
Effects of Minimalist vs. Traditional Running Shoes on Abdominal Lumbopelvic Muscle Activity in Women Running at Different Speeds: A Randomized Cross-Over Clinical Trial
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
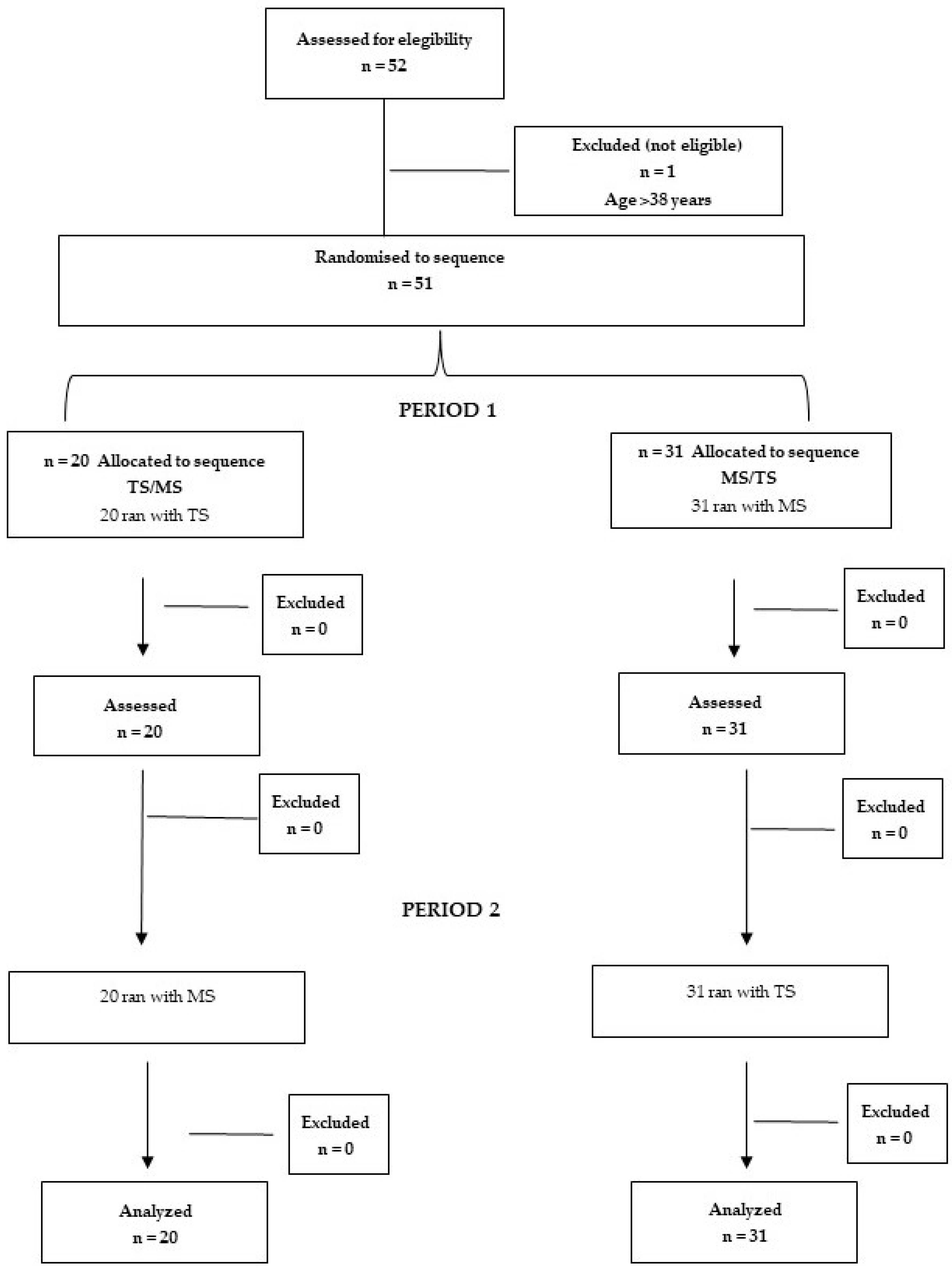
2.1. Study Design
2.2. Type of Footwear
2.3. Intervention Protocol
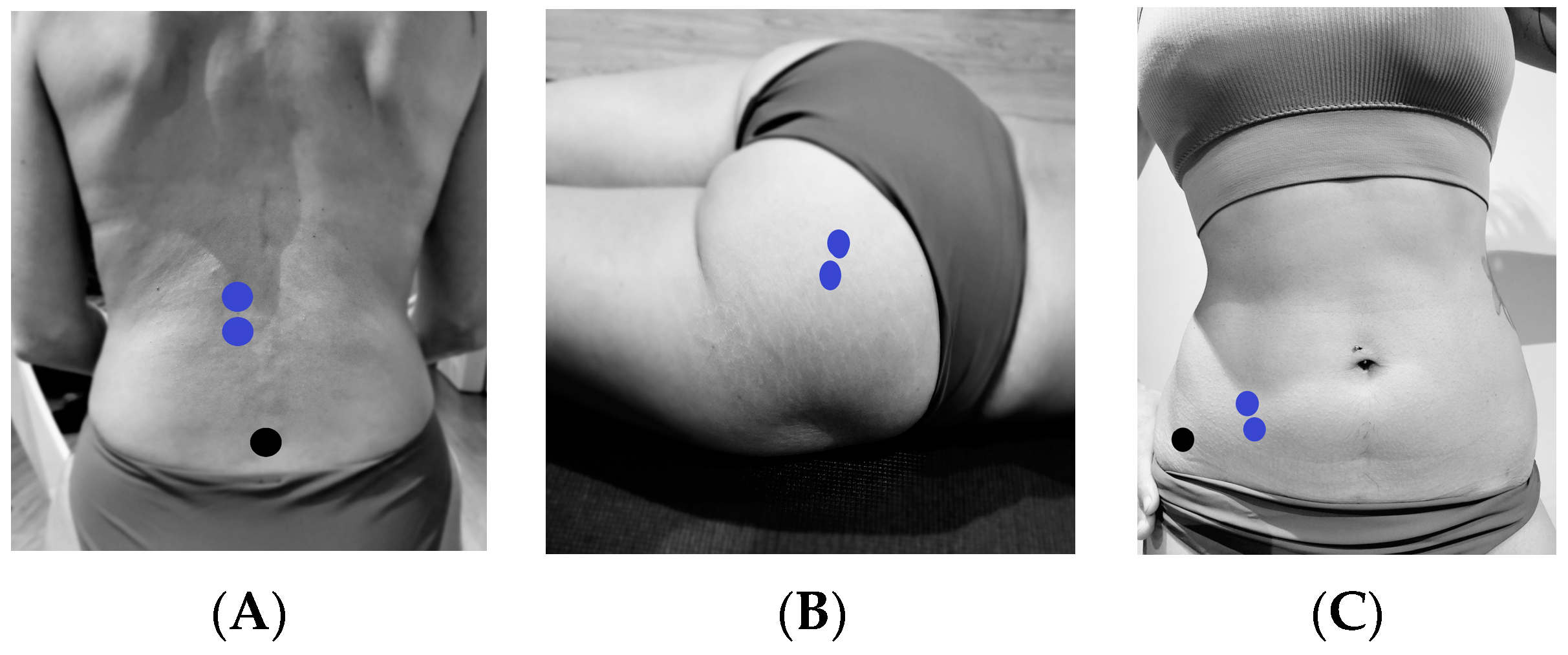
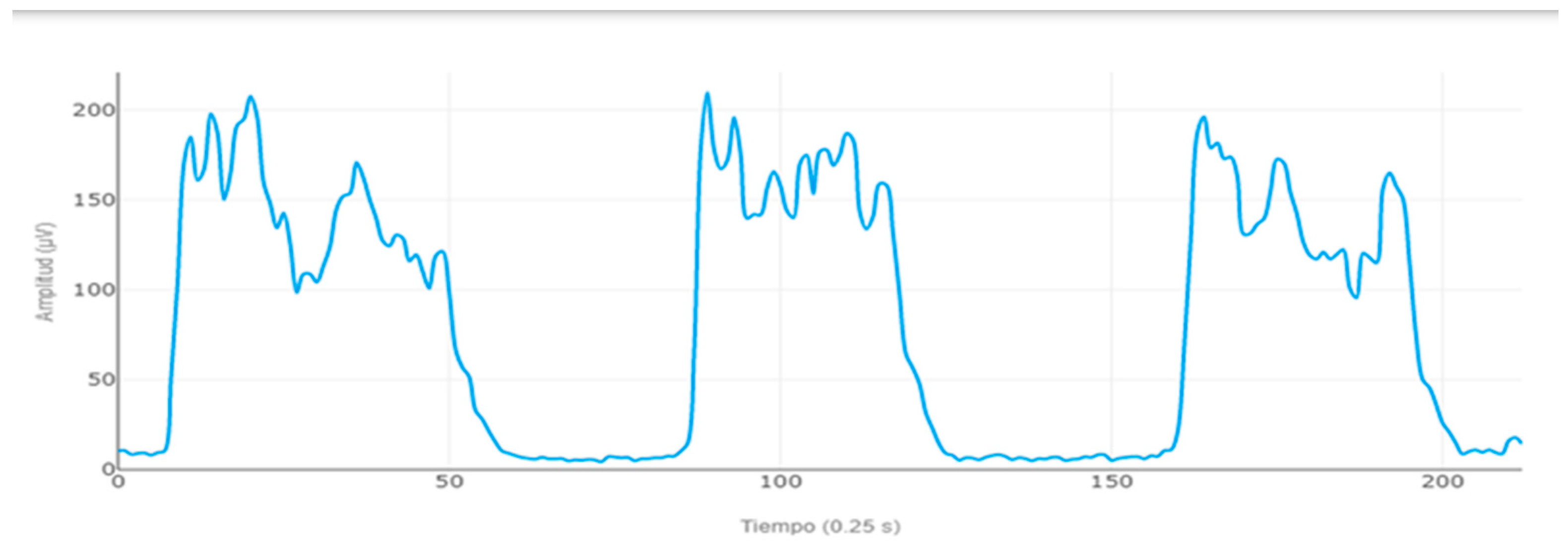
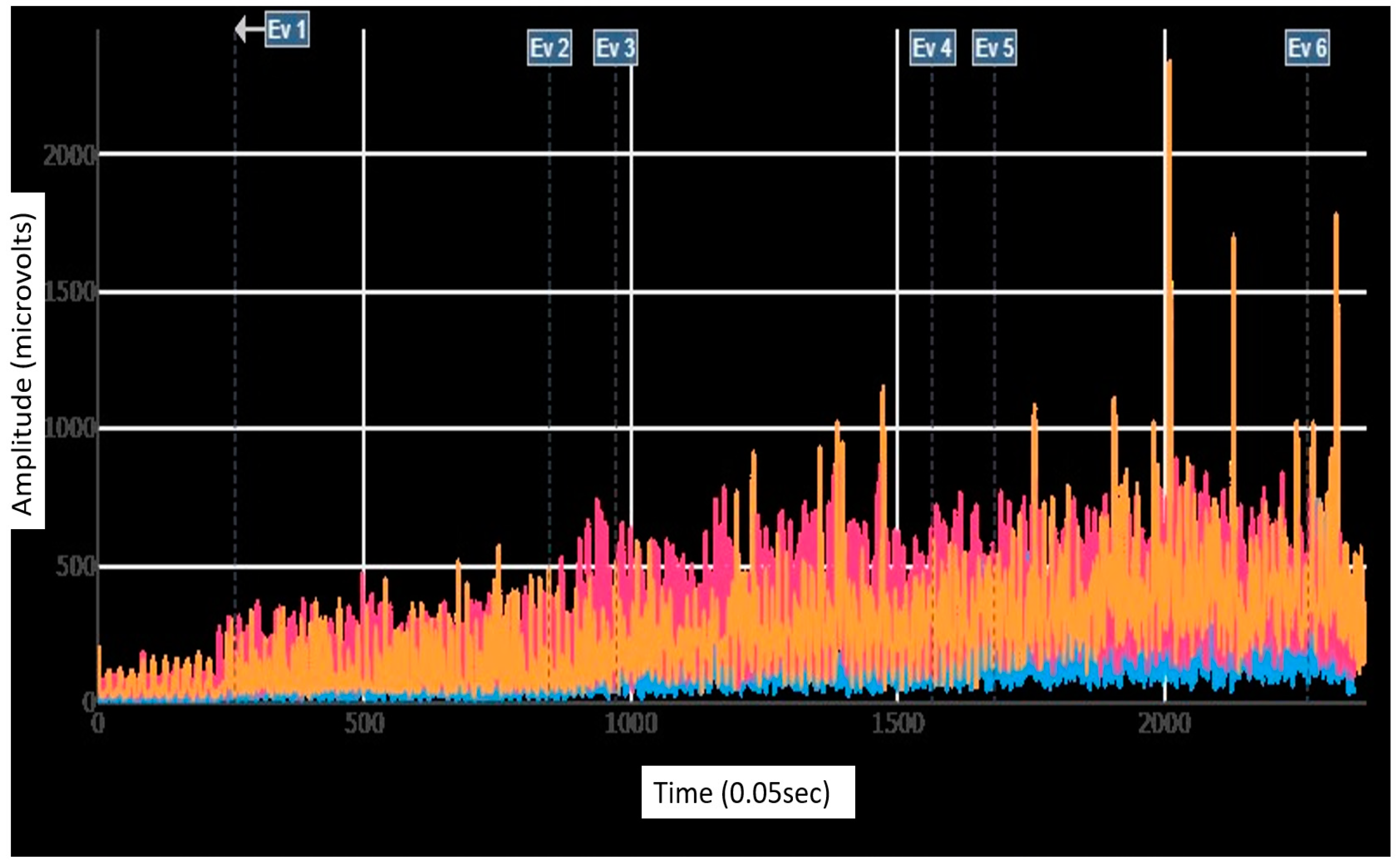
2.4. EMG Data Analysis
2.5. Statistical Analyses
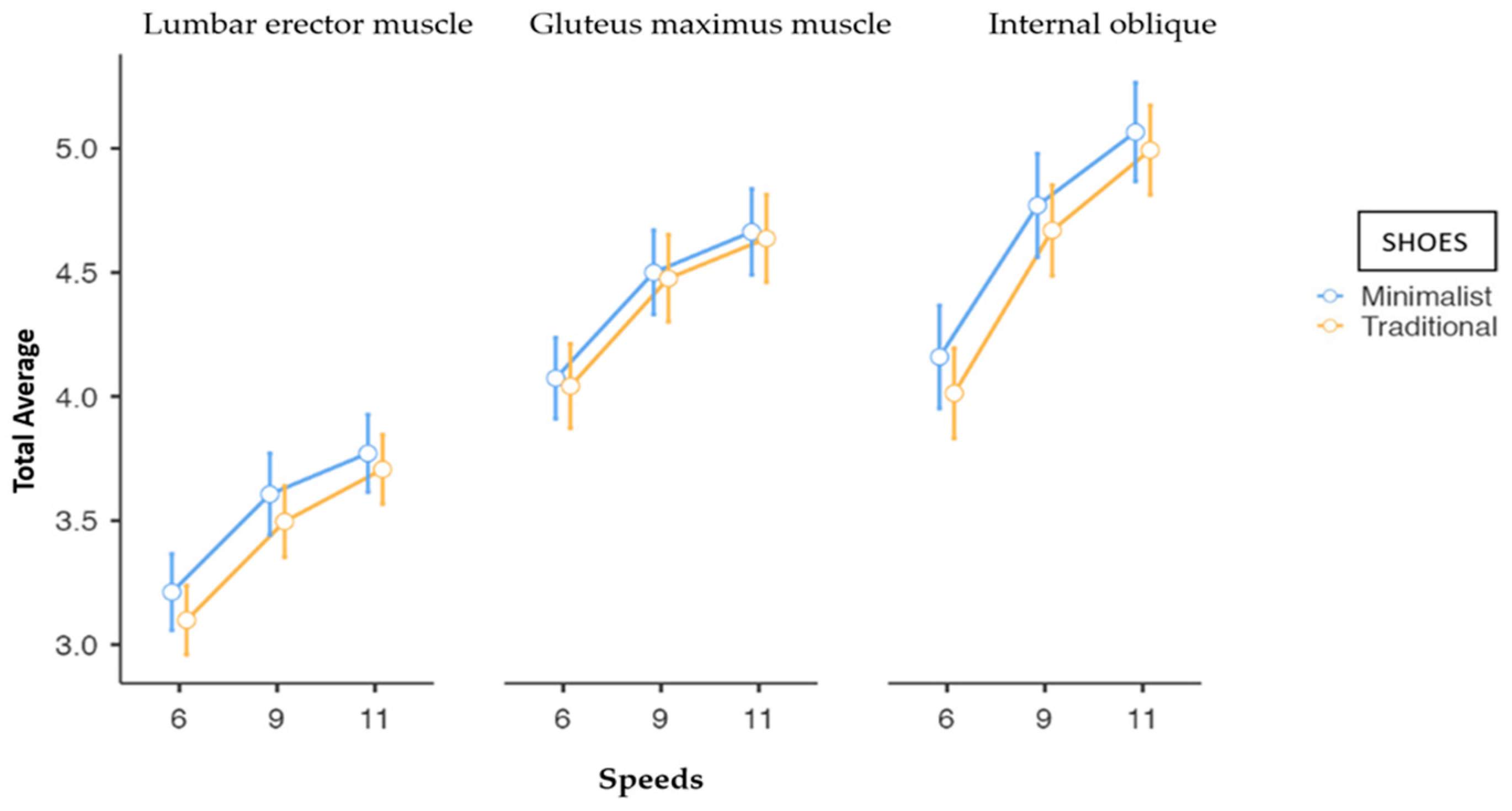
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Silva, R.d.M.; Rodrigues, M.E.S.; Puga, G.M.; Dionisio, V.C.; Baldon, V.S.P.; Resende, A.P.M. The relationship between running kinematics and the pelvic floor muscle function of female runners. Int. Urogynecol. J. 2019, 31, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Warne, J.P.; Gruber, A.H.; Cheung, R.; Bonacci, J. Training and technique choices predict self-reported running injuries: An international study. Phys. Ther. Sport 2020, 48, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Daoud, A.I.; Geissler, G.J.; Wang, F.; Saretsky, J.; Daoud, Y.A.; Lieberman, D.E. Foot strike and injury rates in endurance runners: A retrospective study. Med. Sci. Sports Exerc. 2012, 44, 1325–1334. [Google Scholar] [CrossRef] [PubMed]
