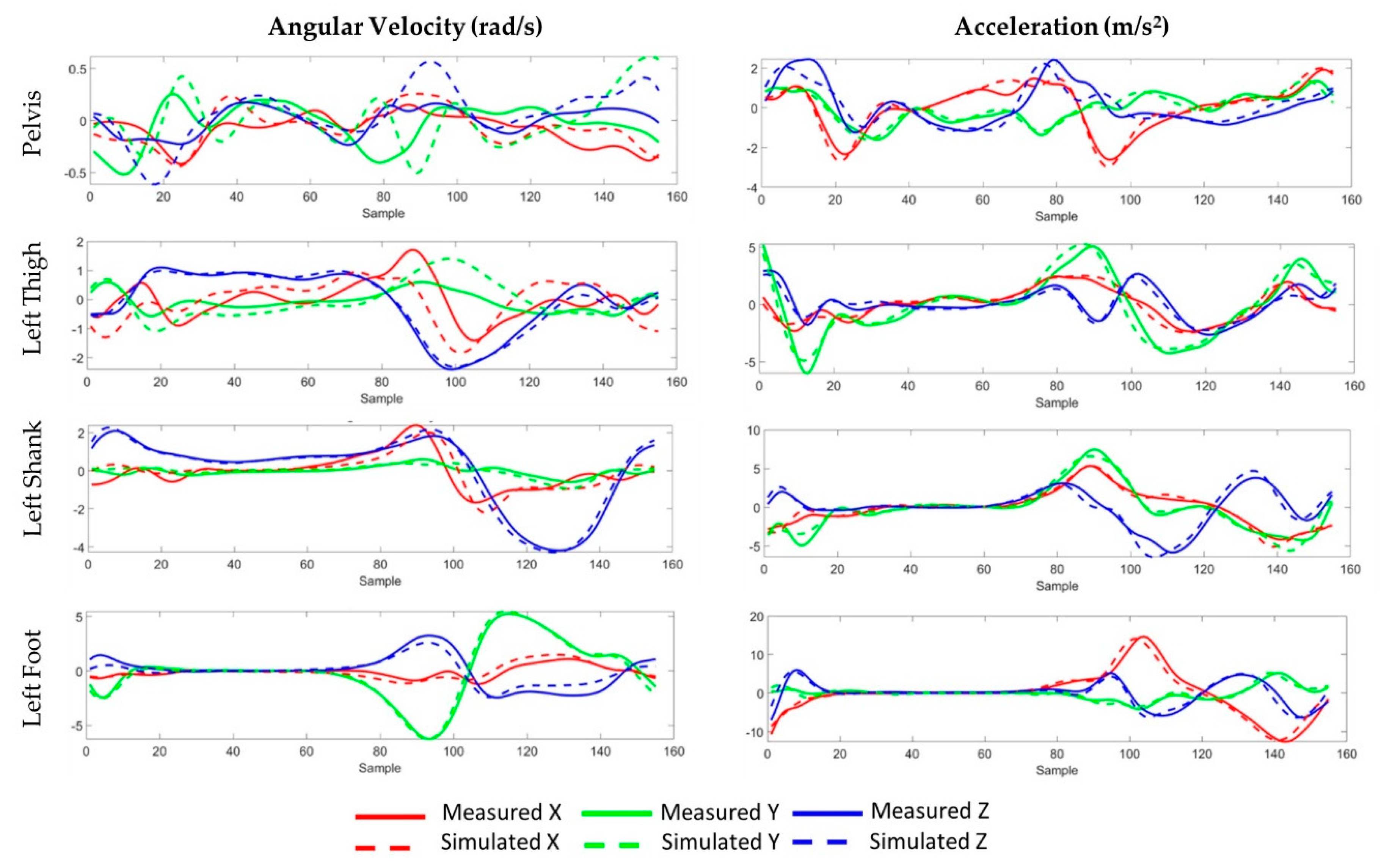
3.1. Simulated IMU Accuracy
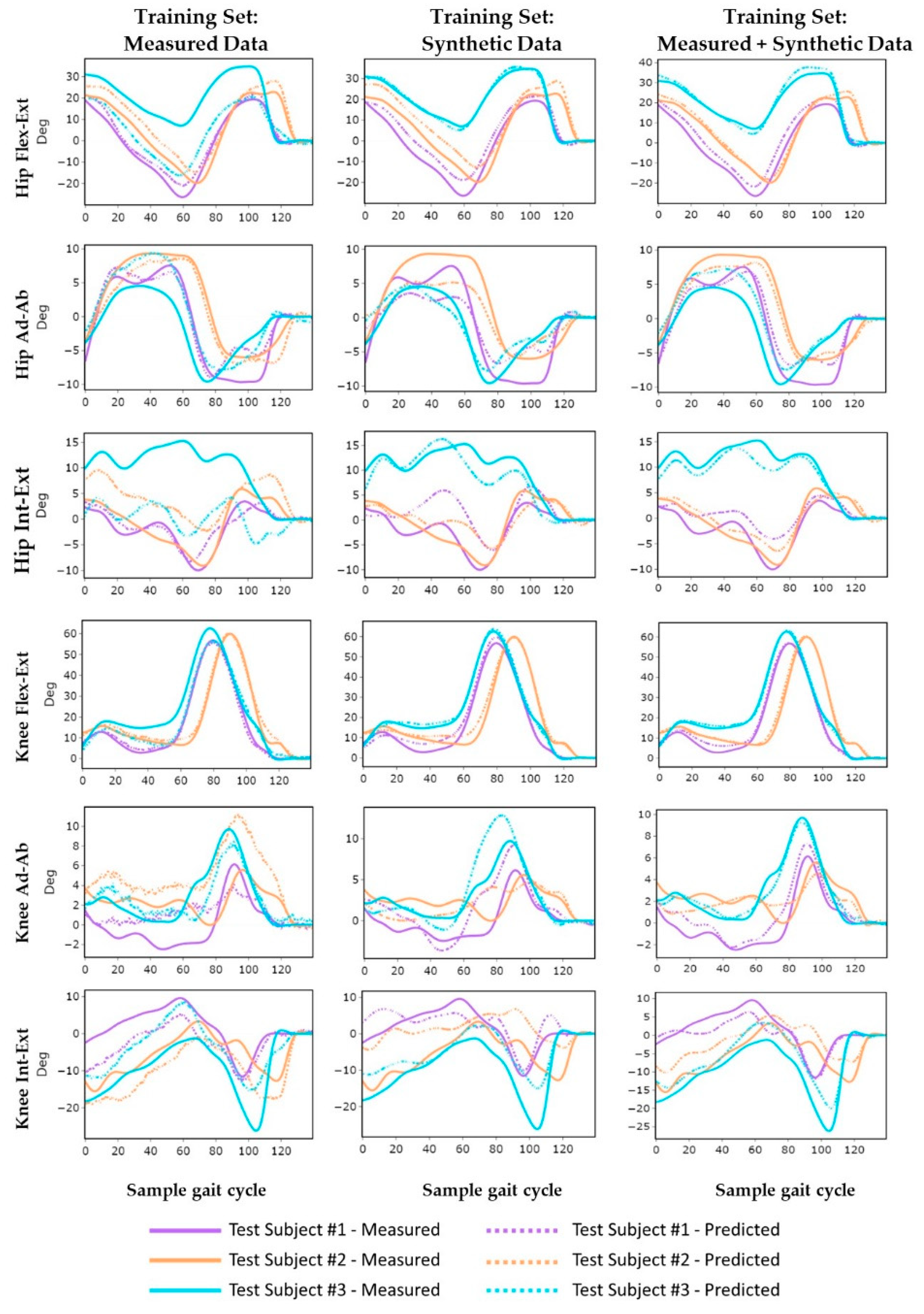
3.2. Model Accuracy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A. Prediction Accuracy for Each of the Three Subjects in the Test Cohort
| Test Subject #1 | |||||||||||||
| Training Set | # Samples | Hip Flex–Ext | Hip Ad–Ab | Hip Int–Ext | Hip Average | ||||||||
| r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | ||
| Measured | 3943 | 0.97 ± 0.02 | 3.4 ± 1.1 | 7.3 ± 2.4 | 0.94 ± 0.04 | 2.0 ± 0.6 | 9.4 ± 3.0 | 0.84 ± 0.08 | 2.0 ± 0.6 | 11.2 ± 3.4 | 0.92 ± 0.04 | 2.4 ± 0.8 | 9.3 ± 2.9 |
| Synthetic | 17,255 | 0.97 ± 0.04 | 0.97 ± 0.04 | 3.7 ± 1.7 | 0.94 ± 0.09 | 2.2 ± 0.7 | 10.6 ± 3.3 | 0.70 ± 0.15 | 2.7 ± 0.8 | 15.3 ± 4.6 | 0.87 ± 0.09 | 2.9 ± 1.1 | 11.2 ± 3.8 |
| Measured + Synthetic | 20,706 | 0.97 ± 0.01 | 0.97 ± 0.01 | 3.5 ± 0.9 | 0.96 ± 0.02 | 1.6 ± 0.4 | 7.4 ± 1.8 | 0.87 ± 0.08 | 2.0 ± 0.5 | 11.1 ± 2.8 | 0.94 ± 0.04 | 2.4 ± 0.6 | 8.7 ± 2.2 |
| Training Set | # Samples | Knee Flex–Ext | Knee Ad–Ab | Knee Int–Ext | Knee Average | ||||||||
| r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | ||
| Measured | 3943 | 0.99 ± 0.01 | 2.2 ± 0.7 | 3.0 ± 0.9 | 0.49 ± 0.20 | 1.9 ± 0.5 | 14.3 ± 3.6 | 0.69 ± 0.11 | 4.6 ± 0.9 | 23.5 ± 4.6 | 0.72 ± 0.10 | 2.9 ± 0.7 | 13.6 ± 30.0 |
| Synthetic | 17,255 | 0.99 ± 0.01 | 2.3 ± 0.7 | 3.1 ± 0.9 | 0.76 ± 0.10 | 2.2 ± 0.6 | 16.9 ± 4.3 | 0.85 ± 0.06 | 2.6 ± 0.4 | 13.3 ± 2.3 | 0.87 ± 0.06 | 2.4 ± 0.6 | 11.1 ± 2.5 |
| Measured + Synthetic | 20,706 | 0.99 ± 0.01 | 1.6 ± 0.4 | 2.2 ± 0.6 | 0.91 ± 0.06 | 0.9 ± 0.3 | 7.0 ± 2.0 | 0.94 ± 0.04 | 2.1 ± 0.5 | 10.5 ± 2.7 | 0.95 ± 0.03 | 1.5 ± 0.4 | 6.6 ± 1.8 |
| Test Subject #2 | |||||||||||||
| Training Set | # Samples | Hip Flex–Ext | Hip Ad–Ab | Hip Int–Ext | Hip Average | ||||||||
| r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | ||
| Measured | 3943 | 0.96 ± 0.05 | 3.6 ± 1.5 | 7.6 ± 3.1 | 0.96 ± 0.04 | 1.9 ± 0.6 | 9.1 ± 2.9 | 0.49 ± 0.20 | 5.0 ± 1.2 | 28.1 ± 6.6 | 0.80 ± 0.10 | 3.5 ± 1.1 | 15.0 ± 4.2 |
| Synthetic | 17,255 | 0.98 ± 0.02 | 2.9 ± 1.2 | 6.3 ± 2.6 | 0.96 ± 0.03 | 2.3 ± 0.4 | 10.8 ± 2.0 | 0.74 ± 0.15 | 2.7 ± 0.5 | 15.3 ± 2.9 | 0.89 ± 0.06 | 2.6 ± 0.7 | 10.8 ± 2.5 |
| Measured + Synthetic | 20,706 | 0.99 ± 0.01 | 1.9 ± 0.7 | 4.0 ± 1.6 | 0.99 ± 0.01 | 1.2 ± 0.4 | 5.7 ± 1.9 | 0.91 ± 0.07 | 2.0 ± 0.6 | 11.2 ± 3.3 | 0.96 ± 0.03 | 1.7 ± 0.6 | 7.0 ± 2.3 |
| Training Set | # Samples | Knee Flex–Ext | Knee Ad–Ab | Knee Int–Ext | Knee Average | ||||||||
| r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | ||
| Measured | 3943 | 0.99 ± 0.01 | 2.7 ± 1.4 | 3.6 ± 1.8 | 0.80 ± 0.09 | 2.9 ± 0.7 | 22.1 ± 5.1 | 0.89 ± 0.07 | 4.4 ± 1.3 | 22.0 ± 6.7 | 0.89 ± 0.06 | 3.3 ± 1.1 | 15.9 ± 4.5 |
| Synthetic | 17,255 | 0.99 ± 0.01 | 2.0 ± 0.5 | 2.7 ± 0.6 | 0.73 ± 0.10 | 1.5 ± 0.4 | 11.5 ± 2.7 | 0.81 ± 0.13 | 3.8 ± 1.1 | 19.3 ± 5.7 | 0.84 ± 0.08 | 2.4 ± 0.6 | 11.1 ± 3.0 |
| Measured + Synthetic | 20,706 | 0.99 ± 0.01 | 1.2 ± 0.5 | 1.6 ± 0.7 | 0.91 ± 0.06 | 0.8 ± 0.3 | 6.2 ± 2.2 | 0.96 ± 0.03 | 2.1 ± 0.6 | 10.5 ± 3.3 | 0.96 ± 0.03 | 1.4 ± 0.5 | 6.1 ± 2.0 |
| Test Subject #3 | |||||||||||||
