
Segmentation Approaches for Diabetic Foot Disorders

 ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Image Acquisition
2.2. Segmentation Approaches
2.2.1. Manual Segmentation: Establishment of the Ground Truth
2.2.2. U-Net + Depth (UPD)
2.2.3. Skin + Depth (SPD)
2.2.4. SegNet
2.3. Evaluation Metrics
2.3.1. Simultaneous Truth and Performance Level Estimation (STAPLE)
2.3.2. Dice Similarity Coefficient (DICE)
2.3.3. Intersection over Union (IoU) or Jaccard
2.3.4. Sensitivity, Specificity, and Precision
2.4. Statistical Analysis
3. Results
3.1. Manual Segmentation: Establishment of the Ground Truth
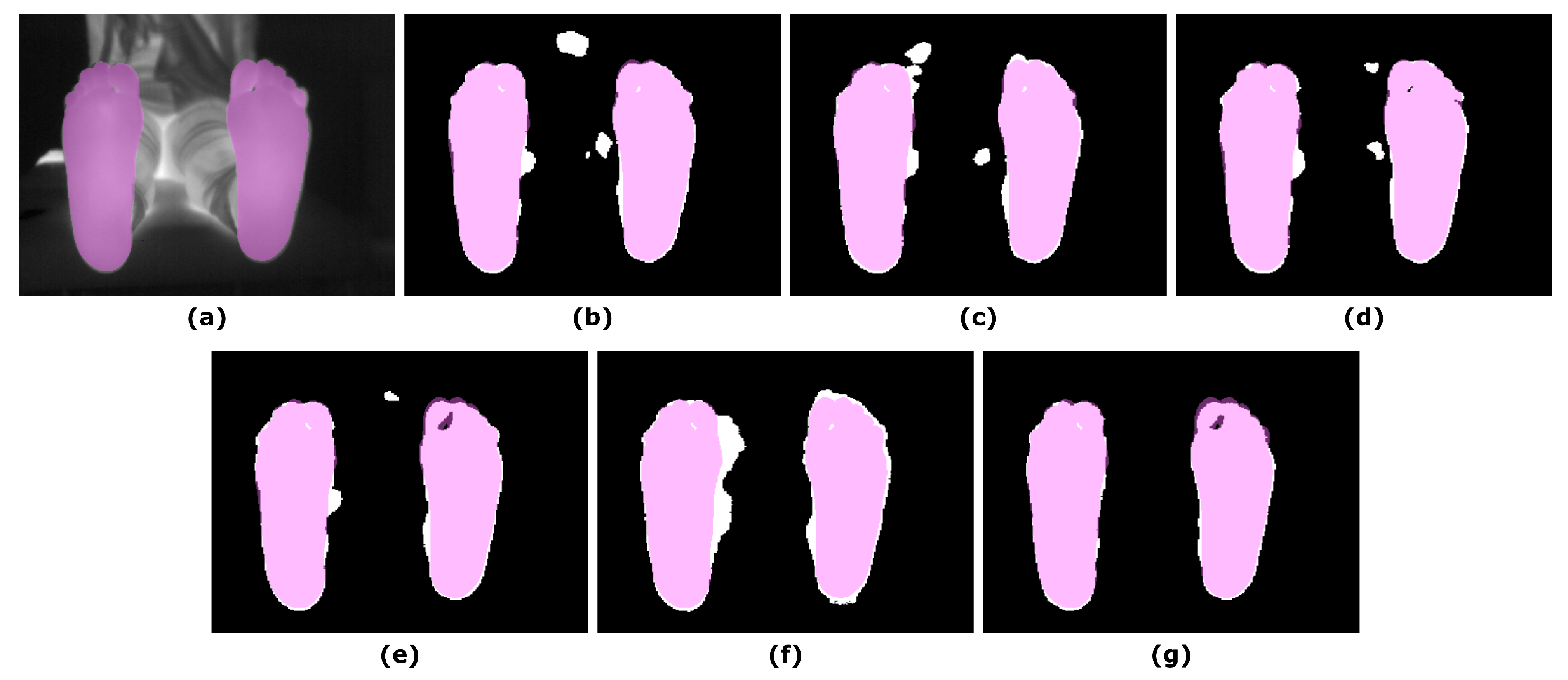
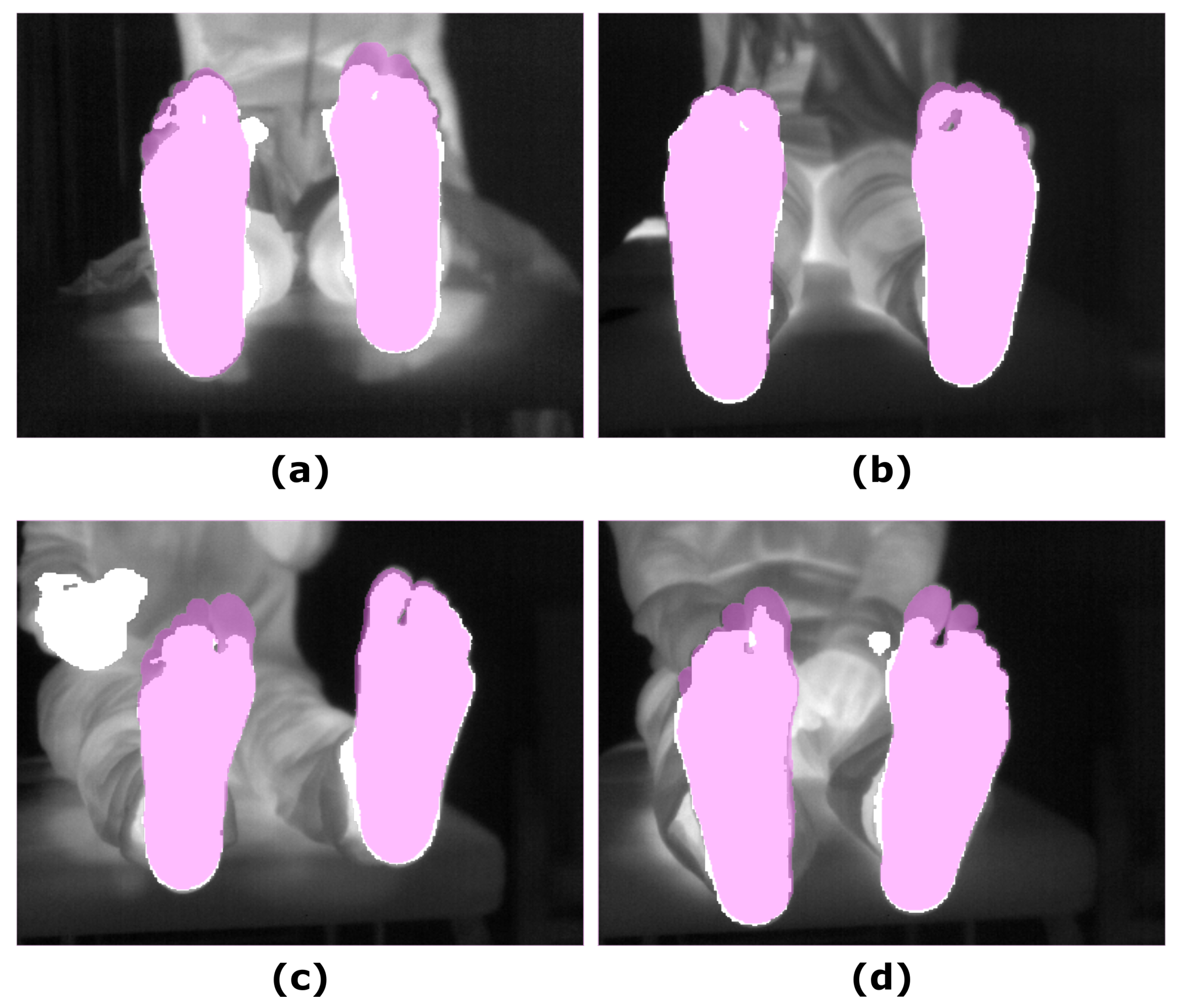
3.2. Segmentation Approaches
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ARGB | RGB with an alpha channel |
| BCE | Binary Cross Entropy |
| DICE | DICE Similarity Coefficient |
| FN | False Negative |
| FOV | Field of View |
| FP | False Positive |
| IoU | Intersection over Union or Jaccard Index |
| IR | Infrared |
| PNG | Portable Network Graphic |
| RANSAC | RANdom Sample Consensus |
| RGB | Red, green and blue color space |
| SegNet | SegNet algorithm |
| SGD | Stochastic Gradient Descent |
| SPD | Skin plus Depth algorithm |
| STAPLE | Simultaneous Truth and Performance Level Estimation |
| TN | True Negative |
| TP | True Positive |
| UPD | U-Net plus Depth algorithm |
| VGG | Visual Geometry Group |
References
- Roback, K. An overview of temperature monitoring devices for early detection of diabetic foot disorders. Expert Rev. Med. Devices 2010, 7, 711–718. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; van Netten, J.J.; Van Baal, J.G.; Bus, S.A.; van Der Heijden, F. Automatic detection of diabetic foot complications with infrared thermography by asymmetric analysis. J. Biomed. Opt. 2015, 20, 026003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klaesner, J.W.; Hastings, M.K.; Zou, D.; Lewis, C.; Mueller, M.J. Plantar tissue stiffness in patients with diabetes mellitus and peripheral neuropathy. Arch. Phys. Med. Rehabil. 2002, 83, 1796–1801. [Google Scholar] [CrossRef] [PubMed]
- Piaggesi, A.; Romanelli, M.; Schipani, E.; Campi, F.; Magliaro, A.; Baccetti, F.; Navalesi, R. Hardness of plantar skin in diabetic neuropathic feet. J. Diabetes Complicat. 1999, 13, 129–134. [Google Scholar] [CrossRef]
