
Technological Requirements and Challenges in Wireless Body Area Networks for Health Monitoring: A Comprehensive Survey

 ,
,
Abstract
:1. Introduction
2. WBAN Applications for Health Monitoring
3. WBAN Sensor Techniques
4. Wireless Transmission in WBANs
4.1. Frequency Bands for WBAN Channel Models
4.2. WBAN Channel Models
4.3. Physical (PHY) Layer and Medium Access Control (MAC) Layer
4.4. Network Protocols
- Multi-level QoS and cross-layer optimization. In a WBAN for various types of medical applications, the network should provide different levels and types of service quality. Thus, it would be necessary to design new or improved link layer, network layer and application layer protocol, to fully guarantee the data transmission QoS with changing demands depending on the characteristics of the information needed [22,100]. In addition, the layers’ protocol for low-power design strategy and cross-layer design and optimization methods are also worthy of attention [101,102].
- Adaptive networking and topology control. WBANs usually consist of different types of nodes, but the node numbers of the same type are not large. The network is more focused on the different types of heterogeneous nodes in networking and service, which is one of the differences between WBANs and common WSNs [103]. Therefore, not only homogeneous nodes but also heterogeneous nodes can be supported in a self-organizing network scheme. To take the posture effects into account in the networking and managing network at the same time, the scheme requires a dynamic topology control method which is able to adapt changes to follow the physical state [10].
- In-network cooperation and feedback optimization. Different heterogeneous nodes cooperate with each other and complete human monitoring and information processing and transmission. This is an important feature of WBANs. To establish a dedicated WBAN architecture, it is essential to develop a collaborative framework and mechanisms between network nodes. These mechanisms include sensor-related technology of event-driven information transfer methods, sleep–wake-up mechanisms and monitoring information data fusion mechanisms [104,105]. It is worth noting that there are usually a lot of feedback loops in a WBAN which could conveniently control the reverse information transmission; thus, how to design closed-loop controlling methods and the corresponding protocol is an important issue for WBANs.
- Heterogeneous interconnection framework. Any one WBAN and other WBANs, personal area networks, LAN, mobile communication networks and the Internet connect together, which is affecting WBAN technology and the development of important technical factors. A heterogeneous network includes two aspects: the interconnection of heterogeneous nodes and a heterogeneous network. On one hand, a common data representation and flexible network connectivity structure should be proposed for internal heterogeneous nodes in a WBAN with the purpose of having interconnections between all kinds of sensor nodes and interconnections between nodes and gateways [106]. On the other hand, to aim at connections between the WBANs and other types of heterogeneous networks, it is necessary to build a common data communication and protocol conversion interface to complete the interconnection of WBANs and the Internet, mobile communications networks and other mainstream networks [107,108]. From the above, the former is conducive to interoperability and interconnection among WBAN devices, and the latter can provide network-level technical support for the implementation of telemedicine, which is significant for remote continuous monitoring.
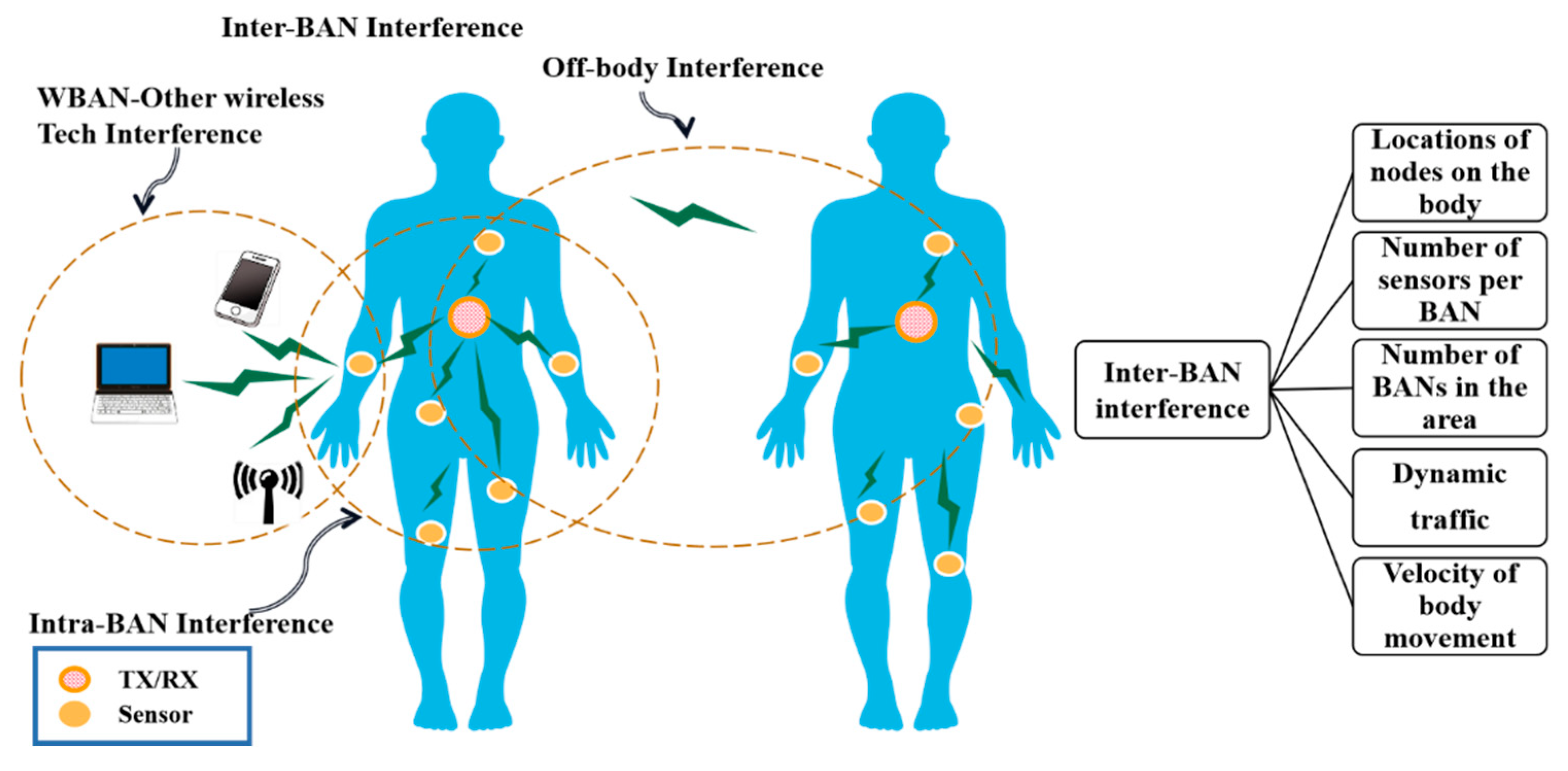
- With the development of the Internet of Things, the increasing number of WBANs and the mobility of WBANs, interference is becoming more challenging. For a single WBAN, intra-BAN interference can be effectively avoided by using TDMA techniques, but multiple WBANs interfere with each other when they are co-located (i.e., inter-WBAN interference). Figure 4 describes the different types of interference in WBANs [109] and the parameters that cause inter-BAN interference.
4.5. Chapter Summary
5. Security and Privacy
6. Energy Efficiency
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization (WHO). World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Raghupathi, W.; Raghupathi, V. An Empirical Study of Chronic Diseases in the United States: A Visual Analytics Approach to Public Health. Int. J. Environ. Res. Public Health 2018, 15, 431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Cardiovascular Diseases (CVDs). Available online: http://www.who.int/mediacentre/factsheets/fs317/en/ (accessed on 6 July 2019).
- World Health Organization (WHO). Diabetes. Available online: http://www.who.int/mediacentre/factsheets/fs312/en/ (accessed on 6 July 2021).