- Hollander, K.; Liebl, D.; Meining, S.; Mattes, K.; Willwacher, S.; Zech, A. Adaptation of Running Biomechanics to Repeated Barefoot Running: A Randomized Controlled Study. Am. J. Sports Med. 2019, 47, 1975–1983. [Google Scholar] [CrossRef] [PubMed]
- Latorre-Román, P.A.; García-Pinillos, F.; Soto-Hermoso, V.M.; Muñoz-Jiménez, M. Effects of 12 weeks of barefoot running on foot strike patterns, inversion–eversion and foot rotation in long-distance runners. J. Sport Health Sci. 2019, 8, 579–584. [Google Scholar] [CrossRef]
- Esculier, J.-F.; Dubois, B.; Dionne, C.E.; Leblond, J.; Roy, J.-S. A consensus definition and rating scale for minimalist shoes. J. Foot Ankle Res. 2015, 8, 42. [Google Scholar] [CrossRef]
- Lafortune, M.A.; Hennig, E.M.; Lake, M.J. Dominant role of interface over knee angle for cushioning impact loading and regulating initial leg stiffness. J. Biomech. 1996, 29, 1523–1529. [Google Scholar] [CrossRef]
- Light, L.; McLellan, G.; Klenerman, L. Skeletal transients on heel strike in normal walking with different footwear. J. Biomech. 1980, 13, 477–480. [Google Scholar] [CrossRef]
- Lieberman, D.E. What We Can Learn About Running from Barefoot Running: An evolutionary medical perspective. Exerc. Sport Sci. Rev. 2012, 40, 63–72. [Google Scholar] [CrossRef]
