Nanotechnology for the Treatment of Allergic Conjunctival Diseases

Abstract
:1. Allergic Conjunctival Diseases
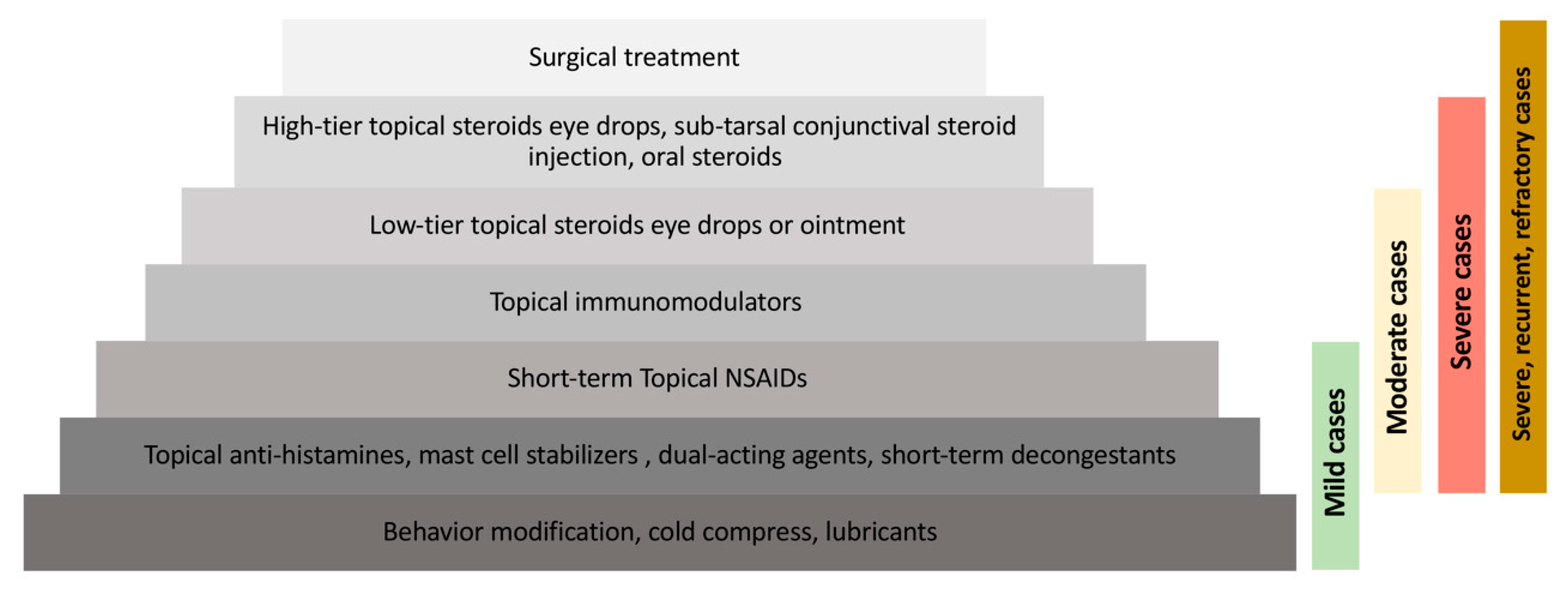
2. Treatment of Allergic Conjunctival Diseases
2.1. Supportive Treatment
2.2. Topical Anti-histamines
2.3. Topical Mast Cell Stabilizers
2.4. Topical Dual-Acting Agents
2.5. Topical Non-steroidal Anti-inflammatory Drugs
2.6. Corticosteroids
2.7. Topical Immunomodulators
2.8. Surgical Management
3. Introduction of Nanotechnology
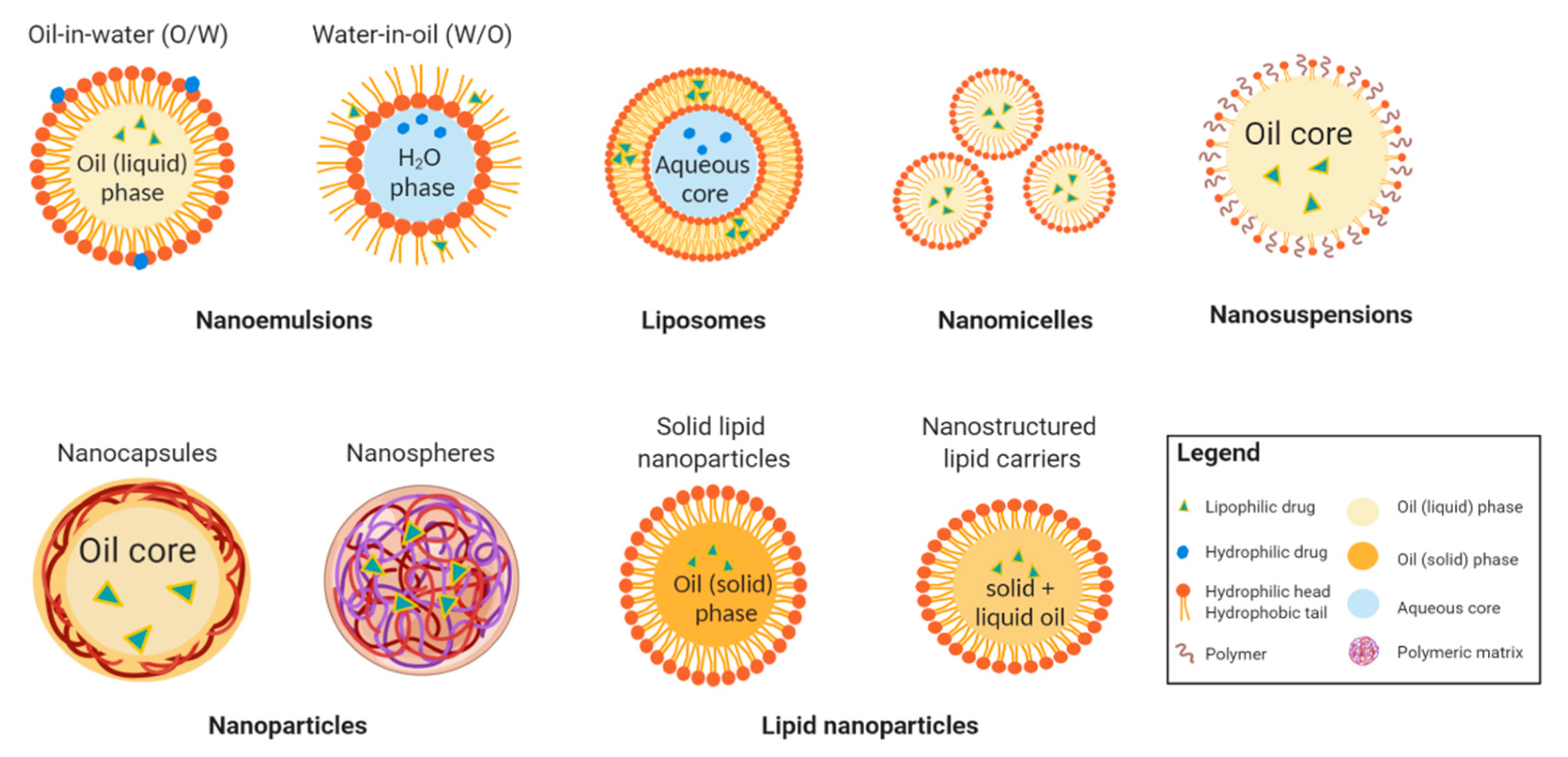
4. Nanotechnology-Based Drug Delivery Systems for Ocular Disorders
4.1. Nanoemulsions
4.2. Liposomes
4.3. Nanomicelles
4.4. Nanoparticles
4.5. Lipid Nanoparticles
4.6. Nanosuspensions
4.7. Advantages, Disadvantages and Challenges of Nanotechnology Based Drug Delivery Systems
5. Nanotechnology for the Treatment of Allergic Conjunctival Diseases
5.1. Immunomodulatory Agents
5.2. NSAIDs
5.3. Corticosteroids
6. Conclusions and Future Directions
Author Contributions
Funding
Conflicts of Interest
References
- Leonardi, A.; Castegnaro, A.; Valerio, A.L.; Lazzarini, D. Epidemiology of allergic conjunctivitis: Clinical appearance and treatment patterns in a population-based study. Curr. Opin. Allergy Clin. Immunol. 2015, 15, 482–488. [Google Scholar] [CrossRef]
- Miyazaki, D.; Fukagawa, K.; Okamoto, S.; Fukushima, A.; Uchio, E.; Ebihara, N.; Shoji, J.; Namba, K.; Shimizu, Y. Epidemiological aspects of allergic conjunctivitis. Allergol. Int. 2020. [Google Scholar] [CrossRef]
- Khan, R.S.; Rizvi, S.; Syed, B.A.; Bielory, L. Current market trends in anterior ocular inflammatory disease landscape. Curr. Opin. Allergy Clin. Immunol. 2019, 19, 503–509. [Google Scholar] [CrossRef]
- Bielory, L.; Schoenberg, D. Ocular allergy: Update on clinical trials. Curr. Opin. Allergy Clin. Immunol. 2019, 19, 495–502. [Google Scholar] [CrossRef]
- Yawata, N.; Selva, K.J.; Liu, Y.C.; Tan, K.P.; Lee, A.W.; Siak, J.; Lan, W.; Vania, M.; Arundhati, A.; Tong, L.; et al. Dynamic change in natural killer cell type in the human ocular mucosa in situ as means of immune evasion by adenovirus infection. Mucosal. Immunol. 2016, 9, 159–170. [Google Scholar] [CrossRef] [Green Version]
- Bielory, L.; Meltzer, E.O.; Nichols, K.K.; Melton, R.; Thomas, R.K.; Bartlett, J.D. An algorithm for the management of allergic conjunctivitis. Allergy Asthma Proc. 2013, 34, 408–420. [Google Scholar] [CrossRef]