| Training Set | # Samples | Hip Flex–Ext | Hip Ad–Ab | Hip Int–Ext | Hip Average | ||||||||
| r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | ||
| Measured | 3943 | 0.74 ± 0.08 | 13.3 ± 1.9 | 28.6 ± 4.1 | 0.93 ± 0.03 | 2.4 ± 0.6 | 11.5 ± 3.1 | 0.62 ± 0.25 | 5.4 ± 1.7 | 30.7 ± 9.4 | 0.76 ± 0.12 | 7.0 ± 1.4 | 23.6 ± 5.5 |
| Synthetic | 17,255 | 0.99 ± 0.01 | 1.6 ± 0.5 | 3.5 ± 1.0 | 0.95 ± 0.03 | 1.6 ± 0.4 | 7.5 ± 1.9 | 0.96 ± 0.02 | 1.5 ± 0.4 | 8.7 ± 2.3 | 0.97 ± 0.02 | 1.6 ± 0.4 | 6.5 ± 1.8 |
| Measured + Synthetic | 20,706 | 0.99 ± 0.01 | 2.4 ± 0.8 | 5.1 ± 1.7 | 0.98 ± 0.01 | 1.1 ± 0.5 | 5.3 ± 2.2 | 0.98 ± 0.01 | 1.3 ± 0.5 | 7.6 ± 3.0 | 0.98 ± 0.01 | 1.6 ± 0.6 | 6.0 ± 2.3 |
| Training Set | # Samples | Knee Flex–Ext | Knee Ad–Ab | Knee Int–Ext | Knee Average | ||||||||
| r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | ||
| Measured | 3943 | 0.98 ± 0.01 | 3.6 ± 0.8 | 4.9 ± 1.0 | 0.91 ± 0.03 | 1.3 ± 0.2 | 10.1 ± 1.8 | 0.72 ± 0.12 | 5.9 ± 0.8 | 30.1 ± 3.9 | 0.87 ± 0.05 | 3.6 ± 0.6 | 15.0 ± 2.3 |
| Synthetic | 17,255 | 0.99 ± 0.01 | 2.1 ± 0.6 | 2.8 ± 0.8 | 0.95 ± 0.02 | 2.2 ± 0.5 | 16.9 ± 4.2 | 0.49 ± 0.24 | 7.3 ± 1.1 | 36.7 ± 5.8 | 0.81 ± 0.09 | 3.8 ± 0.8 | 18.8 ± 3.6 |
| Measured + Synthetic | 20,706 | 0.99 ± 0.01 | 1.4 ± 0.4 | 1.8 ± 0.6 | 0.98 ± 0.01 | 0.9 ± 0.3 | 6.5 ± 2.6 | 0.90 ± 0.09 | 4.0 ± 1.2 | 20.2 ± 5.9 | 0.96 ± 0.04 | 2.1 ± 0.7 | 9.5 ± 3.0 |
References
- Clary, C.W.; Fitzpatrick, C.K.; Maletsky, L.P.; Rullkoetter, P.J. The influence of total knee arthroplasty geometry on mid-flexion stability: An experimental and finite element study. J. Biomech. 2013, 46, 1351–1357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sartori, M.; Lloyd, D.; Farina, D. Corrections to “Neural Data-Driven Musculoskeletal Modeling for Personalized Neurorehabilitation Technologies” [May 16 879-893]. IEEE Trans. Biomed. Eng. 2016, 63, 1341. [Google Scholar] [CrossRef]
- Picerno, P. 25 years of lower limb joint kinematics by using inertial and magnetic sensors: A review of methodological approaches. Gait Posture 2017, 51, 239–246. [Google Scholar] [CrossRef]
- Weygers, I.; Kok, M.; Konings, M.; Hallez, H.; De Vroey, H.; Claeys, K. Inertial Sensor-Based Lower Limb Joint Kinematics: A Methodological Systematic Review. Sensors 2020, 20, 673. [Google Scholar] [CrossRef] [Green Version]
- Karatsidis, A.; Jung, M.; Schepers, H.M.; Bellusci, G.; de Zee, M.; Veltink, P.H.; Andersen, M.S. Predicting kinetics using musculoskeletal modeling and inertial motion capture. arXiv 2018, arXiv:1801.01668. [Google Scholar]
- Dorschky, E.; Nitschke, M.; Seifer, A.-K.; Bogert, A.V.D.; Eskofier, B.M. Estimation of gait kinematics and kinetics from inertial sensor data using optimal control of musculoskeletal models. J. Biomech. 2019, 95, 109278. [Google Scholar] [CrossRef]
- Konrath, J.M.; Karatsidis, A.; Schepers, H.M.; Bellusci, G.; De Zee, M.; Andersen, M.S. Estimation of the Knee Adduction Moment and Joint Contact Force during Daily Living Activities Using Inertial Motion Capture. Sensors 2019, 19, 1681. [Google Scholar] [CrossRef] [Green Version]
