Biodegradable Scaffolds for Bone Regeneration Combined with Drug-Delivery Systems in Osteomyelitis Therapy



 , and
, and 
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Scaffolds for Bone Tissue Regeneration
2.1. Natural Polymers
2.2. Synthetic Biodegradable Polymers
2.3. Ceramics and Bioglasses
3. Scaffolds and Drug Delivery
4. Osteomyelitis and Osteomyelitis Therapy
5. Biodegradable Scaffold-Drug Delivery Systems for Osteomyelitis Treatment
- Proteins such as collagen, gelatin, and thrombin. Collagen-based materials are usually prepared from skin or tendon of animals and can provide sufficient stimulation for bone regeneration with osteoblast proliferation and increased mineralization. Collagen is an elemental part of connective tissue, it is found in all organs, and it does not induce toxicity. Moreover, drug content and elution properties depend on system porosity. In recent studies, local administration of antibiotic-loaded collagen sponges, associated with parenteral therapy, showed promising results for open fracture treatment [106].
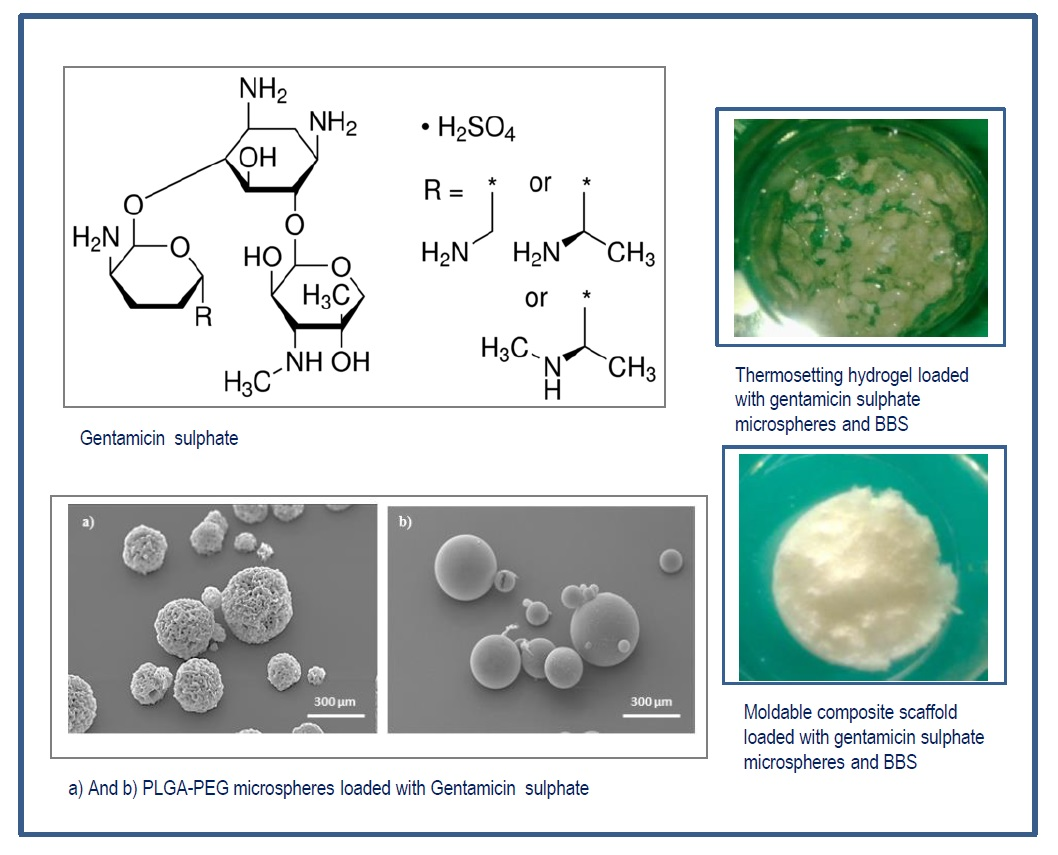
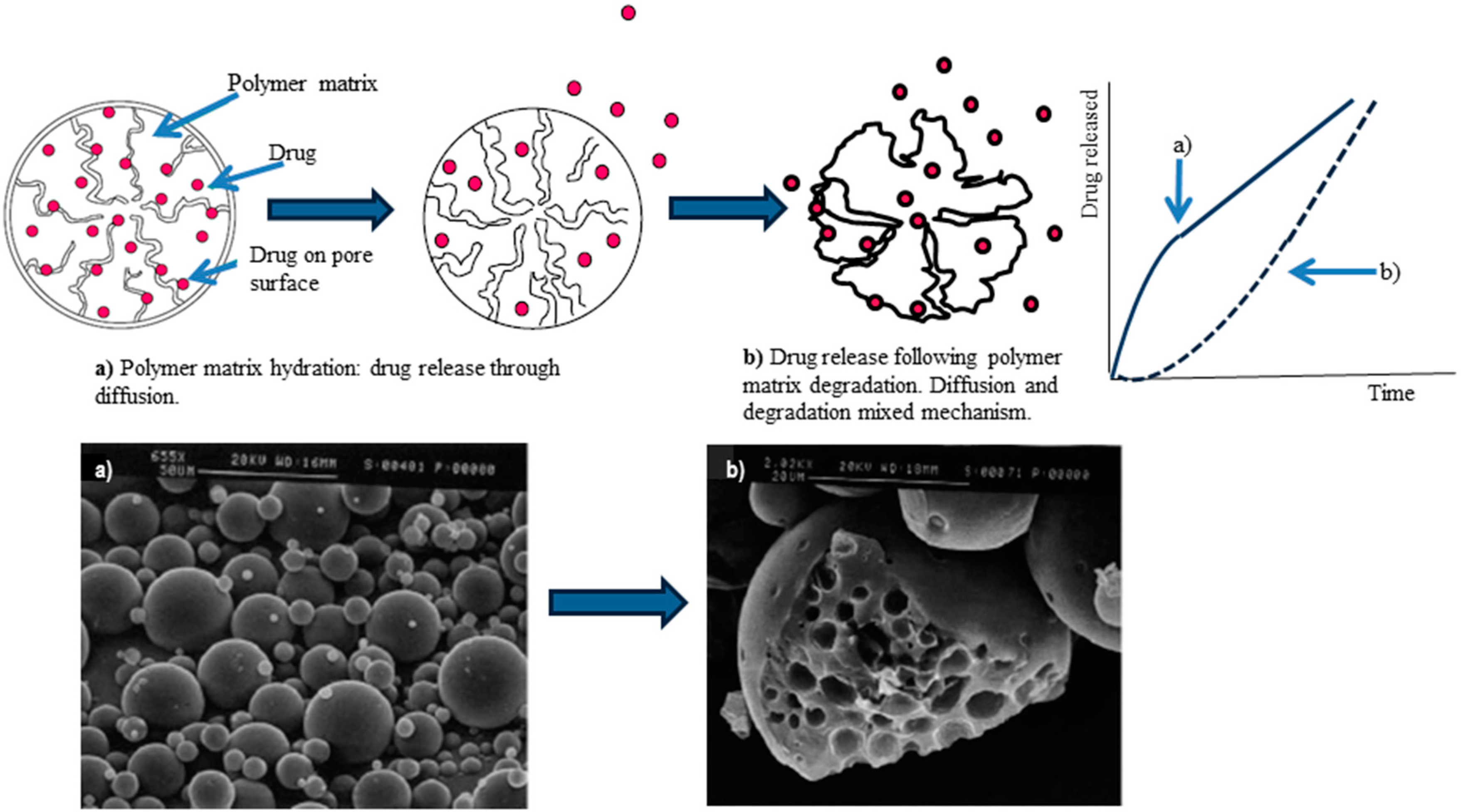
- Synthetic polymers like PLA, PLGA, PCL, their copolymers and pegylated derivatives. They are highly compatible with several antibiotics such as ampicillin, gentamicin, and polymixin-B. These materials can degrade very slowly (months or even years) at physiological pH, providing sustained release of antibiotics. Moreover, drug elution kinetics from these synthetic polymers can be modulated by changing physical, biochemical, and molecular structural properties of the polymer [108].
- Bone graft materials and substitutes. Some antibiotic-loaded bone grafts are available on the market, namely Simplex®P, Osteoset-T®, Collatamp®, Septocoll®, Septopal®, Herafill® beads, and Stimulan® [109]. Antibiotic can be added by directly mixing antibiotic powder to bone graft or soaking bone graft in an antibiotic solution. Due to its low immune reaction, structural properties, and easy reabsorption, calcium sulphate is also used to manage chronic osteomyelitis, and Osteoset-T® is a product on the market. Local application of calcium sulphate impregnated with tobramycin and vancomycin is effective to reduce infections due to implantation of prosthesis, also preventing colonization of bacteria and subsequent biofilm formation.
6. Conclusions
Conflicts of Interest
Abbreviations
| BBS | Bovine bone substitute granules |
| rhBMP-2 | Bone Morphogenetic Protein 2 recombinant |
| BCP | Biphasic calcium phosphate |
| CHS | Chitosan |
| CMC | Carboxymethyl cellulose |
| DDS | Drug delivery system |
| DoE | Design of experiment |
| ECM | Extra Cellular Matrix |
| EMA | European Medicines Agency |
| FDA | Food and Drug Administration |
| FEUNp | Polydopamine-coated eumelanin nanoparticles |
| FEUNp-GS | Gentamicin sulphate loaded polydopamine coated eumelanin nanoparticles |
| GFs | Growth factors |
| β-GP | β-glycerophosphate |
| HA | Hyaluronic acid |
| HAP | Hydroxyapatite |
| HCA | Hydrocarbonate apatite |
| ITCS | Injectable thermosetting composite scaffolds |
| mCS | 3D moldable composite scaffold |
| Nps | Nanoparticles |
| PANH | Poly (1,6-bis-(p-carboxyphenoxy hexane)-co-(sebacic anhydride) |
| PCL | Polycaprolactone |
| PCL-gHAP | poly(ɛ-caprolactone) grafted to hydroxyapatite (PCL-gHAP) |
| PGA | Polyglycolic acid |
| PLA | Polylactide |
| PLGA | Polylactide-co-glycolide |
| PLGA-PEG | Polylactide-co-glycolide-co-polyethylenglycol |
| PMMA | Polymethylmethacrylate |
| PPF | Poly(propylene fumarate |
| β-TCP | β-tricalcium phosphate |
| TE | Tissue engineering |
| ZIF-8 | Zeolitic imidazolate framework-8 |
References
- Lanza, R.; Langer, R.; Vacanti, J. Principles of Tissue Engineering, 4th ed.; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Kumas, V.; Abbas, A.K.; Fousto, N.; Aster, J. Tissue renewal, regeneration, and repair. In Robbins and Cotran Pathologic Basis of Disease, 9th ed.; Elsevier: Amsterdam, The Netherlands, 2014; Chapter 3. [Google Scholar]
