
Adherence and the Diabetic Foot: High Tech Meets High Touch?


Abstract
:1. Introduction
2. Diabetic Peripheral Neuropathy
- Coronary artery disease;
- Increased triglyceride levels;
- Obesity;
- Smoking;
- High blood pressure.
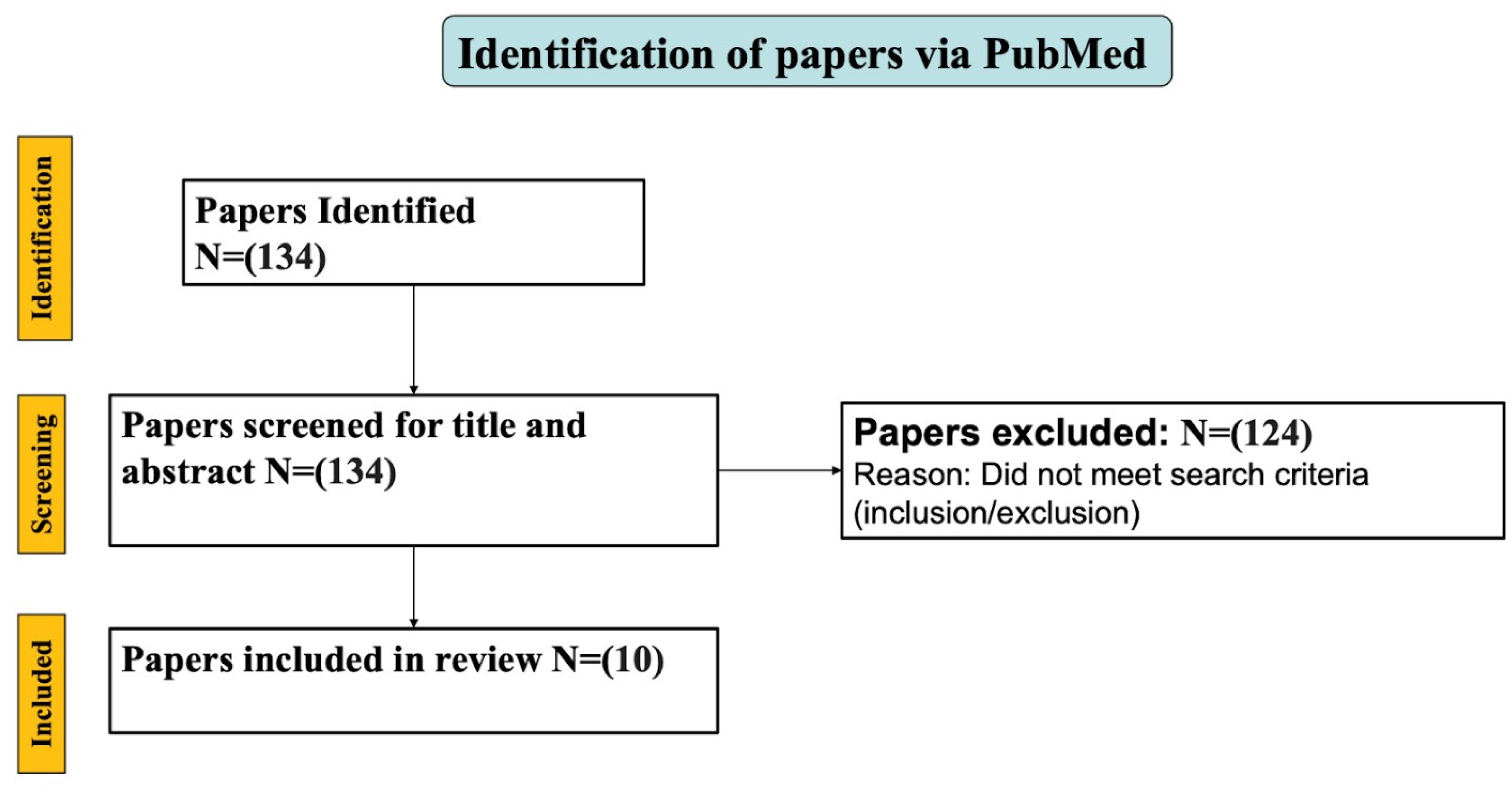
3. Methods
3.1. Search Strategy
3.2. Analysis
4. Results
4.1. Diabetic Foot Micro-Climate Regulating Technology
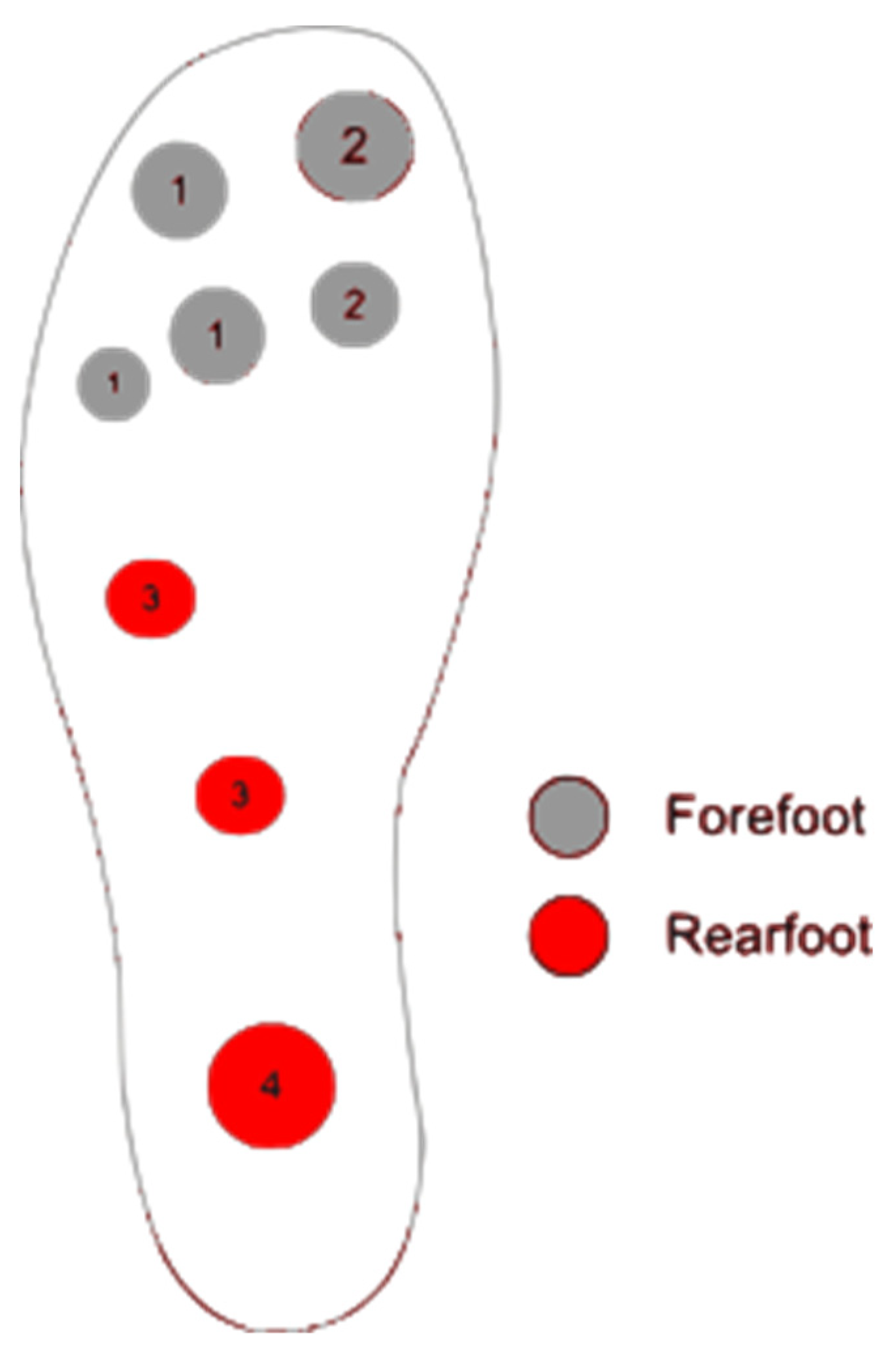
4.2. Monitoring Stress on Plantar Tissue
4.3. Monitoring Wear Time of Boots
5. Summary/Conclusions
Funding
Conflicts of Interest
References
- Williams, L.H.; Rutter, C.M.; Katon, W.J.; Reiber, G.E.; Ciechanowski, P.; Heckbert, S.R.; Lin, E.H.; Ludman, E.J.; Oliver, M.M.; Young, B.A.; et al. Depression and Incident Diabetic Foot Ulcers: A Prospective Cohort Study. Am. J. Med. 2010, 123, 748–754.e3. [Google Scholar] [CrossRef] [Green Version]
- Bădescu, S.; Tătaru, C.; Kobylinska, L.; Georgescu, E.; Zahiu, D.; Zăgrean, A.; Zăgrean, L. The association between Diabetes mellitus and Depression. J. Med. Life 2016, 9, 120–125. [Google Scholar]
- Polikandrioti, M.; Vasilopoulos, G.; Koutelekos, I.; Panoutsopoulos, G.; Gerogianni, G.; Alikari, V.; Dousis, E.; Zartaloudi, A. Depression in diabetic foot ulcer: Associated factors and the impact of perceived social support and anxiety on depression. Int. Wound J. 2020, 17, 900–909. [Google Scholar] [CrossRef]
- Monami, M.; Longo, R.; Desideri, C.M.; Masotti, G.; Marchionni, N.; Mannucci, E. The diabetic person beyond a foot ulcer: Healing, recurrence, and depressive symptoms. J. Am. Podiatr. Med. Assoc. 2008, 98, 130–136. [Google Scholar] [CrossRef]
- DiMatteo, M.R.; Lepper, H.S.; Croghan, T.W. Depression is a risk factor for noncompliance with medical treatment: Meta-analysis of the effects of anxiety and depression on patient adherence. Arch. Intern. Med. 2000, 160, 2101–2107. [Google Scholar] [CrossRef] [Green Version]
- Alsunousi, S.; Marrif, H.I. Diabetic neuropathy and the sensory apparatus “meissner corpuscle and merkel cells”. Front. Neuroanat. 2014, 8, 79. [Google Scholar] [CrossRef] [Green Version]
- Kaur, S.; Pandhi, P.; Dutta, P. Painful diabetic neuropathy: An update. Ann. Neurosci. 2011, 18, 168–175. [Google Scholar] [CrossRef] [Green Version]
- Iraj, B.; Khorvash, F.; Ebneshahidi, A.; Askari, G. Prevention of diabetic foot ulcer. Int. J. Prev. Med. 2013, 4, 373–376. [Google Scholar]
- Park, J.H.; Won, J.C. Patterns of Nerve Conduction Abnormalities in Patients with Type 2 Diabetes Mellitus According to the Clinical Phenotype Determined by the Current Perception Threshold. Diabetes Metab. J. 2018, 42, 519–528. [Google Scholar] [CrossRef]
