VEGF-Related Germinal Polymorphisms May Identify a Subgroup of Breast Cancer Patients with Favorable Outcome under Bevacizumab-Based Therapy—A Message from COMET, a French Unicancer Multicentric Study

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Study Population and Clinical Characteristics of Tumors
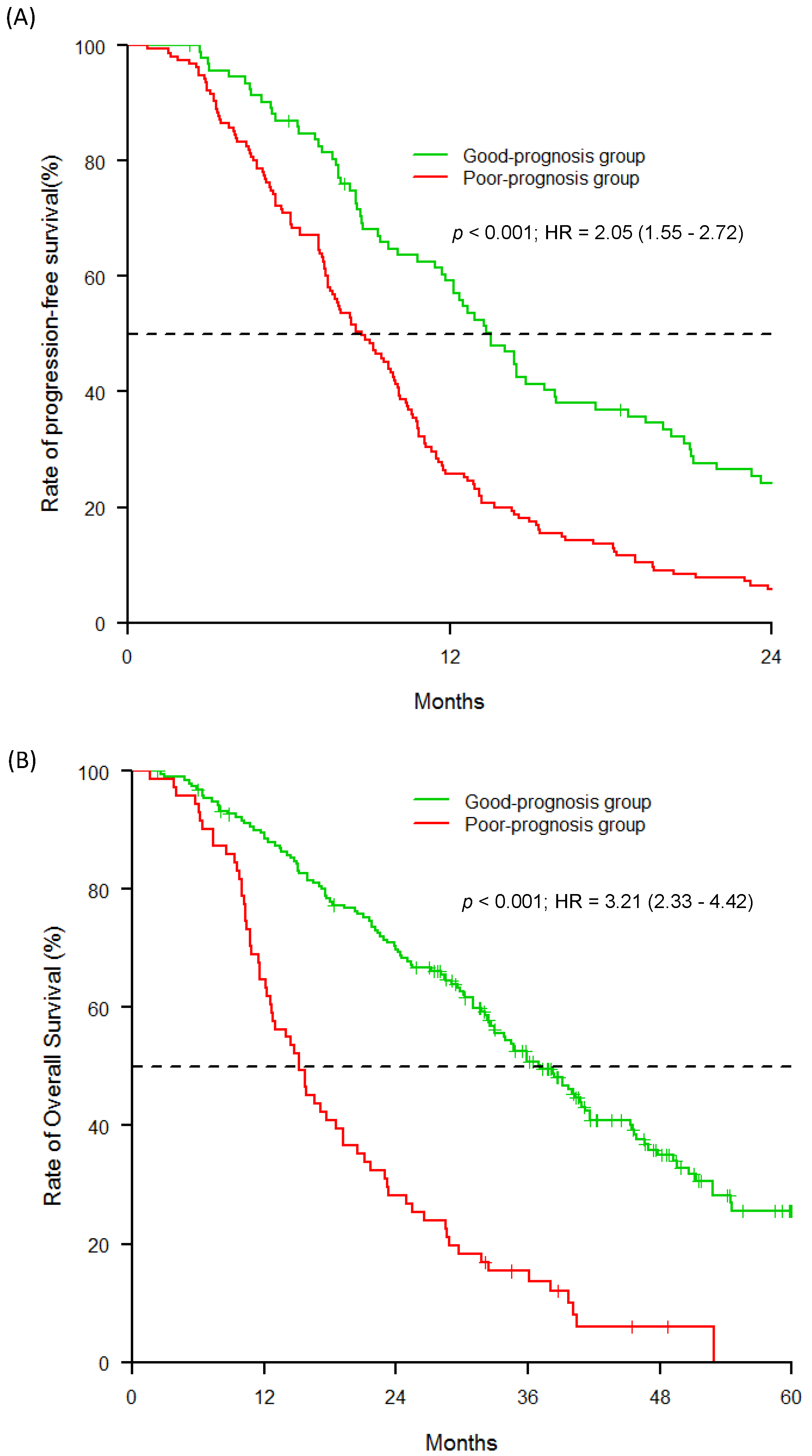
2.2. Association between Progression-Free Survival and Clinico-Pathological Features and SNPs
2.3. Associations among Overall Survival, SNPs and Patient Characteristics
3. Discussion
4. Materials and Methods
4.1. Study Design and Patients
4.2. SNP Selection and Genotyping
4.3. In Silico Analysis
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Conduct or Research
References
- Apte, R.S.; Chen, D.S.; Ferrara, N. VEGF in Signaling and Disease: Beyond Discovery and Development. Cell 2019, 176, 1248–1264. [Google Scholar] [PubMed] [Green Version]
- Garcia, J.; Hurwitz, H.I.; Sandler, A.B.; Miles, D.; Coleman, R.L.; Deurloo, R.; Chinot, O.L. Bevacizumab (Avastin®) in cancer treatment: A review of 15 years of clinical experience and future outlook. Cancer Treat. Rev. 2020, 86, 102017. [Google Scholar] [PubMed]
- Gerriets, V.; Kasi, A. Bevacizumab; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Pinter, M.; Scheiner, B.; Peck-Radosavljevic, M. Immunotherapy for advanced hepatocellular carcinoma: A focus on special subgroups. Gut 2020. [Google Scholar] [CrossRef]
- Lim, Y.W.; Chen-Harris, H.; Mayba, O.; Lianoglou, S.; Wuster, A.; Bhangale, T.; Khan, Z.; Mariathasan, S.; Daemen, A.; Reeder, J.; et al. Germline genetic polymorphisms influence tumor gene expression and immune cell infiltration. Proc. Natl. Acad. Sci. USA 2018, 115, E11701–E11710. [Google Scholar]
