
A Comparative Study on the Voxel Values in Alveolar Bones Acquired by MDCT and Newly Developed Dental Dual-Energy CBCT


Abstract
:1. Introduction
2. Materials and Methods
2.1. Development of Dental DE-CBCT
2.2. Conducted Clinical Trial
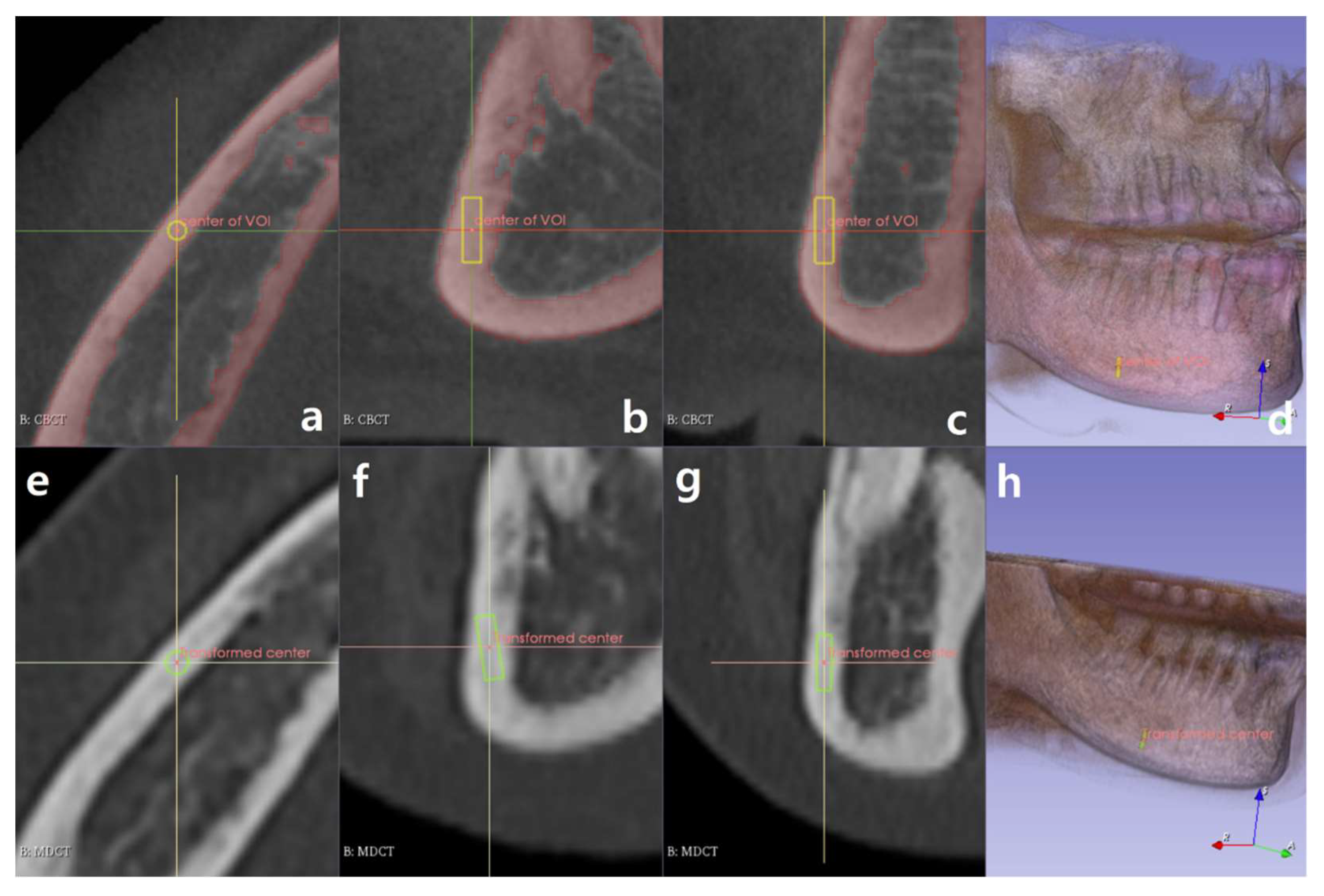
2.3. Software Development to Extract Information of the ROIs
2.4. Criteria for Selecting ROIs
2.5. Statistical Analysis
3. Results
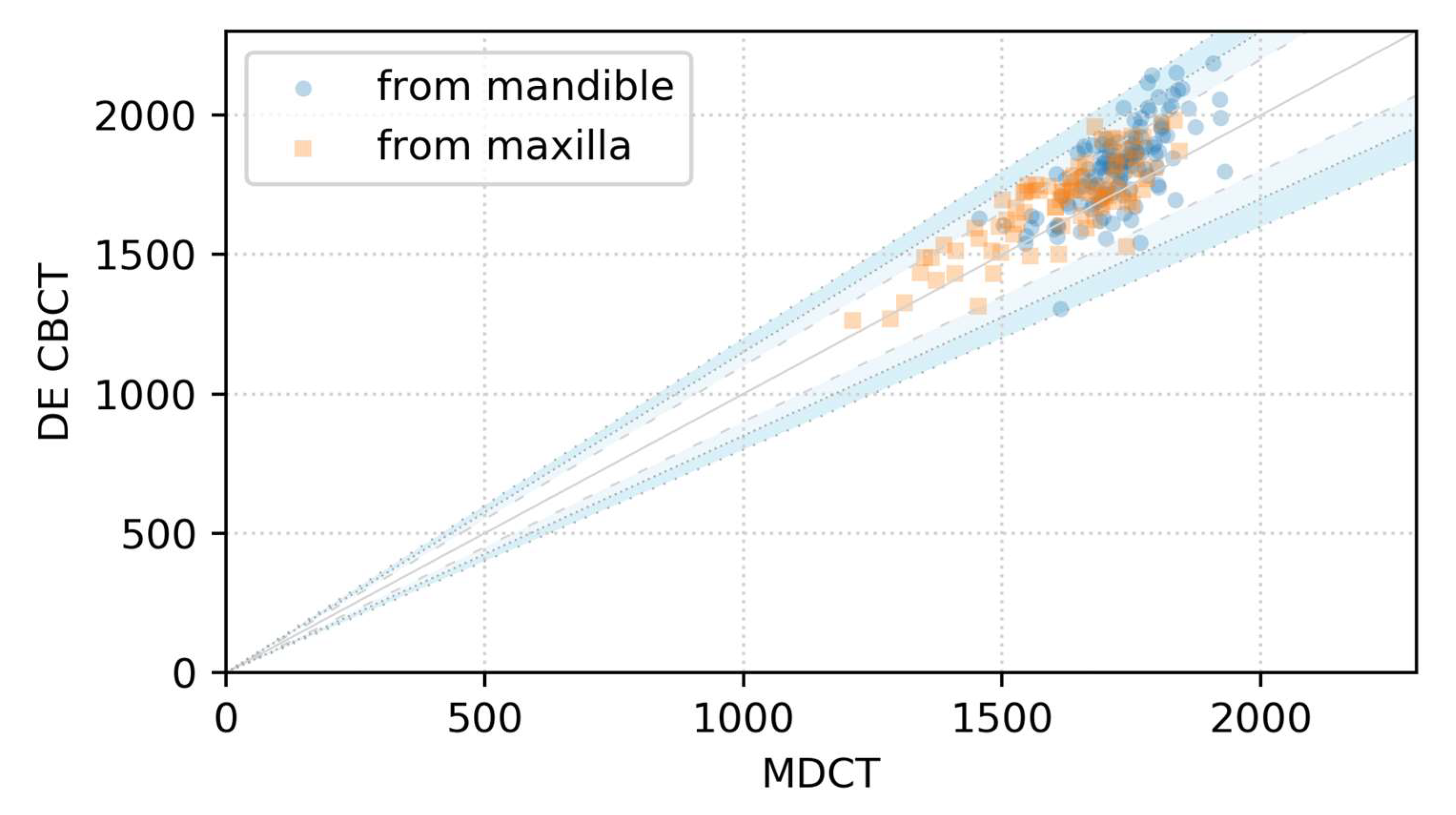
3.1. Scatter Plot over the Identity Line
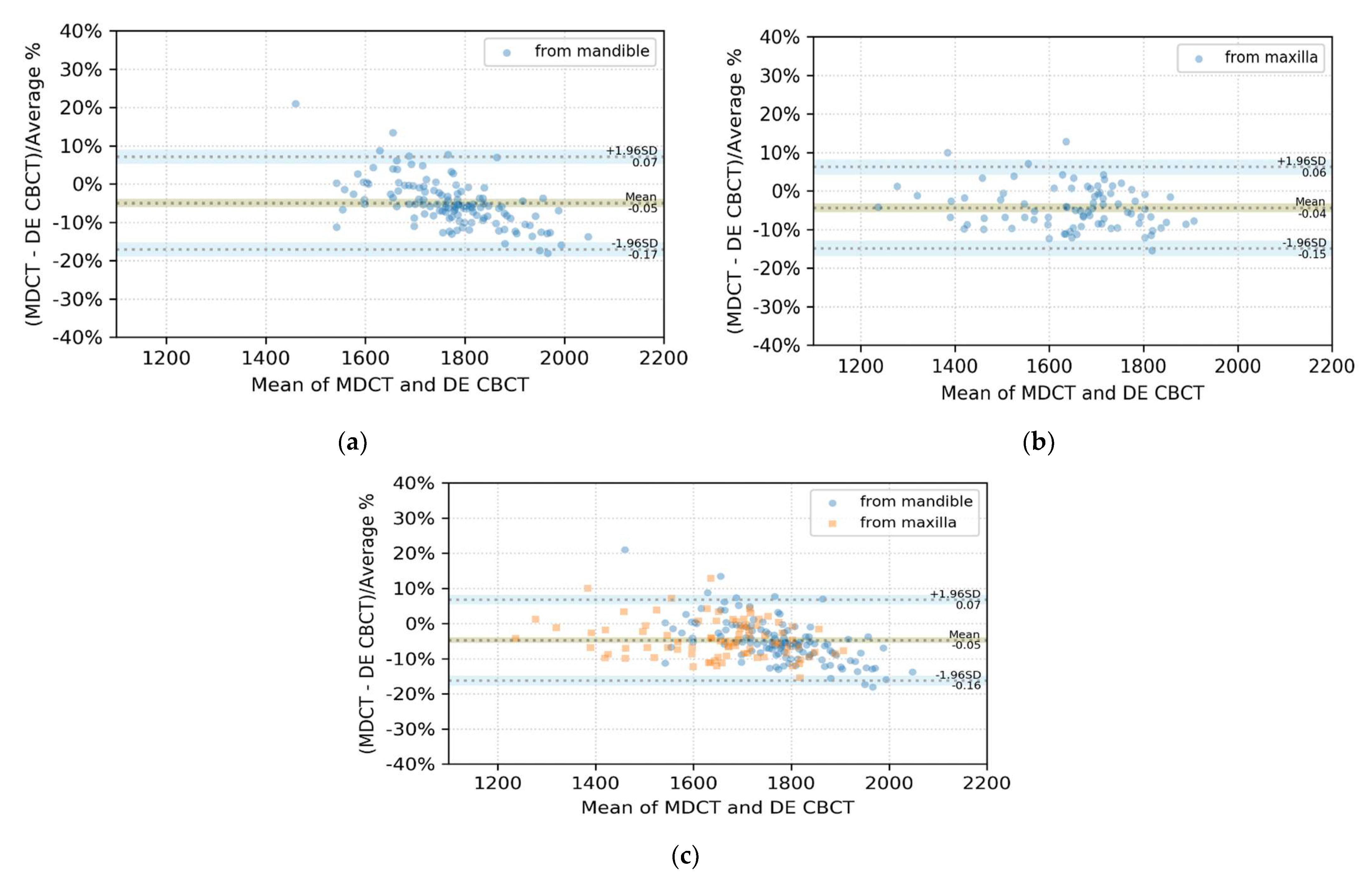
3.2. BA Plot Analysis
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ahmad, M.; Jenny, J.; Downie, M. Application of cone beam computed tomography in oral and maxillofacial surgery: CBCT in oral and maxillofacial surgery. Aust. Dent. J. 2012, 57, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Manikandan, D.; Fathima, S. Cbct in dentistry-an overview. Eur. J. Mol. Clin. Med. 2020, 7, 1403–1408. [Google Scholar]
- Vandenberghe, B. The crucial role of imaging in digital dentistry. Dent. Mater. 2020, 36, 581–591. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, I.; Berglundh, T. Effects of different implant surfaces and designs on marginal bone-level alterations: A review. Clin. Oral Implant. Res. 2009, 20, 207–215. [Google Scholar] [CrossRef]
- Li, J.; Yin, X.; Huang, L.; Mouraret, S.; Brunski, J.B.; Cordova, L.; Salmon, B.; Helms, J.A. Relationships among bone quality, implant osseointegration, and Wnt signaling. J. Dent. Res. 2017, 96, 822–831. [Google Scholar] [CrossRef]
- Ghoncheh, Z.; Kaviani, H.; Ghadiri Harvani, H.; Goodarzipour, D.; Shamshiri, A.R.; Shams, P. Assessment of the capability of bone density contrast dissociation in cone beam computed tomography compared to digital periapical radiography by using a phantom. J. Dent. 2019, 20, 203. [Google Scholar] [CrossRef]