- Samorezov, J.E.; Alsberg, E. Spatial regulation of controlled bioactive factor delivery for bone tissue engineering. Adav. Drug Deliv. Rev. 2015, 84, 45–67. [Google Scholar] [CrossRef] [PubMed]
- Rambhia, K.J.; Ma, P.X. Controlled release for tissue engineering. J. Control. Release 2015, 219, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Vo, T.N.; Kasper, F.K.; Mikos, A.G. Strategies for controlled delivery of growth factors and cells for bone regeneration. Adv. Drug Deliv. Rev. 2012, 64, 1292–1309. [Google Scholar] [CrossRef] [PubMed]
- Turner, N.J.; Badylak, S.F. Biological scaffolds for muscolotendinous tissue repair. Eur. Cell Mater. 2013, 25, 130–143. [Google Scholar] [CrossRef] [PubMed]
- Awada, H.K.; Johnson, N.R.; Wang, Y. Sequential delivery of angigenic growth factorss improves revascularization and heart function after myocardial infarction. J. Control. Release 2015, 207, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.C.; Lee, B.G.; Park, D.W.; Kim, K.; Chu, H.; Kim, K.; Huard, J.; Wang, Y. Controlled dual delivery of fibroblast growth factor-2 and interleukin-10 by heparin-based coacervate synergistically enhances ischemic heart repair. Biomaterials 2015, 72, 138–151. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.M.; Zhang, M.; Wu, Z.F. Towards delivery of multiple growth factors in tissu engineering. Biomaterials 2010, 31, 6279–6308. [Google Scholar] [CrossRef] [PubMed]
- Basmanav, F.B.; Kose, G.T.; Hasirci, V. Sequential growth factor delivery from complexed microspheres for bone tissue engineering. Biomaterials 2008, 29, 4195–4204. [Google Scholar] [CrossRef] [PubMed]
- Long, D.W.; Johnson, N.R.; Jeffries, E.M.; Hara, H.; Wang, Y. Controlled delivery of platelet-derived proteins enhances porcine wound healing. J. Control. Release 2017, 253, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Gu, Q.; Chen, M.; Zhang, C.; Chen, S.; Zhao, J. Controlled delivery of icariin on small intestine submucosa for bone tissue engineering. Mater. Sci. Eng. C 2017, 71, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Cooke, M.J.; Sachewsky, N.; Morshead, C.M.; Shoichet, M.S. Bioengineered sequential growth factor delivery stimulates brain tissue regeneration after stroke. J. Control. Release 2013, 171, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Thatiparti, T.R.; Shoffstal, A.J.; Von Recum, H.A. Cyclodextrin-based device coatings for affinity-based release of antibiotic. Biomaterials 2010, 31, 2335–2347. [Google Scholar] [CrossRef] [PubMed]
- Azodi-Delami, S.; Abdouss, M.; Kordestani, D. Synthesis and characterization of the magnetic molecularly imprinted polymer nanoparticles using N,N-bis methacryloyil ethylenediamine as a new cross-linking agent for controlled release of meloxicam. Appl. Biochem. Biotechnol. 2014, 172, 3271–3286. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, H.; Vedantham, K.; Young, A.A.; Marrito, I.; El-Gannam, A. Tissue engineering scaffold for sequential release of vancomycin and rhBMP2 to treat bone infections. J. Biomed. Mater. Res. A 2014, 102, 4213–4223. [Google Scholar] [CrossRef] [PubMed]
- Li, I.; Zhou, G.; Wang, Y.; Yang, G.; Ding, S.; Zhou, S. Controlled dual delivery of BMP-2 and dexamethasone by nanoparticle-embedded electrospun nanofibers for the efficient repair of critical-sized rat calvarial defect. Biomaterials 2015, 37, 218–229. [Google Scholar] [CrossRef] [PubMed]
- Dreifke, M.B.; Ebraheim, N.A.; Jayasuriya, A.C. Investigation of potential injectable polymeric biomaterials for bone regeneration. J. Biomed. Mater. Res. A 2013, 101, 2436–2447. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.; Qi, C.; Chen, Y.-X.; Zhu, Y.J.; Sun, T.-W.; Chen, F.; Zhang, C.-Q. Comparative study of porous hydroxyapatite/chitosan and whitlockite/chitosan scaffolds for bone regeneration in calvarial defects. Int. J. Nanomed. 2017, 12, 2673–2687. [Google Scholar] [CrossRef] [PubMed]