- Leung, S.W.S.; Shi, Y. The glycolytic process in endothelial cells and its implications. Acta Pharmacol. Sin. 2022, 43, 251–259. [Google Scholar]
- Redza-Dutordoir, M.; Averill-Bates, D.A. Activation of apoptosis signalling pathways by reactive oxygen species. Biochim. Biophys. Acta 2016, 1863, 2977–2992. [Google Scholar] [CrossRef]
- Khawaja, N.; Abu-Shennar, J.; Saleh, M.; Dahbour, S.S.; Khader, Y.S.; Ajlouni, K.M. The prevalence and risk factors of peripheral neuropathy among patients with type 2 diabetes mellitus; the case of Jordan. Diabetol. Metab. Syndr. 2018, 10, 8. [Google Scholar] [CrossRef] [Green Version]
- Van Netten, J.J.; Raspovic, A.; Lavery, L.A.; Monteiro-Soares, M.; Rasmussen, A.; Sacco, I.C.; Bus, S.A. Prevention of foot ulcers in the at-risk patient with diabetes: A systematic review. Diabetes Metab. Res. Rev. 2020, 36 (Suppl. S1), e3270. [Google Scholar]
- Isaac, A.L.; Swartz, T.D.; Miller, M.L.; Short, D.J.; Wilson, E.A.; Chaffo, J.L.; Watson, E.S.; Hu, H.; Petersen, B.J.; Bloom, J.D.; et al. Lower resource utilization for patients with healed diabetic foot ulcers during participation in a prevention program with foot temperature monitoring. BMJ Open Diabetes Res. Care 2020, 8, e001440. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Holtz-Neiderer, K.; Wendel, C.; Mohler, M.J.; Kimbriel, H.R.; Lavery, L.A. Skin Temperature Monitoring Reduces the Risk for Diabetic Foot Ulceration in High-risk Patients. Am. J. Med. 2007, 120, 1042–1046. [Google Scholar] [CrossRef] [PubMed]
- Frykberg, R.G.; Gordon, I.L.; Reyzelman, A.M.; Cazzell, S.M.; Fitzgerald, R.H.; Rothenberg, G.M.; Bloom, J.D.; Petersen, B.J.; Linders, D.R.; Nouvong, A.; et al. Feasibility and Efficacy of a Smart Mat Technology to Predict Development of Diabetic Plantar Ulcers. Diabetes Care 2017, 40, 973–980. [Google Scholar] [CrossRef] [Green Version]
- Reyzelman, A.M.; Koelewyn, K.; Murphy, M.; Shen, X.; Yu, E.; Pillai, R.; Fu, J.; Scholten, H.J.; Ma, R. Continuous Temperature-Monitoring Socks for Home Use in Patients with Diabetes: Observational Study. J. Med. Internet Res. 2018, 20, e12460. [Google Scholar] [CrossRef] [Green Version]
- Bus, S.A.; Lavery, L.A.; Monteiro-Soares, M.; Rasmussen, A.; Raspovic, A.; Sacco, I.C.; van Netten, J.J.; International Working Group on the Diabetic Foot. Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36 (Suppl. S1), e3269. [Google Scholar]
- Najafi, B.; Ron, E.; Enriquez, A.; Marin, I.; Razjouyan, J.; Armstrong, D.G. Smarter sole survival: Will neuropathic patients at high risk for ulceration use a smart insole-based foot protection system? J. Diabetes Sci. Technol. 2017, 11, 702–713. [Google Scholar] [CrossRef] [Green Version]
