4. Discussion
Central to the study is evaluating an innovative MRN registration approach using an LCS, which addresses challenges such as user dependency and being cost-effective while enhancing accuracy in neurosurgical procedures. The method effectively replicates the scanner frame’s position relative to the patient and autonomously performs transformations, aligning tracking space coordinates with the imaging space. This study retrospectively utilized image data from a cohort of patients with intracranial lesions to fabricate life-sized head phantoms. These were then employed in simulated clinical environments to test the LCS-MRN system, focusing on registering image data and head phantoms to ascertain the system’s effectiveness and accuracy. The results demonstrated encouraging outcomes, laying the groundwork for future refinements and clinical applications.
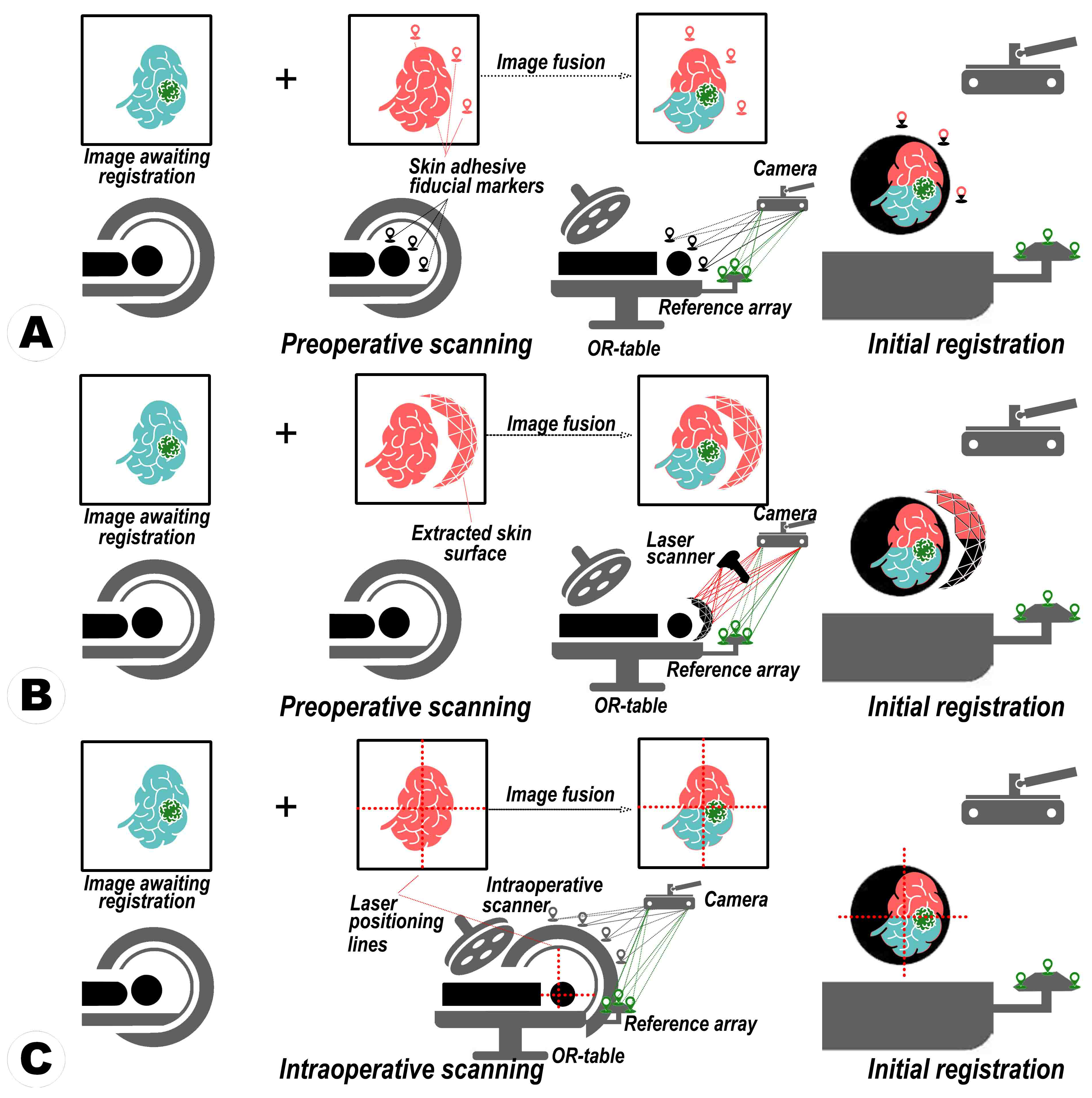
The evolution of MRN can be traced through a series of advancements and challenges. Initial stages featured user-directed adjustments of virtual elements to correspond with real anatomical structures, a method necessitated recurrent recalibrations due to positional changes, thus being inefficient and inconsistent [
11,
12]. Advancements led to adopting a fiducial-based registration method, using distinct markers for more rapid configuration than the manual approach, albeit at the cost of increased
from marker displacement (e.g., skin shift) or equipment degradation (e.g., pointer abrasion) [
8,
21,
23,
31]. Meanwhile, some evolution shifted towards a markerless, surface-oriented strategy deploying computer vision (CV) algorithms, automating patient-image congruence, and minimizing physical interaction [
32,
33,
34,
35]. While streamlining the procedure during this phase, issues were encountered in maintaining registration accuracy due to sensitivity to low image quality, surface irregularities, feature scarcity, and image distortion, all demanding high computational power.