- Ishack, S.; Mediero, A.; Wilder, T.; Ricci, J.L.; Cronstein, B.N. Bone regeneration in critical bone defects using three-dimensionally printed β-tricalcium phosphate/hydroxyapatite scaffolds is enhanced by coating scaffolds with either dipyridamole or BMP-2. J. Biomed. Mater. Res. 2017, 105, 366–375. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Hernadez, J.M.; Escobar-Garcia, D.M.; Escalante, A.; Flores, H.; Gonzales, F.J.; Gatenholm, P.; Toriz, G. In vitro evaluation of osteoblastic cells on bacterial cellulose modified with multi-walled carbon nanotubes as scaffold for bone regeneration. Mater. Sci. Eng. C 2017, 75, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Biondi, M.; Ungaro, F.; Quaglia, F.; Netti, P.A. Controlled drug delivery in tissue regeneration. Adv. Drug Deliv. Rev. 2008, 60, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Polo-Corrales, L.; Latorre-Esteves, M.; Ramirez-Vick, J.E. Scaffold Design for Bone Regeneration. J. Nanosci. Nanotechnol. 2014, 14, 15–56. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.M.; Schenker, M.L.; Ahn, J.; Willett, N.J. Building better bone: The weaving of biologic and engineering strategies for managing bone loss. J. Orthop. Res. 2017, 35, 1855–1864. [Google Scholar] [CrossRef] [PubMed]
- Ye, F.; Zeng, Z.; Wang, J.; Liu, H.; Wang, H.; Zheng, Z. Comparison of the use of rhBMP-7 versus iliac crest autograft in single-level lumbar fusion: A meta-analysis of randomized controlled trials. J. Bone Miner. Metab. 2017. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Ji, Q.; Chen, X.; Sun, Y.; Xu, Q.; Deng, P.; Hu, F.; Yang, J. Accelerated bony defect healing based on chitosan thermosensitive hydrogel scaffolds embedded with chitosan nanoparticles for the delivery of BMP2 plasmid DNA. J. Biomed. Mater. Res. Part A 2017, 105A, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Benazzo, F.; Botta, L.; Scaffino, M.F.; Caliogna, L.; Marullo, M.; Fusi, S.; Gastaldi, G. Trabecular titanium can induce in vitro osteogenic differentiation of adipose derived stem cells without osteogenic factors. J. Biomed. Mater. Res. A 2014, 102, 2061–2071. [Google Scholar] [CrossRef] [PubMed]
- Asti, A.; Gastaldi, G.; Dorati, R.; Saino, E.; Conti, B.; Visai, L.; Benazzo, F. Stem cells grown in osteogenic medium on PLGA, PLGA/HA, and titanium scaffold for surgical applications. Bioinorg. Chem. Appl. 2010. [Google Scholar] [CrossRef] [PubMed]
- Böhrnsen, F.; Rublack, J.; Aeckerle, N.; Foerster, A.; Schwenzer, B.; Reichert, J.; Scharnweber, D.; Schliephake, H. Bone Morphogenetic Protein-2 Hybridized with Nano-Anchored Oligonucleotides on Titanium Implants Enhances Osteogenic Differentiation In Vivo. Int. J. Oral Maxillofac. Implant. 2017, 32, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Camargo, W.A.; Takemoto, S.; Hoekstra, J.W.; Leewenburgh, S.C.; Jansen, J.A.; Van den Beucken, J.J.J.P.; Alghamdi, H.S. Effect of surface alkali-based treatment of titanium implants on ability to promote in vitro mineralization and in vivo bone formation. Acta Biomater. 2017, 15, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Witte, F.; Lu, F.; Wang, J.; Li, J.; Qin, L. Current status on clinical applications of magnesium-based orthopaedic implants: A review from clinical translational perspective. Biomaterials 2017, 112, 287–302. [Google Scholar] [CrossRef] [PubMed]
- AlTamini, A.A.; Rui Alves Fernandes, P.; Peach, C.; Cooper, G.; Diver, C.; Bartolo, P.J. Metallic bone fixation implants: A novel design approach for reducing the stress shielding phenomenon. Virtual Phys. Prototyp. 2017, 12, 141–151. [Google Scholar] [CrossRef]
- Shivaram, A.; Bose, S.; Bandyopadhyay, A. Understanding long-term silver release from surface modified porous titanium implants. Acta Biomater. 2017, 58, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zhang, X.; Huang, C.; Cai, H.; Hu, S.; Wan, Q.; Pei, X.; Wang, J. Osteogenic activity and antibacterial effect of porous titanium modified with metal-organic framework films. J. Biomed. Mater. Res. Part A 2017, 105, 834–846. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.F. On the mechanisms of biocompatibility. Biomaterials 2008, 29, 2941–2953. [Google Scholar] [CrossRef] [PubMed]