- De Smedt, S.; Wildner, G.; Kestelyn, P. Vernal keratoconjunctivitis: An update. Br. J. Ophthalmol. 2013, 97, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Dupuis, P.; Prokopich, C.L.; Hynes, A.; Kim, H. A contemporary look at allergic conjunctivitis. Allergy Asthma Clin. Immunol. 2020, 16, 5. [Google Scholar] [CrossRef]
- Bielory, L.; Delgado, L.; Katelaris, C.H.; Leonardi, A.; Rosario, N.; Vichyanoud, P. ICON: Diagnosis and management of allergic conjunctivitis. Ann. Allergy Asthma Immunol. 2020, 124, 118–134. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Ophthalmology. External Disease and Cornea; American Academy of Ophthalmology: San Francisco, CA, USA, 2018; Volume 8, pp. 207–214. [Google Scholar]
- Ben-Eli, H.; Solomon, A. Topical antihistamines, mast cell stabilizers, and dual-action agents in ocular allergy: Current trends. Curr. Opin. Allergy Clin. Immunol. 2018, 18, 411–416. [Google Scholar] [CrossRef]
- Lim, R.R.; Tan, A.; Liu, Y.C.; Barathi, V.A.; Mohan, R.R.; Mehta, J.S.; Chaurasia, S.S. ITF2357 transactivates Id3 and regulate TGFbeta/BMP7 signaling pathways to attenuate corneal fibrosis. Sci. Rep. 2016, 6, 20841. [Google Scholar] [CrossRef] [Green Version]
- Addis, H.; Jeng, B.H. Vernal keratoconjunctivitis. Clin. Ophthalmol. 2018, 12, 119–123. [Google Scholar] [CrossRef] [Green Version]
- Carnahan, M.C.; Goldstein, D.A. Ocular complications of topical, peri-ocular, and systemic corticosteroids. Curr. Opin. Ophthalmol. 2000, 11, 478–483. [Google Scholar] [CrossRef]
- Liu, Y.C.; Wilkins, M.; Kim, T.; Malyugin, B.; Mehta, J.S. Cataracts. Lancet 2017, 390, 600–612. [Google Scholar] [CrossRef]
- Liu, Y.C.; Ng, X.W.; Teo, E.P.W.; Ang, H.P.; Lwin, N.C.; Chan, N.S.W.; Venkatraman, S.S.; Wong, T.T.; Mehta, J.S. A Biodegradable, Sustained-Released, Tacrolimus Microfilm Drug Delivery System for the Management of Allergic Conjunctivitis in a Mouse Model. Investig. Ophthalmol. Vis. Sci. 2018, 59, 675–684. [Google Scholar] [CrossRef]
- Miyazaki, D.; Tominaga, T.; Kakimaru-Hasegawa, A.; Nagata, Y.; Hasegawa, J.; Inoue, Y. Therapeutic effects of tacrolimus ointment for refractory ocular surface inflammatory diseases. Ophthalmology 2008, 115, 988–992.e5. [Google Scholar] [CrossRef]