- Breine, B.; Malcolm, P.; Van Caekenberghe, I.; Fiers, P.; Frederick, E.C.; De Clercq, D. Initial foot contact and related kinematics affect impact loading rate in running. J. Sports Sci. 2016, 35, 1556–1564. [Google Scholar] [CrossRef]
- Lieberman, D.E.; Venkadesan, M.; Werbel, W.A.; Daoud, A.I.; D’andrea, S.; Davis, I.S.; Mang’eni, R.O.; Pitsiladis, Y. Foot strike patterns and collision forces in habitually barefoot versus shod runners. Nature 2010, 463, 531–535. [Google Scholar] [CrossRef] [PubMed]
- An, W.; Rainbow, M.J.; Cheung, R.T.H. Effects of Surface Inclination on the Vertical Loading Rates and Landing Pattern during the First Attempt of Barefoot Running in Habitual Shod Runners. BioMed Res. Int. 2015, 2015, 240153. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, R.V.; Colla, C.; Sbruzzi, G.; Mallmann, A.; Paiva, L.L. Prevalence of urinary incontinence in female athletes: A systematic review with meta-analysis. Int. Urogynecol. J. 2018, 29, 1717–1725. [Google Scholar] [CrossRef] [PubMed]
- Woolf, S.K.; Barfield, W.R.; Nietert, P.J.; Mainous, A.G.; Glaser, J.A. The Cooper River Bridge Run Study of low back pain in runners and walkers. J. South Orthop. Assoc. 2002, 11, 136–243. [Google Scholar] [PubMed]
- Strauts, J.; Vanicek, N.; Halaki, M. Acute changes in kinematic and muscle activity patterns in habitually shod rearfoot strikers while running barefoot. J. Sports Sci. 2015, 34, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti Garcia, M.A.; Vieira, T.M.M. Surface electromyography: Why, when and how to use it. Rev. Andal. Med. Deport. 2011, 4, 17–28. [Google Scholar]
