
Treatment Options for Troublesome Itch


Abstract
:1. Introduction
2. Pharmacotherapeutic Options for Itch
2.1. Antidepressants
2.2. Antineuralgics
2.3. Cyclosporine A
2.4. Antibiotics
2.5. Crotamiton
2.6. PDE4 Inhibitor
2.7. Botulinum Toxin A
2.8. Herbal Medicines
3. Other Therapeutic Options for Itch
3.1. Phototherapy
3.2. Acupuncture Therapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Ikoma, A. Updated Neurophysiology of Itch. Biol. Pharm. Bull. 2013, 36, 1235–1240. [Google Scholar] [CrossRef]
- Greaves, M.W. Antihistamines in Dermatology. Skin Pharmacol. Physiol. 2005, 18, 220–229. [Google Scholar] [CrossRef]
- Ikoma, A.; Steinhoff, M.; Ständer, S.; Yosipovitch, G.; Schmelz, M. The neurobiology of itch. Nat. Rev. Neurosci. 2006, 7, 535–547. [Google Scholar] [CrossRef]
- Paus, R.; Schmelz, M.; Bíró, T.; Steinhoff, M. Frontiers in pruritus research: Scratching the brain for more effective itch therapy. J. Clin. Investig. 2006, 116, 1174–1185. [Google Scholar] [CrossRef]
- Mettang, T.; Kremer, A.E. Uremic pruritus. Kidney Int. 2015, 87, 685–691. [Google Scholar] [CrossRef]
- Düll, M.M.; Kremer, A.E. Treatment of Pruritus Secondary to Liver Disease. Curr. Gastroenterol. Rep. 2019, 21, 48. [Google Scholar] [CrossRef]
- Iwamoto, S.; Tominaga, M.; Kamata, Y.; Kawakami, T.; Osada, T.; Takamori, K. Association Between Inflammatory Bowel Disease and Pruritus. Crohn Colitis 360 2020, 2, otaa012. [Google Scholar] [CrossRef]
- Bigliardi, P.L.; Tobin, D.J.; Gaveriaux-Ruff, C.; Bigliardi-Qi, M. Opioids and the skin-where do we stand? Exp. Dermatol. 2009, 18, 424–430. [Google Scholar] [CrossRef]
- Inan, S.; Dun, N.J.; Cowan, A. Nalfurafine prevents 5′-guanidinonaltrindole- and compound 48/80-induced spinal c-fos expression and attenuates 5′-guanidinonaltrindole-elicited scratching behavior in mice. Neuroscience 2009, 163, 23–33. [Google Scholar] [CrossRef]
- Simpson, E.L.; Bieber, T.; Guttman-Yassky, E.; Beck, L.A.; Blauvelt, A.; Cork, M.J.; Silverberg, J.I.; Deleuran, M.; Kataoka, Y.; Lacour, J.-P.; et al. Two Phase 3 Trials of Dupilumab versus Placebo in Atopic Dermatitis. N. Engl. J. Med. 2016, 375, 2335–2348. [Google Scholar] [CrossRef]
- Heinz, K.C.; Willems, D.; Hiligsmann, M. Economic evaluation of a JAK inhibitor compared to a monoclonal antibody for treatment of moderate-to-severe atopic dermatitis from a UK perspective. J. Med. Econ. 2022, 25, 491–502. [Google Scholar] [CrossRef]