- Choi, W.; Ahn, B. Monitoring System for Diabetic Foot Ulceration Patients Using Robotic Palpation. Int. J. Control Autom. Syst. 2020, 18, 46–52. [Google Scholar] [CrossRef]
- Etehadtavakol, M.; Ng, E.; Kaabouch, N. Automatic segmentation of thermal images of diabetic-at-risk feet using the snakes algorithm. Infrared Phys. Technol. 2017, 86, 66–76. [Google Scholar] [CrossRef]
- Gordon, I.L.; Rothenberg, G.M.; Lepow, B.D.; Petersen, B.J.; Linders, D.R.; Bloom, J.D.; Armstrong, D.G. Accuracy of a foot temperature monitoring mat for predicting diabetic foot ulcers in patients with recent wounds or partial foot amputation. Diabetes Res. Clin. Pract. 2020, 161, 108074. [Google Scholar] [CrossRef] [Green Version]
- Bergeron, A.; Le Noc, L.; Tremblay, B.; Lagacé, F.; Mercier, L.; Duchesne, F.; Marchese, L.; Lambert, J.; Jacob, M.; Morissette, M.; et al. Flexible 640 × 480 pixel infrared camera module for fast prototyping. In Electro-Optical and Infrared Systems: Technology and Applications VI; International Society for Optics and Photonics: Berlin, Germany, 2009; Volume 7481, p. 74810L. [Google Scholar]
- Martín, Y.; Joven, E.; Reyes, M.; Licandro, J.; Maroto, O.; Díez-Merino, L.; Tomàs, A.; Carbonell, J.; de los Ríos, J.M.; del Peral, L.; et al. Microbolometer Characterization with the Electronics Prototype of the IRCAM for the JEM-EUSO Mission. In Space Telescopes and Instrumentation 2014: Optical, Infrared, and Millimeter Wave; International Society for Optics and Photonics: Montreal, QC, Canada, 2014; Volume 9143, p. 91432A. [Google Scholar]
- Frykberg, R.G.; Gordon, I.L.; Reyzelman, A.M.; Cazzell, S.M.; Fitzgerald, R.H.; Rothenberg, G.M.; Bloom, J.D.; Petersen, B.J.; Linders, D.R.; Nouvong, A.; et al. Feasibility and efficacy of a smart mat technology to predict development of diabetic plantar ulcers. Diabetes Care 2017, 40, 973–980. [Google Scholar] [CrossRef] [Green Version]
- Gorbach, A.M.; Heiss, J.D.; Kopylev, L.; Oldfield, E.H. Intraoperative infrared imaging of brain tumors. J. Neurosurg. 2004, 101, 960–969. [Google Scholar] [CrossRef]
- Bousselham, A.; Bouattane, O.; Youssfi, M.; Raihani, A. 3D brain tumor localization and parameter estimation using thermographic approach on GPU. J. Therm. Biol. 2018, 71, 52–61. [Google Scholar] [CrossRef]
- Hoffmann, N.; Koch, E.; Steiner, G.; Petersohn, U.; Kirsch, M. Learning thermal process representations for intraoperative analysis of cortical perfusion during ischemic strokes. In Deep Learning and Data Labeling for Medical Applications; Springer: Athens, Greece, 2016; pp. 152–160. [Google Scholar]
