
Sensors for Context-Aware Smart Healthcare: A Security Perspective

 , , , and
, , , and 
Abstract
:1. Introduction
- The complete variety of attributes related to people’s health status and their context must be considered so that the s-health service is as beneficial as possible. Sensing devices must be properly selected in accordance with their inner requirements such as accuracy, reliability, dimensions, computational capabilities, cost or power consumption, among others.
- Proper communication technologies must be favoured according to the specifications of the sensing devices and considering the complex nature of WSNs and WBANs. Scalability, density, coverage area and security are important aspects to be taken in mind for communications.
- All s-health-related ICT components must meet with the highest security requirements to thwart malicious activities. All in all, information security and data privacy, as well as the adequate protection of devices, networks and services, is first and foremost.
2. Sensors: Definition and Taxonomy
2.1. User-Centric Sensors
2.1.1. Cardiovascular Activity
2.1.2. Temperature
2.1.3. Respiratory Rate
2.1.4. Brain Activity
2.1.5. Muscular Activity
2.1.6. Electrodermal Activity
2.1.7. Hydration
2.1.8. Location
2.1.9. Body Motion
2.2. Contextual Sensors
2.2.1. Air Temperature
2.2.2. Air Humidity
2.2.3. Barometric Pressure
2.2.4. Air Pollution
2.2.5. Water Contamination
2.2.6. Acoustic Contamination
2.2.7. Electromagnetic Radiation
2.2.8. Seismic Activity
3. Communication Architecture and Technologies
3.1. WBAN Communication Architecture
- Intra-WBAN communications (Tier 1): This tier enables communications between the sensors and actuators (i.e., nodes) placed in, on and around the human body, in a range of approximately two meters. In addition to the direct communications among these nodes, they can also communicate with a sink, a portable device attached to the body, to transmit the user-centric data. The sink, which usually refers to a smartphone in the s-health context, is the WBAN coordinator and gateway to the next tier. Short-range and low-energy communication technologies are desirable in this tier.
- Inter-WBAN communications (Tier 2): This tier aims to connect the users’ WBANs with external networks that are easily accessible for other users, such as the Internet and cellular networks. Hence, the communications in this tier take place between the sink and one or more access points, which are gateways to those networks. Large-range communication technologies, such as ZigBee, BLE, Wi-Fi and cellular, were adopted in this tier.
- Beyond-WBAN communications (Tier 3): The communications in this tier refer to those from the health provider. Having received the user-centric data from the previous tier, it was stored in the healthcare information system (HIS) and then, analysed by physicians, medical staff or automatised systems may act accordingly. With the medical records and the profiles of patients, smart healthcare systems can automate real-time diagnosis, adjust medical treatments or alert the emergency services, relatives and caregivers if needed.
3.2. Wireless Communication Technologies
3.2.1. Bluetooth
3.2.2. ZigBee
3.2.3. IEEE 802.15.6
3.2.4. Wi-Fi
3.2.5. Cellular Networks
3.2.6. Low-Power Wide-Area Networks
3.2.7. Other Technologies
3.3. Evaluation of Wireless Technologies
4. Information Security: Requirements, Attacks and Solutions
4.1. Security Requirements
- Confidentiality: Data confidentiality is the property that guarantees that data are only disclosed to authorised entities (e.g., people, devices, processes…), whilst remaining unintelligible to unauthorised entities. User-centric data, but especially the medical, must be kept confidential during storage periods (susceptible to data leakages) and while being conveyed through the communication networks (susceptible to eavesdropping). The most widely used technique to achieve confidentiality is encryption, in which only authorised entities have access to the secret key required to decode the data.
- Integrity: Data integrity ensures the accuracy, trustworthiness and completeness of data, guaranteeing that the data have not been modified or destroyed by unauthorised entities. For instance, attackers might tamper the data without authorisation during its transmission over the network. Unless properly detected, smart healthcare systems would react to users upon faux data, and potentially endanger their health. Moreover, other non-related human events can also threat integrity, such as hardware glitches. Integrity-oriented protections include cryptographic hashes for detecting data modifications, and redundancy and backup policies enable restoring any affected data if necessary.
- Availability: Data availability guarantees that authorised entities have constant access to the data regardless of their location and time. This property allows the proper functioning of the sensing devices, the communication channels and the information systems at a whole. Smart healthcare systems must guarantee the availability of medical data, since decisions might be made anytime and anywhere. Hence, they must be resilient to service disruptions: either intentional from attackers denying services to legitimate users, or accidental due to natural disasters, hardware failures or system upgrades that require systems breakdowns. Redundancy, recovery policies and fail-over strategies should be considered to avoid availability issues.
- Non-repudiation: Non-repudiation is the guarantee that a particular interaction between two entities actually occurred. This means that, given the communication of a message between two authorised entities in a system, the sender cannot deny having sent a message to the receiver in the future, and the receiver cannot deny having received the message from the sender in the future. Although cryptographic digital signatures can help achieve this property, it is noteworthy that their use in some sensing devices might be limited due to their computational constraints.
- Authentication and authorisation: Authentication and authorisation mechanisms are commonly misconceived or interchanged. On the one hand, authentication refers to the process of confirming the identity of an entity, i.e., determining whether the entity is who it claims to be. On the other hand, authorisation refers to the process of determining whether the authenticated entity has access to the particular resources and services of the system. Within smart healthcare systems, authentication procedures are mandatory in order to establish communications only with properly authenticated entities, and avoiding any communication with illegitimate entities. In general, this is achieved through credentials, e.g., passwords, biometrics or digital certificates. In the case of successful authentication, then systems must ensure whether the entities have permission to do the actions that aim to (e.g., access, modify or delete medical information).
- Privacy: Privacy is a fundamental right that has to be protected. Smart healthcare systems must process personal data in a lawful, fair and transparent manner for a specific, limited and legitimate purpose. Besides, due to the sensitivity of the data, they require the explicit individuals’ consent for their managing and be compliant with the current regulations on data privacy. These systems must adopt the appropriate safeguards to reduce disclosure risks, including identity disclosure, i.e., the direct re-identification of individuals, and attribute disclosure, i.e., the inference of confidential information to a certain individual. Hence, in the case of data leakages or eavesdropping, people’s privacy is not jeopardised. One of the most common data sanitisation techniques for privacy protection is data anonymisation.
4.2. Security Attacks, Threats and Vulnerabilities
- Based on the attack’s nature: passive attacks and active attacks [21]. In passive attacks, attackers monitor and collect information from the system and exploit it to launch further attacks. This kind of attacks does not harm the system, hence victims are not aware of them. On the contrary, active attacks are intended to modify or damage the system by injecting, altering or destroying data or services. Since these attacks impact the systems, victims are informed of them.
- Based on the attack’s origin: internal attacks and external attacks [21]. Internal attacks are initiated by malicious entities located inside the system, i.e., insider attackers. In contrast, external attacks are launched by external entities located outside the system, i.e., outsider attackers.
- Based on the attack’s launch method: physical methods, logical/software-based methods and side-channel methods [272]. Physical methods refer to the attacker’s ability to have physical access to the cyber-physical system in an unauthorised way. Logical or software-based methods exploit vulnerabilities and expose errors in logical systems, such as software, operating systems, applications or protocols, to gain illegitimate access. Side-channel methods observe the indirect physical effects of the systems during their functioning to acquire advanced knowledge.
- Based on the TCP/IP model layer: application layer, transport layer, network layer and network interface layer [272]. Attackers can target different layers of the TCP/IP model to find weaknesses and infiltrate the system. Similar classifications can be performed using the OSI model.
4.2.1. Attacks against Nodes
Node Capture Attacks
False Data Injection Attacks
Sleep Deprivation Attacks
Side-Channel Attacks
Firmware Update Attacks
4.2.2. Attacks against Communications
Eavesdropping
Data Tampering
Replay Attacks
Spoofing Attacks
Man-in-the-Middle Attacks
Denial of Service Attacks
4.2.3. Attacks against HIS
Malware
Data Leakage
4.2.4. Attacks against Users
Phishing Attacks
4.3. Security Solutions
4.3.1. Secure Communications
Lightweight Cryptography
Key Management
4.3.2. Always-On Systems
Secure Routing
DDoS Countermeasures
4.3.3. Trust Management
Authentication Protocols
Access Control Mechanisms
Intrusion Detection Systems
Traceability of Digital Evidence
4.3.4. Data Protection
Privacy Protection Models
Awareness Programmes
5. Future Challenges and Research Opportunities
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| ABE | Attribute-Based Encryption |
| ABG | Arterial Blood Gas |
| AES | Advanced Encryption Standard |
| AI | Artificial Intelligence |
| ARP | Address Resolution Protocol |
| BCG | Ballistocardiography |
| BLE | Bluetooth Low Energy |
| COPD | Chronic Obstructive Pulmonary Disease |
| DDoS | Distributed Denial of Service |
| DNS | Domain Name System |
| DoS | Denial of Service |
| ECC | Elliptic-Curve Cryptography |
| ECG | Electrocardiography |
| EDA | Electrodermal Activity |
| EEG | Electroencephalography |
| EMG | Electromyography |
| FBG | Fibre Bragg Grating |
| fNIRS | Functional Near-Infrared Spectroscopy |
| GDPR | General Data Protection Regulation |
| GPS | Global Positioning System |
| HBC | Human Body Communication |
| HIDS | Host-Based Intrusion Detection Systems |
| HIPAA | Health Insurance Portability and Accountability Act |
| HIS | Healthcare Information System |
| HTTP | Hypertext Transfer Protocol |
| ICMP | Internet Control Message Protocol |
| ICT | Information and Communication Technologies |
| ICU | Intensive Care Unit |
| IDS | Intrusion Detection Systems |
| IEC | International Electrotechnical Commission |
| IMU | Inertial Measurement Units |
| IoMT | Internet of Medical Things |
| IoT | Internet of Things |
| IP | Internet Protocol |
| ISO | International Organisation for Standardisation |
| LPWAN | Low-Power Wide-Area Networks |
| LTE | Long-Term Evolution |
| MAC (address) | Media Access Control |
| MAC (code) | Message Authentication Code |
| MEG | Magnetoencephalography |
| MEMS | Microelectromechanical Systems |
| MitM | Man-in-the-Middle |
| MMG | Mechanomyography |
| MOS | Metal Oxide Semiconductor |
| NB | Narrowband |
| NFC | Near-Field Communication |
| NIDS | Network-Based Intrusion Detection Systems |
| OSI | Open Systems Interconnection |
| OSINT | Open Source Intelligence |
| PCG | Phonocardiography |
| PET | Positron-Emission Tomography |
| PPG | Photoplethysmography |
| PTT | Pulse Transit Time |
| RBAC | Role-Based Access Control |
| RFID | Radio Frequency Identification |
| RGB | Red Green Blue |
| RSA | Rivest–Shamir–Adleman |
| RTS/CTS | Request to Send/Clear To Send |
| SHA | Secure Hash Algorithm |
| TCP | Transmission Control Protocol |
| UV | Ultraviolet |
| UWB | Ultra Wideband |
| WBAN | Wireless Body Area Networks |
| WPA | Wi-Fi Protected Access |
| WPS | WiFi-based Positioning System |
| WSN | Wireless Sensor Networks |
References
- Solanas, A.; Patsakis, C.; Conti, M.; Vlachos, I.S.; Ramos, V.; Falcone, F.; Postolache, O.; Pérez-Martínez, P.A.; Di Pietro, R.; Perrea, D.N.; et al. Smart health: A context-aware health paradigm within smart cities. IEEE Commun. Mag. 2014, 52, 74–81. [Google Scholar] [CrossRef]
- Eysenbach, G. What is e-health? J. Med. Internet Res. 2001, 3, e20. [Google Scholar] [CrossRef]
- Istepanian, R.S.; Laxminarayan, S.; Pattichis, C. (Eds.) M-Health—Emerging Mobile Health Systems; Topics in Biomedical Engineering; Springer: New York, NY, USA, 2006. [Google Scholar]
- Solanas, A.; Casino, F.; Batista, E.; Rallo, R. Trends and Challenges in Smart Healthcare Research: A Journey from Data to Wisdom. In Proceedings of the IEEE 3rd International Forum on Research and Technologies for Society and Industry, Modena, Italy, 11–13 September 2017; pp. 1–6. [Google Scholar]
- Casino, F.; Patsakis, C.; Batista, E.; Borràs, F.; Martínez-Ballesté, A. Healthy Routes in the Smart City. IEEE Softw. 2017, 34, 42–47. [Google Scholar] [CrossRef]
- Patsakis, C.; Papageorgiou, A.; Falcone, F.; Solanas, A. s-Health as a driver towards better emergency response systems in urban environments. In Proceedings of the 10th IEEE International Symposium on Medical Measurements and Application, Turin, Italy, 7–9 May 2015; pp. 214–218. [Google Scholar]
- Sundaravadivel, P.; Kougianos, E.; Mohanty, S.P.; Ganapathiraju, M.K. Everything You Wanted to Know about Smart Health Care: Evaluating the Different Technologies and Components of the Internet of Things for Better Health. IEEE Consum. Electron. Mag. 2017, 7, 18–28. [Google Scholar] [CrossRef]
- Movassaghi, S.; Abolhasan, M.; Lipman, J.; Smith, D.; Jamalipour, A. Wireless Body Area Networks: A Survey. IEEE Commun. Surv. Tutorials 2014, 16, 1658–1686. [Google Scholar] [CrossRef]
- Salayma, M.; Al-Dubai, A.; Romdhani, I.; Nasser, Y. Wireless Body Area Network (WBAN) A Survey on Reliability, Fault Tolerance, and Technologies Coexistence. ACM Comput. Surv. 2017, 50, 1–38. [Google Scholar] [CrossRef] [Green Version]
- Aguirre, E.; Lopez-Iturri, P.; Azpilicueta, L.; Redondo, A.; Astrain, J.J.; Villadangos, J.; Bahillo, A.; Perallos, A.; Falcone, F. Design and Implementation of Context Aware Applications WITH Wireless Sensor Network Support in Urban Train Transportation Environments. IEEE Sens. J. 2016, 17, 169–178. [Google Scholar] [CrossRef]
- Lombardo, L.; Corbellini, S.; Parvis, M.; Elsayed, A.; Angelini, E.; Grassini, S. Wireless Sensor Network for Distributed Environmental Monitoring. IEEE Trans. Instrum. Meas. 2017, 67, 1214–1222. [Google Scholar] [CrossRef]
- Czeschik, C. Black Market Value of Patient Data. In Digital Marketplaces Unleashed; Springer: Berlin/Heidelberg, Germany, 2018; pp. 883–893. [Google Scholar]
- Yao, M. Your Electronic Medical Records Could Be Worth $1000 To Hackers. Available online: https://www.forbes.com/sites/mariyayao/2017/04/14/your-electronic-medical-records-can-be-worth-1000-to-hackers/ (accessed on 1 August 2021).
- Yetisen, A.K.; Martinez-Hurtado, J.L.; Ünal, B.; Khademhosseini, A.; Butt, H. Wearables in Medicine. Adv. Mater. 2018, 30, 1706910. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.B.; Xiang, W.; Atkinson, I. Internet of Things for Smart Healthcare: Technologies, Challenges, and Opportunities. IEEE Access 2017, 5, 26521–26544. [Google Scholar] [CrossRef]
- Dian, F.J.; Vahidnia, R.; Rahmati, A. Wearables and the Internet of Things (IoT), Applications, Opportunities, and Challenges: A Survey. IEEE Access 2020, 8, 69200–69211. [Google Scholar] [CrossRef]
- Seneviratne, S.; Hu, Y.; Nguyen, T.; Lan, G.; Khalifa, S.; Thilakarathna, K.; Hassan, M.; Seneviratne, A. A survey of wearable devices and challenges. IEEE Commun. Surv. Tutorials 2017, 19, 2573–2620. [Google Scholar] [CrossRef]
- Negra, R.; Jemili, I.; Belghith, A. Wireless Body Area Networks: Applications and technologies. Proc. Comput. Sci. 2016, 83, 1274–1281. [Google Scholar] [CrossRef] [Green Version]
- Khan, R.A.; Pathan, A.S.K. The state-of-the-art wireless body area sensor networks: A survey. Int. J. Distrib. Sens. Netw. 2018, 14, 1550147718768994. [Google Scholar] [CrossRef] [Green Version]
- Ahad, A.; Tahir, M.; Aman Sheikh, M.; Ahmed, K.I.; Mughees, A.; Numani, A. Technologies Trend towards 5G Network for Smart Health-Care Using IoT: A Review. Sensors 2020, 20, 4047. [Google Scholar] [CrossRef] [PubMed]
- Hajar, M.S.; Al-Kadri, M.O.; Kalutarage, H.K. A survey on wireless body area networks: Architecture, security challenges and research opportunities. Comput. Secur. 2021, 104, 102211. [Google Scholar] [CrossRef]
- Qureshi, F.; Krishnan, S. Wearable Hardware Design for the Internet of Medical Things (IoMT). Sensors 2018, 18, 3812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, S.; Jayaraman, A.; Rogers, J.A. Skin sensors are the future of health care. Nature 2019, 571, 319–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Cardiovascular Diseases (CVDs). Available online: https://www.who.int/health-topics/cardiovascular-diseases (accessed on 27 September 2021).