- Abbott, C.A.; Chatwin, K.E.; Foden, P.; Hasan, A.N.; Sange, C.; Rajbhandari, S.M.; Reddy, P.N.; Vileikyte, L.; Bowling, F.L.; Boulton, A.J.M.; et al. Innovative intelligent insole system reduces diabetic foot ulcer recurrence at plantar sites: A prospective, randomised, proof-of-concept study. Lancet Digit. Health 2019, 1, e308–e318. [Google Scholar] [CrossRef]
- Lutjeboer, T.; Netten, J.; Postema, K.; Hijmans, J. Validity and feasibility of a temperature sensor for measuring use and non-use of orthopaedic footwear. J. Rehabil. Med. 2018, 50, 920–926. [Google Scholar] [CrossRef] [Green Version]
- Boghossian, J.; Miller, J.D.; Armstrong, D.G. Offloading the diabetic foot: Toward healing wounds and extending ulcer-free days in remission. Chronic Wound Care Manag. Res. 2017, 4, 83–88. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Services. Depression. National Institute of Mental Health. Available online: https://www.nimh.nih.gov/health/topics/depression (accessed on 23 February 2023).
- Rock, P.L.; Roiser, J.P.; Riedel, W.J.; Blackwell, A.D. Cognitive impairment in depression: A systematic review and meta-analysis. Psychol. Med. 2014, 44, 2029–2040. [Google Scholar] [CrossRef] [Green Version]
- Veneman, T.; Schaper, N.C.; Bus, S.A. The Concurrent Validity, Test–Retest Reliability and Usability of a New Foot Temperature Monitoring System for Persons with Diabetes at High Risk of Foot Ulceration. Sensors 2021, 21, 3645. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Lavery, L.A.; Liswood, P.J.; Todd, W.F.; Tredwell, J.A. Infrared Dermal Thermometry for the High-Risk Diabetic Foot. Phys. Ther. 1997, 77, 169–175. [Google Scholar] [CrossRef]
- Lavery, L.A.; Higgins, K.R.; Lanctot, D.R.; Constantinides, G.P.; Zamorano, R.G.; Armstrong, D.G.; Athanasiou, K.A.; Agrawal, C.M. Home Monitoring of Foot Skin Temperatures to Prevent Ulceration. Diabetes Care 2004, 27, 2642–2647. [Google Scholar] [CrossRef] [Green Version]
- Lavery, L.A.; Higgins, K.R.; Lanctot, D.R.; Constantinides, G.P.; Zamorano, R.G.; Athanasiou, K.A.; Armstrong, D.G.; Agrawal, C.M. Preventing diabetic foot ulcer recurrence in high-risk patients: Use of temperature monitoring as a self-assessment tool. Diabetes Care 2007, 30, 14–20. [Google Scholar] [CrossRef] [Green Version]
- Chatwin, K.E.; Abbott, C.A.; Rajbhandari, S.M.; Reddy, P.N.; Bowling, F.L.; Boulton, A.J.; Reeves, N.D. An intelligent insole system with personalised digital feedback reduces foot pressures during daily life: An 18-month randomised controlled trial. Diabetes Res. Clin. Pract. 2021, 181, 109091. [Google Scholar] [CrossRef]