- Hanna, D.L.; Lenz, H.-J. Novel therapeutics in metastatic colorectal cancer: Molecular insights and pharmacogenomic implications. Expert Rev. Clin. Pharmacol. 2016, 9, 1091–1108. [Google Scholar] [PubMed]
- Hertz, D.L.; Rae, J. Pharmacogenetics of Cancer Drugs. Annu. Rev. Med. 2015, 66, 65–81. [Google Scholar] [PubMed]
- Daily, E.B.; Aquilante, C.L. Cytochrome P450 2C8 pharmacogenetics: A review of clinical studies. Pharmacogenomics 2009, 10, 1489–1510. [Google Scholar] [PubMed] [Green Version]
- Hamidovic, A.; Hahn, K.; Kolesar, J. Clinical significance of ABCB1 genotyping in oncology. J. Oncol. Pharm. Pr. 2010, 16, 39–44. [Google Scholar]
- Etienne-Grimaldi, M.; Formento, P.; Degeorges, A.; Pierga, J.-Y.; Delva, R.; Pivot, X.; Dalenc, F.; Espié, M.; Veyret, C.; Formento, J.-L.; et al. Prospective analysis of the impact of VEGF-A gene polymorphisms on the pharmacodynamics of bevacizumab-based therapy in metastatic breast cancer patients. Br. J. Clin. Pharmacol. 2011, 71, 921–928. [Google Scholar] [PubMed] [Green Version]
- Schneider, B.P.; Wang, M.; Radovich, M.; Sledge, G.W.; Badve, S.; Thor, A.; Flockhart, D.A.; Hancock, B.; Davidson, N.; Gralow, J.; et al. Association of Vascular Endothelial Growth Factor and Vascular Endothelial Growth Factor Receptor-2 Genetic Polymorphisms With Outcome in a Trial of Paclitaxel Compared With Paclitaxel Plus Bevacizumab in Advanced Breast Cancer: ECOG 2100. J. Clin. Oncol. 2008, 26, 4672–4678. [Google Scholar] [PubMed]
- Haunschild, C.; Tewari, K.S. Bevacizumab use in the frontline, maintenance and recurrent settings for ovarian cancer. Futur. Oncol. 2020, 16, 225–246. [Google Scholar]
- Cui, W.; Li, F.; Yuan, Q.; Chen, G.; Chen, C.; Yu, B. Role of VEGFA gene polymorphisms in colorectal cancer patients who treated with bevacizumab. Oncotarget 2017, 8, 105472–105478. [Google Scholar] [PubMed] [Green Version]