- Li, G.; Qian, H.; Guo, S.; Wang, D.; Sun, C.; Du, Y.; Cheng, J.; Jiang, H. Assessment of aging characteristics of female condylar trabecular structure by cone-beam computed tomography. Oral Radiol. 2019, 35, 16–22. [Google Scholar] [CrossRef]
- Martelli, S.J.R.; Damian, M.F.; Schinestsck, A.R.; Schuch, L.F.; Cascaes, A.M.; Vasconcelos, A.C.U. Imaging and histomorphometric evaluation of mandible and tibia of rats treated with bisphosphonates. Oral Maxillofac. Surg. 2019, 23, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Bal, C.; Unsal, G.S.; Turkyilmaz, I. Comparative analysis of bone density measurements by using multislice spiral and cone-beam computed tomography. J. Dent. Sci. 2020, 15, 388–389. [Google Scholar] [CrossRef]
- Rai, S.; Misra, D.; Misra, A. Cone-beam computed tomography assessment of bone using grayscale values in patients with diabetes mellitus. A case-control observational study. J. Indian Soc. Periodontol. 2020, 24, 560–566. [Google Scholar] [CrossRef]
- Schnutenhaus, S.; Götz, W.; Dreyhaupt, J.; Rudolph, H.; Luthardt, R.G.; Edelmann, C. Associations among primary stability, histomorphometric findings, and bone density: A prospective randomized study after alveolar ridge preservation with a collagen cone. Dent. J. 2020, 8, 112. [Google Scholar] [CrossRef]
- Wang, S.-H.; Shen, Y.-W.; Fuh, L.-J.; Peng, S.-L.; Tsai, M.-T.; Huang, H.-L.; Hsu, J.-T. Relationship between cortical bone thickness and cancellous bone density at dental implant sites in the jawbone. Diagnostics 2020, 10, 710. [Google Scholar] [CrossRef] [PubMed]
- Chennoju, S.K.; Pachigolla, R.; Neelima, V.; Mrudula, B.; Swathi, M. Standardization of a cone beam computed tomography machine in evaluating bone density: A novel approach. Minerva Dent. Oral Sci. 2021, 70, 142–146. [Google Scholar] [CrossRef]