- Wakeling, J.M.; Pascual, S.A.; Nigg, B.M. Altering muscle activity in the lower extremities by running with different shoes. Med. Sci. Sports Exerc. 2002, 34, 1529–1532. [Google Scholar] [CrossRef]
- Roca-Dols, A.; Losa-Iglesias, M.E.; Sánchez-Gómez, R.; López-López, D.; Becerro-de-Bengoa-Vallejo, R.; Calvo-Lobo, C. Electromyography comparison of the effects of various footwear in the activity patterns of the peroneus longus and brevis muscles. J. Mech. Behav. Biomed. Mater. 2018, 82, 126–132. [Google Scholar] [CrossRef]
- Molina-Molina, A.; Ruiz-Malagón, E.J.; Carrillo-Pérez, F.; Roche-Seruendo, L.E.; Damas, M.; Banos, O.; García-Pinillos, F. Validation of mDurance, A Wearable Surface Electromyography System for Muscle Activity Assessment. Front. Physiol. 2020, 11, 606287. [Google Scholar] [CrossRef]
- Snijders, C.J.; Ribbers, M.T.; de Bakker, H.V.; Stoeckart, R.; Stam, H.J. EMG recordings of abdominal and back muscles in various standing postures: Validation of a biomechanical model on sacroiliac joint stability. J. Electromyogr. Kinesiol. 1998, 8, 205–214. [Google Scholar] [CrossRef]
