
Pain and Stress Detection Using Wearable Sensors and Devices—A Review




Abstract
:1. Introduction
2. Review Scope
3. Mechanism of Pain
4. Classification of Pain
4.1. Classification of Pain by Its Mechanisms
4.1.1. Nociceptive Pain
4.1.2. Neuropathic Pain
4.1.3. Nociplastic Pain
4.2. Classification of Pain by Its Time Period
4.2.1. Acute Pain
4.2.2. Chronic Pain
5. What Is Stress and what is Its Correlation with Pain?
6. Assessment for Pain and Stress
6.1. Pain Assessment
6.2. Stress Assessment
Stress Induction Tests
- Trier Social Stress Test
- Stroop Color-Word Inference Test
- Cold Pressor Test/Hot Water Immersion Test
- International Affective Picture System Test
6.3. Physiological Signals for Assessment
6.3.1. Heart Activity
6.3.2. Brain Activity
6.3.3. Muscle Activity
6.3.4. Electrodermal Activity
6.3.5. Blood Volume Pulse
6.3.6. Skin Temperature
6.4. Behavioral Signals for Assessment
6.4.1. Speech
6.4.2. Facial Expressions
6.4.3. Keystroke and Mouse Dynamics
6.4.4. Body Gestures and Movements
6.4.5. Mobile Phone Usage
6.4.6. Questionnaires and Surveys
7. Medical Devices or Wearable Sensors used in Pain and Stress Detection
7.1. Medical Devices Used in Pain Detection
7.1.1. Analgesia Nociception Index
7.1.2. Surgical Pleth Index
7.2. Wearable Sensors Used in Stress Detection
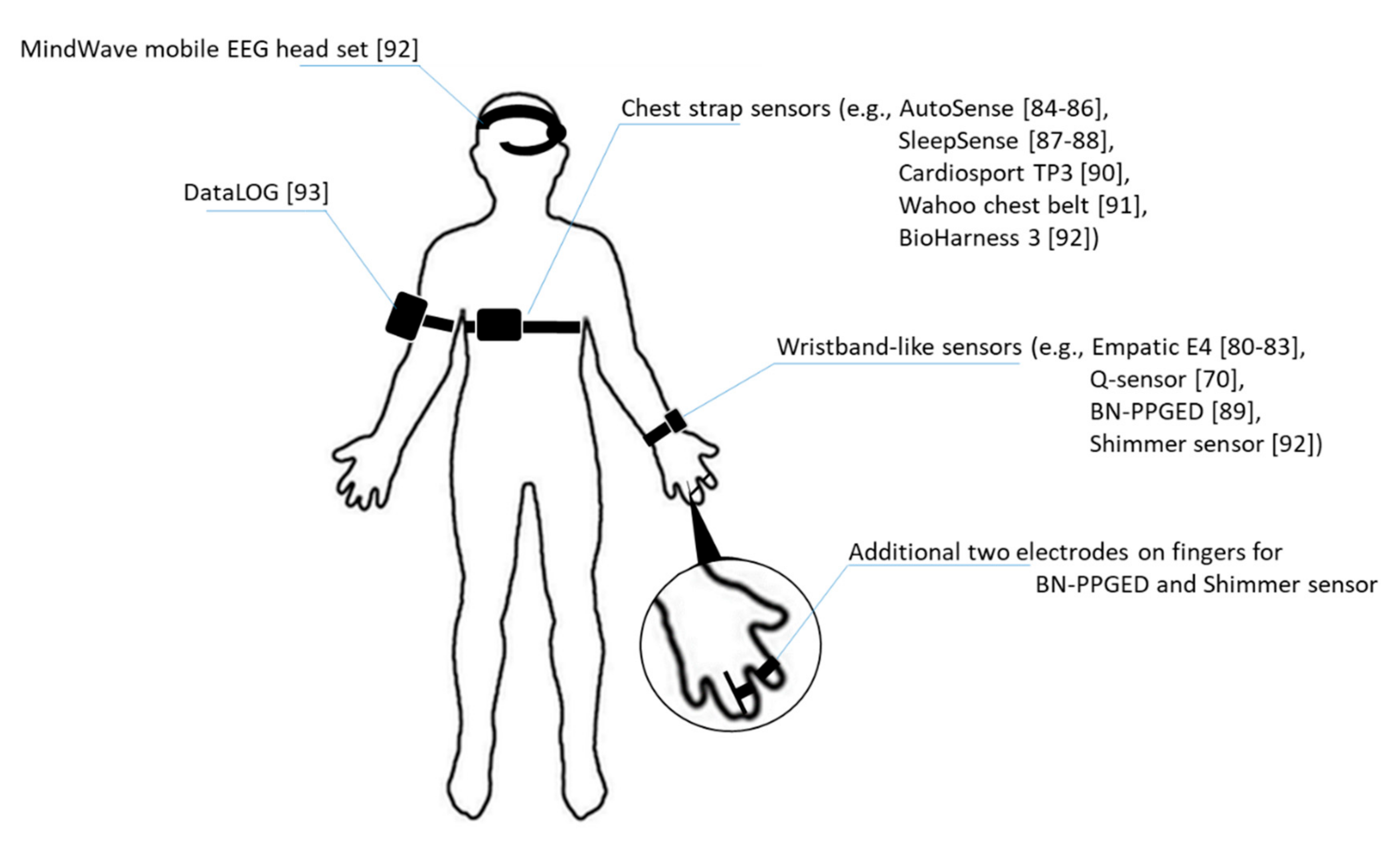
- Empatica E4 wrist band: this device is a wrist band is a real-time physiological data streaming and visualization sensor. As a medical-grade wearable device, it enables researchers to collect multiple physiological data such as BVP for HRV analysis, and EDA that reflects the constantly fluctuating electrical properties of a certain area of skin and peripheral skin temperature. Besides, it also captures motion activity with a 3-axis accelerometer [80,81,82,83].