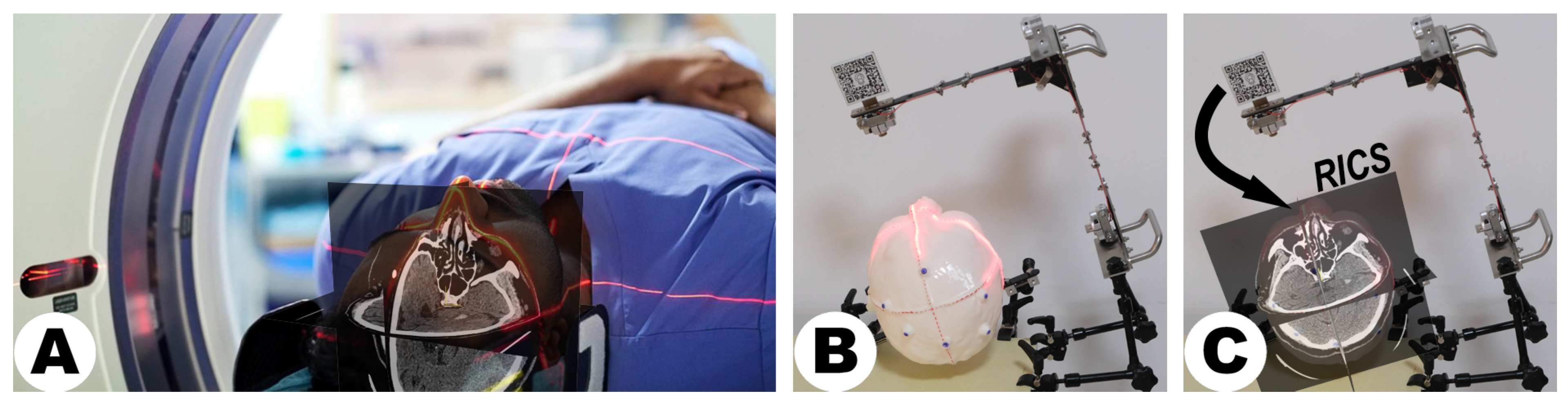
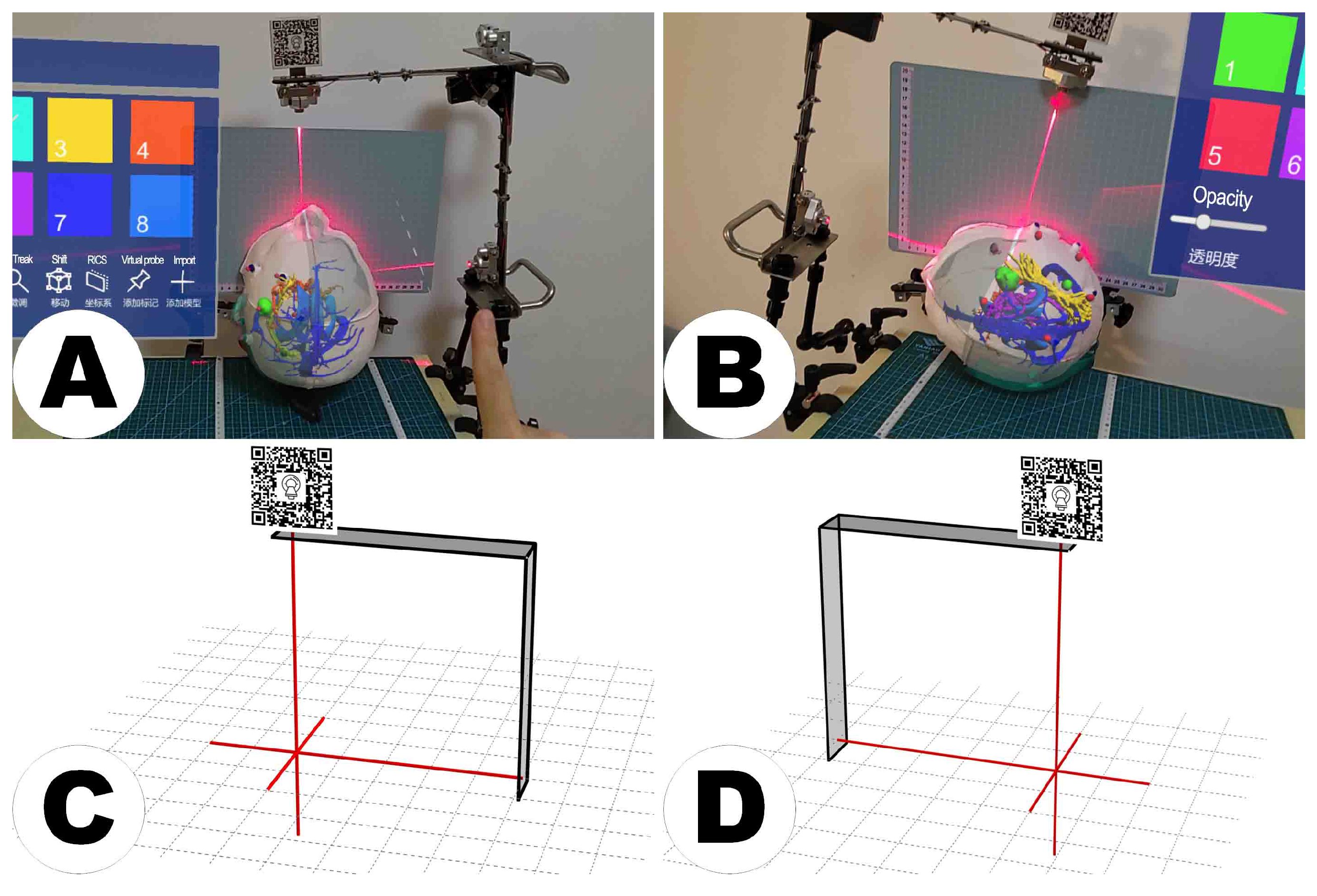
Amidst these developments, the quest for more efficient MRN methods persisted. The LCS-based registration method streamlines MRN by simplifying user involvement by aligning two laser cross-projections, surpassing the complexities of virtual object manipulation. This technique bypasses issues such as pointer degradation and the necessity for pre-defining virtual registration aids, as it employs pre-scanned, user-independent reference planes from DICOM images [
7]. These orthogonally arranged planes ensure a consistent and globally representative registration process. The system is also user-friendly in assembly and operation, characterized by low-cost hardware fabrication and software processes that demand minimal computational power. A comparative analysis of registration techniques within state-of-the-art MRN paradigms is presented in
Table 7, which elucidates the relative advantages and limitations of the LCS-MRN system against conventional systems.
This study’s integration of the LCS with the MRN system presents several navigational benefits. Technically, the LCS offers surgeons an intuitive physical positioning guide, complemented by the MR platform’s detailed visualization of anatomical structures, enhancing surgical area understanding. Visually, the LCS provides stable tracking in the physical space, while the MR platform maintains holographic consistency, even when surgeons adjust their perspectives during the procedure. The swift deployment of the LCS during surgery preparation, coupled with the MR platform’s visual aids, streamlines the surgical workflow. This “hybrid combination” approach, based on the principles of complementarity and compatibility, ensures that each system’s strengths are utilized while compensating for any limitations. This novel application of the LCS in establishing a consistent coordinate origin with CT or MRI data marks a significant advancement in MRN, offering improved integration and alignment accuracy. Bridging these technical and visual advantages, the dual-sided capability of the LCS’s MR interface marks a strategic innovation that optimizes spatial utility in the operating room (OR). This adaptability ensures the integration system’s functionality is maximized, allowing for flexible positioning that accommodates the surgeon’s needs and the constraints of the surgical environment.