- Park, C.; Mishra, R.; Vigano, D.; Macagno, M.; Rossotti, S.; D’huyvetter, K.; Garcia, J.; Armstrong, D.G.; Najafi, B. Smart Offloading Boot System for Remote Patient Monitoring: Toward Adherence Reinforcement and Proper Physical Activity Prescription for Diabetic Foot Ulcer Patients. J. Diabetes Sci. Technol. 2023, 17, 42–51. [Google Scholar] [CrossRef]
- Bus, S.A.; van Deursen, R.; Armstrong, D.G.; Lewis, J.E.A.; Caravaggi, C.F.; Cavanagh, P.R.; on behalf of the International Working Group on the Diabetic Foot (IWGDF). Footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in patients with diabetes: A systematic review. Diabetes/Metab. Res. Rev. 2016, 32, 99–118. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Risk Factors | Current Management | Issues with Current Management | Sensors/Devices | Potential Impact on Prevention | References |
|---|---|---|---|---|---|
| Lesions occurring prior to ulceration, arising from irregularities in temperature | Hand-held thermometer device | Might be difficult and time consuming for patients | Continuous at-home plantar temperature monitoring system | Minimizing the risk of potential sites susceptible to ulcer development | [15,16,17] |
| Elevated plantar pressure | Offloading footwear | Irregular adherence | Continuous at-home plantar pressure monitoring system with patient feedback on a mobile device | Improvement of timely offloading and potentially reducing ulcer occurrence | [18,19,20] |
| Irregular adherence | Total Contact Cast (TCC) | Prevent daily wound inspection and dressing changes | Monitoring adherence with temperature sensors and patient feedback on a mobile device | Prolongs patient adherence with diabetic orthopedic wear, which can potentially reduce ulcer recurrence | [21,22] |
| Technology | Functionality | Data Collection and Analysis | User Interface | Intervention and Alerting | References |
|---|---|---|---|---|---|
| SmartMat | Sensors embedded in a mat that integrates an image processing system to compare temperatures between normal and abnormal feet | After 20 s, the data are collected and then uploaded onto a cloud using a cellular component that is already in the mat | Temperature is not displayed on the mat; results are uploaded to a server | No alerts given; however, the temperature measurements will help physicians make informed decisions regarding intervention | [16] |
| Siren Care | Temperature sensors embedded in socks to detect change in temperature throughout the day | Collects the temperature data and sends them to a smartphone for monitoring and analysis | Uses a smartphone to show temperature data and alerts | Smartphone application provides alerts if there is a temperature change and will allow for timely intervention | [17] |