- Gorbach, A.M.; Heiss, J.; Kufta, C.; Sato, S.; Fedio, P.; Kammerer, W.A.; Solomon, J.; Oldfield, E.H. Intraoperative infrared functional imaging of human brain. Ann. Neurol. 2003, 54, 297–309. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, K.P.; Ruff, R.; Kirsch, M. SEP-induced activity and its thermographic cortical representation in a murine model. Biomed. Eng. Technol. 2013, 58, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Benito-de Pedro, M.; Becerro-de Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Rodríguez-Sanz, D.; López-López, D.; Cosín-Matamoros, J.; Martínez-Jiménez, E.M.; Calvo-Lobo, C. Effectiveness between dry needling and ischemic compression in the triceps surae latent myofascial trigger points of triathletes on pressure pain threshold and thermography: A single blinded randomized clinical trial. J. Clin. Med. 2019, 8, 1632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Requena-Bueno, L.; Priego-Quesada, J.I.; Jimenez-Perez, I.; Gil-Calvo, M.; Pérez-Soriano, P. Validation of ThermoHuman automatic thermographic software for assessing foot temperature before and after running. J. Therm. Biol. 2020, 92, 102639. [Google Scholar] [CrossRef] [PubMed]
- Villa, E.; Arteaga-Marrero, N.; Ruiz-Alzola, J. Performance Assessment of Low-Cost Thermal Cameras for Medical Applications. Sensors 2020, 20, 1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bougrine, A.; Harba, R.; Canals, R.; Ledee, R.; Jabloun, M. A joint snake and atlas-based segmentation of plantar foot thermal images. In Proceedings of the IEEE 2017 Seventh International Conference on Image Processing Theory, Tools and Applications (IPTA), Montreal, QC, Canada, 28 November–1 December 2017; pp. 1–6. [Google Scholar]
- Hernández, A.; Arteaga-Marrero, N.; Villa, E.; Fabelo, H.; Callicó, G.M.; Ruiz-Alzola, J. Automatic Segmentation Based on Deep Learning Techniques for Diabetic Foot Monitoring Through Multimodal Images. In Proceedings of the International Conference on Image Analysis and Processing, Trento, Italy, 9–13 September 2019; pp. 414–424. [Google Scholar]
- Müller, J.; Müller, J.; Chen, F.; Tetzlaff, R.; Müller, J.; Böhl, E.; Kirsch, M.; Schnabel, C. Registration and fusion of thermographic and visual-light images in neurosurgery. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 1313–1321. [Google Scholar] [CrossRef]