- Michard, F. A sneak peek into digital innovations and wearable sensors for cardiac monitoring. J. Clin. Monit. Comput. 2017, 31, 253–259. [Google Scholar] [CrossRef]
- Redfern, J. Can Older Adults Benefit from Smart Devices, Wearables, and Other Digital Health Options to Enhance Cardiac Rehabilitation? Clin. Geriatr. Med. 2019, 35, 489–497. [Google Scholar] [CrossRef]
- Kiranyaz, S.; Ince, T.; Gabbouj, M. Personalized Monitoring and Advance Warning System for Cardiac Arrhythmias. Sci. Rep. 2017, 7, 9270. [Google Scholar] [CrossRef]
- Ousaka, D.; Sakano, N.; Morita, M.; Shuku, T.; Sanou, K.; Kasahara, S.; Oozawa, S. A new approach to prevent critical cardiac accidents in athletes by real-time electrocardiographic tele-monitoring system: Initial trial in full marathon. J. Cardiol. Cases 2019, 20, 35–38. [Google Scholar] [CrossRef]
- Nedoma, J.; Fajkus, M.; Martinek, R.; Kepak, S.; Cubik, J.; Zabka, S.; Vasinek, V. Comparison of BCG, PCG and ECG Signals in Application of Heart Rate Monitoring of the Human Body. In Proceedings of the 40th International Conference on Telecommunications and Signal Processing, Barcelona, Spain, 5–7 July 2017; pp. 420–424. [Google Scholar]
- Spanò, E.; Di Pascoli, S.; Iannaccone, G. Low-Power Wearable ECG Monitoring System for Multiple-Patient Remote Monitoring. IEEE Sens. J. 2016, 16, 5452–5462. [Google Scholar] [CrossRef]
- Yang, Z.; Zhou, Q.; Lei, L.; Zheng, K.; Xiang, W. An IoT-cloud Based Wearable ECG Monitoring System for Smart Healthcare. J. Med. Syst. 2016, 40, 286. [Google Scholar] [CrossRef]
- Rachim, V.P.; Chung, W.Y. Wearable Noncontact Armband for Mobile ECG Monitoring System. IEEE Trans. Biomed. Circuits Syst. 2016, 10, 1112–1118. [Google Scholar] [CrossRef] [PubMed]
- Ankhili, A.; Tao, X.; Cochrane, C.; Coulon, D.; Koncar, V. Washable and Reliable Textile Electrodes Embedded into Underwear Fabric for Electrocardiography (ECG) Monitoring. Materials 2018, 11, 256. [Google Scholar] [CrossRef] [Green Version]
- Biswas, D.; Simões-Capela, N.; Van Hoof, C.; Van Helleputte, N. Heart Rate Estimation From Wrist-Worn Photoplethysmography: A Review. IEEE Sens. J. 2019, 19, 6560–6570. [Google Scholar] [CrossRef]
- Fiorini, L.; Cavallo, F.; Martinelli, M.; Rovini, E. Characterization of a PPG Wearable Sensor to be Embedded into an Innovative Ring-Shaped Device for Healthcare Monitoring. In Ambient Assisted Living: Italian Forum 2019; Springer: Cham, Switzerland, 2021; pp. 49–63. [Google Scholar]
- Jo, E.; Lewis, K.; Directo, D.; Kim, M.J.; Dolezal, B.A. Validation of Biofeedback Wearables for Photoplethysmographic Heart Rate Tracking. J. Sport. Sci. Med. 2016, 15, 540. [Google Scholar]
- Chowdhury, S.S.; Hyder, R.; Hafiz, M.S.B.; Haque, M.A. Real-Time Robust Heart Rate Estimation From Wrist-Type PPG Signals Using Multiple Reference Adaptive Noise Cancellation. IEEE J. Biomed. Health Inform. 2016, 22, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Bent, B.; Goldstein, B.A.; Kibbe, W.A.; Dunn, J.P. Investigating sources of inaccuracy in wearable optical heart rate sensors. NPJ Digit. Med. 2020, 3, 18. [Google Scholar] [CrossRef] [Green Version]
- Temko, A. Accurate Heart Rate Monitoring During Physical Exercises Using PPG. IEEE Trans. Biomed. Eng. 2017, 64, 2016–2024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albukhari, A.; Lima, F.; Mescheder, U. Bed-Embedded Heart and Respiration Rates Detection by Longitudinal Ballistocardiography and Pattern Recognition. Sensors 2019, 19, 1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ismail, S.; Siddiqi, I.; Akram, U. Localization and classification of heart beats in phonocardiography signals—A comprehensive review. EURASIP J. Adv. Signal Process. 2018, 2018, 26. [Google Scholar] [CrossRef] [Green Version]
- Cheung, C.C.; Olgin, J.E.; Lee, B.K. Wearable cardioverter-defibrillators: A review of evidence and indications. Trends Cardiovasc. Med. 2021, 31, 196–201. [Google Scholar] [CrossRef]
- Wäßnig, N.K.; Günther, M.; Quick, S.; Pfluecke, C.; Rottstädt, F.; Szymkiewicz, S.J.; Ringquist, S.; Strasser, R.H.; Speiser, U. Experience with the Wearable Cardioverter-Defibrillator in Patients at High Risk for Sudden Cardiac Death. Circulation 2016, 134, 635–643. [Google Scholar] [CrossRef]
- Kutyifa, V.; Moss, A.J.; Klein, H.; Biton, Y.; McNitt, S.; MacKecknie, B.; Zareba, W.; Goldenberg, I. Use of the Wearable Cardioverter Defibrillator in High-Risk Cardiac Patients: Data From the Prospective Registry of Patients Using the Wearable Cardioverter Defibrillator (WEARIT-II Registry). Circulation 2015, 132, 1613–1619. [Google Scholar] [CrossRef]
- Phattraprayoon, N.; Sardesai, S.; Durand, M.; Ramanathan, R. Accuracy of pulse oximeter readings from probe placement on newborn wrist and ankle. J. Perinatol. 2012, 32, 276–280. [Google Scholar] [CrossRef] [Green Version]
- Seifi, S.; Khatony, A.; Moradi, G.; Abdi, A.; Najafi, F. Accuracy of pulse oximetry in detection of oxygen saturation in patients admitted to the intensive care unit of heart surgery: Comparison of finger, toe, forehead and earlobe probes. BMC Nurs. 2018, 17, 15. [Google Scholar] [CrossRef]
- Chen, Q.; Tang, L. A wearable blood oxygen saturation monitoring system based on bluetooth low energy technology. Coputer Commun. 2020, 160, 101–110. [Google Scholar] [CrossRef]
- Davies, H.J.; Williams, I.; Peters, N.S.; Mandic, D.P. In-Ear SpO2: A Tool for Wearable, Unobtrusive Monitoring of Core Blood Oxygen Saturation. Sensors 2020, 20, 4879. [Google Scholar] [CrossRef]
- Ma, G.; Zhu, W.; Zhong, J.; Tong, T.; Zhang, J.; Wang, L. Wearable Ear Blood Oxygen Saturation and Pulse Measurement System Based on PPG. In Proceedings of the IEEE SmartWorld, Ubiquitous Intelligence & Computing, Advanced & Trusted Computing, Scalable Computing & Communications, Cloud & Big Data Computing, Internet of People and Smart City Innovation, Guangzhou, China, 8–12 October 2018; pp. 111–116. [Google Scholar]
- Lochner, C.M.; Khan, Y.; Pierre, A.; Arias, A.C. All-organic optoelectronic sensor for pulse oximetry. Nat. Commun. 2014, 5, 5745. [Google Scholar] [CrossRef] [Green Version]
- Coyle, S.; Lau, K.T.; Moyna, N.; O’Gorman, D.; Diamond, D.; Di Francesco, F.; Costanzo, D.; Salvo, P.; Trivella, M.G.; De Rossi, D.E.; et al. BIOTEX — Biosensing Textiles for Personalised Healthcare Management. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 364–370. [Google Scholar] [CrossRef] [Green Version]
- Arakawa, T. Recent Research and Developing Trends of Wearable Sensors for Detecting Blood Pressure. Sensors 2018, 18, 2772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kachuee, M.; Kiani, M.M.; Mohammadzade, H.; Shabany, M. Cuffless Blood Pressure Estimation Algorithms for Continuous Health-Care Monitoring. IEEE Trans. Biomed. Eng. 2016, 64, 859–869. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Ivanov, K.; Wang, Y.; Wang, L. Toward a Smartphone Application for Estimation of Pulse Transit Time. Sensors 2015, 15, 27303–27321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carek, A.M.; Conant, J.; Joshi, A.; Kang, H.; Inan, O.T. SeismoWatch: Wearable Cuffless Blood Pressure Monitoring Using Pulse Transit Time. In Proceedings of the ACM on Interactive, Mobile, Wearable and Ubiquitous Technologies; Association for Computing Machinery: New York, NY, USA, 2017; Volume 1, pp. 1–16. [Google Scholar]
- Kario, K. Management of Hypertension in the Digital Era: Small Wearable Monitoring Devices for Remote Blood Pressure Monitoring. Hypertension 2020, 76, 640–650. [Google Scholar] [CrossRef]
- Ringrose, J.; Padwal, R. Wearable Technology to Detect Stress-Induced Blood Pressure Changes: The Next Chapter in Ambulatory Blood Pressure Monitoring? Am. J. Hypertens. 2021, 34, 330–331. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Xu, W.; Guan, N.; Ji, D.; Wei, Y.; Yi, W. Noninvasive and Continuous Blood Pressure Monitoring Using Wearable Body Sensor Networks. IEEE Intell. Syst. 2015, 30, 38–48. [Google Scholar] [CrossRef]
- Holz, C.; Wang, E.J. Glabella: Continuously Sensing Blood Pressure Behavior using an Unobtrusive Wearable Device. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2017, 1, 58. [Google Scholar] [CrossRef]
- Chang, S.H.; Chiang, R.D.; Wu, S.J.; Chang, W.T. A Context-Aware, Interactive M-Health System for Diabetics. IT Prof. 2016, 18, 14–22. [Google Scholar] [CrossRef]
- Valenzuela, F.; García, A.; Vázquez, M.; Cortez, J.; Espinoza, A. An IoT-Based Glucose Monitoring Algorithm to Prevent Diabetes Complications. Appl. Sci. 2020, 10, 921. [Google Scholar] [CrossRef] [Green Version]
- Al-Taee, M.A.; Al-Nuaimy, W.; Muhsin, Z.J.; Al-Ataby, A. Robot Assistant in Management of Diabetes in Children Based on the Internet of Things. IEEE Internet Things J. 2016, 4, 437–445. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Campbell, A.S.; Wang, J. Wearable non-invasive epidermal glucose sensors: A review. Talanta 2018, 177, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Bandodkar, A.J.; Jia, W.; Yardımcı, C.; Wang, X.; Ramirez, J.; Wang, J. Tattoo-Based Noninvasive Glucose Monitoring: A Proof-of-Concept Study. Anal. Chem. 2015, 87, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Tan, X.; Chen, X.; Chen, S.; Zhang, Z.; Zhang, H.; Wang, J.; Huang, Y.; Zhang, P.; Zheng, L.; et al. An Implantable RFID Sensor Tag toward Continuous Glucose Monitoring. IEEE J. Biomed. Health Inform. 2015, 19, 910–919. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.; Bensaali, F.; Jaber, F. Novel Approach to Non-Invasive Blood Glucose Monitoring Based on Transmittance and Refraction of Visible Laser Light. IEEE Access 2017, 5, 9163–9174. [Google Scholar] [CrossRef]
- Haxha, S.; Jhoja, J. Optical Based Noninvasive Glucose Monitoring Sensor Prototype. IEEE Photonics J. 2016, 8, 6805911. [Google Scholar] [CrossRef] [Green Version]
- Yadav, K.S.; Kapse-Mistry, S.; Peters, G.J.; Mayur, Y.C. E-drug delivery: A futuristic approach. Drug Discov. Today 2019, 24, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Eggenberger, P.; MacRae, B.A.; Kemp, S.; Bürgisser, M.; Rossi, R.M.; Annaheim, S. Prediction of Core Body Temperature Based on Skin Temperature, Heat Flux, and Heart Rate Under Different Exercise and Clothing Conditions in the Heat in Young Adult Males. Front. Physiol. 2018, 9, 1780. [Google Scholar] [CrossRef]
- De Andrade Fernandes, A.; dos Santos Amorim, P.R.; Brito, C.J.; de Moura, A.G.; Moreira, D.G.; Costa, C.M.A.; Sillero-Quintana, M.; Marins, J.C.B. Measuring skin temperature before, during and after exercise: A comparison of thermocouples and infrared thermography. Physiol. Meas. 2014, 35, 189. [Google Scholar] [CrossRef] [Green Version]
- Huang, M.; Tamura, T.; Tang, Z.; Chen, W.; Kanaya, S. A Wearable Thermometry for Core Body Temperature Measurement and Its Experimental Verification. IEEE J. Biomed. Health Inform. 2016, 21, 708–714. [Google Scholar] [CrossRef]
- Atallah, L.; Ciuhu, C.; Wang, C.; Bongers, E.; Blom, T.; Paulussen, I.; Noordergraaf, G.J. An Ergonomic Wearable Core Body Temperature Sensor. In Proceedings of the IEEE 15th International Conference on Wearable and Implantable Body Sensor Networks, Las Vegas, NV, USA, 4–7 March 2018; pp. 70–73. [Google Scholar]
- Shin, J.; Jeong, B.; Kim, J.; Binh Nam, V.; Yoon, Y.; Jung, J.; Hong, S.; Lee, H.; Eom, H.; Yeo, J.; et al. Sensitive Wearable Temperature Sensor with Seamless Monolithic Integration. Adv. Mater. 2020, 32, 1905527. [Google Scholar] [CrossRef]
- Mizuno, T.; Kume, Y. Development of a Glasses-Like Wearable Device to Measure Nasal Skin Temperature. In Proceedings of the International Conference on Human—Computer Interaction, Los Angeles, CA, USA, 2–7 August 2015; Springer: Cham, Switzerland, 2015; pp. 727–732. [Google Scholar]
- Xu, X.; Karis, A.J.; Buller, M.J.; Santee, W.R. Relationship between core temperature, skin temperature, and heat flux during exercise in heat. Eur. J. Appl. Physiol. 2013, 113, 2381–2389. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Yang, H.; Li, E.; Liu, Z.; Wei, K. Wearable sensors in intelligent clothing for measuring human body temperature based on optical fiber Bragg grating. Opt. Express 2012, 20, 11740–11752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Ren, Z.; Guo, H.; Cheng, X.; Zhang, H. Self-powered flexible and transparent smart patch for temperature sensing. Appl. Phys. Lett. 2020, 116, 043902. [Google Scholar] [CrossRef]
- Shi, X.; Wu, P. A Smart Patch with On-Demand Detachable Adhesion for Bioelectronics. Small 2021, 17, 2101220. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Lu, B.; Chen, Y.; Feng, X. Breathable and Stretchable Temperature Sensors Inspired by Skin. Sci. Rep. 2015, 5, 11505. [Google Scholar] [CrossRef] [Green Version]
- Rajan, G.; Morgan, J.J.; Murphy, C.; Torres Alonso, E.; Wade, J.; Ott, A.K.; Russo, S.; Alves, H.; Craciun, M.F.; Neves, A.I.S. Low Operating Voltage Carbon–Graphene Hybrid E-textile for Temperature Sensing. ACS Appl. Mater. Interfaces 2020, 12, 29861–29867. [Google Scholar] [CrossRef]
- Fleury, A.; Sugar, M.; Chau, T. E-textiles in Clinical Rehabilitation: A Scoping Review. Electronics 2015, 4, 173–203. [Google Scholar] [CrossRef] [Green Version]
- Fleming, S.; Thompson, M.; Stevens, R.; Heneghan, C.; Plüddemann, A.; Maconochie, I.; Tarassenko, L.; Mant, D. Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: A systematic review of observational studies. Lancet 2011, 377, 1011–1018. [Google Scholar] [CrossRef] [Green Version]
- Massaroni, C.; Nicolò, A.; Lo Presti, D.; Sacchetti, M.; Silvestri, S.; Schena, E. Contact-Based Methods for Measuring Respiratory Rate. Sensors 2019, 19, 908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, M.; Nguyen, T.; Pandey, V.; Zhou, Y.; Pham, H.N.; Bar-Yoseph, R.; Radom-Aizik, S.; Jain, R.; Cooper, D.M.; Khine, M. Respiration rate and volume measurements using wearable strain sensors. NPJ Digit. Med. 2019, 2, 8. [Google Scholar] [CrossRef] [PubMed]
- Naranjo-Hernández, D.; Talaminos-Barroso, A.; Reina-Tosina, J.; Roa, L.M.; Barbarov-Rostan, G.; Cejudo-Ramos, P.; Márquez-Martín, E.; Ortega-Ruiz, F. Smart Vest for Respiratory Rate Monitoring of COPD Patients Based on Non-Contact Capacitive Sensing. Sensors 2018, 18, 2144. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Chen, K.; Dai, Y.; Zhang, S. Utility of transthoracic impedance and novel algorithm for sleep apnea screening in pacemaker patient. Sleep Breath. 2019, 23, 741–746. [Google Scholar] [CrossRef]
- Heydari, F.; Ebrahim, M.P.; Yuce, M.R. Chest-based Real-Time Pulse and Respiration Monitoring Based on Bio-Impedance. In Proceedings of the 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society, Montreal, QC, Canada, 20–24 July 2020; pp. 4398–4401. [Google Scholar]
- Wang, F.T.; Chan, H.L.; Wang, C.L.; Jian, H.M.; Lin, S.H. Instantaneous Respiratory Estimation from Thoracic Impedance by Empirical Mode Decomposition. Sensors 2015, 15, 16372–16387. [Google Scholar] [CrossRef]
- Lapi, S.; Lavorini, F.; Borgioli, G.; Calzolai, M.; Masotti, L.; Pistolesi, M.; Fontana, G.A. Respiratory rate assessments using a dual-accelerometer device. Respir. Physiol. Neurobiol. 2014, 191, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, A.G.; Fernandes, D.; Branco, S.; Monteiro, J.L.; Cabral, J.; Catarino, A.P.; Rocha, A.M. A Smart Wearable System for Sudden Infant Death Syndrome Monitoring. In Proceedings of the IEEE International Conference on Industrial Technology, Taipei, Taiwan, 14–17 March 2016; pp. 1920–1925. [Google Scholar]
- Sharma, P.; Hui, X.; Zhou, J.; Conroy, T.B.; Kan, E.C. Wearable radio-frequency sensing of respiratory rate, respiratory volume, and heart rate. NPJ Digit. Med. 2020, 3, 98. [Google Scholar] [CrossRef]
- Al-Halhouli, A.; Al-Ghussain, L.; El Bouri, S.; Habash, F.; Liu, H.; Zheng, D. Clinical Evaluation of Stretchable and Wearable Inkjet-Printed Strain Gauge Sensor for Respiratory Rate Monitoring at Different Body Postures. Appl. Sci. 2020, 10, 480. [Google Scholar] [CrossRef] [Green Version]
- Piuzzi, E.; Pisa, S.; Pittella, E.; Podestà, L.; Sangiovanni, S. Wearable Belt With Built-In Textile Electrodes for Cardio—Respiratory Monitoring. Sensors 2020, 20, 4500. [Google Scholar] [CrossRef] [PubMed]
- Jun, Z.; Chun-na, L.; Wen-liang, Z.; Hong, Z.; Yong-feng, L.; Xue-feng, H. Wearable respiratory strain monitoring system based on textile-based capacitive strain sensor. J. Phys. Conf. Ser. 2020, 1570, 012033. [Google Scholar] [CrossRef]
- Oletic, D.; Bilas, V. Energy-Efficient Respiratory Sounds Sensing for Personal Mobile Asthma Monitoring. IEEE Sensors J. 2016, 16, 8295–8303. [Google Scholar] [CrossRef]
- Corbishley, P.; Rodriguez-Villegas, E. Breathing Detection: Towards a Miniaturized, Wearable, Battery-Operated Monitoring System. IEEE Trans. Biomed. Eng. 2007, 55, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Larson, E.C.; Goel, M.; Boriello, G.; Heltshe, S.; Rosenfeld, M.; Patel, S.N. SpiroSmart: Using a Microphone to Measure Lung Function on a Mobile Phone. In Proceedings of the ACM Conference on Ubiquitous Computing, Pittsburgh, PA, USA, 5–8 September 2012; pp. 280–289. [Google Scholar]
- Milici, S.; Lorenzo, J.; Lázaro, A.; Villarino, R.; Girbau, D. Wireless Breathing Sensor Based on Wearable Modulated Frequency Selective Surface. IEEE Sens. J. 2016, 17, 1285–1292. [Google Scholar] [CrossRef]
- Kano, S.; Kim, K.; Fujii, M. Fast-Response and Flexible Nanocrystal-Based Humidity Sensor for Monitoring Human Respiration and Water Evaporation on Skin. ACS Sens. 2017, 2, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Varon, C.; Caicedo, A.; Testelmans, D.; Buyse, B.; Van Huffel, S. A novel algorithm for the automatic detection of sleep apnea from single-lead ECG. IEEE Trans. Biomed. Eng. 2015, 62, 2269–2278. [Google Scholar] [CrossRef]
- Varon, C.; Morales, J.; Lázaro, J.; Orini, M.; Deviaene, M.; Kontaxis, S.; Testelmans, D.; Buyse, B.; Borzée, P.; Sörnmo, L.; et al. A Comparative Study of ECG-derived Respiration in Ambulatory Monitoring using the Single-lead ECG. Sci. Rep. 2020, 10, 5704. [Google Scholar] [CrossRef]
- Touw, H.R.W.; Verheul, M.H.; Tuinman, P.R.; Smit, J.; Thöne, D.; Schober, P.; Boer, C. Photoplethysmography respiratory rate monitoring in patients receiving procedural sedation and analgesia for upper gastrointestinal endoscopy. J. Clin. Monit. Comput. 2017, 31, 747–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlen, W.; Raman, S.; Ansermino, J.M.; Dumont, G.A. Multiparameter Respiratory Rate Estimation From the Photoplethysmogram. IEEE Trans. Biomed. Eng. 2013, 60, 1946–1953. [Google Scholar] [CrossRef]
- AL-Khalidi, F.Q.; Saatchi, R.; Burke, D.; Elphick, H.; Tan, S. Respiration Rate Monitoring Methods: A Review. Pediatr. Pulmonol. 2011, 46, 523–529. [Google Scholar] [CrossRef] [Green Version]
- Massaroni, C.; Lo Presti, D.; Formica, D.; Silvestri, S.; Schena, E. Non-Contact Monitoring of Breathing Pattern and Respiratory Rate via RGB Signal Measurement. Sensors 2019, 19, 2758. [Google Scholar] [CrossRef] [Green Version]