- Blauvelt, A.; Teixeira, H.D.; Simpson, E.L.; Costanzo, A.; De Bruin-Weller, M.; Barbarot, S.; Prajapati, V.H.; Lio, P.; Hu, X.; Wu, T.; et al. Efficacy and Safety of Upadacitinib vs. Dupilumab in Adults With Moderate-to-Severe Atopic Dermatitis: A Randomized Clinical Trial. JAMA Dermatol. 2021, 157, 1047–1055. [Google Scholar] [CrossRef]
- Gunawan, A.; Harrington, P.; Garcia-Curto, N.; McLornan, D.; Radia, D.; Harrison, C. Ruxolitinib for the Treatment of Essential Thrombocythemia. HemaSphere 2018, 2, e56. [Google Scholar] [CrossRef]
- Conti, P.; Shaik-Dasthagirisaheb, Y.B. Mast Cell Serotonin Immunoregulatory Effects Impacting on Neuronal Function: Implications for Neurodegenerative and Psychiatric Disorders. Neurotox. Res. 2015, 28, 147–153. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Nagasawa, T.; Satoh, M.; Kuraishi, Y. Itch-associated response induced by intradermal serotonin through 5-HT2 receptors in mice. Neurosci. Res. 1999, 35, 77–83. [Google Scholar] [CrossRef]
- Akiyama, T.; Ivanov, M.; Nagamine, M.; Davoodi, A.; Carstens, M.I.; Ikoma, A.; Cevikbas, F.; Kempkes, C.; Buddenkotte, J.; Steinhoff, M.; et al. Involvement of TRPV4 in Serotonin-Evoked Scratching. J. Investig. Dermatol. 2016, 136, 154–160. [Google Scholar] [CrossRef]
- Zylicz, Z.; Krajnik, M.; van Sorge, A.A.; Costantini, M. Paroxetine in the treatment of severe non-dermatological pruritus: A randomized, controlled trial. J. Pain Symptom Manag. 2003, 26, 1105–1112. [Google Scholar] [CrossRef]
- Tefferi, A.; Fonseca, R. Selective serotonin reuptake inhibitors are effective in the treatment of polycythemia vera–associated pruritus. Blood 2002, 99, 2627. [Google Scholar] [CrossRef]
- Biondi, M.; Arcangeli, T.; Petrucci, R. Paroxetine in a Case of Psychogenic Pruritus and Neurotic Excoriations. Psychother. Psychosom. 2000, 69, 165–166. [Google Scholar] [CrossRef]
- Ständer, S.; Böckenholt, B.; Schürmeyer-Horst, F.; Weishaupt, C.; Heuft, G.; Schneider, T. Treatment of Chronic Pruritus with the Selective Serotonin Re-uptake Inhibitors Paroxetine and Fluvoxamine: Results of an Open-labelled, Two-arm Proof-of-concept Study. Acta Derm. Venereol. 2009, 89, 45–51. [Google Scholar] [CrossRef]
- Thébaut, A.; Habes, D.; Gottrand, F.; Rivet, C.; Cohen, J.; Debray, D.; Jacquemin, E.; Gonzales, E. Sertraline as an Additional Treatment for Cholestatic Pruritus in Children. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 431–435. [Google Scholar] [CrossRef]
- Hundley, J.L.; Yosipovitch, G. Mirtazapine for reducing nocturnal itch in patients with chronic pruritus: A pilot study. J. Am. Acad. Dermatol. 2004, 50, 889–891. [Google Scholar] [CrossRef]
