
Review of Real-Time Biomechanical Feedback Systems in Sport and Rehabilitation



Abstract
:1. Introduction
2. Methods
- What type of activity (sport or therapy) is being performed?
- What type of sensor or sensor system is used to acquire movement parameters?
- How many sensors are used and where are they placed?
- Is sensor fusion being used?
- What type of system architecture is used in the implementation?
- Where and how is data processing performed?
- What type of modality is used for feedback?
- What type and technology is used for communication?
- What is the intended use of the system (aim, user, environment)?
3. Results
3.1. Activity
3.2. Sensors
3.3. System Architecture and Data Processing
3.4. Feedback Modality and Actuators
3.5. Communication
3.6. Primary User and Environment
4. Findings
4.1. Activity
4.2. Sensors
4.3. System Architecture and Data Processing
4.4. Feedback Modality and Actuators
4.5. Primary User and Environment
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, J.; Wheeler, K.; James, D.A. Wearable Sensors in Sport: A Practical Guide to Usage and Implementation; SpringerBriefs in Applied Sciences and Technology; Springer: Singapore, 2019; ISBN 9789811337765. [Google Scholar]
- Kos, A.; Umek, A. Biomechanical Biofeedback Systems and Applications; Springer: Cham, Switzerland, 2018; ISBN 978-3-319-91349-0. [Google Scholar]
- Lightman, K. Silicon Gets Sporty. IEEE Spectr. 2016, 53, 48–53. [Google Scholar] [CrossRef]
- Baca, A.; Dabnichki, P.; Heller, M.; Kornfeind, P. Ubiquitous Computing in Sports: A Review and Analysis. J. Sports Sci. 2009, 27, 1335–1346. [Google Scholar] [CrossRef] [PubMed]
- Pustišek, M.; Wei, Y.; Sun, Y.; Umek, A.; Kos, A. The Role of Technology for Accelerated Motor Learning in Sport. Pers. Ubiquitous Comput. 2019, 25, 969–978. [Google Scholar] [CrossRef]
- Zhang, X.; Shan, G.; Wang, Y.; Wan, B.; Li, H. Wearables, Biomechanical Feedback, and Human Motor-Skills’ Learning & Optimization. Appl. Sci. 2019, 9, 226. [Google Scholar] [CrossRef] [Green Version]
- Giggins, O.M.; Persson, U.M.; Caulfield, B. Biofeedback in Rehabilitation. J. Neuroeng. Rehabil. 2013, 10, 60. [Google Scholar] [CrossRef] [Green Version]
- Kos, A.; Tomažič, S.; Umek, A. Suitability of Smartphone Inertial Sensors for Real-Time Biofeedback Applications. Sensors 2016, 16, 301. [Google Scholar] [CrossRef] [Green Version]
- Heikenfeld, J.; Jajack, A.; Rogers, J.; Gutruf, P.; Tian, L.; Pan, T.; Li, R.; Khine, M.; Kim, J.; Wang, J.; et al. Wearable Sensors: Modalities, Challenges, and Prospects. Lab Chip. 2018, 18, 217–248. [Google Scholar] [CrossRef] [Green Version]
- Van Hooren, B.; Goudsmit, J.; Restrepo, J.; Vos, S. Real-Time Feedback by Wearables in Running: Current Approaches, Challenges and Suggestions for Improvements. J. Sports Sci. 2020, 38, 214–230. [Google Scholar] [CrossRef]
- Aroganam, G.; Manivannan, N.; Harrison, D. Review on Wearable Technology Sensors Used in Consumer Sport Applications. Sensors 2019, 19, 1983. [Google Scholar] [CrossRef] [Green Version]
- Freedson, P.S.; Miller, K. Objective Monitoring of Physical Activity Using Motion Sensors and Heart Rate. Res. Q. Exerc. Sport 2000, 71, 21–29. [Google Scholar] [CrossRef]
- Camomilla, V.; Bergamini, E.; Fantozzi, S.; Vannozzi, G. Trends Supporting the In-Field Use of Wearable Inertial Sensors for Sport Performance Evaluation: A Systematic Review. Sensors 2018, 18, 873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attig, C.; Rauh, N.; Franke, T.; Krems, J. System Latency Guidelines Then and Now—Is Zero Latency Really Considered Necessary? In International Conference on Engineering Psychology and Cognitive Ergonomics; Springer: Cham, Switzerland, 2017; pp. 3–14. [Google Scholar]
- Amano, K.; Goda, N.; Nishida, S.; Ejima, Y.; Takeda, T.; Ohtani, Y. Estimation of the Timing of Human Visual Perception from Magnetoencephalography. J. Neurosci. 2006, 26, 3981–3991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Alahakone, A.U.; Senanayake, A. A Real-Time Interactive Biofeedback System for Sports Training and Rehabilitation. Proc. Inst. Mech. Eng. Part P-J. Sports Eng. Technol. 2010, 224, 181–190. [Google Scholar] [CrossRef]
- Wang, I.-L.; Wang, L.-I.; Liu, Y.; Su, Y.; Yao, S.; Ho, C.-S. Application of Real-Time Visual Feedback System in Balance Training of the Center of Pressure with Smart Wearable Devices. Int. J. Environ. Res. Public Health 2021, 18, 9637. [Google Scholar] [CrossRef]
- Wang, I.-L.; Wang, L.-I.; Xue, S.-J.; Hu, R.; Jian, R.-J.; Ho, C.-S. Gender Differences of the Improvement in Balance Control Based on the Real-Time Visual Feedback System with Smart Wearable Devices. Acta Bioeng. Biomech. 2021, 23, 163–171. [Google Scholar] [CrossRef]
- Vando, S.; Longo, S.; Cavaggioni, L.; Maurino, L.; Larion, A.; Invernizzi, P.L.; Padulo, J. The Effects of Short-Term Visual Feedback Training on the Stability of the Roundhouse Kicking Technique in Young Karatekas. Int. J. Environ. Res. Public Health 2021, 18, 1961. [Google Scholar] [CrossRef]
- Yokota, H.; Naito, M.; Mizuno, N.; Ohshima, S. Framework for Visual-Feedback Training Based on a Modified Self-Organizing Map to Imitate Complex Motion. Proc. Inst. Mech. Eng. Part P-J. Sport. Eng. Technol. 2020, 234, 49–58. [Google Scholar] [CrossRef]
- Xu, J.Y.; Nan, X.; Ebken, V.; Wang, Y.; Pottie, G.J.; Kaiser, W.J. Integrated Inertial Sensors and Mobile Computing for Real-Time Cycling Performance Guidance via Pedaling Profile Classification. IEEE J. Biomed. Health Inf. 2015, 19, 440–445. [Google Scholar] [CrossRef]
- Peeters, T.; Vleugels, J.; Garimella, R.; Truijen, S.; Saeys, W.; Verwulgen, S. Vibrotactile Feedback for Correcting Aerodynamic Position of a Cyclist. J. Sports Sci. 2020, 38, 2193–2199. [Google Scholar] [CrossRef]
- Grosshauser, T.; Blaesing, B.; Spieth, C.; Hermann, T. Wearable Sensor-Based Real-Time Sonification of Motion and Foot Pressure in Dance Teaching and Training. J. Audio Eng. Soc. 2012, 60, 580–589. [Google Scholar]
