

Clinical Efficacy and Safety of Chinese Herbal Medicine in the Treatment of Uremic Pruritus: A Meta-Analysis of Randomized Controlled Trials

Abstract
:
1. Introduction
2. Results
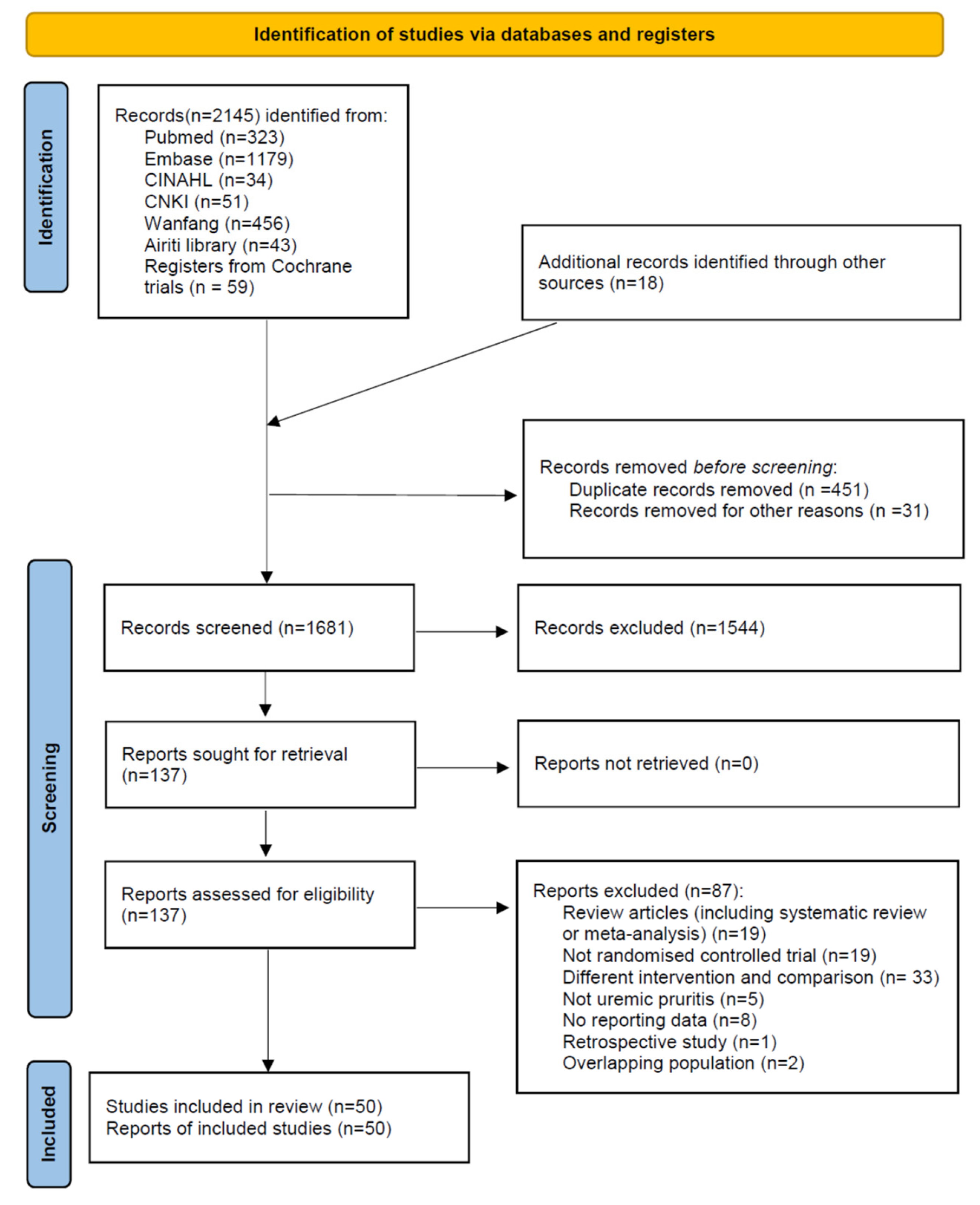
2.1. Characteristics of Included Studies
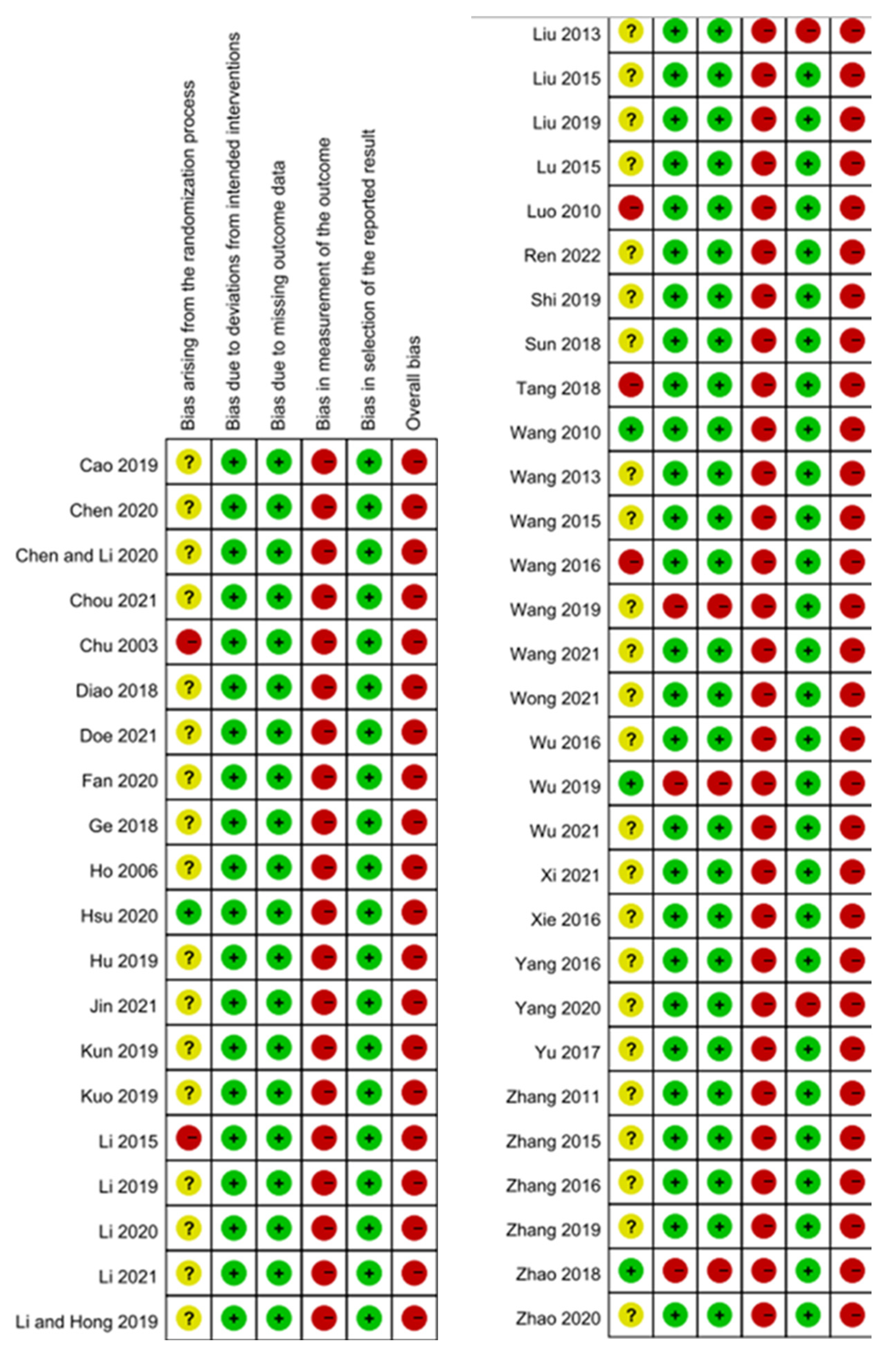
2.2. Risk of Bias
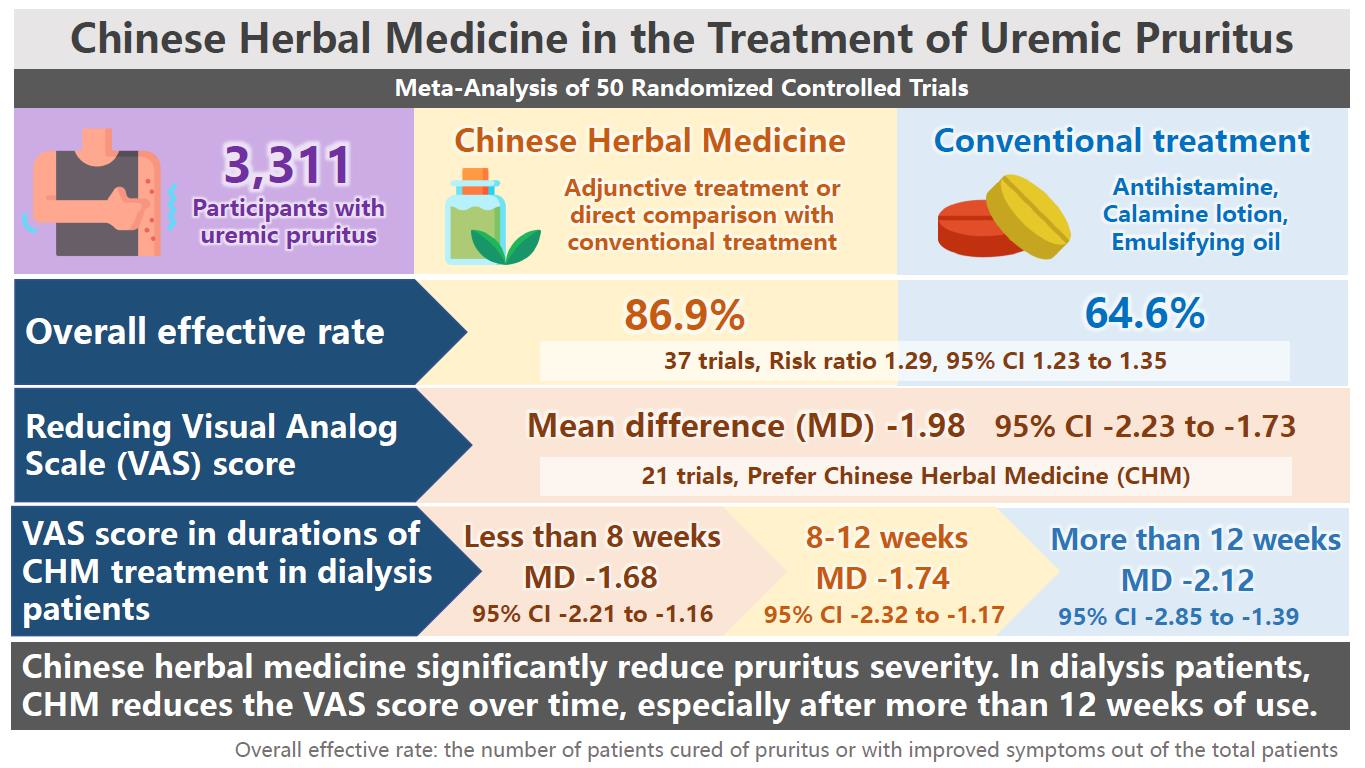
2.3. Primary Outcome
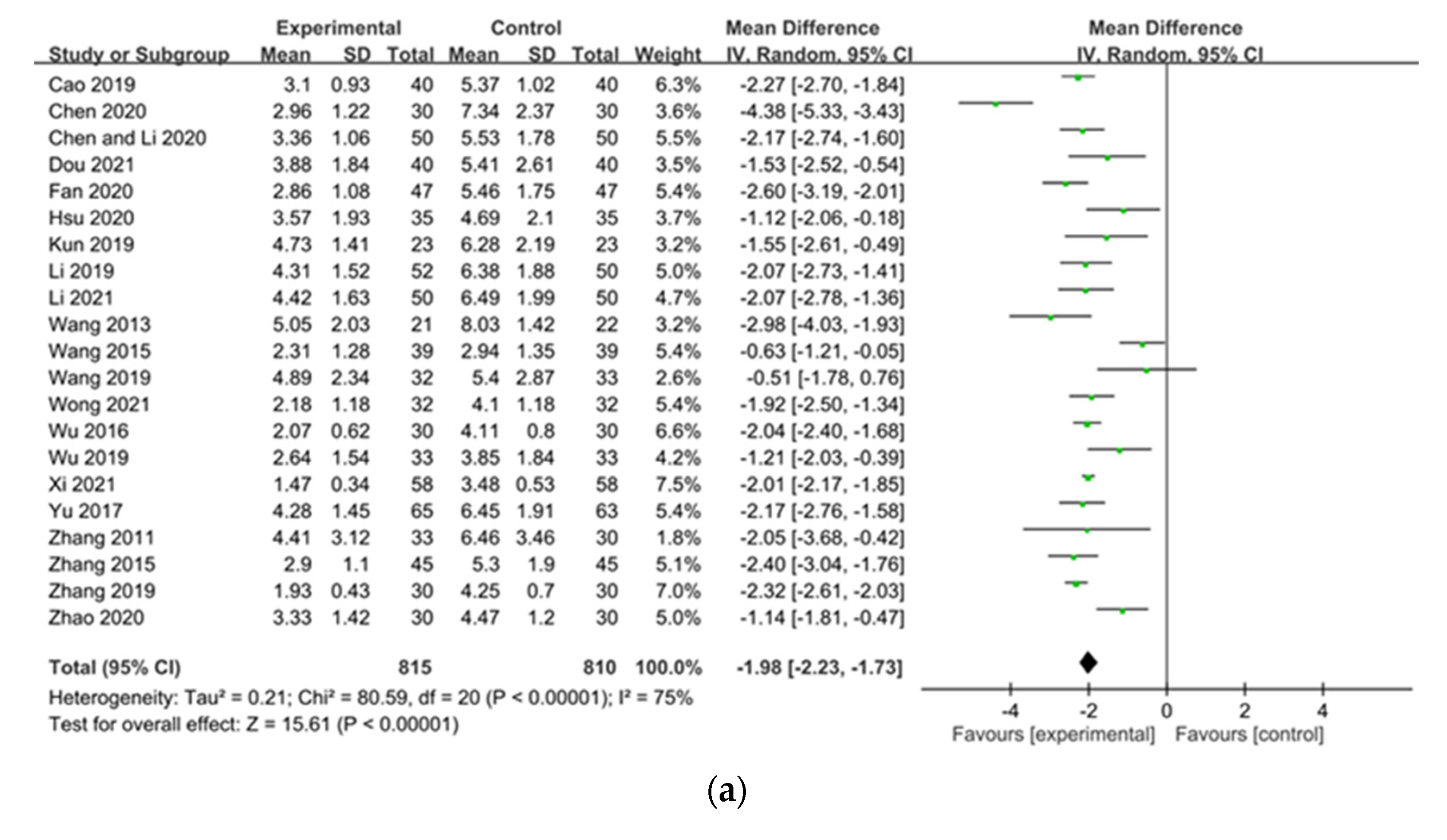
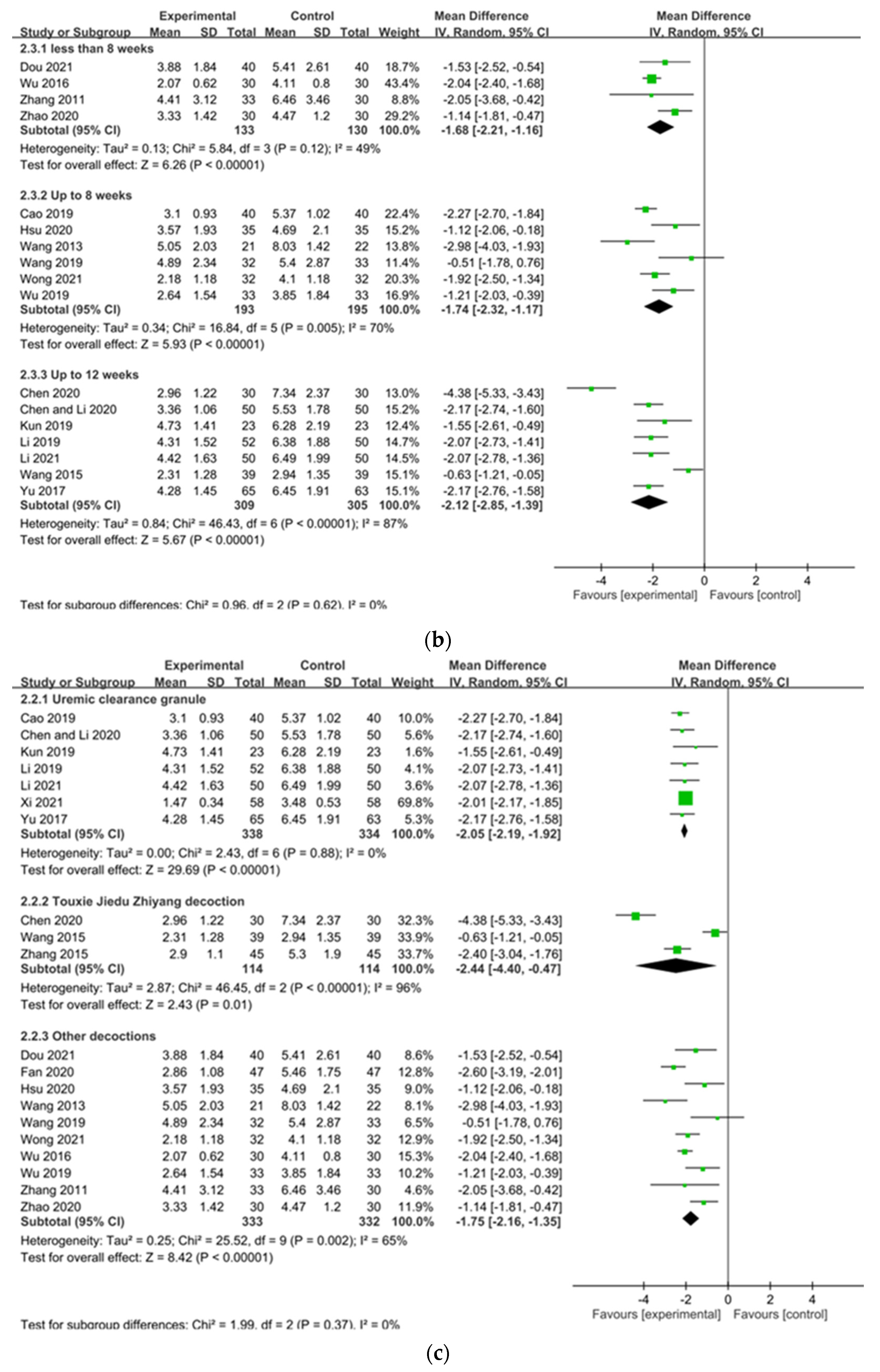
2.3.1. Pruritus Severity (Visual Analog Scale (VAS), Duo, Dirk R. Kuypers Itching Scale)
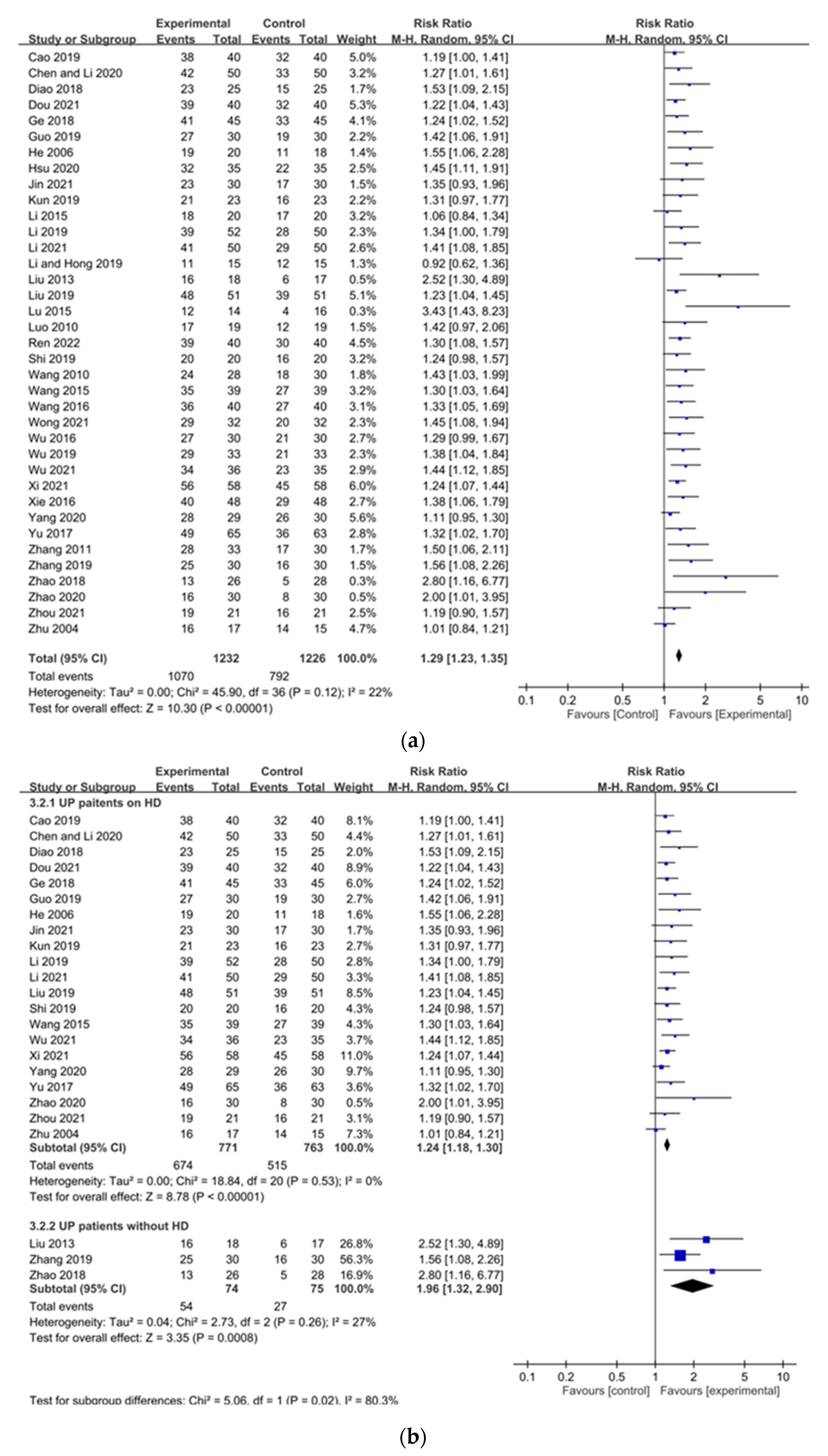
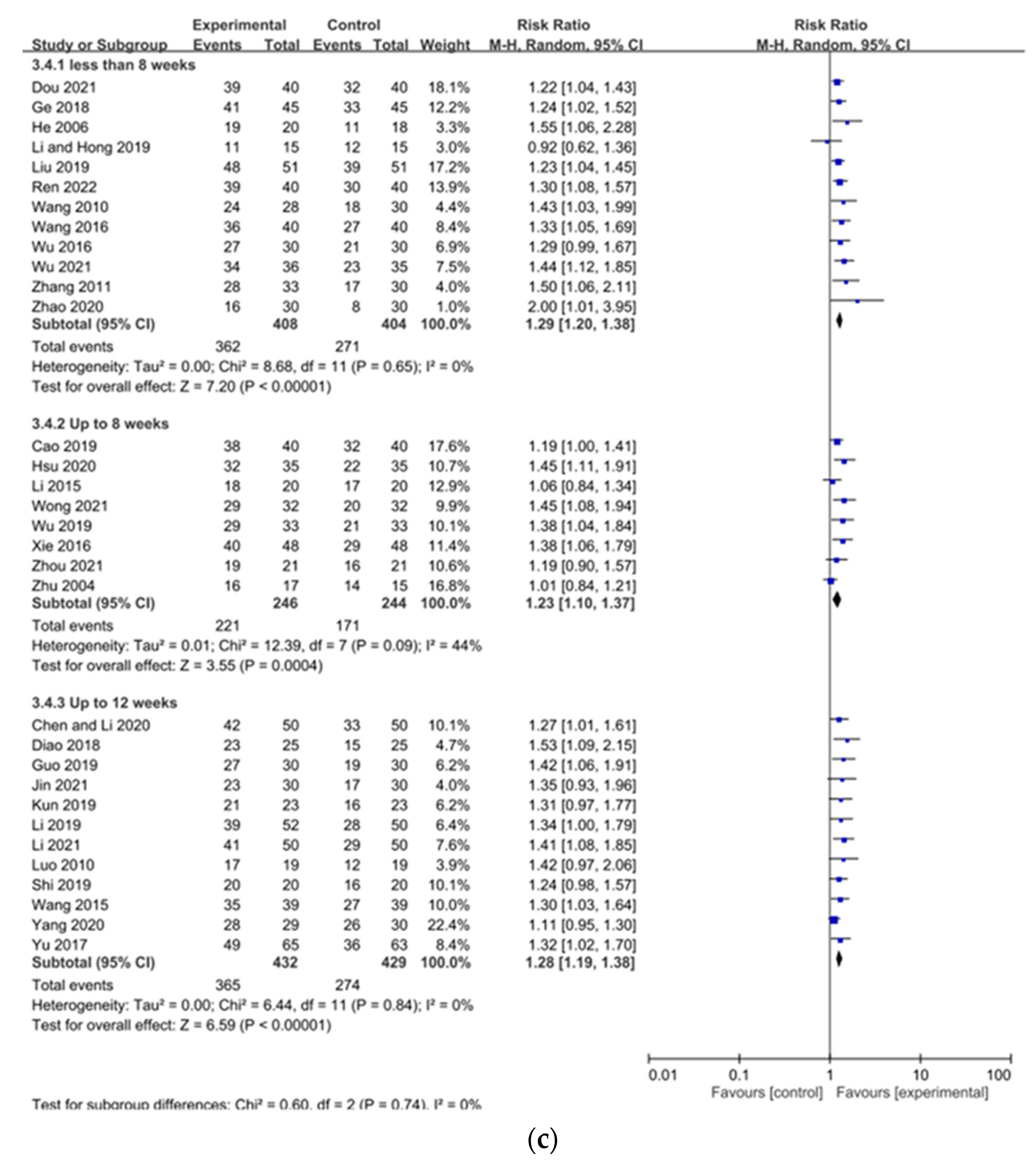
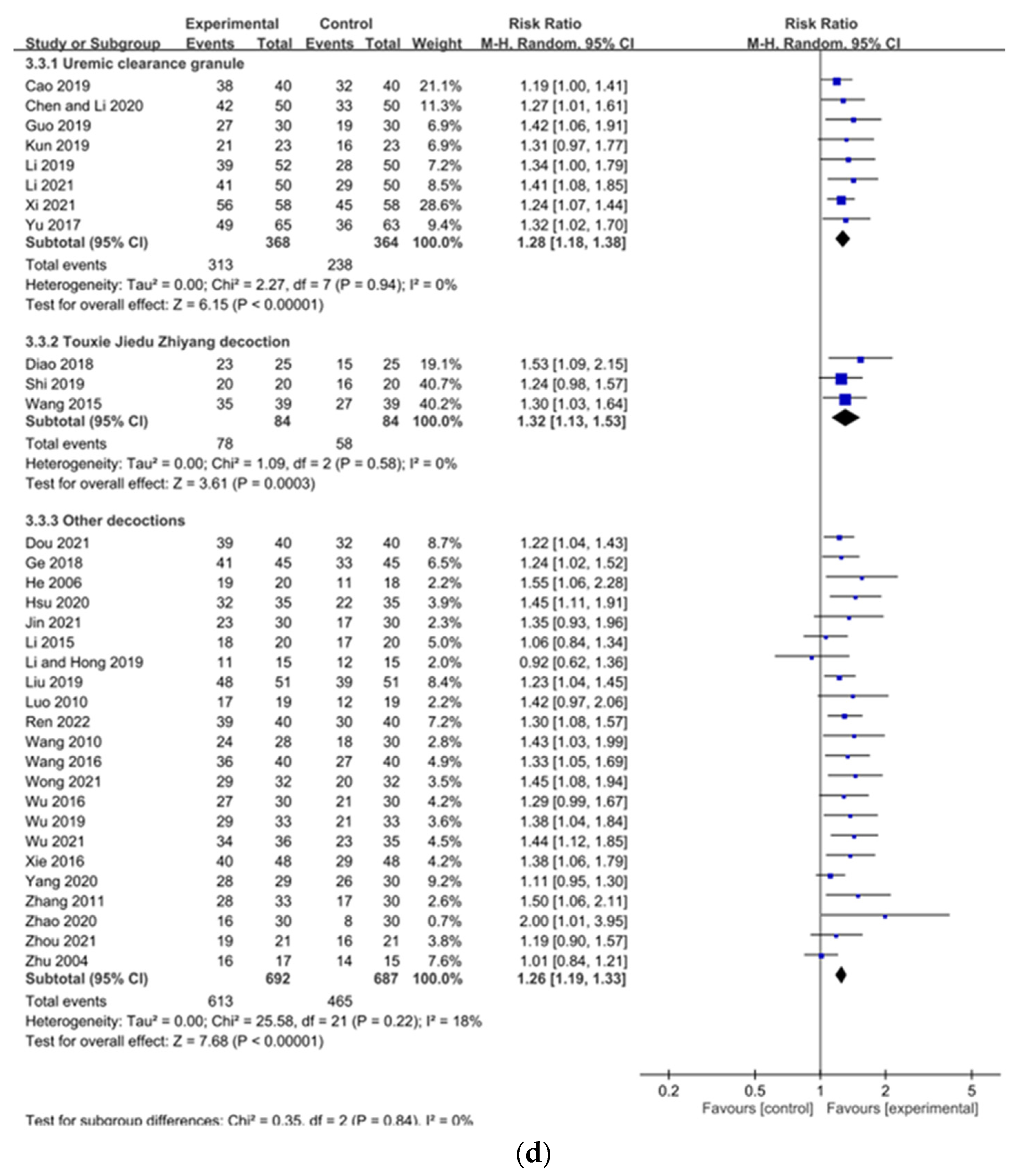
2.3.2. Overall Effectiveness
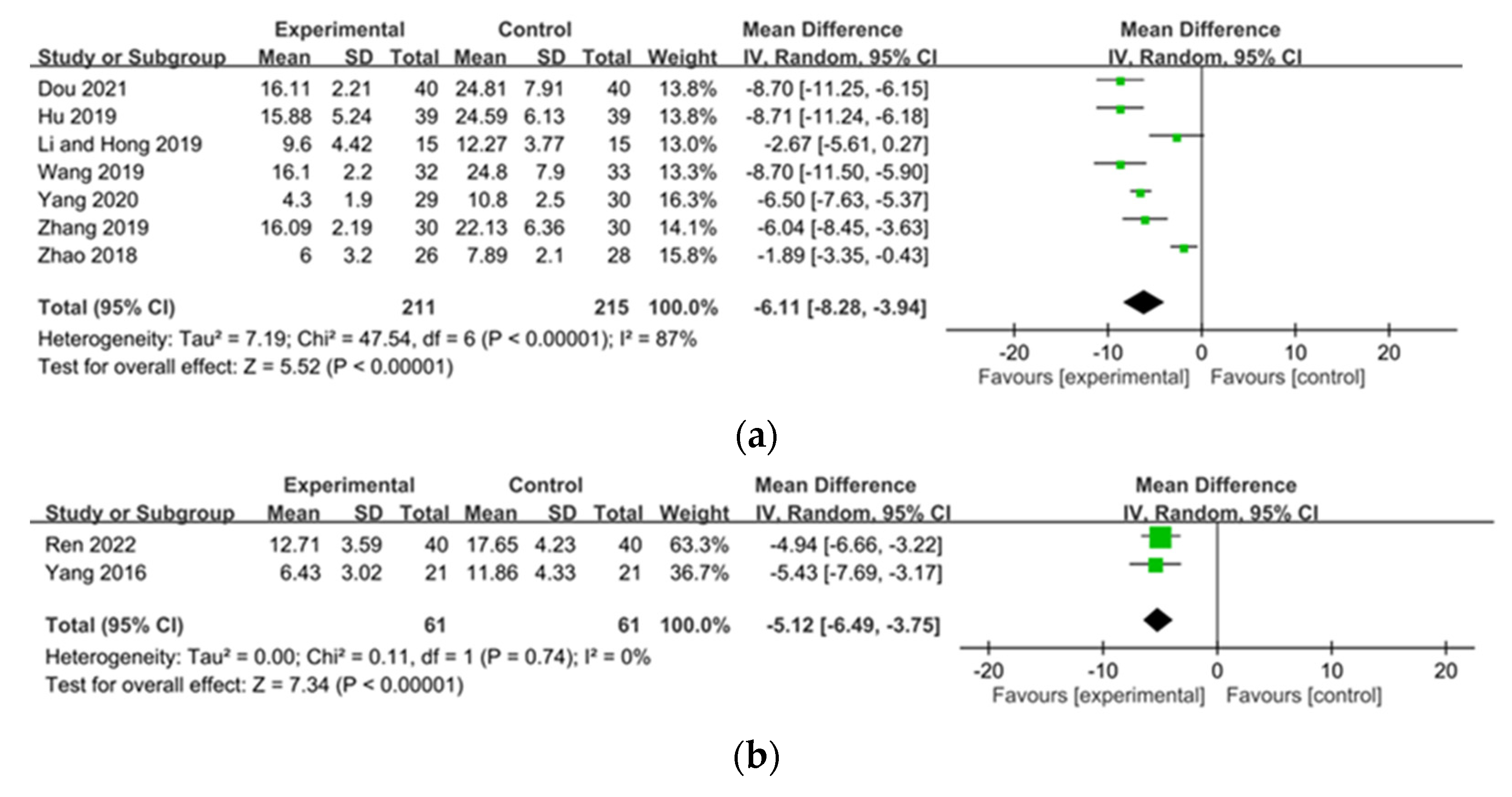
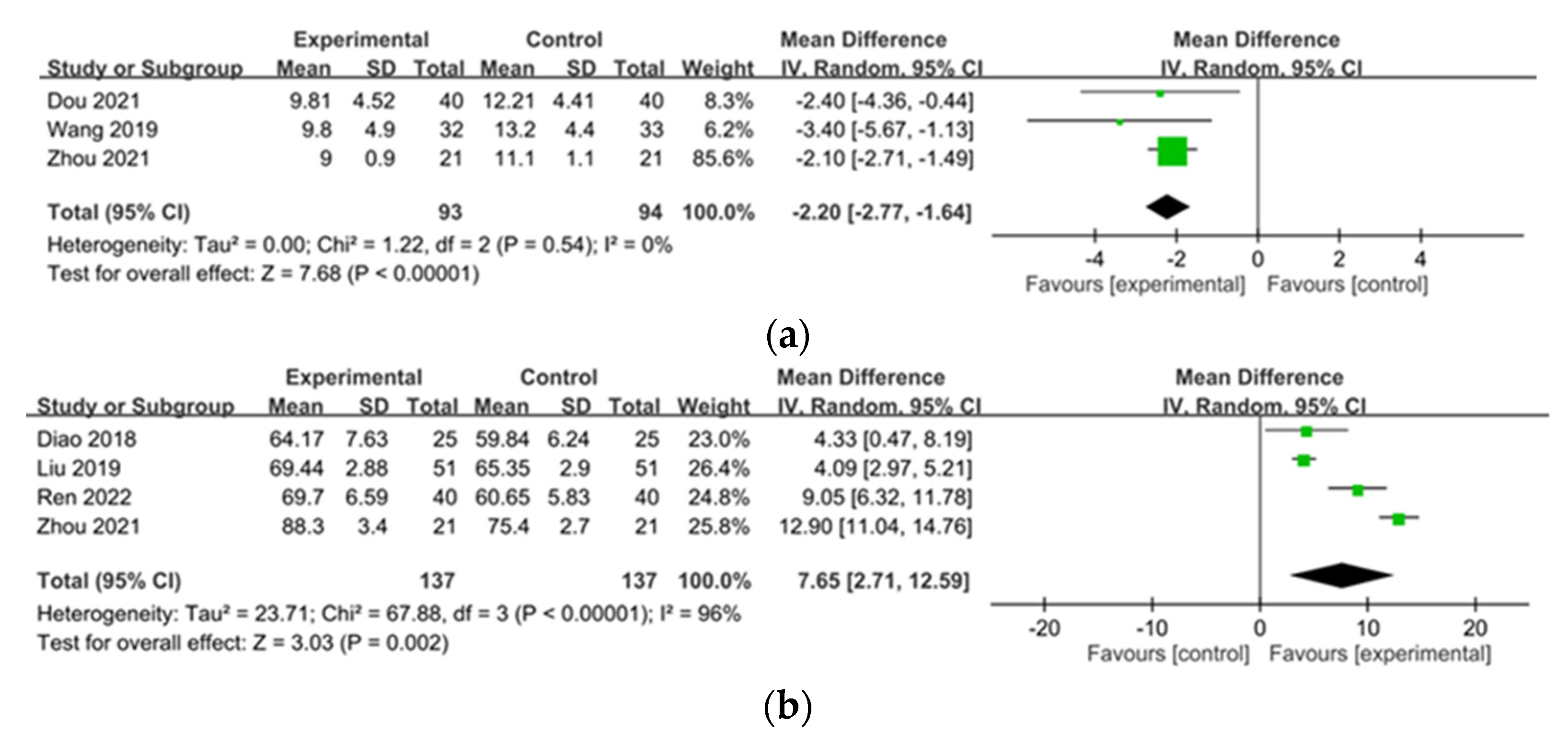
2.3.3. Pittsburgh Sleep Quality Index (PSQI), Quality of Life (QOL)
2.4. Secondary Outcomes—Effects of Chinese Herbal Medicine on Laboratory Parameters
2.5. Adverse Drug Reactions
2.6. Publication Bias
2.7. Quality of Evidence
3. Discussion
4. Materials and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Simonsen, E.; Komenda, P.; Lerner, B.; Askin, N.; Bohm, C.; Shaw, J.; Tangri, N.; Rigatto, C. Treatment of uremic pruritus: A systematic review. Am. J. Kidney Dis. 2017, 70, 638–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satti, M.Z.; Arshad, D.; Javed, H.; Shahroz, A.; Tahir, Z.; Ahmed, M.M.H.; Kareem, A. Uremic pruritus: Prevalence and impact on quality of life and depressive symptoms in hemodialysis patients. Cureus 2019, 11, e5178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attia, E.A.; Hassan, A.A. Uremic pruritus pathogenesis, revisited. Arab. J. Nephrol. Transplant. 2014, 7, 91–96. [Google Scholar]
- Duque, M.I.; Thevarajah, S.; Chan, Y.H.; Tuttle, A.B.; Freedman, B.I.; Yosipovitch, G. Uremic pruritus is associated with higher kt/v and serum calcium concentration. Clin. Nephrol. 2006, 66, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Makhlough, A.; Emadi, N.; Sedighi, O.; Khademloo, M.; Bicmohamadi, A.R. Relationship between serum intact parathyroid hormone and pruritus in hemodialysis patients. Iran. J. Kidney Dis. 2013, 7, 42–46. [Google Scholar]
- Shirazian, S.; Kline, M.; Sakhiya, V.; Schanler, M.; Moledina, D.; Patel, C.; Hazzan, A.; Fishbane, S. Longitudinal predictors of uremic pruritus. J. Ren. Nutr. 2013, 23, 428–431. [Google Scholar] [CrossRef]
- Ozen, N.; Cinar, F.I.; Askin, D.; Mut, D. Uremic pruritus and associated factors in hemodialysis patients: A multi-center study. Kidney Res. Clin. Pract. 2018, 37, 138–147. [Google Scholar] [CrossRef] [Green Version]
- Schricker, S.; Kimmel, M. Unravelling the pathophysiology of chronic kidney disease-associated pruritus. Clin. Kidney J. 2021, 14, i23–i31. [Google Scholar] [CrossRef]
- Virga, G.; Visentin, I.; La Milia, V.; Bonadonna, A. Inflammation and pruritus in haemodialysis patients. Nephrol. Dial. Transplant. 2002, 17, 2164–2169. [Google Scholar] [CrossRef] [Green Version]
- Kimmel, M.; Alscher, D.M.; Dunst, R.; Braun, N.; Machleidt, C.; Kiefer, T.; Stülten, C.; van der Kuip, H.; Pauli-Magnus, C.; Raub, U.; et al. The role of micro-inflammation in the pathogenesis of uraemic pruritus in haemodialysis patients. Nephrol. Dial. Transplant. 2006, 21, 749–755. [Google Scholar] [CrossRef] [Green Version]
- Malekmakan, L.; Malekmakan, A.; Sayadi, M.; Pakfetrat, M.; Sepaskhah, M.; Roozbeh, J. Association of high-sensitive c-reactive protein and dialysis adequacy with uremic pruritus. Saudi J. Kidney Dis. Transplant. 2015, 26, 890–895. [Google Scholar]
- Zhao, J.H.; Zhu, Q.S.; Li, Y.W.; Wang, L.L. Determinants of the intensity of uremic pruritus in patients receiving maintenance hemodialysis: A cross-sectional study. PLoS ONE 2021, 16, e0245370. [Google Scholar] [CrossRef] [PubMed]
- Suseł, J.; Batycka-Baran, A.; Reich, A.; Szepietowski, J.C. Uraemic pruritus markedly affects the quality of life and depressive symptoms in haemodialysis patients with end-stage renal disease. Acta Derm.-Venereol. 2014, 94, 276–281. [Google Scholar] [CrossRef]
- Lu, P.H.; Tai, Y.C.; Yu, M.C.; Lin, I.H.; Kuo, K.L. Western and complementary alternative medicine treatment of uremic pruritus: A literature review. Tzu Chi Med. J. 2021, 33, 350–358. [Google Scholar] [PubMed]
- Vila, T.; Gommer, J.; Scates, A.C. Role of gabapentin in the treatment of uremic pruritus. Ann. Pharmacother. 2008, 42, 1080–1084. [Google Scholar] [CrossRef] [PubMed]
- Church, M.K.; Church, D.S. Pharmacology of antihistamines. Indian J. Dermatol. 2013, 58, 219–224. [Google Scholar] [CrossRef]
- Gilchrest, B.A.; Rowe, J.W.; Brown, R.S.; Steinman, T.I.; Arndt, K.A. Relief of uremic pruritus with ultraviolet phototherapy. N. Engl. J. Med. 1977, 297, 136–138. [Google Scholar] [CrossRef]
- Yeam, C.T.; Yo, T.E.; Tan, Y.L.C.; Liew, A.; Seng, J.J.B. Complementary and alternative medicine therapies for uremic pruritus—A systematic review of randomized controlled trials. Complement. Ther. Med. 2021, 56, 102609. [Google Scholar] [CrossRef]