- Dorati, R.; Colonna, C.; Genta, I.; Conti, B. Polymer Scaffolds for Bone Tissue Regeneration. In Active Implants and Scaffolds for Tissue Regeneration; Zilberman, M., Ed.; Studies in Mechanobiology, Tissue Engineering and Biomaterials Book Series; Springer: Berlin, Germany, 2011; Volume 8, pp. 259–285. [Google Scholar]
- Wu, J.; Xie, L.; Zhi, W.; Lin, Y.; Chen, Q. Biomimetic nanofibrous scaffolds for neural tissue engineering and drug development. Drug Discov. Today 2017, 22, 1375–1384. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Chen, Q.; Liu, W.; He, Z.; Lin, J.-M. Recent advances in microfluidic 3D cellular scaffolds for drug assays. Trends Anal. Chem. 2017, 87, 19–31. [Google Scholar] [CrossRef]
- Krishnakumar, G.S.; Gostynska, N.; Campodoni, E.; Dapporto, M.; Montesi, M.; Panseri, S.; Tampieri, A.; Kon, E.; Marcacci, M.; Sprio, S.; et al. Ribose mediated crosslinking of collagen-hydroxyapatite hybrid scaffolds for bone tissue regeneration using biomimetic strategies. Mater. Sci. Eng. C 2017, 77, 594–605. [Google Scholar] [CrossRef] [PubMed]
- Martínez, A.; Blanco, M.D.; Davidenko, N.; Cameron, R.E. Tailoring chitosan/collagen scaffolds for tissue engineering: Effect of composition and different crosslinking agents on scaffold properties. Carbohydr. Polym. 2015, 132, 606–619. [Google Scholar] [CrossRef] [PubMed]
- Basu, P.; Sharan, B.S.; Narendra Kumar, U.; Manjubala, I. Polymer Ceramic Composite for Bone Regeneration Application. Int. J. ChemTech Res. 2014, 6, 4038–4041. [Google Scholar]
- Saravanan, S.; Chawla, A.; Vairamani, M.; Sastry, T.P.; Subramanian, K.S.; Selvamurugan, M. Scaffolds containing chitosan, gelatin and graphene oxide for bone tissue regeneration in vitro and in vivo. Int. J. Biol. Macromol. 2017, 104, 1975–1985. [Google Scholar] [CrossRef] [PubMed]
- Xue, C.; Ren, H.; Zhu, H.; Gu, X.; Guo, Q.; Zhou, Y.; Huang, J.; Wang, S.; Zha, G.; Gu, J.; et al. Bone marrow mesenchymal stem cell-derived acellular matrix-coated chitosan/silk scaffolds for neural tissue regeneration. J. Mater. Chem. B 2017, 5, 1246–1257. [Google Scholar] [CrossRef]
- Chevrier, A.; Darras, V.; Picard, G.; Nelea, M.; Veilleux, D.; Lavertu, M.; Hoemann, C.D.; Buschman, M.D. Injectable chitosan-platelet-rich plasma implants to promote tissue regeneration: In vitro properties, in vivo residence, degradation, cell recruitment and vascularization. J. Tissue Eng. Regen. Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Tonda-Turo, C.; Ruini, F.; Ramella, M.; Boccafoschi, F.; Gentile, P.; Gioffredi, E.; Falvo D’Urso Labate, G. Non-covalently crosslinked chitosan nanofibrous mats prepared by electrospinning as substrates for soft tissue regeneration. Carbohydr. Polym. 2017, 162, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Dorati, R.; Colonna, C.; Genta, I.; De Trizio, A.; Modena, T.; Klöss, H.; Conti, B. In vitro characterization of an injectable in situ forming composite system for bone reconstruction. Polym. Degrad. Stab. 2015, 119, 151–158. [Google Scholar] [CrossRef]
- Li, G.C.; Li, J.; Tian, X.J.; Cheng, X.; He, B.; Wang, H.M. Microstructure and properties of a novel titanium alloy Ti-6Al-2V-1.5Mo-0.5Zr-0.3Si manufactured by laser additive manufacturing. Mater. Sci. Eng. A 2017, 684, 233–238. [Google Scholar] [CrossRef]
- Cho, J.H.; Kim, S.H.; Park, K.D.; Jung, M.C.; Yang, W.I.; Han, S.W.; Noh, J.Y.; Lee, J.W. Chondrogenic differentiation of human mesenchymal stem cells using a thermosensitive poly(N-isopropylacrylamide) and water-soluble chitosan copolymer. Biomaterials 2004, 25, 5743–5751. [Google Scholar] [CrossRef] [PubMed]
