
Discrimination of the Cognitive Function of Community Subjects Using the Arterial Pulse Spectrum and Machine-Learning Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
4.1. Differences in the Spectral Indices of the Pulse Waveform
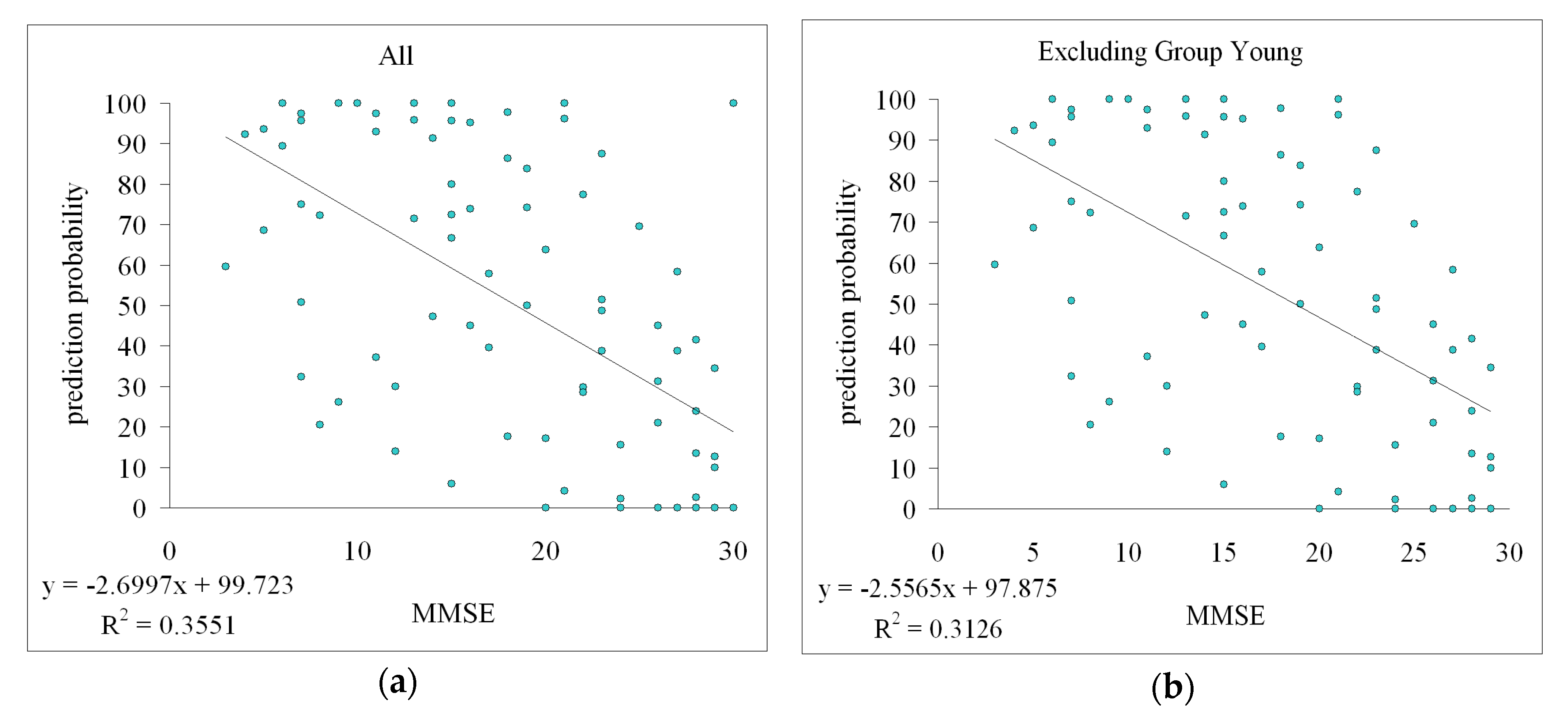
4.2. Correlation between Prediction Probability and MMSE Score
5. Conclusions
- ∎
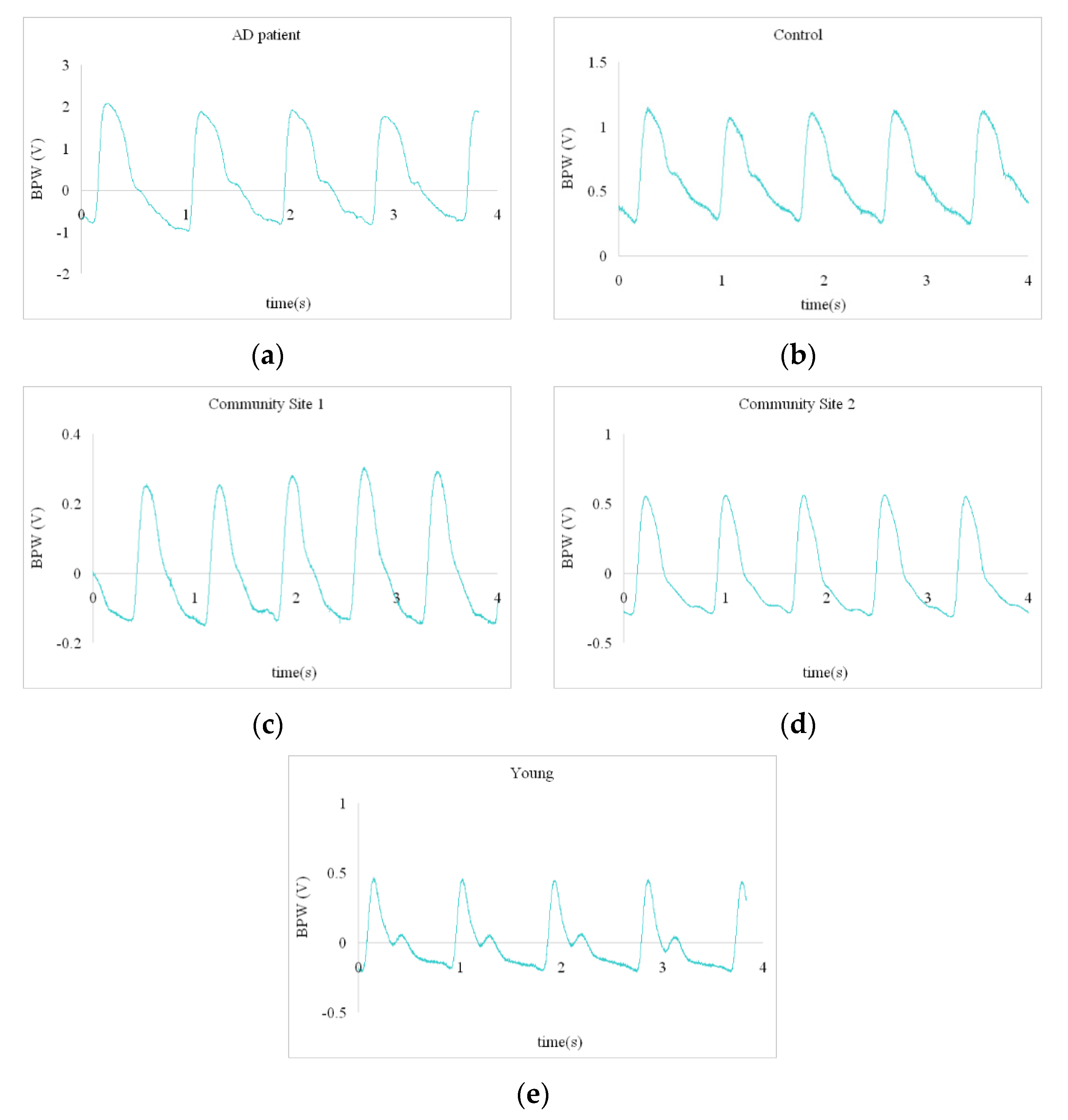