- AutoSense: this is a wireless sensor suite that packs six sensors in a small form factor which are capable of collecting cardiovascular, respiratory and thermoregularity measurements through radio transmission and processes collected signals for detecting the general stress state of subjects. The wearable sensor has advantages of excessive lifetime while fully charged which allows prolonging its use for constant data collection [84,85,86].
- BN-PPGED: this is a physiological sensor for measuring BVP via optical plethysmographic methods and EDA activity. The sensor could be worn as a wristband with an additional two electrodes situated on two fingers [89].
- Cardiosport TP3: this is also a belt-like wearable sensor. By attaching the sensor pod to the chest strap, the TP3 will be activated to collect HR and millisecond RR intervals as long as the HR is detected [90].
- Q-sensor: this is a wireless sensor designed by the Massachusetts Institute of Technology that aimed to “detect and record physiological signs of stress and excitement by measuring slight electrical changes in the skin.” The emotion detection sensor could benefit individuals with autism who usually do not show his/her stress outward and helping to manifest the emotions before breakdown. The sensor could obtain the accelerometer data and skin conductance by measuring inner wrists of subject’s hand [70].
- Wahoo chest belt: Wahoo chest belt is equipped with a sensor which collects HRV data on a chest belt. Besides provides the heart rate and calorie burn data for workout evaluation, the HRV data could also be an indicator of the autonomic nervous system activity [91].
- BioHarness 3: this is physiological monitoring telemetry device that are usable for subjects in the workplace. The device can store and transmit data such as HR, HRV, respiration rate, and 3-axis accelerometer data through Bluetooth [92].
- Shimmer sensor: the shimmer sensor is a monitoring wearable sensor for EDA. Composed of two finger electrodes and a main unit, the shimmer sensor can transmit data to personal computer or other devices through Bluetooth connections [92].
- MindWave mobile EEG headset: it is an EEG headset capable of logging single channel EEG raw data at a 512 Hz sampling rate then provides index of attention and meditation of the user after power spectral density analysis [92].
- DataLOG: this is a portable EMG signal collection and monitoring devices designed by Biometrics. It could be placed on the arm, the leg or waist for various fields studies like human performance, sports science, medical research, industrial ergonomics, gait laboratories, and educational settings [93].

{kind=link}
| Type of Signal | Commercialized Wearable Sensors Used in Relevant Research | Wearable Sensors Not Yet Commercialized but Used in Relevant Research |
|---|---|---|
| Heart activity | Empatica E4 wrist band, AutoSense, Cardiosport TP3, Wahoo chest belt, BioHarness 3 | |
| Brain activity | MindWave mobile EEG headset | Device 1, Device 2 |
| Muscle activity | DataLOG | Device 3 |
| Electrodermal activity | Empatica E4 wrist band, BN-PPGED, Q-sensor, Shimmer sensor | |
| Respiratory | AutoSense, SleepSense | |
| Blood volume pulse/pulse plethysmograph | Empatica E4 wrist band, BN-PPGED | |
| Body/skin temperature | Empatica E4 wrist band, AutoSense | |
| Three-axis accelerometer data | Empatica E4 wrist band, Q-sensor |

8. Wearable Sensors in Healthcare
9. Discussion
10. Conclusions
Funding
Conflicts of Interest
References
- Beecher, H.K. The measurement of pain. Pharmacol. Rev. 1957, 9, 59–209. [Google Scholar] [PubMed]
- Jin, H.; Ma, X.; Liu, Y.; Yin, X.; Zhu, J.; Wang, Z.; Fan, W.; Jin, Y.; Pu, J.; Zhao, J.; et al. Back Pain-Inducing Test, a Novel and Sensitive Screening Test for Painful Osteoporotic Vertebral Fractures: A Prospective Clinical Study. J. Bone Miner. Res. 2019, 35, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Karcioglu, O.; Topacoglu, H.; Dikme, O.; Dikme, O. A systematic review of the pain scales in adults: Which to use? Am. J. Emerg. Med. 2018, 36, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Panure, T.; Sonawani, S. Stress Detection Using Smartphone and Wearable Devices: A Review. Asian J. Converg. Technol. 2019, 5, 1–4. [Google Scholar] [CrossRef]