- Wang, J.J.; Ren, K.; Zhou, K. Jiebiao qufengzhiyang particles in treatment of uremic pruritus. Chin. J. New Drugs Clin. Remedies 2010, 29, 691–693. [Google Scholar]
- Luo, J.P.; Tang, C.Q. Chinese medicine treatment in maintenance hemodialysis patients skin pruritus 19 cases. J. Pract. Tradit. Chin. Intern. Med. 2010, 24, 97–98. [Google Scholar]
- Zhang, L.; Bao, X.X.; Jian, C.P. Clinical observation of yang yin qing xin treatment in hemodialysis patients with skin pruritus. Mod. J. Intrgrated Tradit. Chin. West. Med. 2011, 20, 27–28. [Google Scholar]
- Li, P. Clinical observation of chinese medicine treatment in hemodialysis patients with refractory skin pruritus. Med. Inf. 2015, 28, 258. [Google Scholar]
- Wang, H.J.; Zhang, R.H.; Fu, W.L. Treatment of shengyang xiehuo decoction in 40 patients with uremic pruritus. Guangming J. Chin. Med. 2016, 31, 825–827. [Google Scholar]
- Wu, F.X. Clinical observation on 30 cases of uremic pruritus treated with jiawei jiedu huoxue decoction. China Mod. Med. 2016, 23, 153–155. [Google Scholar]
- Xie, C.L. Clinical effect of jiawei siwu decoction in treatment of dialysis patients with refractory pruritus: A clinical analysis of 48 cases. Hunan J. Tradtional Chin. Med. 2016, 32, 12–14. [Google Scholar]
- Li, S.T.; Hong, Y.C.; Huang, S.X.; Weng, Z.M. A clinical study on treating pruritus in hemodialysis patients with danggui yinzi plus blood perfusion. Clin. J. Chin. Med. 2019, 11, 79–81. [Google Scholar]
- Wu, Q.X. Clinical Observation of Wushe Rongpi Decoction on Hemodialysis Patients with Pruritus of Blood Deficiency, Wind Dryness and Blood Stasis. Master’s Thesis, Fujian University of Traditional Chinese Medicine, Fuzhou, China, 2019. [Google Scholar]
- Hsu, Q.T. Clinical Study of Danggui Yinzi Addition and Subtration on Pruritus of Skin in Maintenance Hemodialysis Patients with Blood Deficiency and Wind Dryness. Master’s Thesis, Zhejiang Chinese Medical University, Hangzhou, China, 2020. [Google Scholar]
- Li, Q.N. Clinical effect of mahuang lianqiao chixiaodou decoction in patients with uremic pruritus. Guide China Med. 2020, 18, 181. [Google Scholar]
- Wong, Y.F. Clinical Observation of Taohong Danggui Yinzi for the Treatment on Hemodialysis Patients with Pruritus of Blood Deficiency, Wind Dryness and Blood Stasis. Master’s Thesis, Fujian University of Traditional Chinese Medicine, Fuzhou, China, 2021. [Google Scholar]
- Ren, D.Y. The effects of the xiaofeng zhiyang granules plus hemodialysis on uremia skin itching and its influence on calcium and phosphorus metabolism. Clin. J. Chin. Med. 2022, 14, 95–98. [Google Scholar]
- Liu, S.J. Clinical Observation of Treating the Skin Itching of Chronic Renal Failure (Qi Deficency and Blood Stasis Syndrome) with Yiqihuoxue Method. Master’s Thesis, Chengdu University of Traditional Chinese Medicine, Chengdu, China, 2013. [Google Scholar]
- Lu, P. Clinical observation on treatment of chronic renal failure skin pruritus by toxin-eliminating and itch-relieving therapy. Master’s Thesis, Chengdu University of Traditional Chinese Medicine, Chendu, China, 2015. [Google Scholar]
- Zhao, R. Clinical Study on the Treatment of the Skin Itching of Chronic Renal Failure (Spleen and Kidney Deficiency and Turbid Toxin Syndrome) with Qingjiangxiezhuo Method. Master’s Thesis, Shandong University of Traditional Chinese Medicine, Jinan, China, 2018. [Google Scholar]
- Zhang, W.Y. The clinical efficacy of yiqi huoxue qufeng method in treating pruritus in ckd4–5 non-dialysis patients with spleen-kidney-qi deficiency and blood stasis. Master’s Thesis, Guangxi University of Chinese Medicine, Nanning, China, 2019. [Google Scholar]
- Yang, Y.L. The Influence of Niaoduqing Particle on Uremic Pruritus in Maintenance Hemodialysis Patients. Master’s Thesis, Hubei University of Chinese Medicine, Wuhan, China, 2016. [Google Scholar]
- Sun, J.K.; Chen, J. Hemodialysis for uremic patients with niaoduqing inflammation and itch of skin effect. Mod. Med. Health Res. 2018, 2, 1–4. [Google Scholar]
- Guo, X.W.; Li, X.; Guo, W.J. Study on the efficacy of niaoduqing granules in treating pruritus and removing blood toxin in hemodialysis patients. J. Eng. Clin. Med. 2019, 26, 485–486. [Google Scholar]
- Yu, D.; Li, L.Z.; Zhang, S.Y. Clinical effect of niaoduqing particle combined with high-flux hemodialysis in the treatment of patients with uremic pruritus. Pract. J. Clin. Med. 2017, 14, 204–205. [Google Scholar]
- Cao, Y.G. Clinical observation of niaoduquing granule combined with high flux hemodialysis in treating uremic pruritus. Chin. Med. Mod. Distance Educ. China 2019, 17, 117–118. [Google Scholar]
- Kun, D.Z.; Yu, S.J.; Li, M. The feasibility of niaoduqing granule in adjunctive treatment of uremic pruritus. World Latest Med. Inf. 2019, 19, 182–183. [Google Scholar]
- Li, X.; Guo, X.W. The feasibility of niaoduqing granule in adjuvant treatment of uremic pruritus. Jilin Med. J. 2019, 40, 91–92. [Google Scholar]