- Chun, S.; Kang, D.; Choi, H.-R.; Park, A.; Lee, K.-K.; Kim, J. A Sensor-Aided Self Coaching Model for Uncocking Improvement in Golf Swing. Multimed. Tools Appl. 2014, 72, 253–279. [Google Scholar] [CrossRef]
- Jakus, G.; Stojmenova, K.; Tomazic, S.; Sodnik, J. A System for Efficient Motor Learning Using Multimodal Augmented Feedback. Multimed. Tools Appl. 2017, 76, 20409–20421. [Google Scholar] [CrossRef]
- Koyama, Y.; Nishiyama, M.; Watanabe, K. Self Sports Motion Instruction System with Auditory Feedback Using Multi-Function Hetero-Core Fiber Optics. IEEJ Trans. Sens. Micromach. 2016, 136, 55–64. [Google Scholar] [CrossRef]
- Umek, A.; Tomažič, S.; Kos, A. Autonomous Wearable Personal Training System with Real-Time Biofeedback and Gesture User Interface. In Proceedings of the 2014 International Conference on Identification, Information and Knowledge in the Internet of Things, IIKI 2014, Beijing, China, 17–18 October 2014; pp. 122–125. [Google Scholar]
- Demircan, E. A Pilot Study on Locomotion Training via Biomechanical Models and a Wearable Haptic Feedback System. ROBOMECH J. 2020, 7, 19. [Google Scholar] [CrossRef]
- Garofolini, A.; Oppici, L.; Taylor, S. A Real-Time Feedback Method to Reduce Loading Rate during Running: Effect of Combining Direct and Indirect Feedback. J. Sports Sci. 2020, 38, 2446–2453. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.P.K.; Chan, Z.Y.S.; Au, I.P.H.; Lam, B.M.F.; Lam, W.K.; Cheung, R.T.H. Biomechanical Effects Following Footstrike Pattern Modification Using Wearable Sensors. J. Sci. Med. Sport 2021, 24, 30–35. [Google Scholar] [CrossRef]
- Clansey, A.C.; Hanlon, M.; Wallace, E.S.; Nevill, A.; Lake, M.J. Influence of Tibial Shock Feedback Training on Impact Loading and Running Economy. Med. Sci. Sports Exerc. 2014, 46, 973–981. [Google Scholar] [CrossRef]
- Cheung, R.T.H.; Davis, I.S. Landing Pattern Modification to Improve Patellofemoral Pain in Runners: A Case Series. J. Orthop. Sports Phys. 2011, 41, 914–919. [Google Scholar] [CrossRef]
- Crowell, H.P.; Milner, C.E.; Hamill, J.; Davis, I.S. Reducing Impact Loading during Running with the Use of Real-Time Visual Feedback. J. Orthop. Sports Phys. 2010, 40, 206–213. [Google Scholar] [CrossRef] [Green Version]
- Fiorentino, M.; Uva, A.E.; Foglia, M.M. Self Calibrating Wearable Active Running Asymmetry Measurement and Correction. Control. Eng. Appl. Inform. 2011, 13, 3–8. [Google Scholar]
- Sheerin, K.R.; Reid, D.; Taylor, D.; Besier, T.F. The Effectiveness of Real-Time Haptic Feedback Gait Retraining for Reducing Resultant Tibial Acceleration with Runners. Phys. Sport 2020, 43, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Van den Berghe, P.; Gosseries, M.; Gerlo, J.; Lenoir, M.; Leman, M.; de Clercq, D. Change-Point Detection of Peak Tibial Acceleration in Overground Running Retraining. Sensors 2020, 20, 1720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, J.B.; Goss, D.L.; Miller, E.M.; Davis, I.S. Using Real-Time Biofeedback to Alter Running Biomechanics: A Randomized Controlled Trial. Transl. Sports Med. 2020, 3, 63–71. [Google Scholar] [CrossRef]
- Nyman, E.J.; Armstrong, C.W. Real-Time Feedback during Drop Landing Training Improves Subsequent Frontal and Sagittal Plane Knee Kinematics. Clin. Biomech. 2015, 30, 988–994. [Google Scholar] [CrossRef]
- Effenberg, A.O.; Fehse, U.; Schmitz, G.; Krueger, B.; Mechling, H. Movement Sonification: Effects on Motor Learning beyond Rhythmic Adjustments. Front. Neurosci. 2016, 10, 219. [Google Scholar] [CrossRef]
- Ruffaldi, E.; Filippeschi, A.; Avizzano, C.A.; Bergamasco, M. Skill Modeling and Feedback Design for Training Rowing with Virtual Environments. In Advances in Cognitive Ergonomics; CRC Press: Boca Raton, FL, USA, 2016; pp. 832–841. ISBN 978-1-4398-3492-3. [Google Scholar]
- Ma, K. Artificial Intelligence Aided Training in Ping Pong Sport Education. In Proceedings of the 2020 Second International Conference on Transdisciplinary AI (TransAI), Irvine, CA, USA, 21–23 September 2020; pp. 43–49. [Google Scholar]
- Oagaz, H.; Schoun, B.; Choi, M.-H. Performance Improvement and Skill Transfer in Table Tennis Through Training in Virtual Reality. IEEE Trans. Vis. Comput. Graph. 2021, 1–12. [Google Scholar] [CrossRef]
- Godbout, A.; Boyd, J.E. Rhythmic Sonic Feedback for Speed Skating by Real-Time Movement Synchronization. Int. J. Comput. Sci. Sport 2012, 11, 37–51. [Google Scholar]
- Santos, M.O.; Costa, J.; Fernandes, T.R.; Silva, C.; Faria, S.M.M. Wearable Inertial and Bio-Signal Device for Real-Time Swimmer’s Monitoring. In Proceedings of the 2021 Telecoms Conference (Conf℡E), Leiria, Portugal, 11–12 February 2021; pp. 1–6. [Google Scholar]
- Li, J.; Di, F. Application of Video Real-Time Analysis Feedback and Motion Capture System in Ski Touring. In Proceedings of the 2020 2nd International Conference on Big Data and Artificial Intelligence; Association for Computing Machinery, New York, NY, USA, 28 April 2020; pp. 174–177. [Google Scholar]
- Kuwahara, T.; Takahashi, I.; Harikae, S. Real-Time Snowboard Training System for a Novice Using Visual and Auditory Feedback. In Proceedings of the 2020 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Toronto, ON, Canada, 11–14 October 2020; pp. 4230–4235. [Google Scholar]
- Chalker, W.J.; Shield, A.J.; Opar, D.A.; Rathbone, E.N.; Keogh, J.W.L. Effect of Acute Augmented Feedback on between Limb Asymmetries and Eccentric Knee Flexor Strength during the Nordic Hamstring Exercise. PeerJ 2018, 6, e4972. [Google Scholar] [CrossRef] [Green Version]
- Umek, A.; Kos, A. Smart Equipment Design Challenges for Real-Time Feedback Support in Sport. Facta Univ. Ser. Mech. Eng. 2018, 16, 389–403. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.-Y.; Tran, V.T.; Kim, D. A Novel Head Mounted Display Based Methodology for Balance Evaluation and Rehabilitation. Sustainability 2019, 11, 6453. [Google Scholar] [CrossRef] [Green Version]
- Alahakone, A.U.; Senanayake, S.M.N.A. A Real-Time System with Assistive Feedback for Postural Control in Rehabilitation. IEEE-ASME Trans. Mechatron. 2010, 15, 226–233. [Google Scholar] [CrossRef]