- Dorati, R.; Colonna, C.; Genta, I.; Modena, T.; Conti, B. Effect of porogen on the physico-chemical properties and degradation performance of PLGA scaffolds. Polym. Degrad. Stab. 2010, 95, 694–701. [Google Scholar] [CrossRef]
- Stevens, M.M. Biomaterials for bone tissue engineering. Mater. Today 2008, 11, 18–25. [Google Scholar] [CrossRef]
- Ku, K.-L.; Grøndahl, L.; Dao, H.; Du, K.; Puttick, S.; Lai, P.-L.; Peng, H.; Chu, I.-M.; Whittaker, A.K. In vitro degradation study of polyanhydride copolymers/surface grafted hydroxyapatite composites for bone tissue application. Polym. Degrad. Stab. 2017, 140, 136–146. [Google Scholar] [CrossRef]
- Deng, M.; Kumbar, S.G.; Nair, L.S.; Weikel, A.L.; Allcock, H.R.; Laurencin, C.T. Biomimetic structures: Biological implications of dipeptide-substituted polyphosphazene-polyester blend nanofiber matrices for load-bearing bone regeneration. Adv. Funct. Mater. 2011, 21, 2641–2651. [Google Scholar] [CrossRef]
- Ogueri, K.S.; Ivirico, J.L.E.; Nair, L.S.; Allcock, H.R.; Laurencin, C.T. Biodegradable Polyphosphazene-Based Blends for Regenerative Engineering. Regen. Eng. Transl. Med. 2017, 3, 15–31. [Google Scholar] [CrossRef] [PubMed]
- Bouler, J.M.; Pilet, P.; Gauthier, O.; Verron, E. Biphasic calcium phosphate ceramics for bone reconstruction: A review of biological response. Acta Biomater. 2017, 53, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hench, L.L. Bioactive materials: The potential for tissue regeneration. J. Biomed. Mater. Res. 1998, 41, 511–518. [Google Scholar] [CrossRef]
- Hench, L.L. Bioceramics: From concept to clinic. J. Am. Ceram. Soc. 1991, 74, 1487–1510. [Google Scholar] [CrossRef]
- Hench, L.L.; Splinter, R.J.; Allen, W.C.; Greenlee, T.K., Jr. Bonding mechanisms at the interface of ceramic prosthetic materials. J. Biomed. Mater. Res. 1971, 2, 117–141. [Google Scholar] [CrossRef]
- Hench, L.L.; Polak, J.M. Third-generation biomedical materials. Science 2002, 295, 1014–1017. [Google Scholar] [CrossRef] [PubMed]
- Rahaman, M.N.; Day, D.E.; Bal, B.S.; Fu, Q.; Jung, S.B.; Bonewald, L.F.; Tomsia, A.P. Bioactive glass in tissue engineering. Acta Biomater. 2011, 7, 2355–2373. [Google Scholar] [CrossRef] [PubMed]
- Gerhardt, L.C.; Boccaccini, A.R. Bioactive glass and glass-ceramic scaffolds for bone tissue engineering. Materials 2010, 3, 3867–3910. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, E.; Bretcanu, O.A.; Marshall, M.; Birch, M.A.; McCaskie, W.; Dalgamo, K.W. Novel biolasses for bone tissue repair and regeneration: Effect of glass design on sintering ability, ion release and biocompatibility. Mater. Des. 2017, 129, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.R. Review of bioactive glass: From Hench to hybrids. Acta Biomater. 2013, 9, 4457–4486. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.H.; El-Amin, S.E.; Scott, K.D.; Laurencin, C.T. Three-dimensional, bioactive, biodegradable, polymer-bioactive glass composite scaffolds with improved mechanical properties support collagen synthesis and mineralization of human osteoblast-like cells in vitro. J. Biomed. Mater. Res. Part A 2003, 64A, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Allo, B.A.; Rizkalia, A.S.; Mequanint, K. Synthesis and electrospinning of epsilon-polycaprolactone-bioactive glass hybrid biomaterials via a sol-gel process. Langmuir 2010, 26, 18340–18348. [Google Scholar] [CrossRef] [PubMed]
- Gomide, V.S.; Zonari, A.; Ocarino, N.M.; Goes, A.M.; Serakides, R.; Pereira, M.M. In vitro and in vivo osteogenesis potential of bioactive glass-PVA hybrid scaffolds colonized by mesenchymal stem cells. Biomed. Mater. 2012, 7. [Google Scholar] [CrossRef] [PubMed]
- El-Batal, F.H.; El-Kheshen, A.A.; El Aty, A.A.A.; El-Bassyouni, G.T. Studies of Bone-Bonding Ability and Antibacterial Properties of Ag+, Cu2+ or Zn2+ ions Doping within Hench’s Bioglass and Glass-Ceramic Derivatives. Silicon 2017. [Google Scholar] [CrossRef]