- Roberts, C.K.; Barnard, R.J. Effects of exercise and diet on chronic disease. J. Appl. Physiol. 2005, 98, 3–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimokoti, R.W.; Millen, B.E. Nutrition for the Prevention of Chronic Diseases. Med. Clin. N. Am. 2016, 100, 1185–1198. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.N.; Liu, R.; Liu, Z.P.; Li, M.Y.; Aihara, K. Detecting early-warning signals for sudden deterioration of complex diseases by dynamical network biomarkers. Sci. Rep. 2012, 2, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daowd, A.; Faizan, S.; Abidi, S.; Abusharekh, A.; Shehzad, A.; Abidi, S.S.R. Towards Personalized Lifetime Health: A Platform for Early Multimorbid Chronic Disease Risk Assessment and Mitigation. In Proceedings of the 17th World Congress of Medical and Health Informatics (MEDINFO), Lyon, France, 25–30 August 2019; pp. 935–939. [Google Scholar]
- He, K.; Huang, S.; Qian, X.N. Early detection and risk assessment for chronic disease with irregular longitudinal data analysis. J. Biomed. Inform. 2019, 96, 12. [Google Scholar] [CrossRef]
- Qu, Y.T.; Zheng, G.Q.; Ma, H.H.; Wang, X.T.; Ji, B.F.; Wu, H.H. A Survey of Routing Protocols in WBAN for Healthcare Applications. Sensors 2019, 19, 1638. [Google Scholar] [CrossRef] [Green Version]
- Haider, Z.; Jamal, T.; Asam, M.; Butt, S.; Ajaz, A. Mitigation of wireless body area networks challenges using cooperation. Int. J. Secur. Its Appl. 2020, 14, 15–30. [Google Scholar] [CrossRef]
- Sodagari, S.; Bozorgchami, B.; Aghvami, H. Technologies and Challenges for Cognitive Radio Enabled Medical Wireless Body Area Networks. IEEE Access 2018, 6, 29567–29586. [Google Scholar] [CrossRef]
- Movassaghi, S.; Abolhasan, M.; Lipman, J.; Smith, D.; Jamalipour, A. Wireless Body Area Networks: A Survey. IEEE Commun. Surv. Tutor. 2014, 16, 1658–1686. [Google Scholar] [CrossRef]
- Khan, R.A.; Pathan, A.K. The state-of-the-art wireless body area sensor networks: A survey. Int. J. Distrib. Sens. Netw. 2018, 14, 1550147718768994. [Google Scholar] [CrossRef] [Green Version]
- Ghamari, M.; Janko, B.; Sherratt, R.S.; Harwin, W.; Piechockic, R.; Soltanpur, C. A Survey on Wireless Body Area Networks for eHealthcare Systems in Residential Environments. Sensors 2016, 16, 831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nidhya, R.; Arunachalamand, V.; Karthik, S. A study on requirements, challenges and applications of wireless body area network. Asian J. Electr. Sci. 2017, 6, 30–36. [Google Scholar]
- Salayma, M.; Al-Dubai, A.; Romdhani, I.; Nasser, Y. Wireless Body Area Network (WBAN): A Survey on Reliability, Fault Tolerance, and Technologies Coexistence. ACM Comput. Surv. 2017, 50, 38. [Google Scholar] [CrossRef] [Green Version]
- Taleb, H.; Nasser, A.; Andrieux, G.; Charara, N.; Cruz, E.M. Wireless technologies, medical applications and future challenges in WBAN: A survey. Wirel. Netw. 2021, 27, 5271–5295. [Google Scholar] [CrossRef]
- Pan, Q.; Brulin, D.; Campo, E.J.J.B.E. Current Status and Future Challenges of Sleep Monitoring Systems: Systematic Review. Wirel. Commun. Mob. Comput. 2020, 5, e20921. [Google Scholar] [CrossRef]
- Ajerla, D.; Mahfuz, S.; Zulkernine, F.H. A Real-Time Patient Monitoring Framework for Fall Detection. Wirel. Commun. Mob. Comput. 2019, 2019, 9507938. [Google Scholar] [CrossRef]
- Joshi, R.; Constantinides, C.; Podilchak, S.K.; Soh, P.J. Dual-Band Folded-Shorted Patch Antenna for Military Search and Rescue Operations and Emergency Communications. In Proceedings of the 18th International Symposium on Antenna Technology and Applied Electromagnetics (ANTEM), Waterloo, ON, Canada, 19–22 August 2018. [Google Scholar]
- Ullah, S.; Higgins, H.; Braem, B.; Latre, B.; Blondia, C.; Moerman, I.; Saleem, S.; Rahman, Z.; Kwak, K.S. A Comprehensive Survey of Wireless Body Area Networks On PHY, MAC, and Network Layers Solutions. J. Med. Syst. 2012, 36, 1065–1094. [Google Scholar] [CrossRef] [Green Version]
- Chakraborty, C.; Gupta, B.; Ghosh, S.K. A Review on Telemedicine-Based WBAN Framework for Patient Monitoring. Telemed. e-Health 2013, 19, 619–626. [Google Scholar] [CrossRef]
- Teshome, A.K.; Kibret, B.; Lai, D.T.H. A Review of Implant Communication Technology in WBAN: Progress and Challenges. IEEE Rev. Biomed. Eng. 2019, 12, 88–99. [Google Scholar] [CrossRef]
- Bouazizi, A.; Zaibi, G.; Samet, M.; Kachouri, A. A Miniaturized Invasive Antenna Study for a Better performance in Medical Application. In Proceedings of the 32nd IEEE International Conference on Advanced Information Networking and Applications (IEEE AINA), Krakow, Poland, 16–18 May 2018; pp. 98–103. [Google Scholar]
- Yu, Y.C.; Nguyen, T.; Tathireddy, P.; Roundy, S.; Young, D.J. An In-Vitro Study of Wireless Inductive Sensing and Robust Packaging for Future Implantable Hydrogel-Based Glucose Monitoring Applications. IEEE Sens. J. 2020, 20, 2145–2155. [Google Scholar] [CrossRef]
- Mahmood, S.N.; Ishak, A.J.; Saeidi, T.; Soh, A.C.; Jalal, A.; Imran, M.A.; Abbasi, Q.H. Full Ground Ultra-Wideband Wearable Textile Antenna for Breast Cancer and Wireless Body Area Network Applications. Micromachines 2021, 12, 322. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.R. A real-time streaming control for quality-of-service coexisting wireless body area networks. Appl. Soft. Comput. 2018, 68, 719–732. [Google Scholar] [CrossRef]
- Darwish, A.; Hassanien, A.E. Wearable and Implantable Wireless Sensor Network Solutions for Healthcare Monitoring. Sensors 2011, 11, 5561–5595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Punj, R.; Kumar, R. Technological aspects of WBANs for health monitoring: A comprehensive review. Wirel. Netw. 2019, 25, 1125–1157. [Google Scholar] [CrossRef]
- Wang, J.C.; Han, K.N.; Alexandridis, A.; Chen, Z.Y.; Zilic, Z.; Pang, Y.; Jeon, G.; Piccialli, F. A blockchain-based eHealthcare system interoperating with WBANs. Futur. Gener. Comp. Syst. 2020, 110, 675–685. [Google Scholar] [CrossRef]
- Yang, Y.; Chae, S.; Shim, J.; Han, T.-D. EMG sensor-based two-hand smart watch interaction. In Proceedings of the UIST ’15 Adjunct, 28th Annual ACM Symposium on User Interface Software & Technology, Daegu, Korea, 8–11 November 2015; pp. 73–74. [Google Scholar]
- Al Rasyid, M.U.H.; Lee, B.H.; Sudarsono, A.; Taufiqurrahman. Implementation of Body Temperature and Pulseoximeter Sensors for Wireless Body Area Network. Sens. Mater. 2015, 27, 727–732. [Google Scholar]
- Muramatsu, D.; Koshiji, F.; Koshiji, K.; Sasaki, K. Effect of User’s Posture and Device’s Position on Human Body Communication with Multiple Devices. In Proceedings of the 2015 International Conference on Electronic Packaging and iMAPS All Asia Conference (ICEP-IAAC), Kyoto, Japan, 14–17 April 2015; pp. 124–127. [Google Scholar]