- Massaroni, C.; Lopes, D.S.; Lo Presti, D.; Schena, E.; Silvestri, S. Contactless Monitoring of Breathing Patterns and Respiratory Rate at the Pit of the Neck: A Single Camera Approach. J. Sens. 2018, 2018, 4567213. [Google Scholar] [CrossRef]
- Pereira, C.B.; Yu, X.; Goos, T.; Reiss, I.; Orlikowsky, T.; Heimann, K.; Venema, B.; Blazek, V.; Leonhardt, S.; Teichmann, D. Noncontact Monitoring of Respiratory Rate in Newborn Infants Using Thermal Imaging. IEEE Trans. Biomed. Eng. 2018, 66, 1105–1114. [Google Scholar] [CrossRef]
- Kusche, R.; John, F.; Cimdins, M.; Hellbrück, H. Contact-Free Biosignal Acquisition via Capacitive and Ultrasonic Sensors. IEEE Access 2020, 8, 95629–95641. [Google Scholar] [CrossRef]
- Min, S.D.; Kim, J.K.; Shin, H.S.; Yun, Y.H.; Lee, C.K.; Lee, M. Noncontact Respiration Rate Measurement System Using an Ultrasonic Proximity Sensor. IEEE Sens. J. 2010, 10, 1732–1739. [Google Scholar]
- Casson, A.J.; Yates, D.C.; Smith, S.J.M.; Duncan, J.S.; Rodriguez-Villegas, E. Wearable Electroencephalography: What Is It, Why Is It Needed, and What Does It Entail? IEEE Eng. Med. Biol. Mag. 2010, 29, 44–56. [Google Scholar] [CrossRef] [Green Version]
- Apicella, A.; Arpaia, P.; Frosolone, M.; Moccaldi, N. High-wearable EEG-based distraction detection in motor rehabilitation. Sci. Rep. 2021, 11, 5297. [Google Scholar] [CrossRef]
- Byrom, B.; McCarthy, M.; Schueler, P.; Muehlhausen, W. Brain Monitoring Devices in Neuroscience Clinical Research: The Potential of Remote Monitoring Using Sensors, Wearables, and Mobile Devices. Clin. Pharmacol. Ther. 2018, 104, 59–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau-Zhu, A.; Lau, M.P.H.; McLoughlin, G. Mobile EEG in research on neurodevelopmental disorders: Opportunities and challenges. Dev. Cogn. Neurosci. 2019, 36, 100635. [Google Scholar] [CrossRef]
- Mihajlović, V.; Grundlehner, B.; Vullers, R.; Penders, J. Wearable, Wireless EEG Solutions in Daily Life Applications: What are we Missing? IEEE J. Biomed. Health Inform. 2014, 19, 6–21. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.T.; Chuang, C.H.; Cao, Z.; Singh, A.K.; Hung, C.S.; Yu, Y.H.; Nascimben, M.; Liu, Y.T.; King, J.T.; Su, T.P.; et al. Forehead EEG in Support of Future Feasible Personal Healthcare Solutions: Sleep Management, Headache Prevention, and Depression Treatment. IEEE Access 2017, 5, 10612–10621. [Google Scholar] [CrossRef]
- Athavipach, C.; Pan-ngum, S.; Israsena, P. A Wearable In-Ear EEG Device for Emotion Monitoring. Sensors 2019, 19, 4014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, Y.; Cleeren, E.; Dan, J.; Claes, K.; Van Paesschen, W.; Van Huffel, S.; Hunyadi, B. Comparison between Scalp EEG and Behind-the-Ear EEG for Development of a Wearable Seizure Detection System for Patients with Focal Epilepsy. Sensors 2018, 18, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casson, A.J. Wearable EEG and beyond. Biomed. Eng. Lett. 2019, 9, 53–71. [Google Scholar] [CrossRef] [PubMed]
- Von Lühmann, A.; Zimmermann, B.B.; Ortega-Martinez, A.; Perkins, N.; Yücel, M.A.; Boas, D.A. Towards Neuroscience in the Everyday World: Progress in wearable fNIRS instrumentation and applications. In Proceedings of the Biophotonics Congress: Biomedical Optics 2020, Ford Lauderdale, FL, USA, 20–23 April 2020. OSA Technical Digest (Optical Society of America, US. 2020, paper BM3C.2. [Google Scholar]
- Kassab, A.; Le Lan, J.; Tremblay, J.; Vannasing, P.; Dehbozorgi, M.; Pouliot, P.; Gallagher, A.; Lesage, F.; Sawan, M.; Nguyen, D.K. Multichannel Wearable fNIRS-EEG System for Long-Term Clinical Monitoring. Hum. Brain Mapp. 2018, 39, 7–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boto, E.; Seedat, Z.A.; Holmes, N.; Leggett, J.; Hill, R.M.; Roberts, G.; Shah, V.; Fromhold, T.M.; Mullinger, K.J.; Tierney, T.M.; et al. Wearable neuroimaging: Combining and contrasting magnetoencephalography and electroencephalography. NeuroImage 2019, 201, 116099. [Google Scholar] [CrossRef]
- Melroy, S.; Bauer, C.; McHugh, M.; Carden, G.; Stolin, A.; Majewski, S.; Brefczynski-Lewis, J.; Wuest, T. Development and Design of Next-Generation Head-Mounted Ambulatory Microdose Positron-Emission Tomography (AM-PET) System. Sensors 2017, 17, 1164. [Google Scholar] [CrossRef] [Green Version]
- Ossig, C.; Antonini, A.; Buhmann, C.; Classen, J.; Csoti, I.; Falkenburger, B.; Schwarz, M.; Winkler, J.; Storch, A. Wearable sensor-based objective assessment of motor symptomsin Parkinson’s disease. J. Neural Transm. 2016, 123, 57–64. [Google Scholar] [CrossRef]
- Vescio, B.; Nisticò, R.; Augimeri, A.; Quattrone, A.; Crasà, M.; Quattrone, A. Development and Validation of a New Wearable Mobile Device for the Automated Detection of Resting Tremor in Parkinson’s Disease and Essential Tremor. Diagnostics 2021, 11, 200. [Google Scholar] [CrossRef]
- Mazzetta, I.; Gentile, P.; Pessione, M.; Suppa, A.; Zampogna, A.; Bianchini, E.; Irrera, F. Stand-Alone Wearable System for Ubiquitous Real-Time Monitoring of Muscle Activation Potentials. Sensors 2018, 18, 1748. [Google Scholar] [CrossRef] [Green Version]
- Song, M.S.; Kang, S.G.; Lee, K.T.; Kim, J. Wireless, Skin-Mountable EMG Sensor for Human–Machine Interface Application. Micromachines 2019, 10, 879. [Google Scholar] [CrossRef] [Green Version]
- Cerone, G.L.; Botter, A.; Vieira, T.; Gazzoni, M. Design and Characterization of a Textile Electrode System for the Detection of High-Density sEMG. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1110–1119. [Google Scholar] [CrossRef]
- Pino, E.J.; Arias, Y.; Aqueveque, P. Wearable EMG Shirt for Upper Limb Training. In Proceedings of the 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Honolulu, HI, USA, 18–21 July 2018; pp. 4406–4409. [Google Scholar]
- Cole, B.T.; Roy, S.H.; De Luca, C.J.; Nawab, S.H. Dynamical Learning and Tracking of Tremor andDyskinesia From Wearable Sensors. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 982–991. [Google Scholar] [CrossRef]
- Leone, A.; Rescio, G.; Caroppo, A.; Siciliano, P. A Wearable EMG-based System Pre-fall Detector. Proc. Eng. 2015, 120, 455–458. [Google Scholar] [CrossRef] [Green Version]
- Jung, P.G.; Lim, G.; Kim, S.; Kong, K. A Wearable Gesture Recognition Devicefor Detecting Muscular Activities Basedon Air-Pressure Sensors. IEEE Trans. Ind. Inform. 2015, 11, 485–494. [Google Scholar]
- Ghassemi, M.; Triandafilou, K.; Barry, A.; Stoykov, M.E.; Roth, E.; Mussa-Ivaldi, F.A.; Kamper, D.G.; Ranganathan, R. Development of an EMG-controlled Serious Game for Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 283–292. [Google Scholar] [CrossRef]
- Leonardis, D.; Barsotti, M.; Loconsole, C.; Solazzi, M.; Troncossi, M.; Mazzotti, C.; Castelli, V.P.; Procopio, C.; Lamola, G.; Chisari, C.; et al. An EMG-controlled robotic hand exoskeleton for bilateral rehabilitation. IEEE Trans. Haptics 2015, 8, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Hussain, I.; Salvietti, G.; Spagnoletti, G.; Prattichizzo, D. The Soft-SixthFinger: A Wearable EMG Controlled Robotic Extra-Finger for Grasp Compensation in Chronic Stroke Patients. IEEE Robot. Autom. Lett. 2016, 1, 1000–1006. [Google Scholar] [CrossRef] [Green Version]
- Bi, Z.; Wang, Y.; Wang, H.; Zhou, Y.; Xie, C.; Zhu, L.; Wang, H.; Wang, B.; Huang, J.; Lü, X.; et al. Wearable EMG Bridge-a Multiple-Gesture Reconstruction System Using Electrical Stimulation Controlled by the Volitional Surface Electromyogram of a Healthy Forearm. IEEE Access 2020, 8, 137330–137341. [Google Scholar] [CrossRef]
- Freed, A.; Chan, A.D.C.; Lemaire, E.D.; Parush, A. Wearable EMG Analysis for Rehabilitation (WEAR)—Surface electromyography in clinical gait analysis. In Proceedings of the IEEE International Symposium on Medical Measurements and Applications, Bari, Italy, 30–31 May 2011; pp. 601–604. [Google Scholar]
- Chowdhury, R.H.; Reaz, M.B.I.; Ali, M.A.B.M.; Bakar, A.A.A.; Chellappan, K.; Chang, T.G. Surface Electromyography Signal Processing and Classification Techniques. Sensors 2013, 13, 12431–12466. [Google Scholar] [CrossRef] [PubMed]
- Plewa, K.; Samadani, A.; Chau, T. Comparing electro-and mechano-myographic muscle activation patterns in self-paced pediatric gait. J. Electromyogr. Kinesiol. 2017, 36, 73–80. [Google Scholar] [CrossRef]
- Booth, R.; Goldsmith, P. A Wrist-Worn Piezoelectric Sensor Array for Gesture Input. J. Med. Biol. Eng. 2018, 38, 284–295. [Google Scholar] [CrossRef]
- Wilson, S.; Vaidyanathan, R. Upper-Limb Prosthetic Control using Wearable Multichannel Mechanomyography. In Proceedings of the International Conference on Rehabilitation Robotics, London, UK, 17–20 July 2017; pp. 1293–1298. [Google Scholar]
- Esposito, D.; Andreozzi, E.; Fratini, A.; Gargiulo, G.D.; Savino, S.; Niola, V.; Bifulco, P. A Piezoresistive Sensor to Measure Muscle Contraction and Mechanomyography. Sensors 2018, 18, 2553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krueger, E.; Popović-Maneski, L.; Nohama, P. Mechanomyography-Based Wearable Monitor of Quasi-Isometric Muscle Fatigue for Motor Neural Prostheses. Artif. Organs 2018, 42, 208–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Rodrigo, A.; Fernández-Caballero, A.; Silva, F.; Novais, P. Monitoring Electrodermal Activity for Stress Recognition Using a Wearable. In Proceedings of the 12th International Conference on Intelligent Environments, London, UK, 12–13 September 2016; pp. 416–425. [Google Scholar]
- Zangróniz, R.; Martínez-Rodrigo, A.; Pastor, J.M.; López, M.T.; Fernández-Caballero, A. Electrodermal Activity Sensor for Classification of Calm/Distress Condition. Sensors 2017, 17, 2324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, B.; Jebelli, H.; Lee, S. Feasibility analysis of electrodermal activity (EDA) acquired from wearable sensors to assess construction workers’ perceived risk. Saf. Sci. 2019, 115, 110–120. [Google Scholar] [CrossRef]
- Herlan, A.; Ottenbacher, J.; Schneider, J.; Riemann, D.; Feige, B. Electrodermal activity patterns in sleep stages and their utility for sleep versus wake classification. J. Sleep Res. 2019, 28, e12694. [Google Scholar] [CrossRef]
- Arriba-Pérez, D.; Caeiro-Rodríguez, M.; Santos-Gago, J.M. Collection and Processing of Data from Wrist Wearable Devices in Heterogeneous and Multiple-User Scenarios. Sensors 2016, 16, 1538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagai, Y.; Jones, C.I.; Sen, A. Galvanic Skin Response (GSR)/Electrodermal/Skin Conductance Biofeedback on Epilepsy: A Systematic Review and Meta-Analysis. Front. Neurol. 2019, 10, 377. [Google Scholar] [CrossRef]
- Nagai, Y.; Critchley, H.D. Novel Therapeutic Application of Galvanic Skin Response (GSR) Biofeedback to a Neurological Disorder: Mechanisms Underlying Biofeedback in Epilepsy Management. In Epilepsy Research Progress; Nova Science Publishers: New York, NY, USA, 2008; pp. 175–205. [Google Scholar]
- Posada-Quintero, H.F.; Chon, K.H. Innovations in Electrodermal Activity Data Collection and Signal Processing: A Systematic Review. Sensors 2020, 20, 479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pope, G.C.; Halter, R.J. Design and Implementation of an Ultra-Low Resource Electrodermal Activity Sensor for Wearable Applications. Sensors 2019, 19, 2450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gjoreski, M.; Lustrek, M.; Gams, M.; Gjoreski, H. Monitoring stress with a wrist device using context. J. Biomed. Inform. 2017, 73, 159–170. [Google Scholar] [CrossRef]
- Geršak, G.; Drnovšek, J. Electrodermal activity patient simulator. PLoS ONE 2020, 15, e0228949. [Google Scholar] [CrossRef]
- Trafton, A. Hydration Sensor Could Improve Dialysis. Available online: http://news.mit.edu/2019/hydration-sensor-dialysis-0724 (accessed on 1 August 2021).
- Yao, S.; Myers, A.; Malhotra, A.; Lin, F.; Bozkurt, A.; Muth, J.F.; Zhu, Y. A Wearable Hydration Sensor with Conformal Nanowire Electrodes. Adv. Healthc. Mater. 2017, 6, 1601159. [Google Scholar] [CrossRef] [PubMed]
- Koh, A.; Kang, D.; Xue, Y.; Lee, S.; Pielak, R.M.; Kim, J.; Hwang, T.; Min, S.; Banks, A.; Bastien, P.; et al. A Soft, Wearable Microfluidic Device for the Capture, Storage, and Colorimetric Sensing of Sweat. Sci. Transl. Med. 2016, 8, 366ra165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, X.; Yeo, W.H.; Liu, Y.; Rogers, J.A. Epidermal Differential Impedance Sensor for Conformal Skin Hydration Monitoring. Biointerphases 2012, 7, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, W.; Emaminejad, S.; Nyein, H.Y.Y.; Challa, S.; Chen, K.; Peck, A.; Fahad, H.M.; Ota, H.; Shiraki, H.; Kiriya, D.; et al. Fully integrated wearable sensor arrays for multiplexed in situ perspiration analysis. Nature 2016, 529, 509–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, G.; Alomari, M.; Sahin, B.; Snelgrove, S.E.; Edwards, J.; Mellinger, A.; Kaya, T. Real-time sweat analysis via alternating current conductivity of artificial and human sweat. Appl. Phys. Lett. 2015, 106, 133702. [Google Scholar] [CrossRef]
- Huang, X.; Liu, Y.; Cheng, H.; Shin, W.J.; Fan, J.A.; Liu, Z.; Lu, C.J.; Kong, G.W.; Chen, K.; Patnaik, D.; et al. Materials and Designs for Wireless Epidermal Sensors of Hydration and Strain. Adv. Funct. Mater. 2014, 24, 3846–3854. [Google Scholar] [CrossRef]
- Schiavoni, R.; Monti, G.; Tedesco, A.; Tarricone, L.; Piuzzi, E.; de Benedetto, E.; Masciullo, A.; Cataldo, A. Microwave Wearable System for Sensing Skin Hydration. In Proceedings of the IEEE International Instrumentation and Measurement Technology Conference, Glasgow, UK, 17–20 May 2021; pp. 1–6. [Google Scholar]
- Yokus, M.A.; Daniele, M.A. Skin Hydration Sensor for Customizable Electronic Textiles. MRS Adv. 2016, 1, 2671–2676. [Google Scholar] [CrossRef] [Green Version]
- Batista, E.; Borras, F.; Martínez-Ballesté, A. Monitoring People with MCI: Deployment in a Real Scenario for Low-Budget Smartphones. In Proceedings of the International Conference on Information, Intelligence, Systems and Applications, Corfu, Greece, 6–8 July 2015; pp. 1–6. [Google Scholar]
- Cao, H.R.; Zhan, C. A Novel Emergency Healthcare System for Elderly Community in Outdoor Environment. Wirel. Commun. Mob. Comput. 2018, 2018, 7841026. [Google Scholar] [CrossRef]
- Nguyen, Q.H.; Johnson, P.; Nguyen, T.T.; Randles, M. A novel architecture using iBeacons for localization and tracking of people within healthcare environment. In Global IoT Summit; IEEE: New York, NY, USA, 2019; pp. 1–6. [Google Scholar]
- Torres, J.; Belmonte, Ó.; Montoliu, R.; Trilles, S.; Calia, A. How feasible is WiFi fingerprint-based indoor positioning for in-home monitoring? In Proceedings of the 12th International Conference on Intelligent Environments, London, UK, 14–16 September 2016; pp. 68–75. [Google Scholar]
- Kim, S.C.; Jeong, Y.S.; Park, S.O. RFID-based indoor location tracking to ensure the safety of the elderly in smart home environments. Pers. Ubiquitous Comput. 2013, 17, 1699–1707. [Google Scholar] [CrossRef]
- Shi, G.; Ming, Y. Survey of indoor positioning systems based on ultra-wideband (UWB) technology. In Wireless Communications, Networking and Applications; Springer: New Delhi, India, 2016; pp. 1269–1278. [Google Scholar]
- Ferre, M.; Batista, E.; Solanas, A.; Martínez-Ballesté, A. Smart Health-Enhanced Early Mobilisation in Intensive Care Units. Sensors 2021, 21, 5408. [Google Scholar] [CrossRef]
- Chang, H.C.; Hsu, Y.L.; Yang, S.C.; Lin, J.C.; Wu, Z.H. A Wearable Inertial Measurement System With Complementary Filter for Gait Analysis of Patients With Stroke or Parkinson’s Disease. IEEE Access 2016, 4, 8442–8453. [Google Scholar] [CrossRef]
- Lin, F.; Wang, A.; Zhuang, Y.; Tomita, M.R.; Xu, W. Smart Insole: A Wearable Sensor Device for Unobtrusive Gait Monitoring in Daily Life. IEEE Trans. Ind. Inform. 2016, 12, 2281–2291. [Google Scholar] [CrossRef]
- Chen, S.; Lach, J.; Lo, B.; Yang, G.Z. Toward Pervasive Gait Analysis With WearableSensors: A Systematic Review. IEEE J. Biomed. Health Inform. 2016, 20, 1521–1537. [Google Scholar] [CrossRef]
- Bisio, I.; Garibotto, C.; Lavagetto, F.; Sciarrone, A. When eHealth Meets IoT: A Smart Wireless System for Post-Stroke Home Rehabilitation. IEEE Wirel. Commun. 2019, 26, 24–29. [Google Scholar] [CrossRef]
- Ding, Z.Q.; Luo, Z.Q.; Causo, A.; Chen, I.M.; Yue, K.X.; Yeo, S.H.; Ling, K.V. Inertia sensor-based guidance system for upperlimb posture correction. Med Eng. Phys. 2013, 35, 269–276. [Google Scholar] [CrossRef]
- Wang, Q.; Chen, W.; Timmermans, A.A.A.; Karachristos, C.; Martens, J.B.; Markopoulos, P. Smart Rehabilitation Garment for posture monitoring. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Milan, Italy, 25–29 August 2015; pp. 5736–5739. [Google Scholar]
- Khojasteh, S.B.; Villar, J.R.; Chira, C.; González, V.M.; de la Cal, E. Improving Fall Detection Using an On-Wrist Wearable Accelerometer. Sensors 2018, 18, 1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sucerquia, A.; López, J.D.; Vargas-Bonilla, J.F. Real-Life/Real-Time Elderly Fall Detection with a Triaxial Accelerometer. Sensors 2018, 18, 1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cippitelli, E.; Fioranelli, F.; Gambi, E.; Spinsante, S. Radar and RGB-Depth Sensors for Fall Detection: A Review. IEEE Sensors J. 2017, 17, 3585–3604. [Google Scholar] [CrossRef] [Green Version]
- Bisio, I.; Delfino, A.; Lavagetto, F.; Sciarrone, A. Enabling IoT for In-Home Rehabilitation: Accelerometer Signals Classification Methods for Activity and Movement Recognition. IEEE Internet Things J. 2016, 4, 135–146. [Google Scholar] [CrossRef]
- Lu, Y.; Wei, Y.; Liu, L.; Zhong, J.; Sun, L.; Liu, Y. Towards unsupervised physical activity recognition using smartphone accelerometers. Multimed. Tools Appl. 2017, 76, 10701–10719. [Google Scholar] [CrossRef]
- Fleron, M.K.; Ubbesen, N.C.H.; Battistella, F.; Dejtiar, D.L.; Oliveira, A.S. Accuracy between optical and inertial motion capture systems for assessing trunk speed during preferred gait and transition periods. Sport. Biomech. 2019, 18, 366–377. [Google Scholar] [CrossRef]
- Robert-Lachaine, X.; Mecheri, H.; Muller, A.; Larue, C.; Plamondon, A. Validation of a low-cost inertial motion capture system for whole-body motion analysis. J. Biomech. 2020, 99, 109520. [Google Scholar] [CrossRef]
- Hesse, N.; Pujades, S.; Romero, J.; Black, M.J.; Bodensteiner, C.; Arens, M.; Hofmann, U.G.; Tacke, U.; Hadders-Algra, M.; Weinberger, R.; et al. Learning an Infant Body Model from RGB-D Data for Accurate Full Body Motion Analysis. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Granada, Spain, 16–20 September 2018; pp. 792–800. [Google Scholar]
- De Vries, N.M.; Smilowska, K.; Hummelink, J.; Abramiuc, B.; van Gilst, M.M.; Bloem, B.R.; Overeem, S. Exploring the Parkinson patients’ perspective on home-based video recording for movement analysis: A qualitative study. BMC Neurol. 2019, 19, 71. [Google Scholar] [CrossRef]
- Gaglio, S.; Re, G.L.; Morana, M. Human Activity Recognition Process Using 3-D Posture Data. IEEE Trans.-Hum.-Mach. Syst. 2014, 45, 586–597. [Google Scholar] [CrossRef]