- Marchand, S. The Physiology of Pain Mechanisms: From the Periphery to the Brain. Rheum. Dis. Clin. North Am. 2008, 34, 285–309. [Google Scholar] [CrossRef]
- Sasaki, H.; Kishimoto, S. Diagnostic strategy for diabetic polyneuropathy: Focus on nerve fiber type and magnetic resonance neurography. J. Diabetes Ingestig. 2020. [Google Scholar] [CrossRef]
- Sadashivaiah, V.; Sacré, P.; Guan, Y.; Anderson, W.S.; Sarma, S.V. Selective relay of afferent sensory-induced action poten-tials from peripheral nerve to brain and the effects of electrical stimulation. In Proceedings of the 40th Annual International Conference of the IEEE EMBC, Honolulu, Hl, USA, 18–21 July 2018. [Google Scholar]
- Melzack, R.; Wall, P.D. Pain mechanism: A new theory. Science 1965, 150, 971–979. [Google Scholar] [CrossRef]
- Raffa, R.B.; Ossipov, M.H.; Porreca, F. Opiod analesicas and antagonists. In Pharmacology and Therapeutics for Dentistry, 7th ed.; Mosby: St. Louis, MI, USA, 2017; pp. 241–256. [Google Scholar]
- Krabbenbos, I.P.; van Dongen, E.P.A.; Nijhuis, H.J.A.; Liem, A.L. Mechanisms of Spinal cord Stimulation in Neuropathic Pain; IntechOpen: London, UK, 2012. [Google Scholar]
- Keefe, F.J.; Lumley, M.; Anderson, T.; Lynch, T.; Carson, K.L. Pain and emotion: New research directions. J. Clin. Psychol. 2001, 57, 587–607. [Google Scholar] [CrossRef]
- Loggia, M.L.; Schweinhardt, P.; Villemure, C.; Bushnell, M.C. Effects of psychological state on pain perception in the dental environment. J. Canadian Dent. Assoc. 2008, 74, 651–656. [Google Scholar]
- Williams, D.A.; Robinson, M.E.; Geisser, M.E. Pain beliefs: Assessment and utility. Pain 1994, 59, 71–78. [Google Scholar] [CrossRef] [Green Version]
- Nakagami, Y.; Sugihara, G.; Takei, N.; Fujii, T.; Hashimoto, M.; Murakami, K.; Furu, M.; Moritoshi, F.; Uda, M.; Torii, M.; et al. Effect of Physical State on Pain Mediated Through Emotional Health in Rheumatoid Arthritis. Arthritis Rheum. 2019, 71, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- Arnold, L.M.; Clauw, D. Challenges of implementing fibromyalgia treatment guidelines in current clinical practice. Postgrad. Med. 2017, 129, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Thienhaus, O.; Cole, B.E. The classification of pain. In Pain Management a Practical Guide for Clinicians; Weiner, R.S., Ed.; CRC Press LLC: London, UK, 2002. [Google Scholar]
- Shraim, M.A.; Massé-Alarie, H.; Hall, L.M.; Hodges, P.W. Systematic review and synthesis of mechanism-based classifica-tion systems for pain experienced in the musculoskeletal system. Clin. J. Pain 2020, 36, 793–812. [Google Scholar] [CrossRef]
- Jensen, T.S.; Baron, R.; Haanpää, M.; Kalso, E.; Loeer, J.D.; Rice, A.S.C.; Treede, R.D. A new definition of neuropathic pain. Pain 2011, 152, 2204–2205. [Google Scholar] [CrossRef] [PubMed]
- Kosek, E.; Cohen, M.; Baron, R.; Gebhart, G.F.; Mico, J.-A.; Rice, A.S.; Rief, W.; Sluka, A.K. Do we need a third mechanistic descriptor for chronic pain states? Pain 2016, 157, 1382–1386. [Google Scholar] [CrossRef]
- Trouvin, A.-P.; Perrot, S. New concepts of pain. Best Pr. Res. Clin. Rheumatol. 2019, 33, 101415. [Google Scholar] [CrossRef]
- Aydede, M.; Shriver, A. Recently introduced definition of “nociplastic pain” by the International Association for the Study of Pain needs better formulation. Pain 2018, 159, 1176–1177. [Google Scholar] [CrossRef]
- Grichnik, K.P.; Ferrante, F.M. The difference between acute and chronic pain. Mt. Sinai J. Med. A J. Transl. Pers. Med. 1991, 58, 217–220. [Google Scholar]
- Auvenshine, R.C. Acute vs. chronic pain. Tex. Dent. J. 2000, 117, 14–20. [Google Scholar]
- Melzack, R. Pain and stress: A new perspective. In Psychosocial Factors in Pain: Critical Perspectives; Gatchel, R.J., Turk, D.C., Eds.; The Guilford Press: New York, NY, USA, 1999; pp. 89–106. [Google Scholar]