- Zanjani, H.; Aminifard, M.N.; Ghafourian, A.; Pourazizi, M.; Maleki, A.; Arish, M.; Shahrakipoor, M.; Rohani, M.R.; Abrishami, M.; Khafri Zare, E.; et al. Comparative Evaluation of Tacrolimus Versus Interferon Alpha-2b Eye Drops in the Treatment of Vernal Keratoconjunctivitis: A Randomized, Double-Masked Study. Cornea 2017, 36, 675–678. [Google Scholar] [CrossRef]
- Shoughy, S.S. Topical tacrolimus in anterior segment inflammatory disorders. Eye Vis. 2017, 4, 7. [Google Scholar] [CrossRef] [Green Version]
- Erdinest, N.; Ben-Eli, H.; Solomon, A. Topical tacrolimus for allergic eye diseases. Curr. Opin. Allergy Clin. Immunol. 2019, 19, 535–543. [Google Scholar] [CrossRef]
- Siegl, C.; Konig-Schuster, M.; Nakowitsch, S.; Koller, C.; Graf, P.; Unger-Manhart, N.; Schindlegger, Y.; Kirchoff, N.; Knecht, C.; Prieschl-Grassauer, E.; et al. Pharmacokinetics of topically applied tacrolimus dissolved in Marinosolv, a novel aqueous eye drop formulation. Eur. J. Pharm. Biopharm. 2019, 134, 88–95. [Google Scholar] [CrossRef]
- Uno, T.; Yamaguchi, T.; Li, X.K.; Suzuki, Y.; Hashimoto, H.; Harada, Y.; Kimura, T.; Kazui, T. The pharmacokinetics of water-in-oil-in-water-type multiple emulsion of a new tacrolimus formulation. Lipids 1997, 32, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.C.; Peng, Y.; Lwin, N.C.; Venkatraman, S.S.; Wong, T.T.; Mehta, J.S. A biodegradable, sustained-released, prednisolone acetate microfilm drug delivery system effectively prolongs corneal allograft survival in the rat keratoplasty model. PLoS ONE 2013, 8, e70419. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.C.; Peng, Y.; Lwin, N.C.; Wong, T.T.; Venkatraman, S.S.; Mehta, J.S. Optimization of subconjunctival biodegradable microfilms for sustained drug delivery to the anterior segment in a small animal model. Investig. Ophthalmol. Vis. Sci. 2013, 54, 2607–2615. [Google Scholar] [CrossRef] [Green Version]
- Iyer, G.; Agarwal, S.; Srinivasan, B. Outcomes and Rationale of Excision and Mucous Membrane Grafting in Palpebral Vernal Keratoconjunctivitis. Cornea 2018, 37, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Rai, M.; Ingle, A.P.; Gaikwad, S.; Padovani, F.H.; Alves, M. The role of nanotechnology in control of human diseases: Perspectives in ocular surface diseases. Crit. Rev. Biotechnol. 2016, 36, 777–787. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, Z.; Tao, C.; Lin, X.; Zhang, M.; Zeng, L.; Chen, X.; Song, H. Cationic nanoemulsions with prolonged retention time as promising carriers for ophthalmic delivery of tacrolimus. Eur. J. Pharm. Sci. 2020, 144, 105229. [Google Scholar] [CrossRef]