- Hess, P.L.; Al-Khatib, S.M.; Han, J.Y.; Edwards, R.; Bardy, G.H.; Bigger, J.T.; Buxton, A.; Cappato, R.; Dorian, P.; Hallstrom, A.; et al. Survival Benefit of the Primary Prevention Implantable Cardioverter-Defibrillator Among Older Patients Does Age Matter? An Analysis of Pooled Data From 5 Clinical Trials. Circ. Cardiovasc. Qual. Outcomes 2015, 8, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Sajatovic, M.; Levin, J.B.; Sams, J.; Cassidy, K.A.; Akagi, K.; Aebi, M.E.; Ramirez, L.F.; Safren, S.A.; Tatsuoka, C. Symptom severity, self-reported adherence, and electronic pill monitoring in poorly adherent patients with bipolar disorder. Bipolar Disorders 2015, 17, 653–661. [Google Scholar] [CrossRef] [Green Version]
- Sugiura, T.; Imai, M.; Yu, J.; Takeuchi, Y. A low-energy application specific instruction-set processor towards a low-computational lossless compression method for stimuli position data of artificial vision systems. J. Inf. Processing 2017, 25, 210–219. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Hua, K. Secured ECG signal transmission for human emotional stress classification in wireless body area networks. EURASIP J. Inf. Secur. 2016, 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Balasubramanian, V.; Stranieri, A. A scalable cloud Platform for Active healthcare monitoring applications. In Proceedings of the 2014 IEEE Conference on e-Learning, e-Management and e-Services (IC3e), Hawthrone, Australia, 10–12 December 2014; IEEE: Piscataway, NJ, USA, 2014; pp. 93–98. [Google Scholar]
- Msayib, Y.; Gaydecki, P.; Callaghan, M.; Dale, N.; Ismail, S. An Intelligent Remote Monitoring System for Total Knee Arthroplasty Patients. J. Med. Syst. 2017, 41, 90. [Google Scholar] [CrossRef] [PubMed]
- Elgazzar, K.; Aboelfotoh, M.; Martin, P.; Hassanein, H.S. Ubiquitous health monitoring using mobile web services. Procedia Comput. Sci. 2012, 10, 332–339. [Google Scholar] [CrossRef] [Green Version]
- Hassan, M.K.; El Desouky, A.I.; Elghamrawy, S.M.; Sarhan, A.M. Intelligent hybrid remote patient-monitoring model with cloud-based framework for knowledge discovery. Comput. Electr. Eng. 2018, 70, 1034–1048. [Google Scholar] [CrossRef]
- Saha, J.; Biswas, S.; Bhattacharyya, T.; Chowdhury, C. A Framework for Monitoring of Depression Patient using WBAN. In Proceedings of the IEEE International Conference on Wireless Communications, Signal Processing and Networking (WiSPNET), Dept Elect & Commun Engn, Chennai, India, 23–25 March 2016; pp. 410–415. [Google Scholar]
- Yang, G.; Jiang, M.Z.; Ouyang, W.; Ji, G.C.; Xie, H.B.; Rahmani, A.M.; Liljeberg, P.; Tenhunen, H. IoT-Based Remote Pain Monitoring System: From Device to Cloud Platform. IEEE J. Biomed. Health Inform. 2018, 22, 1711–1719. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Hu, X.P.; Zhang, L.L. The IoT-based heart disease monitoring system for pervasive healthcare service. In Proceedings of the 21st International Conference on Knowledge—Based and Intelligent Information and Engineering Systems (KES), Marseille, France, 6–8 September 2017; pp. 2328–2334. [Google Scholar]
- Hidalgo, J.A.; Cajiao, A.; Hernández, C.M.; López, D.M.; Quintero, V.M. VISIGNET: A wireless body area network with cloud data storage for the telemonitoring of vital signs. Health Technol. 2015, 5, 115–126. [Google Scholar] [CrossRef]
- Melillo, P.; Orrico, A.; Scala, P.; Crispino, F.; Pecchia, L. Cloud-Based Smart Health Monitoring System for Automatic Cardiovascular and Fall Risk Assessment in Hypertensive Patients. J. Med. Syst. 2015, 39, 109. [Google Scholar] [CrossRef]
- Boursalie, O.; Samavi, R.; Doyle, T.E. M4CVD: Mobile Machine Learning Model for Monitoring Cardiovascular Disease. In Proceedings of the 6th International Conference on Emerging Ubiquitous Systems and Pervasive Networks (EUSPN)/5th International Conference on Current and Future Trends of Information and Communication Technologies in Healthcare (ICTH), Berlin, Germany, 27–30 September 2015; pp. 384–391. [Google Scholar]
- Zulj, S.; Seketa, G.; Dzaja, D.; Sklebar, F.; Drobnjak, S.; Celic, L.; Magjarevic, R. Supporting diabetic patients with a remote patient monitoring systems. In Proceedings of the VII Latin American Congress on Biomedical Engineering CLAIB 2016, Bucaramanga, Colombia, 26–28 October 2016; pp. 577–580. [Google Scholar]
- Vivekanandan, S.; Devanand, M. Remote monitoring for diabetes disorder: Pilot study using InDiaTel prototype. Eur. Res. Telemed. 2015, 4, 63–69. [Google Scholar] [CrossRef]
- Mohammed, M.S.; Sendra, S.; Lloret, J.; Bosch, I. Systems and WBANs for Controlling Obesity. J. Healthc. Eng. 2018, 2018, 21. [Google Scholar] [CrossRef]
- Patel, M.; Wang, J.F. Applications, Challenges, and Prospective in Emerging Body Area Networking Technologies. IEEE Wirel. Commun. 2010, 17, 80–88. [Google Scholar] [CrossRef]
- Hanson, M.A.; Powell, H.C.; Barth, A.T.; Ringgenberg, K.; Calhoun, B.H.; Aylor, J.H.; Lach, J. Body area sensor networks: Challenges and Opportunities. Computer 2009, 42, 58–65. [Google Scholar] [CrossRef]
- Cao, H.S.; Leung, V.; Chow, C.; Chan, H. Enabling Technologies for Wireless Body Area Networks: A Survey and Outlook. IEEE Commun. Mag. 2009, 47, 84–93. [Google Scholar] [CrossRef]
- Chen, C.; Wang, Z.Y.; Li, W.; Chen, H.Y.; Mei, Z.N.; Yuan, W.; Tao, L.K.; Zhao, Y.T.; Huang, G.S.; Mei, Y.F.; et al. Novel Flexible Material-Based Unobtrusive and Wearable Body Sensor Networks for Vital Sign Monitoring. IEEE Sens. J. 2019, 19, 8502–8513. [Google Scholar] [CrossRef]
- Chou, J.C.; Chen, J.T.; Liao, Y.H.; Lai, C.H.; Chen, R.T.; Tsai, Y.L.; Lin, C.Y.; Chen, J.S.; Huang, M.S.; Chou, H.T. Wireless Sensing System for Flexible Arrayed Potentiometric Sensor Based on XBee Module. IEEE Sens. J. 2016, 16, 5588–5595. [Google Scholar] [CrossRef]
- Chen, C.M.; Anastasova, S.; Zhang, K.; Rosa, B.G.; Lo, B.P.L.; Assender, H.E.; Yang, G.Z. Towards Wearable and Flexible Sensors and Circuits Integration for Stress Monitoring. IEEE J. Biomed. Health Inform. 2020, 24, 2208–2215. [Google Scholar] [CrossRef] [PubMed]
- Rahman, H.; Ahmed, M.U.; Begum, S. Non-Contact Physiological Parameters Extraction Using Facial Video Considering Illumination, Motion, Movement and Vibration. IEEE Trans. Biomed. Eng. 2020, 67, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Manas, M.; Sinha, A.; Sharma, S.; Mahboob, M.R. A novel approach for IoT based wearable health monitoring and messaging system. J. Ambient Intell. Humaniz. Comput. 2019, 10, 2817–2828. [Google Scholar] [CrossRef]
- Gao, L.; Zhang, G.F.; Yu, B.; Qiao, Z.W.; Wang, J.C. Wearable human motion posture capture and medical health monitoring based on wireless sensor networks. Measurement 2020, 166, 12. [Google Scholar] [CrossRef]
- Al-Naggar, N.Q.; Al-Hammadi, H.M.; Al-Fusail, A.M.; Al-Shaebi, Z.A. Design of a Remote Real-Time Monitoring System for Multiple Physiological Parameters Based on Smartphone. J. Healthc. Eng. 2019, 2019, 13. [Google Scholar] [CrossRef] [Green Version]
- Lv, W.; Guo, J.J. Real-time ECG signal acquisition and monitoring for sports competition process oriented to the Internet of Things. Measurement 2021, 169, 9. [Google Scholar] [CrossRef]