- Papachristos, A.; Kemos, P.; Katsila, T.; Panoilia, E.; Patrinos, G.P.; Kalofonos, H.P.; Sivolapenko, G.B. VEGF-A and ICAM-1 Gene Polymorphisms as Predictors of Clinical Outcome to First-Line Bevacizumab-Based Treatment in Metastatic Colorectal Cancer. Int. J. Mol. Sci. 2019, 20, 5791. [Google Scholar]
- Motz, G.T.; Coukos, G. The parallel lives of angiogenesis and immunosuppression: Cancer and other tales. Nat. Rev. Immunol. 2011, 11, 702–711. [Google Scholar]
- Gabriel, S.; Ziaugra, L.; Tabbaa, D. SNP Genotyping Using the Sequenom MassARRAY iPLEX Platform. Curr. Protoc. Hum. Genet. 2009, 60, 2.12.1–2.12.18. [Google Scholar]
- Mangin, B.; Siberchicot, A.; Nicolas, S.; Doligez, A.; This, P.; Cierco-Ayrolles, C. Novel measures of linkage disequilibrium that correct the bias due to population structure and relatedness. Heredity 2012, 108, 285–291. [Google Scholar]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar]
- Grambsch, P.M.; Therneau, T.M. Proportional Hazards Tests and Diagnostics Based on Weighted Residuals. Biometrika 1994, 81, 515–526. [Google Scholar]
- Dardis, C.; Dardis, M.C. Package ‘survMisc’. Available online: https://CRAN.R-project.org/package=survMisc (accessed on 1 October 2020).
- Blanche, P. TimeROC: Time-Dependent ROC Curve Estimation. Available online: https://CRAN.R-project.org/package=timeROC (accessed on 1 October 2020).
- Kassambara, A.; Kosinski, M.; Biecek, P.; Fabian, S. Package ‘Survminer’. Drawing Survival Curves Using ‘ggplot2’. R Package Version 0.3.1. Available online: https://CRAN.R-project.org/package=survminer (accessed on 1 October 2020).
- Desrousseaux, D.; Sandron, F.; Siberchicot, A.; Cierco-Ayrolles, C.; Mangin, B. LDcorSV: Linkage Disequilibrium Corrected by the Structure and the Relatedness. R Package Version 1.3.1. Available online: https://CRAN.R-project.org/package=LDcorSV (accessed on 1 October 2020).