- Collin, J.; Davidson, P.; Kirkko-Jaakkola, M.; Leppäkoski, H. Inertial Sensors and Their Applications. In Handbook of Signal Processing Systems; Springer: New York, NY, USA, 2019; pp. 51–85. [Google Scholar]
- Martínez-Ballesté, A.; Gimeno, P.; Mariné, A.; Batista, E.; Solanas, A. e-PEMICU: An e-Health Platform to Support Early Mobilisation in Intensive Care Units. In Proceedings of the 10th International Conference on Information, Intelligence, Systems and Applications, Patras, Greece, 15–17 July 2019; pp. 1–6. [Google Scholar]
- Villeneuve, E.; Harwin, W.; Holderbaum, W.; Janko, B.; Sherratt, R.S. Reconstruction of Angular Kinematics From Wrist-Worn Inertial Sensor Data for Smart Home Healthcare. IEEE Access 2017, 5, 2351–2363. [Google Scholar] [CrossRef]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Kinney, P.L.; Petkova, E.P.; Lavigne, E.; Zanobetti, A.; Schwartz, J.D.; Tobias, A.; Leone, M.; et al. Temporal Variation in Heat–Mortality Associations: A Multicountry Study. Environ. Health Perspect. 2015, 123, 1200–1207. [Google Scholar] [CrossRef]
- Zeng, W.; Lao, X.; Rutherford, S.; Xu, Y.; Xu, X.; Lin, H.; Liu, T.; Luo, Y.; Xiao, J.; Hu, M.; et al. The effect of heat waves on mortality and effect modifiers in four communities of Guangdong Province, China. Sci. Total. Environ. 2014, 482, 214–221. [Google Scholar] [CrossRef]
- Ou, C.Q.; Song, Y.F.; Yang, J.; Chau, P.Y.K.; Yang, L.; Chen, P.Y.; Wong, C.M. Excess Winter Mortality and Cold Temperatures in a Subtropical City, Guangzhou, China. PLoS ONE 2013, 8, e77150. [Google Scholar] [CrossRef]
- Yang, C.; Meng, X.; Chen, R.; Cai, J.; Zhao, Z.; Wan, Y.; Kan, H. Long-term variations in the association between ambient temperature and daily cardiovascular mortality in Shanghai, China. Sci. Total. Environ. 2015, 538, 524–530. [Google Scholar] [CrossRef]
- Cui, L.; Geng, X.; Ding, T.; Tang, J.; Xu, J.; Zhai, J. Impact of ambient temperature on hospital admissions for cardiovascular disease in Hefei City, China. Int. J. Biometeorol. 2019, 63, 723–734. [Google Scholar] [CrossRef]
- Phung, D.; Thai, P.K.; Guo, Y.; Morawska, L.; Rutherford, S.; Chu, C. Ambient temperature and risk of cardiovascular hospitalization: An updated systematic review and meta-analysis. Sci. Total. Environ. 2016, 550, 1084–1102. [Google Scholar] [CrossRef]
- Xu, Z.; Crooks, J.L.; Davies, J.M.; Khan, A.F.; Hu, W.; Tong, S. The association between ambient temperature and childhood asthma: A systematic review. Int. J. Biometeorol. 2018, 62, 471–481. [Google Scholar] [CrossRef]
- Mullins, J.T.; White, C. Temperature and Mental Health: Evidence from the Spectrum of Mental Health Outcomes. J. Health Econ. 2019, 68, 102240. [Google Scholar] [CrossRef] [Green Version]
- Kamat, R.K.; Naik, G.M. Thermistors—In search of new applications, manufacturers cultivate advanced NTC techniques. Sens. Rev. 2002, 22, 334–340. [Google Scholar] [CrossRef]
- Wolkoff, P. Indoor air humidity, air quality, and health—An overview. Int. J. Hyg. Environ. Health 2018, 221, 376–390. [Google Scholar] [CrossRef]
- Lukcso, D.; Guidotti, T.L.; Franklin, D.E.; Burt, A. Indoor environmental and air quality characteristics, building-related health symptoms, and worker productivity in a federal government building complex. Arch. Environ. Occup. Health 2016, 71, 85–101. [Google Scholar] [CrossRef]
- Angelon-Gaetz, K.A.; Richardson, D.B.; Marshall, S.W.; Hernandez, M.L. Exploration of the effects of classroom humidity levels on teachers’ respiratory symptoms. Int. Arch. Occup. Environ. Health 2016, 89, 729–737. [Google Scholar] [CrossRef] [Green Version]
- Ijaz, M.K.; Zargar, B.; Wright, K.E.; Rubino, J.R.; Sattar, S.A. Generic aspects of the airborne spread of human pathogens indoors and emerging air decontamination technologies. Am. J. Infect. Control. 2016, 44, S109–S120. [Google Scholar] [CrossRef]
- Najeeb, M.A.; Ahmad, Z.; Shakoor, R.A. Organic Thin-Film Capacitive and Resistive Humidity Sensors: A Focus Review. Adv. Mater. Interfaces 2018, 5, 1800969. [Google Scholar] [CrossRef]
- Ascorbe, J.; Corres, J.M.; Arregui, F.J.; Matias, I.R. Recent Developments in Fiber Optics Humidity Sensors. Sensors 2017, 17, 893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, Y.G. Relative Humidity Sensors Based on Microfiber Knot Resonators—A Review. Sensors 2019, 19, 5196. [Google Scholar] [CrossRef] [Green Version]
- Maini, K.; Schuster, N.M. Headache and Barometric Pressure: A Narrative Review. Curr. Pain Headache Rep. 2019, 23, 87. [Google Scholar] [CrossRef]
- Kimoto, K.; Aiba, S.; Takashima, R.; Suzuki, K.; Takekawa, H.; Watanabe, Y.; Tatsumoto, M.; Hirata, K. Influence of Barometric Pressure in Patients with Migraine Headache. Intern. Med. 2011, 50, 1923–1928. [Google Scholar] [CrossRef] [Green Version]
- McAlindon, T.; Formica, M.; Schmid, C.H.; Fletcher, J. Changes in Barometric Pressure and Ambient Temperature Influence Osteoarthritis Pain. Am. J. Med. 2007, 120, 429–434. [Google Scholar] [CrossRef]
- Brennan, S.A.; Harney, T.; Queally, J.M.; McGoona, J.O.; Gormley, I.C.; Shannon, F.J. Influence of weather variables on pain severity in end-stage osteoarthritis. Int. Orthop. 2012, 36, 643–646. [Google Scholar] [CrossRef] [Green Version]
- Song, P.; Ma, Z.; Ma, J.; Yang, L.; Wei, J.; Zhao, Y.; Zhang, M.; Yang, F.; Wang, X. Recent Progress of Miniature MEMS Pressure Sensors. Micromachines 2020, 11, 56. [Google Scholar] [CrossRef] [Green Version]
- Javed, Y.; Mansoor, M.; Shah, I.A. A review of principles of MEMS pressure sensing with its aerospace applications. Sens. Rev. 2019, 39, 652–664. [Google Scholar] [CrossRef]
- Tenzer, Y.; Jentoft, L.P.; Howe, R.D. The Feel of MEMS Barometers: Inexpensive and Easily Customized Tactile Array Sensors. IEEE Robot. Autom. Mag. 2014, 21, 89–95. [Google Scholar] [CrossRef]
- World Health Organization. Air Pollution. Available online: https://www.who.int/health-topics/air-pollution (accessed on 1 July 2021).
- Manisalidis, I.; Stavropoulou, E.; Stavropoulos, A.; Bezirtzoglou, E. Environmental and Health Impacts of Air Pollution: A Review. Front. Public Health 2020, 8, 14. [Google Scholar] [CrossRef] [Green Version]
- Anderson, J.O.; Thundiyil, J.G.; Stolbach, A. Clearing the Air: A Review of the Effects of Particulate Matter Air Pollution on Human Health. J. Med. Toxicol. 2012, 8, 166–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurt, O.K.; Zhang, J.; Pinkerton, K.E. Pulmonary Health Effects of Air Pollution. Curr. Opin. Pulm. Med. 2016, 22, 138. [Google Scholar] [CrossRef] [PubMed]
- Ye, D.; Klein, M.; Chang, H.H.; Sarnat, J.A.; Mulholland, J.A.; Edgerton, E.S.; Winquist, A.; Tolbert, P.E.; Sarnat, S.E. Estimating acute cardiorespiratory effects of ambient volatile organic compounds. Epidemiology 2017, 28, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Idrees, Z.; Zheng, L. Low cost air pollution monitoring systems: A review of protocols and enabling technologies. J. Ind. Inf. Integr. 2020, 17, 100123. [Google Scholar] [CrossRef]
- Baron, R.; Saffell, J. Amperometric Gas Sensors as a Low Cost Emerging Technology Platform for Air Quality Monitoring Applications: A Review. ACS Sens. 2017, 2, 1553–1566. [Google Scholar] [CrossRef]
- Rai, A.C.; Kumar, P.; Pilla, F.; Skouloudis, A.N.; Di Sabatino, S.; Ratti, C.; Yasar, A.; Rickerby, D. End-user perspective of low-cost sensors for outdoor air pollution monitoring. Sci. Total. Environ. 2017, 607, 691–705. [Google Scholar] [CrossRef] [Green Version]
- Karagulian, F.; Gerboles, M.; Barbiere, M.; Kotsev, A.; Lagler, F.; Borowiak, A. Review of Sensors for Air Quality Monitoring; European Commission: Luxembourg, 2019.
- Lewis, A.C.; Lee, J.D.; Edwards, P.M.; Shaw, M.D.; Evans, M.J.; Moller, S.J.; Smith, K.R.; Buckley, J.W.; Ellis, M.; Gillot, S.R.; et al. Evaluating the performance of low cost chemical sensors for air pollution research. Faraday Discuss. 2016, 189, 85–103. [Google Scholar] [CrossRef]
- Levallois, P.; Villanueva, C.M. Drinking Water Quality and Human Health: An Editorial. Int. J. Environ. Res. Public Health 2019, 16, 631. [Google Scholar] [CrossRef] [Green Version]
- Højris, B.; Kornholt, S.N.; Christensen, S.C.B.; Albrechtsen, H.J.; Olesen, L.S. Detection of drinking water contamination by an optical real-time bacteria sensor. H2Open J. 2018, 1, 160–168. [Google Scholar] [CrossRef] [Green Version]
- Hatiboruah, D.; Das, T.; Chamuah, N.; Rabha, D.; Talukdar, B.; Bora, U.; Ahamad, K.U.; Nath, P. Estimation of trace-mercury concentration in water using a smartphone. Measurement 2020, 154, 107507. [Google Scholar] [CrossRef]
- Lambrou, T.P.; Anastasiou, C.C.; Panayiotou, C.G.; Polycarpou, M.M. A Low-Cost Sensor Network for Real-Time Monitoring and Contamination Detection in Drinking Water Distribution Systems. IEEE Sens. J. 2014, 14, 2765–2772. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, X.; Chen, J.; Cheng, Z.; Wang, D. Camera sensor-based contamination detection for water environment monitoring. Environ. Sci. Pollut. Res. 2019, 26, 2722–2733. [Google Scholar] [CrossRef]
- Münzel, T.; Schmidt, F.P.; Steven, S.; Herzog, J.; Daiber, A.; Sørensen, M. Environmental Noise and the Cardiovascular System. J. Am. Coll. Cardiol. 2018, 71, 688–697. [Google Scholar] [CrossRef]
- Hahad, O.; Kröller-Schön, S.; Daiber, A.; Münzel, T. The Cardiovascular Effects of Noise. Dtsch. ÄRzteblatt Int. 2019, 116, 245. [Google Scholar] [CrossRef] [PubMed]
- Van Kempen, E.; Casas, M.; Pershagen, G.; Foraster, M. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Cardiovascular and Metabolic Effects: A Summary. Int. J. Environ. Res. Public Health 2018, 15, 379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazmi, A.; Tragos, E.; Serrano, M. Underpinning IoT for Road Traffic Noise Management in Smart Cities. In Proceedings of the IEEE International Conference on Pervasive Computing and Communications, Athens, Greece, 19–23 March 2018; pp. 765–769. [Google Scholar]
- Segura Garcia, J.; Pérez Solano, J.J.; Cobos Serrano, M.; Navarro Camba, E.A.; Felici Castell, S.; Soriano Asensi, A.; Montes Suay, F. Spatial Statistical Analysis of Urban Noise Data from a WASN Gathered by an IoT System: Application to a Small City. Appl. Sci. 2016, 6, 380. [Google Scholar] [CrossRef]
- Moan, J.; Grigalavicius, M.; Baturaite, Z.; Dahlback, A.; Juzeniene, A. The relationship between UV exposure and incidence of skin cancer. Photodermatol. Photoimmunol. Photomed. 2015, 31, 26–35. [Google Scholar] [CrossRef]
- Genuis, S.J. Fielding a current idea: Exploring the public health impact of electromagnetic radiation. Public Health 2008, 122, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Xiang, F.; Lucas, R.; Hales, S.; Neale, R. Incidence of Nonmelanoma Skin Cancer in Relation to Ambient UV Radiation in White Populations, 1978-2012 Empirical Relationships. JAMA Dermatol. 2014, 150, 1063–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardell, L. World Health Organization, radiofrequency radiation and health—A hard nut to crack. Int. J. Oncol. 2017, 51, 405–413. [Google Scholar] [CrossRef] [Green Version]
- Kržanović, N.; Stanković, K.; Živanović, M.; Đaletić, M.; Ciraj-Bjelac, O. Development and testing of a low cost radiation protection instrument based on an energy compensated Geiger-Müller tube. Radiat. Phys. Chem. 2019, 164, 108358. [Google Scholar] [CrossRef]
- Wang, P.; Tang, X.B.; Gong, P.; Huang, X.; Wen, L.S.; Han, Z.Y.; He, J.P. Des. Portable Dose Rate Detect. Based Double -Geiger -Mueller Count. Nucl. Instrum. Methods Phys. Res. Sect. Accel. Spectrom. Detect. Assoc. Equip. 2018, 879, 147–152. [Google Scholar] [CrossRef]
- Tocchi, A.; Roca, V.; Angrisani, L.; Bonavolontà, F.; Moriello, R.S.L. First step towards an IoT implementation of a wireless sensors network for environmental radiation monitoring. In Proceedings of the IEEE International Instrumentation and Measurement Technology Conference, Turin, Italy, 22–25 May 2017; pp. 1–6. [Google Scholar]
- Joo, H.; Kim, R.; Moon, J.H. Radioactivity Measurement of Radioactive Contaminated Soil by Using a Fiber-Optic Radiation Sensor. J. Korean Phys. Soc. 2016, 68, 1287–1290. [Google Scholar] [CrossRef]
- Kim, R.; Lee, S.B.; Kim, J.W.; Moon, J.H. Development and Comparison of Fiber-Optic Beta Radiation Sensors with Different Diameters of Their Sensing Probes. J. Sens. 2017, 2017, 1452765. [Google Scholar] [CrossRef] [Green Version]
- McGrath, M.J.; Scanaill, C.N.; Nafus, D. Sensor Technologies: Healthcare, Wellness and Environmental Applications; Apress: New York, NY, USA, 2014. [Google Scholar]
- Lee, J.; Khan, I.; Choi, S.; Kwon, Y.W. A Smart IoT Device for Detecting and Responding to Earthquakes. Electronics 2019, 8, 1546. [Google Scholar] [CrossRef] [Green Version]
- Zambrano, A.M.; Perez, I.; Palau, C.; Esteve, M. Technologies of Internet of Things applied to an Earthquake Early Warning System. Future Gener. Comput. Syst. 2017, 75, 206–215. [Google Scholar] [CrossRef]
- Alphonsa, A.; Ravi, G. Earthquake Early Warning System by IOT using Wireless Sensor Networks. In Proceedings of the International Conference on Wireless Communications, Signal Processing and Networking, Chennai, India, 23–25 March 2016; pp. 1201–1205. [Google Scholar]
- Pisco, M.; Bruno, F.A.; Galluzzo, D.; Nardone, L.; Gruca, G.; Rijnveld, N.; Bianco, F.; Cutolo, A.; Cusano, A. Opto-mechanical lab-on-fibre seismic sensors detected the Norcia earthquake. Sci. Rep. 2018, 8, 6680. [Google Scholar] [CrossRef] [Green Version]
- Alzaid, H.; Foo, E.; Gonzalez Nieto, J.M. Secure Data Aggregation in Wireless Sensor Network: A survey. In Proceedings of the 6th Australasian Information Security Conference, Wollongong, NSW, Australia, 1 January 2008; Volume 81, pp. 93–105. [Google Scholar]
- Anwar, M.; Abdullah, A.H.; Altameem, A.; Qureshi, K.N.; Masud, F.; Faheem, M.; Cao, Y.; Kharel, R. Green Communication for Wireless Body Area Networks: Energy Aware Link Efficient Routing Approach. Sensors 2018, 18, 3237. [Google Scholar] [CrossRef] [Green Version]
- Filipe, L.; Fdez-Riverola, F.; Costa, N.; Pereira, A. Wireless Body Area Networks for Healthcare Applications: Protocol Stack Review. Int. J. Distrib. Sens. Netw. 2015, 11, 213705. [Google Scholar] [CrossRef]
- Jawad, H.M.; Nordin, R.; Gharghan, S.K.; Jawad, A.M.; Ismail, M. Energy-Efficient Wireless Sensor Networks for Precision Agriculture: A Review. Sensors 2017, 17, 1781. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, N.; Michelin, R.A.; Xue, W.; Ruj, S.; Malaney, R.; Kanhere, S.S.; Seneviratne, A.; Hu, W.; Janicke, H.; Jha, S.K. A Survey of COVID-19 Contact Tracing Apps. IEEE Access 2020, 8, 134577–134601. [Google Scholar] [CrossRef]
- IEEE. IEEE Standard for Local and metropolitan area networks—Part 15.6: Wireless Body Area Networks. In IEEE Standards Association; IEEE: New York, NY, USA, 2012; pp. 1–271. [Google Scholar]
- Toorani, M. Security analysis of the IEEE 802.15.6 standard. Int. J. Commun. Syst. 2016, 29, 2471–2489. [Google Scholar] [CrossRef]
- Afaqui, M.S.; Garcia-Villegas, E.; Lopez-Aguilera, E. IEEE 802.11ax: Challenges and requirements for future high efficiency Wi-Fi. IEEE Wirel. Commun. 2016, 24, 130–137. [Google Scholar] [CrossRef]
- Al-Absi, M.A.; Al-Absi, A.A.; Sain, M.; Lee, H.J. A State of the Art: Future Possibility of 5G with IoT and Other Challenges. In Smart Healthcare Analytics in IoT Enabled Environment; Springer: Cham, Switzerland, 2020; pp. 35–65. [Google Scholar]
- Ahad, A.; Tahir, M.; Yau, K.L.A. 5G-Based Smart Healthcare Network: Architecture, Taxonomy, Challenges and Future Research Directions. IEEE Access 2019, 7, 100747–100762. [Google Scholar] [CrossRef]
- Lloret, J.; Parra, L.; Taha, M.; Tomás, J. An architecture and protocol for smart continuous eHealth monitoring using 5G. Comput. Netw. 2017, 129, 340–351. [Google Scholar] [CrossRef]
- Jusak, J.; Pratikno, H.; Putra, V.H. Internet of Medical Things for Cardiac Monitoring: Paving The Way to 5G Mobile Networks. In Proceedings of the 5th IEEE International Conference on Communication, Networks and Satellite, Surabaya, Indonesia, 8–10 December 2016; pp. 75–79. [Google Scholar]
- Raza, U.; Kulkarni, P.; Sooriyabandara, M. Low Power Wide Area Networks: An Overview. IEEE Commun. Surv. Tutorials 2017, 19, 855–873. [Google Scholar] [CrossRef] [Green Version]
- Del Campo, G.; Gomez, I.; Cañada, G.; Piovano, L.; Santamaria, A. Guidelines and criteria for selecting the optimal low-power wide-area network technology. In LPWAN Technologies for IoT and M2M Applications; Elsevier: Amsterdam, The Netherlands, 2020; pp. 281–305. [Google Scholar]
- Alam, M.M.; Malik, H.; Khan, M.I.; Pardy, T.; Kuusik, A.; Le Moullec, Y. A Survey on the Roles of Communication Technologies in IoT-Based Personalized Healthcare Applications. IEEE Access 2018, 6, 36611–36631. [Google Scholar] [CrossRef]
- Mekki, K.; Bajic, E.; Chaxel, F.; Meyer, F. A comparative study of LPWAN technologies for large-scale IoT deployment. ICT Express 2019, 5, 1–7. [Google Scholar] [CrossRef]
- Aernouts, M.; Berkvens, R.; Van Vlaenderen, K.; Weyn, M. Sigfox and LoRaWAN Datasets for Fingerprint Localization in Large Urban and Rural Areas. Data 2018, 3, 13. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Raghunathan, A.; Jha, N.K. Hijacking an Insulin Pump: Security Attacks and Defenses for a Diabetes Therapy System. In Proceedings of the IEEE 13th International Conference on E-Health Networking, Applications and Services, Columbia, MO, USA, 13–15 June 2011; pp. 150–156. [Google Scholar]
- Kuehn, B.M. Pacemaker Recall Highlights Security Concerns for Implantable Devices. Circulation 2018, 138, 1597–1598. [Google Scholar] [CrossRef] [PubMed]
- Liebowitz, J.; Schaller, R. Biological Warfare: Tampering with implantable medical devices. IT Prof. 2015, 17, 70–72. [Google Scholar] [CrossRef]
- Halperin, D.; Heydt-Benjamin, T.S.; Ransford, B.; Clark, S.S.; Defend, B.; Morgan, W.; Fu, K.; Kohno, T.; Maisel, W.H. Pacemakers and Implantable Cardiac Defibrillators: Software Radio Attacks and Zero-Power Defenses. In Proceedings of the IEEE Symposium on Security and Privacy, Oakland, CA, USA, 18–22 May 2008; pp. 129–142. [Google Scholar]
- Yaqoob, T.; Abbas, H.; Atiquzzaman, M. Security Vulnerabilities, Attacks, Countermeasures, and Regulations of Networked Medical Devices—A Review. IEEE Commun. Surv. Tutorials 2019, 21, 3723–3768. [Google Scholar] [CrossRef]
- Fiaidhi, J.; Mohammed, S. Security and Vulnerability of Extreme Automation Systems: The IoMT and IoA Case Studies. IT Prof. 2019, 21, 48–55. [Google Scholar] [CrossRef]
- Papageorgiou, A.; Strigkos, M.; Politou, E.; Alepis, E.; Solanas, A.; Patsakis, C. Security and Privacy Analysis of Mobile Health Applications: The Alarming State of Practice. IEEE Access 2018, 6, 9390–9403. [Google Scholar] [CrossRef]
- Aliasgari, M.; Black, M.; Yadav, N. Security Vulnerabilities in Mobile Health Applications. In Proceedings of the IEEE Conference on Application, Information and Network Security, Langkawi, Malaysia, 21–22 November 2018; pp. 21–26. [Google Scholar]