- Flor, H.; Turk, D.C.; Birbaumer, N. Assessment of stress-related psychophysiological reactions in chronic back pain patients. J. Consult. Clin. Psychol. 1985, 53, 354–364. [Google Scholar] [CrossRef]
- Kühl, L.K. Effects of Stress Mechanisms on Pain Processing. Ph.D. Thesis, University of Trier, Trier, Germany, September 2010. [Google Scholar]
- Quartana, P.J.; Campbell, C.M.; Edwards, R.R. Pain catastrophizing: A critical review. Expert Rev. Neurother. 2009, 9, 745–758. [Google Scholar] [CrossRef]
- Tsigos, C.; Kyrou, I.; Kassi, E.; Chrousos, G.P. Stress: Endocrine physiology and pathophysiology. In Endotext; MDText: South Dartmouth, MA, USA, 2020. [Google Scholar]
- Guilliams, T.G.; Edwards, L. Chronic Stress and the HPA Axis: Clinical Assessment and Therapeutic Considerations; Point Institute of Nutraceutical Research: Wilmington, NC, USA, 2010; Volume 9. [Google Scholar]
- Dhabhar, F.S. A hassle a day may keep the pathogens away: The fight-or-flight stress response and the augmentation of immune function. Integr. Comp. Biol. 2009, 49, 215–236. [Google Scholar] [CrossRef] [PubMed]
- Dai, S.; Mo, Y.; Wang, Y.; Xiang, B.; Liao, Q.; Zhou, M.; Li, X.; Li, Y.; Xiong, W.; Li, G.; et al. Chronic stress promotes cancer development. Front. Oncol. 2020, 10, 1492. [Google Scholar] [CrossRef] [PubMed]
- Levy, N.; Sturgess, J.; Mills, P. “Pain as the fifth vital sign” and dependence on the “numerical pain scale” is being aban-doned in the US: Why? Br. J. Anaesth. 2018, 120, 435–438. [Google Scholar] [CrossRef] [Green Version]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M.R. Measures of adult pain: Visual analog scale for pain (vas pain), numeric rating scale for pain (nrs pain), mcgill pain questionnaire (mpq), short-form mcgill pain questionnaire (sf-mpq), chronic pain grade scale (cpgs), short form-36 bodily pain scale (sf-36 bps), and measure of intermittent and constant osteoarthritis pain (icoap). Arthritis Rheum. 2011, 63, S240–S252. [Google Scholar] [CrossRef]
- Smeets, R.J.E.M.; Hijdra, H.J.M.; Kester, A.D.M.; Hitters, M.W.G.C.; Knottnerus, J.A. The usability of six physical performance tasks in a rehabilitation population with chronic low back pain. Clin. Rehabil. 2006, 20, 989–997. [Google Scholar] [CrossRef] [PubMed]
- Abbey, J.; Piller, N.; De Bellis, A.; Esterman, A.; Parker, D.; Giles, L.; Lowcay, B. The Abbey pain scale: A 1-minute numerical indicator for people with end-stage dementia. Int. J. Palliat. Nurs. 2004, 10, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Chanques, G.; Tarri, T.; Ride, A.; Prades, A.; De Jong, A.; Carr, J.; Molinari, N.; Jaber, S. Analgesia nociception index for the assessment of pain in critically ill patients: A diagnostic accuracy study. Br. J. Anaesth. 2017, 119, 812–820. [Google Scholar] [CrossRef] [Green Version]
- Morone, N.E.; Weiner, D.K. Pain as the Fifth Vital Sign: Exposing the Vital Need for Pain Education. Clin. Ther. 2013, 35, 1728–1732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lesage, F.-X.; Berjot, S.; Deschamps, F. Clinical stress assessment using a visual analogue scale. Occup. Med. 2012, 62, 600–605. [Google Scholar] [CrossRef] [Green Version]
- Bali, A.; Jaggi, A.S. Clinical experimental stress studies: Methods and assessment. Rev. Neurosci. 2015, 26, 555–579. [Google Scholar] [CrossRef] [PubMed]
- Rose, D.M.; Seidler, A.; Nübling, M.; Latza, U.; Brähler, E.; Klein, E.M.; Wiltink, J.; Michal, M.; Nickels, S.; Wild, P.S.; et al. Associations of fatigue to work-related stress, mental and physical health in an employed community sample. BMC Psychiatry 2017, 17, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirschbaum, C.; Pirke, K.M.; Hellhammer, D.H. The “trier social stress test”—A tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology 1993, 28, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Allen, A.J.; Kennedy, P.J.; Dockray, S.; Cryan, J.F.; Dinan, T.G.; Clarke, G. The Trier Social Stress Test: Principles and practice. Neurobiol. Stress 2017, 6, 113–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, A.R.; Rohwer, W.D., Jr. The stroop color-word test: A review. Acta Psychol. 1996, 25, 36–93. [Google Scholar] [CrossRef]