- Yin, C.; Hsueh, Y.-H.; Yeh, C.-Y.; Lo, H.-C.; Lan, Y.-T. A Virtual Reality-Cycling Training System for Lower Limb Balance Improvement. BioMed Res. Int. 2016, 2016, 9276508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, B.-C.; Chen, S.; Sienko, K.H. A Wearable Device for Real-Time Motion Error Detection and Vibrotactile Instructional Cuing. IEEE Trans. Neural. Syst. Rehabil. Eng. 2011, 19, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Gopalai, A.A.; Senanayake, S.M.N.A. A Wearable Real-Time Intelligent Posture Corrective System Using Vibrotactile Feedback. IEEE-Asme Trans. Mechatron. 2011, 16, 827–834. [Google Scholar] [CrossRef]
- Takeda, K.; Mani, H.; Hasegawa, N.; Sato, Y.; Tanaka, S.; Maejima, H.; Asaka, T. Adaptation Effects in Static Postural Control by Providing Simultaneous Visual Feedback of Center of Pressure and Center of Gravity. J. Physiol. Anthr. 2017, 36, 31. [Google Scholar] [CrossRef] [Green Version]
- Chiari, L.; Dozza, M.; Cappello, A.; Horak, F.B.; Macellari, V.; Giansanti, D. Audio-Biofeedback for Balance Improvement: An Accelerometry-Based System. IEEE Trans. Biomed. Eng. 2005, 52, 2108–2111. [Google Scholar] [CrossRef]
- Mansfield, A.; Aqui, A.; Fraser, J.E.; Rajachandrakumar, R.; Lakhani, B.; Patterson, K.K. Can Augmented Feedback Facilitate Learning a Reactive Balance Task among Older Adults? Exp. Brain Res. 2017, 235, 293–304. [Google Scholar] [CrossRef]
- Lee, B.-C.; Kim, J.; Chen, S.; Sienko, K.H. Cell Phone Based Balance Trainer. J. Neuroeng. Rehabil. 2012, 9, 10. [Google Scholar] [CrossRef] [Green Version]
- Vérité, F.; Bachta, W.; Morel, G. Closed Loop Kinesthetic Feedback for Postural Control Rehabilitation. IEEE Trans. Haptics 2014, 7, 150–160. [Google Scholar] [CrossRef]
- Bieryla, K.A.; Dold, N.M. Feasibility of Wii Fit Training to Improve Clinical Measures of Balance in Older Adults. Clin. Interv. Aging 2013, 8, 775–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwenk, M.; Grewal, G.S.; Honarvar, B.; Schwenk, S.; Mohler, J.; Khalsa, D.S.; Najafi, B. Interactive Balance Training Integrating Sensor-Based Visual Feedback of Movement Performance: A Pilot Study in Older Adults. J. Neuroeng. Rehabil. 2014, 11, 164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwenk, M.; Grewal, G.S.; Holloway, D.; Muchna, A.; Garland, L.; Najafi, B. Interactive Sensor-Based Balance Training in Older Cancer Patients with Chemotherapy-Induced Peripheral Neuropathy: A Randomized Controlled Trial. Gerontology 2016, 62, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Schwenk, M.; Sabbagh, M.; Lin, I.; Morgan, P.; Grewal, G.S.; Mohler, J.; Coon, D.W.; Najafi, B. Sensor-Based Balance Training with Motion Feedback in People with Mild Cognitive Impairment. J. Rehabil. Res. Dev. 2016, 53, 945–958. [Google Scholar] [CrossRef] [PubMed]
- Grewal, G.S.; Schwenk, M.; Lee-Eng, J.; Parvaneh, S.; Bharara, M.; Menzies, R.A.; Talal, T.K.; Armstrong, D.G.; Najafi, B. Sensor-Based Interactive Balance Training with Visual Joint Movement Feedback for Improving Postural Stability in Diabetics with Peripheral Neuropathy: A Randomized Controlled Trial. Gerontology 2015, 61, 567–574. [Google Scholar] [CrossRef]
- Lee, B.-C.; Thrasher, T.A.; Fisher, S.P.; Layne, C.S. The Effects of Different Sensory Augmentation on Weight-Shifting Balance Exercises in Parkinson’s Disease and Healthy Elderly People: A Proof-of-Concept Study. J. Neuroeng. Rehabil. 2015, 12, 75. [Google Scholar] [CrossRef] [Green Version]
- van den Heuvel, M.R.C.; Daffertshofer, A.; Beek, P.J.; Kwakkel, G.; van Wegen, E.E.H. The Effects of Visual Feedback during a Rhythmic Weight-Shifting Task in Patients with Parkinson’s Disease. Gait Posture 2016, 48, 140–145. [Google Scholar] [CrossRef]
- Lakhani, B.; Mansfield, A. Visual Feedback of the Centre of Gravity to Optimize Standing Balance. Gait Posture 2015, 41, 499–503. [Google Scholar] [CrossRef] [Green Version]
- Junata, M.; Cheng, K.C.-C.; Man, H.S.; Lai, C.W.-K.; Soo, Y.O.-Y.; Tong, R.K.-Y. Kinect-Based Rapid Movement Training to Improve Balance Recovery for Stroke Fall Prevention: A Randomized Controlled Trial. J. Neuro Eng. Rehabil. 2021, 18, 150. [Google Scholar] [CrossRef]
- Finkelstein, J.; Jeong, I.C. Feasibility of Interactive Biking Exercise System for Telemanagement in Elderly. Stud. Health Technol. Inf. 2013, 192, 642–646. [Google Scholar]
- Kuo, Y.-L.; Wang, P.-S.; Ko, P.-Y.; Huang, K.-Y.; Tsai, Y.-J. Immediate Effects of Real-Time Postural Biofeedback on Spinal Posture, Muscle Activity, and Perceived Pain Severity in Adults with Neck Pain. Gait Posture 2019, 67, 187–193. [Google Scholar] [CrossRef]
- Tamei, T.; Orito, Y.; Funaya, H.; Ikeda, K.; Okada, Y.; Shibata, T. Kinect-Based Posturography for in-Home Rehabilitation of Balance Disorders. APSIPA Trans. Signal Inf. Process. 2015, 4, e17. [Google Scholar] [CrossRef] [Green Version]
- Cortell-Tormo, J.M.; Garcia-Jaen, M.; Ruiz-Fernandez, D.; Fuster-Lloret, V. Lumbatex: A Wearable Monitoring System Based on Inertial Sensors to Measure and Control the Lumbar Spine Motion. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 1644–1653. [Google Scholar] [CrossRef]
- Kuo, Y.-L.; Huang, K.-Y.; Kao, C.-Y.; Tsai, Y.-J. Sitting Posture during Prolonged Computer Typing with and without a Wearable Biofeedback Sensor. Int. J. Environ. Res. Public Health 2021, 18, 5430. [Google Scholar] [CrossRef]
- Alsubaie, A.M.; Martinez-Valdes, E.; De Nunzio, A.M.; Falla, D. Trunk Control during Repetitive Sagittal Movements Following a Real-Time Tracking Task in People with Chronic Low Back Pain. J. Electromyogr. Kinesiol. 2021, 57, 102533. [Google Scholar] [CrossRef]
- Bonnette, S.; DiCesare, C.A.; Kiefer, A.W.; Riley, M.A.; Foss, K.D.B.; Thomas, S.; Diekfuss, J.A.; Myer, G.D. A Technical Report on the Development of a Real-Time Visual Biofeedback System to Optimize Motor Learning and Movement Deficit Correction. J. Sports Sci. Med. 2020, 19, 84–94. [Google Scholar]