- Zuo, C.; Wen, H.; Lin, Z.; Zhang, Y. Automatic Fingerprinting of Vulnerable BLE IoT Devices with Static UUIDs from Mobile Apps. In Proceedings of the ACM SIGSAC Conference on Computer and Communications Security, London, UK, 11–15 November 2019; pp. 1469–1483. [Google Scholar]
- Aloseel, A.; He, H.; Shaw, C.; Khan, M.A. Analytical Review of Cybersecurity for Embedded Systems. IEEE Access 2020, 9, 961–982. [Google Scholar] [CrossRef]
- Agrawal, S.; Das, M.L.; Lopez, J. Detection of Node Capture Attack in Wireless Sensor Networks. IEEE Syst. J. 2018, 13, 238–247. [Google Scholar] [CrossRef]
- Wang, C.; Wang, D.; Tu, Y.; Xu, G.; Wang, H. Understanding Node Capture Attacks in User Authentication Schemes for Wireless Sensor Networks. IEEE Trans. Dependable Secur. Comput. 2020, 1–20. [Google Scholar] [CrossRef]
- Lin, C.; Wu, G.; Qiu, T.; Deng, J. A low-cost node capture attack algorithm for wireless sensor networks. Int. J. Commun. Syst. 2016, 29, 1251–1268. [Google Scholar] [CrossRef]
- Bostami, B.; Ahmed, M.; Choudhury, S. False Data Injection Attacks in Internet of Things. In Performability in Internet of Things; Springer: Cham, Switzerland, 2019; pp. 47–58. [Google Scholar]
- Ahmed, M.; Pathan, A.S.K. False data injection attack (FDIA): An overview and new metrics for fair evaluation of its countermeasure. Complex Adapt. Syst. Model. 2020, 8, 4. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.; Barkat Ullah, A.S.S.M. False Data Injection Attacks in Healthcare. In Proceedings of the 15th Australasian Conference on Data Mining, Melbourne, VIC, Australia, 19–20 August 2017; Springer: Singapore, 2017; pp. 192–202. [Google Scholar]
- Pirretti, M.; Zhu, S.; Vijaykrishnan, N.; McDaniel, P.; Kandemir, M.; Brooks, R. The Sleep Deprivation Attack in Sensor Networks: Analysis and Methods of Defense. Int. J. Distrib. Sens. Netw. 2006, 2, 267–287. [Google Scholar] [CrossRef]
- Nguyen, V.L.; Lin, P.C.; Hwang, R.H. Energy Depletion Attacks in Low Power Wireless Networks. IEEE Access 2019, 7, 51915–51932. [Google Scholar] [CrossRef]
- Hei, X.; Du, X.; Wu, J.; Hu, F. Defending Resource Depletion Attacks on Implantable Medical Devices. In Proceedings of the 53th IEEE Global Telecommunications Conference, Miami, FL, USA, 6–10 December 2010; pp. 1–5. [Google Scholar]
- Marin, E.; Singelee, D.; Garcia, F.D.; Chothia, T.; Willems, R.; Preneel, B. On the (in)security of the Latest Generation Implantable Cardiac Defibrillators and How to Secure Them. In Proceedings of the 32nd Annual Conference on Computer Security Applications, Los Angeles, CA, USA, 5–8 December 2016; pp. 226–236. [Google Scholar]
- Spreitzer, R.; Moonsamy, V.; Korak, T.; Mangard, S. Systematic Classification of Side-Channel Attacks: A Case Study for Mobile Devices. IEEE Commun. Surv. Tutorials 2017, 20, 465–488. [Google Scholar] [CrossRef] [Green Version]
- Spence, A.; Bangay, S. Side-Channel Sensing: Exploiting Side-Channels to Extract Information for Medical Diagnostics and Monitoring. IEEE J. Transl. Eng. Health Med. 2020, 8, 4900213. [Google Scholar] [CrossRef]
- Maiti, A.; Jadliwala, M.; He, J.; Bilogrevic, I. Side-Channel Inference Attacks on Mobile Keypads Using Smartwatches. IEEE Trans. Mob. Comput. 2018, 17, 2180–2194. [Google Scholar] [CrossRef] [Green Version]
- Maiti, A.; Heard, R.; Sabra, M.; Jadliwala, M. Towards Inferring Mechanical Lock Combinations using Wrist-Wearables as a Side-Channel. In Proceedings of the 11th ACM Conference on Security & Privacy in Wireless and Mobile Networks, Stockholm, Sweden, 18–20 June 2018; pp. 111–122. [Google Scholar]
- Liu, X.; Zhou, Z.; Diao, W.; Li, Z.; Zhang, K. When Good Becomes Evil: Keystroke Inference with Smartwatch. In Proceedings of the 22nd ACM SIGSAC Conference on Computer and Communications Security, Denver, CO, USA, 12–16 October 2015; pp. 1273–1285. [Google Scholar]
- Kune, D.F.; Backes, J.; Clark, S.S.; Kramer, D.; Reynolds, M.; Fu, K.; Kim, Y.; Xu, W. Ghost Talk: Mitigating EMI Signal Injection Attacks against Analog Sensors. In Proceedings of the IEEE Symposium on Security and Privacy, Berkeley, CA, USA, 19–22 May 2013; pp. 145–159. [Google Scholar]
- HP Inc. HP Study Reveals Smartwatches Vulnerable to Attack. Available online: https://www8.hp.com/us/en/hp-news/press-release.html?id=2037386 (accessed on 1 August 2021).
- Shim, J.; Lim, K.; Jeong, J.; Cho, S.J.; Park, M.; Han, S. A Case Study on Vulnerability Analysis and Firmware Modification Attack for a Wearable Fitness Tracker. IT Converg. Pract. 2017, 5, 25–33. [Google Scholar]
- Rieck, J. Attacks on Fitness Trackers Revisited: A Case-Study of Unfit Firmware Security. arXiv 2016, arXiv:1604.03313. [Google Scholar]
- Arias, O.; Wurm, J.; Hoang, K.; Jin, Y. Privacy and Security in Internet of Things and Wearable Devices. IEEE Trans. Multi-Scale Comput. Syst. 2015, 1, 99–109. [Google Scholar] [CrossRef]
- Classen, J.; Wegemer, D.; Patras, P.; Spink, T.; Hollick, M. Anatomy of a Vulnerable Fitness Tracking System: Dissecting the Fitbit Cloud, App, and Firmware. Proc. ACM Interact. Mobile Wear. Ubiquitous Technol. 2018, 2, 5. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.; Park, S.; Choi, K.; Kim, Y. BurnFit: Analyzing and Exploiting Wearable Devices. In Proceedings of the International Workshop on Information Security Applications, Jeju Island, Korea, 20–22 August 2015; Springer: Cham, Switzerland, 2015; pp. 227–239. [Google Scholar]
- Hanna, S.; Rolles, R.; Molina-Markham, A.; Poosankam, P.; Blocki, J.; Fu, K.; Song, D. Take Two Software Updates and See Me in the Morning: The Case for Software Security Evaluations of Medical Devices. In Proceedings of the 2nd USENIX Workshop on Health Security and Privacy, San Francisco, CA, USA, 9 August 2011. [Google Scholar]
- Zou, Y.; Wang, G. Intercept Behavior Analysis of Industrial Wireless Sensor Networks in the Presence of Eavesdropping Attack. IEEE Trans. Ind. Inform. 2015, 12, 780–787. [Google Scholar] [CrossRef] [Green Version]
- Xu, Q.; Ren, P.; Song, H.; Du, Q. Security Enhancement for IoT Communications Exposed to Eavesdroppers with Uncertain Locations. IEEE Access 2016, 4, 2840–2853. [Google Scholar] [CrossRef]
- Zorz, Z. Critical Bluetooth Flaw Opens Millions of Devices to Eavesdropping Attacks. Available online: https://www.helpnetsecurity.com/2019/08/16/bluetooth-cve-2019-9506/ (accessed on 1 August 2021).
- Ryan, M. Bluetooth: With Low Energy comes Low Security. In Proceedings of the 7th USENIX Workshop on Offensive Technologies, Washington, DC, USA, 13 August 2013; pp. 1–7. [Google Scholar]
- Fawaz, K.; Kim, K.H.; Shin, K.G. Protecting Privacy of BLE Device Users. In Proceedings of the 25th USENIX Security Symposium, Austin, TX, USA, 10–12 August 2016; pp. 1205–1221. [Google Scholar]
- Moses, V.; Korah, I. Lack of Security of Networked Medical Equipment in Radiology. Am. J. Roentgenol. 2015, 204, 343–353. [Google Scholar] [CrossRef]
- Cusack, B.; Antony, B.; Ward, G.; Mody, S. Assessment of security vulnerabilities in wearable devices. Proceedings of 15th Australian Information Security Management Conference, Edith Cowan University, Perth, WA, Australia, 5–6 December 2017; pp. 42–48. [Google Scholar]
- Goyal, R.; Dragoni, N.; Spognardi, A. Mind The Tracker You Wear—A Security Analysis of Wearable Health Trackers. In Proceedings of the 31st Annual ACM Symposium on Applied Computing, Pisa, Italy, 4–8 April 2016; pp. 131–136. [Google Scholar]
- Das, A.K.; Pathak, P.H.; Chuah, C.N.; Mohapatra, P. Uncovering Privacy Leakage in BLE Network Traffic of Wearable Fitness Trackers. In Proceedings of the 17th International Workshop on Mobile Computing Systems and Applications, St. Augustine, FL, USA, 23–24 February 2016; pp. 99–104. [Google Scholar]
- Lotfy, K.; Hale, M.L. Assessing Pairing and Data Exchange Mechanism Security in the Wearable Internet of Things. In Proceedings of the IEEE International Conference on Mobile Services, San Francisco, CA, USA, 27 June–2 July 2016; pp. 25–32. [Google Scholar]
- Rahman, M.; Carbunar, B.; Topkara, U. Secure Management of Low Power Fitness Trackers. IEEE Trans. Mob. Comput. 2015, 15, 447–459. [Google Scholar] [CrossRef] [Green Version]
- Hei, X.; Du, X.; Lin, S.; Lee, I.; Sokolsky, O. Patient Infusion Pattern based Access Control Schemes for Wireless Insulin Pump System. IEEE Trans. Parallel Distrib. Syst. 2014, 26, 3108–3121. [Google Scholar] [CrossRef]
- Li, Y.; Barthelemy, J.; Sun, S.; Perez, P.; Moran, B. A Case Study of WiFi Sniffing Performance Evaluation. IEEE Access 2020, 8, 129224–129235. [Google Scholar] [CrossRef]
- Morgner, P.; Mattejat, S.; Benenson, Z.; Müller, C.; Armknecht, F. Insecure to the Touch: Attacking ZigBee 3.0 via Touchlink Commissioning. In Proceedings of the 10th ACM Conference on Security and Privacy in Wireless and Mobile Networks, Boston, MA, USA, 18–20 July 2017; pp. 230–240. [Google Scholar]
- Bodei, C.; Galletta, L. Tracking sensitive and untrustworthy data in IoT. In Proceedings of the The Italian Conference on Cybersecurity, Venice, Italy, 17–20 January 2017; Volume 1816, pp. 38–52. [Google Scholar]
- Siddiqi, M.; Sivaraman, V.; Jha, S. Timestamp Integrity in Wearable Healthcare Devices. In Proceedings of the IEEE International Conference on Advanced Networks and Telecommunications Systems, Bangalore, India, 6–9 November 2016; pp. 1–6. [Google Scholar]
- Kimergård, A.; Breindahl, T.; Hindersson, P.; Deluca, P. Tampering of opioid analgesics: A serious challenge for public health? Addiction 2016, 111, 1701–1702. [Google Scholar] [CrossRef]
- Fereidooni, H.; Frassetto, T.; Miettinen, M.; Sadeghi, A.R.; Conti, M. Fitness Trackers: Fit for Health but Unfit for Security and Privacy. In Proceedings of the IEEE/ACM International Conference on Connected Health: Applications, Systems and Engineering Technologies, Philadelphia, PA, USA, 17–19 July 2017; pp. 19–24. [Google Scholar]
- Morgner, P.; Pfennig, S.; Salzner, D.; Benenson, Z. Malicious IoT Implants: Tampering with Serial Communication over the Internet. In Proceedings of the International Symposium on Research in Attacks, Intrusions, and Defenses, Heraklion, Crete, Greece, 10–12 September 2018; pp. 535–555. [Google Scholar]
- Kim, J.; Song, J. A Simple and Efficient Replay Attack Prevention Scheme for LoRaWAN. In Proceedings of the 7th International Conference on Communication and Network Security, Tokyo, Japan, 24–26 November 2017; pp. 32–36. [Google Scholar]
- Jin, H.; Zhou, K.; Jiang, H.; Lei, D.; Wei, R.; Li, C. Full integrity and freshness for cloud data. Future Gener. Comput. Syst. 2018, 80, 640–652. [Google Scholar] [CrossRef]
- Belkhouja, T.; Du, X.; Mohamed, A.; Al-Ali, A.K.; Guizani, M. New Plain-Text Authentication Secure Scheme for Implantable Medical Devices with Remote Control. In Proceedings of the IEEE Global Communications Conference, Singapore, 4–8 December 2017; pp. 1–5. [Google Scholar]
- Rughoobur, P.; Nagowah, L. A Lightweight Replay Attack Detection Framework for Battery Depended IoT Devices Designed for Healthcare. In Proceedings of the International Conference on Infocom Technologies and Unmanned Systems, Dubai, United Arab Emirates, 18–20 December 2017; pp. 811–817. [Google Scholar]
- Spring, R.; Freudenthal, E.; Estevez, L. Practical Techniques for Limiting Disclosure of RF-Equipped Medical Devices. In Proceedings of the IEEE Dallas Engineering in Medicine and Biology Workshop, Dallas, TX, USA, 11–12 November 2007; pp. 82–85. [Google Scholar]
- Ali, A.; Khan, F.A. Energy-efficient cluster-based security mechanism for intra-WBAN and inter-WBAN communications for healthcare applications. EURASIP J. Wirel. Commun. Netw. 2013, 2013, 216. [Google Scholar] [CrossRef] [Green Version]
- Radcliffe, J. Hacking Medical Devices for Fun and Insulin: Breaking the Human SCADA System. In Proceedings of the Black Hat Conference, Las Vegas, NV, USA, 30 July–4 August 2011; Volume 2011. [Google Scholar]
- Yılmaz, M.H.; Arslan, H. A Survey: Spoofing Attacks in Physical Layer Security. In Proceedings of the IEEE 40th Local Computer Networks Conference, Clearwater Beach, FL, USA, 26–29 October 2015; pp. 812–817. [Google Scholar]
- Mirkovic, J.; Kline, E.; Reiher, P. RESECT: Self–Learning Traffic Filters for IP Spoofing Defense. In Proceedings of the 33rd Annual Computer Security Applications Conference, Orlando, FL, USA, 4–8 December 2017; pp. 474–485. [Google Scholar]
- Zhang, C.; Hu, G.; Chen, G.; Sangaiah, A.K.; Zhang, P.; Yan, X.; Jiang, W. Towards a SDN-Based Integrated Architecture for Mitigating IP Spoofing Attack. IEEE Access 2017, 6, 22764–22777. [Google Scholar] [CrossRef]
- Park, Y.; Son, Y.; Shin, H.; Kim, D.; Kim, Y. This ain’t your dose: Sensor Spoofing Attack on Medical Infusion Pump. In Proceedings of the 10th USENIX Workshop on Offensive Technologies, Austin, TX, USA, 8–9 August 2016; pp. 1–11. [Google Scholar]
- Zhang, P.; Nagarajan, S.G.; Nevat, I. Secure Location of Things (SLOT): Mitigating Localization Spoofing Attacks in the Internet of Things. IEEE Internet Things J. 2017, 4, 2199–2206. [Google Scholar] [CrossRef]
- Tippenhauer, N.O.; Pöpper, C.; Rasmussen, K.B.; Capkun, S. On the Requirements for Successful GPS Spoofing Attacks. In Proceedings of the 18th ACM Conference on Computer and communications Security, Chicago, IL, USA, 17–21 October 2011; pp. 75–86. [Google Scholar]
- Conti, M.; Dragoni, N.; Lesyk, V. A Survey of Man In The Middle Attacks. IEEE Commun. Surv. Tutorials 2016, 18, 2027–2051. [Google Scholar] [CrossRef]
- Wazid, M.; Das, A.K.; Rodrigues, J.J.P.C.; Shetty, S.; Park, Y. IoMT Malware Detection Approaches: Analysis and Research Challenges. IEEE Access 2019, 8, 182459–182476. [Google Scholar] [CrossRef]
- Navas, R.E.; Le Bouder, H.; Cuppens, N.; Cuppens, F.; Papadopoulos, G.Z. Do not trust your neighbors! A small IoT platform illustrating a man-in-the-middle attack. In Proceedings of the International Conference on Ad-Hoc Networks and Wireless, Saint-Malo, France, 5–7 September 2018; pp. 120–125. [Google Scholar]
- Hale, M.L.; Lotfy, K.; Gamble, R.F.; Walter, C.; Lin, J. Developing a platform to evaluate and assess the security of wearable devices. Digit. Commun. Netw. 2019, 5, 147–159. [Google Scholar] [CrossRef]
- Sun, D.Z.; Mu, Y.; Susilo, W. Man-in-the-Middle Attacks on Secure Simple Pairing in Bluetooth Standard V5.0 and Its Countermeasure. Pers. Ubiquitous Comput. 2018, 22, 55–67. [Google Scholar] [CrossRef]
- Belkhouja, T.; Mohamed, A.; Al-Ali, A.K.; Du, X.; Guizani, M. Light-Weight Solution to Defend Implantable Medical Devices against Man-In-The-Middle Attack. In Proceedings of the IEEE Global Communications Conference, Abu Dhabi, United Arab Emirates, 9–13 December 2018; pp. 1–5. [Google Scholar]
- Ahmad, F.; Adnane, A.; Franqueira, V.N.L.; Kurugollu, F.; Liu, L. Man-In-The-Middle Attacks in Vehicular Ad-Hoc Networks: Evaluating the Impact of Attackers’ Strategies. Sensors 2018, 18, 4040. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, F.; Kurugollu, F.; Adnane, A.; Hussain, R.; Hussain, F. MARINE: Man-in-the-middle Attack Resistant trustmodel IN connEcted vehicles. IEEE Internet Things J. 2020, 7, 3310–3322. [Google Scholar] [CrossRef] [Green Version]
- Kazlouski, A.; Marchioro, T.; Manifavas, H.; Markatos, E.P. I still See You! Inferring Fitness Data from Encrypted Traffic of Wearables. In Proceedings of the 14th International Joint Conference on Biomedical Engineering Systems and Technologies, Lisbon, Portugal, 11–13 February 2021; pp. 369–376. [Google Scholar]
- Fereidooni, H.; Classen, J.; Spink, T.; Patras, P.; Miettinen, M.; Sadeghi, A.R.; Hollick, M.; Conti, M. Breaking Fitness Records without Moving: Reverse Engineering and Spoofing Fitbit. In Proceedings of the International Symposium on Research in Attacks, Intrusions, and Defenses, Atlanta, GA, USA, 18–20 September 2017; pp. 48–69. [Google Scholar]
- Pournaghshband, V.; Sarrafzadeh, M.; Reiher, P. Securing Legacy Mobile Medical Devices. In Proceedings of the International Conference on Wireless Mobile Communication and Healthcare, Paris, France, 21–23 November 2012; Springer: Berlin/Heidelberg, Germany, 2012; pp. 163–172. [Google Scholar]
- Marin, E.; Argones-Rúa, E.; Singelée, D.; Preneel, B. A survey on physiological-signal-based security for medical devices. IACR Cryptol. Eprint Arch. 2016, 2016, 867. [Google Scholar]
- Rostami, M.; Burleson, W.; Koushanfar, F.; Juels, A. Balancing Security and Utility in Medical Devices? In Proceedings of the 50th Annual Design Automation Conference, Austin, TX, USA, 29 May 2013–7 June 2013; pp. 1–6. [Google Scholar]
- Hoque, N.; Bhattacharyya, D.K.; Kalita, J.K. Botnet in DDoS Attacks: Trends and Challenges. IEEE Commun. Surv. Tutorials 2015, 17, 2242–2270. [Google Scholar] [CrossRef]
- Vadlamani, S.; Eksioglu, B.; Medal, H.; Nandi, A. Jamming attacks on wireless networks: A taxonomic survey. Int. J. Prod. Econ. 2016, 172, 76–94. [Google Scholar] [CrossRef]
- Subasini, C.A.; Karuppiah, S.P.; Sheeba, A.; Padmakala, S. Developing an attack detection framework for wireless sensor network-based healthcare applications using hybrid convolutional neural network. Trans. Emerg. Telecommun. Technol. 2021, e4336. [Google Scholar]
- Kolias, C.; Kambourakis, G.; Stavrou, A.; Voas, J. DDoS in the IoT: Mirai and Other Botnets. Computer 2017, 50, 80–84. [Google Scholar] [CrossRef]
- De Donno, M.; Dragoni, N.; Giaretta, A.; Spognardi, A. DDoS-Capable IoT Malwares: Comparative Analysis and Mirai Investigation. Secur. Commun. Netw. 2018, 2018, 7178164. [Google Scholar] [CrossRef] [Green Version]
- Ellouze, N.; Allouche, M.; Ahmed, H.B.; Rekhis, S.; Boudriga, N. Security of implantable medical devices: Limits, requirements, and proposals. Secur. Commun. Netw. 2014, 7, 2475–2491. [Google Scholar] [CrossRef]
- Ye, Y.; Li, T.; Adjeroh, D.; Iyengar, S.S. A Survey on Malware Detection Using Data Mining Techniques. ACM Comput. Surv. 2017, 50, 1–40. [Google Scholar] [CrossRef]
- Or-Meir, O.; Nissim, N.; Elovici, Y.; Rokach, L. Dynamic Malware Analysis in the Modern Era—A State of the Art Survey. ACM Comput. Surv. 2019, 52, 41. [Google Scholar] [CrossRef] [Green Version]
- Hernandez-Castro, J.; Cartwright, A.; Cartwright, E. An economic analysis of ransomware and its welfare consequences. R. Soc. Open Sci. 2020, 7, 190023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vignau, B.; Khoury, R.; Hallé, S. 10 Years of IoT Malware: A Feature-Based Taxonomy. In Proceedings of the IEEE 19th International Conference on Software Quality, Reliability and Security Companion, Sofia, Bulgaria, 22–26 July 2019; pp. 458–465. [Google Scholar]
- Martin, G.; Ghafur, S.; Kinross, J.; Hankin, C.; Darzi, A. WannaCry—A year on. BMJ 2018, 361, k2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isaak, J.; Hanna, M.J. User Data Privacy: Facebook, Cambridge Analytica, and Privacy Protection. Computer 2018, 51, 56–59. [Google Scholar] [CrossRef]
- Newcomb, A. Hacked MyFitnessPal Data Goes on Sale on the Dark Web—One Year After the Breach. Available online: https://fortune.com/2019/02/14/hacked-myfitnesspal-data-sale-dark-web-one-year-breach/ (accessed on 1 August 2021).