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number of Patients (N = 306) | % |
|---|---|---|
| Mean age (min–max) at inclusion | 55.528–80 | |
| Histology | ||
| Invasive ductal carcinoma | 237 | 79.5 |
| Invasive lobular carcinoma | 38 | 12.5 |
| Mixed (ductal and lobular) | 10 | 3.5 |
| Other | 13 | 4.5 |
| Menopausal status at inclusion | ||
| Premenopausal | 88 | 29 |
| Postmenopausal | 213 | 71 |
| Unknown | 5 | |
| Performance status at inclusion | ||
| 0 | 172 | 56 |
| 1/2 | 134 | 43 |
| Histological grade | ||
| I | 23 | |
| II | 135 | 8 |
| III | 121 | 48.5 |
| Unknown | 27 | 43.5 |
| Subtype | ||
| Triple-negative | 64 | |
| Hormonal receptor-positive | 206 | 23.5 |
| Unknown | 36 | 76.5 |
| Tumor stage at initial diagnosis | ||
| pT0/pT1 | 109 | |
| pT2 | 84 | 46.5 |
| pT3/pT4 | 41 | 36 |
| Unknown | 72 | 17.5 |
| Axillary lymph node status at initial diagnosis | ||
| pN0 | 83 | |
| pN+ | 153 | 35 |
| Unknown | 68 | 65 |
| Prior (neo)adjuvant chemotherapy | ||
| Yes | 210 | 68 |
| No | 96 | 32 |
| Number of metastatic sites | ||
| <3 | 211 | |
| ≥3 | 24 | 90 |
| Unknown | 71 | 10 |
| Metastasis-free interval | ||
| 0 months | 17 | 7 |
| 0–24 months | 71 | 30.5 |
| 24 months | 147 | 62.5 |
| Unknown | 71 | |
| Metastatic sites | ||
| Liver | 97 | 41 |
| Distant node | 60 | 25.5 |
| Bone | 37 | 15.5 |
| Skin | 13 | 5.5 |
| Lung | 19 | 8.0 |
| Other 1 | 9 | 4.5 |
| Unknown | 71 |
| Progression-Free Survival | Overall Survival | ||||
| Significant Gene Polymorphisms | HR 95% CI | p-Value | HR 95% CI | p-Value | |
| VEGFA | rs699947 | ||||
| C/C or A/C | 1 | Referent | 1 | - | |
| A/A | 1.3 (1–1.8) | 0.042 | 1.5 (1.1–2.1) | 0.007 | |
| rs833061 | |||||
| T/T or T/C | 1 | Referent | 1 | - | |
| C/C | 1.4 (1–1.8) | 0.028 | 1.6 (1.1–2.1) | 0.005 | |
| rs2010963 | |||||
| G/G | 1 | Referent | - | - | |
| G/C or C/C | 0.77 (0.6–0.97) | 0.026 | - | - | |
| VEGFR1 | rs9582036 | ||||
| A/A | 1 | Referent | 1 | - | |
| C/A or C/C | 1.4 (1.1–1.7) | 0.010 | 1.4 (1.1–1.9) | 0.010 | |
| VEGFR2 | rs1870377 | ||||
| T/A or A/A | - | - | 1 | - | |
| T/T | - | - | 1.4 (1–1.8) | 0.021 | |
| Significant Clinical Characteristics | HR 95% CI | p-Value | HR 95% CI | p-Value | |
| Histological grade | |||||
| Grade I or II | 1 | Referent | 1 | - | |
| Grade III | 1.6 (1.2–2) | <0.001 | 1.4 (1.1–1.9) | 0.011 | |
| Subtype | |||||
| Hormonal receptor-positive | 1 | Referent | 1 | - | |
| Triple-negative | 1.9 (1.4–2.5) | <0.001 | 2.4 (1.7–3.3) | <0.001 | |
| Significant Gene Polymorphisms | Progression-Free Survival | ||||||
|---|---|---|---|---|---|---|---|
| Model A: Genetic | Model B: Clinico-Pathological | Model C: Combined | |||||
| HR [95% CI] | p-Value | HR [95% CI] | p-Value | HR [95% CI] | p-Value | ||
| VEGFA | rs833061 | ||||||
| T/T or T/C | 1 | - | - | - | 1 | - | |
| C/C | 1.35 (1.02–1.80) | 0.032 | - | - | 1.39 (1.01–1.91) | 0.037 | |
| VEGFR1 | rs9582036 | ||||||
| A/A | 1 | - | - | - | - | - | |
| C/A or C/C | 1.34 (1.06–1.71) | 0.011 | - | - | - | - | |
| Significant clinical characteristics | |||||||