- Salama, A.H.; Shamma, R.N. Tri/tetra-block co-polymeric nanocarriers as a potential ocular delivery system of lornoxicam: In-vitro characterization, and in-vivo estimation of corneal permeation. Int. J. Pharm. 2015, 492, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Kamaleddin, M.A. Nano-ophthalmology: Applications and considerations. Nanomed. Nanotechnol. Biol. Med. 2017, 13, 1459–1472. [Google Scholar] [CrossRef]
- Agarwal, R.; Iezhitsa, I.; Agarwal, P.; Nasir, N.A.A.; Razali, N.; Alyautdin, R.; Ismail, N.M. Liposomes in topical ophthalmic drug delivery: An update. Drug Deliv. 2016, 23, 1075–1091. [Google Scholar] [CrossRef]
- Chen, H.; Pan, H.; Li, P.; Wang, H.; Wang, X.; Pan, W.; Yuan, Y. The potential use of novel chitosan-coated deformable liposomes in an ocular drug delivery system. Colloids Surf. B Biointerfaces 2016, 143, 455–462. [Google Scholar] [CrossRef]
- Patra, J.K.; Das, G.; Fraceto, L.F.; Campos, E.V.R.; del Pilar Rodriguez-Torres, M.; Acosta-Torres, L.S.; Diaz-Torres, L.A.; Grillo, R.; Swamy, M.K.; Sharma, S. Nano based drug delivery systems: Recent developments and future prospects. J. Nanobiotechnol. 2018, 16, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omerović, N.; Vranić, E. Application of nanoparticles in ocular drug delivery systems. Health Technol. 2019, 10, 61–78. [Google Scholar] [CrossRef]
- Mansuri, S.; Kesharwani, P.; Jain, K.; Tekade, R.K.; Jain, N. Mucoadhesion: A promising approach in drug delivery system. React. Funct. Polym. 2016, 100, 151–172. [Google Scholar] [CrossRef]
- Liu, Y.C.; Ng, A.H.C.; Ng, X.W.; Yan, P.; Venkatraman, S.S.; Mehta, J.S.; Wong, T.T. Evaluation of a Sustained-Release Prednisolone Acetate Biodegradable Subconjunctival Implant in a Non-Human Primate Model. Transl. Vis. Sci. Technol. 2017, 6, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaib, S.; Iqbal, J. Nanotechnology: Applications, Techniques, Approaches, & the Advancement in Toxicology and Environmental Impact of Engineered Nanomaterials. 2019. Available online: https://meddocsonline.org/ebooks/ebook-nanotechnology/Importance-Application-of-Nanotechnology_GP_11_06_2019.pdf (accessed on 20 August 2020).