- Karatsidis, A.; Jung, M.K.; Schepers, H.M.; Bellusci, G.; de Zee, M.; Veltink, P.H.; Andersen, M.S. Musculoskeletal model-based inverse dynamic analysis under ambulatory conditions using inertial motion capture. Med. Eng. Phys. 2019, 65, 68–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seel, T.; Raisch, J.; Schauer, T. IMU-Based Joint Angle Measurement for Gait Analysis. Sensors 2014, 14, 6891–6909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gholami, M.; Napier, C.; Menon, C. Estimating Lower Extremity Running Gait Kinematics with A Single Accelerometer: A Deep Learning Approach. Sensors 2020, 20, 2939. [Google Scholar] [CrossRef]
- Halilaj, E.; Rajagopal, A.; Fiterau, M.; Hicks, J.L.; Hastie, T.J.; Delp, S.L. Machine learning in human movement biomechanics: Best practices, common pitfalls, and new opportunities. J. Biomech. 2018, 81, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hendry, D.; Leadbetter, R.; McKee, K.; Hopper, L.; Wild, C.; O’Sullivan, P.; Straker, L.; Campbell, A. An Exploration of Machine-Learning Estimation of Ground Reaction Force from Wearable Sensor Data. Sensors 2020, 20, 740. [Google Scholar] [CrossRef] [Green Version]
- Johnson, W.R.; Mian, A.; Robinson, M.A.; Verheul, J.; Lloyd, D.G.; Alderson, J.A. Multidimensional Ground Reaction Forces and Moments From Wearable Sensor Accelerations via Deep Learning. IEEE Trans. Biomed. Eng. 2020, 68, 289–297. [Google Scholar] [CrossRef]
- Komaris, D.-S.; Perez-Valero, E.; Jordan, L.; Barton, J.; Hennessy, L.; O’Flynn, B.; Tedesco, S. Predicting Three-Dimensional Ground Reaction Forces in Running by Using Artificial Neural Networks and Lower Body Kinematics. IEEE Access 2019, 7, 156779–156786. [Google Scholar] [CrossRef]
- Wouda, F.J.; Giuberti, M.; Bellusci, G.; Maartens, E.; Reenalda, J.; Van Beijnum, B.-J.F.; Veltink, P.H. Estimation of Vertical Ground Reaction Forces and Sagittal Knee Kinematics During Running Using Three Inertial Sensors. Front. Physiol. 2018, 9, 218. [Google Scholar] [CrossRef] [PubMed]
- Johnson, W.R.; Mian, A.; Lloyd, D.G.; Alderson, J.A. On-field player workload exposure and knee injury risk monitoring via deep learning. J. Biomech. 2019, 93, 185–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Argent, R.; Drummond, S.; Remus, A.; O’Reilly, M.; Caulfield, B. Evaluating the use of machine learning in the assessment of joint angle using a single inertial sensor. J. Rehabil. Assist. Technol. Eng. 2019, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, H.; Kim, B.; Park, S. Prediction of Lower Limb Kinetics and Kinematics during Walking by a Single IMU on the Lower Back Using Machine Learning. Sensors 2019, 20, 130. [Google Scholar] [CrossRef] [Green Version]
- Stetter, B.J.; Ringhof, S.; Krafft, F.C.; Sell, S.; Stein, T. Estimation of Knee Joint Forces in Sport Movements Using Wearable Sensors and Machine Learning. Sensors 2019, 19, 3690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaroug, A.; Lai, D.T.H.; Mudie, K.; Begg, R. Lower Limb Kinematics Trajectory Prediction Using Long Short-Term Memory Neural Networks. Front. Bioeng. Biotechnol. 2020, 8, 362. [Google Scholar] [CrossRef]