- Andoh, T.; Gotoh, Y.; Kuraishi, Y. Milnacipran inhibits itch-related responses in mice through the enhancement of noradrenergic transmission in the spinal cord. J. Pharmacol. Sci. 2013, 123, 199–202. [Google Scholar] [CrossRef]
- Browning, J. Long-term efficacy of sertraline as a treatment for cholestatic pruritus in patients with primary biliary cirrhosis. Am. J. Gastroenterol. 2003, 98, 2736–2741. [Google Scholar] [CrossRef]
- Yrondi, A.; Fiori, L.M.; Frey, B.N.; Lam, R.W.; MacQueen, G.M.; Milev, R.; Müller, D.J.; Foster, J.; Kennedy, S.H.; Turecki, G. Association Between Side Effects and Blood microRNA Expression Levels and Their Targeted Pathways in Patients With Major Depressive Disorder Treated by a Selective Serotonin Reuptake Inhibitor, Escitalopram: A CAN-BIND-1 Report. Int. J. Neuropsychopharmacol. 2020, 23, 88–95. [Google Scholar] [CrossRef]
- Sadegzadeh, F.; Sakhaie, N.; Dehghany, R.; Adak, O.; Saadati, H. Effects of adolescent administration of fluoxetine on novel object recognition memory, anxiety-like behaviors, and hippocampal brain-derived neurotrophic factor level. Life Sci. 2020, 260, 118338. [Google Scholar] [CrossRef]
- Zhang, X.; Yin, Y.; Yue, L.; Gong, L. Selective Serotonin Reuptake Inhibitors Aggravate Depression-Associated Dry Eye Via Activating the NF-kappaB Pathway. Investig. Ophthalmol. Vis. Sci. 2019, 60, 407–419. [Google Scholar] [CrossRef]
- Krasowska, D.; Szymanek, M.; Schwartz, R.A.; Myśliński, W. Cutaneous effects of the most commonly used antidepressant medication, the selective serotonin reuptake inhibitors. J. Am. Acad. Dermatol. 2007, 56, 848–853. [Google Scholar] [CrossRef]
- Tominaga, M.; Takamori, K. Itch and nerve fibers with special reference to atopic dermatitis: Therapeutic implications. J. Dermatol. 2014, 41, 205–212. [Google Scholar] [CrossRef]
- Fehrenbacher, J.C.; Taylor, C.P.; Vasko, M.R. Pregabalin and gabapentin reduce release of substance P and CGRP from rat spinal tissues only after inflammation or activation of protein kinase C. Pain 2003, 105, 133–141. [Google Scholar] [CrossRef]
- Foroutan, N.; Etminan, A.; Nikvarz, N.; Abadi, M.S.S. Comparison of pregabalin with doxepin in the management of uremic pruritus: A randomized single blind clinical trial. Hemodial. Int. 2016, 21, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Cevikbas, F.; Steinhoff, M.; Ikoma, A. Role of Spinal Neurotransmitter Receptors in Itch: New Insights into Therapies and Drug Development. CNS Neurosci. Ther. 2010, 17, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Li, L.; Chen, S.R.; Chen, H.; Xie, J.D.; Sirrieh, R.E.; Maclean, D.M.; Zhang, Y.; Zhou, M.-H.; Jayaraman, V.; et al. The α2δ-1-NMDA Receptor Complex Is Critically Involved in Neuropathic Pain Development and Gabapentin Therapeutic Actions. Cell Rep. 2018, 22, 2307–2321. [Google Scholar] [CrossRef]