- Poguntke, R.; Wirth, M.; Gradl, S. Same same but different: Exploring the effects of the stroop color word test in virtual reality. Human-computer interaction. In Proceedings of the 17th IFIP TC 13 International Conference, Paphos, Cyprus, 2–6 September 2019; pp. 699–708. [Google Scholar]
- Schwabe, L.; Schächinger, H. Ten years of research with the Socially Evaluated Cold Pressor Test: Data from the past and guidelines for the future. Psychoneuroendocrinology 2018, 92, 155–161. [Google Scholar] [CrossRef]
- McRae, A.L.; Saladin, M.E.; Brady, K.T.; Upadhyaya, H.; Back, S.E.; Timmerman, M.A. Stress reactivity: Biological and subjec-tive responses to the cold pressor and trier social stressors. Hum. Psychopharmacol Clin. Exp. 2006, 21, 377–385. [Google Scholar] [CrossRef]
- Rhudy, M.B.; Dolan, S.K.; Wagner, A.R. A Pilot Study on Monitoring Airline Pilot Stress Levels. AIAA Scitech 2020 Forum 2020. [Google Scholar] [CrossRef]
- Van Bilsen, M.; Patel, H.C.; Bauersachs, J.; Böhm, M.; Borggrefe, M.; Brutsaert, D.; Coats, A.J.; De Boer, R.A.; De Keulenaer, G.W.; Filippatos, G.S.; et al. The autonomic nervous system as a therapeutic target in heart failure: A scientific position statement from the Translational Research Committee of the Heart Failure Association of the European Society of Cardiology. Eur. J. Hear. Fail. 2017, 19, 1361–1378. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.-G.; Cheon, E.-J.; Bai, D.-S.; Lee, Y.H.; Koo, B.-H. Stress and Heart Rate Variability: A Meta-Analysis and Review of the Literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef] [Green Version]
- Hernando, D.; Roca, S.; Sancho, J.; Alesanco, Á.; Bailón, R. Validation of the apple watch for heart rate variability measure-ments during relax and mental stress in healthy subjects. Sensors 2018, 18, 2619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bu, N. Stress evaluation index based on Poincaré plot for wearable health devices. In Proceedings of the 2017 IEEE 19th International Conference on e-Health Networking, Applications and Services (Healthcom), Dalian, China, 12–15 October 2017; pp. 1–6. [Google Scholar]
- Weygandt, M.; Meyer-Arndt, L.; Behrens, J.R.; Wakoning, K.; Bellmann-Strobl, J.; Ritter, K.; Scheel, M.; Brandt, A.U.; Labadie, C.; Hetzer, S.; et al. Stress-induced brain activity, brain atrophy, and clinical disability in multiple sclerosis. Proc. Natl. Acad. Sci. USA 2016, 113, 13444–13449. [Google Scholar] [CrossRef] [Green Version]
- Buzzell, G.A.; Barker, T.V.; Troller-Renfree, S.V.; Bernat, E.M.; Bowers, M.E.; Morales, S.; Bowman, L.C.; Henderson, H.A.; Pine, D.S.; Fox, N.A. Adolescent cognitive control, theta oscillations, and social observation. NeuroImage 2019, 198, 13–30. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.-M.; Chou, S.-L.; Gale, E.N.; McCall, W. Human masticatory muscle activity and jaw position under experimental stress. J. Oral Rehabil. 2002, 29, 44–51. [Google Scholar] [CrossRef] [PubMed]
- George, J.P.; Boone, M.E. Aclinical study of rest position using the kinesiograph and myomonitor. J. Prosthet. Dent. 1979, 41, 456–462. [Google Scholar] [CrossRef]
- Song, X.; Li, H.; Gao, W. MyoMonitor: Evaluating Muscle Fatigue with Commodity Smartphones. Smart Health 2020, 100175. [Google Scholar] [CrossRef]
- Wickramasuriya, D.S.; Qi, C.; Faghih, R.T. A state-space approach for detecting stress from Electrodermal activity. In Proceedings of the 40th Annual Internationa Conference of the IEEE Engineering in Medicine and Biology Society, Honolulu, HI, USA, 18–21 July 2018. [Google Scholar]
- Posada-Quintero, H.F.; Kong, Y.; Nguyen, K.; Tran, C.; Beardslee, L.; Chen, L.; Guo, T.; Cong, X.; Feng, B.; Chon, K.H. Using electrodermal activity to validate multilevel pain stimulation in healthy volunteers evoked by thermal grills. Am. J. Physiol. Integr. Comp. Physiol. 2020, 319, R366–R375. [Google Scholar] [CrossRef]
- Posada-Quintero, H.F.; Chon, K.H. Innovations in Electrodermal Activity Data Collection and Signal Processing: A Systematic Review. Sensors 2020, 20, 479. [Google Scholar] [CrossRef] [Green Version]
