
Evaluation of the Healing Effect of Ointments Based on Bee Products on Cutaneous Lesions in Wistar Rats


 ,
, .png)

Abstract
:1. Introduction
2. Results
2.1. HPLC Analysis of Propolis and Honey Samples
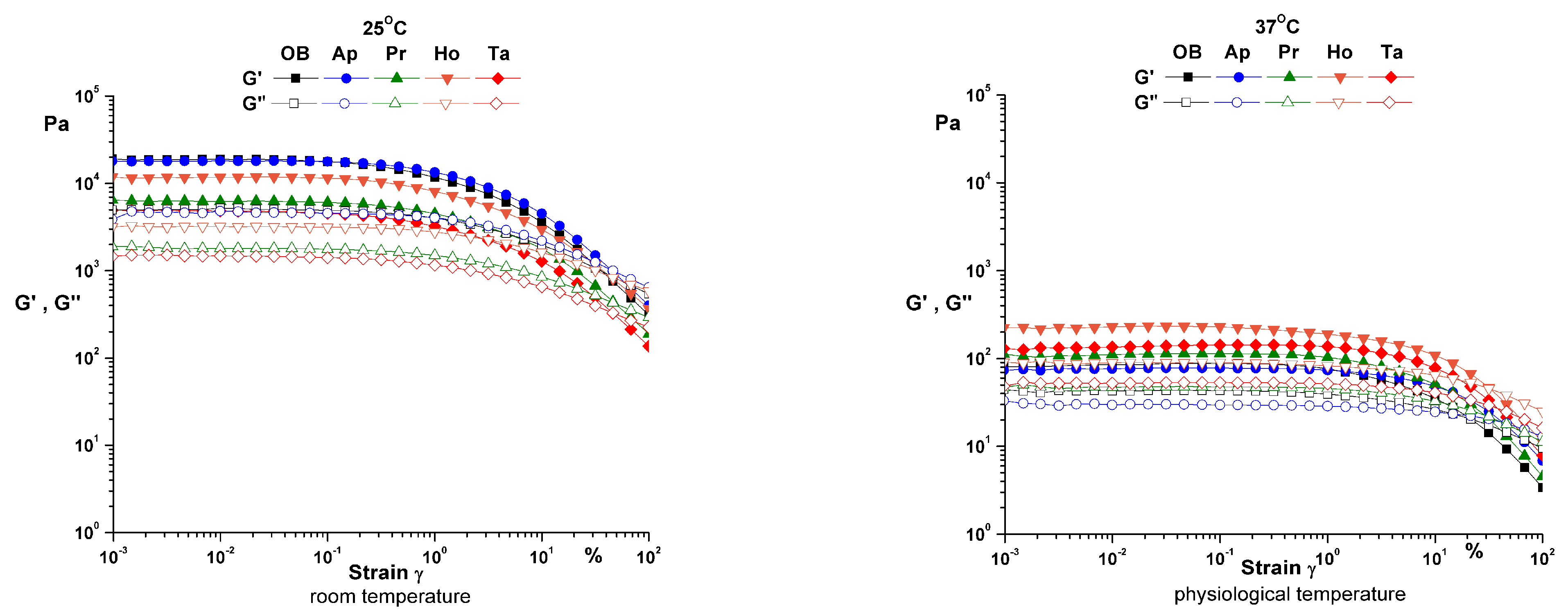
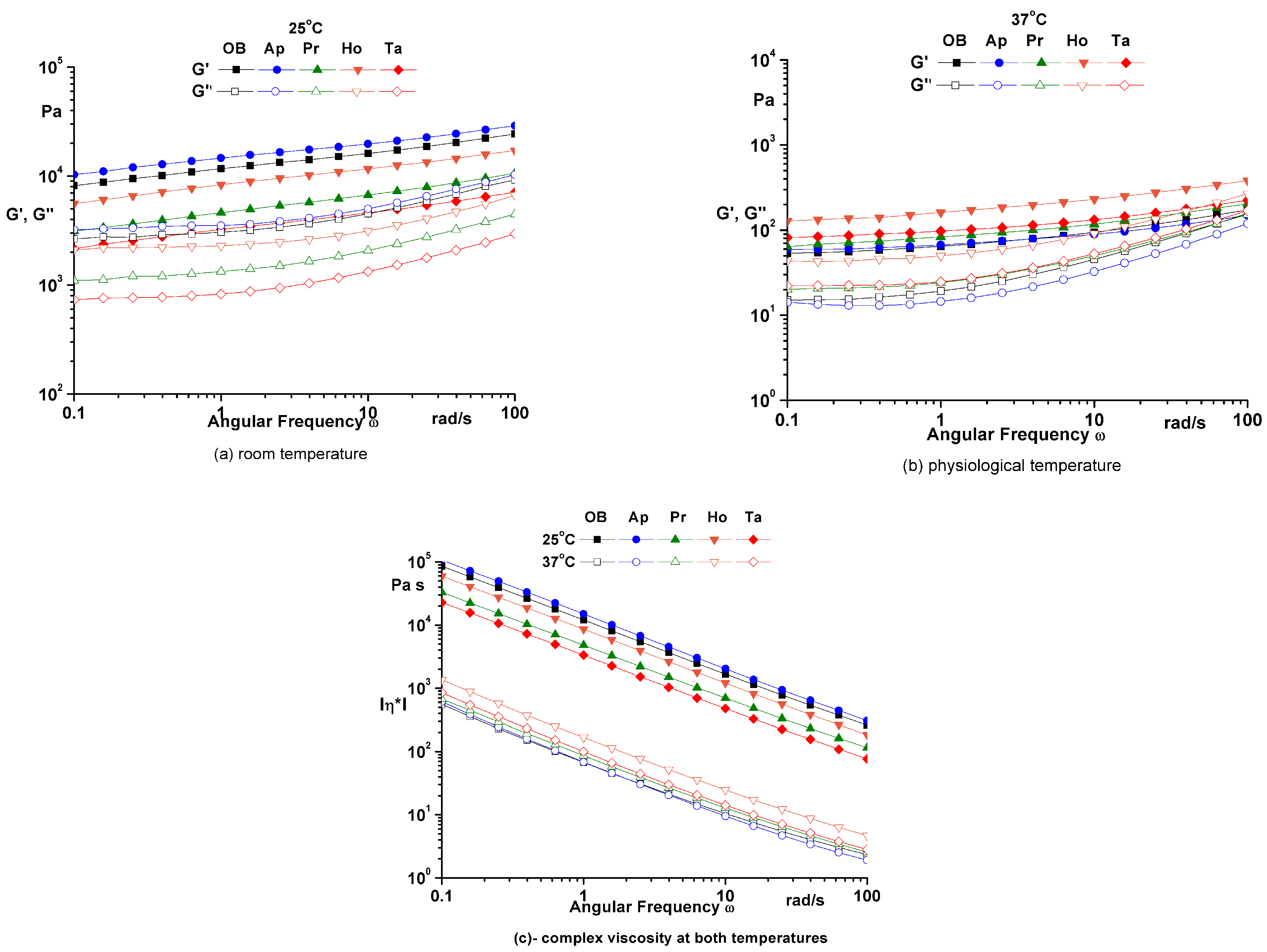
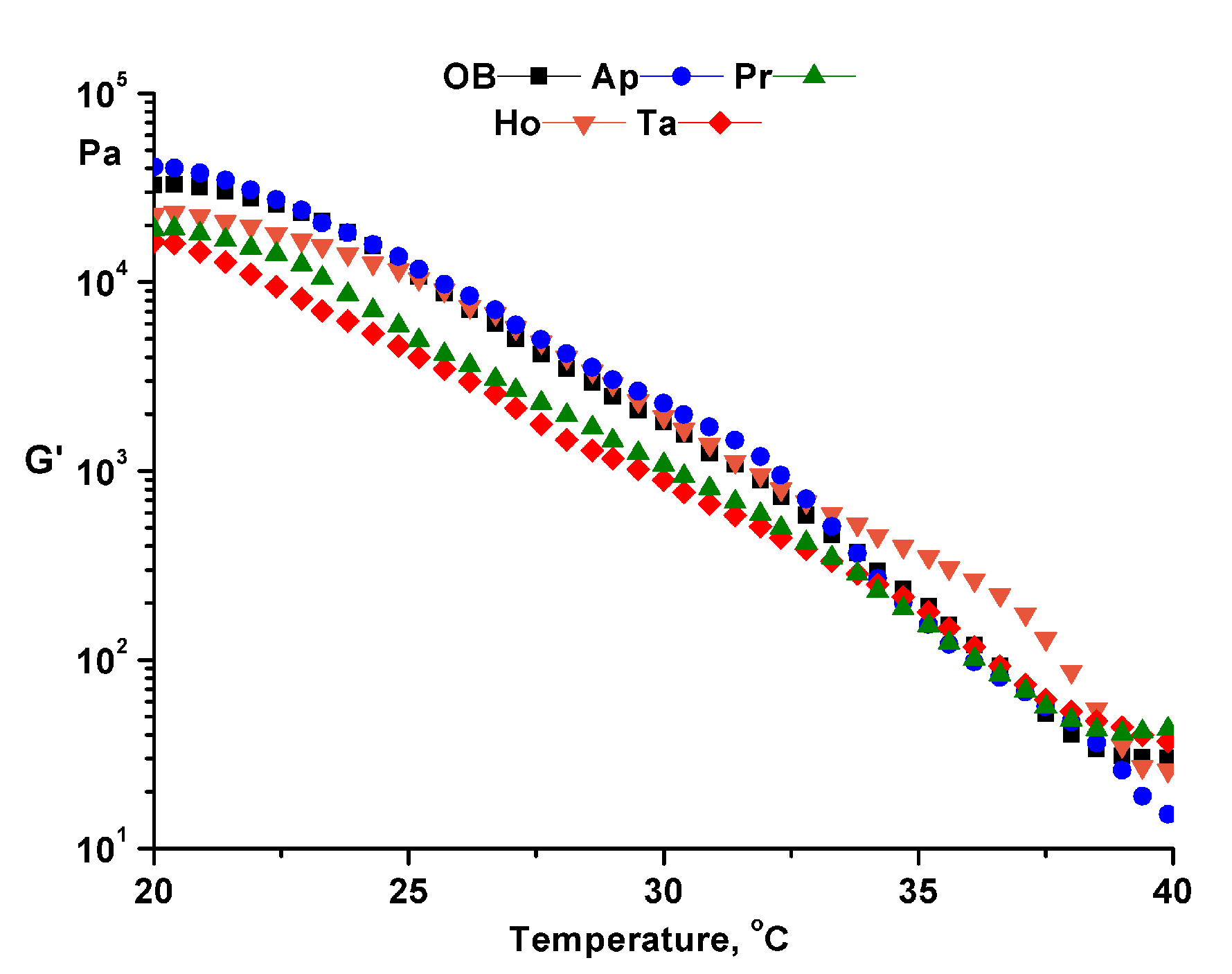
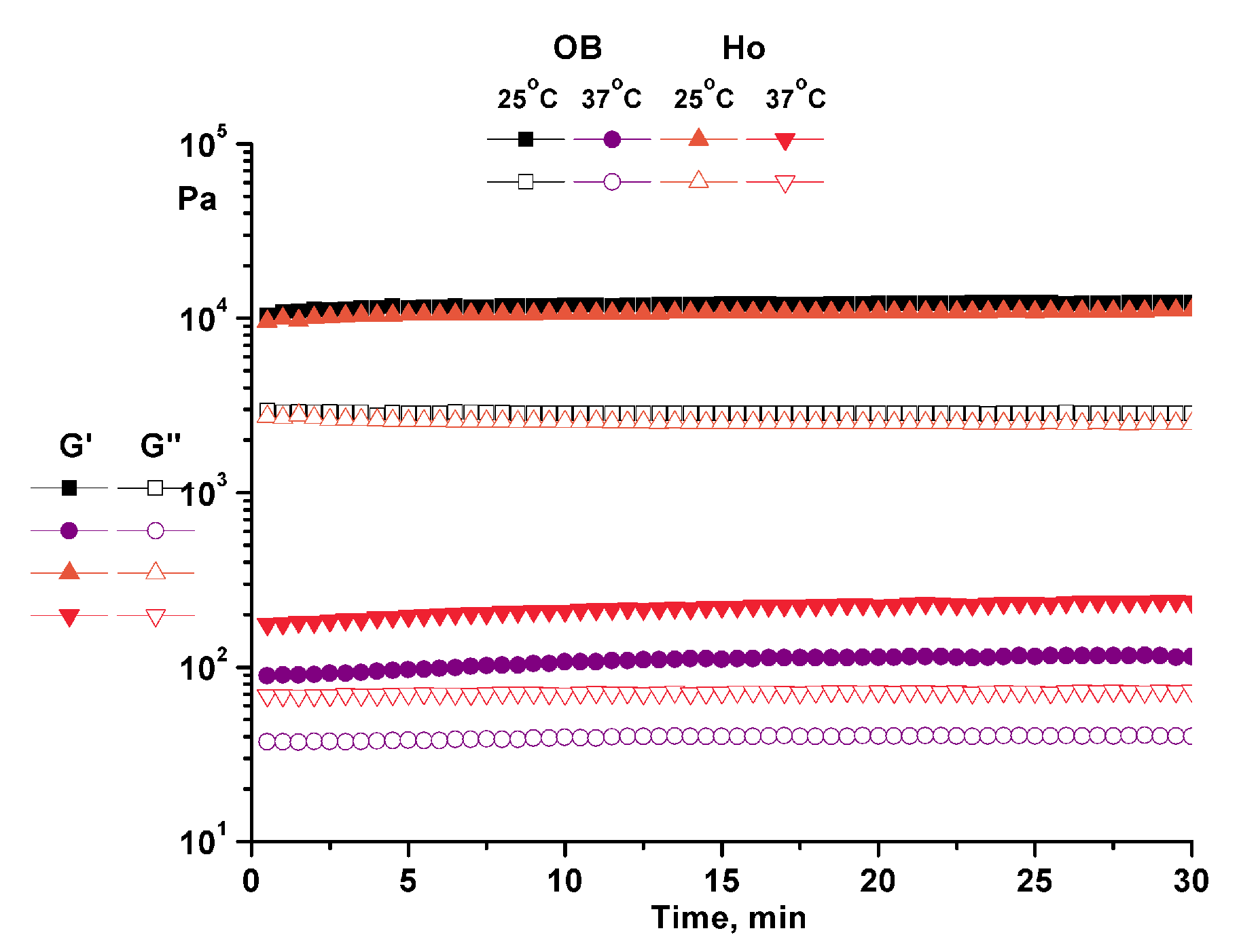
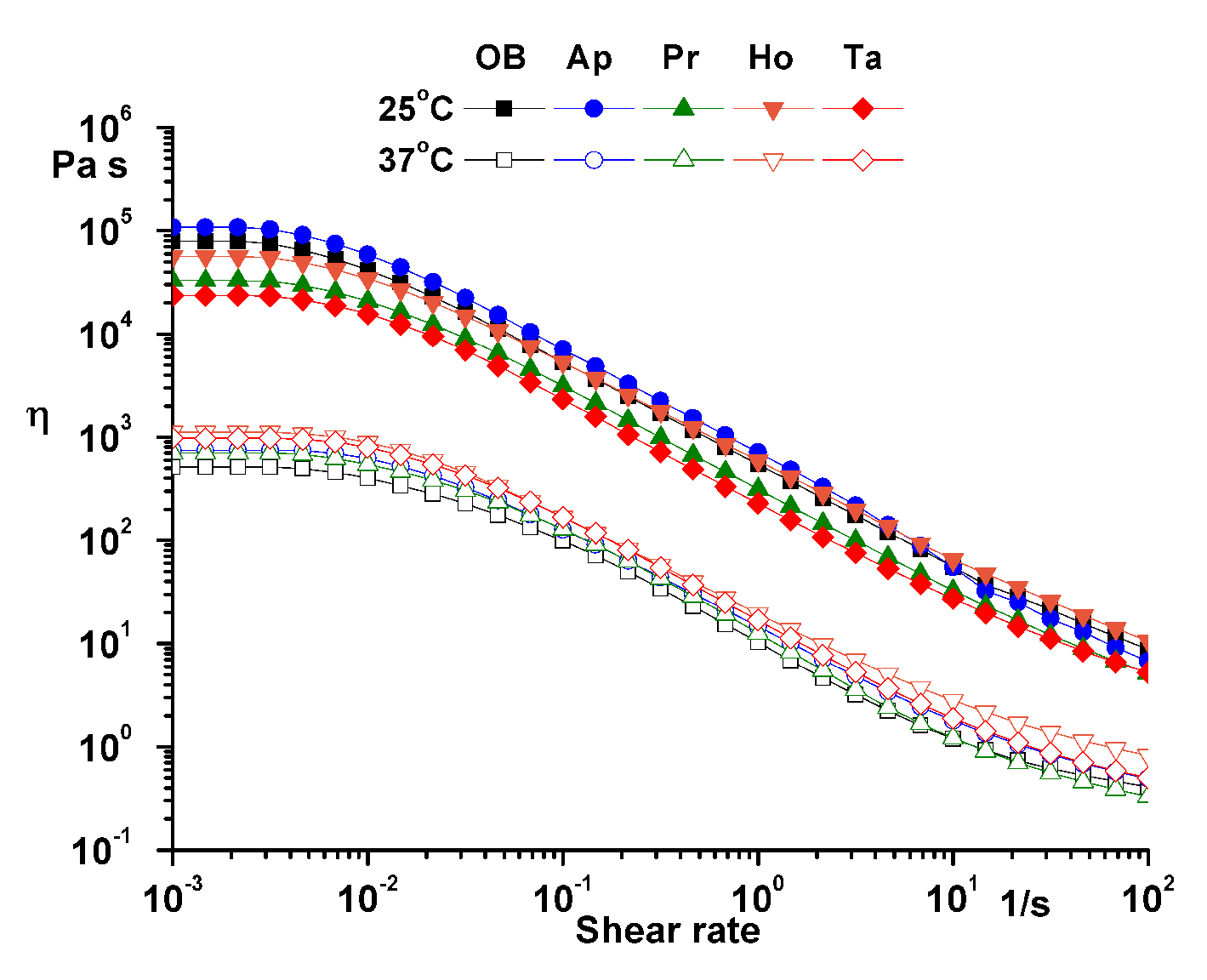
2.2. Rheological Characterization
2.3. Wound Healing Evaluation Parameters
2.3.1. Period of Re-epithelialization and Wound Contraction Rate
2.3.2. Histological Examination
3. Discussion
4. Materials and Methods
4.1. Chromatographi Conditions for HPLC Analysis
4.1.1. Polyphenol Analysis
4.1.2. Caffeic and Chlorogenic Acids Analysis
4.1.3. Methoxylated Flavonoids Analysis
4.2. Ointments Preparation
4.2.1. The Ointment with Propolis Extract
4.2.2. The Ointment with Honey
4.2.3. The Ointment with Apilarnil
4.2.4. The Ointment with a Mixture of Bee Products
4.3. Chemical Reagents and Bee Products
4.4. Rheological Characterization of Ointments
4.5. Experimental Skin Lesions
4.5.1. Evaluated Parameters
Wound Contraction Rate Measurement (WCR)
Measurement of the Re-Epithelialization Period
Histopathological Examination
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Afonso, A.; Gonçalves, J.; Luís, Â.; Gallardo, E.; Duarte, A.P. Evaluation of the In Vitro Wound-Healing Activity and Phytochemical Characterization of Propolis and Honey. Appl. Sci. 2020, 10, 1845. [Google Scholar] [CrossRef] [Green Version]
- Oryan, A.; Alemzadeh, E.; Moshiri, A. Potential role of propolis in wound healing: Biological properties and therapeutic activities. Biomed. Pharmacother. 2018, 98, 469–483. [Google Scholar] [CrossRef] [PubMed]
- Bărnuţiu, L.I.; Mărghitaş, L.A.; Dezmirean, D.; Bobiş, O.; Mihai, C.; Pavel, C. Physico-Chemical Composition of Apilarnil (Bee Drone Larvae); Scientific Papers-Animal husbandry Series; USAMV: Iasi, Romania, 2013; Volume 59, pp. 199–202. [Google Scholar]
- Sidor, E.; Dżugan, M. Drone Brood Homogenate as Natural Remedy for Treating Health Care Problem: A Scientific and Practical Approach. Molecules 2020, 25, 5699. [Google Scholar] [CrossRef] [PubMed]
- Sawczuk, R.; Karpinska, J.; Miltyk, W. What do we need to know about drone brood homogenate and what is known. J. Ethnopharmacol. 2019, 245, 111581. [Google Scholar] [CrossRef] [PubMed]
