
Deep Learning-Based Transfer Learning for Classification of Skin Cancer

 ,
,  ,
, 
 ,
,  and
and
Abstract
:1. Introduction
Literature Background
- To classify the images from HAM10000 dataset into seven different types of skin cancer.
- To use transfer learning nets for feature selection and classification so as to identify all types of lesions found in skin cancer.
- To properly balance the dataset using replication on only training data and perform a detailed analysis using different transfer learning models.
2. Materials and Methods
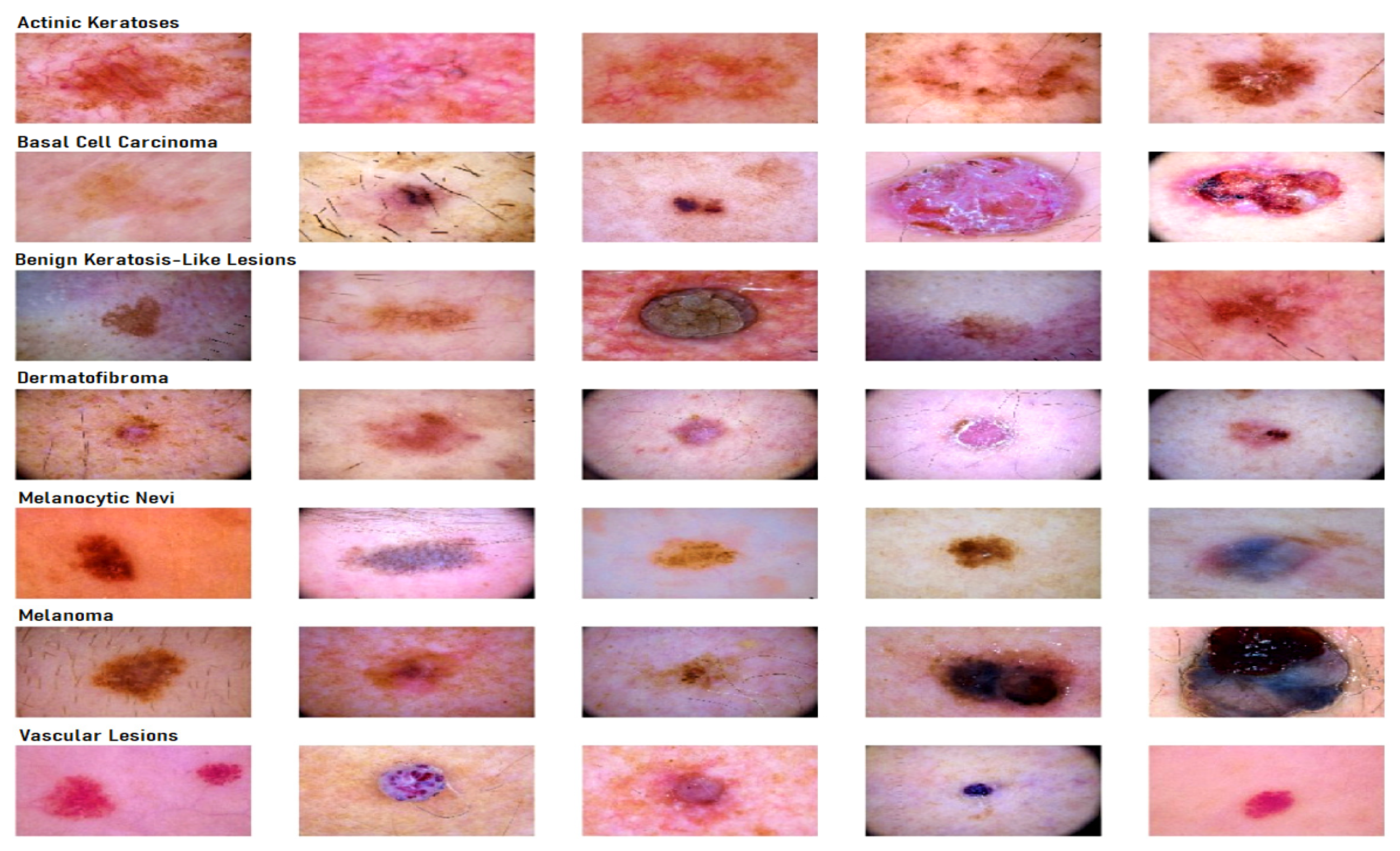
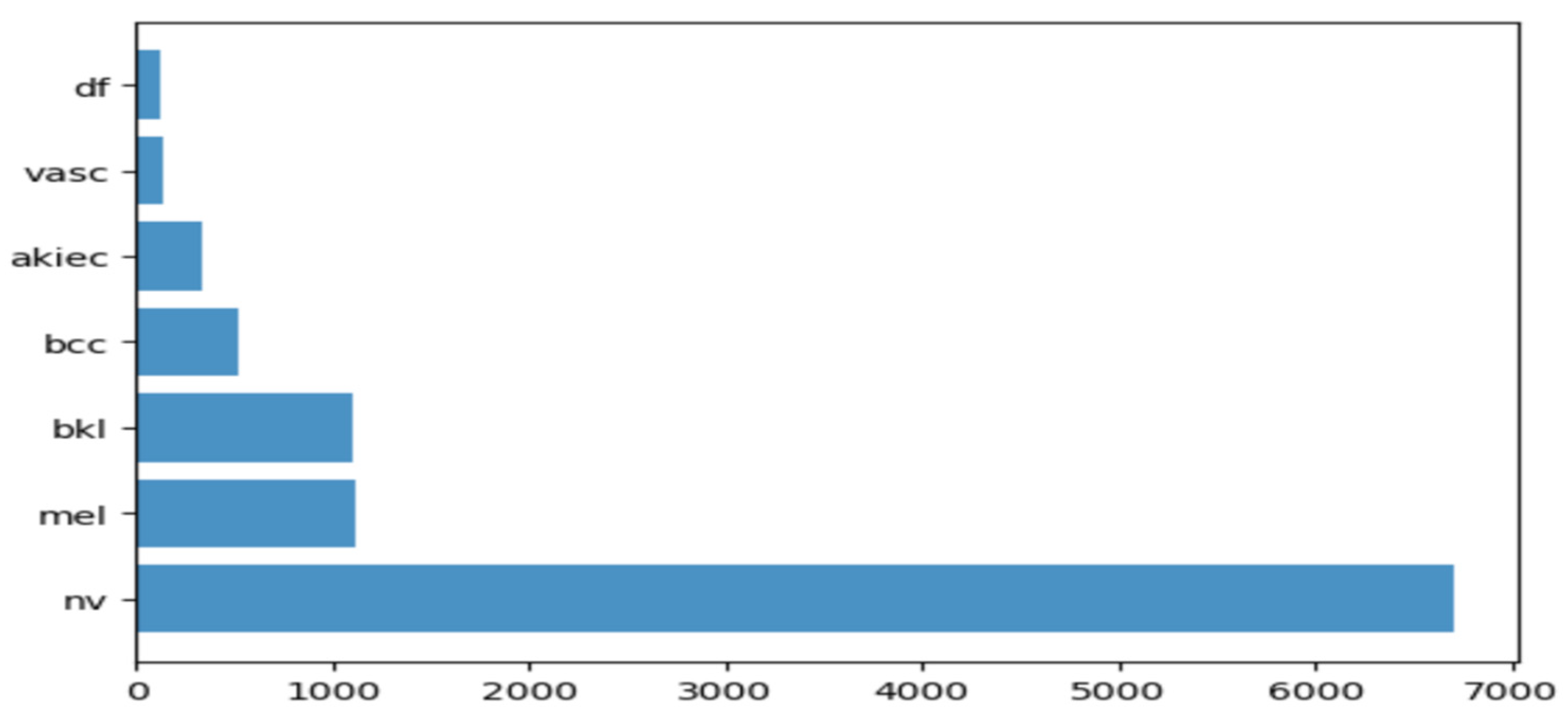
2.1. Dataset Description for Skin Lesion
2.2. Transfer Learning Nets
2.2.1. VGG19
2.2.2. InceptionV3
2.2.3. InceptionResnetv2
2.2.4. ResNet50
2.2.5. Xception
2.2.6. MobileNet