- Campos, M.J.D.S.; de Souza, T.S.; Mota Júnior, S.L.; Fraga, M.R.; Vitral, R.W.F. Bone mineral density in cone beam computed tomography: Only a few shades of gray. World J. Radiol. 2014, 6, 607. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, M.; Stefanelli, L.V.; Pacifici, A.; Pacifici, L.; Barbato, E. How accurate is CBCT in measuring bone density? A comparative CBCT-CT in vitro study: Bone density assessment. Clin. Implant Dent. Relat. Res. 2014, 16, 471–478. [Google Scholar] [CrossRef]
- Razi, T.; Niknami, M.; Alavi Ghazani, F.A. Relationship between Hounsfield unit in CT scan and gray scale in CBCT. J. Dent. Res. Dent. Clin. Dent. Prospects 2014, 8, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, R.; Jacobs, R.; Singer, S.R.; Mupparapu, M. CBCT-based bone quality assessment: Are hounsfield units applicable? Dento. Maxillo. Facial Rad. 2015, 44, 20140238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kivovics, M.; Szabó, B.T.; Németh, O.; Iványi, D.; Trimmel, B.; Szmirnova, I.; Orhan, K.; Mijiritsky, E.; Szabó, G.; Dobó-Nagy, C. Comparison between micro-computed tomography and cone-beam computed tomography in the assessment of bone quality and a long-term volumetric study of the augmented sinus grafted with an albumin impregnated allograft. JCM 2020, 9, 303. [Google Scholar] [CrossRef] [Green Version]
- Harms, J.; Lei, Y.; Wang, T.; Zhang, R.; Zhou, J.; Tang, X.; Curran, W.J.; Liu, T.; Yang, X. Paired cycle-GAN-based image correction for quantitative cone-beam computed tomography. Med. Phys. 2019, 46, 3998–4009. [Google Scholar] [CrossRef]