- Andritoiu, C.V.; Andriescu, C.E.; Danu, M.; Lungu, C.; Ivanescu, B.; Havarneanu, C.; Popa, M. Evaluation of the Wound Healing Potential of Some Natural Polymers on Three Experimental Models. Pharmaceuticals 2021, 14, 465. [Google Scholar] [CrossRef]
- Andritoiu, C.V.; Andriescu, C.E.; Ibanescu, C.; Lungu, C.; Ivanescu, B.; Vlase, L.; Havarneanu, C.; Popa, M. Effects and Characterization of Some Topical Ointments Based on Vegetal Extracts on Incision, Excision, and Thermal Wound Models. Molecules 2020, 25, 5356. [Google Scholar] [CrossRef]
- Ibănescu, C.; Danu, M.; Nanu, A.; Lungu, M.; Simionescu, B.C. Stability of disperse systems estimated using rheological oscillatory shear tests. Rev. Roum. Chim. 2010, 55, 933–940. [Google Scholar]
- Lukic, M.; Jaksic, I.; Krstonosic, V.; Cekic, N.; Savic, S. A combined approach in characterization of an effective w/o hand cream: The influence of emollient on textural, sensorial and in vivo skin performance. Int. J. Cosmet. Sci. 2012, 34, 140–149. [Google Scholar] [CrossRef]
- Cobzaru, C.; Gherghescu, O.; Aursulesei, A.E.; Ibănescu, C.; Danu, M.; Apostolescu, G.A.; Cernătescu, C. Rheological behaviour of cold creams with cinnamon and Thuja alcoholic extract. Rev. Chim. 2017, 68, 1959–1962. [Google Scholar] [CrossRef]
- Bairagi, U.; Mittal, P.; Singh, J.; Mishra, B. Preparation, characterization, and in vivo evaluation of nano formulations of ferulic acid in diabetic wound healing. Drug Dev. Ind. Pharm. 2018, 44, 1783–1796. [Google Scholar] [CrossRef]
- Ghaisas, M.M.; Kshirsagar, S.B.; Sahane, R.S. Evaluation of wound healing activity of ferulic acid in diabetic rats. Int. Wound J. 2014, 11, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Boeing, T.; Costa, P.; Venzon, L.; Meurer, M.; Mariano, L.N.B.; França, T.C.S.; Gouveia, L.; de Bassi, A.C.; Steimbach, V.; de Souza, P.; et al. Gastric healing effect of p-coumaric acid isolated from Baccharis dracunculifolia DC on animal model. Naunyn Schmiedebergs Arch. Pharmacol. 2021, 394, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Contardi, M.; Heredia-Guerrero, J.A.; Guzman-Puyol, S.; Summa, M.; Benítez, J.J.; Goldoni, L.; Caputo, G.; Cusimano, G.; Picone, P.; Di Carlo, M.; et al. Combining dietary phenolic antioxidants with polyvinylpyrrolidone: Transparent biopolymer films based on p-coumaric acid for controlled release. J. Mater. Chem. B 2019, 7, 1384–1396. [Google Scholar] [CrossRef] [PubMed]