- Mendes, J.J.A.; Vieira, M.E.M.; Pires, M.B.; Stevan, S.L. Sensor Fusion and Smart Sensor in Sports and Biomedical Applications. Sensors 2016, 16, 1569. [Google Scholar] [CrossRef]
- King, R.C.; Villeneuve, E.; White, R.J.; Sherratt, R.S.; Holderbaum, W.; Harwin, W.S. Application of data fusion techniques and technologies for wearable health monitoring. Med. Eng. Phys. 2017, 42, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Abdelmoneem, R.M.; Shaaban, E.; Benslimane, A. A Survey on Multi-Sensor Fusion Techniques in IoT for Healthcare. In Proceedings of the 13th International Conference on Computer Engineering and Systems (ICCES), Cairo, Egypt, 18–19 December 2018; pp. 157–162. [Google Scholar]
- Hanebeck, U.; Baum, M.; Huber, M.F. Guest Editorial Special Section on Multisensor Fusion and Integration for Intelligent Systems. IEEE Trans. Ind. Inform. 2018, 14, 1124–1126. [Google Scholar] [CrossRef]
- Zhou, T.L.; Chen, M.; Zou, J. Reinforcement Learning Based Data Fusion Method for Multi-Sensors. IEEE-CAA J. Autom. Sin. 2020, 7, 1489–1497. [Google Scholar] [CrossRef]
- Pan, D.H.; Liu, H.W.; Qu, D.M.; Zhang, Z. Human Falling Detection Algorithm Based on Multisensor Data Fusion with SVM. Mob. Inf. Syst. 2020, 2020, 9. [Google Scholar] [CrossRef]
- Maman, M.; Ouvry, L. BATMAC: An adaptive TDMA MAC for body area networks performed with a space-time dependent channel model. In Proceedings of the 2011 5th International Symposium on Medical Information and Communication Technology, Montreux, Switzerland, 27–30 March 2011; pp. 1–5. [Google Scholar]
- Wang, J.F.; Ghosh, M.; Challapali, K. Emerging Cognitive Radio Applications: A Survey. IEEE Commun. Mag. 2011, 49, 74–81. [Google Scholar] [CrossRef]
- Kang, T.; Oh, K.; Park, H.; Kang, S. Review of capacitive coupling human body communications based on digital transmission. ICT Express 2016, 2, 180–187. [Google Scholar] [CrossRef]
- Alam, M.M.; Ben Hamida, E. Surveying Wearable Human Assistive Technology for Life and Safety Critical Applications: Standards, Challenges and Opportunities. Sensors 2014, 14, 9153–9209. [Google Scholar] [CrossRef] [Green Version]
- Chávez-Santiago, R.; Mateska, A.; Chomu, K.; Gavrilovska, L.; Balasingham, I. Applications of software-defined radio (SDR) technology in hospital environments. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 1266–1269. [Google Scholar]
- Chepuri, S.P.; Francisco, R.d.; Leus, G. Performance evaluation of an IEEE 802.15.4 cognitive radio link in the 2360-2400 MHz band. In Proceedings of the 2011 IEEE Wireless Communications and Networking Conference, Cancun, Mexico, 28–31 March 2011; pp. 2155–2160. [Google Scholar]
- Chávez-Santiago, R.; Balasingham, I. Cognitive radio for medical wireless body area networks. In Proceedings of the 2011 IEEE 16th International Workshop on Computer Aided Modeling and Design of Communication Links and Networks (CAMAD), Osaka, Japan, 10–11 June 2011; IEEE: Piscataway, NJ, USA, 2011; pp. 148–152. [Google Scholar]
- Taparugssanagorn, A.; Pomalaza-Ráez, C.; Isola, A.; Tesi, R.; Hämäläinen, M.; Iinatti, J. UWB channel modeling for wireless body area networks in medical applications. In Proceedings of the Proceedings International Symposium on Medical Information and Communication Technology (ISMICT), Osaka, Japan, 13–16 September 2009. [Google Scholar]
- Cho, N.; Yoo, J.; Song, S.; Lee, J.; Jeon, S.; Yoo, H. The Human Body Characteristics as a Signal Transmission Medium for Intrabody Communication. IEEE Trans. Microw. Theory Technol. 2007, 55, 1080–1086. [Google Scholar] [CrossRef] [Green Version]
- Wegmueller, M.S.; Kuhn, A.; Froehlich, J.; Oberle, M.; Felber, N.; Kuster, N.; Fichtner, W. An Attempt to Model the Human Body as a Communication Channel. IEEE Trans. Biomed. Eng. 2007, 54, 1851–1857. [Google Scholar] [CrossRef]
- Fort, A.; Ryckaert, J.; Desset, C.; Doncker, P.D.; Wambacq, P.; Biesen, L.V. Ultra-wideband channel model for communication around the human body. IEEE J. Sel. Areas Commun. 2006, 24, 927–933. [Google Scholar] [CrossRef]
- Cotton, S.L.; Conway, G.A.; Scanlon, W.G. A Time-Domain Approach to the Analysis and Modeling of On-Body Propagation Characteristics Using Synchronized Measurements at 2.45 GHz. IEEE Trans. Antennas Propag. 2009, 57, 943–955. [Google Scholar] [CrossRef]
- Hasan, K.; Biswas, K.; Ahmed, K.; Nafi, N.S.; Islam, M.S. A comprehensive review of wireless body area network. J. Netw. Comput. Appl. 2019, 143, 178–198. [Google Scholar] [CrossRef]
- IEEE P802.15 Wireless Personal Area Networks. Available online: https://mentor.ieee.org/802.15/dcn/08/15-08-0780-09-0006-tg6-channel-model.pdf (accessed on 24 April 2022).
- Ferreira, V.; Muchaluat-Saade, D.; Albuquerque, C. B-Move: A Transmission Scheduler Based on Human Body Movements for WBANs. In Proceedings of the 2020 IEEE 33rd International Symposium on Computer-Based Medical Systems (CBMS), Rochester, MN, USA, 28–30 July 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 315–320. [Google Scholar]
- Mohamed, M.; Joseph, W.; Vermeeren, G.; Tanghe, E.; Cheffena, M. Characterization of dynamic wireless body area network channels during walking. Eurasip J. Wirel. Commun. Netw. 2019, 2019, 104. [Google Scholar] [CrossRef]
- Sun, W.Y.; Zhao, J.; Huang, Y.X.; Sun, Y.N.; Yang, H.Z.; Liu, Y.P. Dynamic Channel Modeling and OFDM System Analysis for Capacitive Coupling Body Channel Communication. IEEE Trans. Biomed. Circuits Syst. 2019, 13, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Maman, M.; Dehmas, F.; Errico, R.D.; Ouvry, L. Evaluating a TDMA MAC for body area networks using a space-time dependent channel model. In Proceedings of the 2009 IEEE 20th International Symposium on Personal, Indoor and Mobile Radio Communications, Tokyo, Japan, 13–16 September 2009; IEEE: Piscataway, NJ, USA, 2009; pp. 2101–2105. [Google Scholar]
- Errico, R.D.; Ouvry, L. Time-variant BAN channel characterization. In Proceedings of the 2009 IEEE 20th International Symposium on Personal, Indoor and Mobile Radio Communications, Tokyo, Japan, 13–16 September 2009; IEEE: Piscataway, NJ, USA, 2009; pp. 3000–3004. [Google Scholar]
- Roberts, N.E.; Oh, S.; Wentzloff, D.D. Exploiting Channel Periodicity in Body Sensor Networks. IEEE J. Emerg. Sel. Top. Circuits Syst. 2012, 2, 4–13. [Google Scholar] [CrossRef]
- Oliveira, C.; Mackowiak, M.; Correia, L.M. Modelling on- and off-body channels in Body Area Networks. In Proceedings of the 2013 SBMO/IEEE MTT-S International Microwave & Optoelectronics Conference (IMOC), Rio de Janeiro, Brazil, 4–7 August 2013; IEEE: Piscataway, NJ, USA, 2013; pp. 1–5. [Google Scholar]
- IEEE Std 802.15.6-2012; IEEE Standard for Local and Metropolitan Area Networks—Part 15.6: Wireless Body Area Networks. IEEE: New York, NY, USA, 2012. [CrossRef]
- Otal, B.; Alonso, L.; Verikoukis, C. Highly reliable energy-saving mac for wireless body sensor networks in healthcare systems. IEEE J. Sel. Areas Commun. 2009, 27, 553–565. [Google Scholar] [CrossRef]