- Taylor, C.P.; Angelotti, T.; Fauman, E. Pharmacology and mechanism of action of pregabalin: The calcium channel α2–δ (alpha2–delta) subunit as a target for antiepileptic drug discovery. Epilepsy Res. 2007, 73, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Domon, Y.; Arakawa, N.; Inoue, T.; Matsuda, F.; Takahashi, M.; Yamamura, N.; Kai, K.; Kitano, Y. Binding Characteristics and Analgesic Effects of Mirogabalin, a Novel Ligand for the alpha2delta Subunit of Voltage-Gated Calcium Channels. J. Pharmacol. Exp. Ther. 2018, 365, 573–582. [Google Scholar] [CrossRef]
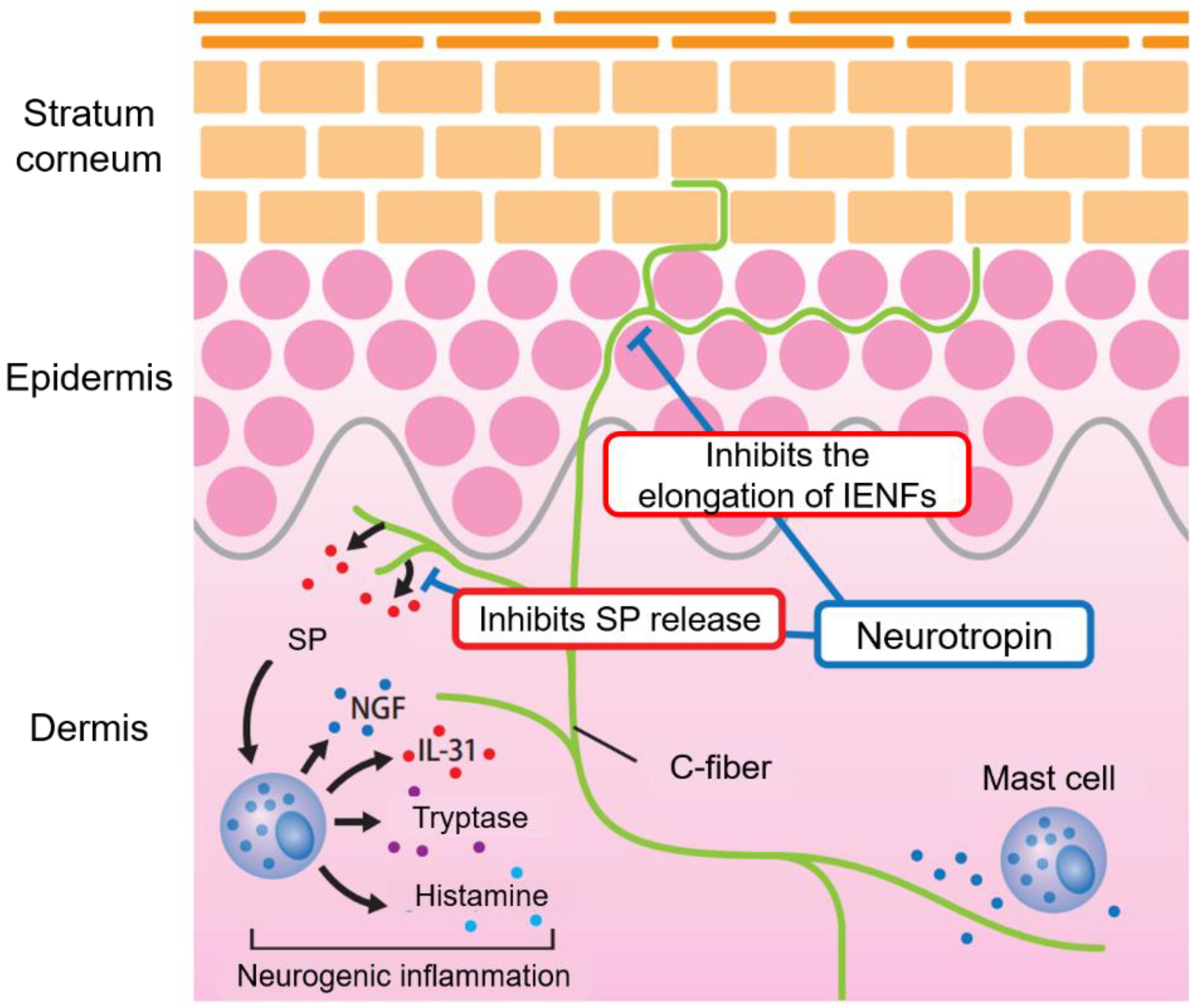
- Kamo, A.; Tominaga, M.; Matsuda, H.; Kina, K.; Kamata, Y.; Umehara, Y.; Ogawa, H.; Takamori, K. Neurotropin suppresses itch-related behavior in NC/Nga mice with atopic dermatitis-like symptoms. J. Dermatol. Sci. 2015, 81, 212–215. [Google Scholar] [CrossRef]
- Kamo, A.; Tominaga, M.; Taneda, K.; Ogawa, H.; Takamori, K. Neurotropin inhibits the increase in intraepidermal nerve density in the acetone-treated dry-skin mouse model. Clin. Exp. Dermatol. 2013, 38, 665–668. [Google Scholar] [CrossRef]
- Taneda, K.; Tominaga, M.; Tengara, S.; Ogawa, H.; Takamori, K. Neurotropin inhibits both capsaicin-induced substance P release and nerve growth factor-induced neurite outgrowth in cultured rat dorsal root ganglion neurones. Clin. Exp. Dermatol. 2009, 35, 73–77. [Google Scholar] [CrossRef]
- Schmitt, J.; Schmitt, N.; Meurer, M. Cyclosporin in the treatment of patients with atopic eczema? A systematic review and meta-analysis. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 606–619. [Google Scholar] [CrossRef]
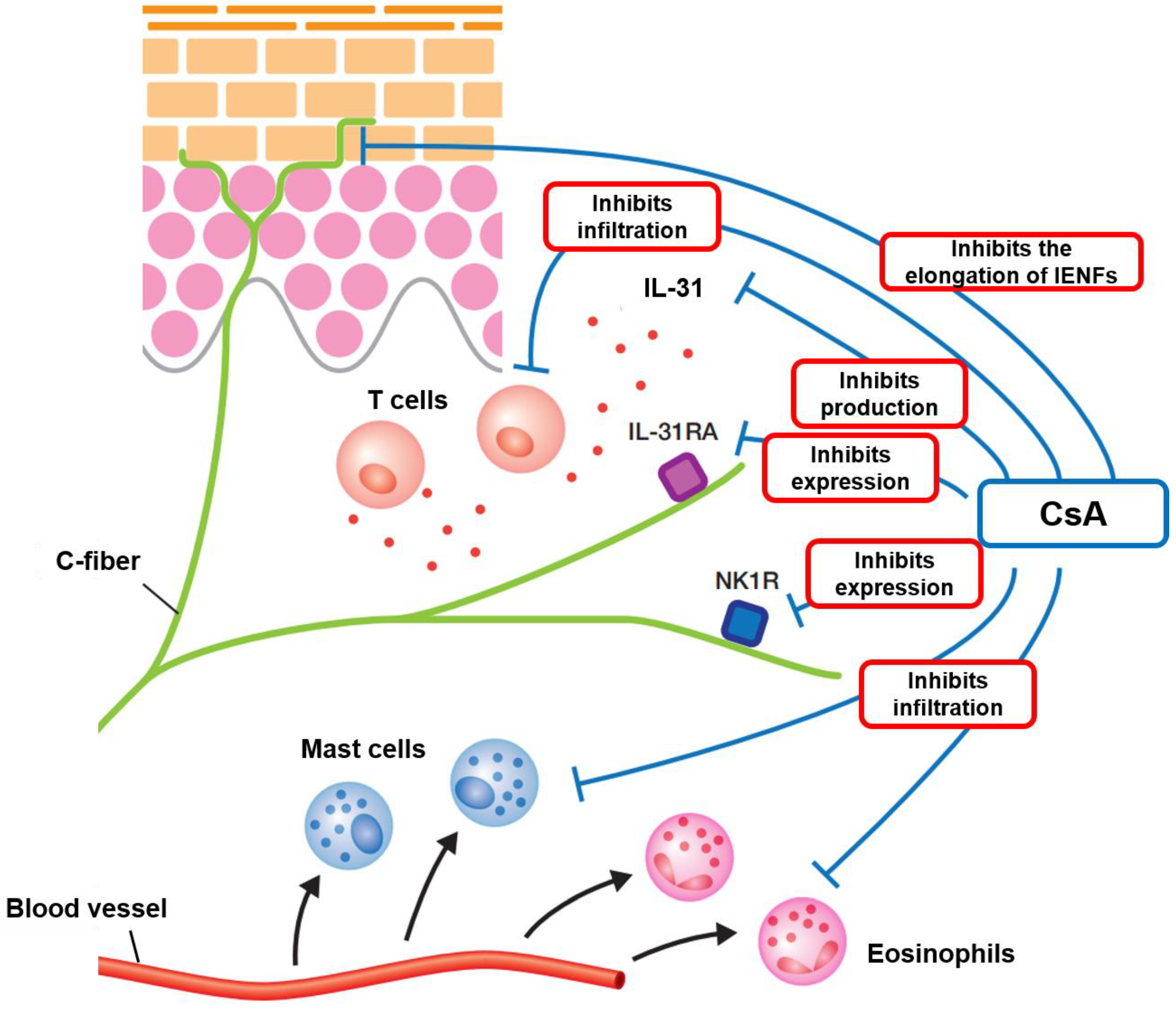
- Ko, K.; Tominaga, M.; Kamata, Y.; Umehara, Y.; Matsuda, H.; Takahashi, N.; Kina, K.; Ogawa, M.; Ogawa, H.; Takamori, K. Possible Antipruritic Mechanism of Cyclosporine A in Atopic Dermatitis. Acta Derm. Venereol. 2016, 96, 624–629. [Google Scholar] [CrossRef]
- Kabashima, K.; Irie, H. Interleukin-31 as a Clinical Target for Pruritus Treatment. Front. Med. 2021, 8, 638325. [Google Scholar] [CrossRef] [PubMed]
- Touw, C.; Roijen, L.H.-V.; Verboom, P.; Paul, C.; Rutten, F.; Finlay, A. Quality of life and clinical outcome in psoriasis patients using intermittent cyclosporin. Br. J. Dermatol. 2001, 144, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Catinean, A.; Neag, M.A.; Mitre, A.O.; Bocsan, C.I.; Buzoianu, A.D. Microbiota and Immune-Mediated Skin Diseases—An Overview. Microorganisms 2019, 7, 279. [Google Scholar] [CrossRef] [PubMed]