- Bishop, B.N.; Greenstein, J.; Etnoyer-Slaski, J.L.; Sterling, H.; Topp, R. Electromyographic Analysis of Gluteus Maximus, Gluteus Medius, and Tensor Fascia Latae During Therapeutic Exercises with and Without Elastic Resistance. Int. J. Sports Phys. Ther. 2018, 13, 668–675. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, K.M.; Da Roza, T.; Mochizuki, L.; Arbieto, E.R.M.; da Luz, S.C.T. Assessment of abdominal and pelvic floor muscle function among continent and incontinent athletes. Int. Urogynecol. J. 2018, 30, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Vigotsky, A.D.; Halperin, I.; Lehman, G.J.; Trajano, G.S.; Vieira, T.M. Interpreting Signal Amplitudes in Surface Electromyography Studies in Sport and Rehabilitation Sciences. Front. Physiol. 2018, 8, 985. [Google Scholar] [CrossRef] [PubMed]
- Schlink, B.R.; Nordin, A.D.; Ferris, D.P. Human myoelectric spatial patterns differ among lower limb muscles and locomotion speeds. Physiol. Rep. 2020, 8, e14652. [Google Scholar] [CrossRef] [PubMed]
- Chumanov, E.S.; Wille, C.M.; Michalski, M.P.; Heiderscheit, B.C. Changes in muscle activation patterns when running step rate is increased. Gait Posture 2012, 36, 231–235. [Google Scholar] [CrossRef]
- Perkins, K.P.; Hanney, W.J.; Rothschild, C.E. The risks and benefits of running barefoot or in minimalist shoes: A systematic review. Sports Health A Multidiscip. Approach 2014, 6, 475–480. [Google Scholar] [CrossRef]