- Xie, J.; Wen, W.; Liu, G.; Chen, C.; Zhang, J.; Liu, H. Identifying strong stress and weak stress through blood volume pulse. In Proceedings of the 2016 International Conference on Progress in Informatics and Computing (PIC), Shanghai, China, 23–25 December 2016; pp. 179–182. [Google Scholar]
- Vinkers, C.H.; Penning, R.; Hellhammer, J.; Verster, J.C.; Klaessens, J.H.G.M.; Olivier, B.; Kalkman, C.J. The effect of stress on core and peripheral body temperature in humans. Stress 2013, 16, 520–530. [Google Scholar] [CrossRef]
- Herborn, K.A.; Graves, J.L.; Jerem, P.; Evans, N.P.; Nager, R.G.; McCafferty, D.J.; McKeegan, D.E. Skin temperature reveals the intensity of acute stress. Physiol. Behav. 2015, 152, 225–230. [Google Scholar] [CrossRef] [Green Version]
- Simantiraki, O.; Giannakakis, G.; Pampouchidou, A.; Tsiknakis, M. Stress detection from speech using spectral slope measurements. In Proceedings of the Pervasive Computing Paradigms for Mental Health, FABULOUS 2016, Belgrade, Serbia, 24–26 October 2016; Volume 207. [Google Scholar]
- Zhang, J.; Mei, X.; Liu, H.; Yuan, S.; Qian, T. Detecting Negative Emotional Stress Based on Facial Expression in Real Time. In Proceedings of the 2019 IEEE 4th International Conference on Signal and Image Processing (ICSIP), Wuxi, China, 19–21 July 2019; pp. 430–434. [Google Scholar]
- Orguc, S.; Khurana, H.S.; Stankovic, K.M.; Lee, H.-S.; Chandrakasan, A.P. EMG-based Real Time Facial Gesture Recognition for Stress Monitoring. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; Volume 2018, pp. 2651–2654. [Google Scholar]
- Lau, S.H. Stress Detection for Keystroke Dynamics. Ph.D. Thesis, Carnegie Mellon University, Pittsburgh, PA, USA, May 2018. [Google Scholar]
- Carneiro, D.; Novais, P.; Sousa, N.; Pêgo, J.M.; Neves, J. Mouse dynamics correlates to student behavior in computer-based exams. Logic J. IGPL 2017, 25, 967–978. [Google Scholar] [CrossRef]
- Aigrain, J.; Dubuisson, S.; Detyniecki, M.; Chetouani, M. Person-specific behavioral features for automatic stress detection. In Proceedings of the 11th IEEE International Conference and Workshops on Automatic Face and Gesture Recognition, Ljubljana, Slovenia, 4–8 May 2015. [Google Scholar]
- Gao, T.; Li, J.; Zhang, H.; Gao, J.; Kong, Y.; Hu, Y.; Mei, S. The influence of alexithymia on mobile phone addiction: The role of depression, anxiety and stress. J. Affect. Disord. 2018, 225, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Sano, A.; Picard, R.W. Stress Recognition Using Wearable Sensors and Mobile Phones. In Proceedings of the 2013 Humaine Association Conference on Affective Computing and Intelligent Interaction, Geneva, Switzerland, 2–5 September 2013; pp. 671–676. [Google Scholar]
- Jeanne, M.; Clément, C.; De Jonckheere, J.; Logier, R.; Tavernier, B. Variations of the analgesia nociception index during general anaesthesia for laparoscopic abdominal surgery. J. Clin. Monit. 2012, 26, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Can, Y.S.; Arnrich, B.; Ersoy, C. Stress detection in daily life scenarios using smart phones and wearable sensors: A survey. J. Biomed. Informatics 2019, 92, 103139. [Google Scholar] [CrossRef] [PubMed]
- Abdullayev, R.; Uludağ, Ö.; Celik, B. Analgesia Nociception Index: Assessment of acute postoperative pain. Braz. J. Anesthesiol. (English Ed.) 2019, 69, 396–402. [Google Scholar] [CrossRef]
- Le Guen, M.; Jeanne, M.; Siever, K.; Al Moubarik, M.; Chazot, T.; Laloë, P.A.; Dreyfus, J.F.; Fischler, M. The analgesia nociception index: A pilot study to evaluation of a new pain parameter during labor. Int. J. Obstet. Anesth. 2012, 21, 146–151. [Google Scholar] [CrossRef]
- Abdullayev, R.; Yildirim, E.; Celik, B.; Sarica, L.T. Analgesia nociception index: Hear rate variability analysis of emotional status. Cureus 2019, 11, e4365. [Google Scholar] [CrossRef] [Green Version]
- Huiku, M.; Uutela, K.; Van Gils, M.; Korhonen, I.; Kymäläinen, M.; Meriläinen, P.; Paloheimo, M.; Rantanen, M.; Takala, P.; Viertiö-Oja, H.; et al. Assessment of surgical stress during general anaesthesia. Br. J. Anaesth. 2007, 98, 447–455. [Google Scholar] [CrossRef] [Green Version]