- Gandolla, M.; Alessandra, P.; Simona, F.; Andrea, C.; Dario, B.; Stefano, S.; Federico, V.; Marco, B.; Francesco, B.; Stefano, M. Wearable Biofeedback Suit to Promote and Monitor Aquatic Exercises: A Feasibility Study. IEEE Trans. Instrum. Meas. 2020, 69, 1219–1231. [Google Scholar] [CrossRef]
- Kos, A.; Umek, A. Wearable Sensor Devices for Prevention and Rehabilitation in Healthcare: Swimming Exercise with Real-Time Therapist Feedback. IEEE Internet Things J. 2019, 6, 1331–1341. [Google Scholar] [CrossRef]
- Pignolo, L.; Basta, G.; Carozzo, S.; Bilotta, M.; Todaro, M.R.; Serra, S.; Ciancarelli, I.; Tonin, P.; Cerasa, A. A Body-Weight-Supported Visual Feedback System for Gait Recovering in Stroke Patients: A Randomized Controlled Study. Gait Posture 2020, 82, 287–293. [Google Scholar] [CrossRef]
- Statton, M.A.; Toliver, A.; Bastian, A.J. A Dual-Learning Paradigm Can Simultaneously Train Multiple Characteristics of Walking. J. Neurophysiol. 2016, 115, 2692–2700. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, C.; Washabaugh, E.P.; Seetharaman, Y. A Low Cost Real-Time Motion Tracking Approach Using Webcam Technology. J. Biomech. 2015, 48, 544–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Femery, V.G.; Moretto, P.G.; Hespel, J.-M.G.; Thévenon, A.; Lensel, G. A Real-Time Plantar Pressure Feedback Device for Foot Unloading. Arch. Phys. Med. Rehabil. 2004, 85, 1724–1728. [Google Scholar] [CrossRef] [PubMed]
- Dingwell, J.B.; Davis, B.L. A Rehabilitation Treadmill with Software for Providing Real-Time Gait Analysis and Visual Feedback. J. Biomech. Eng. 1996, 118, 253–255. [Google Scholar] [CrossRef] [PubMed]
- Redd, C.B.; Bamberg, S.J.M. A Wireless Sensory Feedback Device for Real-Time Gait Feedback and Training. IEEE-Asme Trans. Mechatron. 2012, 17, 425–433. [Google Scholar] [CrossRef]
- Held, J.P.O.; Yu, K.; Pyles, C.; Veerbeek, J.M.; Bork, F.; Heining, S.-M.; Navab, N.; Luft, A.R. Augmented Reality-Based Rehabilitation of Gait Impairments: Case Report. JMIR Mhealth Uhealth 2020, 8, e17804. [Google Scholar] [CrossRef] [PubMed]
- Armitano-Lago, C.; Pietrosimone, B.; Davis-Wilson, H.C.; Evans-Pickett, A.; Franz, J.R.; Blackburn, T.; Kiefer, A.W. Biofeedback Augmenting Lower Limb Loading Alters the Underlying Temporal Structure of Gait Following Anterior Cruciate Ligament Reconstruction. Hum. Mov. Sci. 2020, 73, 102685. [Google Scholar] [CrossRef]
- Pizzolato, C.; Reggiani, M.; Saxby, D.J.; Ceseracciu, E.; Modenese, L.; Lloyd, D.G. Biofeedback for Gait Retraining Based on Real-Time Estimation of Tibiofemoral Joint Contact Forces. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 1612–1621. [Google Scholar] [CrossRef] [Green Version]
- Fickey, S.N.; Browne, M.G.; Franz, J.R. Biomechanical Effects of Augmented Ankle Power Output during Human Walking. J. Exp. Biol. 2018, 221, jeb182113. [Google Scholar] [CrossRef] [Green Version]
- Ma, C.Z.-H.; Zheng, Y.-P.; Lee, W.C.-C. Changes in Gait and Plantar Foot Loading upon Using Vibrotactile Wearable Biofeedback System in Patients with Stroke. Top Stroke Rehabil. 2018, 25, 20–27. [Google Scholar] [CrossRef]
- Liu, J.; Kim, H.B.; Wolf, S.L.; Kesar, T.M. Comparison of the Immediate Effects of Audio, Visual, or Audiovisual Gait Biofeedback on Propulsive Force Generation in Able-Bodied and Post-Stroke Individuals. Appl. Psychophysiol. Biofeedback 2020, 45, 211–220. [Google Scholar] [CrossRef]
- Vadnerkar, A.; Figueiredo, S.; Mayo, N.E.; Kearney, R.E. Design and Validation of a Biofeedback Device to Improve Heel-to-Toe Gait in Seniors. IEEE J. Biomed. Health Inform. 2018, 22, 140–146. [Google Scholar] [CrossRef]
- Reh, J.; Hwang, T.-H.; Schmitz, G.; Effenberg, A.O. Dual Mode Gait Sonification for Rehabilitation After Unilateral Hip Arthroplasty. Brain Sci. 2019, 9, 66. [Google Scholar] [CrossRef] [Green Version]
- Szydlowski, G.; O’Neil, J.; Mrowczynski, J.; Inglis, L.; Ross, M. Electroskip Auditory Biofeedback in a Patient with Parkinson Disease: A Case Report. J. Exerc. Rehabil. 2019, 15, 688–695. [Google Scholar] [CrossRef]
- Hamacher, D.; Bertram, D.; Fölsch, C.; Schega, L. Evaluation of a Visual Feedback System in Gait Retraining: A Pilot Study. Gait Posture 2012, 36, 182–186. [Google Scholar] [CrossRef]
- Ginis, P.; Nieuwboer, A.; Dorfman, M.; Ferrari, A.; Gazit, E.; Canning, C.G.; Rocchi, L.; Chiari, L.; Hausdorff, J.M.; Mirelman, A. Feasibility and Effects of Home-Based Smartphone-Delivered Automated Feedback Training for Gait in People with Parkinson’s Disease: A Pilot Randomized Controlled Trial. Parkinsonism Relat. Disord. 2016, 22, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Ryu, S.; Kim, J.; Kim, W.-S.; Park, S.-K. Immediate Effects of Real-Time Visual Bio-Feedback Using Ground Reaction Forces on Gait Symmetry in Elderly Males. Int. J. Precis. Eng. Manuf. 2020, 21, 117–126. [Google Scholar] [CrossRef]
- Day, K.A.; Cherry-Allen, K.M.; Bastian, A.J. Individualized Feedback to Change Multiple Gait Deficits in Chronic Stroke. J. Neuroeng. Rehabil. 2019, 16, 158. [Google Scholar] [CrossRef] [Green Version]
- Mahajan, A.; Swarnalatha, R.; Sherwani, K.; Kumar, N. LabVIEW Based Monitoring and Rehabilitation Module for Freezing of Gait in Parkinson’s Disease. J. Med. Eng. Technol. 2019, 43, 48–54. [Google Scholar] [CrossRef]
- Hasegawa, N.; Takeda, K.; Sakuma, M.; Mani, H.; Maejima, H.; Asaka, T. Learning Effects of Dynamic Postural Control by Auditory Biofeedback versus Visual Biofeedback Training. Gait Posture 2017, 58, 188–193. [Google Scholar] [CrossRef]
- An, W.W.; Ting, K.-H.; Au, I.P.H.; Zhang, J.H.; Chan, Z.Y.S.; Davis, I.S.; So, W.K.Y.; Chan, R.H.M.; Cheung, R.T.H. Neurophysiological Correlates of Gait Retraining with Real-Time Visual and Auditory Feedback. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 1341–1349. [Google Scholar] [CrossRef]
- Khoo, I.-H.; Marayong, P.; Krishnan, V.; Balagtas, M.; Rojas, O.; Leyba, K. Real-Time Biofeedback Device for Gait Rehabilitation of Post-Stroke Patients. Biomed. Eng. Lett. 2017, 7, 287–298. [Google Scholar] [CrossRef] [PubMed]