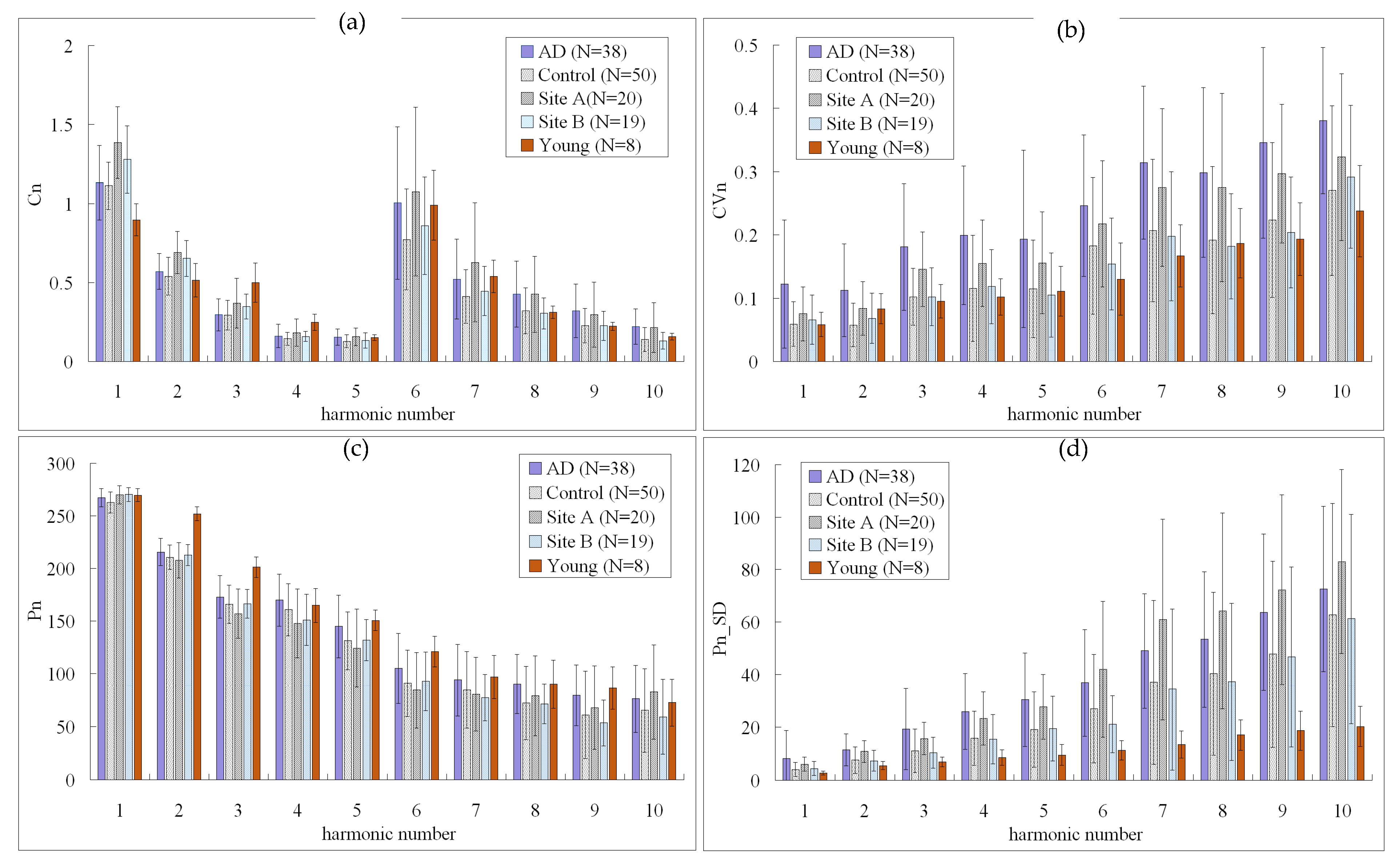
- Significant differences in spectral indices of the BPW were found between the AD patients and control subjects.
- ∎
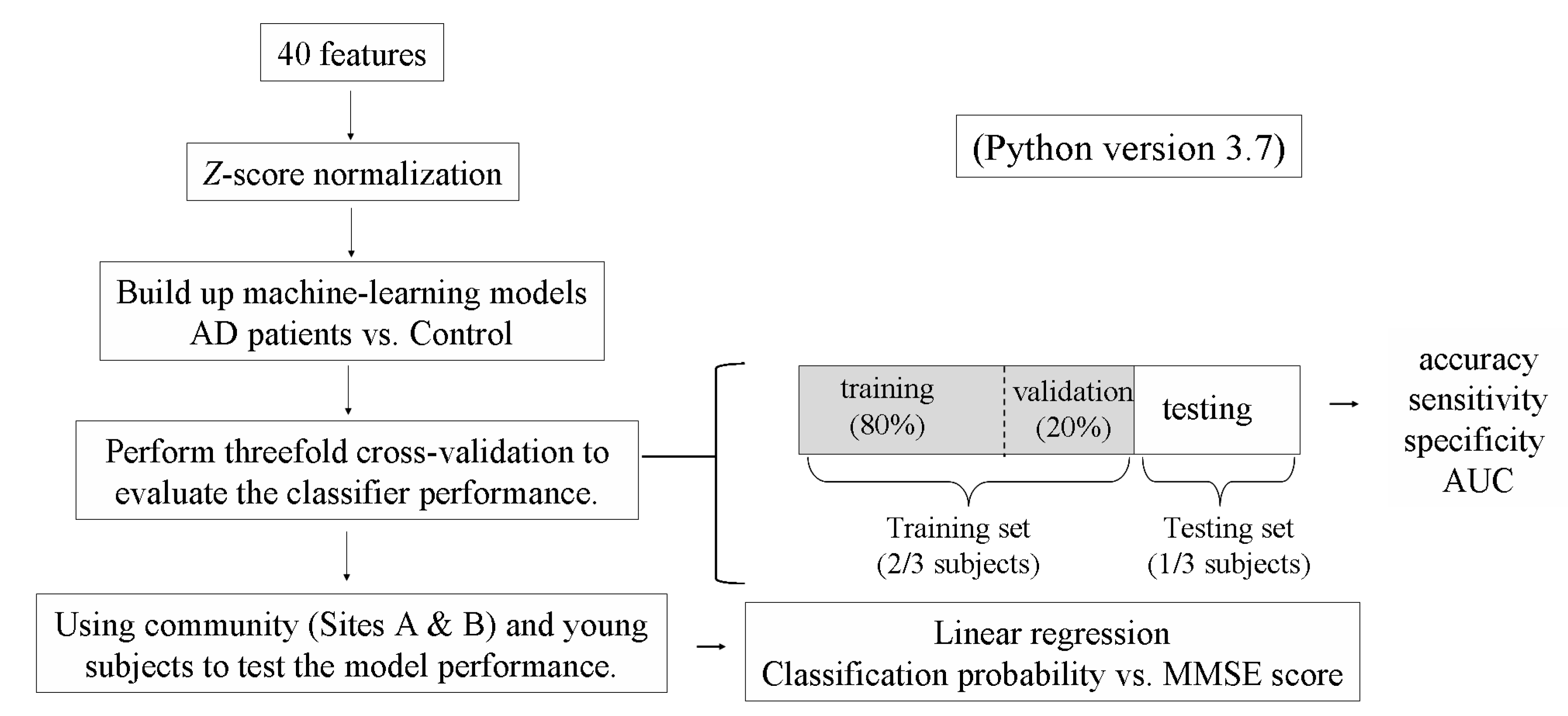