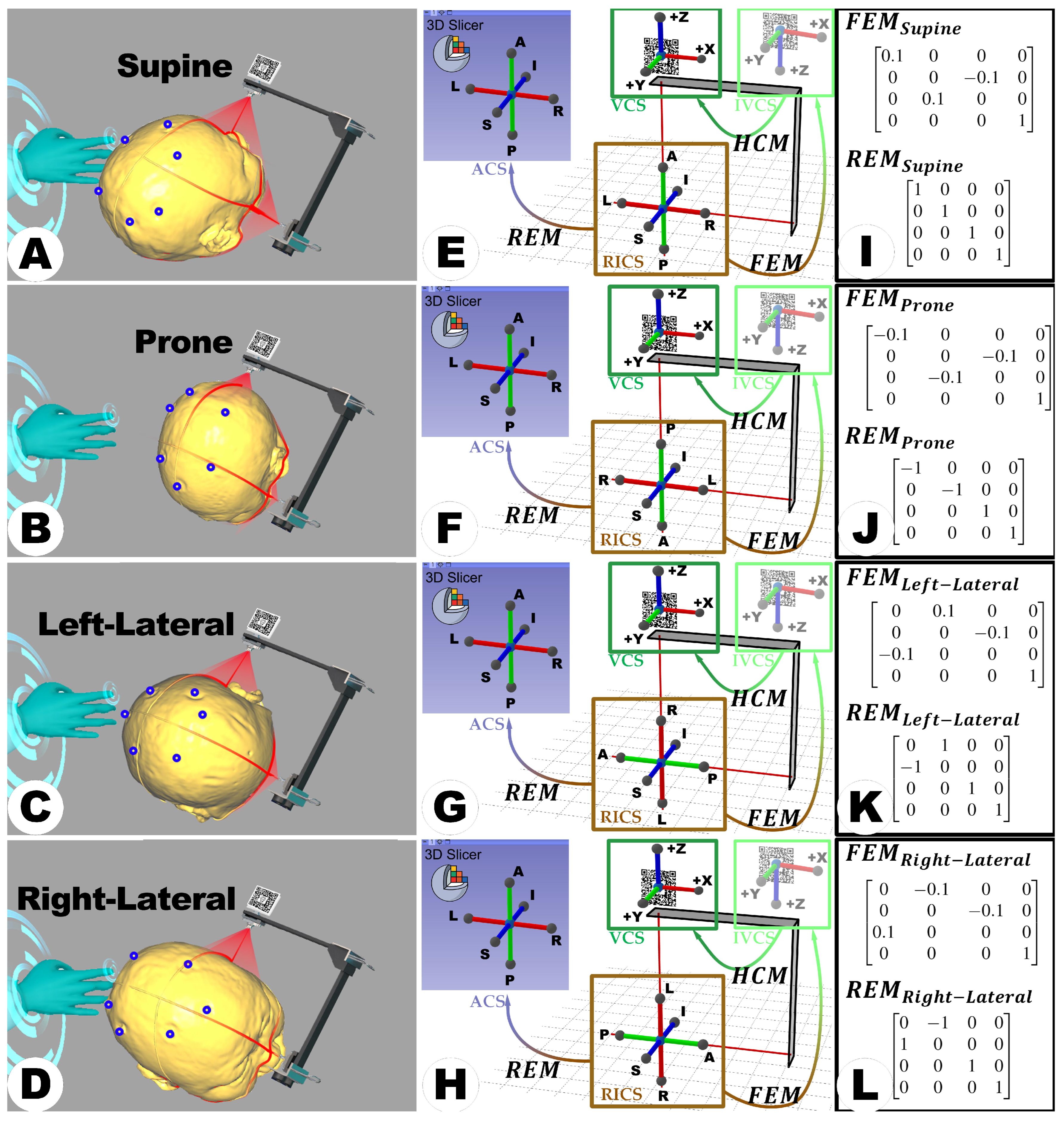
Building on the advancements introduced by the LCS-MRN system, its versatility and scalability further extend its potential impact in the medical field. The scalability of the LCS-MRN system is highlighted by its effectiveness in various surgical positions, overcoming the limitations of traditional MRN paradigms, which are often restricted to supine positioning. The proposed system is equally effective in prone and lateral positions, broadening its applicability in diverse surgical contexts. Moreover, its foundational design centered on reference scans and integration with RICS presents the potential for compatibility with diverse imaging modalities, potentially including ultrasound and functional MRI. As long as modalities can align with RICS, they can integrate seamlessly with the LCS-MRN system, extending its applicability. Furthermore, the streamlined structural design of the LCS-MRN allows for adaptation across varied clinical settings, from advanced operating rooms to resource-limited environments, augmenting its global applicability and addressing a spectrum of medical requirements.
As a novel MRN approach, LCS-MRN aims to enhance neurosurgeons’ visual and spatial skills through perception and interaction. Theoretically, procedures that depend on these skills, such as lesion localization, understanding complex anatomical relationships, and planning