- Shen, Y.; Yu, Y.; Chaurasiya, B.; Li, X.; Xu, Y.; Webster, T.J.; Tu, J.; Sun, R. Stability, safety, and transcorneal mechanistic studies of ophthalmic lyophilized cyclosporine-loaded polymeric micelles. Int. J. Nanomed. 2018, 13, 8281. [Google Scholar] [CrossRef] [Green Version]
- Ludwig, J.V.A. Ocular drug delivery_nanomedicine applications. Future Med. 2007, 2, 11–21. [Google Scholar]
- Shen, H.H.; Chan, E.C.; Lee, J.H.; Bee, Y.S.; Lin, T.W.; Dusting, G.J.; Liu, G.S. Nanocarriers for treatment of ocular neovascularization in the back of the eye: New vehicles for ophthalmic drug delivery. Nanomedicine 2015, 10, 2093–2107. [Google Scholar] [CrossRef] [Green Version]
- Connor, E.E.; Mwamuka, J.; Gole, A.; Murphy, C.J.; Wyatt, M.D. Gold nanoparticles are taken up by human cells but do not cause acute cytotoxicity. Small 2005, 1, 325–327. [Google Scholar] [CrossRef]
- Ahamed, M. Silica nanoparticles-induced cytotoxicity, oxidative stress and apoptosis in cultured A431 and A549 cells. Hum. Exp. Toxicol. 2013, 32, 186–195. [Google Scholar] [CrossRef]
- Leonardi, A.; Doan, S.; Amrane, M.; Ismail, D.; Montero, J.; Németh, J.; Aragona, P.; Bremond-Gignac, D.; Group, V.S. A randomized, controlled trial of cyclosporine A cationic emulsion in pediatric vernal keratoconjunctivitis: The VEKTIS study. Ophthalmology 2019, 126, 671–681. [Google Scholar] [CrossRef] [Green Version]
- Araújo, J.; Gonzalez, E.; Egea, M.A.; Garcia, M.L.; Souto, E.B. Nanomedicines for ocular NSAIDs: Safety on drug delivery. Nanomed. Nanotechnol. Biol. Med. 2009, 5, 394–401. [Google Scholar] [CrossRef]
- Sahoo, S.K.; Dilnawaz, F.; Krishnakumar, S. Nanotechnology in ocular drug delivery. Drug Discov. Today 2008, 13, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Garrigue, J.-S.; Amrane, M.; Faure, M.-O.; Holopainen, J.M.; Tong, L. Relevance of lipid-based products in the management of dry eye disease. J. Ocular Pharmacol. Ther. 2017, 33, 647–661. [Google Scholar] [CrossRef] [PubMed]
- Seyfoddin, A.; Shaw, J.; Al-Kassas, R. Solid lipid nanoparticles for ocular drug delivery. Drug Deliv. 2010, 17, 467–489. [Google Scholar] [CrossRef]
- Bangham, A.; Standish, M.M.; Watkins, J.C. Diffusion of univalent ions across the lamellae of swollen phospholipids. J. Mol. Biol. 1965, 13, 238. [Google Scholar] [CrossRef]
- Battaglia, L.; Serpe, L.; Foglietta, F.; Muntoni, E.; Gallarate, M.; Del Pozo, R.A.; Solinis, M.A. Application of lipid nanoparticles to ocular drug delivery. Expert Opin. Drug Deliv. 2016, 13, 1743–1757. [Google Scholar] [CrossRef] [PubMed]
- Kaur, I.P.; Garg, A.; Singla, A.K.; Aggarwal, D. Vesicular systems in ocular drug delivery: An overview. Int. J. Pharm. 2004, 269, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Kutlehria, S.; Vhora, I.; Bagde, A.; Chowdhury, N.; Behl, G.; Patel, K.; Singh, M. Tacrolimus loaded PEG-cholecalciferol based micelles for treatment of ocular inflammation. Pharm. Res. 2018, 35, 117. [Google Scholar] [CrossRef]
- Cholkar, K.; Patel, A.; Vadlapudi, A.D.; Mitra, A.K. Novel nanomicellar formulation approaches for anterior and posterior segment ocular drug delivery. Recent Pat. Nanomed. 2012, 2, 82–95. [Google Scholar] [CrossRef]
- Weng, Y.; Liu, J.; Jin, S.; Guo, W.; Liang, X.; Hu, Z. Nanotechnology-based strategies for treatment of ocular disease. Acta Pharm. Sin. B 2017, 7, 281–291. [Google Scholar] [CrossRef] [Green Version]
- Civiale, C.; Licciardi, M.; Cavallaro, G.; Giammona, G.; Mazzone, M. Polyhydroxyethylaspartamide-based micelles for ocular drug delivery. Int. J. Pharm. 2009, 378, 177–186. [Google Scholar] [CrossRef]
- Paolicelli, P.; Prego, C.; Sanchez, A.; Alonso, M.J. Surface-modified PLGA-based nanoparticles that can efficiently associate and deliver virus-like particles. Nanomedicine 2010, 5, 843–853. [Google Scholar] [CrossRef] [PubMed]
- Kondiah, P.P.; Choonara, Y.E.; Kondiah, P.J.; Marimuthu, T.; Kumar, P.; du Toit, L.C.; Modi, G.; Pillay, V. Nanocomposites for therapeutic application in multiple sclerosis. In Applications of Nanocomposite Materials in Drug Delivery; Elsevier: Amsterdam, The Netherlands, 2018; pp. 391–408. [Google Scholar]