- Brunner, T.; Lauffenburger, J.-P.; Changey, S.; Basset, M. Magnetometer-Augmented IMU Simulator: In-Depth Elaboration. Sensors 2015, 15, 5293–5310. [Google Scholar] [CrossRef] [PubMed]
- Mundt, M.; Thomsen, W.; Witter, T.; Koeppe, A.; David, S.; Bamer, F.; Potthast, W.; Markert, B. Prediction of lower limb joint angles and moments during gait using artificial neural networks. Med. Biol. Eng. Comput. 2019, 58, 211–225. [Google Scholar] [CrossRef]
- Zimmermann, T.; Taetz, B.; Bleser, G. IMU-to-Segment Assignment and Orientation Alignment for the Lower Body Using Deep Learning. Sensors 2018, 18, 302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, A.D.; Ling, M.J.; Arvind, D.K. IMUSim: A simulation environment for inertial sensing algorithm design and evaluation. In Proceedings of the IPSN 2011: The 10th International Conference on Information Processing in Sensor Networks, Chicago, IL, USA, 12–14 April 2011; pp. 199–210. [Google Scholar]
- Mundt, M.; Koeppe, A.; David, S.; Witter, T.; Bamer, F.; Potthast, W.; Markert, B. Estimation of Gait Mechanics Based on Simulated and Measured IMU Data Using an Artificial Neural Network. Front. Bioeng. Biotechnol. 2020, 8, 41. [Google Scholar] [CrossRef] [PubMed]
- Dorschky, E.; Nitschke, M.; Martindale, C.F.; Bogert, A.V.D.; Koelewijn, A.D.; Eskofier, B.M. CNN-Based Estimation of Sagittal Plane Walking and Running Biomechanics From Measured and Simulated Inertial Sensor Data. Front. Bioeng. Biotechnol. 2020, 8, 604. [Google Scholar] [CrossRef]
- Delp, S.L.; Anderson, F.C.; Arnold, A.S.; Loan, P.; Habib, A.; John, C.T.; Guendelman, E.; Thelen, D.G. OpenSim: Open-Source Software to Create and Analyze Dynamic Simulations of Movement. IEEE Trans. Biomed. Eng. 2007, 54, 1940–1950. [Google Scholar] [CrossRef] [Green Version]
- Renani, M.S.; Myers, C.A.; Zandie, R.; Mahoor, M.H.; Davidson, B.S.; Clary, C.W. Deep Learning in Gait Parameter Prediction for OA and TKA Patients Wearing IMU Sensors. Sensors 2020, 20, 5553. [Google Scholar] [CrossRef] [PubMed]
- Vydhyanathan, A.; Bellusci, G. XSens Mti-G White Paper: The Next Generation Xsens Motion Trackers for Industrial Applications; Xsens: Enschede, The Netherlands, 2015; pp. 1–10. [Google Scholar]
- Myers, C.A.; Laz, P.; Shelburne, K.B.; Judd, D.L.; Huff, D.N.; Winters, J.D.; Stevens-Lapsley, J.; Rullkoetter, P.J. The impact of hip implant alignment on muscle and joint loading during dynamic activities. Clin. Biomech. 2018, 53, 93–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Um, T.T.; Pfister, F.M.J.; Pichler, D.; Endo, S.; Lang, M.; Hirche, S.; Fietzek, U.; Kulic, D. Data augmentation of wearable sensor data for Parkinson’s disease monitoring using convolutional neural networks. In Proceedings of the ICMI 2017—Proceedings of the 19th ACM International Conference on Multimodal Interaction, Glasgow, UK, 13–17 November 2017. [Google Scholar]
- Tran, L.; Choi, D. Data Augmentation for Inertial Sensor-Based Gait Deep Neural Network. IEEE Access 2020, 8, 12364–12378. [Google Scholar] [CrossRef]
- Wen, Q.; Sun, L.; Song, X.; Gao, J.; Wang, X.; Xu, H. Time Series Data Augmentation for Deep Learning: A Survey. arXiv 2020, arXiv:2002.12478. [Google Scholar]