- Zhang, Y.; Yue, N.; Su, M.; Liu, B.; Ding, Y.; Zhou, Y.; Wang, H.; Kuang, Y.; Nie, K. Improving CBCT quality to CT level using deep learning with generative adversarial network. Med. Phys. 2021, 48, 2816–2826. [Google Scholar] [CrossRef]
- Yong, T.-H.; Yang, S.; Lee, S.-J.; Park, C.; Kim, J.-E.; Huh, K.-H.; Lee, S.-S.; Heo, M.-S.; Yi, W.-J. QCBCT-NET for direct measurement of bone mineral density from quantitative cone-beam CT: A human skull phantom study. Sci. Rep. 2021, 11, 15083. [Google Scholar] [CrossRef]
- Chang, S.; Lee, S.C. A phantom study of a dual-energy dental cone beam computed tomography prototype. In Proceedings of the 2019 IEEE Nuclear Science Symposium and Medical Imaging Conference (NSS/MIC), Manchester, UK, 26 October–2 November 2019; pp. 1–3. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, J.E.; Choo, J.; Min, J.; Chang, S.; Lee, S.C.; Pyun, W.B.; Seo, K.-S.; Karm, M.-H.; Koo, K.-T.; et al. A clinical pilot study of jawbone mineral density measured by the newly developed dual-energy cone-beam computed tomography method compared to calibrated multislice computed tomography. Imaging Sci. Dent. 2019, 49, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.M.; Sonka, M.; et al. 3D slicer as an image computing platform for the quantitative imaging network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marstal, K.; Berendsen, F.; Staring, M.; Klein, S. SimpleElastix: A user-friendly, multi-lingual library for medical image registration. In Proceedings of the International Workshop on Biomedical Image Registration (WBIR), Las Vegas, NV, USA, 26 June–1 July 2016; pp. 134–142. [Google Scholar]