- Sánchez-López, E.; Esteruelas, G.; Ortiz, A.; Espina, M.; Prat, J.; Muñoz, M.; Cano, A.; Calpena, A.C.; Ettcheto, M.; Camins, A. Dexibuprofen Biodegradable Nanoparticles: One Step Closer towards a Better Ocular Interaction Study. Nanomaterials 2020, 10, 720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almeida, H.; Amaral, M.H.; Lobão, P.; Silva, A.C.; Loboa, J.M.S. Applications of polymeric and lipid nanoparticles in ophthalmic pharmaceutical formulations: Present and future considerations. J. Pharm. Pharm. Sci. 2014, 17, 278–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehnert, W.; Mäder, K. Solid lipid nanoparticles: Production, characterization and applications. Adv. Drug Deliv. Rev. 2012, 64, 83–101. [Google Scholar] [CrossRef]
- Gaudana, R.; Jwala, J.; Boddu, S.H.; Mitra, A.K. Recent perspectives in ocular drug delivery. Pharm. Res. 2009, 26, 1197. [Google Scholar] [CrossRef] [Green Version]
- Sawant, K.K.; Dodiya, S.S. Recent advances and patents on solid lipid nanoparticles. Rec. Pat. Drug Deliv. Formul. 2008, 2, 120–135. [Google Scholar] [CrossRef]
- Müller, R.; Radtke, M.; Wissing, S. Nanostructured lipid matrices for improved microencapsulation of drugs. Int. J. Pharm. 2002, 242, 121–128. [Google Scholar] [CrossRef]
- Balguri, S.P.; Adelli, G.R.; Majumdar, S. Topical ophthalmic lipid nanoparticle formulations (SLN, NLC) of indomethacin for delivery to the posterior segment ocular tissues. Eur. J. Pharm. Biopharm. 2016, 109, 224–235. [Google Scholar] [CrossRef] [Green Version]
- Thattil, J.G.; Kumar, K.K.; Kumar, B.D. Nanosuspension Technology in Pharmaceuticals. J. Bio. Innov. 2018, 7, 660–667. [Google Scholar]
- Jacob, S.; Nair, A.B.; Shah, J. Emerging role of nanosuspensions in drug delivery systems. Biomater. Res. 2020, 24, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassem, M.; Rahman, A.A.; Ghorab, M.; Ahmed, M.; Khalil, R. Nanosuspension as an ophthalmic delivery system for certain glucocorticoid drugs. Int. J. Pharm. 2007, 340, 126–133. [Google Scholar] [CrossRef]
- Gupta, H.; Aqil, M.; Khar, R.K.; Ali, A.; Bhatnagar, A.; Mittal, G. Sparfloxacin-loaded PLGA nanoparticles for sustained ocular drug delivery. Nanomed. Nanotechnol. Biol. Med. 2010, 6, 324–333. [Google Scholar] [CrossRef]
- Garg, V.; Suri, R.; Jain, G.K.; Kohli, K. Proglycosomes: A novel nano-vesicle for ocular delivery of tacrolimus. Colloids Surf. B Biointerfaces 2017, 157, 40–47. [Google Scholar] [CrossRef]
- Garg, V.; Jain, G.K.; Nirmal, J.; Kohli, K. Topical tacrolimus nanoemulsion, a promising therapeutic approach for uveitis. Med. Hypotheses 2013, 81, 901–904. [Google Scholar] [CrossRef] [PubMed]
- Suresh, P.K.; Sah, A.K. Nanocarriers for ocular delivery for possible benefits in the treatment of anterior uveitis: Focus on current paradigms and future directions. Expert Opin. Drug Deliv. 2014, 11, 1747–1768. [Google Scholar] [CrossRef] [PubMed]
- Ako-Adounvo, A.-M.; Nagarwal, R.C.; Oliveira, L.; Boddu, S.H.S.; Wang, X.S.; Dey, S.; Karla, P.K. Recent patents on ophthalmic nanoformulations and therapeutic implications. Recent Pat. Drug Deliv. Formul. 2014, 8, 193–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, N. Challenges in development of nanoparticle-based therapeutics. AAPS J. 2012, 14, 282–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hua, S.; de Matos, M.B.C.; Metselaar, J.M.; Storm, G. Current Trends and Challenges in the Clinical Translation of Nanoparticulate Nanomedicines: Pathways for Translational Development and Commercialization. Front. Pharmacol. 2018, 9, 790. [Google Scholar] [CrossRef]
- Chen, H.; Jin, Y.; Sun, L.; Li, X.; Nan, K.; Liu, H.; Zheng, Q.; Wang, B. Recent developments in ophthalmic drug delivery systems for therapy of both anterior and posterior segment diseases. Colloid Interface Sci. Commun. 2018, 24, 54–61. [Google Scholar] [CrossRef]
- Li, X.; Li, L.; Zhang, Z.; Chen, H. An overview on pharmacokinetics, disposition, and safety of nanoparticles in ocular applications. Curr. Drug Metab. 2013, 14, 857–862. [Google Scholar] [CrossRef]
- Lallemand, F.; Daull, P.; Benita, S.; Buggage, R.; Garrigue, J.S. Successfully improving ocular drug delivery using the cationic nanoemulsion, novasorb. J. Drug Deliv. 2012, 2012, 604204. [Google Scholar] [CrossRef] [PubMed]
- Maroon, J.C.; Bost, J.W. Omega-3 fatty acids (fish oil) as an anti-inflammatory: An alternative to nonsteroidal anti-inflammatory drugs for discogenic pain. Surg. Neurol. 2006, 65, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Kalam, M.A.; Alshamsan, A. Poly (d, l-lactide-co-glycolide) nanoparticles for sustained release of tacrolimus in rabbit eyes. Biomed. Pharmacother. 2017, 94, 402–411. [Google Scholar] [CrossRef]