- Thielman, S. Yahoo Hack: 1bn Accounts Compromised by Biggest Data Breach in History. Available online: https://www.theguardian.com/technology/2016/dec/14/yahoo-hack-security-of-one-billion-accounts-breached (accessed on 1 August 2021).
- Mitnick, K.D.; Simon, W.L. The Art of Deception: Controlling the Human Element of Security; John Wiley & Sons: Hoboken, NJ, USA, 2003. [Google Scholar]
- Chiew, K.L.; Yong, K.S.C.; Tan, C.L. A survey of phishing attacks: Their types, vectors and technical approaches. Expert Syst. Appl. 2018, 106, 1–20. [Google Scholar] [CrossRef]
- Anti-Phishing Working Group. Phishing Activity Trends Report—3rd Quarter 2020; Technical Report; Anti-Phishing Working Group: Washington, DC, USA, 2020. [Google Scholar]
- The US Department of Justice. Department of Justice Announces Disruption of Hundreds of Online COVID-19 Related Scams—Hundreds of Domains Disrupted through Public and Private Sector Cooperative Efforts. Available online: https://www.justice.gov/opa/pr/department-justice-announces-disruption-hundreds-online-COVID-19-related-scams, (accessed on 1 August 2021).
- Symanovich, S. Coronavirus Phishing Emails: How to Protect against COVID-19 Scams. Available online: https://us.norton.com/internetsecurity-online-scams-coronavirus-phishing-scams.html (accessed on 1 August 2021).
- Priestman, W.; Anstis, T.; Sebire, I.G.; Sridharan, S.; Sebire, N.J. Phishing in healthcare organisations: Threats, mitigation and approaches. BMJ Health Care Inform. 2019, 26, e100031. [Google Scholar] [CrossRef] [Green Version]
- Wright, A.; Aaron, S.; Bates, D.W. The Big Phish: Cyberattacks Against U.S. Healthcare Systems. J. Gen. Intern. Med. 2016, 31, 1115–1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalali, M.S.; Bruckes, M.; Westmattelmann, D.; Schewe, G. Why Employees (Still) Click on Phishing Links: Investigation in Hospitals. J. Med. Internet Res. 2020, 22, e16775. [Google Scholar] [CrossRef] [PubMed]
- McKay, K.A.; Bassham, L.; Sönmez Turan, M.; Mouha, N. Report on Lightweight Cryptography; Technical Report DRAFT NISTIR 8114; National Institute of Standards and Technology: Gaithersburg, MD, USA, 2016.
- Buchanan, W.J.; Li, S.; Asif, R. Lightweight cryptography methods. J. Cyber Secur. Technol. 2017, 1, 187–201. [Google Scholar] [CrossRef] [Green Version]
- ISO Central Secretary. Information Technology—Security Techniques—Lightweight Cryptography; Technical Report ISO/IEC Standard 29192; International Organization for Standardization: Geneva, Switzerland, 2012. [Google Scholar]
- Biryukov, A.; Perrin, L. State of the Art in Lightweight Symmetric Cryptography. Cryptology ePrint Archive, Report 2017/511. 2017. Available online: https://eprint.iacr.org/2017/511 (accessed on 1 August 2021).
- Bogdanov, A.; Knudsen, L.R.; Leander, G.; Paar, C.; Poschmann, A.; Robshaw, M.J.B.; Seurin, Y.; Vikkelsoe, C. PRESENT: An Ultra-Lightweight Block Cipher. In International Workshop on Cryptographic Hardware and Embedded Systems; Springer: Berlin/Heidelberg, Germany, 2007; pp. 450–466. [Google Scholar]
- Shirai, T.; Shibutani, K.; Akishita, T.; Moriai, S.; Iwata, T. The 128-Bit Blockcipher CLEFIA. In International Workshop on Fast Software Encryption; Springer: Berlin/Heidelberg, Germany, 2007; pp. 181–195. [Google Scholar]
- Hong, D.; Lee, J.K.; Kim, D.C.; Kwon, D.; Ryu, K.H.; Lee, D.G. LEA: A 128-Bit Block Cipher for Fast Encryption on Common Processors. In International Workshop on Information Security Applications; Springer: Cham, Switzerland, 2013; pp. 3–27. [Google Scholar]
- Watanabe, D.; Ideguchi, K.; Kitahara, J.; Muto, K.; Furuichi, H.; Kaneko, T. Enocoro-80: A Hardware Oriented Stream Cipher. In Proceedings of the 3rd International Conference on Availability, Reliability and Security, Barcelona, Spain, 4–7 March 2008; pp. 1294–1300. [Google Scholar]
- De Canniere, C.; Preneel, B. Trivium. In New Stream Cipher Designs; Springer: Berlin/Heidelberg, Germany, 2008; pp. 244–266. [Google Scholar]
- Lara-Nino, C.A.; Diaz-Perez, A.; Morales-Sandoval, M. Elliptic Curve Lightweight Cryptography: A Survey. IEEE Access 2018, 6, 72514–72550. [Google Scholar] [CrossRef]
- Suárez-Albela, M.; Fraga-Lamas, P.; Fernández-Caramés, T.M. A Practical Evaluation on RSA and ECC-Based Cipher Suites for IoT High-Security Energy-Efficient Fog and Mist Computing Devices. Sensors 2018, 18, 3868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suárez-Albela, M.; Fernández-Caramés, T.M.; Fraga-Lamas, P.; Castedo, L. A Practical Performance Comparison of ECC and RSA for Resource-Constrained IoT Devices. In Proceedings of the Global Internet of Things Summit, Bilbao, Spain, 4–7 June 2018; pp. 1–6. [Google Scholar]
- Liu, Z.; Huang, X.; Hu, Z.; Khan, M.K.; Seo, H.; Zhou, L. On Emerging Family of Elliptic Curves to Secure Internet of Things: ECC Comes of Age. IEEE Trans. Dependable Secur. Comput. 2016, 14, 237–248. [Google Scholar] [CrossRef]
- Marin, L.; Pawlowski, M.P.; Jara, A. Optimized ECC Implementation for Secure Communication between Heterogeneous IoT Devices. Sensors 2015, 15, 21478–21499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, A.; Ning, P. TinyECC: A Configurable Library for Elliptic Curve Cryptographyin Wireless Sensor Networks. In Proceedings of the International Conference on Information Processing in Sensor Networks, St. Louis, MO, USA, 22–24 April 2008; pp. 245–256. [Google Scholar]
- Nejatollahi, H.; Dutt, N.; Ray, S.; Regazzoni, F.; Banerjee, I.; Cammarota, R. Post-Quantum Lattice-Based Cryptography Implementations: A Survey. ACM Comput. Surv. 2019, 51, 129. [Google Scholar] [CrossRef]
- Liu, Z.; Azarderakhsh, R.; Kim, H.; Seo, H. Efficient Software Implementation of Ring-LWE Encryption on IoT Processors. IEEE Trans. Comput. 2017, 69, 1424–1433. [Google Scholar] [CrossRef] [Green Version]
- Xiao, D.; Yu, Y. Cryptanalysis of Compact-LWE and Related Lightweight Public Key Encryption. Secur. Commun. Netw. 2018, 2018, 4957045. [Google Scholar] [CrossRef]
- Guo, J.; Peyrin, T.; Poschmann, A. The PHOTON Family of Lightweight Hash Functions. In Proceedings of the Annual Cryptology Conference; Springer: Berlin/Heidelberg, Germany, 2011; pp. 222–239. [Google Scholar]
- Bogdanov, A.; Knežević, M.; Leander, G.; Toz, D.; Varıcı, K.; Verbauwhede, I. SPONGENT: A Lightweight Hash Function. In International Workshop on Cryptographic Hardware and Embedded Systems; Springer: Berlin/Heidelberg, Germany, 2011; pp. 312–325. [Google Scholar]
- Hirose, S.; Ideguchi, K.; Kuwakado, H.; Owada, T.; Preneel, B.; Yoshida, H. A Lightweight 256-Bit Hash Function for Hardware and Low-End Devices: Lesamnta-LW. In Proceedings of the International Conference on Information Security and Cryptology, Seoul, Korea, 1–3 December 2010; Springer: Berlin/Heidelberg, Germany, 2010; pp. 151–168. [Google Scholar]
- Luykx, A.; Preneel, B.; Tischhauser, E.; Yasuda, K. A MAC Mode for Lightweight Block Ciphers. In Proceedings of the 23rd International Conference on Fast Software Encryption; Springer: Berlin/Heidelberg, Germany, 2016; pp. 43–59. [Google Scholar]
- Mouha, N.; Mennink, B.; Van Herrewege, A.; Watanabe, D.; Preneel, B.; Verbauwhede, I. Chaskey: An Efficient MAC Algorithm for 32-bit Microcontrollers. In Proceedings of the International Conference on Selected Areas in Cryptography; Springer: Cham, Switzerland, 2014; pp. 306–323. [Google Scholar]
- Bakiri, M.; Guyeux, C.; Couchot, J.F.; Marangio, L.; Galatolo, S. A Hardware and Secure Pseudorandom Generator for Constrained Devices. IEEE Trans. Ind. Inform. 2018, 14, 3754–3765. [Google Scholar] [CrossRef]
- Orúe López, A.B.; Hernández Encinas, L.; Martín Muñoz, A.; Montoya Vitini, F. A Lightweight Pseudorandom Number Generator for Securing the Internet of Things. IEEE Access 2017, 5, 27800–27806. [Google Scholar] [CrossRef]
- Wallace, K.; Moran, K.; Novak, E.; Zhou, G.; Sun, K. Toward Sensor-Based Random Number Generation for Mobile and IoT Devices. IEEE Internet Things J. 2016, 3, 1189–1201. [Google Scholar] [CrossRef]
- Xu, F.; Qin, Z.; Tan, C.C.; Wang, B.; Li, Q. IMDGuard: Securing Implantable Medical Devices with the External Wearable Guardian. In Proceedings of the IEEE INFOCOM, Shanghai, China, 10–15 April 2011; pp. 1862–1870. [Google Scholar]
- Zhang, Z.; Wang, H.; Vasilakos, A.V.; Fang, H. ECG-Cryptography and Authentication in Body Area Networks. IEEE Trans. Inf. Technol. Biomed. 2012, 16, 1070–1078. [Google Scholar] [CrossRef]
- Yao, L.; Liu, B.; Yao, K.; Wu, G.; Wang, J. An ECG-Based Signal Key Establishment Protocol in Body Area Networks. In Proceedings of the 7th International Conference on Ubiquitous Intelligence & Computing and 7th International Conference on Autonomic & Trusted Computing, Xi’an, China, 26–29 October 2010; pp. 233–238. [Google Scholar]
- Rushanan, M.; Rubin, A.D.; Kune, D.F.; Swanson, C.M. SoK: Security and Privacy in Implantable Medical Devices and Body Area Networks. In Proceedings of the IEEE Symposium on Security and Privacy, Berkeley, CA, USA, 18–21 May 2014; pp. 524–539. [Google Scholar]
- Hu, C.; Cheng, X.; Zhang, F.; Wu, D.; Liao, X.; Chen, D. OPFKA: Secure and Efficient Ordered-Physiological-Feature-based Key Agreement for Wireless Body Area Networks. In Proceedings of the IEEE INFOCOM, Turin, Italy, 14–19 April 2013; pp. 2274–2282. [Google Scholar]
- Xu, W.; Javali, C.; Revadigar, G.; Luo, C.; Bergmann, N.; Hu, W. Gait-Key: A Gait-Based Shared Secret Key Generation Protocol for Wearable Devices. ACM Trans. Sens. Netw. 2017, 13, 6. [Google Scholar] [CrossRef]
- Revadigar, G.; Javali, C.; Xu, W.; Vasilakos, A.V.; Hu, W.; Jha, S. Accelerometer and Fuzzy Vault-Based Secure Group Key Generation and Sharing Protocol for Smart Wearables. IEEE Trans. Inf. Forensics Secur. 2017, 12, 2467–2482. [Google Scholar] [CrossRef]
- Effatparvar, M.; Dehghan, M.; Rahmani, A.M. A comprehensive survey of energy-aware routing protocols in wireless body area sensor networks. J. Med. Syst. 2016, 40, 201. [Google Scholar] [CrossRef]
- Bhanumathi, V.; Sangeetha, C.P. A guide for the selection of routing protocols in WBAN for healthcare applications. Hum.-Centric Comput. Inf. Sci. 2017, 7, 24. [Google Scholar] [CrossRef]
- Airehrour, D.; Gutierrez, J.; Ray, S.K. Secure routing for internet of things: A survey. J. Netw. Comput. Appl. 2016, 66, 198–213. [Google Scholar] [CrossRef]
- Boudargham, N.; Abdo, J.B.; Demerjian, J.; Guyeux, C.; Atechian, T. Efficient Cluster-Based Routing Algorithm for Body Sensor Networks. In Proceedings of the IEEE Middle East and North Africa Communications Conference, Jounieh, Lebanon, 18–20 April 2018; pp. 1–6. [Google Scholar]
- Rajagopalan, R. Energy Efficient Routing Algorithm for Patient Monitoring in Body Sensor Networks. In Proceedings of the IEEE 13th International Conference on Wearable and Implantable Body Sensor Networks, San Francisco, CA, USA, 14–17 June 2016; pp. 141–146. [Google Scholar]
- Nidhya, R.; Karthik, S.; Smilarubavathy, G. An End-to-End Secure and Energy-Aware Routing Mechanism for IoT-Based Modern Health Care System. In Soft Computing and Signal Processing; Springer: Singapore, 2019; pp. 379–388. [Google Scholar]
- Su, H.; Wang, Z.; An, S. MAEB: Routing Protocol for IoT Healthcare. Adv. Internet Things 2013, 3, 8–15. [Google Scholar] [CrossRef]
- Zargar, S.T.; Joshi, J.; Tipper, D. A Survey of Defense Mechanisms Against Distributed Denial of Service (DDoS) Flooding Attacks. IEEE Commun. Surv. Tutorials 2013, 15, 2046–2069. [Google Scholar] [CrossRef] [Green Version]
- Kalkan, K.; Gür, G.; Alagöz, F. Filtering-Based Defense Mechanisms Against DDoS Attacks: A Survey. IEEE Syst. J. 2016, 11, 2761–2773. [Google Scholar] [CrossRef]
- Yu, S.; Zhou, W.; Guo, S.; Guo, M. A Feasible IP Traceback Framework through Dynamic Deterministic Packet Marking. IEEE Trans. Comput. 2015, 65, 1418–1427. [Google Scholar] [CrossRef]
- Bhuyan, M.H.; Bhattacharyya, D.K.; Kalita, J.K. E-LDAT: A lightweight system for DDoS flooding attack detection and IP traceback using extended entropy metric. Secur. Commun. Netw. 2016, 9, 3251–3270. [Google Scholar] [CrossRef] [Green Version]
- Kalkan, K.; Alagöz, F. A distributed filtering mechanism against DDoS attacks: ScoreForCore. Comput. Netw. 2016, 108, 199–209. [Google Scholar] [CrossRef]
- Nooribakhsh, M.; Mollamotalebi, M. A review on statistical approaches for anomaly detection in DDoS attacks. Inf. Secur. J. Glob. Perspect. 2020, 29, 118–133. [Google Scholar] [CrossRef]
- Jian-Qi, Z.; Feng, F.; Ke-Xin, Y.; Yan-Heng, L. Dynamic entropy based DoS attack detection method. Comput. Electr. Eng. 2013, 39, 2243–2251. [Google Scholar] [CrossRef]
- Doshi, R.; Apthorpe, N.; Feamster, N. Machine Learning DDoS Detection for Consumer Internet of Things Devices. In Proceedings of the IEEE Security and Privacy Workshops, San Francisco, CA, USA, 24 May 2018; pp. 29–35. [Google Scholar]
- Idhammad, M.; Afdel, K.; Belouch, M. Semi-supervised machine learning approach for DDoS detection. Appl. Intell. 2018, 48, 3193–3208. [Google Scholar] [CrossRef]
- Yuan, X.; Li, C.; Li, X. DeepDefense: Identifying DDoS Attack via Deep Learning. In Proceedings of the IEEE International Conference on Smart Computing, Hong Kong, China, 29–31 May 2017; pp. 1–8. [Google Scholar]
- Wu, G.; Wang, J.; Zhang, Y.; Jiang, S. A Continuous Identity Authentication Scheme Based on Physiological and Behavioral Characteristics. Sensors 2018, 18, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enamamu, T.S.; Clarke, N.; Haskell-Dowland, P.; Li, F. Smart Watch based Body-Temperature Authentication. In Proceedings of the International Conference on Computing Networking and Informatics, Lagos, Nigeria, 29–31 October 2017; pp. 1–7. [Google Scholar]
- Rostami, M.; Juels, A.; Koushanfar, F. Heart-to-Heart (H2H): Authentication for Implanted Medical Devices. In Proceedings of the ACM SIGSAC Conference on Computer & Communications Security, Berlin, Germany, 4–8 November 2013; pp. 1099–1112. [Google Scholar]