- Lin, L.; Wong, K.J.; Kumar, A.; Tan, S.L. A novel TDMA-based MAC protocol for mobile in-vivo body sensor networks. In Proceedings of the 2012 IEEE 14th International Conference on e-Health Networking, Applications and Services (Healthcom), Beijing, China, 10–13 October 2012; IEEE: Piscataway, NJ, USA, 2012; pp. 273–278. [Google Scholar]
- Donovan, T.O.; Donoghue, J.O.; Sreenan, C.; Sammon, D.; Reilly, P.O.; Connor, K.A.O. A context aware wireless body area network (BAN). In Proceedings of the 2009 3rd International Conference on Pervasive Computing Technologies for Healthcare, London, UK, 1–3 April 2009; IEEE: Piscataway, NJ, USA, 2009; pp. 1–8. [Google Scholar]
- Omeni, O.; Wong, A.C.W.; Burdett, A.J.; Toumazou, C. Energy Efficient Medium Access Protocol for Wireless Medical Body Area Sensor Networks. IEEE Trans. Biomed. Circuits Syst. 2008, 2, 251–259. [Google Scholar] [CrossRef]
- Li, H.; Tan, J. Heartbeat-Driven Medium-Access Control for Body Sensor Networks. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 44–51. [Google Scholar] [CrossRef]
- Liu, B.; Yan, Z.; Chen, C.W. Medium Access Control for Wireless Body Area Networks with QoS Provisioning and Energy Efficient Design. IEEE Trans. Mob. Comput. 2017, 16, 422–434. [Google Scholar] [CrossRef]
- TONG, B.; LIN, J.; PANG, Y. A protocol with self-adaptive guard band for body area networks. IET Commun. 2018, 12, 1042–1047. [Google Scholar]
- Lin, C.H.; Lin, K.C.J.; Chen, W.T. Channel-Aware Polling-Based MAC Protocol for Body Area Networks: Design and Analysis. IEEE Sens. J. 2017, 17, 2936–2948. [Google Scholar] [CrossRef]
- Alam, M.M.; Ben-Hamida, E. Strategies for Optimal MAC Parameters Tuning in IEEE 802.15.6 Wearable Wireless Sensor Networks. J. Med. Syst. 2015, 39, 16. [Google Scholar] [CrossRef] [PubMed]
- Waheed, T.; Rehman, A.U.; Karim, F.; Ghani, S. QoS Enhancement of AODV Routing for MBANs. Wirel. Pers. Commun. 2021, 116, 1379–1406. [Google Scholar] [CrossRef]
- Shahbazi, Z.; Byun, Y.C. Towards a Secure Thermal-Energy Aware Routing Protocol in Wireless Body Area Network Based on Blockchain Technology. Sensors 2020, 20, 3604. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Xu, Y.X.; Liu, A.F. Cross Layer Design for Optimizing Transmission Reliability, Energy Efficiency, and Lifetime in Body Sensor Networks. Sensors 2017, 17, 900. [Google Scholar] [CrossRef] [Green Version]
- Bakin, E.; Ivanov, I.; Shelest, M.; Turlikov, A. Analysis of Energy Harvesting Efficiency for Power Supply of WBAN Nodes in Heterogeneous Scenarios. In Proceedings of the 8th International Congress on Ultra Modern Telecommunications and Control Systems and Workshops (ICUMT), Lisbon, Portugal, 18–20 October 2016; pp. 111–118. [Google Scholar]
- Al Ameen, M.; Hong, C.S. An On-Demand Emergency Packet Transmission Scheme for Wireless Body Area Networks. Sensors 2015, 15, 30584–30616. [Google Scholar] [CrossRef] [Green Version]
- Chelloug, S.A. An intelligent closed-loop learning automaton for real-time congestion control in wireless body area networks. Int. J. Sens. Netw. 2018, 26, 190–199. [Google Scholar] [CrossRef]
- Mehmood, G.; Khan, M.Z.; Abbas, S.; Faisal, M.; Rahman, H.U. An Energy-Efficient and Cooperative Fault-Tolerant Communication Approach for Wireless Body Area Network. IEEE Access 2020, 8, 69134–69147. [Google Scholar] [CrossRef]
- Rekha, K.S.; Sreenivas, T.H.; Kulkarni, A.D. Remote Monitoring and Reconfiguration of Environment and Structural Health Using Wireless Sensor Networks. In Proceedings of the International Conference on Processing of Materials, Minerals and Energy (PMME), Ongole, India, 29–30 July 2016; pp. 1169–1175. [Google Scholar]
- Kaur, R.; Kaur, B.P.; Singla, R.P.; Kaur, J. AMERP: Adam moment estimation optimized mobility supported energy efficient routing protocol for wireless body area networks. Sust. Comput. 2021, 31, 9. [Google Scholar] [CrossRef]
- Movassaghi, S.; Majidi, A.; Jamalipour, A.; Smith, D.; Abolhasan, M. Enabling interference-aware and energy-efficient coexistence of multiple wireless body area networks with unknown dynamics. IEEE Access 2016, 4, 2935–2951. [Google Scholar] [CrossRef]
- Toorani, M. Cryptanalysis of Two PAKE Protocols for Body Area Networks and Smart Environments. Int. J. Netw. Secur. 2015, 17, 629–636. [Google Scholar]
- Ananthi, J.V.; Jose, P. A Perspective Review of Security Challenges in Body Area Networks for Healthcare Applications. Int. J. Wirel. Inf. Netw. 2021, 28, 451–466. [Google Scholar] [CrossRef] [PubMed]
- Bengag, A.; Bengag, A.; Moussaoui, O. Effective and Robust Detection of Jamming Attacks for WBAN-Based Healthcare Monitoring Systems. In Proceedings of the International Conference on Electronic Engineering and Renewable Energy, Saidia, Morocco, 13–15 April 2020; Springer: Berlin/Heidelberg, Germany, 2020; pp. 169–174. [Google Scholar]
- Arya, K.; Gore, R. Data security for WBAN in e-health IoT applications. In Intelligent Data Security Solutions for e-Health Applications; Elsevier: Amsterdam, The Netherlands, 2020; pp. 205–218. [Google Scholar]
- Al Hayajneh, A.; Bhuiyan, M.Z.A.; McAndrew, I. Security of Broadcast Authentication for Cloud-Enabled Wireless Medical Sensor Devices in 5G Networks. Comput. Inf. Sci. 2020, 13, 1–13. [Google Scholar] [CrossRef]
- Thamilarasu, G.; Odesile, A.; Hoang, A. An Intrusion Detection System for Internet of Medical Things. IEEE Access 2020, 8, 181560–181576. [Google Scholar] [CrossRef]
- Umar, M.; Wu, Z.; Liao, X. Mutual Authentication in Body Area Networks Using Signal Propagation Characteristics. IEEE Access 2020, 8, 66411–66422. [Google Scholar] [CrossRef]
- Dharshini, S.; Subashini, M.M. DMASK-BAN: Improving the Security of Body Area Networks. Comput. Fraud. Secur. 2020, 2020, 13–19. [Google Scholar] [CrossRef]
- Suchithra, M.; Baskar, M.; Ramkumar, J.; Kalyanasundaram, P.; Amutha, B. Invariant packet feature with network conditions for efficient low rate attack detection in multimedia networks for improved QoS. J. Ambient Intell. Humaniz. Comput. 2021, 12, 5471–5477. [Google Scholar] [CrossRef]
- Kumar, M.; Chand, S. A Lightweight Cloud-Assisted Identity-Based Anonymous Authentication and Key Agreement Protocol for Secure Wireless Body Area Network. IEEE Syst. J. 2021, 15, 2779–2786. [Google Scholar] [CrossRef]
- Rao, J.D.; Sridevi, K. Novel security system for wireless body area networks based on fuzzy logic and trust factor considering residual energy. In Proceedings of the International Conference on Advances in Materials Research (ICAMR), Bannari Amman Inst Technol, Sathyamangalam, India, 6–7 December 2019; pp. 1498–1501. [Google Scholar]
- Ali, Z.; Ghani, A.; Khan, I.; Chaudhry, S.A.; Islam, S.K.H.; Giri, D. A robust authentication and access control protocol for securing wireless healthcare sensor networks. J. Inf. Secur. Appl. 2020, 52, 14. [Google Scholar] [CrossRef]