- Jin, X.; Jiang, Q.; Yao, S.; Zhou, D.; Nie, R.; Hai, J.; He, K. A survey of infrared and visual image fusion methods. Infrared Phys. Technol. 2017, 85, 478–501. [Google Scholar] [CrossRef]
- Li, R.; Zhang, Y.; Xing, L.; Li, W. An Adaptive Foot-image Segmentation Algorithm Based on Morphological Partition. In Proceedings of the 2018 IEEE International Conference on Progress in Informatics and Computing (PIC), Suzhou, China, 14–16 December 2018; pp. 231–235. [Google Scholar]
- Bougrine, A.; Harba, R.; Canals, R.; Ledee, R.; Jabloun, M. On the segmentation of plantar foot thermal images with Deep Learning. In Proceedings of the IEEE 2019 27th European Signal Processing Conference (EUSIPCO), A Coruña, Spain, 2–6 September 2019; pp. 1–5. [Google Scholar]
- Yushkevich, P.A.; Piven, J.; Cody Hazlett, H.; Gimpel Smith, R.; Ho, S.; Gee, J.C.; Gerig, G. User-Guided 3D Active Contour Segmentation of Anatomical Structures: Significantly Improved Efficiency and Reliability. Neuroimage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [Green Version]
- Warfield, S.K.; Zou, K.H.; Wells, W.M. Simultaneous truth and performance level estimation (STAPLE): An algorithm for the validation of image segmentation. IEEE Trans. Med. Imaging 2004, 23, 903–921. [Google Scholar] [CrossRef] [Green Version]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar]
- Iglovikov, V.; Shvets, A. Ternausnet: U-net with vgg11 encoder pre-trained on imagenet for image segmentation. arXiv 2018, arXiv:1801.05746. [Google Scholar]
- Fischler, M.A.; Bolles, R.C. Random sample consensus: A paradigm for model fitting with applications to image analysis and automated cartography. Commun. ACM 1981, 24, 381–395. [Google Scholar] [CrossRef]
- Kolkur, S.; Kalbande, D.; Shimpi, P.; Bapat, C.; Jatakia, J. Human skin detection using RGB, HSV and YCbCr color models. arXiv 2017, arXiv:1708.02694. [Google Scholar]
- Badrinarayanan, V.; Handa, A.; Cipolla, R. Segnet: A deep convolutional encoder-decoder architecture for robust semantic pixel-wise labelling. arXiv 2015, arXiv:1505.07293. [Google Scholar]
- Bloice, M.D.; Roth, P.M.; Holzinger, A. Biomedical image augmentation using Augmentor. Bioinformatics 2019, 35, 4522–4524. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. Imagenet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef] [Green Version]