- Chen, X.; Li, L.J.; Wu, D. Uremic clearance combined with high-flux hemodialysis on uremia pruritus. China Pharm. 2020, 29, 63–65. [Google Scholar]
- Xi, M.M. Clinical observation of niaoduqing granules combined with high-flux hemodialysis in treating uremic skin pruritus. Guide China Med. 2021, 19, 112–113. [Google Scholar]
- Li, Y. Feasibility of niaoduqing granules in the auxillary treatment of uremia skin pruritus. World Latest Med. Inf. 2021, 21, 473–474. [Google Scholar]
- Wang, F.; Zhang, P.K.; Zhang, Y.X. Observation of chinese herbal medicine combined with hemodialysis and hemoperfusion in treating skin pruritus. Chin. J. Mod. Drug Appl. 2015, 9, 239–240. [Google Scholar]
- Zhang, G.S.; Zhu, G.L.; Hou, X.J.; Zhang, P.K. Touxie zhiyang decoction to treat pruritus in patients receiving maintenance hemodialysis therapy. China Health Stand. Manag. 2015, 6, 139–140. [Google Scholar]
- Zhang, Y.X.; Zhang, G.S.; Li, R.; Wang, F. Clinic study of touxie zhiyang decoction in treatment of pruritus patients with maintenance hemodialysis. Acta Chin. Med. 2016, 31, 718–721. [Google Scholar]
- Diao, Y.J.; Deng, P.; Hu, L. Clinical efficacy of touxie jiedu zhiyang decoction in treatment of pruritus patients with maintenance hemodialysis. J. China Prescr. Drug 2018, 16, 113. [Google Scholar]
- Shi, W.L. Effect of touxie zhiyang decoction on skin itching in patients with maintenance hemodialysis. Syst. Med. 2019, 4, 86–88. [Google Scholar]
- Chen, J. Effect evaluation of touxie jiedu zhiyang decoction on skin pruritus of maintenance hemodialysis patients. J. Pract. Tradit. Chin. Intern. Med. 2020, 34, 110–111. [Google Scholar]
- Liu, H. The value of yangxue runfu yin in improving pruritus symptoms of hemodialysis patients complicated with pruritus. Chin. J. Dial. Artif. Organs 2015, 26, 11–12. [Google Scholar]
- Hu, T.F. Clincal effect of modified yangxue runfu yin in maintenance hemodialysis patients with xue xu feng zao type of uremic pruritus. World Latest Med. Inf. 2019, 19, 178–179. [Google Scholar]
- Wang, J.T.; Li, S.J.; Ruan, S.W.; Qiu, Y.L.; Zhang, W.J. Modified yangxue runfu yin treatment in 32 patients with xue xu feng zao type of uremic pruritus. Fujian J. Tradit. Chin. Med. 2019, 50, 13–14, 17. [Google Scholar]
- Dou, L.Y. Efficacy of modified yangxue runfu yin in hemodialysis patients with xue xu feng zao type of uremic pruritus. Mod. Med. Health Res. 2021, 5, 23–25. [Google Scholar]
- Zhu, X.L.; Xu, W.F.; Ye, M.H. Chinese medicine combined with western medicine treatment in 17 hemodialysis patients with uremic pruritus. Chin. J. Integr. Tradit. West. Med. 2004, 24, 74. [Google Scholar]
- He, G.S. Chinese medicine combined with western medicine treatment in 20 hemodialysis patients with uremic pruritus. J. Pract. Tradit. Chin. Med. 2006, 22, 547. [Google Scholar]
- Wang, W.H.; Wang, J.J.; Xie, Y.Q.; Li, X.Z. Effect of xiaoyang particles and hemoperfusion in maintenance hemodialysis patients with pruritus. China Health Care Nutr. 2013, 5, 2582–2583. [Google Scholar]
- Ge, J. Clinical research on clinical effect of treating itchy skin of uremia patients with xiaofeng zhiyang particles, loratadine tablets and hematodialysis. Chin. Arch. Tradit. Chin. Med. 2018, 36, 1497–1499. [Google Scholar]
- Tang, L.J.; Wang, S.J.; Zhao, M.; Chen, D. Treatment of self-made zhiyang decoction combined with gabapentin in maintenance hemodialysis patients with skin pruritus. Cardiovasc. Dis. J. Integr. Tradit. Chin. West. Med. 2018, 6, 151–152. [Google Scholar]
- Liu, S.J.; Huang, L.Y.; Wu, B.X. Clinical effect of cetrizine combined with jingfu zhiyang particles in hemodialysis patients with uremic pruritus. J. North Pharm. 2019, 16, 65–66. [Google Scholar]
- Fan, Z.Z. Effect of touxie jiedu zhiyang decoction on clinical symptoms and qol score of skin pruritus in maintenance hemodialysis patients. J. Pract. Tradit. Chin. Intern. Med. 2020, 34, 15–17. [Google Scholar]
- Yang, Y.J.; Yang, S.L. Clinical observation of combined artificial kidney combined with traditional chinese medicine in the treatment of uremia with refractory skin itch. Chin. Community Dr. 2020, 36, 128–129. [Google Scholar]
- Zhao, Y. Effect of Shenhuangliangyue Lotion Combined with Siwu Decoction on Skin Pruritus of Maintenance Hemodialysis Patients. Master’s Thesis, Hunan University of Chinese Medicine, Hunan, China, 2020. [Google Scholar]
- Jin, F.H.; Qin, Z.H.; Pan, P.Q.; Kong, C.W. Clinical observation on high-throughput hemodialysis combined with oral administration of traditional chinese medicine in the treatment of skin pruritus in patients with hemodialysis. Chin. Med. Mod. Distance Educ. China 2021, 19, 141–143. [Google Scholar]
- Wang, X.G.; Pi, L.F.; Jiang, J.X.; Li, Y.M.; Zhang, X.Y. Clinical observation of feng xue qing yin combined with hemodialysis therapy in end stage renal disease patients with skin pruritus. Res. Intergrated Tradit. Chin. West. Med. 2021, 13, 396–397, 401. [Google Scholar]
- Wu, F.X.; Gao, Y. Clinical observation on modified qufeng decoction in the treatment of skin pruritus in maintenance hemodialysis. Guangming J. Chin. Med. 2021, 36, 3645–3647. [Google Scholar]