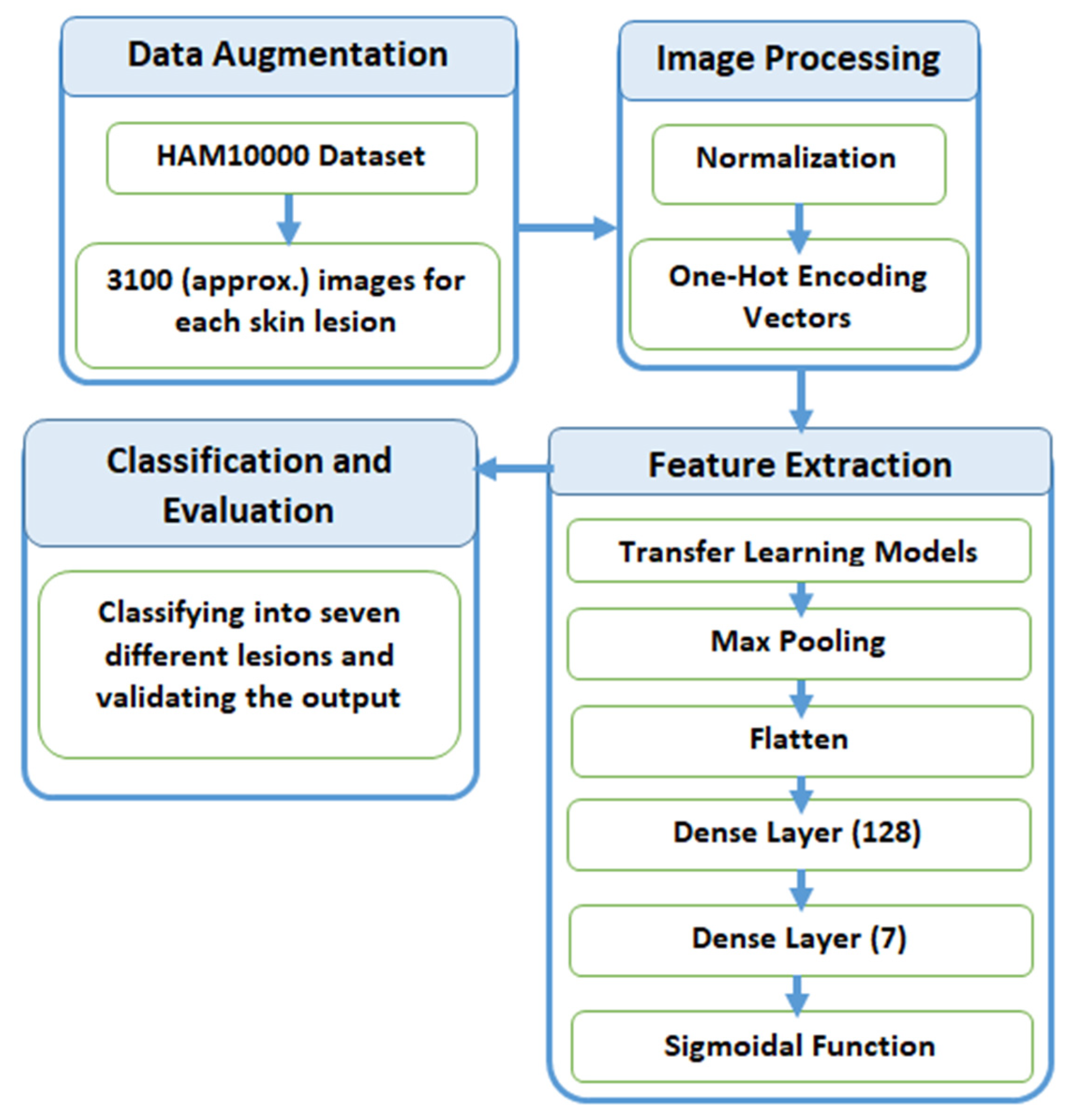
2.3. Proposed Methodology
2.3.1. Data Augmentation
2.3.2. Preprocessing
2.3.3. Feature Extraction
2.3.4. Classification and Evaluation
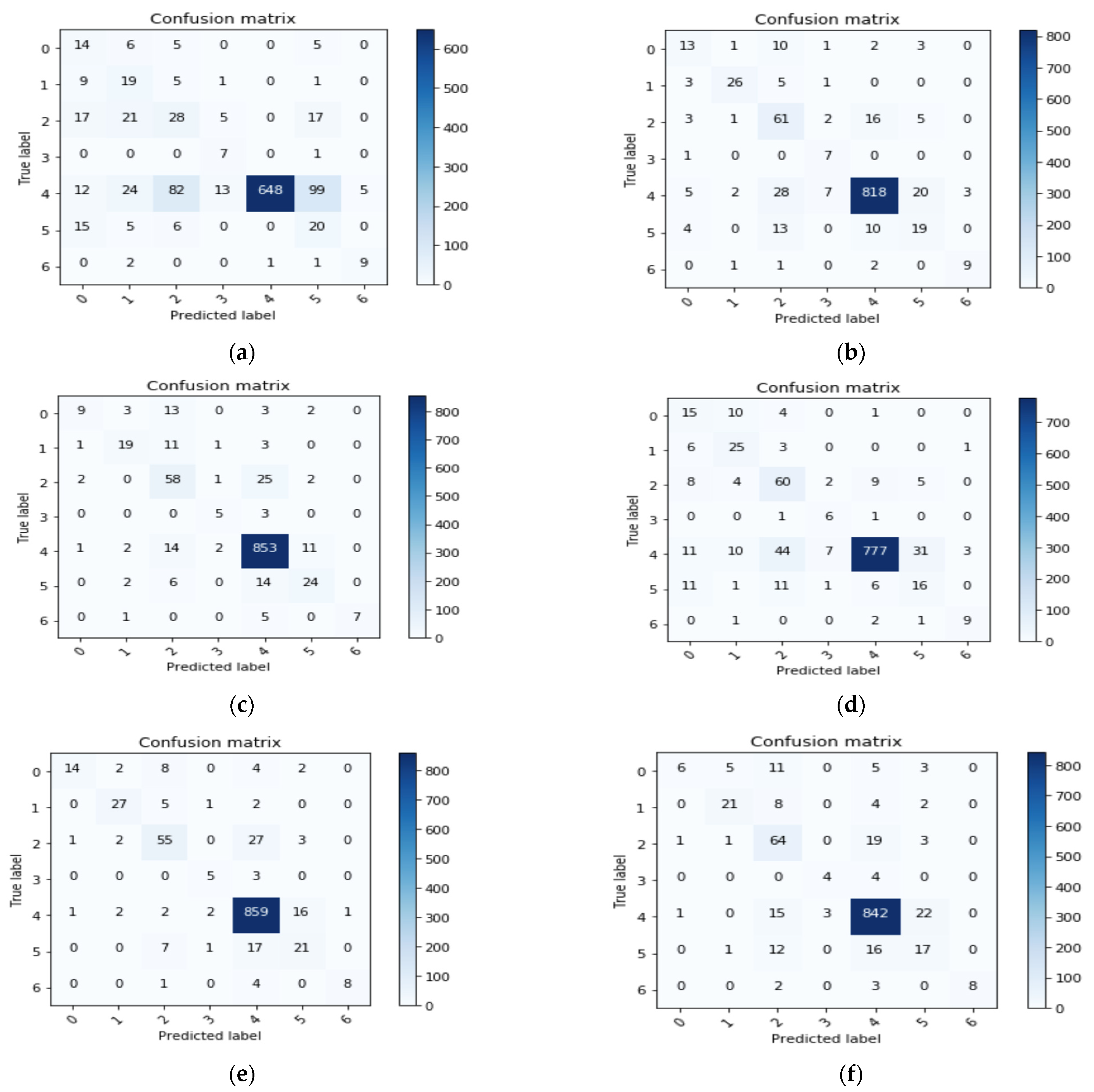
3. Results
Computational Cost
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kricker, A.; Armstrong, B.K.; English, D.R. Sun exposure and non-melanocytic skin cancer. Cancer Causes Control 1994, 5, 367–392. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, B.K.; Kricker, A. The epidemiology of UV induced skin cancer. J. Photochem. Photobiol. B 2001, 63, 8–18. [Google Scholar] [CrossRef]
- American Cancer Society. Cancer Facts and Figures. 2020. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2020/cancer-facts-and-figures-2020.pdf (accessed on 5 July 2021).