- Matsui, K.; Tamai, S.; Ikeda, R. Effects of Macrolide Antibiotics on Th1 Cell and Th2 Cell Development Mediated by Langerhans Cells. J. Pharm. Pharm. Sci. 2016, 19, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Matsui, K.; Nakamura, M.; Obana, N. Effects of Josamycin on Scratching Behavior in NC/Nga Mice with Atopic Dermatitis-Like Skin Lesions. Biol. Pharm. Bull. 2021, 44, 798–803. [Google Scholar] [CrossRef]
- Tamaki, K. Antipruritic Effect ofMacrolide Antibiotics. J. Dermatol. 2000, 27, 66–67. [Google Scholar]
- Moniaga, C.; Tominaga, M.; Takamori, K. Mechanisms and Management of Itch in Dry Skin. Acta Derm. Venereol. 2020, 100, adv00024. [Google Scholar] [CrossRef]
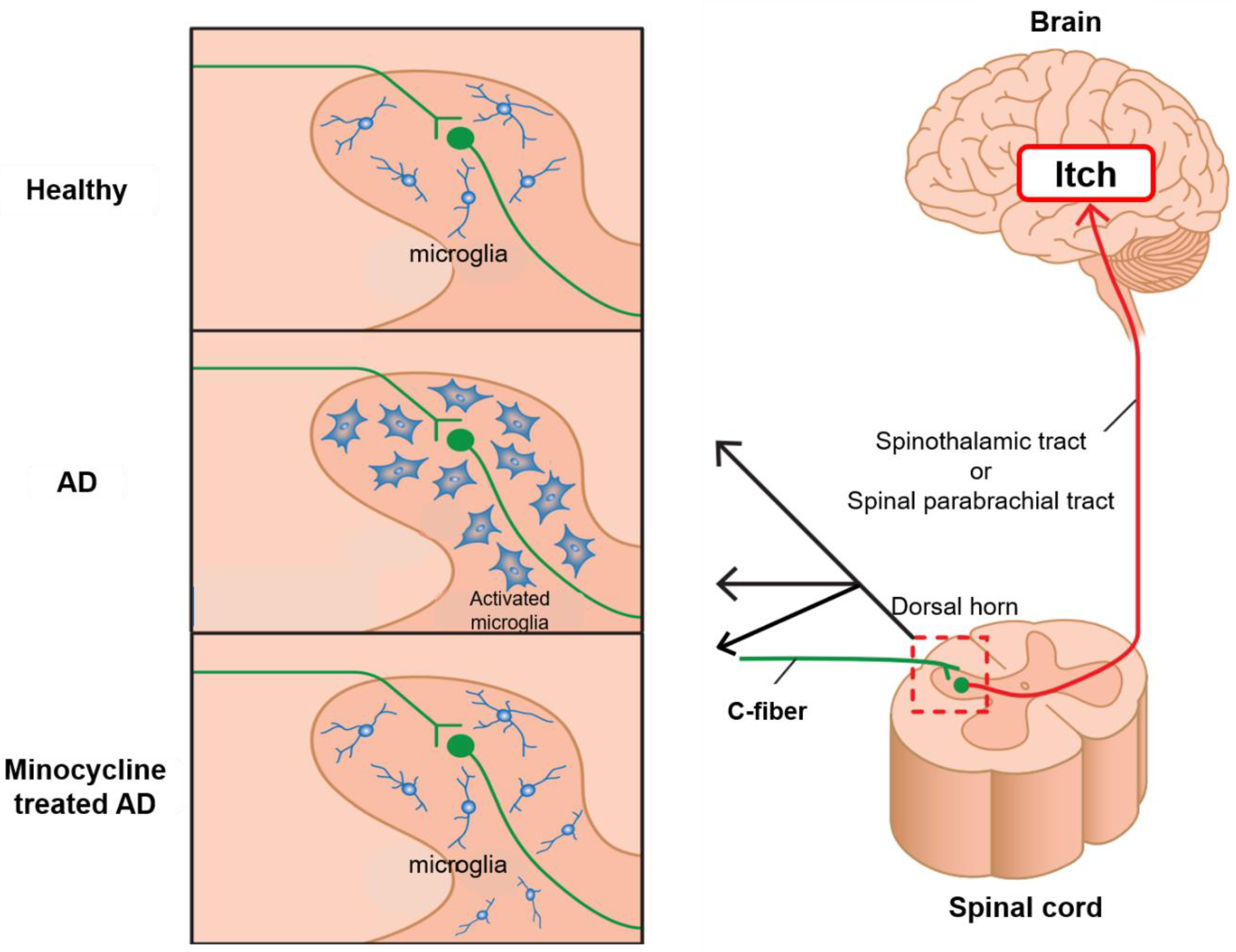
- Torigoe, K.; Tominaga, M.; Ko, K.C.; Takahashi, N.; Matsuda, H.; Hayashi, R.; Ogawa, H.; Takamori, K. Intrathecal Minocycline Suppresses Itch-Related Behavior and Improves Dermatitis in a Mouse Model of Atopic Dermatitis. J. Investig. Dermatol. 2016, 136, 879–881. [Google Scholar] [CrossRef]
- Sekine, R.; Satoh, T.; Takaoka, A.; Saeki, K.; Yokozeki, H. Anti pruritic effects of topical crotamiton, capsaicin, and a corticosteroid on pruritogen-induced scratching behavior. Exp. Dermatol. 2011, 21, 201–204. [Google Scholar] [CrossRef]
- Choi, D.-S.; Ji, Y.; Jang, Y.; Lee, W.-J.; Shim, W.-S. Crotamiton, an Anti-Scabies Agent, Suppresses Histamine- and Chloroquine-Induced Itch Pathways in Sensory Neurons and Alleviates Scratching in Mice. Biomol. Ther. 2020, 28, 569–575. [Google Scholar] [CrossRef]
- Kittaka, H.; Yamanoi, Y.; Tominaga, M. Transient receptor potential vanilloid 4 (TRPV4) channel as a target of crotamiton and its bimodal effects. Pflüg. Arch.-Eur. J. Physiol. 2017, 469, 1313–1323. [Google Scholar] [CrossRef] [PubMed]
- Tominaga, M.; Takamori, K. Peripheral itch sensitization in atopic dermatitis. Allergol. Int. 2022, 71, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Andoh, T.; Kuraishi, Y. Antipruritic mechanisms of topical E6005, a phosphodiesterase 4 inhibitor: Inhibition of responses to proteinase-activated receptor 2 stimulation mediated by increase in intracellular cyclic AMP. J. Dermatol. Sci. 2014, 76, 206–213. [Google Scholar] [CrossRef]