- Song, H.S.; Park, T.W.; Sohn, U.D.; Shin, Y.K.; Choi, B.C.; Kim, C.J.; Sim, S.S. The Effect of Caffeic Acid on Wound Healing in Skin-incised Mice. Korean J. Physiol. Pharmacol. 2008, 12, 343–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olgierd, B.; Kamila, Ż.; Anna, B.; Emilia, M. The Pluripotent Activities of Caffeic Acid Phenethyl Ester. Molecules 2021, 26, 1335. [Google Scholar] [CrossRef]
- Carvalho, M.T.B.; Araújo-Filho, H.G.; Barreto, A.S.; Quintans-Júnior, L.J.; Quintans, J.S.S.; Barreto, R.S.S. Wound healing properties of flavonoids: A systematic review highlighting the mechanisms of action. Phytomedicine 2021, 90, 153636. [Google Scholar] [CrossRef]
- Freinkel, R.K. Carbohydrate metabolism of epidermis. In Biology of the Skin; Freinkel, R.K., Woodley, D., Eds.; Parthenon Publishing Group: London, UK, 2001; pp. 452–454. [Google Scholar]
- Alecu, M. Molecular Pathology of Skin; Medical Publishing: Bucharest, Romania, 2006; pp. 56–64. [Google Scholar]
- Andriţoiu, C.V.; Prisăcaru, A.I.; Andriescu, C.; Popa, M.I. Evaluation of the efficacy of some bee products upon the chemically induced cutaneous erythema in Wistar rats. Ann. Rom. Soc. Cell Biol. 2012, XVII, 258–264. [Google Scholar]
- Andriţoiu, C.V.; Popa, M. New Natural Biocompatible Materials with Applications in Wound-Healing; Lap Lambert Publishing: Saarbrücken, Germany, 2014. [Google Scholar]
- Scepankova, H.; Combarros-Fuertes, P.; Fresno, J.M.; Tornadijo, M.E.; Dias, M.S.; Pinto, C.A.; Saraiva, J.A.; Estevinho, L.M. Role of Honey in Advanced Wound Care. Molecules 2021, 26, 4784. [Google Scholar] [CrossRef]
- Almasaudi, S. The antibacterial activities of honey. Saudi J. Biol. Sci. 2021, 28, 2188–2196. [Google Scholar] [CrossRef]
- Pullar, J.M.; Carr, A.C.; Vissers, M.C.M. The Roles of Vitamin C in Skin Health. Nutrients 2017, 9, 866. [Google Scholar] [CrossRef] [Green Version]