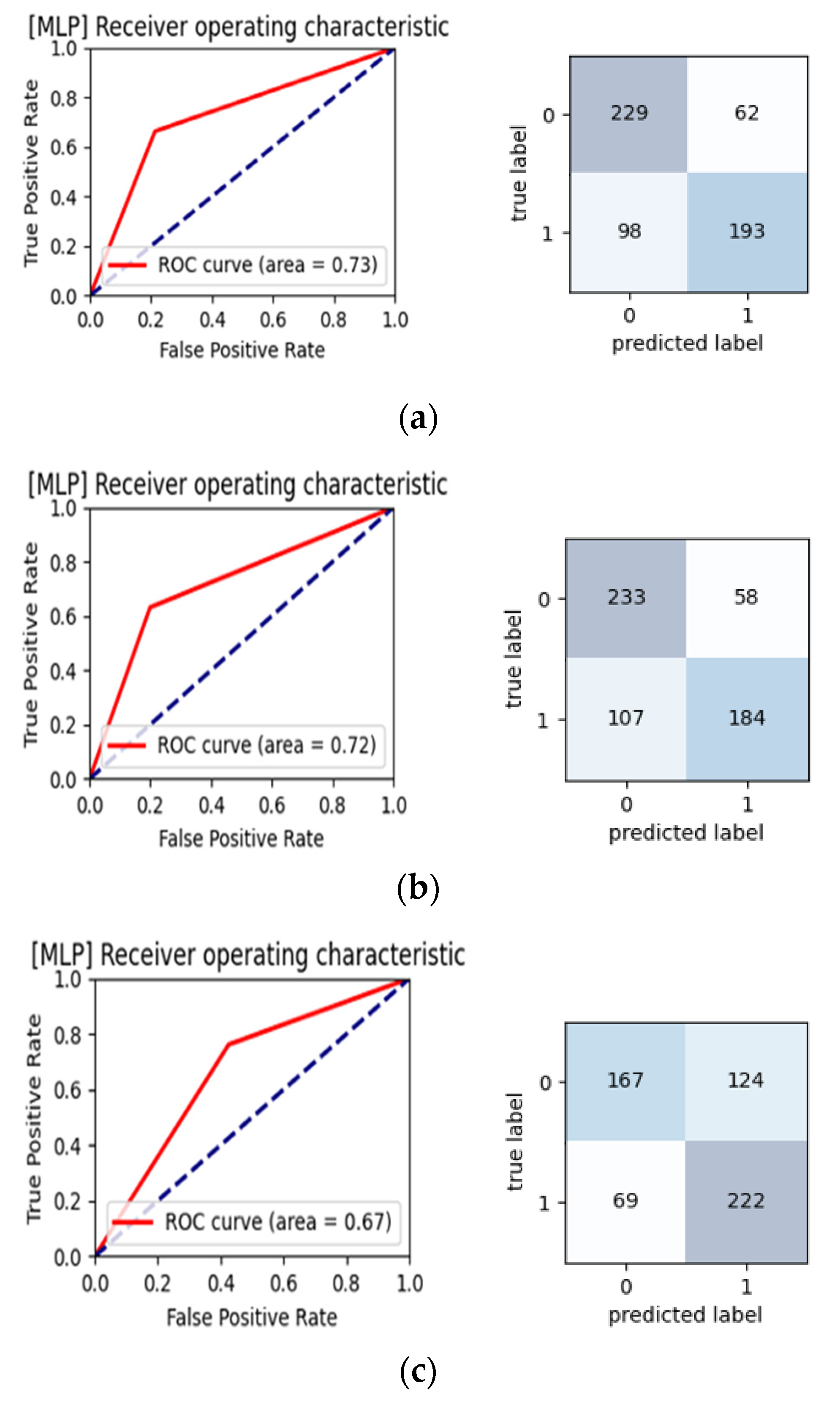
- The threefold cross-validation results indicated an AUC of 0.70 in the threefold cross-validation when using MLP, which indicated acceptable discrimination performance.