- Morales-Sandoval, M.; De-la-Parra-Aguirre, R.; Galeana-Zapien, H.; Galaviz-Mosqueda, A. A Three-Tier Approach for Lightweight Data Security of Body Area Networks in E-Health Applications. IEEE Access 2021, 9, 146350–146365. [Google Scholar] [CrossRef]
- Tan, X.; Zhang, J.L.; Zhang, Y.J.; Qin, Z.; Ding, Y.; Wang, X.W. A PUF-Based and Cloud-Assisted Lightweight Authentication for Multi-Hop Body Area Network. Tsinghua Sci. Technol. 2021, 26, 36–47. [Google Scholar] [CrossRef]
- Liu, J.W.; Zhang, Z.H.; Chen, X.F.; Kwak, K.S. Certificateless Remote Anonymous Authentication Schemes for Wireless Body Area Networks. IEEE Trans. Parallel Distrib. Syst. 2014, 25, 332–342. [Google Scholar] [CrossRef]
- He, D.B.; Zeadally, S.; Kumar, N.; Lee, J.H. Anonymous Authentication for Wireless Body Area Networks With Provable Security. IEEE Syst. J. 2017, 11, 2590–2601. [Google Scholar] [CrossRef]
- Gangadari, B.R.; Ahamed, S.R. Design of cryptographically secure AES like S-Box using second-order reversible cellular automata for wireless body area network applications. Healthc. Technol. Lett. 2016, 3, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Tripathy, A.; Pradhan, S.K.; Nayak, A.K.; Tripathy, A.R. Key Predistribution Technique based on Matrix Decomposition in Wireless Sensor Network. In Proceedings of the 2021 1st Odisha International Conference on Electrical Power Engineering, Communication and Computing Technology(ODICON), Bhubaneswar, India, 8–9 January 2021; IEEE: Piscataway, NJ, USA, 2021; pp. 1–5. [Google Scholar]
- Saikia, M.; Hussain, M.A. Combinatorial group based approach for key pre-distribution scheme in wireless sensor network. In Proceedings of the 2017 International Conference on Computing, Communication and Automation (ICCCA), Greater Noida, India, 5–6 May 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 498–503. [Google Scholar]
- Seepers, R.M.; Strydis, C.; Sourdis, I.; Zeeuw, C.I.D. Enhancing Heart-Beat-Based Security for mHealth Applications. IEEE J. Biomed. Health Inform. 2017, 21, 254–262. [Google Scholar] [CrossRef]
- Bai, T.; Lin, J.Z.; Li, G.Q.; Wang, H.Q.; Ran, P.; Li, Z.Y.; Li, D.; Pang, Y.; Wu, W.; Jeon, G. A lightweight method of data encryption in BANs using electrocardiogram signal. Futur. Gener. Comp. Syst. 2019, 92, 800–811. [Google Scholar] [CrossRef]
- Shen, J.; Chang, S.H.; Shen, J.; Liu, Q.; Sun, X.M. A lightweight multi-layer authentication protocol for wireless body area networks. Futur. Gener. Comp. Syst. 2018, 78, 956–963. [Google Scholar] [CrossRef]
- Shou, Y.; Guyennet, H.; Lehsaini, M. Parallel scalar multiplication on elliptic curves in wireless sensor networks. In Proceedings of the International Conference on Distributed Computing and Networking, Mumbai, India, 3–6 January 2013; Springer: Berlin/Heidelberg, Germany, 2013; pp. 300–314. [Google Scholar]
- Al-Janabi, S.; Al-Shourbaji, I.; Shojafar, M.; Shamshirband, S. Survey of main challenges (security and privacy) in wireless body area networks for healthcare applications. Egypt. Inform. J. 2017, 18, 113–122. [Google Scholar] [CrossRef] [Green Version]
- Cavallari, R.; Martelli, F.; Rosini, R.; Buratti, C.; Verdone, R. A Survey on Wireless Body Area Networks: Technologies and Design Challenges. IEEE Commun. Surv. Tutor. 2014, 16, 1635–1657. [Google Scholar] [CrossRef]
- Wang, J.C.; Han, K.N.; Alexandridis, A.; Zilic, Z.; Pang, Y.; Lin, J.Z. An ASIC Implementation of Security Scheme for Body Area Networks. In Proceedings of the IEEE International Symposium on Circuits and Systems (ISCAS), Florence, Italy, 27–30 May 2018. [Google Scholar]
- Rabby, M.K.M.; Alam, M.S.; Shawkat, M. A priority based energy harvesting scheme for charging embedded sensor nodes in wireless body area networks. PLoS ONE 2019, 14, e0214716. [Google Scholar] [CrossRef]
- Hao, Y.X.; Peng, L.M.; Lu, H.M.; Hassan, M.M.; Alamri, A. Energy Harvesting Based Body Area Networks for Smart Health. Sensors 2017, 17, 1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Y.H.; Xie, J.W.; Zhang, Y.G.; Hua, M.; Zhou, W. Reinforcement Learning (RL)-Based Energy Efficient Resource Allocation for Energy Harvesting-Powered Wireless Body Area Network. Sensors 2020, 20, 44. [Google Scholar] [CrossRef] [Green Version]
- Hovakeemian, Y.; Naik, K.; Nayak, A. A survey on dependability in Body Area Networks. In Proceedings of the 2011 5th International Symposium on Medical Information and Communication Technology, Montreux, Switzerland, 27–30 March 2011; IEEE: Piscataway, NJ, USA, 2011; pp. 10–14. [Google Scholar]
- Dey, N.; Hassanien, A.E.; Bhatt, C.; Ashour, A.; Satapathy, S.C. Internet of Things and Big Data Analytics Toward Next-Generation Intelligence; Springer: Berlin/Heidelberg, Germany, 2018; Volume 35. [Google Scholar]
- Samal, T.; Kabat, M.R.; Priyadarshini, S.B.B. Energy Saving Delay Constraint MAC Protocol in Wireless Body Area Network. In Intelligent and Cloud Computing; Springer: Berlin/Heidelberg, Germany, 2021; pp. 623–630. [Google Scholar]
- Liu, X.; Zheng, Y.J.; Zhao, B.; Wang, Y.S.; Phyu, M.W. An Ultra Low Power Baseband Transceiver IC for Wireless Body Area Network in 0.18-mu m CMOS Technology. IEEE Trans. Very Large Scale Integr. Syst. 2011, 19, 1418–1428. [Google Scholar] [CrossRef]
- Chen, M.; Han, J.; Fang, D.; Zou, Y.; Zeng, X. An ultra low-power and area-efficient baseband processor for WBAN transmitter. In Proceedings of the 2013 Asia-Pacific Signal and Information Processing Association Annual Summit and Conference, Kaohsiung, Taiwan, 29 October–1 November 2013; IEEE: Piscataway, NJ, USA, 2013; pp. 1–4. [Google Scholar]
- Liang, Y.; Zhou, Y.; Li, Y. The design and implementation of IEEE 802.15. 6 Baseband on FPGA. In The International Conference on Health Informatics; Springer: Berlin/Heidelberg, Germany, 2014; pp. 231–235. [Google Scholar]
- Chougrani, H.; Schwoerer, J.; Horren, P.H.; Baghdadi, A.; Dehmas, F. UWB-IR digital baseband architecture for IEEE 802.15.6 wireless BAN. In Proceedings of the 2014 21st IEEE International Conference on Electronics, Circuits and Systems (ICECS), Marseille, France, 7–10 December 2014; IEEE: Piscataway, NJ, USA, 2014; pp. 866–869. [Google Scholar]
- Mathew, P.; Augustine, L.; Kushwaha, D.; Desalphine, V.; Selvakumar, A.D. Implementation of NB PHY transceiver of IEEE 802.15.6 WBAN on FPGA. In Proceedings of the 2015 International Conference on VLSI Systems, Architecture, Technology and Applications (VLSI-SATA), Bengaluru, India, 8–10 January 2015; IEEE: Piscataway, NJ, USA, 2015; pp. 1–6. [Google Scholar]
- Wang, J.C.; Han, K.N.; Alexandridis, A.; Zilic, Z.; Lin, J.Z.; Pang, Y.; Yang, X.M. A baseband processing ASIC for body area networks. J. Ambient Intell. Humaniz. Comput. 2019, 10, 3975–3982. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medical | Wearable WBAN | Aiding Professional and Amature Athletic Training [17] Wearable Health Monitoring [18] Asthma Monitoring [18] Sleep Staging or Monitoring [19] Fall Detection [20] Assessing Soldier Fatigue and Battle Readiness [21] Patient Monitoring [22] Telemedicine Systems [23] |