surgical pathways for intraoperative guidance, will potentially benefit from this technology. In previous studies, these neurosurgical scenarios often employed in MRN evaluations serve to validate the system’s practicality and efficacy [
8,
11,
12,
22,
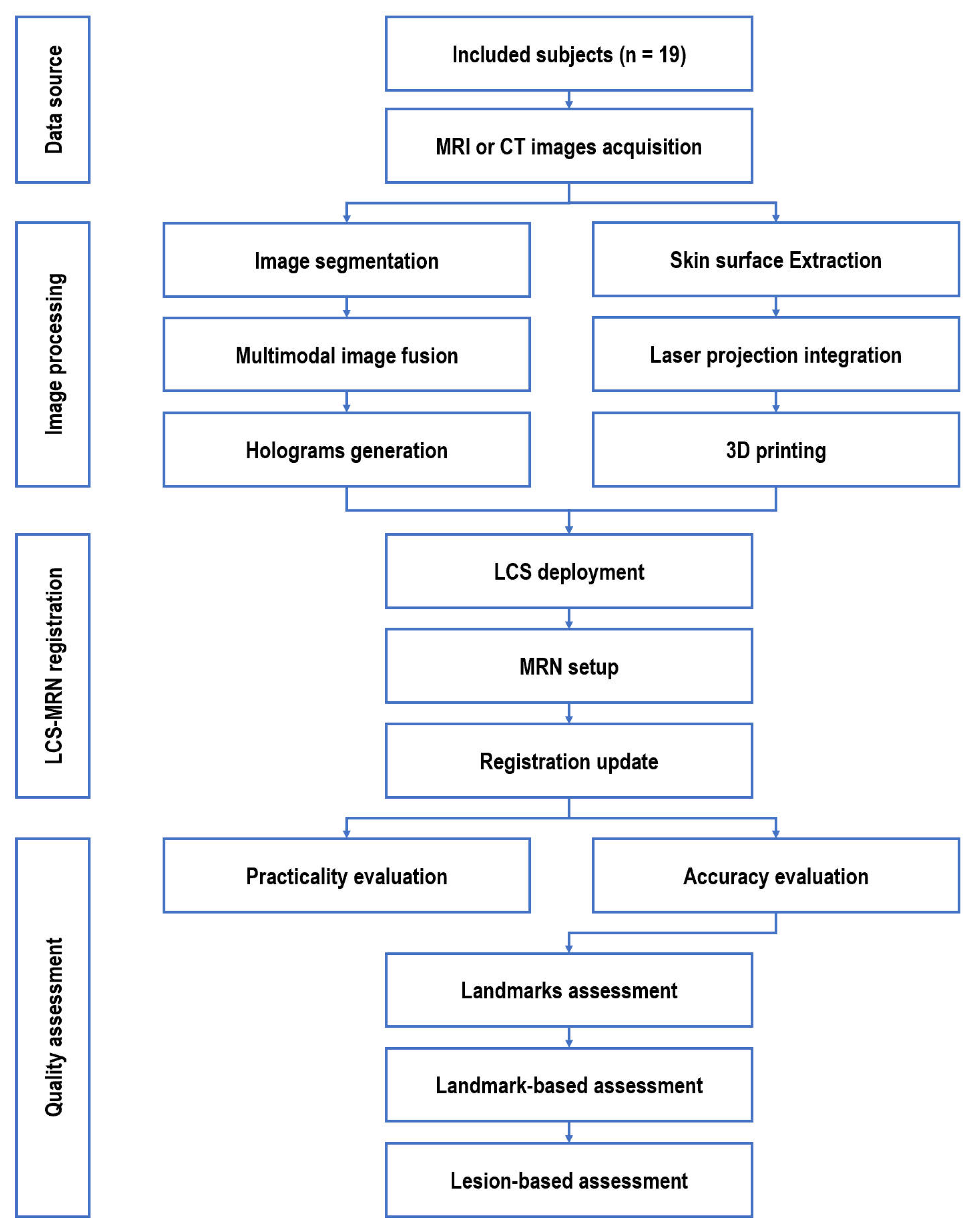
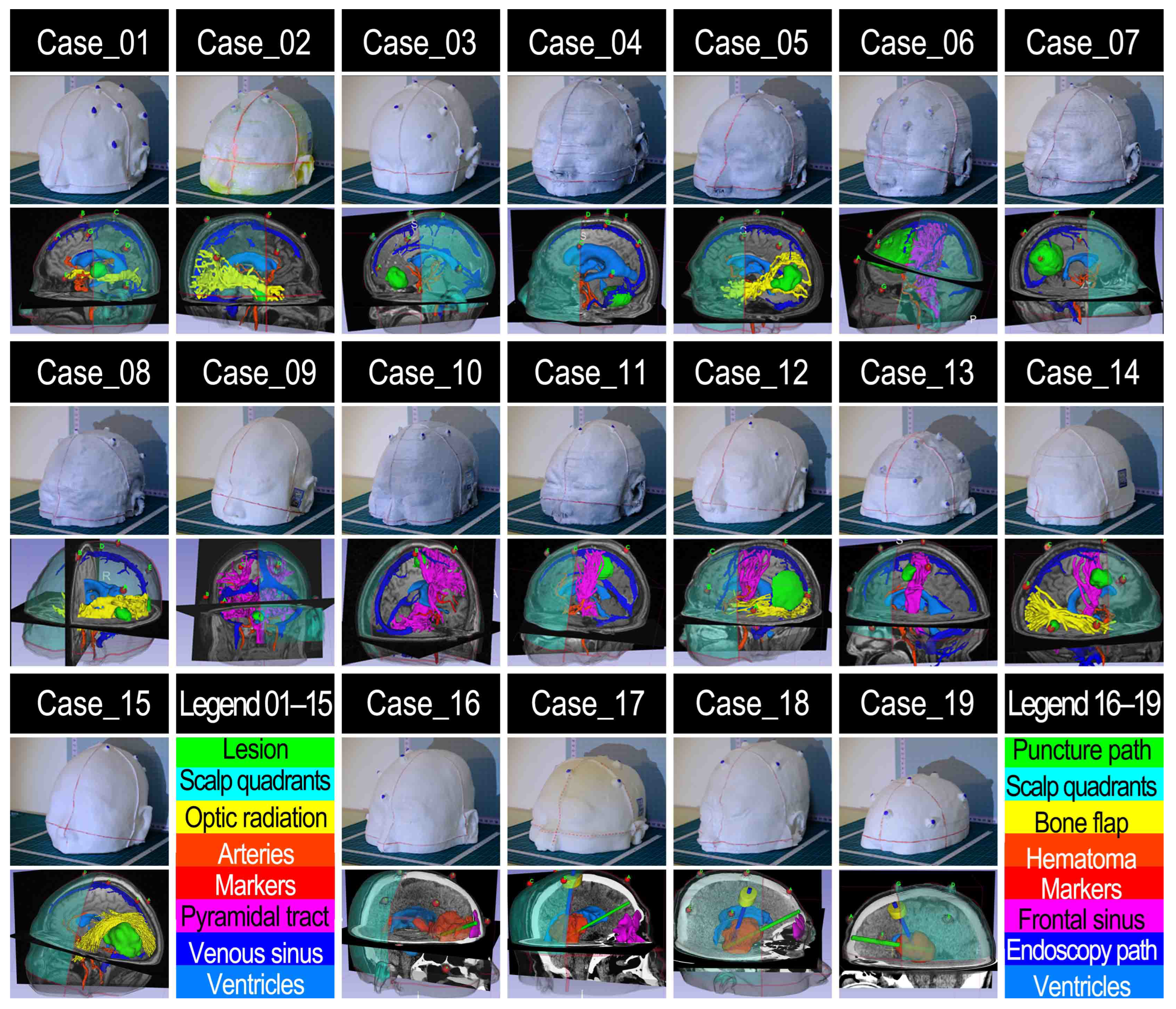
39]. Within this study, the capabilities of the LCS-MRN system were analyzed in a diverse patient cohort of 19 human subjects, covering various pathologies, locations, and surgical objectives, including lesion resection, craniotomy planning, hemorrhage drainage, and endoscopic procedures. This analysis, conducted in a simulated clinical environment with patient imaging data, demonstrated the system’s technical performance and overall utility, confirming its effectiveness in supporting neurosurgical procedures.
The concept of accuracy in MRN systems is often variably interpreted. Still, the
remains a widely recognized measure for gauging navigation accuracy, applicable from initial registration stages to later phases of surgical intervention. Despite potential complications such as brain-shift-induced non-linear deformations during later surgical stages, accurate initial registration is paramount, as it fundamentally influences the accuracy and dependability of all subsequent procedural stages [
26]. The
quantifies the discrepancy between specific points in the virtual environment and their real-world counterparts. The