- ∎
- Using AD patients and control subjects as training data, a significant correlation was found between the prediction probability of the test data (comprising community subjects at two sites and young subjects) and the MMSE score. Although significant, the correlation in Figure 5 was modestly correlated. Further collection of subject data in future work is necessary to strengthen the present conjecture.
- ∎
- Age did not markedly interfere with the identified correlation between the prediction probability and the MMSE score.
- ∎
- The present findings based on pulse waveform measurements and machine-learning analysis may be meaningful for the development of a noninvasive, rapid, and objective method for monitoring the cognitive condition.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Creavin, S.T.; Wisniewski, S.; Noel-Storr, A.H.; Trevelyan, C.M.; Hampton, T.; Rayment, D.; Thom, V.M.; Nash, K.J.; Elhamoui, H.; Milligan, R.; et al. Mini-Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Cochrane Database Syst. Rev. 2016, 13, CD011145. [Google Scholar] [CrossRef] [Green Version]
- Patnode, C.D.; Perdue, L.A.; Rossom, R.C.; Rushkin, M.C.; Redmond, N.; Thomas, R.G.; Lin, J.S. Screening for Cognitive Impairment in Older Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2020, 323, 764–785. [Google Scholar] [CrossRef]
- Dequanter, S.; Buyl, R.; Fobelets, M. Quality indicators for community dementia care: A systematic review. Eur. J. Public Health 2020, 30, 879–885. [Google Scholar] [CrossRef]
- Iadecola, C.; Gottesman, R.F. Cerebrovascular alterations in Alzheimer disease: Incidental or pathogenic? Circ. Res. 2018, 123, 406–408. [Google Scholar] [CrossRef] [PubMed]
- Cortes-Canteli, M.; Iadecola, C. Alzheimer’s disease and vascular aging: JACC Focus Seminar. J. Am. Coll. Cardiol. 2020, 75, 942–951. [Google Scholar] [CrossRef] [PubMed]
- Kuller, L.H.; Lopez, O.L.; Mackey, R.H.; Rosano, C.; Edmundowicz, D.; Becker, J.T.; Newman, A.B. Subclinical cardiovascular disease and death, dementia, and coronary heart disease in patients 80+ years. J. Am. Coll. Cardiol. 2016, 67, 1013–1022. [Google Scholar] [CrossRef]
- O’Rourke, M.F.; Adji, A.; Safar, M.E. Structure and Function of Systemic Arteries: Reflections on the Arterial Pulse. Am. J. Hypertens. 2018, 31, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, I.B.; Cockcroft, J.R.; Webb, D.J. Pulse wave analysis and arterial stiffness. J. Cardiovasc. Pharmacol. 1998, 32 (Suppl. 3), S33–S37. [Google Scholar]
- Oh, Y.S. Arterial stiffness and hypertension. Clin. Hypertens. 2018, 24, 17. [Google Scholar] [CrossRef] [PubMed]
- Hsiu, H.; Liu, J.C.; Yang, C.J.; Chen, H.S.; Wu, M.S.; Hao, W.R.; Lee, K.Y.; Hu, C.J.; Wang, Y.H.; Fang, Y.A. Discrimination of vascular aging using the arterial pulse spectrum and machine-learning analysis. Microvasc. Res. 2021, 139, 104240. [Google Scholar] [CrossRef]
- Lin, S.K.; Hsiu, H.; Chen, H.S.; Yang, C.J. Classification of patients with Alzheimer’s disease using the arterial pulse spectrum and a multilayer-perceptron analysis. Sci. Rep. 2021, 11, 8882. [Google Scholar] [CrossRef]