- Bartels, B.M.; Moreno, A.; Quezada, M.J.; Sivertson, H.; Abbas, J.; Krishnamurthi, N. Real-Time Feedback Derived from Wearable Sensors to Improve Gait in Parkinson’s Disease. Technol. Innov. 2018, 20, 37–46. [Google Scholar] [CrossRef]
- Franz, J.R.; Maletis, M.; Kram, R. Real-Time Feedback Enhances Forward Propulsion during Walking in Old Adults. Clin. Biomech. 2014, 29, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Pu, F.; Ren, W.; Fan, X.; Chen, W.; Li, S.; Li, D.; Wang, Y.; Fan, Y. Real-Time Feedback of Dynamic Foot Pressure Index for Gait Training of Toe-Walking Children with Spastic Diplegia. Disabil. Rehabil. 2017, 39, 1921–1925. [Google Scholar] [CrossRef]
- van den Noort, J.C.; Steenbrink, F.; Roeles, S.; Harlaar, J. Real-Time Visual Feedback for Gait Retraining: Toward Application in Knee Osteoarthritis. Med. Biol. Eng. Comput. 2015, 53, 275–286. [Google Scholar] [CrossRef]
- Horsak, B.; Dlapka, R.; Iber, M.; Gorgas, A.-M.; Kiselka, A.; Gradl, C.; Siragy, T.; Doppler, J. SONIGait: A Wireless Instrumented Insole Device for Real-Time Sonification of Gait. J. Multimodal User Interfaces 2016, 10, 195–206. [Google Scholar] [CrossRef] [Green Version]
- Feasel, J.; Whitton, M.C.; Kassler, L.; Brooks, F.P.; Lewek, M.D. The Integrated Virtual Environment Rehabilitation Treadmill System. IEEE Trans. Neural Syst. Rehabil. Eng. 2011, 19, 290–297. [Google Scholar] [CrossRef] [Green Version]
- Booth, A.T.C.; van der Krogt, M.M.; Buizer, A.I.; Steenbrink, F.; Harlaar, J. The Validity and Usability of an Eight Marker Model for Avatar-Based Biofeedback Gait Training. Clin. Biomech. 2019, 70, 146–152. [Google Scholar] [CrossRef]
- Schließmann, D.; Nisser, M.; Schuld, C.; Gladow, T.; Derlien, S.; Heutehaus, L.; Weidner, N.; Smolenski, U.; Rupp, R. Trainer in a Pocket—Proof-of-Concept of Mobile, Real-Time, Foot Kinematics Feedback for Gait Pattern Normalization in Individuals after Stroke, Incomplete Spinal Cord Injury and Elderly Patients. J. Neuroeng. Rehabil. 2018, 15, 44. [Google Scholar] [CrossRef] [Green Version]
- Phongamwong, C.; Rowe, P.; Chase, K.; Kerr, A.; Millar, L. Treadmill Training Augmented with Real-Time Visualisation Feedback and Function Electrical Stimulation for Gait Rehabilitation after Stroke: A Feasibility Study. BMC Biomed. Eng. 2019, 1, 20. [Google Scholar] [CrossRef] [Green Version]
- Karatsidis, A.; Richards, R.E.; Konrath, J.M.; van den Noort, J.C.; Schepers, H.M.; Bellusci, G.; Harlaar, J.; Veltink, P.H. Validation of Wearable Visual Feedback for Retraining Foot Progression Angle Using Inertial Sensors and an Augmented Reality Headset. J. Neuroeng. Rehabil. 2018, 15, 78. [Google Scholar] [CrossRef] [PubMed]
- Tirosh, O.; Steinberg, N.; Nemet, D.; Eliakim, A.; Orland, G. Visual Feedback Gait Re-Training in Overweight Children Can Reduce Excessive Tibial Acceleration during Walking and Running: An Experimental Intervention Study. Gait Posture 2019, 68, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.K.Y.; Haller, M.; Besier, T.F. Wearable Lower Limb Haptic Feedback Device for Retraining Foot Progression Angle and Step Width. Gait Posture 2017, 55, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Biesmans, S.; Markopoulos, P. Design and Evaluation of SONIS, a Wearable Biofeedback System for Gait Retraining. Multimodal Technol. Interact. 2020, 4, 60. [Google Scholar] [CrossRef]
- Fukuyama, K.; Kurose, I.; Ikeuchi, H. Examination of Screen-Indicated Methods of Gait Training System with Real-Time Audiovisual Feedback Function of Ground Reaction Force*. In Proceedings of the 2020 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Las Vegas, NV, USA, 24 October 2020–24 January 2021; pp. 4155–4160. [Google Scholar]
- Reh, J.; Schmitz, G.; Hwang, T.-H.; Effenberg, A.O. Acoustic Feedback in Gait Rehabilitation—Pre-Post Effects in Patients with Unilateral Hip Arthroplasty. Front. Sports Act. Living 2021, 3, 106. [Google Scholar] [CrossRef]
- Liu, J.; Santucci, V.; Eicholtz, S.; Kesar, T.M. Comparison of the Effects of Real-Time Propulsive Force versus Limb Angle Gait Biofeedback on Gait Biomechanics. Gait Posture 2021, 83, 107–113. [Google Scholar] [CrossRef]
- Tiwari, A.; Joshi, D. Design and Validation of a Real-Time Visual Feedback System to Improve Minimum Toe Clearance (MTC) in Transfemoral Amputees. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1711–1722. [Google Scholar] [CrossRef]
- Shoei, N.; Kouki, N. Extension of the Interface for Visual Feedback of Center of Foot Pressure in Insole Type Measurement Device. In Proceedings of the 2021 World Automation Congress (WAC), Taipei, Taiwan, 1–5 August 2021; pp. 160–163. [Google Scholar]
- Liu, X.; Oliveira, N.; Ehrenberg, N.; Cheng, J.; Bentley, K.; Blochlinger, S.; Shoval, H.; Barrance, P. Feasibility of a Real-Time Pattern-Based Kinematic Feedback System for Gait Retraining in Pediatric Cerebral Palsy. J. Rehabil. Assist. Technol. Eng. 2021, 8, 20556683211014124. [Google Scholar] [CrossRef]
- Martini, E.; Cesini, I.; D’Abbraccio, J.; Arnetoli, G.; Doronzio, S.; Giffone, A.; Meoni, B.; Oddo, C.M.; Vitiello, N.; Crea, S. Increased Symmetry of Lower-Limb Amputees Walking with Concurrent Bilateral Vibrotactile Feedback. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 74–84. [Google Scholar] [CrossRef]
- Soltane, S.; Al-Mutabeq, S.; Masood, M.; Al-Otaibi, R.; Raouf, S.A.; Khan, W. Therapeutic Smart Feedback System with a Real-Time GUI Used after Foot Surgery. In Proceedings of the 2021 International Conference of Women in Data Science at Taif University (WiDSTaif), Taif, Saudi Arabia, 30–31 March 2021; pp. 1–5. [Google Scholar]
- Chamorro-Moriana, G.; Sevillano, J.L.; Perez-Cabezas, V. Versatile GCH Control Software for Correction of Loads Applied to Forearm Crutches During Gait Recovery Through Technological Feedback: Development and Implementation Study. J. Med. Internet Res. 2021, 23, e27602. [Google Scholar] [CrossRef]