- Yao, W.; Fuglevand, R.J.; Enoka, R.M.; Del Vecchio, A.; Negro, F.; Felici, F.; Farina, D.; Song, W.; Martin, J.H.; Rana, S.; et al. Motor-unit synchronization increases EMG amplitude and decreases force steadiness of simulated contractions. J. Neurophysiol. 2000, 83, 441–452. [Google Scholar] [CrossRef]
- Lieberman, D.E.; Raichlen, D.A.; Pontzer, H.; Bramble, D.M.; Cutright-Smith, E. The human gluteus maximus and its role in running. J. Exp. Biol. 2006, 209, 2143–2155. [Google Scholar] [CrossRef]
- Divert, C.; Mornieux, G.; Baur, H.; Mayer, F.; Belli, A. Mechanical comparison of barefoot and shod running. Int. J. Sports Med. 2004, 26, 593–598. [Google Scholar] [CrossRef]
- Kerrigan, D.C.; Franz, J.R.; Keenan, G.S.; Dicharry, J.; Della Croce, U.; Wilder, R.P. The effect of running shoes on lower extremity joint torques. PMR 2009, 1, 1058–1063. [Google Scholar] [CrossRef]
- Jafarnezhadgero, A.; Alavi-Mehr, S.M.; Granacher, U. Effects of anti-pronation shoes on lower limb kinematics and kinetics in female runners with pronated feet: The role of physical fatigue. PLoS ONE 2019, 14, e0216818. [Google Scholar] [CrossRef] [PubMed]
- Brinkman, H.; Yanchek, A.; Thorton, E. Barefoot Training: Effect on Lateral Pelvic Drop and EMG Activity of Gluteus Medius and TFL. Physical Therapy Scholarly Projects. 643. 2018. Available online: https://commons.und.edu/pt-grad/ (accessed on 10 February 2023).