- Silberstein, L.; Anastasi, J. Hematology: Basic Principles and Practice; Elsevier: Amsterdam, The Netherlands, 2017; p. 2408. [Google Scholar]
- Kadampur, M.A.; Al Riyaee, S. Skin cancer detection: Applying a deep learning based model driven architecture in the cloud for classifying dermal cell images. Inform. Med. Unlocked 2020, 18, 100282. [Google Scholar] [CrossRef]
- Haenssle, H.A.; Fink, C.; Schneiderbauer, R.; Toberer, F.; Buhl, T.; Blum, A.; Kalloo, A.; Hassen, A.B.H.; Thomas, L.; Enk, A.; et al. Man against machine: Diagnostic performance of a deep learning convolutional neural network for dermoscopic melanoma recognition in comparison to 58 dermatologists. Ann. Oncol. 2018, 29, 1836–1842. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, S.; Snasel, V.; Hassanien, A.E.; Saha, S.; Tripathy, B.K. Deep Learning: Research and Applications; De Gruyter: Berlin, Germany; Boston, MA, USA, 2020. [Google Scholar] [CrossRef]
- Dhanamjayulu, C.; Nizhal, N.U.; Maddikunta, P.K.R.; Gadekallu, T.R.; Iwendi, C.; Wei, C.; Xin, Q. Identification of malnutrition and prediction of BMI from facial images using real-time image processing and machine learning. IET Image Process. 2021. [Google Scholar] [CrossRef]
- Adate, A.; Arya, D.; Shaha, A.; Tripathy, B.K. Deep Learning: Research and Applications. In 4 Impact of Deep Neural Learning on Artificial Intelligence Research; Siddhartha, B., Vaclav, S., Aboul Ella, H., Satadal, S., Tripathy, B.K., Eds.; De Gruyter: Berlin, Germany, 2020; pp. 69–84. [Google Scholar] [CrossRef]
- Adate, A.; Tripathy, B.K. Deep Learning Techniques for Image Processing Machine Learning for Big Data Analysis; Bhattacharyya, S., Bhaumik, H., Mukherjee, A., De, S., Eds.; De Gruyter: Berlin, Germany, 2018; pp. 69–90. [Google Scholar] [CrossRef]
- Ayoub, A.; Mahboob, K.; Javed, A.R.; Rizwan, M.; Gadekallu, T.R.; Alkahtani, M.; Abidi, M.H. Classification and Categorization of COVID-19 Outbreak in Pakistan. Comput. Mater. Contin. 2021, 69, 1253–1269. [Google Scholar] [CrossRef]
- Abidi, M.H.; Alkhalefah, H.; Mohammed, M.K.; Umer, U.; Qudeiri, J.E.A. Optimal Scheduling of Flexible Manufacturing System Using Improved Lion-Based Hybrid Machine Learning Approach. IEEE Access 2020, 8, 96088–96114. [Google Scholar] [CrossRef]
- Abidi, M.H.; Umer, U.; Mohammed, M.K.; Aboudaif, M.K.; Alkhalefah, H. Automated Maintenance Data Classification Using Recurrent Neural Network: Enhancement by Spotted Hyena-Based Whale Optimization. Mathematics 2020, 8, 2008. [Google Scholar] [CrossRef]
- Ch, R.; Gadekallu, T.R.; Abidi, M.H.; Al-Ahmari, A. Computational System to Classify Cyber Crime Offenses using Machine Learning. Sustainability 2020, 12, 4087. [Google Scholar] [CrossRef]
- Abidi, M.H.; Alkhalefah, H.; Umer, U. Fuzzy harmony search based optimal control strategy for wireless cyber physical system with industry 4.0. J. Intell. Manuf. 2021. [Google Scholar] [CrossRef]
- Kumar, P.A.; Shankar, G.S.; Maddikunta, P.K.R.; Gadekallu, T.R.; Al-Ahmari, A.; Abidi, M.H. Location Based Business Recommendation Using Spatial Demand. Sustainability 2020, 12, 4124. [Google Scholar]