| Implantable WBAN [24] | Cardiovascular Diseases [25] Diabetes Control [26] Cancer Detection [27] | |
| Non-Medical | Real-Time Streaming [28] | Video steaming Data file transfer 3D video Sports |
| Emergency (non-medical) [13] | Life-threatening conditions monitoring: firefighters, soldiers, deep-sea explorers, and space explorers. | |
| Entertainment Applications [17] | Games Social networking |
| Diseases | Collected Data | Sensor | Transmission Protocol |
|---|---|---|---|
| Depression [43] | the location, the posture, pressure→accelerometers | Barometric pressure sensor data | — |
| Pain assessment [44] | facial surface EMG | wearable sensor with a biosensing facial mask | hotspot of a cellphone/a smart gateway/a general router |
| Heart diseases [45] | BP, ECG, SpO2, heart rate, pulse rate, blood fat blood glucose, patients’ risk and location | ECG; blood sensing device | Bluetooth |
| Knees rehabilitation [39] | EMG; ECG | Accelerometer; EMG; ECG | Smartphones act as a gateway |
| Knee arthroplasty [40] | the angles of knee flexion | a master and slave sensor unit, the flexion angle sensor | mobile telephone network |
| Chronic diseases [46] | heart rate, body temperature, and blood pressure | corresponding three sensors | Bluetooth |
| Hypertension [47] | ECG, HRV | ECG | Bluetooth |
| Ubiquitous monitoring system [41] | four types of vital signs, oxygen saturation, blood pressure, heart rate, and sugar level | body sensor network | 3G/Wi-Fi/Bluetooth |
| Cardiovascular diseases [48] | Physiological signals include ECG, BP, stress level, SpO2 | Accelerometers; ECG | Mobile device |
| Heart diseases [42] | BP, pulse, body temperature, patient position, ECG | ECG; airflow; body position; BP sensor; Ambient sensors | Wi-Fi/3G/GPRS, ZigBee/Bluetooth |
| Diabetes [49] | blood glucose; Blood pressure; ECG | corresponding sensors | Bluetooth |
| Diabetes [50] | EMG, Body temperature, Heart rate, Blood pressure, Blood glucose | corresponding sensors | ZigBee |
| Fall detection [20] | real-time activity and fall data | motion sensors | Bluetooth |
| Obesity [51] | heart rate, waist circumference, physical activity, weight, glucose | chest strap; band; pedometer; pressure sensor; patch | GPRS/3G/4G/Wi-Fi |
| Application | Data Rate | Nodes Number | Topology | Setup Time | P2P Latency | BER | Duty Cycle | Battery Lifetime |
|---|---|---|---|---|---|---|---|---|
| ECG | 72 kb/s | <6 | Star | <3 s | <250 ms | <10–10 | <10% | >1 week |
| EMG | 1.54 Mb/s | <6 | Star | <3 s | <250 ms | <10–10 | <10% | >1 week |
| EEG | 86.4 kb/s | <6 | Star | <3 s | <250 ms | <10–10 | <10% | >1 week |
| Drug dosage | <1 kb/s | 2 | P2P | <3 s | <250 ms | <10–10 | <1% | >24 h |
| Hearing aid | 200 kb/s | 3 | Star | <3 s | <250 ms | <10–10 | <10% | >40 h |
| Capsule endoscope | 1 Mb/s | 2 | P2P | <3 s | <250 ms | <10–10 | <50% | >24 h |
| Deep brain stimulation | 1 Mb/s | 2 | P2P | <3 s | <250 ms | <10–3 | <50% | >3 years |
| Imaging | <10 Mb/s | 2 | P2P | <3 s | <100 ms | <10–5 | <50% | >12 h |
| Audio | 1 Mb/s | 3 | Star | <3 s | <100 ms | <10–5 | <50% | >24 h |
| temp/respiration/glucose monitor/accelerometer | <10 kb/s | <12 | Star | <3 s | <250 ms | <10–10 | <10% | >1 week |
| Characteristic | Requirement | Desired Range |
|---|---|---|
| Operating distance | In, on or around the body | Typically limited in 3 m |
| Peak power consumption | Ultra-low | µW level in sleep mode, up to 30 mW fully active mode |
| Data rate | Scalable | From 1 kb/s to 10 Mb/s |
| Network size | Modest | ~50 devices per BAN |
| Frequency band | Global unlicensed and medical bands | MedRadio, ISM, WMTS, UWB |
| MAC | Scalable, reliable, versatile, self-forming | Low power, synchronization, listening, wake up, turn-around |
| QoS | Real-time data, periodic parametric data, episodic data and emergency alarms | P2P latency: from 10 ms to 250 ms, BER: from 10–10 to 10–3, reservation and prioritization |
| Coexistence | Coexistence with legacy devices and self-coexistence | Simultaneous co-located operation of up to 10 independent WBANs |
| Topology | Star, Mesh or Tree | Self-forming, distributed with multi-hop support |
| Environment | Body shadowing, attenuation | Seamless operation of multiple nodes in and out of scope with each other |
| Setup time | Not to be perceived | Up to 3 s |
| Security | Various levels | Authentication, Encryption, Authorization, Privacy, Confidentiality, Message integrity |
| Safety/Biocompatibility | Long-term continuous use without harmful effects | regulatory requirements |
| Ergonomic consideration | Size, weight, shape and form factors limited by location and organ | Non-invasive, appropriate size, weight and form factors |
| Reprogramming, Calibration, Customization | Personalized, configurable, integrated and context-aware services | reprogram, recalibrate, tune and configure devices wirelessly |
| Non-Invasive Sensors | Invasive/Implantable Sensors |
|---|---|
| EEG/ECG/EMG | Pacemaker |
| Position/Motion sensor | Deep brain stimulator |
| BP/SpO2 | Implantable defibrillators |
| Glucose sensor | Cochlear implants |
| Temperature/Pressure sensor | Electronic pill for drug delivery |
| Pulse oximeter | Wireless capsule endoscope (electronic pill) |
| Oxygen, pH value | Retina implants |
| Sensor | Working Mechanism | Power Consumption | Data Rate |
|---|---|---|---|
| Blood sugar | Uses non-invasive methods such as optical measurement at the eye and breath analysis | Very low | Low |
| Blood pressure | Measures systolic and diastolic pressure | High | Low |
| ECG/EEG/EMG | Differential measurement via electrodes placed on the body | Low | High |
| Temperature | Uses an integrated circuit to detect the temperature changes by measuring resistance | Low | Very low |
| Respiration | Measures the dissolved oxygen in a liquid with two electrodes, a cathode and an anode covered by a thin membrane | Low | Low |
| Accelerometer | Measures the acceleration relative to freefall in three axes | High | High |
| Carbon dioxide | measures the gas absorption using infrared light | Low | Low |
| Gyroscope | Measures the orientation based on the principles of angular momentum | High | High |
| Pulse oximetry | Measures the changes of absorbance ratio by the red or infrared light passing through the fingertip or earlobe | Low | Low |
| Humidity | Measures the conductivity changes | Low | Very low |
| Specifications | Requirements |
|---|---|
| Topology | Star or star mesh hybrid, bidirectional link |
| Devices | Number Typically 6, Up to 16 |
| Data Rate | 10 Kb/s–10 Mb/s |
| Range | >3 m with low data rate under IEEE Channel Model |
| PER | <10% with a link success probability of 95% overall channel conditions |
| Latency | <125 ms (medical), <250 ms (non-medical) |