- Mariappan, C.R.; Ranga, N. Influence of silver on the structure, dielectric and antibacterial effect of silver doped bioglass-ceramic nanoparticles. Ceram. Int. 2017, 43, 2196–2201. [Google Scholar] [CrossRef]
- Echezarreta-López, M.M.; De Miguel, T.; Quintero, F.; Pou, J.; Landin, M. Fabrication of Zn-Sr-doped laser-spinning glass nanofibers with antibacterial properties. J. Biomater. Appl. 2017, 31, 819–831. [Google Scholar] [CrossRef]
- Rivadeneira, J.; DiVirgilio, A.L.; Audisio, M.C.; Boccaccini, A.R.; Gorustovich, A.A. 45S5 Bioglass® concentrations modulate the release of vancomycin hydrochloride from gelatin-starch films: Evaluation of antibacterial and cytotoxic effects. J. Mater. Sci. 2017, 52, 9091–9102. [Google Scholar] [CrossRef]
- Dorati, R.; Genta, I.; Ferrari, M.; Vigone, G.; Merico, V.; Garagna, S.; Zuccotti, M.; Conti, B. Formulation and stability evaluation of 3D-alginate beads potentially useful for cuumuls oocyte complexes culture. J. Microencapsul. 2016, 33, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Galvez-Martín, P.M.; Martin, J.M.; Ruiz, A.; Clares, B. Encapsulation in Cell Therapy: Methodologies, Materials, and Clinical Applications. Curr. Pharm. Biotechnol. 2017, 18, 365–377. [Google Scholar] [CrossRef] [PubMed]
- Klausner, E.A.; Zhang, Z.; Wong, S.P.; Chapman, R.L.; Volin, M.V.; Harbottle, R.P. Corneal gene delivery: Chitosan oligomer as a carrier of CpG rich, CpG free or S/MAR plasmid DNA. J. Gene Med. 2012, 14, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Chaimov, D.; Baruch, L.; Krishtul, S.; Meivar-Levy, I.; Ferber, S.; Machluf, M. Innovative encapsulation platform based on pancreatic extracellular matrix achieve substantial insulin delivery. J. Control. Release 2017, 257, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, R.; Alexander, M.; Robles, L.; Foster, C.E., 3rd; Lakey, J.R. Islet and stem cell encapsulationfor clinical transplantation. Rev. Diabet. Stud. 2014, 11, 84–101. [Google Scholar] [CrossRef] [PubMed]
- Kizilel, S.; Scavone, A.; Liu, X.; Nothia, J.M.; Ostrega, D.; Witowski, P.; Millis, M. Encapsulation of pancreatic islets within nano-thin functional polyethylene glycol coatings for enhanced insulin secretion. Tissue Eng. Part A 2010, 16, 2217–2228. [Google Scholar] [CrossRef] [PubMed]
- Robles, L.; Storrs, R.; Lamb, M.; Alexander, M.; Lakey, J.R. Current status of islet encapsulation. Cell Transplant. 2014, 23, 1321–1348. [Google Scholar] [CrossRef] [PubMed]
- Costa, P.F.; Puga, A.M.; Diaz-Gomez, L.; Concheiro, A.; Busch, D.H.; Alvarez-Lorenzo, C. Additive manufacturing of scaffolds with dexamethasone controlled release for enhanced bone regeneration. Int. J. Pharm. 2015, 496, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Sabaeifard, P.; Abdi-Ali, A.; Soudi, R.M.; Gamazo, C.; Irache, M.J. Amikacin loaded PLGA nanoparticles against Pseudomonas aeruginosa. Eur. J. Pharm. Sci. 2016, 93, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Saidykhan, L.; Abu Bakar, M.Z.; Rukayadi, Y.; Kura, A.U.; Latifah, S.Y. Development of nanoantibiotic delivery system using cockle shell-derived aragonite nanoparticles for treatment of osteomyelitis. Int. J. Nanomed. 2016, 11, 661–673. [Google Scholar]
- Isa, T.; Zakaria, Z.A.; Rukayadi, Y.; Mohd Hezmee, M.N.; Jaji, A.Z.; Imam, M.U.; Hammadi, I.; Mahmood, K. Antibacterial activity of ciprofloxacina-encapsulated cockle shells calcium carbonate (aragonite) nanoparticles and its biocompatability in macrophages J774A.1. Int. J. Mol. Sci. 2016, 17, 713. [Google Scholar] [CrossRef] [PubMed]
- Abdelghany, S.M.; Quinn, D.J.; Ingram, R.J.; Gilmore, B.F.; Donnelly, R.F.; Taggart, C.C.; Scott, C.J. Gentamicin-loaded nanoparticles show improved antimicrobial effects towards Pseudomonas aeruginosa infection. Int. J. Nanomed. 2012, 7, 4053–4063. [Google Scholar]
- Stanton, T.; Haas, J.; Phillips, M.; Immerman, I. Study Points to Savings with Infection-Screening Program before TJR. AAOS Now. 2010. Available online: http://www.aaos.org/news/aaosnow/mar10/clinical10.asp (accessed on 1 June 2011).