- Marks, R. The epidemiology of non-melanoma skin cancer: Who, why and what can we do about it. J. Dermatol. 1995, 22, 853–857. [Google Scholar] [CrossRef]
- Farooq, A.; Jia, X.; Hu, J.; Zhou, J. Transferable Convolutional Neural Network for Weed Mapping With Multisensor Imagery. IEEE Trans. Geosci. Remote Sens. 2021, 1–16. [Google Scholar] [CrossRef]
- Farooq, A.; Jia, X.; Hu, J.; Zhou, J. Knowledge Transfer via Convolution Neural Networks for Multi-Resolution Lawn Weed Classification. In Proceedings of the 2019 10th Workshop on Hyperspectral Imaging and Signal Processing: Evolution in Remote Sensing (WHISPERS), Amsterdam, The Netherlands, 24–26 September 2019; pp. 1–5. [Google Scholar]
- Bose, A.; Tripathy, B.K. Deep Learning for Audio Signal Classification. In Deep Learning: Research and Applications; Bhattacharyya, S., Snasel, V., Ella Hassanien, A., Saha, S., Tripathy, B.K., Eds.; De Gruyter: Berlin, Germany, 2020; pp. 105–136. [Google Scholar] [CrossRef]
- Ghayvat, H.; Pandya, S.N.; Bhattacharya, P.; Zuhair, M.; Rashid, M.; Hakak, S.; Dev, K. CP-BDHCA: Blockchain-based Confidentiality-Privacy preserving Big Data scheme for healthcare clouds and applications. IEEE J. Biomed. Health Inform. 2021, 1. [Google Scholar] [CrossRef]
- Shah, A.; Ahirrao, S.; Pandya, S.; Kotecha, K.; Rathod, S. Smart Cardiac Framework for an Early Detection of Cardiac Arrest Condition and Risk. Front. Public Health 2021, 9, 762303. [Google Scholar] [CrossRef] [PubMed]
- Ghayvat, H.; Awais, M.; Gope, P.; Pandya, S.; Majumdar, S. ReCognizing SUspect and PredictiNg ThE SpRead of Contagion Based on Mobile Phone LoCation DaTa (COUNTERACT): A system of identifying COVID-19 infectious and hazardous sites, detecting disease outbreaks based on the internet of things, edge computing, and artificial intelligence. Sustain. Cities Soc. 2021, 69, 102798. [Google Scholar] [CrossRef]
- Kaul, D.; Raju, H.; Tripathy, B.K. Deep Learning in Healthcare. In Deep Learning in Data Analytics: Recent Techniques, Practices and Applications; Acharjya, D.P., Mitra, A., Zaman, N., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 97–115. [Google Scholar] [CrossRef]
- Nugroho, A.A.; Slamet, I.; Sugiyanto. Skins cancer identification system of HAMl0000 skin cancer dataset using convolutional neural network. AIP Conf. Proc. 2019, 2202, 020039. [Google Scholar] [CrossRef]
- Voulodimos, A.; Doulamis, N.; Doulamis, A.; Protopapadakis, E. Deep Learning for Computer Vision: A Brief Review. Comput. Intell. Neurosci. 2018, 2018, 7068349. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Liu, Y.; Oerlemans, A.; Lao, S.; Wu, S.; Lew, M.S. Deep learning for visual understanding: A review. Neurocomputing 2016, 187, 27–48. [Google Scholar] [CrossRef]
- Garcia-Garcia, A.; Orts-Escolano, S.; Oprea, S.; Villena-Martinez, V.; Garcia-Rodriguez, J. A Review on Deep Learning Techniques Applied to Semantic Segmentation. arXiv 2017, arXiv:1704.06857. Available online: https://ui.adsabs.harvard.edu/abs/2017arXiv170406857G (accessed on 1 April 2017).