| Reliability | <1 s for alarm, <10 ms for applications with feedback |
| Power Consumption | >1 year (1% LDC and 500 mAh battery), >9 h (always “on” and 50 mAh battery) |
| Coexistence | Less than 10 BANs in a volume of 6 m × 6 m × 6 m |
| Operation Bands | Frequency Range | Disadvantages | Application | |
|---|---|---|---|---|
| >Medical device radio communications [12] | 401–406, 413–419, 426–432, 438–444, 451–457 MHz | Limited bandwidth [70] | In-body and on-body | |
| Human body communications (HBC) | 5–50 MHz | Affected by the human posture and surroundings [71] | In-body [72] and on-body [13] | |
| Medical implant communication service spectrum [70] | 402–405 MHz | Limited bandwidth | In-body [13] | |
| Wireless medical telemetry service | 608–614, 1395–1400, 1427–1432 MHz | Limited bandwidth [70] Not harmonized globally or regionally [73] | On-body | |
| Industrial, scientific and medical (ISM) | 2360–2500 MHz | 2360–2390 MHz | Not suitable for critical life situations due to coexistence with aeronautical mobile telemetry [74] | On-body |
| 2390–2400 MHz | Limited bandwidth | On-body | ||
| 2400–2500 MHz | Unlicensed WBAN, occupied by IEEE 802.15.6, Wi-Fi, Blue-tooth, ZigBee. | On-body | ||
| Ultra wideband (UWB) | 3.1–10.6 GHz | Incomplete spectrum monitoring campaign [75] | On-body | |
| Scenario | Description | Frequency Band | Channel Model |
|---|---|---|---|
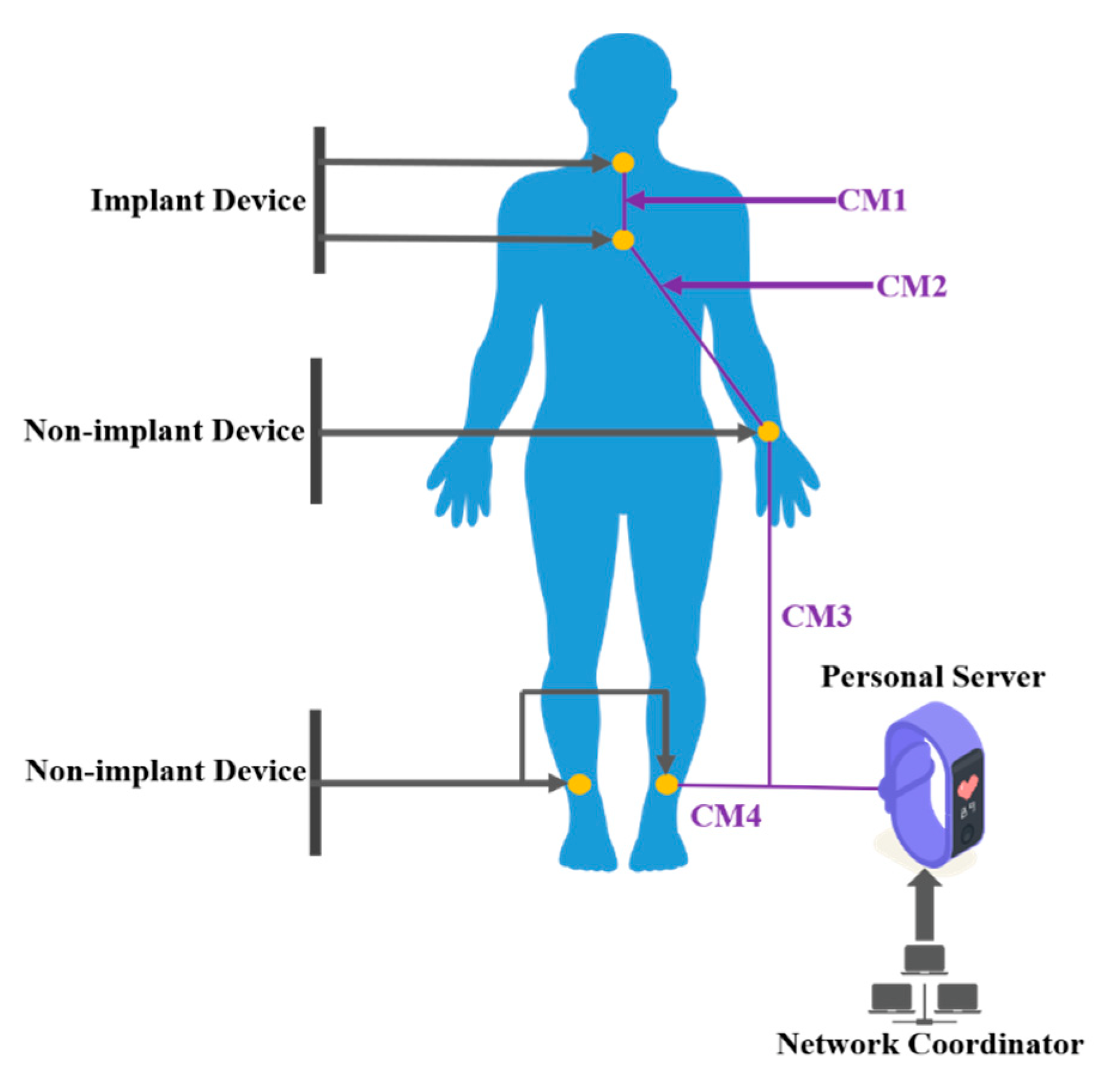
| S1 | Implant to Implant | 420-405 MHz | CM1 |
| S2 | Implant to Body Surface | 420-405 MHz | CM2 |
| S3 | Body surface to Body Surface | 13.5, 50, 400, 600, 900 MHz 2.4, 3.1–10.6 GHz | CM3 |
| S4 | Body Surface to External | 900MHz, 2.4, 3.1–10.6 GHz | CM4 |
| Model Descriptions | Scenarios | Method | Propagation Effects | Mobility | Link Type |
|---|---|---|---|---|---|
| Dynamic channel model [84] | on-body, off-body, and body-to-body | finite-difference time-domain | fade variation and their corresponding amplitude distributions | walking | hand and thigh |
| A filter based probabilistic model [85] | Intra-WBAN | orthogonal frequency-division multiplexing | fading and dynamic variation challenges | static sitting and dynamic walking | hand |
| Simulations-based space-time dependent channel model [86] | Intra-WBAN, Indoor or Anechoic Chamber | Combination of frequency, distances in free space and around the body | Spatial and temporal characteristics-based fading. Shadowing due to body parts length and size. | Standing. walking and running | Hip to Wrist/Foot/Thigh. Arm to Foot and Head to Head |
| Measurement-based time-varying model [87] | Intra-WBAN, Indoor or Anechoic Chamber | Time-frequency and scenario-based | Slow and fast fading. Shadowing correlation between links. | Standing still, walking and running on the spot | Hip to Chest/right thigh/right wrist/right foot. etc. |
| Measurement and periodic characteristics-based model [88] | Intra-WBAN, Indoor or Anechoic | Distance and periodic function | Slow and fast fading along with Periodic Correlation | Standing, walking and running | Hip to Ankle/Wrist, Wrist to Wrist/Chest, Chest to Wrist/Hip |
| Simulation-based On and Off Body Multi antenna-channel model [89] | Intra-WBAN, Indoor | Geometrical-based statistical model | Multipath cluster of scatters | Walking | Head to Front/Back |
| IEEE proposed models [90] | Intra-WBAN. Indoor or Anechoic Chamber | Distance-based | Without spatial or temporal features | Static | Around torso and on-front part on the body |
| Security Levels | Protection Levels | Transmitted Frames |
|---|---|---|
| Level 0: lowest security level | Unsecured Communication | Data are transmitted in unsecured frames without encryption and authentication. |
| Level 1: medium security level | Authentication but no Encryption | Data are transmitted in plaintext form but secured authentication are involved. |
| Level 2: highest security level | Authentication and Encryption | Data are transmitted in secured authentication and encryption. |
| Authors | Research Issues | Methodology | Outcome |
|---|---|---|---|
| Bengag et al. [112] | Jamming Attacks | Two MAC Protocols involved (ZIGBEE and TMAC) | Successful packet delivery rate |
| Arya et al. [113] | Data security | Constant monitoring for critical patients | Data authentication and authorization |
| Hayajneh et al. [114] | Lesser users | Increased storage level | More users and network lifetime |
| Thamilarasu et al. [115] | Network-level intrusion attacks | Machine learning and regression algorithms | Accurate results and lesser resource overhead |
| Umar et al. [116] | Active and passive network attacks | Enables mutual trust and used seed update algorithm | Minimal routing overhead and less computational cost |
| Dharshini et al. [117] | Vulnerable attacks | Secret key extraction with movement aided from DoS attacks | Minimum power consumption with high QoS |
| Suchithra et al. [118]. | High-rate attacks | Maintain the bandwidth conditions in cooperative routing | Low-rate attacks |
| Kumar et al. [119]. | Several security issues | Cloud technology and wireless communication | High storage and low computation cost |
| Rao et al. [120]. | High residual power | Fuzzy logic technique | Secure and stable performance |
| Ali et al. [121]. | User impersonation attacks | Bilinear pairing and elliptic curve cryptography | High security |
| Authors | Wang et al. [147] | Chen et al. [143] | Liu et al. [142] |
|---|---|---|---|
| Process technology (nm) | 65 | 130 | 180 |
| Modulation | DBPSK, DQPSK, D8PSK | DBPSK, DQPSK, D8PSK | BFSK a |
| Power supply (V) | 1.2 | 1.0 | 1.1 |
| Core power of transmitter (μW) | 1.69 | 9.89 | 34 |
| Core power of receiver (μW) | 20.46 | — | 39.6 |
| Maximum throughput (Mbps) | 10 | 0.97 | 0.625 |
| Core size (mm2) | 0.017 | 0.016 b | 0.31 |
| Size of transmitter (mm2) | 0.002 | 0.97 | — |
| Size of receiver (mm2) | 0.015 | — | — |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhong, L.; He, S.; Lin, J.; Wu, J.; Li, X.; Pang, Y.; Li, Z. Technological Requirements and Challenges in Wireless Body Area Networks for Health Monitoring: A Comprehensive Survey. Sensors 2022, 22, 3539. https://doi.org/10.3390/s22093539
Zhong L, He S, Lin J, Wu J, Li X, Pang Y, Li Z. Technological Requirements and Challenges in Wireless Body Area Networks for Health Monitoring: A Comprehensive Survey. Sensors. 2022; 22(9):3539. https://doi.org/10.3390/s22093539
Chicago/Turabian StyleZhong, Lisha, Shuling He, Jinzhao Lin, Jia Wu, Xi Li, Yu Pang, and Zhangyong Li. 2022. "Technological Requirements and Challenges in Wireless Body Area Networks for Health Monitoring: A Comprehensive Survey" Sensors 22, no. 9: 3539. https://doi.org/10.3390/s22093539
APA StyleZhong, L., He, S., Lin, J., Wu, J., Li, X., Pang, Y., & Li, Z. (2022). Technological Requirements and Challenges in Wireless Body Area Networks for Health Monitoring: A Comprehensive Survey. Sensors, 22(9), 3539. https://doi.org/10.3390/s22093539