- Thee, C.; Ilies, C.; Gruenewald, M.; Kleinschmidt, A.; Steinfath, M.; Bein, B. Reliability of the surgical Pleth index for assessment of postoperative pain. Eur. J. Anaesthesiol. 2015, 32, 44–48. [Google Scholar] [CrossRef]
- Ledowski, T.; Schneider, M.; Gruenewald, M.; Goyal, R.; Teo, S.; Hruby, J. Surgical pleth index: Prospective validation of the score to predict moderate-to-severe postoperative pain. Br. J. Anaesth. 2019, 123, e328–e332. [Google Scholar] [CrossRef] [Green Version]
- Sağbaş, E.A.; Korukoglu, S.; Ballı, S. Stress Detection via Keyboard Typing Behaviors by Using Smartphone Sensors and Machine Learning Techniques. J. Med. Syst. 2020, 44, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ollander, S.; Godin, C.; Campagne, A.; Charbonnier, S. A Comparison of Wearable and Stationary Sensors for Stress Detection. In Proceedings of the 2016 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Budapest, Hungary, 9–12 October 2016; pp. 4362–4366. [Google Scholar]
- Indikawati, F.I.; Winiarti, S. Stress Detection from Multimodal Wearable Sensor Data. In Proceedings of the 2nd International Conference on Engineering and Applied Sciences (2nd InCEAS), Yogyakarta, Indonesia, 16 November 2019; Volume 771. [Google Scholar]
- Carreiro, S.; Chintha, K.K.; Shrestha, S.; Chapman, B.; Smelson, D.; Indic, P. Wearable sensor-based detection of stress and craving in patients during treatment for substance use disorder: A mixed methods pilot study. Drug Alcohol Depend. 2020, 209, 107929. [Google Scholar] [CrossRef] [PubMed]
- Kaczor, E.; Carreiro, S.; Stapp, J.; Chapman, B.; Indic, P. Objective Measurement of Physician Stress in the Emergency Department Using a Wearable Sensor. In Proceedings of the 53rd Hawaii International Conference on System Sciences, Honolulu, HI, USA, 7–10 January 2020; pp. 3729–3738. [Google Scholar] [CrossRef] [Green Version]
- Ertin, E.; Raij, A.; Stohs, N.; Al’Absi, M.; Kumar, S.; Mitra, S. An unobtrusively wearable sensor suite for inferring the onset, causality, and consequences of stress in the field. In Proceedings of the 9th ACM Conference on Recommender Systems, Seattle, WA, USA, 1–4 November 2011; pp. 437–438. [Google Scholar]
- Kennedy, A.P.; Epstein, D.H.; Jobes, M.L.; Agage, D.; Tyburski, M.; Phillips, K.A.; Ali, A.A.; Bari, R.; Hossain, S.M.; Hovsepian, K.; et al. Continuous in-the-field measurement of heart rate: Correlates of drug use, craving, stress, and mood in polydrug users. Drug Alcohol Depend. 2015, 151, 159–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakajima, M.; Lemieux, A.M.; Fiecas, M.; Chatterjee, S.; Sarker, H.; Saleheen, N.; Ertin, E.; Kumar, S.; Al’Absi, M. Using novel mobile sensors to assess stress and smoking lapse. Int. J. Psychophysiol. 2020, 158, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Wijsman, J.; Grundlehner, B.; Liu, H.; Hermens, H.J.; Penders, J. Towards mental stress detection using wearable physiological sensors. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 1798–1801. [Google Scholar] [CrossRef]
- Mühl1, C.; Jeunet, C.; Lotte, F. EEG-based workload estimation across affective contexts. Front. Neurosci. 2014, 8, 114. [Google Scholar]
- Sandulescu, V.; Andrews, S.; Ellis, D.A.; Bellotto, N.; Mozos, O.M. Stress Detection Using Wearable Physiological Sensors. Proceedings of International Work-Conference on the Interplay Between Natural and Artificial Computation, IWINAC 2015, Elche, Spain, 1–5 June 2015; pp. 526–532. [Google Scholar]
- Salai, M.; Vassányi, I.; Kósa, I. Stress Detection Using Low Cost Heart Rate Sensors. J. Health Eng. 2016, 2016, 1–13. [Google Scholar] [CrossRef]
- Muaremi, A.; Arnrich, B.; Tröster, G. Towards Measuring Stress with Smartphones and Wearable Devices During Workday and Sleep. BioNanoScience 2013, 3, 172–183. [Google Scholar] [CrossRef] [Green Version]
- Betti, S.; Lova, R.M.; Rovini, E.; Acerbi, G.; Santarelli, L.; Cabiati, M.; Del Ry, S.; Cavallo, F. Evaluation of an Integrated System of Wearable Physiological Sensors for Stress Monitoring in Working Environments by Using Biological Markers. IEEE Trans. Biomed. Eng. 2018, 65, 1748–1758. [Google Scholar] [CrossRef]