- Husmann, M.; Jacomella, V.; Thalhammer, C.; Amann-Vesti, B.R. Markers of arterial stiffness in peripheral arterial disease. Vasa 2015, 44, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, I.S.; Wilkinson, I.B.; Cockcroft, J.R. Assessment of arterial stiffness in clinical practice. QJM 2002, 95, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Liao, J.; Farmer, J. Arterial stiffness as a risk factor for coronary artery disease. Curr. Atheroscler Rep. 2014, 16, 387. [Google Scholar] [CrossRef]
- Lin, F.C.; Hsiu, H.; Chiu, H.S.; Chen, C.T.; Hsu, C.H. Characteristics of pulse-waveform and laser-Doppler indices in frozen-shoulder patients. Biomed. Signal Process. Control 2020, 56, 101718. [Google Scholar] [CrossRef]
- Chen, C.T.; Hsiu, H.; Hung, S.H.; Chen, G.Z.; Huang, Y.L. Characteristics of spectral indexes of the blood pressure waveform in patients with breast cancer. Blood Press. Monit. 2017, 22, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.W.; Hsiu, H.; Yang, S.H.; Fang, W.H.; Tsai, H.C. Characteristics of beat-to-beat photoplethysmography waveform indexes in subjects with metabolic syndrome. Microvasc. Res. 2016, 106, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.L.; Hsiu, H.; Hsu, W.C.; Chen, C.Y. Characteristics of harmonic indexes of the arterial blood pressure waveform in polycystic ovary syndrome. Blood Press Monit. 2014, 19, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.T.; Ting, C.T.; Chen, C.Y.; Lyu, Z.J.; Chen, C.C.; Chou, Y.S.; Cheng, C.F.; Hsu, C.H.; Hsiu, H. Pulse-waveform and laser-Doppler indices for identifying colorectal-cancer patients. Biom. Eng. Appl. Basis Comm. 2020, 33, 2150005. [Google Scholar] [CrossRef]
- Sorelli, M.; Perrella, A.; Bocchi, L. Detecting vascular age using the analysis of peripheral pulse. IEEE Trans. Biomed. Eng. 2018, 65, 2742–2750. [Google Scholar] [CrossRef]
- Stergiou, G.S.; Ntineri, A.; Kollias, A.; Ohkubo, T.; Imai, Y.; Parati, G. Blood pressure variability assessed by home measurements: A systematic review. Hypertens. Res. 2014, 37, 565–572. [Google Scholar] [CrossRef]
- Lam, L.C.; Tam, C.W.; Lui, V.W.; Chan, W.C.; Chan, S.S.; Wong, S.; Wong, A.; Tham, M.K.; Ho, K.S.; Chan, W.M.; et al. Prevalence of very mild and mild dementia in community-dwelling older Chinese people in Hong Kong. Int. Psychogeriatr. 2008, 20, 135–148. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, D. Cochrane Review Summary: Mini-Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Prim. Health Care Res. Dev. 2017, 18, 527–528. [Google Scholar] [CrossRef] [Green Version]
- Ahamed, F.; Shahrestani, S.; Cheung, H. Internet of Things and Machine Learning for Healthy Ageing: Identifying the Early Signs of Dementia. Sensors 2020, 20, 6031. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Lau, K.K.; Wong, G.H.Y.; Chan, W.C.; Mak, H.K.F.; Zhang, Q.; Knapp, M.; Wong, I.C.K. Predicting dementia diagnosis from cognitive footprints in electronic health records: A case-control study protocol. BMJ Open 2020, 10, e043487. [Google Scholar] [CrossRef] [PubMed]
- Yim, D.; Yeo, T.Y.; Park, M.H. Mild cognitive impairment, dementia, and cognitive dysfunction screening using machine learning. J. Int. Med. Res. 2020, 48, 300060520936881. [Google Scholar] [CrossRef]