- Zhou, Y.; Ye, H.L.; Huang, Z.Z.; Duo, A.P.; Zhou, Y.Q. Efficacy of hemodialysis combined with chinese herbal medicine in hemodialysis patients with refractory skin pruritus. J. Color. Anal Surg. 2021, 27, 53–54. [Google Scholar]
- Xue, W.; Zhao, Y.; Yuan, M.; Zhao, Z. Chinese herbal bath therapy for the treatment of uremic pruritus: Meta-analysis of randomized controlled trials. BMC Complement. Altern. Med. 2019, 19, 103. [Google Scholar] [CrossRef]
- Lu, P.H.; Keng, J.L.; Kuo, K.L.; Wang, Y.F.; Tai, Y.C.; Kuo, C.Y. An apriori algorithm-based association rule analysis to identify herb combinations for treating uremic pruritus using chinese herbal bath therapy. Evid.-Based Complement. Altern. Med. 2020, 2020, 8854772. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, M.H.; Yang, G.; Huh, Y.; Kim, S.H.; Yang, W.M. Effects of topical application of astragalus membranaceus on allergic dermatitis. Immunopharmacol. Immunotoxicol. 2013, 35, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.O.; Rhubarb. Drugs and Lactation Database (lactmed); National Library of Medicine (US): Bethesda, MD, USA, 2006. [Google Scholar]
- Zhang, Z.H.; Wei, F.; Vaziri, N.D.; Cheng, X.L.; Bai, X.; Lin, R.C.; Zhao, Y.Y. Metabolomics insights into chronic kidney disease and modulatory effect of rhubarb against tubulointerstitial fibrosis. Sci. Rep. 2015, 5, 14472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, D.; Chen, Y.; Hou, X.; Xu, J.; Mu, X.; Chen, W. Influence of paeonia lactiflora roots extract on camp-phosphodiesterase activity and related anti-inflammatory action. J. Ethnopharmacol. 2011, 137, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Chen, Z.; Li, M.; Zhang, Y.; Xu, S.; Huang, H.; Wu, X.; Zheng, X. Herbal pair huangqin-baishao: Mechanisms underlying inflammatory bowel disease by combined system pharmacology and cell experiment approach. BMC Complement. Med. Ther. 2020, 20, 292. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.T.; Kuan, Y.C.; Chang, H.H.; Sheu, F. Molecular cloning of a poria cocos protein that activates th1 immune response and allays th2 cytokine and ige production in a murine atopic dermatitis model. J. Agric. Food Chem. 2014, 62, 2861–2871. [Google Scholar] [CrossRef]
- Buyanravjikh, S.; Han, S.; Lee, S.; Jeong, A.L.; Ka, H.I.; Park, J.Y.; Boldbaatar, A.; Lim, J.S.; Lee, M.S.; Yang, Y. Cryptotanshinone inhibits ige-mediated degranulation through inhibition of spleen tyrosine kinase and tyrosine-protein kinase phosphorylation in mast cells. Mol. Med. Rep. 2018, 18, 1095–1103. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Choi, Y.Y.; Kim, M.H.; Han, J.M.; Lee, J.E.; Kim, E.H.; Hong, J.; Kim, J.; Yang, W.M. Topical application of angelica sinensis improves pruritus and skin inflammation in mice with atopic dermatitis-like symptoms. J. Med. Food 2016, 19, 98–105. [Google Scholar] [CrossRef]
- Park, G.; Moon, B.C.; Ryu, S.M.; Kim, W.J.; Lim, H.S. Cicadidae periostracum attenuates atopic dermatitis symptoms and pathology via the regulation of nlrp3 inflammasome activation. Oxidative Med. Cell. Longev. 2021, 2021, 8878153. [Google Scholar] [CrossRef]
- Yang, J.S.; Wu, C.C.; Lee, H.Z.; Hsieh, W.T.; Tang, F.Y.; Bau, D.T.; Lai, K.C.; Lien, J.C.; Chung, J.G. Suppression of the tnf-alpha level is mediated by gan-lu-yin (traditional chinese medicine) in human oral cancer cells through the nf-kappa b, akt, and erk-dependent pathways. Environ. Toxicol. 2016, 31, 1196–1205. [Google Scholar] [CrossRef]
- Xue, P.; Wang, Y.; Zeng, F.; Xiu, R.; Chen, J.; Guo, J.; Yuan, P.; Liu, L.; Xiao, J.; Lu, H.; et al. Paeonol suppresses solar ultraviolet-induced skin inflammation by targeting t-lak cell-originated protein kinase. Oncotarget 2017, 8, 27093–27104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swarna, S.S.; Aziz, K.; Zubair, T.; Qadir, N.; Khan, M. Pruritus associated with chronic kidney disease: A comprehensive literature review. Cureus 2019, 11, e5256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, M.K.; Elshahid, A.R.; El Baz, T.Z.; Elazab, R.M.; Elhoseiny, S.A.; Elsaie, M.L. Impact of uraemic pruritus on quality of life among end stage renal disease patients on dialysis. J. Clin. Diagn. Res. 2016, 10, WC01–WC05. [Google Scholar] [CrossRef] [PubMed]
- Xie, Q.; Hu, N.; Chen, Y. Chronic kidney disease-associated pruritus significantly impacts on quality of life of patients on haemodialysis and associates with increased levels of serum calcium and phosphorus. Postgrad. Med. J. 2021, 98, e16. [Google Scholar] [CrossRef]
- Xiong, W.; He, F.F.; You, R.Y.; Xiong, J.; Wang, Y.M.; Zhang, C.; Meng, X.F.; Su, H. Acupuncture application in chronic kidney disease and its potential mechanisms. Am. J. Chin. Med. 2018, 46, 1169–1185. [Google Scholar] [CrossRef]
- Kim, K.H.; Lee, M.S.; Kim, T.H.; Kang, J.W.; Choi, T.Y.; Lee, J.D. Acupuncture and related interventions for symptoms of chronic kidney disease. Cochrane Database Syst. Rev. 2016, 2016, Cd009440. [Google Scholar] [CrossRef]