- Dice, L.R. Measures of the amount of ecologic association between species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- Jaccard, P. The distribution of the flora in the alpine zone. 1. New Phytol. 1912, 11, 37–50. [Google Scholar] [CrossRef]
- Yerushalmy, J. Statistical problems in assessing methods of medical diagnosis, with special reference to X-ray techniques. Public Health Rep. 1947, 62, 1432–1449. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. Diagnostic tests. 1: Sensitivity and specificity. Br. Med. J. 1994, 308, 1552. [Google Scholar] [CrossRef] [Green Version]
- Altman, D.G.; Bland, J.M. Statistics Notes: Diagnostic tests. 2: Predictive values. Br. Med. J. 1994, 309, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- RStudio Team. RStudio: Integrated Development Environment for R; RStudio: Boston, MA, USA, 2020. [Google Scholar]
- Bauer, D.F. Constructing confidence sets using rank statistics. J. Am. Stat. Assoc. 1972, 67, 687–690. [Google Scholar] [CrossRef]
- Toutenburg, H.; Hollander, M.; Wolfe, D.A. Nonparametric Statistical Methods; John Wiley & Sons: Hoboken, NJ, USA, 1973. [Google Scholar]
- Hochberg, Y. A sharper Bonferroni procedure for multiple tests of significance. Biometrika 1988, 75, 800–802. [Google Scholar] [CrossRef]
- Shaik, K.B.; Ganesan, P.; Kalist, V.; Sathish, B.; Jenitha, J.M.M. Comparative study of skin color detection and segmentation in HSV and YCbCr color space. Procedia Comput. Sci. 2015, 57, 41–48. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overlap Measures | Left Feet (T0) | Right Feet (T0) | Left Feet (T5) | Right Feet (T5) |
|---|---|---|---|---|
| DICE | 98.91 ± 0.50 | 99.27 ± 0.37 | 98.74 ± 0.52 | 99.25 ± 0.37 |
| IoU | 97.85 ± 0.97 | 98.55 ± 0.73 | 97.52 ± 1.00 | 98.51 ± 0.73 |
| Researcher | Mask | Time | Specificity | Sensitivity |
|---|---|---|---|---|
| Researcher 1 | L | T0 | 99.95 ± 0.04 | 99.23 ± 0.49 |
| R | T0 | 99.94 ± 0.06 | 99.64 ± 0.23 | |
| L | T5 | 99.95 ± 0.05 | 99.08 ± 0.48 | |
| R | T5 | 99.94 ± 0.06 | 99.65 ± 0.27 | |
| Researcher 2 | L | T0 | 99.88 ± 0.07 | 99.68 ± 0.26 |
| R | T0 | 99.95 ± 0.04 | 99.62 ± 0.35 | |
| L | T5 | 99.86 ± 0.08 | 99.66 ± 0.32 | |
| R | T5 | 99.95 ± 0.05 | 99.59 ± 0.36 |
| Segmentation | DICE (T0) | IoU (T0) | DICE (T5) | IoU (T5) |
|---|---|---|---|---|
| U-Net | 87.45 ± 6.52 | 78.24 ± 10.20 | 89.95 ± 6.52 | 82.27 ± 9.73 |
| UPD | 95.35 ± 0.40 | 91.11 ± 0.72 | 95.26 ± 0.41 | 90.95 ± 0.74 |