- Hanifin, J.M.; Ellis, C.; Frieden, I.J.; Fölster-Holst, R.; Gold, L.F.S.; Secci, A.; Smith, A.J.; Zhao, C.; Kornyeyeva, E.; Eichenfield, L.F. OPA-15406, a novel, topical, nonsteroidal, selective phosphodiesterase-4 (PDE4) inhibitor, in the treatment of adult and adolescent patients with mild to moderate atopic dermatitis (AD): A phase-II randomized, double-blind, placebo-controlled study. J. Am. Acad. Dermatol. 2016, 75, 297–305. [Google Scholar] [CrossRef]
- Saeki, H.; Kawashima, M.; Sugaya, S.; Oshiden, K.; Tsubouchi, H. Efficacy and safety of topical OPA-15406, a new phosphodiesterase 4 inhibitor, in Japanese patients with atopic dermatitis for 8 weeks: A phase 2, randomized, double-blind, placebo-controlled study. J. Dermatol. 2019, 46, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Saeki, H.; Baba, N.; Oshiden, K.; Abe, Y.; Tsubouchi, H. Phase 2, randomized, double-blind, placebo-controlled, 4-week study to evaluate the safety and efficacy of OPA-15406 (difamilast), a new topical selective phosphodiesterase type-4 inhibitor, in Japanese pediatric patients aged 2-14 years with atopic dermatitis. J. Dermatol. 2019, 47, 17–24. [Google Scholar] [PubMed]
- Samrao, A.; Berry, T.M.; Goreshi, R.; Simpson, E.L. A Pilot Study of an Oral Phosphodiesterase Inhibitor (Apremilast) for Atopic Dermatitis in Adults. Arch. Dermatol. 2012, 148, 890–897. [Google Scholar] [CrossRef] [PubMed]
- Farahnik, B.; Beroukhim, K.; Nakamura, M.; Abrouk, M.; Zhu, T.H.; Singh, R.; Lee, K.; Bhutani, T.; Koo, J.; Liao, W. Use of an oral phosphodiesterase-4 inhibitor (apremilast) for the treatment of chronic, severe atopic dermatitis: A case report. Dermatol. Online J. 2017, 23, 9. [Google Scholar] [CrossRef]
- Vossen, A.R.; van Doorn, M.B.; van der Zee, H.H.; Prens, E.P. Apremilast for moderate hidradenitis suppurativa: Results of a randomized controlled trial. J. Am. Acad. Dermatol. 2019, 80, 80–88. [Google Scholar] [CrossRef]
- Strand, V.; Fiorentino, D.; Hu, C.; Day, R.M.; Stevens, R.M.; Papp, K. Improvements in patient-reported outcomes with apremilast, an oral phosphodiesterase 4 inhibitor, in the treatment of moderate to severe psoriasis: Results from a phase IIb randomized, controlled study. Health Qual. Life Outcomes 2013, 11, 82. [Google Scholar] [CrossRef]
- Paul, C.; Cather, J.; Gooderham, M.; Poulin, Y.; Mrowietz, U.; Ferrandiz, C.; Crowley, J.; Hu, C.; Stevens, R.M.; Shah, K.; et al. Efficacy and safety of apremilast, an oral phosphodiesterase 4 inhibitor, in patients with moderate-to-severe plaque psoriasis over 52 weeks: A phase III, randomized controlled trial (ESTEEM 2). Br. J. Dermatol. 2015, 173, 1387–1399. [Google Scholar] [CrossRef] [PubMed]