- Choi, A.; Jung, H.; Mun, J.H. Single Inertial Sensor-Based Neural Networks to Estimate COM-COP Inclination Angle During Walking. Sensors 2019, 19, 2974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Żuk, M.; Pezowicz, C. Kinematic Analysis of a Six-Degrees-of-Freedom Model Based on ISB Recommendation: A Repeatability Analysis and Comparison with Conventional Gait Model. Appl. Bionics Biomech. 2015, 2015, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Hochreiter, S.; Schmidhuber, J. Long Short-Term Memory. Neural. Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef]
- Siami-Namini, S.; Tavakoli, N.; Namin, A.S. The Performance of LSTM and BiLSTM in Forecasting Time Series. In Proceedings of the Proceedings—2019 IEEE International Conference on Big Data, Los Angeles, CA, USA, 9–12 December 2019. [Google Scholar]
- Burton, W.S.; Myers, C.A.; Rullkoetter, P.J. Machine learning for rapid estimation of lower extremity muscle and joint loading during activities of daily living. J. Biomech. 2021, 123, 110439. [Google Scholar] [CrossRef]
- Kingma, D.P.; Ba, J.L. Adam: A method for stochastic optimization. In Proceedings of the 3rd International Conference on Learning Representations, ICLR 2015—Conference Track Proceedings, San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- Raschka, S. Model evaluation, model selection, and algorithm selection in machine learning Performance Estimation: Generalization Performance vs. Model Selection. arXiv 2018, arXiv:1810.02513. [Google Scholar]
- Ruiz, N.; Schulter, S.; Chandraker, M. Learning to simulate. arXiv 2018, arXiv:1810.02513. [Google Scholar]
- Rapp, E.; Shin, S.; Thomsen, W.; Ferber, R.; Halilaj, E. Estimation of kinematics from inertial measurement units using a combined deep learning and optimization framework. J. Biomech. 2021, 116, 110229. [Google Scholar] [CrossRef] [PubMed]
- Mundt, M.; Koeppe, A.; Bamer, F.; David, S.; Markert, B. Artificial Neural Networks in Motion Analysis—Applications of Unsupervised and Heuristic Feature Selection Techniques. Sensors 2020, 20, 4581. [Google Scholar] [CrossRef] [PubMed]
- Benoit, D.L.; Ramsey, D.; Lamontagne, M.; Xu, L.; Wretenberg, P.; Renström, P. Effect of skin movement artifact on knee kinematics during gait and cutting motions measured in vivo. Gait Posture 2006, 24, 152–164. [Google Scholar] [CrossRef]
- Myers, C.A.; Laz, P.; Shelburne, K.B.; Davidson, B.S. A Probabilistic Approach to Quantify the Impact of Uncertainty Propagation in Musculoskeletal Simulations. Ann. Biomed. Eng. 2014, 43, 1098–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mundt, M.; Johnson, W.R.; Potthast, W.; Markert, B.; Mian, A.; Alderson, J. A Comparison of Three Neural Network Approaches for Estimating Joint Angles and Moments from Inertial Measurement Units. Sensors 2021, 21, 4535. [Google Scholar] [CrossRef] [PubMed]
- Zrenner, M.; Gradl, S.; Jensen, U.; Ullrich, M.; Eskofier, B.M. Comparison of Different Algorithms for Calculating Velocity and Stride Length in Running Using Inertial Measurement Units. Sensors 2018, 18, 4194. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, K.R.; Hughes, C.; Morrey, B.F.; Morrey, M.; An, K.-N. Gait characteristics of patients with knee osteoarthritis. J. Biomech. 2001, 34, 907–915. [Google Scholar] [CrossRef]