- Nusgens, B.V.; Humbert, P.; Rougier, A.; Colige, A.C.; Haftek, M.; Lambert, C.A.; Richard, A.; Creidi, P.; Lapière, C.M. Topically applied vitamin C enhances the mRNA level of collagens I and III, their processing enzymes and tissue inhibitor of matrix metalloproteinase 1 in the human dermis. J. Investig. Dermatol. 2001, 116, 853–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humbert, P.; Louvrier, L.; Saas, P.; Viennet, C. Vitamin C, aged skin, skin health. In Vitamin C—An Update on Current Uses and Functions; LeBlanc, J.G., Ed.; IntechOpen: London, UK, 2018. [Google Scholar] [CrossRef] [Green Version]
- Pessolato, A.G.; Martins Ddos, S.; Ambrósio, C.E.; Mançanares, C.A.; de Carvalho, A.F. Propolis and amnion reepithelialise second-degree burns in rats. Burns 2011, 37, 1192–1201. [Google Scholar] [CrossRef] [PubMed]
- Mathew-Steiner, S.S.; Roy, S.; Sen, C.K. Collagen in wound healing. Bioengineering 2021, 8, 63. [Google Scholar] [CrossRef]
- dos Santos, J.S.; Monte-Alto-Costa, A. Caffeic acid phenethyl ester improves burn healing in rats through anti-inflammatory and antioxidant effects. J. Burn Care Res. 2013, 34, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Romana-Souza, B.; Dos Santos, J.S.; Monte-Alto-Costa, A. Caffeic acid phenethyl ester promotes wound healing of mice pressure ulcers affecting NF-κB, NOS2 and NRF2 expression. Life Sci. 2018, 207, 158–165. [Google Scholar] [CrossRef]
- Gregory, S.R.; Piccolo, N.; Piccolo, M.T.; Piccolo, M.S.; Heggers, J.P. Comparison of propolis skin cream to silver sulfadiazine: A naturopathic alternative to antibiotics in treatment of minor burns. J. Altern. Complement. Med. 2002, 8, 77–83. [Google Scholar] [CrossRef]
- Henshaw, F.R.; Bolton, T.; Nube, V.; Hood, A.; Veldhoen, D.; Pfrunder, L.; McKew, G.L.; Macleod, C.; McLennan, S.V.; Twigg, S.M. Topical application of the bee hive protectant propolis is well tolerated and improves human diabetic foot ulcer healing in a prospective feasibility study. J. Diabetes Complicat. 2014, 28, 850–857. [Google Scholar] [CrossRef] [Green Version]
- Kucharzewski, M.; Kózka, M.; Urbanek, T. Topical treatment of nonhealing venous leg ulcer with propolis ointment. Evid. Based Complement. Alternat. Med. 2013, 2013, 254017. [Google Scholar] [CrossRef] [Green Version]
- Silici, S. Chemical Content and Bioactive Properties of Drone Larvae (Apilarnil). Mellifera 2019, 19, 14–22. [Google Scholar]
- Ivanescu, B.; Lungu, C.; Vlase, L.; Gheldiu, A.M.; Grigorescu, C.; Corciova, A. Bioactive compounds from Artemisia campestris L. subsp. campestris. Rev. Chim. 2018, 69, 3076–3081. [Google Scholar] [CrossRef]