- Kim, Y.; Lee, W.S.; Raghunathan, V.; Jha, N.K.; Raghunathan, A. Vibration-based Secure Side Channel for Medical Devices. In Proceedings of the 52nd ACM/EDAC/IEEE Design Automation Conference, San Francisco, CA, USA, 8–12 June 2015; pp. 1–6. [Google Scholar]
- Das, A.K.; Wazid, M.; Kumar, N.; Khan, M.K.; Choo, K.K.R.; Park, Y. Design of Secure and Lightweight Authentication Protocol for Wearable Devices Environment. IEEE J. Biomed. Health Inform. 2017, 22, 1310–1322. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.; Grover, H.S. A secure authentication protocol for wearable devices environment using ECC. J. Inf. Secur. Appl. 2019, 47, 8–15. [Google Scholar] [CrossRef]
- Bilal, M.; Kang, S.G. An Authentication Protocol for Future Sensor Networks. Sensors 2017, 17, 979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Zhang, Y.; Ling, J.; Liu, Z. Secure and fine-grained access control on e-healthcare records in mobile cloud computing. Future Gener. Comput. Syst. 2018, 78, 1020–1026. [Google Scholar] [CrossRef]
- De Carvalho, M.A., Jr.; Bandiera-Paiva, P. Health Information System Role-Based Access Control Current Security Trends and Challenges. J. Healthc. Eng. 2018, 2018, 6510249. [Google Scholar] [CrossRef] [PubMed]
- Goyal, V.; Pandey, O.; Sahai, A.; Waters, B. Attribute-Based Encryption for Fine-Grained Access Control of Encrypted Data. In Proceedings of the 13th ACM Conference on Computer and Communications Security, Alexandria, VA, USA, 30 October–3 November 2006; pp. 89–98. [Google Scholar]
- Ouaddah, A.; Elkalam, A.A.; Ouahman, A.A. Towards a Novel Privacy-Preserving Access Control Model Based on Blockchain Technology in IoT. In Europe and MENA Cooperation Advances in Information and Communication Technologies; Springer: Cham, Switzerland, 2017; pp. 523–533. [Google Scholar]
- Zarpelão, B.B.; Miani, R.S.; Kawakani, C.T.; de Alvarenga, S.C. A survey of intrusion detection in Internet of Things. J. Netw. Comput. Appl. 2017, 84, 25–37. [Google Scholar] [CrossRef]
- Ioannou, C.; Vassiliou, V.; Sergiou, C. An Intrusion Detection System for Wireless Sensor Networks. In Proceedings of the 24th International Conference on Telecommunications, Montreal, QC, Canada, 24–22 August 2005; pp. 1–5. [Google Scholar]
- Ioulianou, P.; Vasilakis, V.; Moscholios, I.; Logothetis, M. A Signature-based Intrusion Detection Systemfor the Internet of Things. In Proceedings of the Information and Communication Technology Form, Graz, Austria, 11–13 July 2018; pp. 1–5. [Google Scholar]
- Bostani, H.; Sheikhan, M. Hybrid of anomaly-based and specification-based IDS for Internet of Things using unsupervised OPF based on MapReduce approach. Comput. Commun. 2017, 98, 52–71. [Google Scholar] [CrossRef]
- Karie, N.M.; Kebande, V.R.; Venter, H.S.; Choo, K.K.R. On the importance of standardising the process of generating digital forensic reports. Forensic Sci. Int. Rep. 2019, 1, 100008. [Google Scholar] [CrossRef]
- ISO Central Secretary. Information Technology—Security Techniques—Guidelines for Identification, Collection, Acquisition and Preservation of Digital Evidence; Technical Report ISO/IEC Standard 27037; International Organization for Standardization: Vernier/Geneva, Switzerland, 2012. [Google Scholar]
- ISO Central Secretary. Information Technology—Security Techniques—Guidance on Assuring Suitability and Adequacy of Incident Investigative Method; Technical Report ISO/IEC Standard 27041; International Organization for Standardization: Vernier/Geneva, Switzerland, 2015. [Google Scholar]
- ISO Central Secretary. Information Technology—Security Techniques—Guidelines for the Analysis and Interpretation of Digital Evidence; Report ISO/IEC Standard 27042; International Organization for Standardization: Vernier/Geneva, Switzerland, 2015. [Google Scholar]
- ISO Central Secretary. Information Technology—Security Techniques—Incident Investigation Principles and Processes; Technical Report ISO/IEC Standard 27043; International Organization for Standardization: Vernier/Geneva, Switzerland, 2015. [Google Scholar]
- López-Aguilar, P.; Solanas, A. An Effective Approach to the Cross-Border Exchange of Digital Evidence Using Blockchain. In Proceedings of the 9th International Conference on Applications in Electronics Pervading Industry, Environment and Society, Pisa, Italy, 21–22 September 2021; pp. 1–5. [Google Scholar]
- European Union. Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data, and repealing Directive 95/46/EC (General Data Protection Regulation). Off. J. Eur. Union 2016, L119, 1–88. [Google Scholar]
- Annas, G.J. HIPAA Regulations—A New Era of Medical-Record Privacy? N. Engl. J. Med. 2003, 348, 1486–1490. [Google Scholar] [CrossRef] [Green Version]
- Muchagata, J.; Ferreira, A. Translating GDPR into the mHealth Practice. In Proceedings of the International Carnahan Conference on Security Technology, Montreal, QC, Canada, 22–25 October 2018; pp. 1–5. [Google Scholar]
- Bolognini, L.; Bistolfi, C. Pseudonymization and impacts of Big (personal/anonymous) Data processing in the transition from the Directive 95/46/EC to the new EU General Data Protection Regulation. Comput. Law Secur. Rev. 2017, 33, 171–181. [Google Scholar] [CrossRef]
- Domingo-Ferrer, J.; Mateo-Sanz, J.M. Practical Data-Oriented Microaggregation for Statistical Disclosure Control. IEEE Trans. Knowl. Data Eng. 2002, 14, 189–201. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, L. K-anonymity: A model for protecting privacy. Int. J. Uncertain. Fuzziness-Knowl.-Based Syst. 2002, 10, 557–570. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.; Song, Z.; Song, H.; Zhou, Y.; Wang, Y.; Wu, G. Differential Privacy Preserving in Big Data Analytics for Connected Health. J. Med. Syst. 2016, 40, 97. [Google Scholar] [CrossRef] [PubMed]
- López-Aguilar, P.; Solanas, A. Human Susceptibility to Phishing Attacks Based on Personality Traits: The Role of Neuroticism. In Proceedings of the IEEE 45th Annual Computers, Software, and Applications Conference, Madrid, Spain, 12–16 July 2021; pp. 1363–1368. [Google Scholar]
- Abramson, A.; Caffarel-Salvador, E.; Soares, V.; Minahan, D.; Tian, R.Y.; Lu, X.; Dellal, D.; Gao, Y.; Kim, S.; Wainer, J.; et al. A luminal unfolding microneedle injector for oral delivery of macromolecules. Nat. Med. 2019, 25, 1512–1518. [Google Scholar] [CrossRef]
- Flores, A.M.; Hosseini-Nassab, N.; Jarr, K.U.; Ye, J.; Zhu, X.; Wirka, R.; Koh, A.L.; Tsantilas, P.; Wang, Y.; Nanda, V.; et al. Pro-efferocytic nanoparticles are specifically taken up by lesional macrophages and prevent atherosclerosis. Nat. Nanotechnol. 2020, 15, 154–161. [Google Scholar] [CrossRef]
- Zamani, R.; Aval, S.F.; Pilehvar-Soltanahmadi, Y.; Nejati-Koshki, K.; Zarghami, N. Recent Advances in Cell Electrospining of Natural and Synthetic Nanofibers for Regenerative Medicine. Drug Res. 2018, 68, 425–435. [Google Scholar] [CrossRef]
- Vahedifard, F.; Chakravarthy, K. Nanomedicine for COVID-19: The role of nanotechnology in the treatment and diagnosis of COVID-19. Emerg. Mater. 2021, 4, 75–99. [Google Scholar] [CrossRef]
- Miraz, M.H.; Ali, M.; Excell, P.S.; Picking, R. Internet of Nano-Things, Things and Everything: Future Growth Trends. Future Internet 2018, 10, 68. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Iturri, P.; Aguirre, E.; Trigo, J.D.; Astrain, J.J.; Azpilicueta, L.; Serrano, L.; Villadangos, J.; Falcone, F. Implementation and Operational Analysis of an Interactive Intensive Care Unit within a Smart Health Context. Sensors 2018, 18, 389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguirre, E.; Lopez-Iturri, P.; Azpilicueta, L.; Rivarés, C.; Astrain, J.J.; Villadangos, J.; Falcone, F. Design and performance analysis of wireless body area networks in complex indoor e-Health hospital environments for patient remote monitoring. Int. J. Distrib. Sens. Netw. 2016, 12, 1550147716668063. [Google Scholar] [CrossRef]
- Yu, F.R.; Zhang, X.; Leung, V.C.M. Green Communications and Networking; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar]
- Ali, Z.; Henna, S.; Akhunzada, A.; Raza, M.; Kim, S.W. Performance Evaluation of LoRaWAN for Green Internet of Things. IEEE Access 2019, 7, 164102–164112. [Google Scholar] [CrossRef]
- Gandotra, P.; Jha, R.K.; Jain, S. Green Communication in Next Generation Cellular Networks: A Survey. IEEE Access 2017, 5, 11727–11758. [Google Scholar] [CrossRef]
- Huang, T.; Yang, W.; Wu, J.; Ma, J.; Zhang, X.; Zhang, D. A Survey on Green 6G Network: Architecture and Technologies. IEEE Access 2019, 7, 175758–175768. [Google Scholar] [CrossRef]
- Rose, S.; Borchert, O.; Mitchell, S.; Connelly, S. Zero Trust Architecture; Technical Report Special Publication 800-207; National Institute of Standards and Technology: Gaithersburg, MD, USA, 2020.
- Bertino, E. Zero Trust Architecture: Does It Help? IEEE Secur. Priv. 2021, 19, 95–96. [Google Scholar] [CrossRef]
- Dasaklis, T.K.; Casino, F.; Patsakis, C. Blockchain Meets Smart Health: Towards Next Generation Healthcare Services. In Proceedings of the 9th International Conference on Information, Intelligence, Systems and Applications, Zakynthos, Greece, 23–25 July 2018; pp. 1–8. [Google Scholar]
- Kroll, J.A.; Michael, J.B.; Thaw, D.B. Enhancing Cybersecurity via Artificial Intelligence: Risks, Rewards, and Frameworks. Computer 2021, 54, 64–71. [Google Scholar] [CrossRef]
- Taddeo, M.; McCutcheon, T.; Floridi, L. Trusting artificial intelligence in cybersecurity is a double-edged sword. Nat. Mach. Intell. 2019, 1, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Truong, T.C.; Zelinka, I.; Plucar, J.; Čandík, M.; Šulc, V. Artificial Intelligence and Cybersecurity: Past, Presence, and Future. In Artificial Intelligence and Evolutionary Computations in Engineering Systems; Springer: Singapore, 2020; pp. 351–363. [Google Scholar]
- Choi, I.S.; Hong, J.; Kim, T.W. Multi-Agent Based Cyber Attack Detection and Mitigation for Distribution Automation System. IEEE Access 2020, 8, 183495–183504. [Google Scholar] [CrossRef]
- Zeadally, S.; Adi, E.; Baig, Z.; Khan, I.A. Harnessing Artificial Intelligence Capabilities to Improve Cybersecurity. IEEE Access 2020, 8, 23817–23837. [Google Scholar] [CrossRef]
- Gerke, S.; Minssen, T.; Cohen, G. Ethical and legal challenges of artificial intelligence-driven healthcare. In Artificial Intelligence in Healthcare; Elsevier: Amsterdam, The Netherlands, 2020; pp. 295–336. [Google Scholar]
- Siemens, G. Connectivism: A Learning Theory for the Digital Age. Int. J. Instr. Technol. Distance Learn. 2005, 2, 3–10. [Google Scholar]
- Mostashari, A.; Arnold, F.; Mansouri, M.; Finger, M. Cognitive cities and intelligent urban governance. Netw. Ind. Q. 2011, 13, 4–7. [Google Scholar]
- Machin, J.; Batista, E.; Martínez-Ballesté, A.; Solanas, A. Privacy and Security in Cognitive Cities: A Systematic Review. Appl. Sci. 2021, 11, 4471. [Google Scholar] [CrossRef]







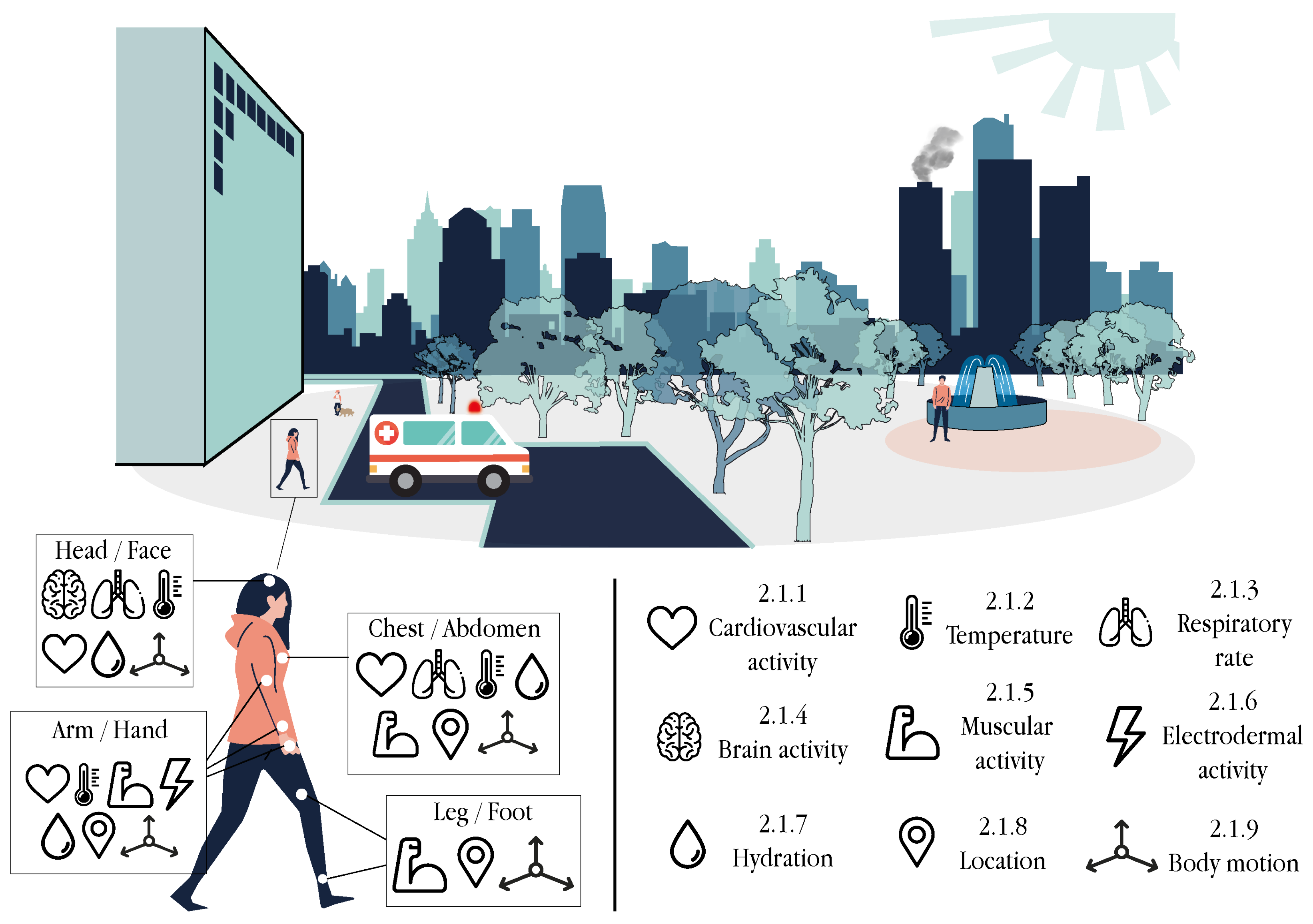{kind=link}
{kind=link}
{kind=link}
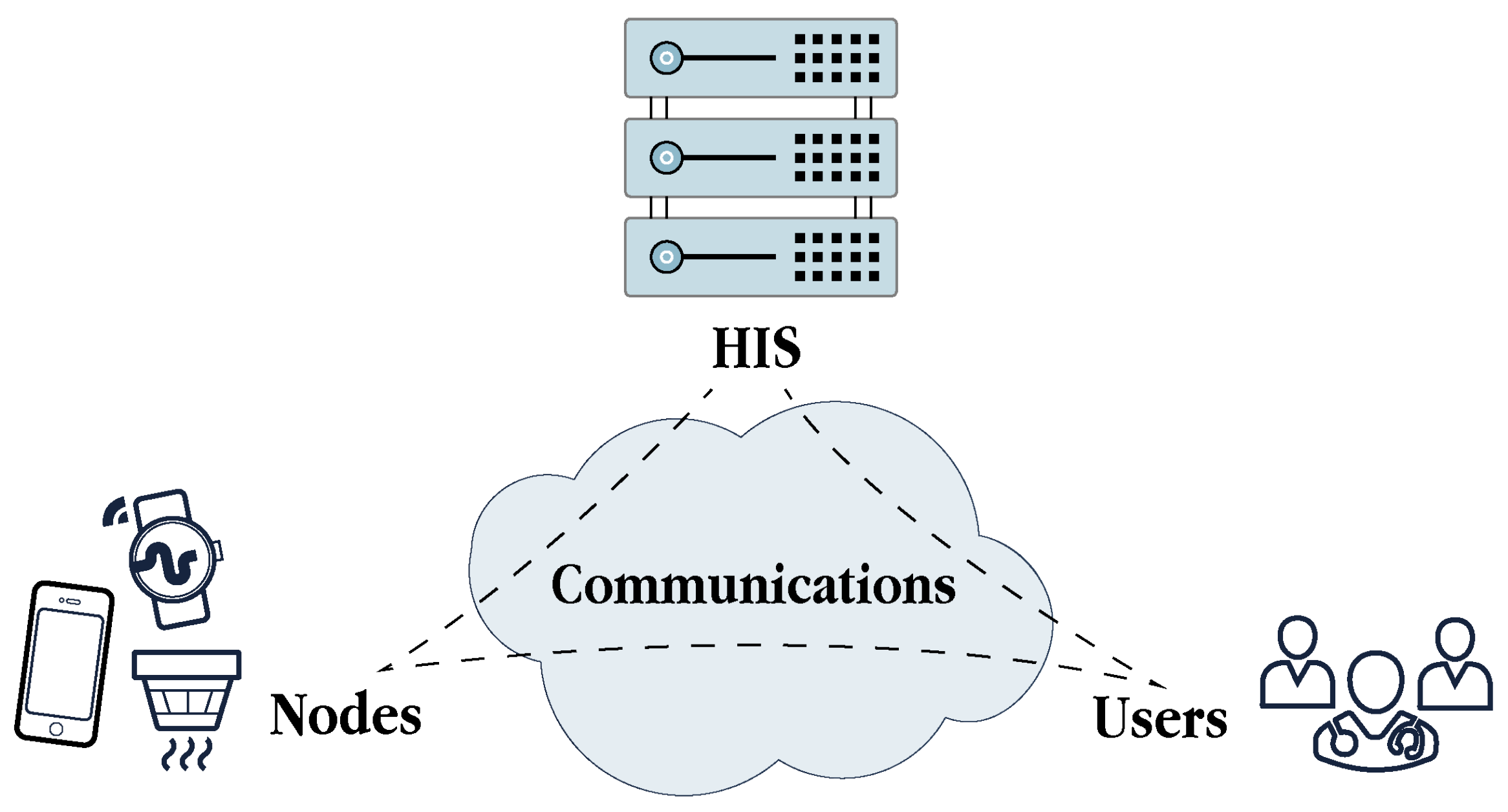{kind=link}
{kind=link}
{kind=link}
| User-Centric | Contextual | ||
|---|---|---|---|
| Heart rate | Blood oxygen | Air temperature | Air humidity |
| Blood pressure | Blood glucose | Barometric pressure | Air pollution |
| Body temperature | Skin temperature | Water contamination | Acoustic contamination |
| Respiratory rate | Brain activity | Electromagnetic radiation | Seismic activity |
| Muscular activity | Electrodermal activity | ||
| Hydration | Location | ||
| Body motion | |||
| Attribute | Method | Sensor | Device/ Wearable | Location | Properties | Suitable for Smart Health |
|---|---|---|---|---|---|---|
| Heart rate | Traditional ECG | Skin electrodes | Holter monitor | Chest | ✓ Accuracy ~ Cost ~ Cont. monit. ✕ Non invasive | ✕ |
| Heart rate | Wireless ECG | Skin electrodes | Patch Band Textile | Chest Arm | ✓ Accuracy ~ Cost ✓ Cont. monit. ~ Non-invasive | ✓ |
| Heart rate | PPG | Pulse oximeter | Smartwatch Wristband Ring | Wrist Finger | ~ Accuracy ✓ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Heart rate | BCG | Tilt Force Pressure | Patch | Chest | ✕Accuracy ~ Cost ~ Cont. monit. ✓ Non-invasive | ~ |
| Heart rate | PCG | Sound | Microphone Smartphone Electronic stethoscope | Chest | ✕ Accuracy ✓ Cost ~ Cont. monit. ✓ Non-invasive | ~ |
| Blood oxygen | ABG | Chemical | Chemical analyser | Arm Wirst | ✓ Accuracy ✕ Cost ✕ Cont. monit. ✕ Non-invasive | ✕ |
| Blood oxygen | PPG | Pulse oximeter | Smartwatch Strap Band Textile | Wrist Earlobe Finger | ~ Accuracy ✓ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Blood pressure | Traditional | Pressure | Sphygmomanometer | Arm | ✓ Accuracy ✓ Cost ✕ Cont. monit. ✕ Non-invasive | ✕ |
| Blood pressure | PTT (ECG and PPG) | Pulse oximeter Electrodes | Smartwatch Band Patch | Wrist Arm Ear Chest | ✓ Accuracy ~ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Blood glucose | Traditional (chemical) | Electrochemical | Glucose meter | Finger | ✓ Accuracy ✓ Cost ✕ Cont. monit. ✕ Non-invasive | ✕ |
| Blood glucose | Epidermal chemical | Electrochemical | Wristband Patch Tattoo | Wrist Arm | ~ Accuracy ~ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Blood glucose | Optical spectroscopy | Photo-sensor Infrared | Wristband Patch | Wrist Finger Earlobe | ~ Accuracy ~ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Attribute | Method | Sensor | Device/ Wearable | Location | Properties | Suitable for Smart Health |
|---|---|---|---|---|---|---|
| Body temperature | Traditional (chemical) | Mercury | Mercury-in- glass thermometer | Oral Rectal | ✓ Accuracy ✓ Cost ✕ Cont. monit. ✕ Non-invasive | ✕ |
| Skin temperature | Electrical | Thermistor | Patch Band | Arm Chest Ear Forehead | ~ Accuracy ✓ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Skin temperature | Electrical | Thermocouple | Patch Band | Arm Chest Ear Forehead | ✕ Accuracy ✓ Cost ✓ Cont. monit. ✓ Non-invasive | ~ |