- Feng, Q.; Wan, Y.; Jiang, C.; Wang, C.; Wei, Q.; Zhao, Q.; Yao, J. [Mechanisms and effects of chinese herbal medicine delaying progression of chronic renal failure]. China J. Chin. Mater. Med. 2011, 36, 1122–1128. [Google Scholar]
- Dou, C.; Wan, Y.; Sun, W.; Zhagn, H.; Chen, J.; Shui, G.; Yao, J. [Mechanism of chinese herbal medicine delaying progression of chronic kidney disease]. China J. Chin. Mater. Med. 2009, 34, 939–943. [Google Scholar]
- Chen, K.Z.; Shi, J.L.; Lü, M.Z.; He, Z.G.; Qin, R.A. [Effects of acupoint thread implantation and chinese herb on pth and tgf-beta1 in the rate of chronic renal failure]. Chin. Acupunct. Moxibustion 2006, 26, 511–514. [Google Scholar]
- Wang, Y.J.; He, L.Q.; Sun, W.; Lu, Y.; Wang, X.Q.; Zhang, P.Q.; Wei, L.B.; Cao, S.L.; Yang, N.Z.; Ma, H.Z.; et al. Optimized project of traditional chinese medicine in treating chronic kidney disease stage 3: A multicenter double-blinded randomized controlled trial. J. Ethnopharmacol. 2012, 139, 757–764. [Google Scholar] [CrossRef]
- Yin, J.Z.; Zhu, B.; Chen, H.Y.; Li, P.; Lu, J.C.; Yan, M.H. Meta-analysis of niaoduqing granules in the treatment of chronic kidney disease stages 3~5. Chin. J. Integr. Tradit. West. Nephrol. 2020, 21, 136–142. [Google Scholar]
- Zhang, H.W.; Lin, Z.X.; Xu, C.; Leung, C.; Chan, L.S. Astragalus (a traditional chinese medicine) for treating chronic kidney disease. Cochrane Database Syst. Rev. 2014, 10, Cd008369. [Google Scholar] [CrossRef]
- Liu, J.; Wang, Z.; Lin, J.; Li, T.; Guo, X.; Pang, R.; Dong, L.; Duan, M. Xuebijing injection in septic rats mitigates kidney injury, reduces cortical microcirculatory disorders, and suppresses activation of local inflammation. J. Ethnopharmacol. 2021, 276, 114199. [Google Scholar] [CrossRef] [PubMed]
- Xie, F.; Zhang, B.; Dai, S.; Jin, B.; Zhang, T.; Dong, F. Efficacy and safety of salvia miltiorrhiza (salvia miltiorrhiza bunge) and ligustrazine injection in the adjuvant treatment of early-stage diabetic kidney disease: A systematic review and meta-analysis. J. Ethnopharmacol. 2021, 281, 114346. [Google Scholar] [CrossRef] [PubMed]
- Oweis, A.O.; Al-Qarqaz, F.; Bodoor, K.; Heis, L.; Alfaqih, M.A.; Almomani, R.; Obeidat, M.A.; Alshelleh, S.A. Elevated interleukin 31 serum levels in hemodialysis patients are associated with uremic pruritus. Cytokine 2021, 138, 155369. [Google Scholar] [CrossRef]
- Ko, M.J.; Peng, Y.S.; Chen, H.Y.; Hsu, S.P.; Pai, M.F.; Yang, J.Y.; Wen, S.Y.; Jee, S.H.; Wu, H.Y.; Chiu, H.C. Interleukin-31 is associated with uremic pruritus in patients receiving hemodialysis. J. Am. Acad. Dermatol. 2014, 71, 1151–1159.e1151. [Google Scholar] [CrossRef]
- Haller, C. Hypoalbuminemia in renal failure: Pathogenesis and therapeutic considerations. Kidney Blood Press. Res. 2005, 28, 307–310. [Google Scholar] [CrossRef]
- Mukai, H.; Villafuerte, H.; Qureshi, A.R.; Lindholm, B.; Stenvinkel, P. Serum albumin, inflammation, and nutrition in end-stage renal disease: C-reactive protein is needed for optimal assessment. Semin. Dial. 2018, 31, 435–439. [Google Scholar] [CrossRef]
- Feng, M.; Yuan, W.; Zhang, R.; Fu, P.; Wu, T. Chinese herbal medicine huangqi type formulations for nephrotic syndrome. Cochrane Database Syst. Rev. 2013, 6, Cd006335. [Google Scholar] [CrossRef]
- Bolanos, C.G.; Pham, N.M.; Mair, R.D.; Meyer, T.W.; Sirich, T.L. Metabolomic analysis of uremic pruritus in patients on hemodialysis. PLoS ONE 2021, 16, e0246765. [Google Scholar] [CrossRef]
- Iseki, K.; Kohagura, K. Anemia as a risk factor for chronic kidney disease. Kidney International. Suppl. 2007, 72, S4–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Yu, S.; Jia, Q.; Chen, L.; Zhong, J.; Pan, Y.; Shen, P.; Shen, Y.; Wang, S.; Wei, Z.; et al. Niaoduqing granules relieve chronic kidney disease symptoms by decreasing renal fibrosis and anemia. Oncotarget 2017, 8, 55920–55937. [Google Scholar] [CrossRef] [Green Version]
- Bai, Y.S.; Zhou, C.Y.; Wang, J.Q. [Clinical observation on auxiliary treatment of hormone dependence dermatitis by shufeng liangxue decoction]. Chin. J. Integr. Tradit. West. Med. 2008, 28, 1121–1123. [Google Scholar]
- Ballotin, V.R.; Bigarella, L.G.; Brandão, A.B.M.; Balbinot, R.A.; Balbinot, S.S.; Soldera, J. Herb-induced liver injury: Systematic review and meta-analysis. World J. Clin. Cases 2021, 9, 5490–5513. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. Rob 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The prisma 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. Grade guidelines: 1. Introduction-grade evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Control/ Comparison a | Intervention/ Exposure a | No. of Patients (I/C) | Age (Years) | Dosage and Frequency | Duration | Pruritus Severity Assessment | Pruritus Score (Before → After) |
|---|---|---|---|---|---|---|---|---|
| Uremic clearance granule (UCG) | ||||||||