- Faconti, L.; Bruno, R.M.; Ghiadoni, L.; Taddei, S.; Virdis, A. Ventricular and vascular stiffening in aging and hypertension. Curr. Hypertens. Rev. 2015, 11, 100–109. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Machine-Learning Methods | Model Parameters |
|---|---|
| SVM (support vector machine) | C = 1; kernel: rbf; gamma: auto; tol = 0.0001; max_iter = −1; class_weight: none |
| MLP (multilayer perception) | hidden_layer_sizes = 100; solver: adam; alpha = 0.0001; batch_size: auto; max_iter = 200; learning_rate_int = 0.001 |
| GNB (Gaussian Naive Bayes) | Priors: none |
| DT (decision tree) | Criterion: gini; Splitter: best; max_depth: none; min_samples_split = 2; min_samples_leaf = 1; min_weight_fraction_leaf = 0; max_features: none; max_leaf_nodes: none; min_impurity_split = 0.0 |
| RF (random forest) | n_estimators = 100; criterion: gini; max_depth: none; min_samples_split = 2; min_samples_leaf = 1; min_weight_fraction_leaf = 0; max_features: none; max_leaf_nodes: none |
| LR (logistic regression) | Penalty: l2; Solver: lbfgs; multi_class: auto; class_weight: none |
| LDA (linear discriminant analysis) | Solver: svd; Shrinkage: none; Priors: none |
| KNN (K-nearest neighbor classification) | n_neighbors = 5; weights: uniform; algorithm: auto; n_jobs: none; p: none |
| AD patients | ||||||
| Mild dementia 16 < MMSE < 24 | Moderate dementia 10 < MMSE ≤ 16 | Heavy dementia MMSE ≤ 10 | ||||
| gender | male | female | male | female | male | female |
| Subject number | 4 | 6 | 5 | 7 | 6 | 10 |
| subject number (male + female) | 10 | 12 | 16 | |||
| Total subject number | 38 | |||||
| Age | 71.33 ± 6.5 | 73.86 ± 7.86 | 67 ± 19 | 77.42 ± 11.51 | 74.33 ± 9.29 | 77.4 ± 7.02 |
| Age(male + female) | 73.1 ± 7.21 | 73.08 ± 15.27 | 76.25 ± 7.79 | |||
| Age (all) | 74.42 ± 10.44 | |||||
| HR | 68 ± 11.53 | 70.14 ± 11.86 | 67 ± 3.53 | 67.85 ± 16.24 | 66.4 ± 13.92 | 67.6 ± 9.64 |
| HR (male + female) | 69.5 ± 11.57 | 67.5 ± 12.19 | 68.87 ± 11.1 | |||
| HR (all) | 68.8 ± 11.18 | |||||
| Community Site A (Taipei Veterans Home) | ||||||
| MMSE > 24 | Mild dementia 16 < MMSE < 24 | Moderate dementia 10 < MMSE ≤ 16 | ||||
| gender | male | female | male | female | male | female |
| Subject number | 8 | 0 | 7 | 0 | 5 | 0 |
| subject number (male + female) | 8 | 7 | 5 | |||
| Total subject number | 20 | |||||
| Age | 81.09 ± 10.31 | 83.43± 9.02 | 77.08 ± 5.36 | 0 | ||
| Age(male + female) | 81 ± 10.31 | 83± 9.02 | 86.4 ± 7.92 | |||
| Age (all) | 83.05 ± 9.10 | |||||
| HR | 67.25 ± 15.26 | 68.29 ± 4.72 | 62.20 ± 5.22 | |||
| HR (male + female) | 67.25 ± 15.26 | 68.29 ± 4.72 | 62.20 ± 5.22 | |||
| HR (all) | 66.35 ± 10.43 | |||||
| Community Site B (Hoping LOHAS Daycare Center) | ||||||
| MMSE > 24 | Mild dementia 16 < MMSE ≤ 24 | Moderate dementia 10 < MMSE ≤ 16 | ||||
| gender | male | female | male | female | male | female |
| Subject number | 2 | 8 | 1 | 6 | 2 | 0 |
| subject number (male + female) | 10 | 7 | 2 | |||
| Total subject number | 19 | |||||
| Age | 71.53 ± 0.71 | 75.64± 6.97 | 76.23 | 81.26 ± 4.51 | 84.46 ± 6.36 | |