- Pourmohammadi, S.; Maleki, A. Stress detection using ECG and EMG signals: A comprehensive study. Comput. Methods Programs Biomed. 2020, 193, 105482. [Google Scholar] [CrossRef]
- Hu, B.; Peng, H.; Zhao, Q.; Hu, B.; Majoe, D.; Zheng, F.; Moore, P. Signal Quality Assessment Model for Wearable EEG Sensor on Prediction of Mental Stress. IEEE Trans. NanoBioscience 2015, 14, 553–561. [Google Scholar] [CrossRef]
- Ahn, J.W.; Ku, Y.; Kim, H.C. A Novel Wearable EEG and ECG Recording System for Stress Assessment. Sensors 2019, 19, 1991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijsman, J.; Grundlehner, B.; Penders, J.; Hermens, H.J. Trapezius muscle EMG as predictor of mental stress. ACM Trans. Embed. Comput. Syst. 2013, 12, 1–20. [Google Scholar] [CrossRef]
- Quer, G.; Radin, J.M.; Gadaleta, M.; Baca-Motes, K.; Ariniello, L.; Ramos, E.; Kheterpal, V.; Topol, E.J.; Steinhubl, S.R. Wearable sensor data and self-reported symptoms for COVID-19 detection. Nat. Med. 2021, 27, 73–77. [Google Scholar] [CrossRef]
- Pantelopoulos, A.; Bourbakis, N.G. A Survey on Wearable Sensor-Based Systems for Health Monitoring and Prognosis. IEEE Trans. Syst. Man, Cybern. Part C (Applications Rev.) 2010, 40, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Hao, Y.; Foster, R. Wireless body sensor networks for health-monitoring applications. Physiol. Meas. 2008, 29, R27–R56. [Google Scholar] [CrossRef]
- Bonato, P. Advances in wearable technology and applications in physical medicine and rehabilitation. J. Neuroeng. Rehabil. 2005, 2, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Abbod, M.F.; Shieh, J.-S. Integrations between Autonomous Systems and Modern Computing Techniques: A Mini Review. Sensors 2019, 19, 3897. [Google Scholar] [CrossRef] [Green Version]
- Brennan, F.; Carr, D.B.; Cousins, M. Pain Management: A Fundamental Human Right. Anesth. Analg. 2007, 105, 205–221. [Google Scholar] [CrossRef] [Green Version]
- Brennan, F.; Carr, D.; Cousins, M. Access to Pain Management—Still Very Much a Human Right. Pain Med. 2016, 17, 1785–1789. [Google Scholar] [CrossRef]
- Noroozian, M.; Raeesi, S.; Hashemi, R.; Khedmat, L.; Vahabi, Z. Pain: The neglect issue in old people’s life. J. Med. Sci. 2018, 6, 1773–1778. [Google Scholar] [CrossRef] [Green Version]
- Gulzhaina, K.K.; Aigerim, K.N. Stress management techniques for students. Advances in social Science, Education and Humanities Research. In Proceedings of the International Conference on the Theory and Practice of Personality Formation in Modern Society (ICTPPFMS 2018), Yurga, Russia, 20–22 September 2018; Volume 198, pp. 47–56. [Google Scholar]
- Petković, A.I.; Nikolić, V. Educational needs of employees in work-related stress management. Work 2020, 65, 661–669. [Google Scholar] [CrossRef] [PubMed]
| A-alpha | A-beta | A-delta | C | |
|---|---|---|---|---|
| Myelinated/unmyelinated | Myelinated | Myelinated | Myelinated | Unmyelinated |
| Size (diameter) | 13–20 μm | 6–13 μm | 1–5 μm | 0.2–1.5 μm |
| Speed of signal transmission in meter per second | 80–120 m/s | 35–75 m/s | 5–35 m/s | 0.5–2.0 m/s |
| Related perception | Position and spatial awareness | touching | Sharp pain and temperatures sensation | Dull pain temperatures and itches |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.; Abbod, M.; Shieh, J.-S. Pain and Stress Detection Using Wearable Sensors and Devices—A Review. Sensors 2021, 21, 1030. https://doi.org/10.3390/s21041030
Chen J, Abbod M, Shieh J-S. Pain and Stress Detection Using Wearable Sensors and Devices—A Review. Sensors. 2021; 21(4):1030. https://doi.org/10.3390/s21041030
Chicago/Turabian StyleChen, Jerry, Maysam Abbod, and Jiann-Shing Shieh. 2021. "Pain and Stress Detection Using Wearable Sensors and Devices—A Review" Sensors 21, no. 4: 1030. https://doi.org/10.3390/s21041030
APA StyleChen, J., Abbod, M., & Shieh, J. -S. (2021). Pain and Stress Detection Using Wearable Sensors and Devices—A Review. Sensors, 21(4), 1030. https://doi.org/10.3390/s21041030