- Kiss, R.M.; Bejek, Z.; Szendrõi, M. Variability of gait parameters in patients with total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1252–1260. [Google Scholar] [CrossRef] [PubMed]
- Sparkes, V.; Whatling, G.M.; Biggs, P.; Khatib, N.; Al-Amri, M.; Williams, D.; Hemming, R.; Hagen, M.; Saleem, I.; Swaminathan, R.; et al. Comparison of gait, functional activities, and patient-reported outcome measures in patients with knee osteoarthritis and healthy adults using 3D motion analysis and activity monitoring: An exploratory case-control analysis. Orthop. Res. Rev. 2019, 11, 129–140. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | n-Layers Evaluated | Hidden Sizes Evaluated | Optimal n-Layer | Optimal Hidden Size |
|---|---|---|---|---|
| Hip-BiLSTM | 1, 2, 3, 4 | 16, 32, 64, 96, 128 | 1 | 32 |
| Knee-BiLSTM | 1, 2, 3, 4 | 16, 32, 64, 96, 128 | 1 | 128 |
| Segment | IMU DoF | Angular Velocity (rad/s) | Acceleration (m/s2) | ||||
|---|---|---|---|---|---|---|---|
| r | RMSE | nRMSE | r | RMSE | nRMSE | ||
| (Mean ± Std) | (Mean ± Std) | (Mean ± Std) | (Mean ± Std) | (Mean ± Std) | (Mean ± Std) | ||
| Pelvis | x | 0.62 ± 0.15 | 0.40 ± 0.17 | 19.47 ± 4.90 | 0.88 ± 0.10 | 0.65 ± 0.30 | 11.03 ± 3.79 |
| y | 0.29 ± 0.24 | 0.36 ± 0.15 | 32.28 ± 11.00 | 0.79 ± 0.12 | 0.62 ± 0.23 | 12.15 ± 3.02 | |
| z | 0.52 ± 0.32 | 0.46 ± 0.21 | 26.58 ± 9.02 | 0.86 ± 0.11 | 0.75 ± 0.33 | 11.16 ± 3.76 | |
| Left Thigh | x | 0.67 ± 0.13 | 0.71 ± 0.19 | 16.22 ± 4.39 | 0.88 ± 0.10 | 1.64 ± 0.71 | 9.19 ± 3.37 |
| y | 0.61 ± 0.23 | 0.48 ± 0.16 | 23.64 ± 8.01 | 0.75 ± 0.23 | 1.12 ± 0.59 | 11.45 ± 4.90 | |
| z | 0.95 ± 0.05 | 0.40 ± 0.20 | 8.56 ± 4.03 | 0.84 ± 0.12 | 1.17 ± 0.59 | 9.79 ± 3.23 | |
| Left Shank | x | 0.83 ± 0.11 | 0.63 ± 0.17 | 10.5 ± 3.67 | 0.96 ± 0.03 | 1.51 ± 0.70 | 5.32 ± 1.90 |
| y | 0.85 ± 0.21 | 0.33 ± 0.15 | 11.79 ± 7.33 | 0.81 ± 0.19 | 1.51 ± 0.82 | 9.82 ± 4.95 | |
| z | 0.98 ± 0.02 | 0.47 ± 0.18 | 5.22 ± 1.81 | 0.92 ± 0.05 | 1.31 ± 0.51 | 8.00 ± 2.12 | |
| Left Foot | x | 0.39 ± 0.41 | 1.02 ± 0.34 | 20.24 ± 8.14 | 0.95 ± 0.04 | 2.46 ± 1.02 | 5.66 ± 2.11 |
| y | 0.98 ± 0.02 | 0.69 ± 0.27 | 4.69 ± 1.53 | 0.85 ± 0.15 | 2.15 ± 1.15 | 8.39 ± 4.08 | |
| z | 0.85 ± 0.17 | 0.79 ± 0.24 | 11.16 ± 4.49 | 0.87 ± 0.08 | 2.33 ± 1.10 | 9.30 ± 2.65 | |
| Training Set | # Samples | Hip Flex–Ext | Hip Ad–Ab | Hip Int–Ext | Hip Average | ||||||||
| r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | ||
| Measured | 3943 | 0.88 ± 0.12 | 7.2 ± 5.0 | 15.4 ± 10.8 | 0.94 ± 0.04 | 2.1 ± 0.7 | 10.1 ± 3.2 | 0.64 ± 0.24 | 4.2 ± 2.0 | 23.9 ± 11.1 | 0.82 ± 0.13 | 4.5 ± 1.6 | 16.5 ± 8.4 |
| Synthetic | 17,255 | 0.98 ± 0.03 | 2.6 ± 1.5 | 5.7 ± 3.2 | 0.95 ± 0.05 | 2.0 ± 0.6 | 9.5 ± 2.9 | 0.81 ± 0.17 | 2.3 ± 0.8 | 12.8 ± 4.6 | 0.91 ± 0.08 | 2.3 ± 0.3 | 9.3 ± 3.6 |
| Measured + Synthetic | 20,706 | 0.98 ± 0.01 | 2.6 ± 1.1 | 5.5 ± 2.3 | 0.98 ± 0.02 | 1.3 ± 0.5 | 6.1 ± 2.2 | 0.93 ± 0.07 | 1.7 ± 0.6 | 9.8 ± 3.5 | 0.96 ± 0.03 | 1.9 ± 0.2 | 7.1 ± 2.7 |