- Andriţoiu, C.V.; Cadinoiu, A.N.; Prisăcaru, A.I.; Mihailă, D.; Popa, M.; Popa, I.M. New natural biocompatible materials with applications in wound-healing obtained by an environmentally friendly technology, with applications in wound healing. EEMJ 2015, 14, 2185–2199. [Google Scholar]
- Association of Official Analytical Chemists. Vitamin C in Juices and Vitamin Preparations, Official Method 967.21. In AOAC Official Methods of Analysis, 18th ed.; Association of Official Analytical Chemists: Gaithersburg, MD, USA, 2005; p. 45.1.14. [Google Scholar]
- Süntar, I.P.; Akkol, E.K.; Yılmazer, D.; Baykal, T.; Kırmızıbekmez, H.; Alper, M.; Yeşilada, E. Investigations on the in vivo wound healing potential of Hypericum perforatum L. J. Ethnopharmacol. 2010, 127, 468–477. [Google Scholar] [CrossRef]
- DeMesquita, C.J.G.; Leite, J.A.; Fechine, F.V.; deRocha, J.L.C.; Leite, J.G.; Leite Filho, J.A.; Barbosa Filho, R.A. Effect of imiquimod on partial-thickness burns. Burns 2010, 36, 97–108. [Google Scholar] [CrossRef]
- Clark, M.; Peters-Kennedy, J.; Scott, D. Resident lymphocytes in the epidermis and adnexal epithelia of normal dorsolateral thorax of alpacas. Can. J. Vet. Res. 2013, 77, 63–65. [Google Scholar] [PubMed]
- Agbaje, M.; Rutland, C.; Maboni, G.; Blanchard, A.; Bexon, M.; Stewart, C.; Jone, M.; Totemeyer, S. Novel inflammatory cell infiltration scoring system to investigate healthy and footrot affected ovine interdigital skin. PeerJ 2018, 6, e5097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medina, J.; Fourcaudot, A.; Sebastian, E.; Shankar, R.; Brown, A.; Leung, K. Standardization of deep partial-thickness scald burns in C57BL/6 mice. Int. J. Burn. Trauma 2018, 8, 26–33. [Google Scholar]
- Wohlsein, P.; Peteres, M.; Schulze, C.; Baumgärtner, W. Thermal injuries in veterinary forensic pathology. Vet. Pathol. 2016, 53, 1001–1017. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, V.; Galizia, J.P.; Fournier, L. Precise diagnosis of infection in burn wound biopsy specimens. Combination of histologic technique, acridine orange staining, and culture. J. Burn Care Rehabil. 1989, 10, 195–202. [Google Scholar] [CrossRef]