| Skin | 90.03 ± 4.40 | 82.13 ± 7.36 | 89.73 ± 5.25 | 81.75 ± 8.54 |
| SPD | 95.24 ± 0.52 | 90.93 ± 0.95 | 95.21 ± 0.47 | 90.86 ± 0.86 |
| DICE (T0) | IoU (T0) | Precision (T0) | DICE (T5) | IoU (T5) | Precision (T5) | |
|---|---|---|---|---|---|---|
| 0 | 91.99 ± 3.36 | 85.33 ± 5.73 | 89.83 ± 5.36 | 92.93 ± 2.66 | 86.89 ± 4.56 | 90.25 ± 4.76 |
| 0.2 | 90.39 ± 4.17 | 82.70 ± 6.86 | 86.68 ± 6.92 | 90.55 ± 3.93 | 82.94 ± 6.49 | 86.20 ± 6.98 |
| 0.4 | 92.49 ± 3.55 | 86.22 ± 6.07 | 90.19 ± 5.34 | 92.36 ± 3.42 | 85.97 ± 5.87 | 88.82 ± 6.19 |
| 0.6 | 92.15 ± 3.20 | 85.60 ± 5.44 | 90.55 ± 5.57 | 92.55 ± 2.93 | 86.27 ± 5.00 | 89.80 ± 5.35 |
| 0.8 | 88.02 ± 4.31 | 78.83 ± 6.69 | 80.24 ± 7.46 | 88.87 ± 4.44 | 80.24 ± 7.19 | 81.07 ± 7.42 |
| 1 | 92.99 ± 3.25 | 87.05 ± 5.55 | 92.11 ± 5.19 | 93.30 ± 2.91 | 87.57 ± 5.01 | 92.26 ± 5.11 |
| Segmentation | Specificity (T0) | Sensitivity (T0) | Precision (T0) | Specificity (T5) | Sensitivity (T5) | Precision (T5) |
|---|---|---|---|---|---|---|
| U-Net | 93.29 ± 7.10 | 98.41 ± 3.17 | 78.87 ± 10.36 | 92.37 ± 5.78 | 99.91 ± 0.20 | 82.76 ± 9.96 |
| UPD | 97.38 ± 4.83 | 96.09 ± 2.80 | 99.01 ± 0.45 | 97.73 ± 4.24 | 94.81 ± 2.63 | 98.93 ± 0.66 |
| Skin | 93.06 ± 4.14 | 99.18 ± 1.34 | 83.64 ± 7.75 | 95.36 ± 4.21 | 97.57 ± 2.85 | 83.25 ± 9.17 |
| SPD | 99.19 ± 1.83 | 94.57 ± 3.57 | 99.44 ± 0.28 | 99.99 ± 0.02 | 92.97 ± 2.26 | 99.44 ± 0.35 |
| SegNet | 97.72 ± 1.56 | 96.55 ± 2.50 | 92.11 ± 5.19 | 97.93 ± 1.46 | 97.01 ± 1.78 | 92.26 ± 5.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arteaga-Marrero, N.; Hernández, A.; Villa, E.; González-Pérez, S.; Luque, C.; Ruiz-Alzola, J. Segmentation Approaches for Diabetic Foot Disorders. Sensors 2021, 21, 934. https://doi.org/10.3390/s21030934
Arteaga-Marrero N, Hernández A, Villa E, González-Pérez S, Luque C, Ruiz-Alzola J. Segmentation Approaches for Diabetic Foot Disorders. Sensors. 2021; 21(3):934. https://doi.org/10.3390/s21030934
Chicago/Turabian StyleArteaga-Marrero, Natalia, Abián Hernández, Enrique Villa, Sara González-Pérez, Carlos Luque, and Juan Ruiz-Alzola. 2021. "Segmentation Approaches for Diabetic Foot Disorders" Sensors 21, no. 3: 934. https://doi.org/10.3390/s21030934
APA StyleArteaga-Marrero, N., Hernández, A., Villa, E., González-Pérez, S., Luque, C., & Ruiz-Alzola, J. (2021). Segmentation Approaches for Diabetic Foot Disorders. Sensors, 21(3), 934. https://doi.org/10.3390/s21030934