- Koenig, I.; Eichelberger, P.; Blasimann, A.; Hauswirth, A.; Baeyens, J.-P.; Radlinger, L. Wavelet analyses of electromyographic signals derived from lower extremity muscles while walking or running: A systematic review. PLoS ONE 2018, 13, e0206549. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean ± SD | Range |
|---|---|---|
| Age (years) | 26.55 ± 5.11 | (20.0–38.0) |
| Weight (kg) | 58.24 ± 7.06 | (45.0–82.0) |
| Height (m) | 1.65 ± 0.06 | (1.53–1.82) |
| BMI 1 (Kg/m2) | 21.29 ± 2.07 | (17.28–27.40) |
| Running Speed | |||||||
|---|---|---|---|---|---|---|---|
| Variable | Muscle | 6 km/h | 9 km/h | 11 km/h | |||
| MS a | TS b | MS a | TS b | MS a | TS b | ||
| Maximum peaks | LE c | 48.9 | 51.6 | 74.0 | 73.5 | 89.8 | 96.21 |
| (33.7, 112.0) | (32.0, 106.7) | (50.7, 156.5) | (43.5, 155.8) | (55.5, 181.2) | (51.1, 179.1) | ||
| GM d | 163.0 | 193.5 | 232.8 | 238.4 | 254.1 | 278.2 | |
| (65.8, 354.4) | (63.5, 373.8) | (87.0, 551.5) | (88.2, 553.9) | (104.8, 633.7) | (104.0, 605.0) | ||
| IO e | 174.5 | 190.6 | 360.3 | 403.0 | 543.3 | 442.6 | |
| (59.3, 545.7) | (62.9, 449.1) | (115.9, 860.1) | (115.4, 738.4) | (139.7, 1150.1) | (156.6, 972.0) | ||
| Minimum peaks | LE c | 4.8 | 3.9 | 7.7 | 7.6 | 9.25 | 7.95 |
| (2.6, 8.2) | (2.6, 8.9) | (4.0, 15.0) | (3.7, 15.0) | (4.2, 18.7) | (4.3, 17.3) | ||
| GM d | 10.8 | 12.8 | 19.1 | 19.6 | 21.3 | 24.0 | |
| (4.7, 25.0) | (3.7, 24.0) | (8.0, 53.0) | (5.5, 45.7) | (9.1, 59.7) | (7.6, 60.2) | ||
| IO e | 14.5 | 13.8 | 29.3 | 20.4 | 32.9 | 30.0 | |
| (5.8, 31.4) | (5.4, 21.0) | (10.23, 58.1) | (10.2, 47.8) | (14.3, 84.0) | (14.5, 77.2) | ||
| Total average | LE c | 17.9 | 18.0 | 26.0 | 29.7 | 36.0 | 35.1 |
| (12.6, 38.2) | (11.0, 37.6) | (17.9, 53.0) | (15.0, 56.8) | (19.8, 63.1) | (18.4, 67.7) | ||
| GM d | 60.3 | 54.9 | 86.3 | 78.7 | 95.0 | 96.6 | |
| (23.7, 120.0) | (20.3, 119.2) | (36.9, 187.2) | (32.8, 219.6) | (46.5, 233.1) | (40.6, 218.5) | ||
| IO e | 61.2 | 63.6 | 141.4 | 136.4 | 186.1 | 157.9 | |
| (19.7, 187.9) | (23.7, 135.1) | (38.3, 319.6) | (45.2, 253.0) | (56.0, 378.2) | (60.1, 378.8) | ||
| Running Speed | |||||||
|---|---|---|---|---|---|---|---|
| 6 km/h | 9 km/h | 11 km/h | |||||
| Variable | Muscle | Difference (95% CI) | p | Difference (95% CI) | p | Difference (95% CI) | p |
| Maximum peaks | LE a | 0.12 (−0.13, 0.37) | 0.33 | 0.11 (−0.12, 0.33) | 0.35 | 0.07 (−0.17, 0.29) | 0.55 |