- Sobell, J.; Foley, P.; Toth, D.; Mrowietz, U.; Girolomoni, G.; Goncalves, J.; Day, R.; Chen, R.; Yosipovitch, G. Effects of Apremilast on Pruritus and Skin Discomfort/Pain Correlate with Improvements in Quality of Life in Patients with Moderate to Severe Plaque Psoriasis. Acta Derm. Venereol. 2016, 96, 514–520. [Google Scholar] [CrossRef] [PubMed]
- Reich, K.; Gooderham, M.; Bewley, A.; Green, L.; Soung, J.; Petric, R.; Marcsisin, J.; Cirulli, J.; Chen, R.; Piguet, V. Safety and efficacy of apremilast through 104 weeks in patients with moderate to severe psoriasis who continued on apremilast or switched from etanercept treatment: Findings from the LIBERATE study. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Paller, A.S.; Tom, W.L.; Lebwohl, M.G.; Blumenthal, R.L.; Boguniewicz, M.; Call, R.S.; Eichenfield, L.F.; Forsha, D.W.; Rees, W.C.; Simpson, E.L.; et al. Efficacy and safety of crisaborole ointment, a novel, nonsteroidal phosphodiesterase 4 (PDE4) inhibitor for the topical treatment of atopic dermatitis (AD) in children and adults. J. Am. Acad. Dermatol. 2016, 75, 494–503.e6. [Google Scholar] [CrossRef] [PubMed]
- Yosipovitch, G.; Gold, L.; Lebwohl, M.; Silverberg, J.; Tallman, A.; Zane, L. Early Relief of Pruritus in Atopic Dermatitis with Crisaborole Ointment, A Non-steroidal, Phosphodiesterase 4 Inhibitor. Acta Derm. Venereol. 2018, 98, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Bissonnette, R.; Pavel, A.B.; Diaz, A.; Werth, J.L.; Zang, C.; Vranic, I.; Purohit, V.S.; Zielinski, M.A.; Vlahos, B.; Estrada, Y.D.; et al. Crisaborole and atopic dermatitis skin biomarkers: An intrapatient randomized trial. J. Allergy Clin. Immunol. 2019, 144, 1274–1289. [Google Scholar]
- Eichenfield, L.F.; Yosipovitch, G.; Stein Gold, L.F.; Kalabis, M.; Zang, C.; Vlahos, B.; Sanders, P.; Myers, D.E.; Bushmakin, A.G.; Paller, A.S.; et al. Improvement in disease severity and pruritus outcomes with crisaborole ointment, 2%, by baseline atopic dermatitis severity in children and adolescents with mild-to-moderate atopic dermatitis. Pediatr. Dermatol. 2020, 37, 1030–1037. [Google Scholar] [CrossRef]
- Spergel, J.M.; Blaiss, M.S.; Lio, P.; Kessel, A.; Cantrell, W.C.; Takiya, L.; Werth, J.L.; O’Connell, M.A.; Zang, C.; Cork, M.J. Efficacy and safety of crisaborole in patients with mild-to-moderate atopic dermatitis and other atopic comorbidities. Allergy Asthma Proc. 2021, 42, 425–431. [Google Scholar] [CrossRef]
- Furue, M.; Kitahara, Y.; Akama, H.; Hojo, S.; Hayashi, N.; Nakagawa, H.; The JAPANESE E6005 Study Investigators. Safety and efficacy of topical E6005, a phosphodiesterase 4 inhibitor, in Japanese adult patients with atopic dermatitis: Results of a randomized, vehicle-controlled, multicenter clinical trial. J. Dermatol. 2014, 41, 577–585. [Google Scholar] [CrossRef]