- Shull, P.B.; Xia, H.; Charlton, J.M.; Hunt, M.A. Wearable Real-Time Haptic Biofeedback Foot Progression Angle Gait Modification to Assess Short-Term Retention and Cognitive Demand. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1858–1865. [Google Scholar] [CrossRef] [PubMed]
- Donatell, G.J.; Meister, D.W.; O’Brien, J.R.; Thurlow, J.S.; Webster, J.G.; Fellow, L.; Salvi, F.J. A Simple Device to Monitor Flexion and Lateral Bending of the Lumbar Spine. IEEE Trans. Neural Syst. Rehabil. Eng. 2005, 13, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Ianculescu, M.; Andrei, B.; Alexandru, A. A Smart Assistance Solution for Remotely Monitoring the Orthopaedic Rehabilitation Process Using Wearable Technology: Re.Flex System. Stud. Inform. Control. 2019, 28, 317–326. [Google Scholar] [CrossRef]
- Foreman, M.H.; Engsberg, J.R. A Virtual Reality Tool for Measuring and Shaping Trunk Compensation for Persons with Stroke: Design and Initial Feasibility Testing. J. Rehabil. Assist. Technol. Eng. 2019, 6, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Duff, M.; Chen, Y.; Attygalle, S.; Herman, J.; Sundaram, H.; Qian, G.; He, J.; Rikakis, T. An Adaptive Mixed Reality Training System for Stroke Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Zhang, Y.; Wang, Q.M.; Bai, Y.; Wu, Y. An Interactive Motion-Tracking System for Home-Based Assessing and Training Reach-to-Target Tasks in Stroke Survivors—A Preliminary Study. Med. Biol. Eng. Comput. 2020, 58, 1529–1547. [Google Scholar] [CrossRef]
- Roosink, M.; McFadyen, B.J.; Hebert, L.J.; Jackson, P.L.; Bouyer, L.J.; Mercier, C. Assessing the Perception of Trunk Movements in Military Personnel with Chronic Non-Specific Low Back Pain Using a Virtual Mirror. PLoS ONE 2015, 10, e0120251. [Google Scholar] [CrossRef] [Green Version]
- Ghai, S.; Schmitz, G.; Hwang, T.-H.; Effenberg, A.O. Auditory Proprioceptive Integration: Effects of Real-Time Kinematic Auditory Feedback on Knee Proprioception. Front. Neurosci. 2018, 12, 142. [Google Scholar] [CrossRef] [Green Version]
- Kutyina, D.V.; Nakonechny, D.G.; Motailo, A.; Pigareva, Y.I.; Kiseleva, A.N.; Kazantsev, V.B.; Gordleeva, S.Y.; Kaplan, A.Y.; Pimashkin, A.S. Automated Complex of Motion Control Based on Vibrotactile Feedback for Rehabilitation. Sovrem. Tehnol. V Med. 2017, 9, 36–41. [Google Scholar] [CrossRef]
- Hossain, M.S.; Hoda, M.; Muhammad, G.; Almogren, A.; Alamri, A. Cloud-Supported Framework for Patients in Post-Stroke Disability Rehabilitation. Telemat. Inform. 2018, 35, 826–836. [Google Scholar] [CrossRef]
- Dahl-Popolizio, S.; Loman, J.; Cordes, C.C. Comparing Outcomes of Kinect Videogame-Based Occupational/Physical Therapy Versus Usual Care. Games Health J. 2014, 3, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Borghese, N.A.; Pirovano, M.; Lanzi, P.L.; Wüest, S.; de Bruin, E.D. Computational Intelligence and Game Design for Effective At-Home Stroke Rehabilitation. Games Health J. 2013, 2, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Triandafilou, K.M.; Tsoupikova, D.; Barry, A.J.; Thielbar, K.N.; Stoykov, N.; Kamper, D.G. Development of a 3D, Networked Multi-User Virtual Reality Environment for Home Therapy after Stroke. J. Neuroeng. Rehabil. 2018, 15, 88. [Google Scholar] [CrossRef] [PubMed]
- Mittag, C.; Leiss, R.; Lorenz, K.; Seel, T. Development of a Home-Based Wrist Range-of-Motion Training System for Children with Cerebral Palsy. At-Automatisierungstechnik 2020, 68, 967–977. [Google Scholar] [CrossRef]
- Caudron, S.; Guerraz, M.; Eusebio, A.; Gros, J.-P.; Azulay, J.-P.; Vaugoyeau, M. Evaluation of a Visual Biofeedback on the Postural Control in Parkinson’s Disease. Neurophysiol. Clin. 2014, 44, 77–86. [Google Scholar] [CrossRef]
- Stanica, I.-C.; Moldoveanu, F.; Portelli, G.-P.; Dascalu, M.-I.; Moldoveanu, A.; Ristea, M.G. Flexible Virtual Reality System for Neurorehabilitation and Quality of Life Improvement. Sensors 2020, 20, 6045. [Google Scholar] [CrossRef]
- Kontadakis, G.; Chasiouras, D.; Proimaki, D.; Halkiadakis, M.; Fyntikaki, M.; Mania, K. Gamified Platform for Rehabilitation after Total Knee Replacement Surgery Employing Low Cost and Portable Inertial Measurement Sensor Node. Multimed. Tools Appl. 2020, 79, 3161–3188. [Google Scholar] [CrossRef]
- Abujaber, S.; Pozzi, F.; Zeni, J.J. Influence of Weight Bearing Visual Feedback on Movement Symmetry during Sit to Stand Task. Clin. Biomech. 2017, 47, 110–116. [Google Scholar] [CrossRef]
- Dao, T.T.; Tannous, H.; Pouletaut, P.; Gamet, D.; Istrate, D.; Tho, M.C.H.B. Interactive and Connected Rehabilitation Systems for E-Health. IRBM 2016, 37, 289–296. [Google Scholar] [CrossRef]
- Ren, W.; Pu, F.; Fan, X.; Li, S.; Sun, L.; Li, D.; Wang, Y.; Fan, Y. Kinect-Based Skeleton-Matching Feedback for Motor Rehabilitation: Transient Performance Effect of Shoulder Training. J. Mech. Med. Biol. 2016, 16, 1650037. [Google Scholar] [CrossRef]
- Foo, J.; Paterson, K.; Williams, G.; Clark, R. Low-Cost Evaluation and Real-Time Feedback of Static and Dynamic Weight Bearing Asymmetry in Patients Undergoing in-Patient Physiotherapy Rehabilitation for Neurological Conditions. J. Neuroeng. Rehabil. 2013, 10, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antunes, A.; Carnide, F.; Matias, R. Real-Time Kinematic Biofeedback Improves Scapulothoracic Control and Performance during Scapular-Focused Exercises: A Single-Blind Randomized Controlled Laboratory Study. Hum. Mov. Sci. 2016, 48, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Weon, J.-H.; Kwon, O.-Y.; Cynn, H.-S.; Lee, W.-H.; Kim, T.-H.; Yi, C.-H. Real-Time Visual Feedback Can Be Used to Activate Scapular Upward Rotators in People with Scapular Winging: An Experimental Study. J. Physiother. 2011, 57, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.L.; Fujii, S.; Schlaug, G. The Use of Augmented Auditory Feedback to Improve Arm Reaching in Stroke: A Case Series. Disabil. Rehabil. 2016, 38, 1115–1124. [Google Scholar] [CrossRef] [Green Version]
- Ghai, S.; Schmitz, G.; Hwang, T.-H.; Effenberg, A.O. Training Proprioception with Sound: Effects of Real-Time Auditory Feedback on Intermodal Learning. Ann. N. Y. Acad. Sci. 2019, 1438, 50–61. [Google Scholar] [CrossRef]