- Church, D.; Elsayed, S.; Reid, O.; Winston, B.; Lindsay, R. Burn wound infections. Clin. Microbiol. Rev. 2006, 19, 403–434. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compound | Concentration in Extract (µg/mL) |
|---|---|
| p-Coumaric acid | 1516.119 ± 60.64 (n = 3) |
| Ferulic acid | 1771.669 ± 53.15 (n = 3) |
| Isoquercitrin | 1.009 ± 0.08 (n = 3) |
| Rutoside | 0.823 ± 0.05 (n = 3) |
| Quercitrin | 11.573 ± 0.57 (n = 3) |
| Quercetin | 18.295 ± 0.73 (n = 3) |
| Luteolin | 6.604 ± 0.46 (n = 3) |
| Kaempferol | 19.537 ± 0.97 (n = 3) |
| Apigenin | 19.195 ± 0.57 (n = 3) |
| Caffeic acid | 796.40 ± 31.85 (n = 3) |
| Chlorogenic acid | 1.670 ± 0.11 (n = 3) |
| Acacetin | 0.613 ± 0.03 (n = 3) |
| Jaceosidin | 0.821 ± 0.04 (n = 3) |
| Hispidulin | 0.393 ± 0.03 (n = 3) |
| Experimental Groups | Wound Area (mm2) | Re-Epithelialization Area (mm2) | WCR (%) (Mean ± SEM) | |||
|---|---|---|---|---|---|---|
| Day 0 | Day 6 | Day 9 | Day 12 | Day 6 | Day 9 | |
| NC Group | 64.0 (8.0 × 8.0) | 61.6 (7.7 × 8.0) | 56.25 (7.5 × 7.5) | - | 5.78 ± 1.86 | 14.85 ± 2.95 |
| OB Group | 64.0 (8.0 × 8.0) | 45.5 (6.5 × 7.0) | 40.8 (6.0 × 6.8) | - | 26.74 ± 2.13 * | 33.79 ± 2.21 * |
| Ho Group | 64.0 (8.0 × 8.0) | 20.0 (4.0 × 5.0) | 4.0 (2.0 × 2.0) | 1.5 × 2.0 | 69.38 ± 0.63 | 93.65 ± 0.28 |
| Pr Group | 64.0 (8.0 × 8.0) | 16.0 (4.0 × 4.0) | 1.5 (1.0 × 1.5) | 1.0 × 1.0 | 73.06 ± 1.36 | 97.97 ± 0.16 |
| Ap Group | 64.0 (8.0 × 8.0) | 25.0 (5.0 × 5.0) | 9.0 (3.0 × 3.0) | 2.0 × 2.0 | 63.93 ± 2.26 | 84.69 ± 0.68 |
| Ta Group | 64.0 (8.0 × 8.0) | 18.0 (4.0 × 4.5) | 2.0 (1.0 × 2.0) | 1.0 × 1.2 | 72.50 ± 0.36 | 96.54 ± 0.18 |
| Incision | ||
 |  |  |
| lymphocytes, epidermis and dermis (S1, G0) | vascular congestion, hypodermis (S0, G0) | rare periadnexal inflammatory infiltrate (S1, G0) |
| Excision | ||
 |  |  |
| slight edema, perivascular lymphocytes (S2, G0) | hemorrhage in the muscular layer (S0, G0) | hemorrhage in the muscular layer in polarized light microscopy (S0, G0) |
| Thermal Burn | ||
 |  |  |
| severe dermal collagenization (S1, D1, G0) | congestion in hypodermis (S0, D0, G0) | severe dermal collagenization (S0, D0, G0) |
| Experimental Groups | Incision | Excision | Thermal Burn |
|---|---|---|---|
| NC Group |  |  |  |
| abscess in keratin layer—polarized light microscopy (S3, GIa) | acanthosis and vacuolar degeneration, epidermis and dermis (S1, G0) | severe inflammation with hemorrhagic areas (S3, D2, G0) | |