- Vasconcelos, A.; Vega, E.; Perez, Y.; Gomara, M.J.; Garcia, M.L.; Haro, I. Conjugation of cell-penetrating peptides with poly(lactic-co-glycolic acid)-polyethylene glycol nanoparticles improves ocular drug delivery. Int. J. Nanomed. 2015, 10, 609–631. [Google Scholar] [CrossRef] [Green Version]
- Gokce, E.H.; Sandri, G.; Bonferoni, M.C.; Rossi, S.; Ferrari, F.; Güneri, T.; Caramella, C. Cyclosporine A loaded SLNs: Evaluation of cellular uptake and corneal cytotoxicity. Int. J. Pharm. 2008, 364, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Vega, E.; Egea, M.A.; Valls, O.; Espina, M.; Garcia, M.L. Flurbiprofen loaded biodegradable nanoparticles for ophtalmic administration. J. Pharm. Sci. 2006, 95, 2393–2405. [Google Scholar] [CrossRef] [PubMed]
- Badawi, A.A.; El-Laithy, H.M.; El Qidra, R.K.; El Mofty, H.; El Dally, M. Chitosan based nanocarriers for indomethacin ocular delivery. Arch. Pharm. Res. 2008, 31, 1040–1049. [Google Scholar] [CrossRef]
- Attama, A.A.; Reichl, S.; Müller-Goymann, C.C. Diclofenac sodium delivery to the eye: In vitro evaluation of novel solid lipid nanoparticle formulation using human cornea construct. Int. J. Pharm. 2008, 355, 307–313. [Google Scholar] [CrossRef]
- Wissing, S.A.; Kayser, O.; Muller, R.H. Solid lipid nanoparticles for parenteral drug delivery. Adv. Drug Deliv. Rev. 2004, 56, 1257–1272. [Google Scholar] [CrossRef]
- Li, X.; Nie, S.F.; Kong, J.; Li, N.; Ju, C.Y.; Pan, W.S. A controlled-release ocular delivery system for ibuprofen based on nanostructured lipid carriers. Int. J. Pharm. 2008, 363, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Mira, E.; Egea, M.A.; Garcia, M.L.; Souto, E.B. Design and ocular tolerance of flurbiprofen loaded ultrasound-engineered NLC. Colloids Surf. B Biointerfaces 2010, 81, 412–421. [Google Scholar] [CrossRef] [PubMed]
- Gai, X.; Cheng, L.; Li, T.; Liu, D.; Wang, Y.; Wang, T.; Pan, W.; Yang, X. In vitro and in vivo studies on a novel bioadhesive colloidal system: Cationic liposomes of ibuprofen. Aaps Pharmscitech 2018, 19, 700–709. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Gan, L.; Zhu, C.; Zhang, X.; Dong, Y.; Jiang, M.; Zhu, J.; Gan, Y. Novel NSAIDs ophthalmic formulation: Flurbiprofen axetil emulsion with low irritancy and improved anti-inflammation effect. Int. J. Pharm. 2011, 412, 115–122. [Google Scholar] [CrossRef]
- Wong, C.W.; Czarny, B.; Metselaar, J.M.; Ho, C.; Ng, S.R.; Barathi, A.V.; Storm, G.; Wong, T.T. Evaluation of subconjunctival liposomal steroids for the treatment of experimental uveitis. Sci. Rep. 2018, 8, 6604. [Google Scholar] [CrossRef]
- Guo, D.; Li, Q.; Sun, Y.; Guo, J.; Zhao, Q.; Yin, X.; Wei, H.; Wu, S.; Bi, H. Evaluation of controlled-release triamcinolone acetonide-loaded mPEG-PLGA nanoparticles in treating experimental autoimmune uveitis. Nanotechnology 2019, 30, 165702. [Google Scholar] [CrossRef]
- Wen, Y.; Ban, J.; Mo, Z.; Zhang, Y.; An, P.; Liu, L.; Xie, Q.; Du, Y.; Xie, B.; Zhan, X.; et al. A potential nanoparticle-loaded in situ gel for enhanced and sustained ophthalmic delivery of dexamethasone. Nanotechnology 2018, 29, 425101. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | History | Clinical Presentations |
|---|---|---|
| SAC/PAC |
|
|
| VKC |
|
|
| AKC |
|
|
| Advantages |
| Sustained release in a controlled manner |
| Improve bioavailability, solubility and penetration of lipophilic molecules into different layers of the eye |
| Options to employ low-cost, biocompatible, and biodegradable biopolymers in drug encapsulation |
| Flexibility of modifying nanotechnology-based dosage form (i.e., surface charge, types and ratio of surfactants, polymer properties) to allow better drug permeation and corneal retention time |
| Choices to tailor nano-formulations based on the solubility of the drugs to achieve optimal therapeutic effects |
| Nano-formulation can control drug activity by releasing only at the desirable ocular site with prolonged therapeutic effects to reduce frequent doses, improving patient compliance |
| Encapsulation technique reduces drug-associated ocular irritation and toxicity at higher drug concentration |