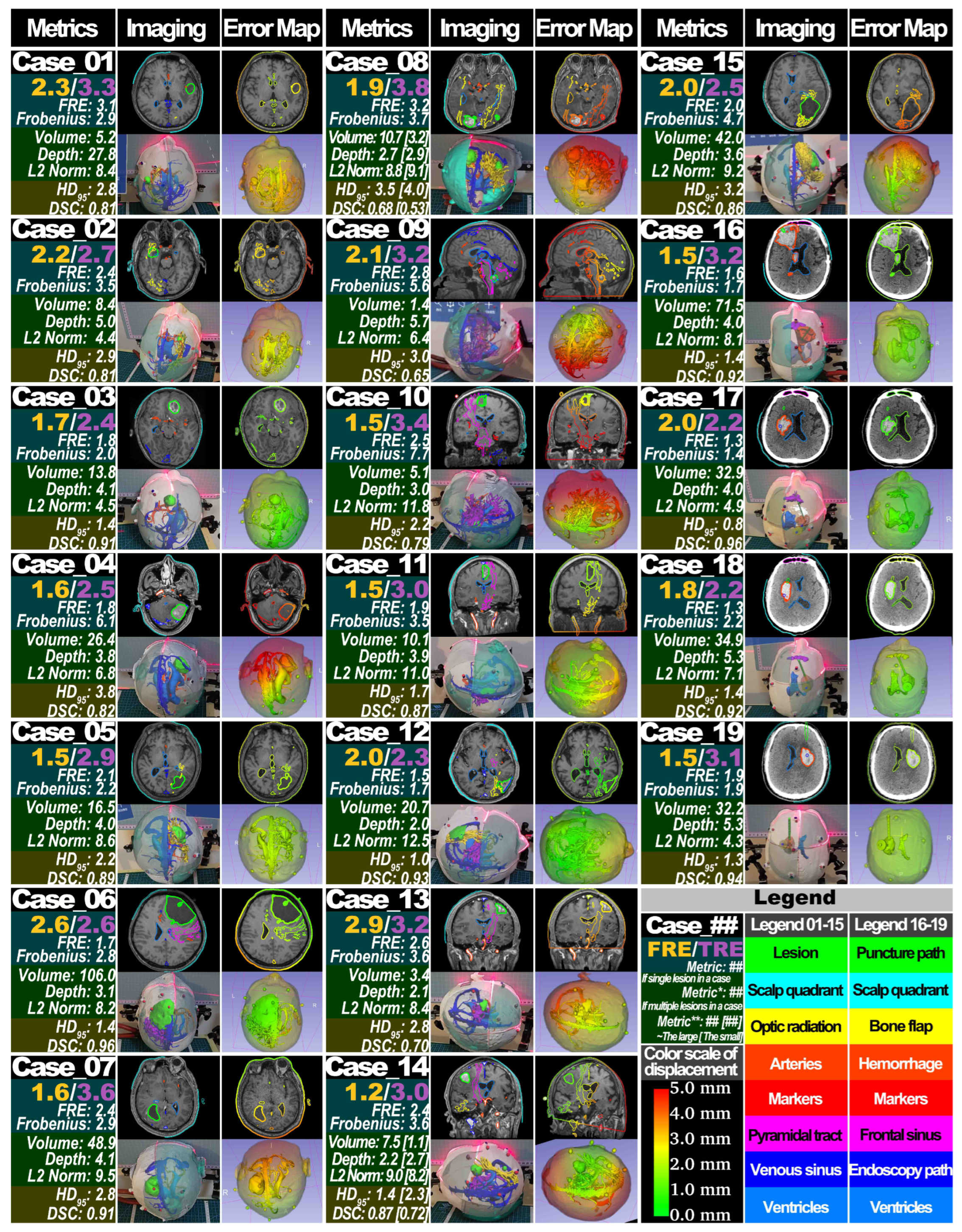
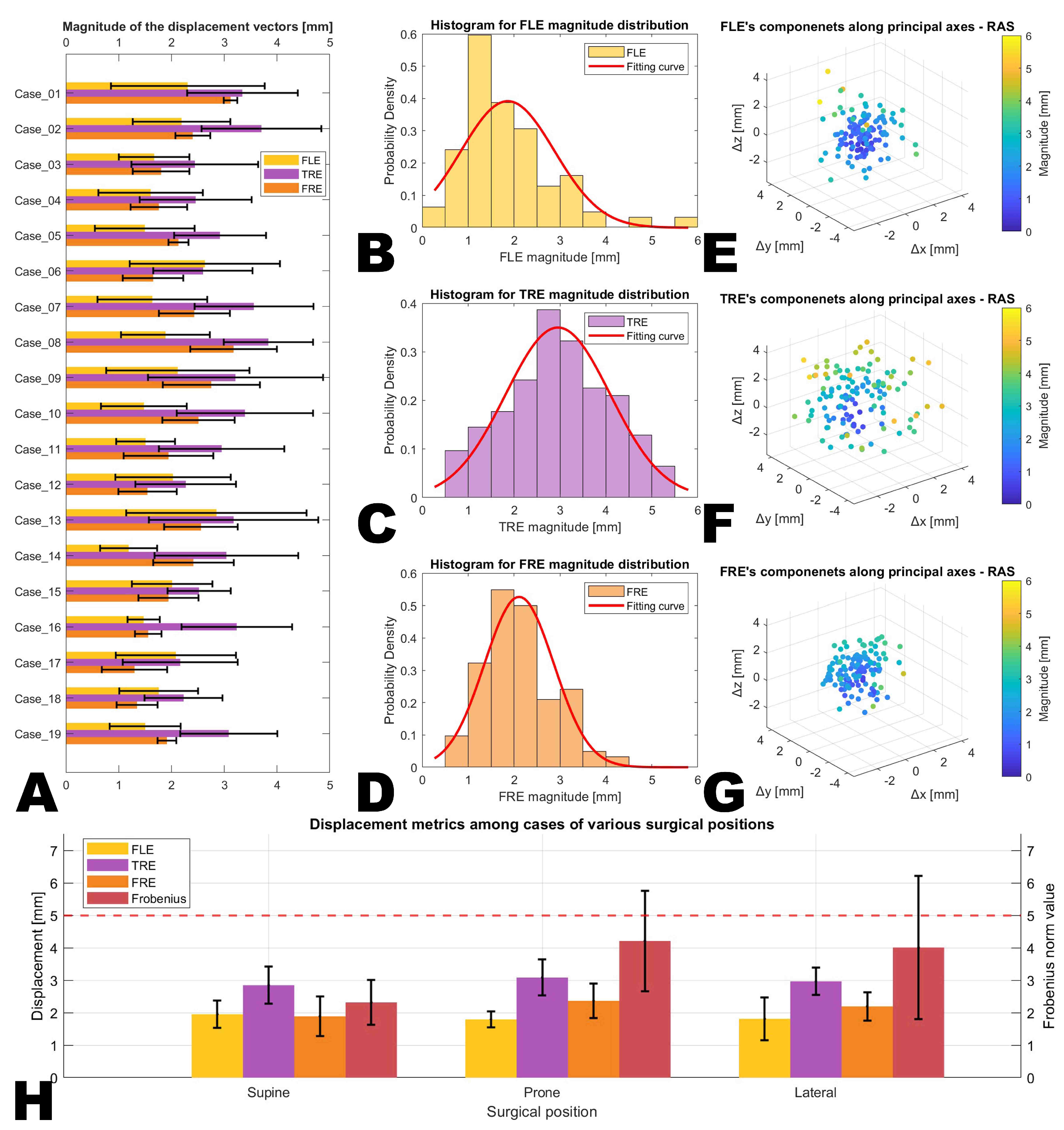
of LCS-MRN in this study was evaluated in a three-dimensional setting. The analyses showed an average
of 3.0 ± 0.5 mm, ranging from 0.6 mm to 5.4 mm. This outcome aligns closely with the
(3.7 ± 1.7 mm) observed in the single-case pilot study of LCS-MRN [
7], as well as another previous study on LCS-MRN using a fiducial-based approach showing an accuracy of 4.1 mm (interquartile range IQR 3.0–4.7 mm) [
8], and is also in line with the reported TRE in conventional navigation systems applying fiducial-base registration (3.49 ± 1.09 mm) [
45]. There appears to be a slight increase in accuracy with the proposed method employed in this study compared to the earlier approach, which might be related to automated approaches. However, it is important to note that these two approaches cannot be directly compared. The fiducial-based method’s accuracy was assessed using the projection error of lesions at the skin surface level as the metric for precision evaluation. While plenty of studies have examined the 3D
in MRN systems utilizing standalone HMDs, it is crucial to acknowledge that direct comparisons of
across these studies are not feasible, given the variations in their objectives and methodologies. The differences in these underline the unique aspects and context of each approach.