- Posadowoska, U. Gentamicin loaded PLGA nanoparticles as local drug delivery system for the osteomyelitis treatment. Acta Bioeng. Biomech. 2015, 17, 41–48. [Google Scholar]
- Wang, L.; Hu, C.; Shao, L. The antimicrobial activity of nanoparticles: Present situation and prospects for the future. Int. J. Nanomed. 2017, 12, 1227–1249. [Google Scholar] [CrossRef] [PubMed]
- Uçkay, L.; Hoffmeyer, P.; Lew, D.; Pittet, D. Prevention of surgical site infections in orthopedic surgery and bone trauma: State-of-the-art update. J. Hosp. Infect. 2013, 84, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Axford, J.S. Joint and bone infections. Medicine 2010, 38, 194–201. [Google Scholar] [CrossRef]
- Birt, M.C.; Anderson, D.W.; Toby, E.B.; Wang, J. Osteomyelitis: Recent advances in pathophysiology and therapeutic strategies. J. Orthop. 2017, 14, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Reizner, W.; Hunter, J.G.; O’Malley, N.T.; Southgate, R.D.; Schwarz, E.M.; Kates, S.L. A systemic review of animal models for staphylococcus aureous osteomyelitis. Eur. Cells Mater. 2014, 27, 192–212. [Google Scholar]
- Pandey, K.C. Optimal management of chronic osteomyelitis: Current perspectives. Orthop. Res. Rev. 2015, 7, 71–81. [Google Scholar] [CrossRef]
- Winkler, H.; Haiden, P. Treatment of chronic bone infection. Oper. Tech. Orthop. 2016, 26, 2–11. [Google Scholar] [CrossRef]
- Nandi, S.K.; Bandyopadhyay, S.; Das, P.; Samanta, I.; Mukherjee, P.; Roy, S.; Kundu, B. Understanding osteomyelitis and its treatment through local drug delivery system. Biotechnol. Adv. 2016, 34, 1305–1317. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, M.; Monteiro, F.J.; Ferraz, M.P. Infection of orthopedic implants with emphasis on bacterial adhesion process and techniques used in studying bacterial-material interactions. Biomatter 2012, 2, 176–194. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Liu, Y.; Guo, J.; Wu, H.; Wang, J.; Wu, G. Biomaterials with abtibacterial and osteoinductive properties to repair infected bone defects. Int. J. Mol. Sci. 2016, 17. [Google Scholar] [CrossRef] [PubMed]
- Eltorai, A.E.; Haglin, J.; Perera, S.; Brea, B.A.; Ruttiman, R.; Garcia, D.R.; Born, C.T.; Daniels, A.H. Antimicrobial technology in orthopedic and spinal implants. World J. Orthop. 2016, 7, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, M.; Rzhepishevska, O.; Grenho, L.; Malheiros, D.; Gonçalves, L.; Almeida, A.J.; Jor dão, L.; Ribeiro, I.A.; Ramstedt, M.; Gomes, P.; et al. Levofloxacin-loaded bone cement delivery system: Highly effective against intracellular bacteria and Staphylococcus aureus biofilms. Int. J. Pharm. 2017, 532, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Zilberman, M. Antibiotic-eluting medical devices for various applications. J. Control. Release 2008, 130, 202–215. [Google Scholar] [CrossRef] [PubMed]
- Van de Belt, H.; Neut, D.; Schenk, W.; Van Horn, J.R.; Van der Mei, H.C.; Busscher, H.J. Infection of orthopedic implants and the use of antibiotic-loaded bone cements. Acta Orthop. Scand. 2001, 72, 557–571. [Google Scholar] [CrossRef] [PubMed]
- Senn, D.; Gehmert, S.; Ochsner, P.E.; Kuhn, K.-D.; Nowakowski, M. Therapy for chronic recurrent osteomyelitis with multi-resistant Pesudomonas aeruginosa using local antibiotic release by polymethylmethacrylate custom-made tibia nail. Surg. Infect. Case Rep. 2017, 2, 26–30. [Google Scholar] [CrossRef]
- Wentao, Z.; Lei, G.; Liu, Y.; Wang, W.; Song, T.; Fan, J. Approach to osteomyelitis treatment with antibiotic loaded PMMA. Microb. Pathog. 2017, 102, 42–44. [Google Scholar] [CrossRef] [PubMed]
- Letchmanan, K.; Shen, S.-C.; Ng, W.K.; Kingshuk, P.; Shi, Z.; Wang, W.; Tan, R.B. Mechanical propeties and antibiotic release characteristics of poly(methylmethacrylate)-based bone cement formulated with mesoporous silica nanoparticles. J. Mech. Behav. Biomed. Mater. 2017, 72, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Anagnostakos, K.; Meyer, C. Antibiotic elution from hip and knee acrylic bone cement spacers: A systematic review. Biomed. Res. Int. 2017. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.R.; Smith, B.T.; Tatara, A.M.; Molina, E.R.; Lee, E.J.; Piepergerdes, T.C.; Uhrig, B.A.; Guldberg, R.E.; Bennett, G.N.; Wenke, J.C.; et al. Effects of Local Antibiotic Delivery from Porous Space Maintainers on Infection Clearance and Induction of an Osteogenic Membrane in an Infected Bone Defect. Tissue Eng. Part A 2017, 23, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Xie, Z.; Cui, X.; Zhao, C.; Huang, W.; Wang, J.; Zhanga, C. Gentamicin-loaded Borate Bioactive Glass eradicates osteomyelitis due to Escherichia coli in a rabbit model. Antimicrob. Agents Chemother. 2013, 57, 3293–3298. [Google Scholar] [CrossRef] [PubMed]
- Pishbin, F.; Mouriño, V.; Flor, S.; Kreppel, S.; Salih, V.; Ryan, M.P.; Boccaccini, A.R. Electrophoretic Deposition of Gentamicin-Loaded Bioactive Glass/Chitosan Composite Coatings for Orthopaedic Implants. Appl. Mater. Interfaces 2014, 6, 8796–8806. [Google Scholar] [CrossRef] [PubMed]
- Knaepler, H. Local application of gentamicin-containing collagen implant in the prophylaxis and treatment of surgical site infection in orthopaedic surgery. Int. J. Surg. 2012, 10 (Suppl. S1), S15–S20. [Google Scholar] [CrossRef] [PubMed]