| Yang (2016) [36] | HD/HD + HP | UCG + HD/HD + HP | 21/21 | I: 51.48 (13.49) C: 51.67 (11.68) | 2.5 g, 2 times/d | 1 M | Kuypers PS | I: 11.57 (2.45) → 6.43 (3.02) C:11.67 (4.98) → 11.86 (4.33) |
| Sun et al. (2018) [37] | HD | UCG + HD | 54/54 | I: 54.12 (5.78) C: 54.08 (6.23) | 2.5 g, 2 times/d | NA | NA | I: 11.56 (3.02) → 5.12 (0.89) C:11.89 (3.12) → 8.28 (2.02) |
| Guo et al. (2019) [38] | HD | UCG + HD | 30/30 | I: 42.6 (3.2) C: 41.9 (3.4) | 5 g, 4 times/d | 3 M | NA | NA |
| Yu et al. (2017) [39] | High-flux HD | UCG + High-flux HD | 65/63 | I: 35-68 C: 36–70 | 5 g, 4 times/d | 3 M | VAS | I: 8.17 (1.94) → 4.28 (1.45) C: 8.21 (1.78) → 6.45 (1.91) |
| Cao (2019) [40] | High-flux HD | UCG + High-flux HD | 40/40 | I: 59.7 C: 59.8 | 5 g, 4 times/d | 2 M | NRS | I: 7.89 (1.31) → 3.10 (0.93) C: 7.95 (1.43) → 5.37 (1.02) |
| Kun et al. (2019) [41] | High-flux HD | UCG + High-flux HD | 23/23 | I: 45.3 (5.3) C: 46.1 (4.9) | 5 g, 4 times/d | 3 M | VAS | I: 8.13 (1.77) → 4.73 (1.41) C: 8.40 (2.07) → 6.28 (2.19) |
| Li et al. (2019) [42] | High-flux HD | UCG + High-flux HD | 52/50 | I: 47.2 (3.7) C: 46.7 (4.2) | 5 g, 4 times/d | 3 M | VAS | I: 8.18 (1.69) → 4.31 (1.52) C: 8.20 (1.96) → 6.38 (1.88) |
| Chen and Li et al. (2020) [43] | High-flux HD | UCG + High-flux HD | 50/50 | I: 65.72 (10.33) C: 64.12 (10.54) | 5 g, 4 times/d | 3 M | VAS | I: 7.62 (1.02) → 3.36 (1.06) C: 7.54 (0.98) → 5.53 (1.78) |
| 5-D Itch Scale | I: 17.37 (3.56) → 6.44 (1.59) C: 16.98(3.72) → 10.82 (2.31) | |||||||
| DLQI | I: 21.84 (5.53) → 8.36 (2.21) C: 21.54 (5.70)→10.55 (3.88) | |||||||
| Xi (2021) [44] | High-flux HD | UCG + High-flux HD | 58/58 | I: 47.88 (3.52) C: 47.79 (3.41) | 5 g, 4 times/d | NA | VAS | I: 7.21 (1.72) → 1.47 (0.34) C: 7.23 (1.71) → 3.48 (0.53) |
| Li (2021) [45] | High-flux HD | UCG + High-flux HD | 50/50 | I: 51.21 (1.92) C: 49.39 (2.74) | 5 g, 4 times/d | 14 Weeks | NA | I: 8.29 (1.70) → 4.42 (1.63) C: 8.31 (2.07) → 6.49 (1.99) |
| Touxie-Jiedu-Zhiyang Decoction | ||||||||
| Wang et al. (2015) [46] | HD | Touxie-Jiedu-Zhiyang Formula + HD | 39/39 | I: 49 (8) C: 52 (10) | 100 mL, 2 times/d | 3 M | VAS | I: 6.95 (1.47) → 2.31 (1.28) C: 6.87 (1.53) → 2.94 (1.35) |
| Zhang et al. (2015) [47] | Antihistamine + Emulsifying oil +HD | Touxie Zhiyang Decoction + HD | 45/45 | NA | NA | NA | VAS | I: 7.2 (2.1) → 2.9 (1.1) C: 7.3 (2.0) → 5.3 (1.9) |
| Zhang et al. (2016) [48] | HD | Touxie-Jiedu-Zhiyang Decoction + HD | 50/50 | I: 58.43 (12.82) C: 59.84 (13.76) | NA, 2 times/d | 3 M | VAS | NA |
| Diao et al. (2018) [49] | HD | Touxie-Jiedu-Zhiyang Decoction + HD | 25/25 | I: 62.3 (4.8) C: 61.6 (5.4) | NA, 2 times/d | 3 M | TCM new drug clinical research guideline | I: 2.51 (0.79) → 0.72 (0.34) C: 2.47 (0.82) → 1.88 (0.45) |
| Shi (2019) [50] | HD | Touxie-Jiedu-Zhiyang Decoction + HD | 20/20 | I: 45.24 (2.78) C: 45.21 (2.42) | NA, 2 times/d | 3 M | NA | NA |
| Chen (2020) [51] | HD | Touxie-Jiedu-Zhiyang Decoction + HD | 30/30 | I: 56.13 (7.45) C: 56.34 (7.12) | NA, 2 times/d | 3 M | VAS | I: 7.35 (2.13) → 2.96 (1.22) C: 7.32 (2.24) → 7.34 (2.37) |
| Yangxue-Runfu-Yin | ||||||||
| Liu (2015) [52] | Loratadine + HD | Yangxue-Runfu-Yin + Loratadine + HD | 20/20 | I: 57.65 (3.21) C: 56.81 (3.04) | NA | NA | NA | NA |
| Hu (2019) [53] | Loratadine + HD | Modified Yangxue-Runfu-Yin + HD | 39/39 | I: 61.05 (7.45) C: 60.86 (7.32) | 1 pack, 1 times/d | NA | Duo PS | I: 32.82 (4.33) → 15.88 (5.24) C: 32.15 (3.46) → 24.59 (6.13) |
| Wang et al. (2019) [54] | Loratadine + HD | Modified Yangxue-Runfu-Yin + HD | 32/33 | I: 50.7 (16.9) C: 52.2 (10.8) | 1 pack, 2 times/d | 2 M | VAS | I: 8.01(2.25) → 4.89(2.34) C: 7.73(1.53) → 5.40(2.87) |
| Duo PS | I: 31.20 (8.90) → 16.10 (2.20) C: 28.90 (9.20) → 24.80 (7.90) | |||||||
| Dou (2021) [55] | Desloratadine + HD | Modified Yangxue-Runfu-Yin + Desloratadine + HD | 40/40 | I: 53.56 (15.67) C: 53.62 (15.48) | 100 mL, 2 times/d | 0.5 M | VAS | I: 8.02 (2.26) → 3.88 (1.84) C: 7.74 (1.54) → 5.41 (2.61) |
| Duo PS | I: 31.21 (8.91) → 16.11 (2.21) C: 28.91 (9.21) → 24.81 (7.91) | |||||||
| Other Chinese herbal decoctions | ||||||||
| Zhu et al. (2004) [56] | Vit A. + Topical tincture + Cetirizine + HD | Yangxue Wensheng Decoction + Vit A. + Topical tincture + Cetirizine + HD | 17/15 | I: 70.2 (4.3) C: 71.6 (3.1) | NA, 2 times/d | 2 M | NA | NA |
| He (2006) [57] | Cetirizine + HD | Siwu Tang + Erzhi Wan + Cetirizine + HD | 20/18 | I: 50.5 C: 49.8 | NA, 2 times/d | 1 Week | NA | NA |
| Wang et al. (2013) [58] | HD/HD + HP | Xiaoyang Particles + HD | 21/22 | NA | 1 pack, 2 times/d | 2 M | VAS | I: 8.08 (1.02) → 5.05 (2.03) C: 7.89 (1.32) → 8.03 (1.42) |
| Ge (2018) [59] | Loratadine + HD | Xiaofeng Zhiyang Particles + Loratadine + HD | 45/45 | I: 56.03 (7.26) C: 55.24 (7.31) | 3 packs, 2 times/d | 0.5 M | TCM new drug clinical research guideline | I: 102.37 (16.87) → 40.32 (20.16) C: 99.26 (17.45) → 64.21 (25.02) |
| Tang et al. (2018) [60] | Gabapentin + HD | Zhiyang Decoction + Gabapentin + HD | 18/18 | I: 57.33 (16.45) C: 58.5 (16.21) | NA, 2 times/d | 1 M | TCM new drug clinical research guideline | NA |