| Training Set | # Samples | Knee Flex–Ext | Knee Ad–Ab | Knee Int–Ext | Knee Average | ||||||||
| r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | r | RMSE (°) | nRMSE | ||
| Measured | 3943 | 0.99 ± 0.01 | 2.9 ± 1.1 | 3.9 ± 1.6 | 0.75 ± 0.22 | 2.0 ± 0.8 | 15.2 ± 6.3 | 0.77 ± 0.14 | 7.0 ± 1.8 | 25.5 ± 6.3 | 0.83 ± 0.12 | 3.3 ± 0.2 | 14.9 ± 4.7 |
| Synthetic | 17,255 | 0.99 ± 0.01 | 2.1 ± 0.6 | 2.9 ± 0.8 | 0.82 ± 0.13 | 2.0 ± 0.6 | 15.1 ± 4.5 | 0.70 ± 0.24 | 6.4 ± 2.8 | 24.0 ± 11.3 | 0.84 ± 0.12 | 2.9 ± 0.7 | 14.0 ± 5.5 |
| Measured + Synthetic | 20,706 | 0.99 ± 0.01 | 1.4 ± 0.5 | 1.9 ± 0.7 | 0.94 ± 0.06 | 1.2 ± 0.4 | 6.6 ± 2.3 | 0.93 ± 0.07 | 3.8 ± 1.6 | 14.1 ± 6.4 | 0.96 ± 0.04 | 1.7 ± 0.4 | 7.5 ± 3.1 |
| DoF | Reference | Sensor Configuration | # Subjects | # Cycles | Data Type | Activity | r | RMSE(°) | nRMSE |
|---|---|---|---|---|---|---|---|---|---|
| Hip Flex–Ext | Current | P T S F | 27 | 3943 + 17,255 | Measured + Synthetic | Gait | 0.98 | 2.6 | 5.5 |
| Mundt 2020a (PS-Net) [43] | P S | 115 | 88,067 | Simulated | Gait | 0.98 | 1.6 | NR | |
| Mundt 2020b (FFNN) [25] | P T S | 93 | 3098 + 46,437 | Measured + Simulated | Gait | 0.99 | 5.2 | NR | |
| Mundt 2019 (FFNN) [22] | P T S F | 75 | 1028 | Simulated | Gait | 0.99 | 1.3 | NR | |
| Dorschky 2020 (CNN) [26] | P T S F | 7 | 418 + 6688 | Measured + Synthetic | Gait and Running | 1 | 5.1 | NR | |
| Rapp 2021 (LSTM) [42] | P T S F | 420 | NR | Simulated | Gait | NR | 4.3 | NR | |
| Gholami 2020 (CNN) [10] | F | 10 | NR | Simulated | Running | 0.8 | 5.6 | 9.9 | |
| Hip Ad–Ab | Current | P T S F | 27 | 3943 + 17,255 | Measured + Synthetic | Gait | 0.98 | 1.3 | 6.1 |
| Mundt 2020a (PS-Net) | P S | 115 | 88,067 | Simulated | Gait | 0.94 | 0.9 | NR | |
| Mundt 2020b (FFNN) | P T S | 93 | 3098 + 46,437 | Measured + Simulated | Gait | 0.96 | 2.1 | NR | |
| Mundt 2019 (FFNN) | P T S F | 75 | 1028 | Simulated | Gait | 0.98 | 1.3 | NR | |
| Rapp 2021 (LSTM) | P T S F | 420 | NR | Simulated | Gait | NR | 2.7 | NR | |
| Hip Int–Ext | Current | P T S F | 27 | 3943 + 17,255 | Measured + Synthetic | Gait | 0.93 | 1.7 | 9.8 |
| Mundt 2020a (PS-Net) | P S | 115 | 88,067 | Simulated | Gait | 0.64 | 2.1 | NR | |
| Mundt 2020b (FFNN) | P T S | 93 | 3098 + 46,437 | Measured + Simulated | Gait | 0.88 | 5.2 | NR | |
| Mundt 2019 (FFNN) | P T S F | 75 | 1028 | Simulated | Gait | 0.86 | 2.5 | NR | |
| Rapp 2021 (LSTM) | P T S F | 420 | NR | Simulated | Gait | NR | 5.2 | NR | |
| Hip Average | Current | P T S F | 27 | 3943 + 17,255 | Measured + Synthetic | Gait | 0.96 | 1.9 | 7.1 |
| Mundt 2020a (PS-Net) | P S | 115 | 88,067 | Simulated | Gait | 0.85 | 1.5 | NR | |
| Mundt 2020b (FFNN) | P T S | 93 | 3098 + 46,437 | Measured + Simulated | Gait | 0.94 | 4.2 | NR | |
| Mundt 2019 (FFNN) | P T S F | 75 | 1028 | Simulated | Gait | 0.94 | 1.7 | NR | |
| Rapp 2021 (LSTM) | P T S F | 420 | NR | Simulated | Gait | NR | 4.1 | NR |
| DoF | Reference | Sensor Configuration | # Subjects | # Cycles | Data Type | Activity | r | RMSE(°) | nRMSE |
|---|---|---|---|---|---|---|---|---|---|