- Maheshwari, K.; Shaha, A.; Arya, D.; Rajasekaran, R.; Tripathy, B.K. Deep Learning: Research and Applications. In Convolutional Neural Networks: A Bottom-Up Approach; Siddhartha, B., Vaclav, S., Aboul Ella, H., Satadal, S., Tripathy, B.K., Eds.; De Gruyter: Berlin, Germany, 2020; pp. 21–50. [Google Scholar] [CrossRef]
- Mateen, M.; Wen, J.; Nasrullah; Song, S.; Huang, Z. Fundus Image Classification Using VGG-19 Architecture with PCA and SVD. Symmetry 2019, 11, 1. [Google Scholar] [CrossRef] [Green Version]
- Canziani, A.; Paszke, A.; Culurciello, E. An Analysis of Deep Neural Network Models for Practical Applications. arXiv 2016, arXiv:1605.07678. [Google Scholar]
- Codella, N.C.F.; Gutman, D.; Celebi, M.E.; Helba, B.; Marchetti, M.A.; Dusza, S.W.; Kalloo, A.; Liopyris, K.; Mishra, N.; Kittler, H.; et al. Skin lesion analysis toward melanoma detection: A challenge at the 2017 International symposium on biomedical imaging (ISBI), hosted by the international skin imaging collaboration (ISIC). In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018; pp. 168–172. [Google Scholar]
- Li, Y.; Shen, L. Skin Lesion Analysis towards Melanoma Detection Using Deep Learning Network. Sensors 2018, 18, 556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, S.S.; Kim, M.S.; Lim, W.; Park, G.H.; Park, I.; Chang, S.E. Classification of the Clinical Images for Benign and Malignant Cutaneous Tumors Using a Deep Learning Algorithm. J. Investig. Dermatol. 2018, 138, 1529–1538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaturvedi, S.S.; Gupta, K.; Prasad, P.S. Skin Lesion Analyser: An Efficient Seven-Way Multi-class Skin Cancer Classification Using MobileNet. Adv. Mach. Learn. Technol. Appl. 2020, 1141, 165–176. [Google Scholar] [CrossRef]
- Milton, M.A.A. Automated Skin Lesion Classification Using Ensemble of Deep Neural Networks in ISIC 2018: Skin Lesion Analysis Towards Melanoma Detection Challenge. arXiv 2019, arXiv:1901.10802. [Google Scholar]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Oakley, A.; Bansal, P.; Dancey, D.; Yap, M.H. Skin Lesion Segmentation in Dermoscopic Images With Ensemble Deep Learning Methods. IEEE Access 2020, 8, 4171–4181. [Google Scholar] [CrossRef]
- Tschandl, P.; Rosendahl, C.; Kittler, H. The HAM10000 dataset, a large collection of multi-source dermatoscopic images of common pigmented skin lesions. Sci. Data 2018, 5, 180161. [Google Scholar] [CrossRef] [PubMed]
- Adate, A.; Tripathy, B.K. A Survey on Deep Learning Methodologies of Recent Applications. In Deep Learning in Data Analytics: Recent Techniques, Practices and Applications; Acharjya, D.P., Mitra, A., Zaman, N., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 145–170. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the Inception Architecture for Computer Vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Szegedy, C.; Wei, L.; Yangqing, J.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the 2015 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A.A. Inception-v4, inception-ResNet and the impact of residual connections on learning. In Proceedings of the Thirty-First AAAI Conference on Artificial Intelligence, San Francisco, CA, USA, 4–9 February 2017; pp. 4278–4284. [Google Scholar]
- Debgupta, R.; Chaudhuri, B.B.; Tripathy, B.K. A Wide ResNet-Based Approach for Age and Gender Estimation in Face Images. In Proceedings of the International Conference on Innovative Computing and Communications, Singapore, 24 October 2020; pp. 517–530. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Chollet, F. Xception: Deep Learning with Depthwise Separable Convolutions. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 1800–1807. [Google Scholar]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Andreetto, M.; Adam, H. Mobilenets: Efficient convolutional neural networks for mobile vision applications. arXiv 2017, arXiv:1704.04861. [Google Scholar]