| PodoTemp | Total of 120 temperature sensors embedded for each foot on a platform that measures temperature differences between each foot | Provides instant readings for analysis after 40 s | Displays the temperature on the device | No alerts given; however, the temperature measurements will help physicians make informed decisions regarding intervention | [25] |
| Technology | Functionality | Data Collection and Analysis | User Interface | Intervention and Alerting | References |
|---|---|---|---|---|---|
| SurroSense Rx© | Insoles embedded with eight pressure sensors per foot; measures pressure on plantar side of feet | Collects pressure readings and sends it to smartwatch if an alert is needed | Displays alerts and readings on smartwatch | Wirelessly connects to a smartwatch to send real-time alerts to patients about plantar pressure distribution | [19] |
| Technology | Functionality | Data Collection and Analysis | User Interface | Intervention and Alerting | References |
|---|---|---|---|---|---|
| Orthotimer© | Microsensor embedded in footwear to monitor how long patients are using the prescribed footwear | Collects temperature every 15 min | Patients cannot see collected temperature | No alerts given; however, the temperature measurements will help physicians make informed decisions regarding intervention and | [21] |
| computer | whether patients are adhering to the prescribed footwear | ||||
| SmartBoot | Uses a smart offloading system in order to monitor real-time adherence to prescribed footwear and monitor patients’ weight bearing activities | Paired with a smartwatch to collect data on patient’s adherence and stores them on a cloud dashboard | Alerts shown on the smartwatch | The smartwatch sends alerts to remind patients to continuously wear the prescribed footwear | [30] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Srass, H.; Ead, J.K.; Armstrong, D.G. Adherence and the Diabetic Foot: High Tech Meets High Touch? Sensors 2023, 23, 6898. https://doi.org/10.3390/s23156898
Srass H, Ead JK, Armstrong DG. Adherence and the Diabetic Foot: High Tech Meets High Touch? Sensors. 2023; 23(15):6898. https://doi.org/10.3390/s23156898
Chicago/Turabian StyleSrass, Hadia, J. Karim Ead, and David G. Armstrong. 2023. "Adherence and the Diabetic Foot: High Tech Meets High Touch?" Sensors 23, no. 15: 6898. https://doi.org/10.3390/s23156898
APA StyleSrass, H., Ead, J. K., & Armstrong, D. G. (2023). Adherence and the Diabetic Foot: High Tech Meets High Touch? Sensors, 23(15), 6898. https://doi.org/10.3390/s23156898