| Great drug efficacy in improving different ocular therapeutics |
| Disadvantages |
| Nanoparticles can be antigenic that may lead to toxicities and side effects due to its properties (i.e., size, surface characteristics, charge, and hydrophobicity) |
| Lack of standardized protocol for the in vivo tolerance test |
| The immunotoxicity in animal models may be unable to accurately predict the safety of nanomedicines in human |
| The presence of surfactants in some cases could cause sticky feel and blurred vision of the eye upon instillation, impeding patient compliance |
| Different toxicity profile when employing different excipients and polymers |
| Difficult to produce in large scale in some nano-formulations and hard to control homogenous particle sizes in nanoparticle dosage formulations |
| Storage instability (e.g., particle aggregation, active agent expulsion) could lead to possible systemic toxicity |
| Not all nano-formulations can undergo aseptic productions via autoclaving, which pose concerns in its clinical applications |
| Absence of standards in regulatory approval examinations due to unique nano-formulations |
| Biomaterials with longer persistence in particular tissues require stringent evaluation from regulatory agency |
| Experimental Models | Drug | Findings |
|---|---|---|
| Excised rabbit corneas [77] | Tacrolimus loaded PLGA nanoparticles (PLGA-NPs) via topical eye drops |
|
| Ex-vivo goat eyes for transcorneal permeation study; Rabbits for precorneal retention study [67] | Proglycosomes modified liposomal tacrolimus topical eye drops |
|
| Rabbit corneal epithelial cells for in-vitro study Rabbit corneas for ex-vivo study [79] | Cyclosporin (CsA)-loaded solid lipid nanoparticles |
|
| Phase III, multicenter, randomized, double-masked, vehicle-controlled trial [42] | CsA cationic nanoemulsion eye drops |
|
| In-vitro study in human corneal epithelial cells; in vivo study in rabbits [37] | CsA-loaded mPEG-PLA nanomicelles via topical instillation |
|
| Drugs | Experimental Models | Administration | Findings |
|---|---|---|---|
| Dexibuprofen | In-vitro and in-vivo ocular irritation assay on chorioallantoic membrane and in rabbits, respectively. Ex-vivo ocular permeation study in rabbits [56] | Polymeric PLGA nanoparticles (NPs) topical eye drops |
|
| Diclofenac sodium | Bio-engineered human cornea construct [82] | Solid lipid nanoparticles (SLNs) |
|
| Ibuprofen | Excised rabbit corneas for in-vitro drug release; rabbits for ocular irritation [84] | Nanostructured lipid carriers (NLCs) topical eye drops |
|
| Excised rabbit cornea for in-vitro drug release; rabbits for pharmacokinetics study [86] | Ibuprofen-loaded cationic liposomal eye drops |
| |
| Flurbiprofen | Rabbit ocular surface inflammation model [80] | PLGA-NPs via topical eye drops |
|
| In-vitro corneal penetration test in isolated rabbit corneas; In-vivo ocular irritation and pre-corneal retention studies in rabbits [31] | Topical chitosan-coated liposomal formulation |
| |
| In-vitro ocular irritation test; In-vivo experiments in rabbits [85] | Ultrasound-engineered NLCs via single instillation |
| |
| Flurbiprofen axetil | Rabbit endotoxin-induced uveitis models [87] | Topical nanoemulsions eye drops |
|
| Indomethacin | Alkaline-burned rabbits [81] | Chitosan-coated nanoemulsion eye drops |
|
| Lornoxicam | In-vivo ocular irritation test in rabbits [28] | Polymeric nanomicelles eye drops |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.-C.; Lin, M.T.-Y.; Ng, A.H.C.; Wong, T.T.; Mehta, J.S. Nanotechnology for the Treatment of Allergic Conjunctival Diseases. Pharmaceuticals 2020, 13, 351. https://doi.org/10.3390/ph13110351
Liu Y-C, Lin MT-Y, Ng AHC, Wong TT, Mehta JS. Nanotechnology for the Treatment of Allergic Conjunctival Diseases. Pharmaceuticals. 2020; 13(11):351. https://doi.org/10.3390/ph13110351
Chicago/Turabian StyleLiu, Yu-Chi, Molly Tzu-Yu Lin, Anthony Herr Cheun Ng, Tina T. Wong, and Jodhbir S. Mehta. 2020. "Nanotechnology for the Treatment of Allergic Conjunctival Diseases" Pharmaceuticals 13, no. 11: 351. https://doi.org/10.3390/ph13110351
APA StyleLiu, Y. -C., Lin, M. T. -Y., Ng, A. H. C., Wong, T. T., & Mehta, J. S. (2020). Nanotechnology for the Treatment of Allergic Conjunctival Diseases. Pharmaceuticals, 13(11), 351. https://doi.org/10.3390/ph13110351