In mathematical terms, the
at specific points within this study’s context is considered a norm, necessitating the measurement of both virtual and physical points within the same coordinate space, either entirely virtual or physical. Distinct coordinate systems for each point prevent meaningful, direct measurements due to representation, scale, and direction differences. Most previous studies measured the
in the physical space using tools such as calipers, directly gauging the perceived distance between virtual and physical points [
8]. While straightforward, this approach risks underestimating the
, as virtual targets could be located underneath the patient or phantom. For deep-seated targets, alternative methods involve marking virtual point locations with physical instruments (e.g., puncture needles, bone anchors) and re-registering these on post-operative images to calculate
[
11,
22,
36,
39,
43]. This invasive approach, however, may alter the original structure and affect reliability.
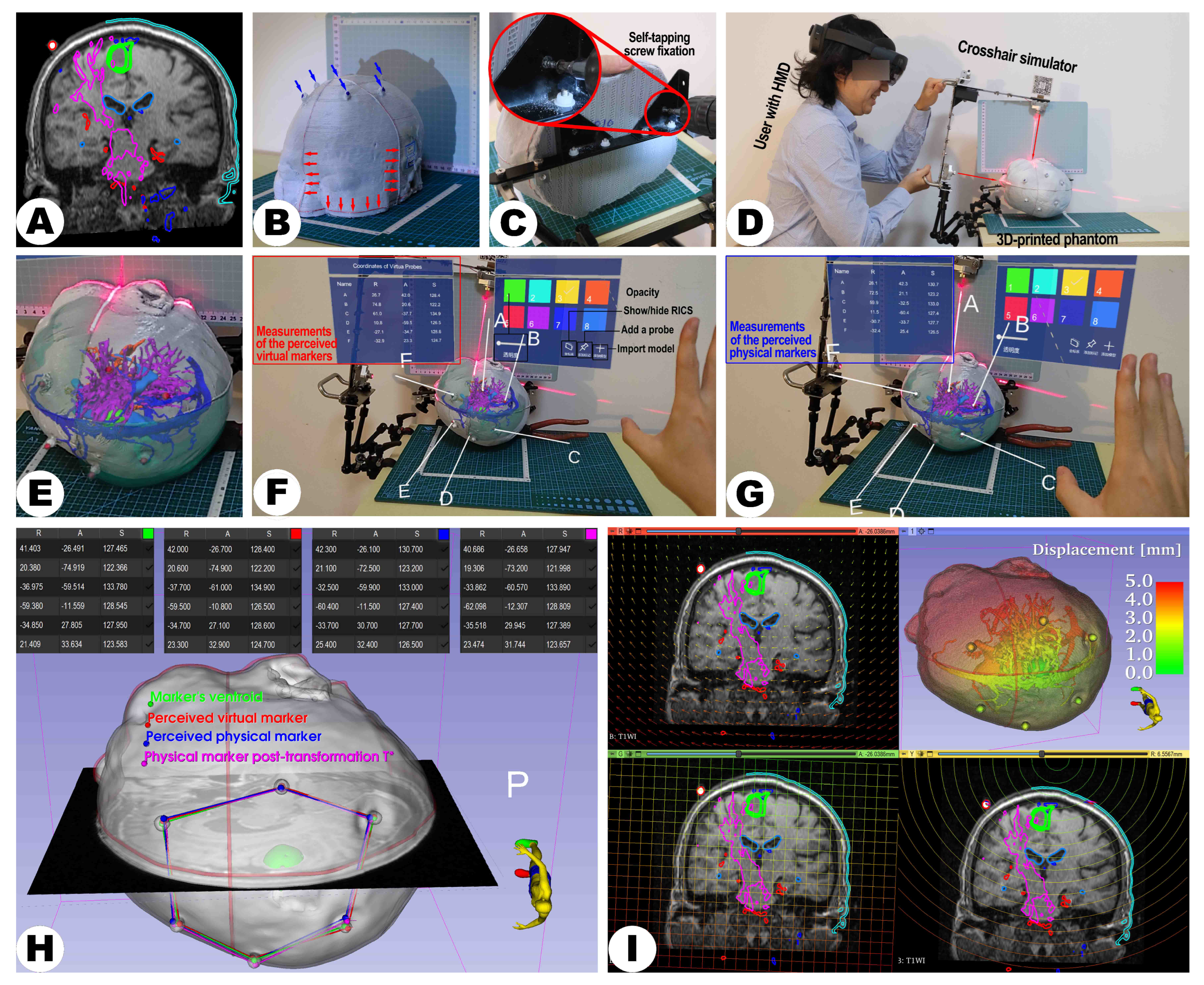
In contrast, virtual space measurements offer repeatability and non-invasiveness [
46,
47,
48]. The previous work regarding LCS-MRN developed a virtual probe for non-invasive, direct manual acquisition of actual marker points in virtual space, measuring the distance to virtual target counterparts [
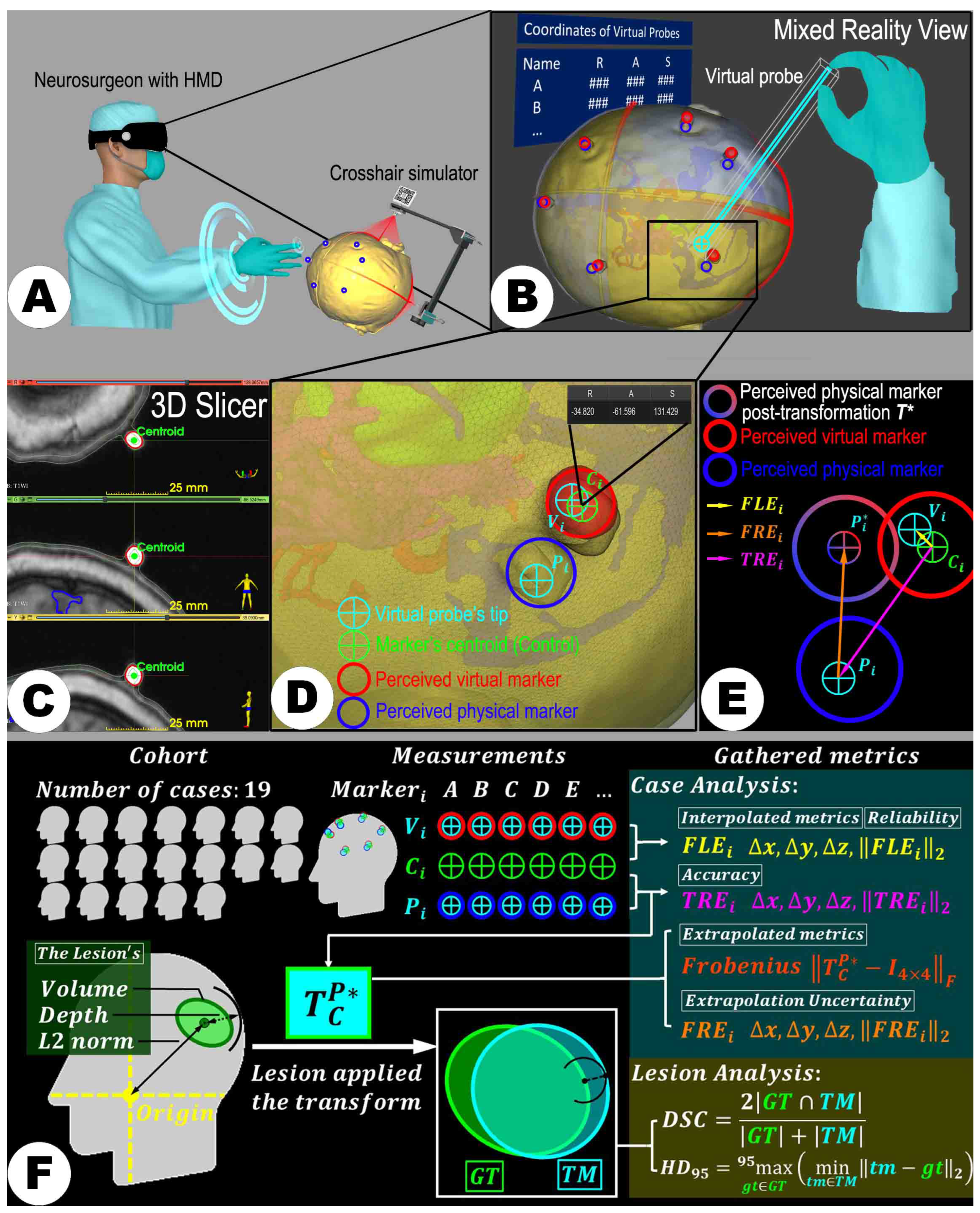
7]. However, moving and placing the virtual probe is subject to human error. To mitigate this, the study’s evaluations were conducted by a single neurosurgeon (Z.Q.) with extensive software/hardware and neurosurgery expertise. The
was introduced as a quality control parameter to reflect the potential inaccuracy due to manual operation. Worthy of note in the study’s design is that the placement of the point set
preceded that of point set
, allowing for the early acquisition of the reference metric
to prevent the accumulation of errors over time from affecting these baseline data, which reflect the quality of the assessment. Results indicated that
did not exceed
in any case, suggesting the manual error was well-monitored and did not compromise the credibility of
measurements.