- Aviv, M.; Berdicevsky, I.; Zilberman, M. Gentamicin-loaded bioresorbable films for prevention of bacterial infections associated with orthopedic implants. J. Biomed. Mater. Res. A 2007, 83, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Van Vugt, T.A.; Geurts, J.; Arts, J.J. Clinical application of antimicrobial bone graft substiutes in ostemyelitis treatment: A systemic review of different bone graft substitutes available in clinical treatment of osteomyelitis. Biomed. Res. Int. 2016. [Google Scholar] [CrossRef] [PubMed]
- Dunne, N.; Buchanan, F.; Hill, J.; Newe, C.; Tunney, M.; Brady, A.; Walker, G. In vitro testing of chitosan in gentamicin-loaded bone cement No antimicrobial effect and reduced mechanical performance. Acta Orthop. 2006, 79, 851–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kluin, O.S.; Busscher, H.J.; Neut, D.; van der Mei, H.C. Poly(Trimethylene Carbonate) as a carrier for Rifampicin and Vancomycin to target therapy-recalcitrant Staphylococcal Biofilms. J. Orthop. Res. 2016, 34, 1828–1837. [Google Scholar] [CrossRef] [PubMed]
- Ter Boo, G.J.; Arens, D.; Metsemakers, W.J.; Zeiter, S.; Richards, R.G.; Grijpma, D.W.; Eglin, D.; Moriarty, T.F. Injectable gentamicin-loaded thermo-responsive hyaluronic acid derivative prevents infection in a rabbit model. Acta Biomater. 2016, 43, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Kong, M.; Cheng, X.G.; King, K.; Park, H.J. Antimicrobial properties of chitosan and mode of action: A state of the art. Int. J. Food Microbiol. 2010, 144, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Tai, C.-L.; Hsieh, P.-H.; Ueng, S.W.N. Gentamicin bone cement. Bone Jt. Res. 2013, 10, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Coraca-Huber, D.C.; Wurm, A.; Fille, M.; Hausdorfer, J.; Nogler, M.; Ku, K.-D. Effect of freezing on the release rate of gentamicin palmitate and gentamicin sulfate from bone tissue. J. Orthop. Res. 2014, 32, 842–847. [Google Scholar] [CrossRef] [PubMed]
- Dorati, R.; DeTrizio, A.; Genta, I.; Grisoli, P.; Merelli, A.; Tomasi, C.; Conti, B. An experimental approach to the preparation of pegylated polylactide-co-glycolide gentamicin loaded microparticles for local antibiotic delivery. Mater. Sci. Eng. C 2016, 58, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Dorati, R.; De Trizio, A.; Genta, I.; Merelli, A.; Modena, T.; Conti, B. Formulation and in vitro characterization of a composite biodegradable scaffold as antibiotic delivery system and regenerative device for bone. J. Drug Deliv. Sci. Tecnol. 2016, 35, 124–133. [Google Scholar] [CrossRef]
- Dorati, R.; DeTrizio, A.; Genta, I.; Merelli, A.; Modena, T.; Conti, B. Gentamicin-loaded thermosetting hydrogel and moldable composite scaffold: Formulation study and biological evaluation. J. Pharm. Sci. 2017, 106, 1596–1607. [Google Scholar] [CrossRef] [PubMed]
- De Trizio, A.; Srisuk, P.; Costa, R.; Fraga, A.; Modena, T.; Genta, I.; Dorati, R.; Pedrosa, J.; Conti, B.; Correlo, V.M.; Reis, R. Natural based eumelanin nanoparticles functionalization and preliminary evaluation as carrier for gentamicin. React. Funct. Polym. 2017, 114, 38–48. [Google Scholar] [CrossRef]
- Lecaroz, C.; Gamazo, C.; Blanco-Prieto, M.J. Nanocarriers with gentamicin to treat intracellular pathogens. J. Nanosci. Nanotechnol. 2006, 6, 3296–3302. [Google Scholar] [CrossRef] [PubMed]
- Long, Y.M.; Hu, L.G.; Yan, X.T.; Zhou, X.C.; Jiang, G.B. Surface ligan controls silver ion release of nanosilver anf its antibacterial activity afgainst Escherichia coli. Int. J. Nanomed. 2017, 12, 3193–3206. [Google Scholar] [CrossRef] [PubMed]
- Sadat, T. Improved drug loading and antibacterial activity of minocycline-loaded PLGA nanoparticles prepared by solid/oil/water ion pairing method. Int. J. Nanomed. 2012, 7, 221–234. [Google Scholar]
- Sans-Serramitjana, E.; Jorba, M.; Pedraz, J.L.; Vinues, T.; Viñas, M. Determination of the spatiotemporal dependence of Pseudomonas aeruginosa biofilm viability after treatment with NLC-colistin. Int. J. Nanomed. 2017, 12, 4409–4413. [Google Scholar] [CrossRef] [PubMed]



© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dorati, R.; DeTrizio, A.; Modena, T.; Conti, B.; Benazzo, F.; Gastaldi, G.; Genta, I. Biodegradable Scaffolds for Bone Regeneration Combined with Drug-Delivery Systems in Osteomyelitis Therapy. Pharmaceuticals 2017, 10, 96. https://doi.org/10.3390/ph10040096
Dorati R, DeTrizio A, Modena T, Conti B, Benazzo F, Gastaldi G, Genta I. Biodegradable Scaffolds for Bone Regeneration Combined with Drug-Delivery Systems in Osteomyelitis Therapy. Pharmaceuticals. 2017; 10(4):96. https://doi.org/10.3390/ph10040096
Chicago/Turabian StyleDorati, Rossella, Antonella DeTrizio, Tiziana Modena, Bice Conti, Francesco Benazzo, Giulia Gastaldi, and Ida Genta. 2017. "Biodegradable Scaffolds for Bone Regeneration Combined with Drug-Delivery Systems in Osteomyelitis Therapy" Pharmaceuticals 10, no. 4: 96. https://doi.org/10.3390/ph10040096
APA StyleDorati, R., DeTrizio, A., Modena, T., Conti, B., Benazzo, F., Gastaldi, G., & Genta, I. (2017). Biodegradable Scaffolds for Bone Regeneration Combined with Drug-Delivery Systems in Osteomyelitis Therapy. Pharmaceuticals, 10(4), 96. https://doi.org/10.3390/ph10040096