| Knee Flex–Ext | Current | P T S F | 27 | 3943 + 17,255 | Measured + Synthetic | Gait | 0.99 | 1.4 | 1.9 |
| Mundt 2020a (PS-Net) | P S | 115 | 88,067 | Simulated | Gait | 0.99 | 1.7 | NR | |
| Mundt 2020b (FFNN) | P T S | 93 | 3098 + 46,437 | Measured + Simulated | Gait | 0.98 | 4.5 | NR | |
| Mundt 2019 (FFNN) | P T S F | 75 | 1028 | Simulated | Gait | 0.99 | 1.4 | NR | |
| Dorschky 2020 (CNN) | P T S F | 7 | 418 + 6688 | Measured + Synthetic | Gait & Running | 0.99 | 4.8 | NR | |
| Rapp 2021 (LSTM) | P T S F | 420 | NR | Simulated | Gait | NR | 3.1 | NR | |
| Gholami 2020 (CNN) | F | 10 | NR | Simulated | Running | 0.93 | 6.5 | 6.5 | |
| Knee Ad–Ab | Current | P T S F | 27 | 3943 + 17,255 | Measured + Synthetic | Gait | 0.94 | 1.2 | 6.6 |
| Mundt 2020a (PS-Net) | P S | 115 | 88,067 | Simulated | Gait | 0.95 | 1.5 | NR | |
| Mundt 2020b (FFNN) | P T S | 93 | 3098 + 46,437 | Measured + Simulated | Gait | 0.80 | 2.5 | NR | |
| Mundt 2019 (FFNN) | P T S F | 75 | 1028 | Simulated | Gait | 0.79 | 1.6 | NR | |
| Rapp 2021 (LSTM) | P T S F | 420 | NR | Simulated | Gait | NR | 3.2 | NR | |
| Knee Int–Ext | Current | P T S F | 27 | 3943 + 17,255 | Measured + Synthetic | Gait | 0.93 | 2.8 | 14.1 |
| Mundt 2020a (PS-Net) | P S | 115 | 88,067 | Simulated | Gait | 0.93 | 2.5 | NR | |
| Mundt 2020b (FFNN) | P T S | 93 | 3098 + 46,437 | Measured + Simulated | Gait | 0.97 | 5.5 | NR | |
| Mundt 2019 (FFNN) | P T S F | 75 | 1028 | Simulated | Gait | 0.95 | 1.7 | NR | |
| Rapp 2021 (LSTM) | P T S F | 420 | NR | Simulated | Gait | NA | 6.4 | NR | |
| Knee Average | Current | P T S F | 27 | 3943 + 17,255 | Measured + Synthetic | Gait | 0.96 | 1.7 | 7.5 |
| Mundt 2020a (PS-Net) | P S | 115 | 88,067 | Simulated | Gait | 0.95 | 1.9 | NR | |
| Mundt 2020b (FFNN) | P T S | 93 | 3098 + 46,437 | Measured + Simulated | Gait | 0.92 | 4.2 | NR | |
| Mundt 2019 (FFNN) | P T S F | 75 | 1028 | Simulated | Gait | 0.91 | 1.6 | NR | |
| Rapp 2021 (LSTM) | P T S F | 420 | NR | Simulated | Gait | NA | 4.2 | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharifi Renani, M.; Eustace, A.M.; Myers, C.A.; Clary, C.W. The Use of Synthetic IMU Signals in the Training of Deep Learning Models Significantly Improves the Accuracy of Joint Kinematic Predictions. Sensors 2021, 21, 5876. https://doi.org/10.3390/s21175876
Sharifi Renani M, Eustace AM, Myers CA, Clary CW. The Use of Synthetic IMU Signals in the Training of Deep Learning Models Significantly Improves the Accuracy of Joint Kinematic Predictions. Sensors. 2021; 21(17):5876. https://doi.org/10.3390/s21175876
Chicago/Turabian StyleSharifi Renani, Mohsen, Abigail M. Eustace, Casey A. Myers, and Chadd W. Clary. 2021. "The Use of Synthetic IMU Signals in the Training of Deep Learning Models Significantly Improves the Accuracy of Joint Kinematic Predictions" Sensors 21, no. 17: 5876. https://doi.org/10.3390/s21175876
APA StyleSharifi Renani, M., Eustace, A. M., Myers, C. A., & Clary, C. W. (2021). The Use of Synthetic IMU Signals in the Training of Deep Learning Models Significantly Improves the Accuracy of Joint Kinematic Predictions. Sensors, 21(17), 5876. https://doi.org/10.3390/s21175876