| Liu et al. (2019) [61] | Cetirizine + HD | Jingfu Zhiyang Particles + Cetirizine + HD | 51/51 | I: 55.43 (11.02) C: 55.47 (11.01) | 6 g, 3 times/d | 1 M | Self-made PS questionnaire | I: 16.26 (4.49) → 6.01 (3.54) C: 16.33 (4.51) → 9.73 (3.55) |
| Fan (2020) [62] | Emulsifying oil + HD | Touxie-Jiedu-Zhiyang Decoction + Emulsifying oil + HD | 47/47 | I: 27.32 (2.13) C: 27.37 (2.42) | 500 mL, 2 times/d | NA | VAS | I: 7.31 (2.11) → 2.86 (1.08) C: 7.17 (2.16) → 5.46 (1.75) |
| Yang et al. (2020) [63] | HD + HP | Baifuzhi Weiliang Decoction + HD + HP | 29/30 | I: 49.1 (8.5) C: 49.5 (8.2) | 150 mL, 2 times/d | 3 M | Sergio PS | I: 30.9 (8.8) → 4.3 (1.9) C: 30.4 (8.6) → 10.8 (2.5) |
| Zhao (2020) [64] | HD | Siwu Decoction + HD | 30/30 | I: 61.17 (13.35) C: 58.83 (14.61) | NA, 2 times/d | 1 M | VAS | I: 6.23 (1.22) → 3.33 (1.42) C: 6.23 (1.63) → 4.47 (1.20) |
| Jin et al. (2021) [65] | High-flux HD | Mahuang Lianqiao Chixiaodou + Yiyifuzhi baijiang Decoction + High-flux HD | 30/30 | I: 53.26 (11.38) C: 53.26 (11.38) | 100 mL, 2 times/d | 6 M | Sergio PS | NA |
| Wang et al. (2021) [66] | HD + HP | Feng Xueqing Yin +HD + HP | 16/16 | I: 57.19 (5.79) C: 53.50 (9.14) | 1 pack,2 times/d | 1 M | VAS | I: 39.21 (2.50) → 17.08 (3.05) C: 39.91 (2.76) → 29.06 (2.86) |
| Wu et al. (2021) [67] | HD | Modified Qufeng Decoction + HD | 36/35 | I: 45.8 (8.4) C: 46.3 (8.6) | 100 mL, 2 times/d | 1 M | VAS | I: 27.65 (3.24) → 4.18 (1.20) C: 27.49 (3.20) → 12.84 (3.62) |
| Zhou et al. (2021) [68] | HD + HP | Chinese herbal medicine b + HD + HP | 21/21 | I: 43.59 (3.72) C: 43.46 (3.68) | 150 mL, 2 times/d | 2M | NA | NA |
| Other Chinese herbal decoctions—Control group with additional treatment | ||||||||
| Wang et al. (2010) [19] | Chlorphenamine + HD | Jiebiao Qufengzhiyang particles + HD | 28/30 | I: 47 (11) C: 46 (9) | 5 g, 2 times/d | 0.5 M | NA | NA |
| Luo et al. (2010) [20] | Calamine lotion + HD | Chinese herbal medicine c + HD | 19/19 | NA | 100 mL, 2 times/d | 3 M | NA | NA |
| Zhang et al. (2011) [21] | Loratadine + HD | Qingxin Lianxi In + HD | 33/30 | I: 59.7 (12.4) C: 60.9 (11.7) | 50 mL, 2 times/d | 20 Days | VAS | I: 8.75 (2.61) → 4.41 (3.12) C: 8.59 (2.86) → 6.46 (3.46) |
| Li (2015) [22] | Loratadine + HD | Modified Siwu Decoction + HD | 20/20 | I: 49.2 (1.2) C: 50.1 (1.5) | NA, 3 times/d | 2 M | VAS | NA |
| Wang et al. (2016) [23] | Charcoal Tablets + HD | Shengyang Xiehuo Decoction + HD | 40/40 | NA | 100 mL, 3 times/d | 1 M | Criteria of diagnosis and therapeutic effect of TCM diseases and syndromes | NA |
| Wu (2016) [24] | Cetirizine + HD | Modified Jiedu Huoxue Decoction + HD | 30/30 | I: 45.8 (5.1) C: 44.6 (5.5) | 100 mL, 3 times/d | 1 M | VAS | I: 6.69 (1.57) → 2.07 (0.62) C: 6.75 (1.53) → 4.11 (0.80) |
| Xie (2016) [25] | HD + HP | Modified Siwu Decoction + HD | 48/48 | I: 43.26 (8.37) C: 44.15 (9.25) | 100 mL, 3 times/d | 2 M | Criteria of diagnosis and therapeutic effect of TCM diseases and syndromes | I: 25.63 (4.55) → 9.06 (4.32) C: 25.87 (5.06) → 17.63 (4.35) |
| Li and Hong et al. (2019) [26] | HD + HP | Danggui Yinzi + HD | 15/15 | I: 50.62 (28.52) C: 47.22 (20.13) | 100 mL, 2 times/d | 1 M | Sergio PS | I: 27.07 (8.17) → 9.60 (4.42) C: 25.60 (7.68) → 12.27 (3.77) |
| Wu (2019) [27] | Loratadine + HD | Wushe Rongpi Decoction + HD | 33/33 | I: 70 C: 71 | 50 mL, 2 times/d | 2 M | VAS | I: 6.33 (1.81) → 2.64 (1.54) C: 6.30 (1.83) → 3.85 (1.84) |
| Hsu (2020) [28] | Loratadine + HD | Modified Danggui Yinzi + HD | 35/35 | I: 54.83 (11.40) C: 58.43 (12.08) | 100 mL, 2 times/d | 2 M | VAS | I: 6.17 (1.98) → 3.57 (1.93) C: 6.37 (2.20) → 4.69 (2.10) |
| Li et al. (2020) [29] | Calamine lotion + HD | Mahuang Lianqiao Chixiaodou decoction + HD | 31/31 | I: 59.3 (8.6) C: 59.6 (8.9) | NA | 0.5 M | Li’s pruritus scale | I: 4.0 (0.9) → 1.9 (0.3) C: 4.1 (0.8) → 2.8 (0.4) |
| Wong (2021) [30] | Loratadine + HD | Taohong Danggui Yinzi + HD | 32/32 | I: 61.82 (11.58) C: 63.45 (11.99) | 50 mL, 2 times/d | 2 M | VAS | I: 6.46 (1.57) → 2.18 (1.18) C: 6.58 (1.73) → 4.10 (1.18) |
| Ren (2022) [31] | Loratadine + HD | Xiaofeng Zhiyang granules + HD | 40/40 | I: 52.32 (11.19) C: 52.37 (11.26) | 18 g, 2 times/d | 1 M | Kuypers PS | I: 22.17 (4.66) → 12.71 (3.59) C: 22.22 (4.88) → 17.65 (4.23) |
| Patients with uremic pruritus without dialysis | ||||||||
| Liu (2013) [32] | CT | Buyanghuanwu Tang + CT | 18/17 | I: 42.22 (9.64) C: 40.59 (9.51) | 100 mL, 3 times/d | 1 M | Modified Duo PS | NA |
| Lu (2015) [33] | CT | Modified JieDu ZhiYang Decoction + CT | 16/14 | I: 55.50 (11.38) C: 49.75 (14.89) | NA | 1 M | NA | I: 4.43 (1.16) → 2.71 (0.99) C: 4.25 (1.24) → 4.13 (1.36) |
| Zhao (2018) [34] | CT | Qingjiangxiezhuo decoction + CT | 26/28 | I: 51.62 (9.64) C: 49.75 (7.73) | 200 mL, 2 times/d | 2 M | Modified Duo PS | I: 8.38 (1.86) → 6.00 (3.20) C: 8.57 (1.64) → 7.89 (2.10) |
| Zhang (2019) [35] | CT + TCM Patent Prescription | Yishen Huoxue Decoction + CT + TCM Patent Prescription | 30/30 | I: 54.37 (12.66) C: 55.53 (12.01) | 75 mL, 2 times/d | 2 M | VAS | I: 6.79 (1.49) → 1.93 (0.43) C: 6.45 (1.32) → 4.25 (0.70) |