- Koritnik, T.; Bajd, T.; Munih, M. Virtual Environment for Lower-Extremities Training. Gait Posture 2008, 27, 323–330. [Google Scholar] [CrossRef]
- Carpinella, I.; Cattaneo, D.; Bonora, G.; Bowman, T.; Martina, L.; Montesano, A.; Ferrarin, M. Wearable Sensor-Based Biofeedback Training for Balance and Gait in Parkinson Disease: A Pilot Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2017, 98, 622–630.e3. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.A. Web-Based Multimedia Hand-Therapy Framework for Measuring Forward and Inverse Kinematic Data. Multimed. Tools Appl. 2017, 76, 8227–8255. [Google Scholar] [CrossRef]
- Bisio, I.; Garibotto, C.; Lavagetto, F.; Sciarrone, A. When EHealth Meets IoT: A Smart Wireless System for Post-Stroke Home Rehabilitation. IEEE Wirel. Commun. 2019, 26, 24–29. [Google Scholar] [CrossRef]
- Bohorquez, J.; McKinney, J.; Keyser, L.; Sutherland, R.; Pulliam, S.J. Development of a Wireless Accelerometer-Based Intravaginal Device to Detect Pelvic Floor Motion for Evaluation of Pelvic Floor Dysfunction. Biomed. Microdevices 2020, 22, 26. [Google Scholar] [CrossRef] [Green Version]
- Caviedes, J.E.; Li, B.; Jammula, V.C. Wearable Sensor Array Design for Spine Posture Monitoring During Exercise Incorporating Biofeedback. IEEE Trans. Biomed. Eng. 2020, 67, 2828–2838. [Google Scholar] [CrossRef] [PubMed]
- Biebl, J.T.; Rykala, M.; Strobel, M.; Kaur Bollinger, P.; Ulm, B.; Kraft, E.; Huber, S.; Lorenz, A. App-Based Feedback for Rehabilitation Exercise Correction in Patients with Knee or Hip Osteoarthritis: Prospective Cohort Study. J. Med. Internet Res. 2021, 23, e26658. [Google Scholar] [CrossRef] [PubMed]
- Torp, D.M.; Thomas, A.C.; Hubbard-Turner, T.; Donovan, L. Biomechanical Response to External Biofeedback During Functional Tasks in Individuals with Chronic Ankle Instability. J. Athl. Train. 2020, 56, 263–271. [Google Scholar] [CrossRef]
- Sanford, S.; Liu, M.; Selvaggi, T.; Nataraj, R. Effects of Visual Feedback Complexity on the Performance of a Movement Task for Rehabilitation. J. Mot. Behav. 2021, 53, 243–257. [Google Scholar] [CrossRef] [PubMed]
- Tannous, H.; Istrate, D.; Perrochon, A.; Daviet, J.-C.; Benlarbi-Delai, A.; Sarrazin, J.; Ho Ba Tho, M.-C.; Dao, T.T. GAMEREHAB@HOME: A New Engineering System Using Serious Game and Multisensor Fusion for Functional Rehabilitation at Home. IEEE Trans. Games 2021, 13, 89–98. [Google Scholar] [CrossRef]
- Luo, Z.; Durairaj, P.; Lau, C.M.; Katsumoto, Y.; Do, E.Y.-L.; Zainuddin, A.S.B.; Kawauchi, K. Gamification of Upper Limb Virtual Rehabilitation in Post Stroke Elderly Using SilverTune—A Multi-Sensory Tactile Musical Assistive System. In Proceedings of the 2021 IEEE 7th International Conference on Virtual Reality (ICVR), Foshan, China, 20–22 May 2021; pp. 149–155. [Google Scholar]
- Ashapkina, M.S.; Alpatov, A.V.; Sablina, V.A.; Melnik, O.V. Vibro-Tactile Portable Device for Home-Base Physical Rehabilitation. In Proceedings of the 2021 10th Mediterranean Conference on Embedded Computing (MECO), Budva, Montenegro, 7–10 June 2021; pp. 1–4. [Google Scholar]
- Chen, Y.; Duff, M.; Lehrer, N.; Liu, S.-M.; Blake, P.; Wolf, S.L.; Sundaram, H.; Rikakis, T. A Novel Adaptive Mixed Reality System for Stroke Rehabilitation: Principles, Proof of Concept, and Preliminary Application in 2 Patients. Top. Stroke Rehabil. 2011, 18, 212–230. [Google Scholar] [CrossRef]
- Mokhlespour Esfahani, M.I.; Nussbaum, M.A. Preferred Placement and Usability of a Smart Textile System vs. Inertial Measurement Units for Activity Monitoring. Sensors 2018, 18, 2501. [Google Scholar] [CrossRef] [Green Version]
- Bergmann, J.H.M.; Chandaria, V.; McGregor, A. Wearable and Implantable Sensors: The Patient’s Perspective. Sensors 2012, 12, 16695–16709. [Google Scholar] [CrossRef] [Green Version]
- Agresta, C.; Brown, A. Gait Retraining for Injured and Healthy Runners Using Augmented Feedback: A Systematic Literature Review. J. Orthop. Sports Phys. 2015, 45, 576–584. [Google Scholar] [CrossRef]
- Rana, M.; Mittal, V. Wearable Sensors for Real-Time Kinematics Analysis in Sports: A Review. IEEE Sens. J. 2021, 21, 1187–1207. [Google Scholar] [CrossRef]
- Tate, J.J.; Milner, C.E. Real-Time Kinematic, Temporospatial, and Kinetic Biofeedback during Gait Retraining in Patients: A Systematic Review. Phys. Ther. 2010, 90, 1123–1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, R.; Lai, D.T.H.; Lee, W. A Survey on Biofeedback and Actuation in Wireless Body Area Networks (WBANs). IEEE Rev. Biomed. Eng. 2017, 10, 162–173. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Field of Study | Activity | Ni | Papers |
|---|---|---|---|
| Sport (N = 33) | Balance | 4 | [17,18,19,20] |
| Cycling | 3 | [21,22,23] | |
| Dancing | 1 | [24] | |
| Golf | 4 | [25,26,27,28] | |
| Running | 11 | [27,29,30,31,32,33,34,35,36,37,38] | |
| Jumping | 1 | [39] | |
| Rowing | 2 | [40,41] | |
| Table tennis | 2 | [42,43] | |
| Skating | 1 | [44] | |
| Swimming | 1 | [45] | |
| Skiing | 2 | [46,47] | |
| Other sport activities | 2 | [48,49] | |
| Rehabilitation (N = 111) | Balance | 19 | [50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68] |
| Cycling | 1 | [69] | |
| Posture | 5 | [70,71,72,73,74] | |
| Squat | 1 | [75] | |
| Swimming | 2 | [76,77] | |
| Gait | 46 | [78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123] | |
| Other rehabilitation activities | 36 | [124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159] |
| Sensor Type | N | Papers |
|---|---|---|
| Kinematic sensor (IMU) | 62 | [17,21,22,24,25,28,29,32,34,35,36,37,38,42,45,46,47,49,50,51,53,54,56,58,61,62,63,64,65,69,70,72,73,76,77,84,90,91,93,94,99,101,105,108,110,111,115,119,123,125,130,136,137,138,139,144,147,149,151,152,157,158,159] |
| Force sensor | 28 | [18,20,30,31,40,48,52,55,57,59,60,66,67,82,85,86,88,92,95,98,102,104,106,114,122,124,140,143] |
| Pressure Sensor | 20 | [18,19,24,33,47,78,81,83,97,100,103,105,113,117,118,120,121,132,151,155] |