| Age(male + female) | 74.3 ± 6.33 | 80.71± 4.61 | 84.46 ± 6.36 | |||
| Age (all) | 78.25 ± 6.88 | |||||
| HR | 79.50 ± 12.02 | 68.38 ± 6.86 | 61.00 | 67.00 ± 8.00 | 65.50 ± 6.36 | |
| HR (male + female) | 70.6 ± 8.64 | 66.14 ± 7.65 | 65.50 ± 6.36 | |||
| HR (all) | 68.42 ± 8.04 | |||||
| Control | Young | |||||
| gender | male | female | male | female | ||
| Subject number | 11 | 27 | 7 | 1 | ||
| Total subject number | 38 | 8 | ||||
| Age | 74.24 ± 3.26 | 72.08 ± 4.94 | 23.85 ± 1.46 | 23 | ||
| Age (all) | 72.71 ± 4.58 | 23.75 ± 1.38 | ||||
| HR | 78.09 ± 9.11 | 79.88 ± 7.27 | 66.00 ± 5.94 | 64.00 | ||
| HR (all) | 79.36 ± 7.76 | 65.75 ± 5.54 | ||||
 |
| Accuracy (%) | SVM | MLP | GNB | DT | RF | LR | LDA | KNN |
| 1 | 70.61 | 72.50 | 61.34 | 63.57 | 64.26 | 71.47 | 76.80 | 64.94 |
| 2 | 56.35 | 71.64 | 55.84 | 64.77 | 69.41 | 62.37 | 71.64 | 62.37 |
| 3 | 60.30 | 66.83 | 60.48 | 59.79 | 63.40 | 62.71 | 56.87 | 63.91 |
| average | 62.42 | 70.32 | 59.22 | 62.71 | 65.69 | 65.52 | 68.44 | 63.74 |
| Sensitivity | SVM | MLP | GNB | DT | RF | LR | LDA | KNN |
| 1 | 0.66 | 0.66 | 0.38 | 0.61 | 0.72 | 0.61 | 0.64 | 0.60 |
| 2 | 0.46 | 0.63 | 0.21 | 0.62 | 0.71 | 0.47 | 0.61 | 0.51 |
| 3 | 0.78 | 0.76 | 0.75 | 0.81 | 0.91 | 0.77 | 0.68 | 0.78 |
| average | 0.63 | 0.68 | 0.45 | 0.68 | 0.78 | 0.62 | 0.64 | 0.63 |
| Specificity | SVM | MLP | GNB | DT | RF | LR | LDA | KNN |
| 1 | 0.74 | 0.78 | 0.84 | 0.65 | 0.56 | 0.81 | 0.89 | 0.69 |
| 2 | 0.66 | 0.80 | 0.90 | 0.66 | 0.67 | 0.77 | 0.81 | 0.73 |
| 3 | 0.41 | 0.57 | 0.45 | 0.37 | 0.35 | 0.48 | 0.45 | 0.49 |
| average | 0.60 | 0.72 | 0.73 | 0.56 | 0.53 | 0.69 | 0.72 | 0.64 |
| AUC | SVM | MLP | GNB | DT | RF | LR | LDA | KNN |
| 1 | 0.70 | 0.72 | 0.61 | 0.63 | 0.64 | 0.71 | 0.76 | 0.64 |
| 2 | 0.56 | 0.71 | 0.55 | 0.64 | 0.69 | 0.62 | 0.71 | 0.62 |
| 3 | 0.60 | 0.66 | 0.60 | 0.59 | 0.63 | 0.62 | 0.56 | 0.63 |
| average | 0.62 | 0.70 | 0.59 | 0.62 | 0.65 | 0.65 | 0.68 | 0.63 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsiu, H.; Lin, S.-K.; Weng, W.-L.; Hung, C.-M.; Chang, C.-K.; Lee, C.-C.; Chen, C.-T. Discrimination of the Cognitive Function of Community Subjects Using the Arterial Pulse Spectrum and Machine-Learning Analysis. Sensors 2022, 22, 806. https://doi.org/10.3390/s22030806
Hsiu H, Lin S-K, Weng W-L, Hung C-M, Chang C-K, Lee C-C, Chen C-T. Discrimination of the Cognitive Function of Community Subjects Using the Arterial Pulse Spectrum and Machine-Learning Analysis. Sensors. 2022; 22(3):806. https://doi.org/10.3390/s22030806
Chicago/Turabian StyleHsiu, Hsin, Shun-Ku Lin, Wan-Ling Weng, Chaw-Mew Hung, Che-Kai Chang, Chia-Chien Lee, and Chao-Tsung Chen. 2022. "Discrimination of the Cognitive Function of Community Subjects Using the Arterial Pulse Spectrum and Machine-Learning Analysis" Sensors 22, no. 3: 806. https://doi.org/10.3390/s22030806
APA StyleHsiu, H., Lin, S. -K., Weng, W. -L., Hung, C. -M., Chang, C. -K., Lee, C. -C., & Chen, C. -T. (2022). Discrimination of the Cognitive Function of Community Subjects Using the Arterial Pulse Spectrum and Machine-Learning Analysis. Sensors, 22(3), 806. https://doi.org/10.3390/s22030806