| Study (Year) | Overall Effectiveness | Pittsburgh Sleep Quality Index (PSQI) (Before → After) | Quality of Life (QOL) (Before → After) | |||||
| Uremic clearance granule (UCG) | ||||||||
| Yang (2016) [36] | NA | NA | NA | |||||
| Sun et al. (2018) [37] | NA | NA | NA | |||||
| Guo et al. (2019) [38] | I: 27/30 C: 19/30 | NA | NA | |||||
| Yu et al. (2017) [39] | I: 49/65 C: 36/63 | NA | NA | |||||
| Cao (2019) [40] | I: 38/40 C: 32/40 | NA | NA | |||||
| Kun et al. (2019) [41] | I: 21/23 C: 16/23 | NA | NA | |||||
| Li et al. (2019) [42] | I: 39/52 C: 28/50 | NA | NA | |||||
| Chen and Li et al. (2020) [43] | I: 42/50 C: 33/50 | NA | NA | |||||
| Xi (2021) [44] | I: 56/58 C: 45/58 | NA | NA | |||||
| Li (2021) [45] | I: 41/50 C: 29/50 | NA | NA | |||||
| Touxie-Jiedu-Zhiyang Decoction | ||||||||
| Wang et al. (2015) [46] | I: 35/39 C: 27/39 | NA | NA | |||||
| Zhang et al. (2015) [47] | NA | NA | NA | |||||
| Zhang et al. (2016) [48] | NA | NA | NA | |||||
| Diao et al. (2018) [49] | I: 23/25 C: 15/25 | NA | I: 34.85 (11.92) → 64.17 (7.63) C: 35.04 (12.65) → 59.84 (6.24) | |||||
| Shi (2019) [50] | I: 20/20 C: 16/20 | NA | NA | |||||
| Chen (2020) [51] | NA | NA | NA | |||||
| Yangxue-Runfu-Yin | ||||||||
| Liu (2015) [52] | NA | NA | NA | |||||
| Hu (2019) [53] | NA | NA | NA | |||||
| Wang et al. (2019) [54] | NA | I: 14.70 (6.10) → 9.80 (4.90) C: 14.50 (5.30) → 13.20 (4.40) | NA | |||||
| Dou (2021) [55] | I: 39/40 C: 32/40 | I: 14.71 (6.11) → 9.81 (4.52) C: 14.51 (5.31) → 12.21 (4.41) | NA | |||||
| Other Chinese herbal decoctions | ||||||||
| Zhu et al. (2004) [56] | I: 16/17 C: 14/15 | NA | NA | |||||
| He (2006) [57] | I: 19/20 C: 11/18 | NA | NA | |||||
| Wang et al. (2013) [58] | NA | NA | NA | |||||
| Ge (2018) [59] | I: 41/45 C: 33/45 | NA | NA | |||||
| Tang et al. (2018) [60] | NA | NA | NA | |||||
| Liu et al. (2019) [61] | I: 48/51 C: 39/51 | NA | I: 55.85 (2.71) → 69.44 (2.88) C: 56.01 (3.76) → 65.35 (2.90) | |||||
| Fan (2020) [62] | NA | NA | I: 21.54 (2.34) → 52.16 (2.47) C: 21.43 (2.16) → 41.38 (2.43) | |||||
| Yang et al. (2020) [63] | I: 28/29 C: 26/30 | NA | NA | |||||
| Zhao (2020) [64] | I: 16/30 C: 8/30 | NA | NA | |||||
| Jin et al. (2021) [65] | I: 23/30 C: 17/30 | NA | NA | |||||
| Wang et al. (2021) [66] | NA | NA | NA | |||||
| Wu et al. (2021) [67] | I: 34/36 C: 23/35 | NA | NA | |||||
| Zhou et al. (2021) [68] | I: 19/21 C: 16/21 | I: 15.5 (1.2) → 9.0 (0.9) C: 15.4 (1.2) → 11.1 (1.1) | I: 62.4 (3.3) → 88.3 (3.4) C: 62.4 (3.4) → 75.4 (2.7) | |||||
| Other Chinese herbal decoctions—Control group with additional treatment | ||||||||
| Wang et al. (2010) [19] | I: 24/28 C: 18/30 | NA | NA | |||||
| Luo et al. (2010) [20] | I: 17/19 C: 12/19 | NA | NA | |||||
| Zhang et al. (2011) [21] | I: 28/33 C: 17/30 | NA | NA | |||||
| Li (2015) [22] | I: 18/20 C: 17/20 | NA | NA | |||||
| Wang et al. (2016) [23] | I: 36/40 C: 27/40 | NA | NA | |||||
| Wu (2016) [24] | I: 27/30 C: 21/30 | NA | NA | |||||
| Xie (2016) [25] | I: 40/48 C: 29/48 | NA | NA | |||||
| Li and Hong et al. (2019) [26] | I: 11/15 C: 12/15 | NA | NA | |||||
| Wu (2019) [27] | I: 29/33 C: 21/33 | NA | NA | |||||
| Hsu (2020) [28] | I: 32/35 C: 22/35 | NA | NA | |||||
| Li et al. (2020) [29] | NA | NA | NA | |||||
| Wong (2021) [30] | I: 29/32 C: 20/32 | NA | NA | |||||
| Ren (2022) [31] | I: 39/40 C: 30/40 | NA | I: 52.80 (7.35) → 69.70 (6.59) C: 52.82 (7.28) → 60.65 (5.83) | |||||
| Patients with uremic pruritus without dialysis | ||||||||
| Liu (2013) [32] | I: 16/18 C: 6/17 | NA | NA | |||||
| Lu (2015) [33] | I: 12/14 C: 4/16 | NA | NA | |||||
| Zhao (2018) [34] | I: 13/26 C: 5/28 | NA | NA | |||||
| Zhang (2019) [35] | I: 25/30 C: 16/30 | NA | NA | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, P.-H.; Lai, C.-C.; Lin, I.-H.; Tsai, F.-M.; Lu, P.-H. Clinical Efficacy and Safety of Chinese Herbal Medicine in the Treatment of Uremic Pruritus: A Meta-Analysis of Randomized Controlled Trials. Pharmaceuticals 2022, 15, 1239. https://doi.org/10.3390/ph15101239
Lu P-H, Lai C-C, Lin I-H, Tsai F-M, Lu P-H. Clinical Efficacy and Safety of Chinese Herbal Medicine in the Treatment of Uremic Pruritus: A Meta-Analysis of Randomized Controlled Trials. Pharmaceuticals. 2022; 15(10):1239. https://doi.org/10.3390/ph15101239
Chicago/Turabian StyleLu, Ping-Hsun, Chien-Cheng Lai, I-Hsin Lin, Fu-Ming Tsai, and Po-Hsuan Lu. 2022. "Clinical Efficacy and Safety of Chinese Herbal Medicine in the Treatment of Uremic Pruritus: A Meta-Analysis of Randomized Controlled Trials" Pharmaceuticals 15, no. 10: 1239. https://doi.org/10.3390/ph15101239
APA StyleLu, P. -H., Lai, C. -C., Lin, I. -H., Tsai, F. -M., & Lu, P. -H. (2022). Clinical Efficacy and Safety of Chinese Herbal Medicine in the Treatment of Uremic Pruritus: A Meta-Analysis of Randomized Controlled Trials. Pharmaceuticals, 15(10), 1239. https://doi.org/10.3390/ph15101239