Another issue worth noting is that the
indicates deviations at specific points, namely markers affixed to the skin surface, and does not necessarily represent the accuracy at the target level, such as lesions, eloquent structures, or proposed pathways, which remain inaccessible at that stage [
7,
12,
49]. The study adopted alternative non-invasive approaches to address this limitation. By computing the transformation
from the fiducials’ centroids in RICS to their observed physical counterparts, the positions of anatomical structures beneath the surface in the physical world are extrapolated in the RICS. Consequently, this allows for using a set of similarity metrics, such as DSC and HD
95, to represent the degree of overlap between virtual and physical models from volumetric and surface perspectives. While the two metrics are commonly used and effective in the context of image segmentation [
50,
51], their application in assessing the accuracy of AR or MR navigation systems, this methodology aligns with previous approaches [
52,
53], where DSC and Hausdorff Distance were similarly employed for assessment of navigation accuracy. Moreover, the study advocates using the “Segment compare” extension module in the open-source software platform 3D Slicer to calculate the DSC and HD
95. This approach effectively ensures convenience and repeatability in the evaluation process.
The LCS-MRN system, designed as a markerless registration framework, presents an intriguing paradox in its validation approach, which employs physical markers on a head phantom for verification purposes. Researchers collected perceived virtual and real point sets from these specific markers. It is important to note that all quantitative accuracy data in this study, both interpolative and extrapolative, are derived from measurements of these markers, both physical and virtual. Subsequently, these measurements are extrapolated to estimate the overall accuracy of the head model. This methodology may raise concerns regarding the representativeness of the extrapolated whole-head data, as it is potentially influenced by the distribution of the markers used in the study. Since the extrapolation is based on a limited set of points, the accuracy and reliability of the whole-head data might be skewed or limited by the spatial configuration, number, and placement of these markers [
54]. This concern is not unique to the LCS-MRN system, but is a common challenge in registration methods, including fiducial-based approaches. Several studies have explored the impact of maker distribution and placement on accuracy and reliability in fiducial-based registration methods [
45,
55]. In essence, the fidelity of the extrapolated data in representing the system’s performance across the entire head is contingent on the assumption that the markers provide a comprehensive and uniform representation of the head’s geometry. However, it is worth highlighting the success of these markers in facilitating accurate registration, evidenced not only in the context of the landmark-based MRN systems [
8,
23], but also in other applications, such as approaches based on an intraoperative scanner that assess TRE [
1,
2]. This success underscores their potential to be a reasonably reliable geometric reference for the entire head. This assertion is grounded in the premise that the strategic placement of markers, validated in earlier phases, might provide a global representativeness capable of inferring accuracy across the whole head. Extrapolation could be considered a pragmatic approach to gauge the system’s performance over the entire head region. It is important to note that, apart from landmark-based measures, other types of accuracy metrics may have been employed to assess the system’s performance comprehensively, such as angle difference [
56,
57], as well as parameters for nonlinear biomechanical modeling, such as Hausdorff distance [
58]. Additionally, artificial intelligence (AI) and machine learning (ML) could serve as innovative strategies in image analysis, especially in object detection tasks [
27], to assess and enhance the accuracy of the MRN system. For instance, regarding virtual-physical correspondence, AI can detect known physical points and their virtual counterparts, automatically computing registration quality parameters for error compensation, thereby improving its precision and reliability.
The LCS-MRN registration technique precisely projects and matches laser crosshairs on surfaces. A pilot study based on simulation modeling suggested that areas with smaller radii of curvature or more drastic curvature changes (e.g., nasal and zygomatic regions) provide more spatial information compared to larger or relatively flat curvature areas (e.g., temporal and occipital regions) [
7]. This enhanced spatial information facilitates easier identification and correction of LCS deployment errors by users. However, it is important to consider the practical application of these findings in a clinical setting. In clinical practice, the visibility and accessibility of different regions on the patient’s head during image acquisition vary. For instance, the occipital region is typically not visible during image acquisition, which poses challenges when relying on crosshair lines in this area for registration. In contrast, registration in the supine and lateral positions can use crosshair lines marked in the nasal, zygomatic, and temporal regions, which are more visible and accessible. The heterogeneous curvature of the human head implies that different challenges and accuracies may arise when performing LCS-MRN registration and localization in various body positions. Landmark-based and lesion-based accuracy analyses indicated larger registration errors in the prone position, as evidenced by increased
,
, HD
95, and DSC values. Although post hoc analysis of the
did not reveal pairwise statistically significant differences after Bonferroni-correction, the significantly heightened
without correction for multiple comparisons in the prone compared to the supine position remains noteworthy, especially considering the conservative nature of Bonferroni correction, which increases the risk of Type II errors in statistical inference. A plausible explanation for this observation is that registration in supine and lateral positions typically utilizes crosshair lines marked in the nasal and zygomatic regions, as well as the temporal region, whereas, in the prone position, registration predominantly relies on crosshair lines in the occipital and temporal regions. The latter scenario involves greater use of flatter areas, potentially increasing the likelihood of LCS deployment errors. In the lesion-based accuracy analysis, the magnitudes of DSC and HD
95 correspond well with the findings of the landmark-based analysis. However, despite some statistically significant differences in pairwise comparisons in the subgroup analysis, these differences cannot yet be considered engineering or clinical significance due to the imbalance in characteristics between the different positioning groups and small effect sizes.