- Fabiano, N.; Radenovic, S. Geometric Brownian motion and a new approach to the spread of Covid-19 in Italy. Gulf J. Math. 2021, 10, 25–30. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Frequency before Augmentation | Multiply Factor (k) | Frequency after Augmentation |
|---|---|---|---|
| Melanocytic Nevi | 3179 | 1 | 3179 |
| Benign Keratosis | 317 | 10 | 3170 |
| Melanoma | 165 | 19 | 3135 |
| Basal Cell Carcinoma | 126 | 25 | 3150 |
| Actinic Keratosis | 109 | 29 | 3161 |
| Vascular Skin Lesions | 46 | 69 | 3174 |
| Dermatofibroma | 28 | 110 | 3080 |
| Model without Repetition | Accuracy | Avg. Recall | Avg. Precision | Avg. F-Measure |
|---|---|---|---|---|
| VGG19 | 0.6718 | 0.67 | 0.78 | 0.71 |
| InceptionV3 | 0.8168 | 0.82 | 0.75 | 0.78 |
| InceptionResnetV2 | 0.8114 | 0.81 | 0.82 | 0.80 |
| ResNet50 | 0.8105 | 0.81 | 0.75 | 0.77 |
| Xception | 0.8096 | 0.81 | 0.78 | 0.78 |
| MobileNet | 0.8241 | 0.82 | 0.84 | 0.80 |
| Model with Repetition | Accuracy | Avg. Recall | Avg. Precision | Avg. F-Measure |
|---|---|---|---|---|
| VGG19 | 0.66 | 0.66 | 0.86 | 0.72 |
| InceptionV3 | 0.79 | 0.79 | 0.87 | 0.82 |
| InceptionResnetV2 | 0.85 | 0.86 | 0.88 | 0.86 |
| ResNet50 | 0.77 | 0.78 | 0.86 | 0.80 |
| Xception | 0.90 | 0.90 | 0.90 | 0.90 |
| MobileNet | 0.88 | 0.89 | 0.88 | 0.88 |
| Model | Accuracy | Avg. Recall | Avg. Precision | Avg. F-Measure |
|---|---|---|---|---|
| VGG19 | 0.6754 | 0.6734 | 0.8548 | 0.7479 |
| InceptionV3 | 0.8640 | 0.8619 | 0.8769 | 0.8713 |
| InceptionResnetV2 | 0.8840 | 0.8762 | 0.8793 | 0.8845 |
| ResNet50 | 0.8232 | 0.8222 | 0.8680 | 0.8416 |
| Xception | 0.8966 | 0.8957 | 0.8876 | 0.8902 |
| MobileNet | 0.8721 | 0.8711 | 0.8838 | 0.8740 |
| Disease | Avg. Precision | Avg. Recall | Avg. F-Measure |
|---|---|---|---|
| Melanocytic Nevi | 0.94 | 0.98 | 0.96 |
| Benign Keratosis | 0.68 | 0.68 | 0.68 |
| Melanoma | 0.58 | 0.48 | 0.52 |
| Basal Cell Carcinoma | 0.88 | 0.80 | 0.84 |
| Actinic Keratosis | 0.92 | 0.37 | 0.52 |
| Vascular Skin Lesions | 1.0 | 0.69 | 0.82 |
| Dermatofibroma | 0.71 | 0.62 | 0.67 |
| Transfer Learning Nets | Accuracy | Loss |
|---|---|---|
| VGG19 | 66.36 | 1.0134 |
| Resnet50 | 77.60 | 0.6855 |
| InceptionResNetV2 | 85.58 | 0.6745 |
| InceptionV3 | 79.23 | 0.6665 |
| Xception | 90.48 | 0.5168 |
| MobileNet | 88.57 | 0.6347 |
| Hardware Use | Specification |
|---|---|
| NVIDIA GPU | Tesla P100 |
| CUDA Version | 9.2 |
| GPU RAM (GB) | 17.1 |
| CPU Chip | Intel Xeon CPU |
| Chip Speed (GHz) | 2.2 or 2.3 |
| CPU Cores | 2 |
| CPU RAM (Total GB) | 16.4 |
| L3 Cache (MB) | 46 |
| Disk Space (Total GB) | 220 |
| Model Name | Computational Time (In Seconds) |
|---|---|
| VGG19 | 746.84069 |
| InceptionV3 | 751.12284 |
| InceptionResnetV2 | 2456.34356 |
| ResNet50 | 761.63929 |
| Xception | 834.66028 |
| MobileNet | 695.36065 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jain, S.; Singhania, U.; Tripathy, B.; Nasr, E.A.; Aboudaif, M.K.; Kamrani, A.K. Deep Learning-Based Transfer Learning for Classification of Skin Cancer. Sensors 2021, 21, 8142. https://doi.org/10.3390/s21238142
Jain S, Singhania U, Tripathy B, Nasr EA, Aboudaif MK, Kamrani AK. Deep Learning-Based Transfer Learning for Classification of Skin Cancer. Sensors. 2021; 21(23):8142. https://doi.org/10.3390/s21238142
Chicago/Turabian StyleJain, Satin, Udit Singhania, Balakrushna Tripathy, Emad Abouel Nasr, Mohamed K. Aboudaif, and Ali K. Kamrani. 2021. "Deep Learning-Based Transfer Learning for Classification of Skin Cancer" Sensors 21, no. 23: 8142. https://doi.org/10.3390/s21238142
APA StyleJain, S., Singhania, U., Tripathy, B., Nasr, E. A., Aboudaif, M. K., & Kamrani, A. K. (2021). Deep Learning-Based Transfer Learning for Classification of Skin Cancer. Sensors, 21(23), 8142. https://doi.org/10.3390/s21238142