| Stretch sensor | 2 | [44,153] |
| Bend/angle sensors | 4 | [24,27,146,158] |
| Optical motion tracking | 34 | [25,26,30,39,43,55,68,71,74,75,79,86,87,89,96,104,107,109,112,116,126,127,129,132,133,134,135,141,142,148,150,156,157,160] |
| Camera | 6 | [40,46,80,128,145,154] |
| Electromyography | 4 | [86,131,138,156] |
| Other | 9 | [23,40,41,45,52,69,117,124,135] |
| Sampling Frequency [Hz] | N | Papers |
|---|---|---|
| <100 | 33 | [27,39,42,44,45,48,50,58,69,71,72,76,80,88,90,91,100,101,109,110,117,119,122,128,130,136,137,143,147,148,149,156] |
| 100 | 27 | [20,21,25,40,49,53,54,56,61,62,63,64,65,77,79,82,87,94,96,105,112,120,123,127,129,153,159] |
| 101–499 | 19 | [18,22,24,29,33,41,55,57,67,75,81,86,104,111,118,140,144,146,155] |
| 500–1000 | 10 | [37,52,55,59,66,83,98,99,102,106] |
| >1000 | 3 | [30,32,34] |
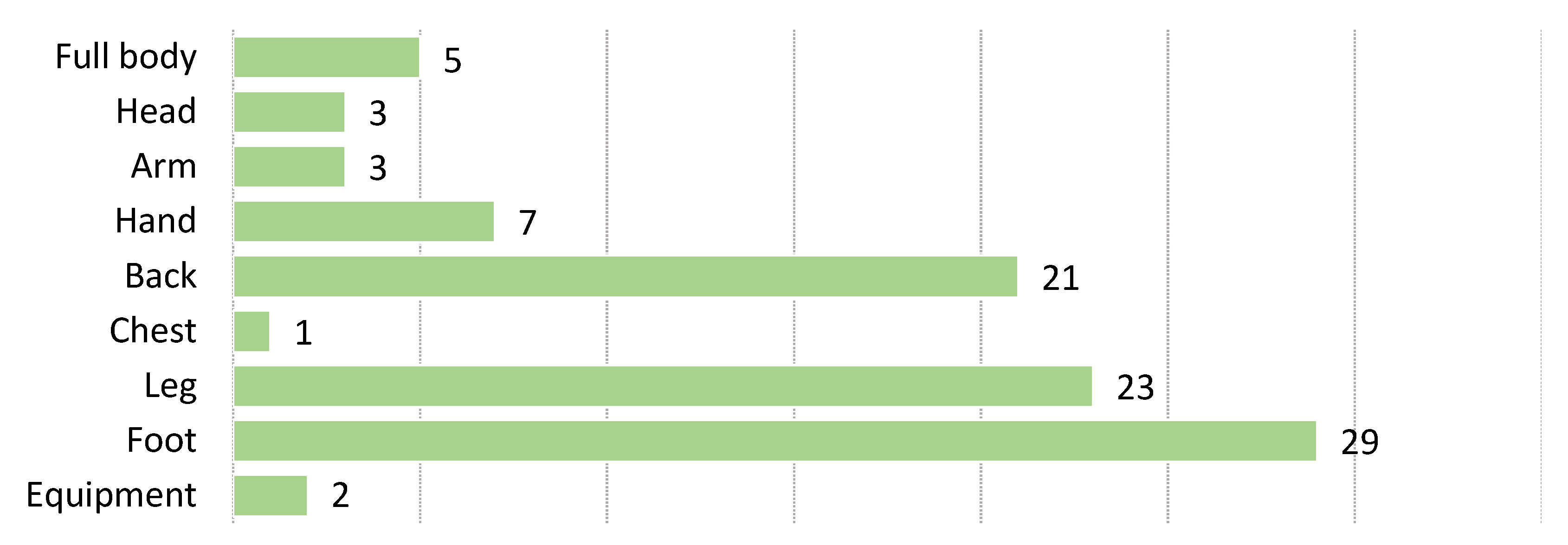
| Sensors Location | N | Papers |
|---|---|---|
| Full body | 5 | [27,76,138,149,156] |
| Head | 3 | [28,50,137] |
| Arm | 3 | [127,131,146] |
| Hand | 7 | [25,69,132,136,150,158,160] |
| Leg | 23 | [21,24,32,34,35,36,61,62,63,64,84,86,87,89,91,102,110,111,115,125,130,139,151] |
| Foot | 29 | [18,22,24,31,33,37,38,44,47,52,69,78,81,83,88,90,97,100,101,103,105,108,113,117,118,120,121,123,155] |
| Chest | 1 | [70] |
| Back | 21 | [23,53,54,56,61,62,63,64,65,72,73,74,77,84,124,130,137,146,153] |
| Equipment | 2 | [25,42] |
| System Architecture | N | Papers |
|---|---|---|
| Compact | 35 | [20,28,29,33,35,37,38,39,44,50,53,58,59,66,67,68,70,82,83,84,88,95,97,100,107,120,121,123,128,133,134,142,154,155,159] |
| Distributed | 109 | [17,18,19,21,22,23,24,25,26,27,30,31,32,34,36,40,41,42,43,45,46,47,48,49,51,52,54,55,56,57,60,61,62,63,64,65,69,71,72,73,74,75,76,77,78,79,80,81,85,86,87,89,90,91,92,93,94,96,98,99,101,102,103,104,105,106,108,109,110,111,112,113,114,115,116,117,118,119,122,124,125,126,127,129,130,131,132,135,136,137,138,139,140,141,143,144,145,146,147,148,149,150,151,152,153,156,157,158,160] |
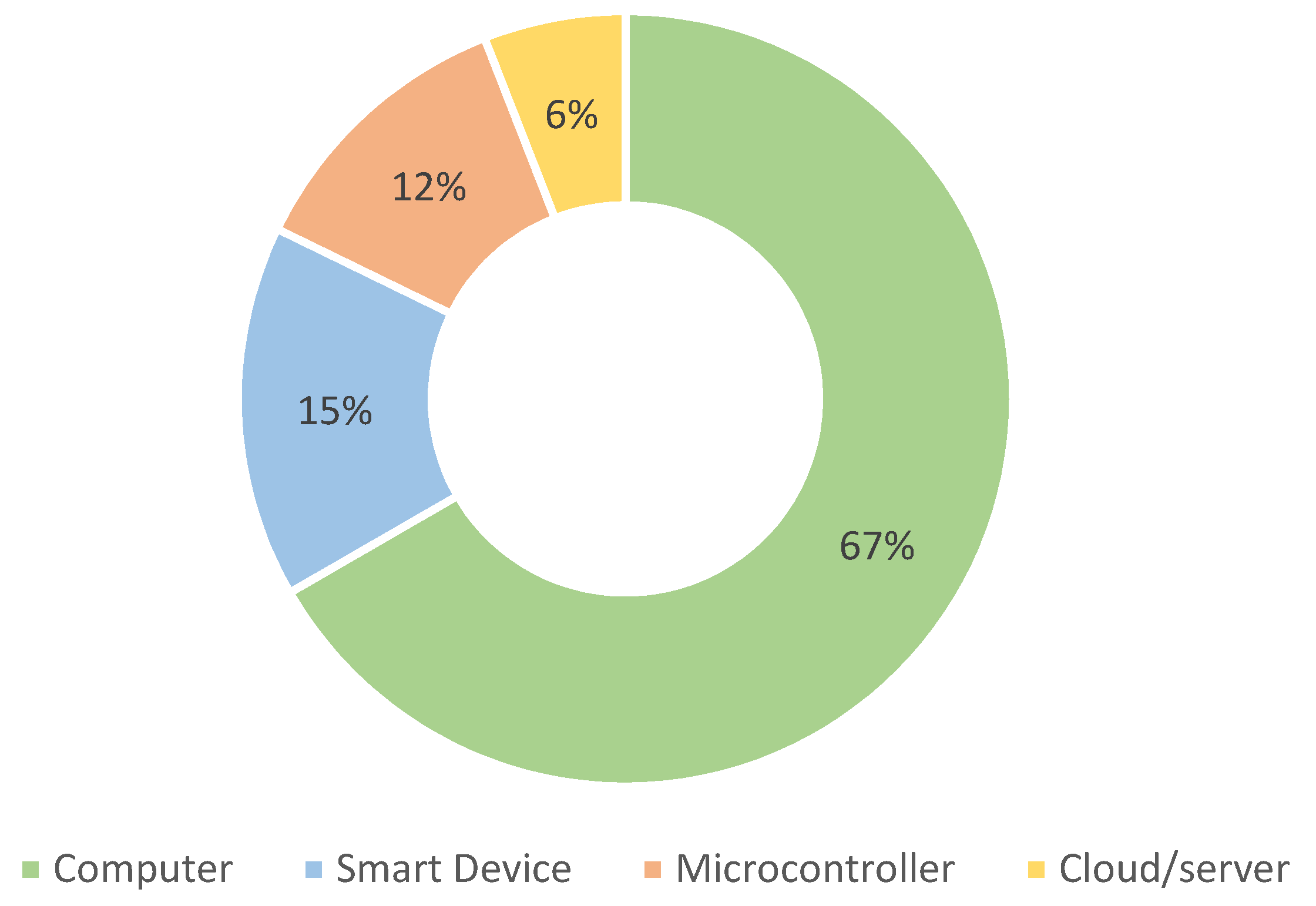
| Processing Device | N | Papers |
|---|---|---|
| Smart Device | 21 | [18,22,28,31,37,50,53,58,70,72,83,84,90,94,101,103,108,113,121,139,154] |
| Embedded systems | 16 | [24,27,33,35,47,49,82,88,97,100,105,112,118,123,155,159] |
| Cloud/server | 8 | [77,93,125,132,141,151,157,158] |
| Computer | 90 | All others |
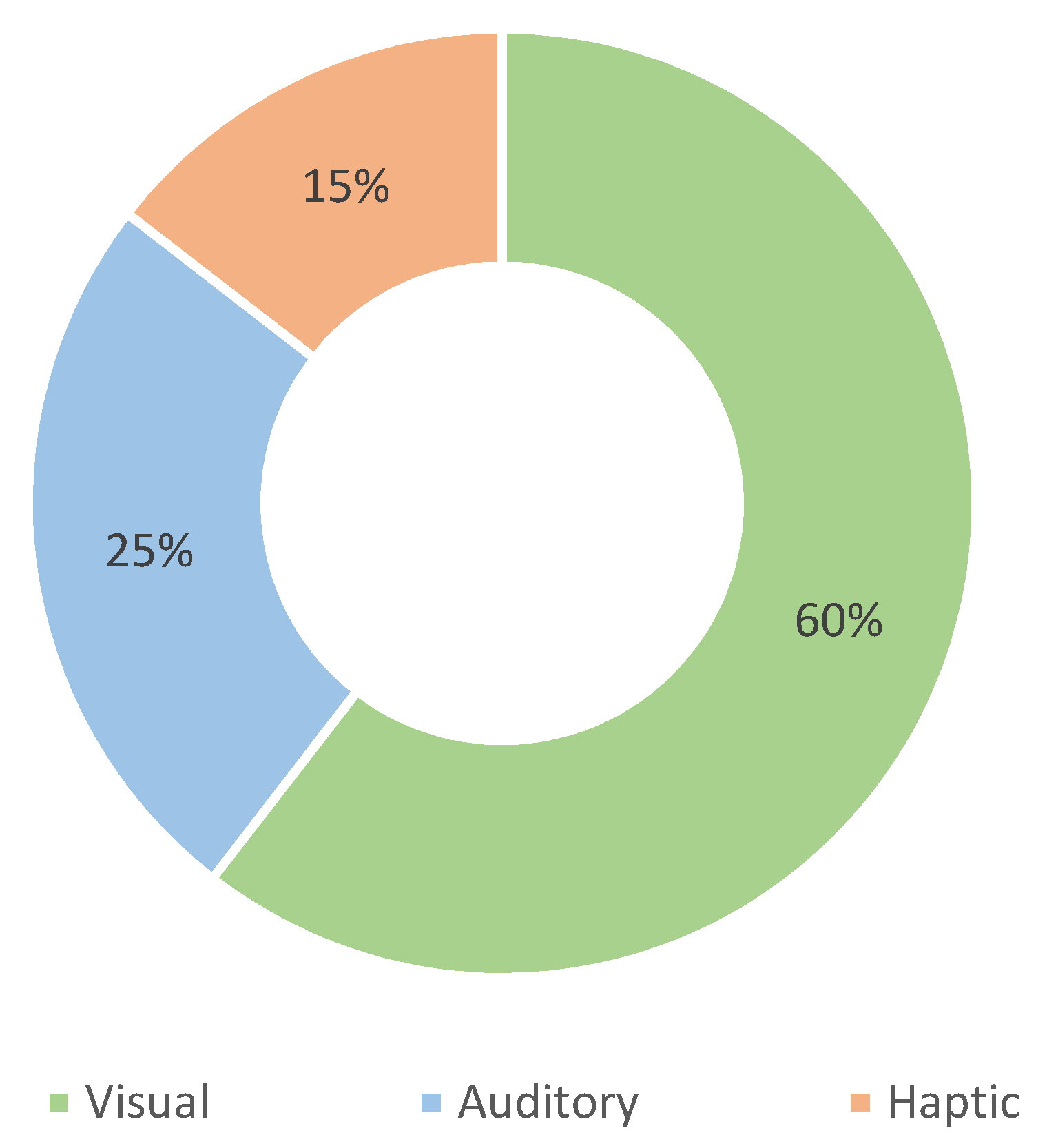
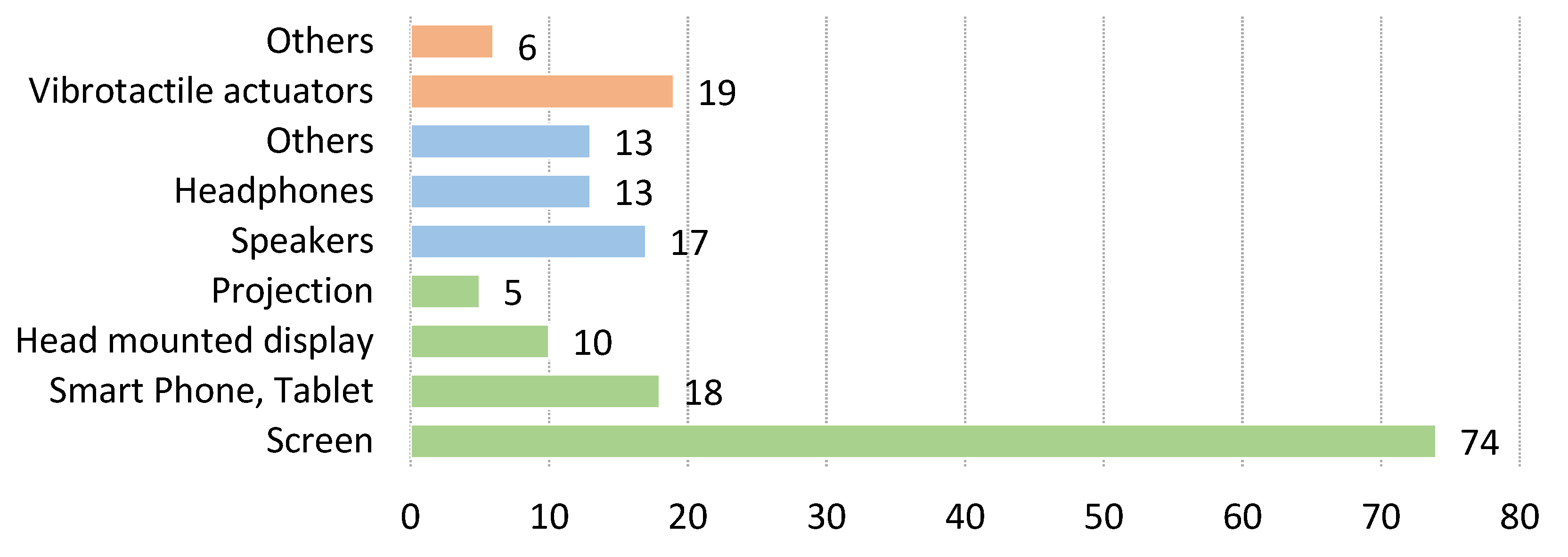
| FB Modality | Device | Ni | Papers |
|---|---|---|---|
| Visual 104 | Screen | 74 | [20,21,25,26,30,34,39,41,42,45,46,48,52,55,57,60,61,62,63,64,65,66,67,68,69,71,74,76,78,79,80,81,82,85,86,89,95,96,98,99,102,104,106,107,109,111,114,116,117,118,119,122,124,126,127,128,132,133,134,135,140,141,142,143,144,145,149,150,152,156,157,158,160] |
| Smart Phone, Tablet | 18 | [18,19,22,38,49,72,77,78,83,90,101,121,125,136,139,151,153,154] | |
| Head mounted display | 10 | [43,47,50,75,84,93,110,132,137,138] | |
| Projection | 5 | [32,40,87,129,148] | |
| Auditory 43 | Speakers | 17 | [24,26,27,31,32,39,81,89,92,98,103,113,114,116,122,127,160] |
| Headphones | 13 | [28,37,40,44,47,56,91,105,108,115,130,146,147] | |
| Others | 13 | [33,38,83,84,94,100,101,121,126,149,153,154,155] | |
| Haptic 25 | Vibrotactile actuators | 19 | [17,23,35,36,41,51,53,54,58,65,70,73,88,97,112,120,123,131,159] |
| Others | 6 | [29,59,83,100,101,109] |
| Communication Mode | Specific Technology | N | Papers |
|---|---|---|---|
| Wired | 31 | [26,30,37,41,42,49,52,55,56,59,67,71,79,80,81,82,87,95,96,99,106,114,117,124,126,127,129,131,140,150,160] | |
| Wireless | Wi-Fi | 4 | [50,54,78,151] |
| Bluetooth | 33 | [20,22,23,24,25,27,28,31,36,46,47,50,53,69,71,72,83,88,90,97,101,105,108,113,117,118,121,143,149,152,153,158] | |
| LoRa | 1 | [45] | |
| Other | [17,19,21,29,35,38,48,51,70,75,76,84,91,92,93,94,100,102,110,111,115,119,122,125,130,135,136,137,147,157,159] |
| Main User | N | Papers |
|---|---|---|
| User | 50 | [19,20,22,24,25,28,29,31,33,35,37,38,42,44,47,53,60,68,70,71,83,84,88,94,97,101,108,113,118,120,121,123,125,128,132,133,134,137,139,141,142,150,151,152,153,154,157,158,159] |
| Expert | 106 | [17,18,21,23,25,26,27,30,32,33,34,36,39,40,41,43,45,46,48,49,51,52,54,55,56,57,58,59,61,62,63,64,65,66,67,69,72,73,74,75,76,77,78,79,80,81,82,85,86,87,89,90,91,92,93,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,114,115,116,117,119,122,124,126,127,129,130,131,132,133,134,135,136,137,138,140,141,142,143,144,145,146,147,148,149,151,155,156,160] |
| Environment | N | Papers |
|---|---|---|
| Professional | 100 | [17,18,21,23,25,26,27,30,32,33,34,36,38,39,40,41,43,45,48,51,52,53,54,55,56,57,58,59,61,62,63,64,65,66,67,69,72,73,74,75,77,78,79,80,81,82,85,86,87,89,90,91,92,93,95,96,97,98,99,100,101,102,103,104,106,107,109,111,112,114,115,116,117,119,122,124,126,127,129,130,131,133,134,135,136,137,138,140,141,142,143,144,145,146,147,148,149,155,156,160] |
| Home | 30 | [20,31,33,50,53,60,68,71,83,84,88,92,94,97,100,101,125,128,132,133,134,135,137,141,142,150,151,154,157,158] |
| In-field | 27 | [19,22,24,25,28,29,35,37,42,44,46,47,49,70,76,105,108,110,113,118,120,121,123,139,152,153,159] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hribernik, M.; Umek, A.; Tomažič, S.; Kos, A. Review of Real-Time Biomechanical Feedback Systems in Sport and Rehabilitation. Sensors 2022, 22, 3006. https://doi.org/10.3390/s22083006
Hribernik M, Umek A, Tomažič S, Kos A. Review of Real-Time Biomechanical Feedback Systems in Sport and Rehabilitation. Sensors. 2022; 22(8):3006. https://doi.org/10.3390/s22083006
Chicago/Turabian StyleHribernik, Matevž, Anton Umek, Sašo Tomažič, and Anton Kos. 2022. "Review of Real-Time Biomechanical Feedback Systems in Sport and Rehabilitation" Sensors 22, no. 8: 3006. https://doi.org/10.3390/s22083006
APA StyleHribernik, M., Umek, A., Tomažič, S., & Kos, A. (2022). Review of Real-Time Biomechanical Feedback Systems in Sport and Rehabilitation. Sensors, 22(8), 3006. https://doi.org/10.3390/s22083006