- Giavarina, D. Understanding bland altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saculinggan, M.; Balase, E.A. Empirical power comparison of goodness of fit tests for normality in the presence of outliers. J. Phys. Conf. S 2013, 435, 012041. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013; Available online: http://www.R-project.org/ (accessed on 2 November 2021).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ROI Group | p Value |
|---|---|
| Mandible | 0.095 |
| Maxilla | 0.213 |
| Mandible and maxilla | 0.047 |
| Deviation from the Identity Line | |||
|---|---|---|---|
| ROI Group | Within ±10% | Between 10% and 15% | Greater Than 15% |
| Mandible | 97 ROIs; 77.0% | 24 ROIs; 19.0% | 5 ROIs; 4.0% |
| Maxilla | 68 ROIs; 81.0% | 15 ROIs; 17.9% | 1 ROI; 1.2% |
| Mandible and maxilla | 165 ROIs; 78.6% | 39 ROIs; 18.5% | 6 ROIs; 2.9% |
| ROI Group | Bias | Gap between the Bias and the AL | CI of AL |
|---|---|---|---|
| Mandible | −4.94% | 12.09% | 3.75% |
| Maxilla | −4.34% | 10.57% | 4.01% |
| Mandible and maxilla | −4.70% | 11.39% | 2.76% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, S.; Lee, S.C. A Comparative Study on the Voxel Values in Alveolar Bones Acquired by MDCT and Newly Developed Dental Dual-Energy CBCT. Sensors 2021, 21, 7552. https://doi.org/10.3390/s21227552
Chang S, Lee SC. A Comparative Study on the Voxel Values in Alveolar Bones Acquired by MDCT and Newly Developed Dental Dual-Energy CBCT. Sensors. 2021; 21(22):7552. https://doi.org/10.3390/s21227552
Chicago/Turabian StyleChang, Sungho, and Sang Chul Lee. 2021. "A Comparative Study on the Voxel Values in Alveolar Bones Acquired by MDCT and Newly Developed Dental Dual-Energy CBCT" Sensors 21, no. 22: 7552. https://doi.org/10.3390/s21227552
APA StyleChang, S., & Lee, S. C. (2021). A Comparative Study on the Voxel Values in Alveolar Bones Acquired by MDCT and Newly Developed Dental Dual-Energy CBCT. Sensors, 21(22), 7552. https://doi.org/10.3390/s21227552