| GM b | 0.06 (−0.10, 0.22) | 0.47 | 0.0 (−0.17, 0.17) | 0.99 | 0.02 (−0.14, 0.18) | 0.82 | |
| IO c | 0.10 (−0.19, 0.39) | 0.50 | 0.10 (−0.16, 0.36) | 0.44 | 0.09 (−0.16, 0.33) | 0.47 | |
| Minimum peaks | LE a | 0.11 (−0.05, 0.27) | 0.17 | 0.10 (−0.09, 0.29) | 0.28 | 0.08 (−0.10, 0.26) | 0.38 |
| GM b | 0.04 (−0.13, 0.21) | 0.66 | 0.04 (−0.15, 0.23) | 0.67 | 0.04 (−0.14, 0.22) | 0.66 | |
| IO c | 0.21 (−0.03, 0.45) | 0.08 | 0.18 (−0.05, 0.40) | 0.12 | 0.10 (−0.13, 0.32) | 0.39 | |
| Total average | LE a | 0.11 (−0.08, 0.31) | 0.25 | 0.11 (−0.10, 0.32) | 0.29 | 0.06 (−0.12, 0.25) | 0.49 |
| GM b | 0.03 (−0.12, 0.19) | 0.68 | 0.02 (−0.15, 0.19) | 0.78 | 0.03 (−0.13, 0.19) | 0.74 | |
| IO c | 0.15 (−0.12, 0.41) | 0.27 | 0.10 (−0.15, 0.35) | 0.43 | 0.07 (−0.16, 0.31) | 0.54 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Arrabé, M.; de la Plaza San Frutos, M.; Bermejo-Franco, A.; del Prado-Álvarez, R.; López-Ruiz, J.; del-Blanco-Muñiz, J.A.; Giménez, M.-J. Effects of Minimalist vs. Traditional Running Shoes on Abdominal Lumbopelvic Muscle Activity in Women Running at Different Speeds: A Randomized Cross-Over Clinical Trial. Sensors 2024, 24, 310. https://doi.org/10.3390/s24020310
García-Arrabé M, de la Plaza San Frutos M, Bermejo-Franco A, del Prado-Álvarez R, López-Ruiz J, del-Blanco-Muñiz JA, Giménez M-J. Effects of Minimalist vs. Traditional Running Shoes on Abdominal Lumbopelvic Muscle Activity in Women Running at Different Speeds: A Randomized Cross-Over Clinical Trial. Sensors. 2024; 24(2):310. https://doi.org/10.3390/s24020310
Chicago/Turabian StyleGarcía-Arrabé, María, Marta de la Plaza San Frutos, Alberto Bermejo-Franco, Rebeca del Prado-Álvarez, Javier López-Ruiz, José Angel del-Blanco-Muñiz, and María-José Giménez. 2024. "Effects of Minimalist vs. Traditional Running Shoes on Abdominal Lumbopelvic Muscle Activity in Women Running at Different Speeds: A Randomized Cross-Over Clinical Trial" Sensors 24, no. 2: 310. https://doi.org/10.3390/s24020310
APA StyleGarcía-Arrabé, M., de la Plaza San Frutos, M., Bermejo-Franco, A., del Prado-Álvarez, R., López-Ruiz, J., del-Blanco-Muñiz, J. A., & Giménez, M. -J. (2024). Effects of Minimalist vs. Traditional Running Shoes on Abdominal Lumbopelvic Muscle Activity in Women Running at Different Speeds: A Randomized Cross-Over Clinical Trial. Sensors, 24(2), 310. https://doi.org/10.3390/s24020310