| OB Group |  |  |  |
| inflammatory infiltrate in hypodermis (S2, G0) | important inflammatory infiltrate in hypodermis (S2, G0) | severe inflammation with hemorrhagic areas (S2, G0) | |
| Ho Group |  |  |  |
| inflammatory infiltrate in hypodermis and interstitial muscle (S2, G0) | inflammatory infiltrate in hypodermis (S2, G0) | inflammation in hypodermis (S2, D0, G0) | |
| Pr Group |  |  |  |
| edema in superficial dermis (S1, G0) | inflammatory infiltrate in hypodermis (S2, D0, G0) | perivascular inflammatory infiltrate (S2, D0, G0) | |
| Ap Group |  |  |  |
| fibroblasts (S1, G0) | interstitial inflammatory infiltrate, striated muscle (S1, G0) | myositis, moderate inflammatory infiltrate in the muscle interstitium (S1, D0, G0) | |
| Ta Group |  |  |  |
| inflammation in hypodermis (S1, G0) | lymphocytes in superficial dermis (S0, G0) | severe inflammation with hemorrhagic areas (S3, D0, G0) |
| Experimental Groups | Incision | Excision | Thermal Burn |
|---|---|---|---|
| NC Group |  |  |  |
| congestion in hypodermis—detail in polarized light microscopy (S1, G0) | exocytosis (S2, G0) | inflammatory infiltrate in hypodermis (S2, D0, G0) | |
| OB Group |  |  |  |
| multinucleated foreign-body giant cell, congestion in hypodermis—detail in polarized light microscopy (S2, G0) | multinucleated foreign-body giant cell—detail in polarized light microscopy (S2, G0) | rare periadnexal inflammatory infiltrate (S2, D0, G0) | |
| Ho Group |  |  |  |
| rare lymphocytes in hypodermis (S1, G0) | mature granulation tissue, residual myocytes in the area of connective tissue organization (S1, G0) | dermal collagenization(S0, D0, G0) | |
| Pr Group |  |  |  |
| collagenization in superficial dermis (S1, G0) | dermal collagenization with congestion (S1, G0) | moderate hypodermic infiltrate (S1, D0, G0) | |
| Ap Group |  |  |  |
| rare perivascular lymphocytes (S1, G0) | severe dermal collagenization (S1, G0) | dermal collagenization (S1, D0, G0) | |
| Ta Group |  |  |  |
| rare lymphocytes in superficial dermis (S1, G0) | dermal collagenization (S1, G0) | inflammatory infiltrate—detail in polarized light microscopy (S1, D0, G0) |
| Experimental Groups | Incision | Excision | Thermal Burn |
|---|---|---|---|
| NC Group |  |  |  |