Furthermore, the results indicated a positive correlation between the lesion volume and the DSC and a significant difference in LCS performance when localizing large lesions compared to smaller ones. The influence of lesion volume on DSC is frequently reported in automatic image segmentation [
50]. However, to our knowledge, this is the first time this study has identified it in the MRN domain. These findings may suggest that the system is more effective in localizing larger lesions than smaller ones. No significant correlations were found between lesion depth and the distance of the lesion from the RICS origin. Future research might require an increased sample size or enhanced effect size to explore these aspects more thoroughly.
Some limitations in the introduced LCS-MRN system and within this study must be addressed in future work. Although the LCS-MRN system has demonstrated effectiveness in the controlled environment of a phantom study, translating these results to a clinical setting introduces additional complexities. The requirement to draw marker lines on the patient’s skin surface during the scanning process for LCS-MRN registration carries several limitations and potential negative effects. Skin movement across different body positions can affect the accuracy and stability of these markers, as the skin may not be in the same position during surgery as it was during scanning. This is particularly in cases where the surgical position differs from the scanning position, such as supine versus prone, which is not unique to the LCS-MRN, but also to conventional navigation systems [
59]. Moreover, obtaining accurate marker lines for surgeries in prone or 3/4 prone positions can be challenging. When patients are scanned supine, the skin area required for the prone surgery markers is not exposed to the laser used for marking and is compressed or stretched, thereby hindering the line acquisition. Thus, the situation may introduce complexities not encountered in the controlled setting of a phantom study. Additional concerns include the risk of the lines being smudged or erased during patient transfer or preparation, which could compromise the registration process. All these factors underscore the need for a more robust and reliable method of establishing a reference frame for LCS-MRN registration in a clinical setting. Regarding this, a set of studies by Perkins et al. [
60,
61,
62], conducted in the context of breast surgery, where skin movement and geometrical distortion are prevalent, opens a new pathway for enhancing LCS-MRN systems. Their conclusive evidence that patterns printed with magnetic ink can be imaged and identified via MRI paves the way for using temporary, flexible skin adhesives printed with this specialized ink as dual-visible skin markings. These markings promise to remain discernible to the naked eye and within MR imaging, potentially significantly improving current skin marking techniques. It can be hypothesized that applying such MR-visible markers and adhesives could substantially mitigate the geometric distortions caused by skin movement in neurosurgical procedures, which are similarly subject to changes in skin topology between imaging and surgery. This would preserve the integrity of surgical navigation markers and contribute to the precision of LCS-MRN registration. Moreover, incorporating MR-visible ink into the LCS-MRN workflow could potentially enhance procedural efficiency by reducing the need for manual line drawing and realignment, thereby shortening the preparation time and decreasing the potential for human error. Thus, further research and development are necessary to integrate MR ink and grid stickers into clinical LCS-MRN systems, including validation studies to confirm their effectiveness and safety.
The current workflow of the LCS-MRN system, although based on the 3D Slicer platform, involves a degree of complexity due to the reliance on multiple extension modules. Future research will aim to develop a dedicated extension module for the LCS-MRN to streamline this process. This specialized module would integrate key functionalities to enhance system efficiency and user experience. It would encompass the compatibility processing of holograms, linear transformations, and the evaluation of reverse engineering metrics. By consolidating these processes into a user-friendly module, the system’s overall complexity can be significantly reduced, leading to a more streamlined and efficient workflow.
Building on the existing LCS-MRN system’s framework, the next development phase will focus on enhancing real-time capabilities and addressing the current limitations in neurosurgical planning. The current LCS-MRN system and its workflow may not fully support real-time neurosurgical planning as traditional standard navigation systems do, such as real-time planning via a workstation with immediate feedback to the surgeon. This limitation arises from the inability of HL-2 to independently perform complex and computationally intensive tasks like image segmentation and 3D reconstruction. These processes are currently executed on separate computers before being transferred to HMDs for holographic visualization. However, the LCS-MRN system, as reported in this study, introduces an innovative approach through specialized MR interactions, notably via virtual probe placement for digitized marking. This feature, distinct from conventional navigation systems, enables a form of indirect ’real-time’ planning. It allows surgeons to non-invasively and non-destructively mark crucial points or pathways intraoperatively, computing their spatial information, which is a unique advantage over traditional navigation systems in real-time planning scenarios. This approach is particularly practical and promising for identifying and compensating for intraoperative brain shift.
The LCS system exhibits certain limitations, evident through its visualization outcomes, aligning with findings from previous studies. The system faces tracking instability, particularly at certain viewing angles, due to its dependence on the Vuforia SDK and the HL-2’s PV camera [
63]. This instability is particularly problematic in the ‘Freeze’ mode, designed to stabilize the hologram’s position. In addition, there is an observed discrepancy between the positions used in preoperative imaging and those in the surgery, such as prone versus supine, leading to issues in registration accuracy. To address these challenges, a two-fold approach could be considered. Enhancing tracking stability might involve implementing alternative or supplementary tracking methods, which could provide stability across a wider range of viewing angles and overcome the limitations of the current hardware. Solutions for optimizing registration in various surgical positions could include aligning the scanning protocol of the preoperative imaging with the actual surgical positioning or integrating intraoperative imaging [
59,
64]. These methods would dynamically adapt the LCS system to the surgical environment, potentially further improving the accuracy and reliability of registration.
In addition to the broader challenges identified with the current methodology, the study is subject to some unique limitations. The current study is primarily a technical validation and proof of concept for the LCS-MRN system based on simulated neurosurgical procedures. It acknowledges the limitations in fully assessing its real-world effectiveness and applicability. Acknowledging this constraint, future research will involve methodical trials with human subjects better to understand the system’s performance in clinical scenarios and aim to conduct long-term studies involving actual surgical procedures. Thus, providing more comprehensive evidence of the system’s practical utility and reliability in real-world neurosurgical settings will be the next step. Moreover, while this initial investigation expands upon previous LCS-MRN research, it remains limited by an unbalanced sample size and a limited number of testers, which has constrained the study’s ability to extensively explore user experience and training. Recognizing this limitation, future studies are planned to more comprehensively evaluate the learning curve and user experience of the LCS-MRN system, especially in comparison to conventional paradigms, aiming to determine its ease of use and training needs for surgeons, which is vital for understanding its clinical practicality. In addition, this study did not include a comparative analysis with other state-of-the-art MRN paradigms due to objective constraints. Nevertheless, the evaluation methodology outlined, along with lesion-based and landmark-based metrics, facilitates future comparisons with various systems. Future research is anticipated to conduct these comparative studies, aiming for a comprehensive assessment of MRN technologies in neurosurgery.
Despite its challenges, the LCS-MRN system is promising and warrants continued refinement. The LCS-based registration improves earlier MRN registration techniques, offering a more straightforward, easy, and user-friendly process. Its streamlined hardware and software setup, coupled with the potential for increased accuracy and flexibility during potential surgical interventions, establishes this method as a noteworthy progression in developing cost-effective, user-friendly MRN systems for neurosurgical applications, leading to enhanced surgical results even in the absence of standard commercial navigation systems.



 ,
, 













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}