| Histological grade | Grade I or II | - | - | 1 | - | 1 | - |
| Grade III | - | - | 1.50 (1.15–1.95) | <0.001 | 2.0 (1.50–2.65) | <0.001 | |
| Subtype | Hormonal receptor-positive | - | - | 1 | - | 1 | - |
| Triple-negative | - | - | 1.75 (1.29–2.37) | <0.001 | 2.26 (1.64–3.12) | <0.001 | |
| Significant Gene Polymorphisms | Overall Survival | ||||||
|---|---|---|---|---|---|---|---|
| Model A: Genetic | Model B: Clinico-Pathological | Model C: Combined | |||||
| HR [95% CI] | p-Value | HR [95% CI] | p-Value | HR [95% CI] | p-Value | ||
| VEGFA | rs833061 | ||||||
| T/T or T/C | 1 | - | - | - | 1 | - | |
| C/C | 1.59 (1.15–2.20) | 0.003 | - | - | 1.40 (1.00–1.98) | 0.049 | |
| VEGFR1 | rs9582036 | ||||||
| A/A | 1 | - | - | - | 1 | - | |
| C/A or C/C | 1.34 (1.01–1.78) | 0.034 | - | - | 1.56 (1.15–2.10) | 0.003 | |
| VEGFR2 | rs1870377 | ||||||
| T/T | 1 | - | - | - | 1 | - | |
| T/A or A/A | 1.39 (1.04–1.86) | 0.020 | - | - | 1.69 (1.24–2.30) | <0.001 | |
| Significant clinical characteristics | |||||||
| Histological grade | Grade I or II | - | - | - | - | - | - |
| Grade III | - | - | - | - | - | - | |
| Subtype | Hormonal receptor-positive | - | - | 1 | - | 1 | - |
| Triple-negative | - | - | 3.42 (2.44–4.81) | <0.001 | 4.22 (2.96–6.01) | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gal, J.; Milano, G.; Brest, P.; Ebran, N.; Gilhodes, J.; Llorca, L.; Dubot, C.; Romieu, G.; Desmoulins, I.; Brain, E.; et al. VEGF-Related Germinal Polymorphisms May Identify a Subgroup of Breast Cancer Patients with Favorable Outcome under Bevacizumab-Based Therapy—A Message from COMET, a French Unicancer Multicentric Study. Pharmaceuticals 2020, 13, 414. https://doi.org/10.3390/ph13110414
Gal J, Milano G, Brest P, Ebran N, Gilhodes J, Llorca L, Dubot C, Romieu G, Desmoulins I, Brain E, et al. VEGF-Related Germinal Polymorphisms May Identify a Subgroup of Breast Cancer Patients with Favorable Outcome under Bevacizumab-Based Therapy—A Message from COMET, a French Unicancer Multicentric Study. Pharmaceuticals. 2020; 13(11):414. https://doi.org/10.3390/ph13110414
Chicago/Turabian StyleGal, Jocelyn, Gérard Milano, Patrick Brest, Nathalie Ebran, Julia Gilhodes, Laurence Llorca, Coraline Dubot, Gilles Romieu, Isabelle Desmoulins, Etienne Brain, and et al. 2020. "VEGF-Related Germinal Polymorphisms May Identify a Subgroup of Breast Cancer Patients with Favorable Outcome under Bevacizumab-Based Therapy—A Message from COMET, a French Unicancer Multicentric Study" Pharmaceuticals 13, no. 11: 414. https://doi.org/10.3390/ph13110414
APA StyleGal, J., Milano, G., Brest, P., Ebran, N., Gilhodes, J., Llorca, L., Dubot, C., Romieu, G., Desmoulins, I., Brain, E., Goncalves, A., Ferrero, J. -M., Cottu, P. -H., Debled, M., Tredan, O., Chamorey, E., Merlano, M. C., Lemonnier, J., Etienne-Grimaldi, M. -C., & Pierga, J. -Y. (2020). VEGF-Related Germinal Polymorphisms May Identify a Subgroup of Breast Cancer Patients with Favorable Outcome under Bevacizumab-Based Therapy—A Message from COMET, a French Unicancer Multicentric Study. Pharmaceuticals, 13(11), 414. https://doi.org/10.3390/ph13110414