| edema and inflammatory infiltrate (S1, G0) | inflammation in muscular layer—detail in polarized light microscopy (S1, G0) | lymphocytes in hypodermis (S1, D0, G0) | |
| OB Group |  |  |  |
| hypodermis with inflammatory infiltrate (S0, D0) | hypodermis with inflammatory infiltrate—detail in polarized light microscopy (S1, G0) | vessel with thickened wall, lymphocytes (S0, D0, G0) | |
| Ho Group |  |  |  |
| slight dermal edema (S0, G0) | dermal collagenization (S0, G0) | severe dermal collagenization (S1, D0, G0) | |
| Pr Group |  |  |  |
| dermal collagenization (S1, G0) | severe dermal collagenization (S1, G0) | severe dermal collagenization (S0, D0, G0) | |
| Ap Group |  |  |  |
| skin appendages (S0, G0) | dermal collagenization and associated inflammatory infiltrate (S0, G0) | moderate inflammatory infiltrate in superficial dermis (S1, D0, G0) | |
| Ta Group |  |  |  |
| hair follicle with rare lymphocytes (S1, G0) | rare lymphocytes (S1, G0) | severe dermal collagenization (S1, D0, G0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andritoiu, C.V.; Lungu, C.; Danu, M.; Ivanescu, B.; Andriescu, C.E.; Vlase, L.; Havarneanu, C.; Iurciuc, C.E.; Popa, M. Evaluation of the Healing Effect of Ointments Based on Bee Products on Cutaneous Lesions in Wistar Rats. Pharmaceuticals 2021, 14, 1146. https://doi.org/10.3390/ph14111146
Andritoiu CV, Lungu C, Danu M, Ivanescu B, Andriescu CE, Vlase L, Havarneanu C, Iurciuc CE, Popa M. Evaluation of the Healing Effect of Ointments Based on Bee Products on Cutaneous Lesions in Wistar Rats. Pharmaceuticals. 2021; 14(11):1146. https://doi.org/10.3390/ph14111146
Chicago/Turabian StyleAndritoiu, Calin Vasile, Cristina Lungu, Maricel Danu, Bianca Ivanescu, Corina Elena Andriescu, Laurian Vlase, Corneliu Havarneanu, Camelia Elena Iurciuc (Tincu), and Marcel Popa. 2021. "Evaluation of the Healing Effect of Ointments Based on Bee Products on Cutaneous Lesions in Wistar Rats" Pharmaceuticals 14, no. 11: 1146. https://doi.org/10.3390/ph14111146
APA StyleAndritoiu, C. V., Lungu, C., Danu, M., Ivanescu, B., Andriescu, C. E., Vlase, L., Havarneanu, C., Iurciuc, C. E., & Popa, M. (2021). Evaluation of the Healing Effect of Ointments Based on Bee Products on Cutaneous Lesions in Wistar Rats. Pharmaceuticals, 14(11), 1146. https://doi.org/10.3390/ph14111146