| Skin temperature | Optical | FBG Infrared | Smartwatch Band Patch Textile | Wrist Chest Ear Forehead | ~ Accuracy ✓ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Attribute | Method | Sensor | Device/ Wearable | Location | Properties | Suitable for Smart Health |
|---|---|---|---|---|---|---|
| Respiratory rate | Traditional (observation of chest or abdomen) | - | - | - | ✓ Accuracy ✓ Cost ✕ Cont. monit. ✓ Non-invasive | ✕ |
| Respiratory rate | Chest wall strain | Resistive Capacitive Inductive | Patch Belt Textile | Chest | ✓ Accuracy ✓ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Respiratory rate | Electrical impedance | Impedance | Patch Belt Textile | Chest | ✓ Accuracy ✓ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Respiratory rate | Motion (contact) | IMU | Patch Belt Textile | Chest Abdomen | ✓ Accuracy ✓ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Respiratory rate | Acoustic | Microphone | Microphone Headset | Nose Mouth Chest | ✕ Accuracy ✓ Cost ✓ Cont. monit. ~ Non-invasive | ~ |
| Respiratory rate | Air temp. (electrical) | Thermistor Thermocouple Pyroelectric | Headset Patch | Nose Mouth | ~ Accuracy ✓ Cost ✓ Cont. monit. ~ Non-invasive | ~ |
| Respiratory rate | Air humid. (electrical) | Capacitive Resistive Nanocrystal | Headset Patch | Nose Mouth | ~ Accuracy ✓ Cost ✓ Cont. monit. ~ Non-invasive | ~ |
| Respiratory rate | Cardiac act. modulation | Pulse oximeter Electrodes | Smartwatch Band Patch | Wrist Chest | ✓ Accuracy ~ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Respiratory rate | Motion (contactless) | Camera | RGB camera Smartphone | - | ~ Accuracy ✓ Cost ✕ Cont. monit. ✓ Non-invasive | ~ |
| Respiratory rate | Thermal imaging | Camera | Infrared camera | - | ~ Accuracy ✕ Cost ✕ Cont. monit. ✓ Non-invasive | ~ |
| Respiratory rate | Ultrasonic | Ultrasonic prox. Capacitive | Recording device | - | ~ Accuracy ✕ Cost ✕ Cont. monit. ✓ Non-invasive | ~ |
| Attribute | Method | Sensor | Device/ Wearable | Location | Properties | Suitable for Smart Health |
|---|---|---|---|---|---|---|
| Brain activity | Traditional EEG | Skin electrodes | Head cap | Scalp | ✓ Accuracy ✕ Cost ✕ Cont. monit. ✕ Non-invasive | ✕ |
| Brain activity | Wireless EEG | Skin electrodes | Headband Headset Tattoo | Scalp Head Forehead Ear | ~ Accuracy ~ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Brain activity | fNIRS | Optodes | Head cap | Scalp Head | ✓ Accuracy ~ Cost ~ Cont. monit. ~ Non-invasive | ✕ |
| Brain activity | MEG | Optically pumped magnetometeres | Head cap | Scalp Head | ✓ Accuracy ✕ Cost ~ Cont. monit. ~ Non-invasive | ✕ |
| Brain activity | PET | Photosensor Photodiode | Head cap Helmet | Head | ✓ Accuracy ✕ Cost ✕ Cont. monit. ✕ Non-invasive | ✕ |
| Muscular activity | Intramuscular EMG | Monopolar or concentric electrodes | Needle and recording device | Region of interest | ✓ Accuracy ✕ Cost ✕ Cont. monit. ✕ Non-invasive | ✕ |
| Muscular activity | Surface EMG | Skin electrodes | Patch Band Cap Textile | Region of interest | ~ Accuracy ✓ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Muscular activity | MMG | Accelerometer Pressure Force-sensitive | Patch Band | Region of interest | ~ Accuracy ✓ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Attribute | Method | Sensor | Device/ Wearable | Location | Properties | Suitable for Smart Health |
|---|---|---|---|---|---|---|
| Electrodermal activity | Electrical | Skin electrodes (wired) | Smartwatch Band Strap | Wrist Finger | ✓ Accuracy ✓ Cost ✓ Cont. monit. ~ Non-Invasive | ∼ |
| Electrodermal activity | Electrical | Skin electrodes (wireless) | Smartwatch Band Strap | Wrist Finger | ✓ Accuracy ✓ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Hydration | Traditional (observation of eyes or lips) | - | - | - | ✓ Accuracy ✓ Cost ✕ Cont. monit. ✓ Non-invasive | ✕ |
| Hydration | Optical spectroscopy | Infrared | Band Patch Textile | Wrist Arm Head | ✓ Accuracy ~ Cost ~ Cont. monit. ✓ Non-invasive | ✓ |
| Hydration | Electromagnetic | Impedance Capacitive | Band Patch Textile | Wrist | ~ Accuracy ✓ Cost ~ Cont. monit. ✓ Non-invasive | ✓ |
| Hydration | Epidermal chemical | Electrochemical | Band Patch Tattoo Textile | Wrist Arm | ✓ Accuracy ~ Cost ~ Cont. monit. ✓ Non-invasive | ✓ |
| Attribute | Method | Sensor | Device/ Wearable | Location | Properties | Suitable for Smart Health |
|---|---|---|---|---|---|---|
| Location | Satellite (outdoor) | GPS GLONASS Galileo | Smartphone Smartwatch Band | Any | ✓ Accuracy ✓ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Location | Proximity (indoor) | BLE beacon WPS RFID UWB | IoT Access point Tag | - | ✓ Accuracy ✓ Cost ~ Cont. monit. ✓ Non-invasive | ✓ |
| Body motion | Optical motion capture | Camera | Camera Marker | Markers distributed in the body | ✓ Accuracy ✕ Cost ✕ Cont. monit. ✕ Non-invasive | ✕ |
| Body motion | Optical | Camera | RGB-depth camera | - | ~ Accuracy ~ Cost ~ Cont. monit. ✓ Non-invasive | ~ |
| Body motion | Kinematic | IMU | Band Patch Textile | Region of interest | ~ Accuracy ✓ Cost ✓ Cont. monit. ✓ Non-invasive | ✓ |
| Attribute | Method | Sensor/Device | Properties | Suitable for Smart Health |
|---|---|---|---|---|
| Air temperature | Electrical | Thermocouple | ✕ Accuracy ✓ Cost ✓ Response time ✗ Energy consumption | ~ |
| Air temperature | Electrical | Resistance temperature detector | ✓ Accuracy ~ Cost ✕ Response time ✓ Energy consumption | ~ |
| Air temperature | Electrical | Thermistor | ✓ Accuracy ~ Cost ✓ Response time ✓ Energy consumption | ✓ |
| Air temperature | Electrical | Semiconductor integrated circuit | ~ Accuracy ✓ Cost ✓ Response time ✓ Energy consumption | ✓ |
| Air humidity | Electrical | Capacitive | ✓ Accuracy ✕ Cost ✓ Response time ✓ Energy consumption | ~ |
| Air humidity | Electrical | Resistive | ~Accuracy ✓ Cost ~ Response time ✓ Energy consumption | ✓ |
| Air humidity | Optical | Fibre-optic | ✓ Accuracy ✕ Cost ~ Response time ✓ Energy consumption | ~ |
| Barometric pressure | MEMS | Piezoresistive pressure | ✓ Accuracy ✓ Cost ✓ Response time ✓ Energy consumption | ✓ |
| Attribute | Method | Sensor/Device | Properties | Suitable for Smart Health |
|---|---|---|---|---|
| Air pollution | Optical spectroscopy | Infrared Fluorescence | ✓ Accuracy ✕ Cost ✕ Response time ~ Energy consumption | ✕ |
| Air pollution | Chemiresistive | MOS | ~ Accuracy ✓ Cost ✓ Response time ~ Energy consumption | ✓ |
| Air pollution | Electrochemical | Electrochemical | ✓ Accuracy ✕ Cost ✓ Response time ✓ Energy consumption> | ~ |
| Water contamination | Traditional (chemical) | In-lab instrumentation | ✓ Accuracy ✕ Cost ✕ Response time ✕ Energy consumption | ✕ |
| Water contamination | Electrochemical | Resistive Capacitive Conductance | ~ Accuracy ~ Cost ✓ Response time ✓ Energy consumption | ✓ |
| Water contamination | Optical | CMOS camera | ~ Accuracy ✓ Cost ✓ Response time ✓ Energy consumption | ✓ |
| Acoustic contamination | Acoustic | Microphone | ✓ Accuracy ✓ Cost ✓ Response time ✓ Energy consumption | ✓ |
| Attribute | Method | Sensor/Device | Properties | Suitable for Smart Health |
|---|---|---|---|---|
| Electromagnetic radiation | Electrical | Geiger–Müller tubes | ✓ Accuracy ✕ Cost ~ Response time ~ Energy consumption | ~ |
| Electromagnetic radiation | Optical | Fibre-optic | ✓ Accuracy ~ Cost ✓ Response time ~ Energy consumption | ✓ |
| Seismic activity | Traditional (motion) | Seismometer | ✓ Accuracy ✕ Cost ~ Response time ~ Energy consumption | ✕ |
| Seismic activity | Kinematic | Accelerometer | ~ Accuracy ✓ Cost ~ Response time ✓ Energy consumption | ✓ |
| Seismic activity | Optical | Opto-mechanical | ~ Accuracy ~ Cost ~ Response time ✓ Energy consumption | ✓ |
| Bluetooth | BLE | ZigBee | IEEE 802.15.6 | Wi-Fi | |
|---|---|---|---|---|---|
| Frequency bands | 2.4 GHz | 2.4 GHz | 868/915 MHz 2.4 GHz | 14–29 MHz (HBC) 400–2400 MHz (NB) 3.2–10.3 GHz (UWB) | 2.4/5 GHz |
| Radio coverage | Short/medium | Medium | Short/medium | Short | Medium |
| 10–100 m | 400 m | 10–100 m | 2 m | 50–100 m | |
| Data rate | Moderate | Moderate | Low | Low/moderate | High |
| 1–3 Mbps | 1–2 Mbps | 20–250 kbps | 10 kbps–15 Mbps | 400 Mbps–10 Gbps | |
| Latency | Moderate | Very low | Very low/Low | Low/moderate | Low |
| 100 ms | 10 ms | 10–30 ms | 125 ms | 50 ms | |
| Power | Moderate | Very low | Very low/low | Very low | High |
| 0.2–0.5 W | 10 mW | 1–60 mW | 0.1–3 mW | 0.8–1 W | |
| Size | 8 | 32,000 | 65,000 | 256 | 250 |
| Topology | Scatternet | Star, mesh | Star, tree, mesh | Star, multi-hop | Star, mesh, ad hoc |
| Security | 56,64,128-bit AES | 128-bit AES | 128-bit AES | Level 1/Level 2 | 128,256-bit AES |
| Cost | Medium | Low | Low | Low | High |
| WBAN tier | Tier 1/Tier 2 | Tier 1/Tier 2 | Tier 2 | Tier 1 | Tier 2/Tier 3 |
| Suitable for smart health | ~ | ✓ | ~ | ✓ | ✓ |
| 4G/LTE | 5G | LoRa | SigFox | NB-IoT | |
|---|---|---|---|---|---|
| Frequency bands | 0.7–2.6 GHz | 600–700 MHz 2.5–3.8 GHz 25–100 GHz | 863–928 MHz | 868/915 MHz | 800–900 MHz |
| Radio coverage | High | Medium/high | High | High | High |
| 10 km | 300 m–1 km | 5–20 km | 10–50 km | 15 km | |
| Data rate | High | Very high | Very low | Very low | Low |
| 10–300 Mbps | 1–20 Gbps | 37.5 kbps | 100–600 bps | 250 kbps | |
| Latency | Low | Very low | High | High | High |
| 50–70 ms | 1–10 ms | 3 s | 10 s | 1 s | |
| Power | Moderate | Low | Low | Low | Low |
| 250–700 mW | N/A | 25 mW | 10–100 mW | 20–200 mW | |
| Size | Thousands per km2 | 1 million per | 1000 | 1,000,000 | 50,000 |
| Topology | Cellular | Cellular | Star of stars | Star | Star |
| Security | 128-bit | 256-bit | 128-bit AES | Optional | 128,256-bit |
| Cost | Medium | High | Low | Low | Low |
| WBAN tier | Tier 2/Tier 3 | Tier 2/Tier 3 | Tier 2 | Tier 2 | Tier 2 |
| Suitable for smart health | ✓ | ✓ | ~ | ✕ | ~ |
| Attack | Target Actor | Nature | Origin | Launch Method | TCP/IP Layer | Requirements Threats |
|---|---|---|---|---|---|---|
| Node capture | Nodes | Active | External | Physical | Network interface | Confidentiality Non-repudiation Authentication Privacy |
| False data injection | Nodes | Active | Internal | Physical | Network interface | Integrity |
| Sleep deprivation | Nodes | Active | External | Physical Logical | Network interface | Availability |
| Side-channel | Nodes | Passive Active | External | Side-channel | Network interface | Confidentiality Availability |
| Firmware update | Nodes | Active | External | Logical | Network interface | Confidentiality Non-repudiation Authentication Authorisation |
| Eavesdropping | Communications | Passive | External | Logical | Network interface Network | Confidentiality Privacy |
| Data tampering | Communications | Active | Internal | Physical | Network interface | Integrity |
| Replay | Communications | Active | Internal | Physical | Network | Integrity Authentication Authorisation |
| Spoofing | Communications | Active | Internal External | Physical | Network interface Network Transport Application | Integrity |
| Man-in-the-middle | Communications | Active | Internal External | Logical | Network Transport | Confidentiality Integrity Authentication Privacy |
| Flooding | Communications | Active | Internal External | Logical | Network Transport Application | Availability |
| Jamming | Communications | Active | External | Physical | Network interface | Availability |
| Black hole | Communications | Active | Internal | Physical | Network | Availability |
| Malware | HIS Nodes | Active | External | Logical | Application | Confidentiality Integrity Availability Non-repudiation Authentication Authorisation Privacy |
| Data leakage | HIS | Passive | External | Logical | Application | Confidentiality Privacy |
| Phishing | Users | Active | External | Logical | Application | Confidentiality Authentication Authorisation Privacy |
| Type | Solution | Actor | TCP/IP Layer | Requirements Protected |
|---|---|---|---|---|
| Secure communications | Lightweight cryptography | Nodes Communications HIS | Network interface | Confidentiality Integrity Non-repudiation Authentication |
| Key management | Nodes HIS | Network interface | Confidentiality Authentication | |
| Always-on systems | Secure routing | Communications | Network | Availability |
| DDoS countermeasures | Nodes Communications HIS | Network | Availability | |
| Trust management | Authentication protocols | Nodes HIS | Transport Application | Authentication Confidentiality Privacy |
| Access control mechanisms | HIS | Application | Authentication Confidentiality Privacy | |
| Intrusion detection systems | Communications HIS | Network Transport Application | Confidentiality Integrity Availability Authentication Privacy | |
| Traceability of digital evidence | HIS | Application | Integrity | |
| Data protection | Privacy protection models | HIS | Application | Privacy |
| Awareness programmes | Users | - | Privacy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batista, E.; Moncusi, M.A.; López-Aguilar, P.; Martínez-Ballesté, A.; Solanas, A. Sensors for Context-Aware Smart Healthcare: A Security Perspective. Sensors 2021, 21, 6886. https://doi.org/10.3390/s21206886
Batista E, Moncusi MA, López-Aguilar P, Martínez-Ballesté A, Solanas A. Sensors for Context-Aware Smart Healthcare: A Security Perspective. Sensors. 2021; 21(20):6886. https://doi.org/10.3390/s21206886
Chicago/Turabian StyleBatista, Edgar, M. Angels Moncusi, Pablo López-Aguilar, Antoni Martínez-Ballesté, and Agusti Solanas. 2021. "Sensors for Context-Aware Smart Healthcare: A Security Perspective" Sensors 21, no. 20: 6886. https://doi.org/10.3390/s21206886
APA StyleBatista, E., Moncusi, M. A., López-Aguilar, P., Martínez-Ballesté, A., & Solanas, A. (2021). Sensors for Context-Aware Smart Healthcare: A Security Perspective. Sensors, 21(20), 6886. https://doi.org/10.3390/s21206886