- Andoh, T.; Yoshida, T.; Kuraishi, Y. Topical E6005, a novel phosphodiesterase 4 inhibitor, attenuates spontaneous itch-related responses in mice with chronic atopy-like dermatitis. Exp. Dermatol. 2014, 23, 359–361. [Google Scholar] [CrossRef]
- Wakita, H.; Ohkuro, M.; Ishii, N.; Hishinuma, I.; Shirato, M. A putative antipruritic mechanism of the phosphodiesterase-4 inhibitor E6005 by attenuating capsaicin-induced depolarization of C-fibre nerves. Exp. Dermatol. 2015, 24, 215–216. [Google Scholar] [CrossRef] [PubMed]
- Saeki, H.; Ito, K.; Yokota, D.; Tsubouchi, H. Difamilast ointment in adult patients with atopic dermatitis: A phase 3 randomized, double-blind, vehicle-controlled trial. J. Am. Acad. Dermatol. 2022, 86, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Heckmann, M.; Heyer, G.; Brunner, B.; Plewig, G. Botulinum toxin type A injection in the treatment of lichen simplex: An open pilot study. J. Am. Acad. Dermatol. 2002, 46, 617–619. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, G.; Tidman, M. Botulinum A toxin and brachioradial pruritus. Br. J. Dermatol. 2011, 166, 1147. [Google Scholar] [CrossRef]
- Gharib, K.; Mostafa, A.; Elsayed, A. Evaluation of Botulinum Toxin Type A Injection in the Treatment of Localized Chronic Pruritus. J. Clin. Aesthet. Dermatol. 2020, 13, 12–17. [Google Scholar]
- Klager, S.; Kumar, M.G. Treatment of pruritus with botulinum toxin in a pediatric patient with Fox-Fordyce disease. Pediatr. Dermatol. 2021, 38, 950–951. [Google Scholar] [CrossRef]
- Gazerani, P.; Pedersen, N.; Drewes, A.; Arendt-Nielsen, L. Botulinum toxin type A reduces histamine-induced itch and vasomotor responses in human skin. Br. J. Dermatol. 2009, 161, 737–745. [Google Scholar] [CrossRef]
- Ramachandran, R.; Marino, M.J.; Paul, S.; Wang, Z.; Mascarenhas, N.L.; Pellett, S.; Johnson, E.A.; DiNardo, A.; Yaksh, T.L. A Study and Review of Effects of Botulinum Toxins on Mast Cell Dependent and Independent Pruritus. Toxins 2018, 10, 134. [Google Scholar] [CrossRef]
- Huang, S.-H.; Wu, K.-W.; Lo, J.-J.; Wu, S.-H. Synergic Effect of Botulinum Toxin Type-A and Triamcinolone Alleviates Scar Pruritus by Modulating Epidermal Hyperinnervation: A Preliminary Report. Aesthet. Surg. J. 2021, 41, NP1721–NP1731. [Google Scholar] [CrossRef]
- Tohda, C.; Sugahara, H.; Kuraishi, Y.; Komatsu, K. Inhibitory effect of Byakko-ka-ninjin-to on itch in a mouse model of atopic dermatitis. Phytother. Res. 2000, 14, 192–194. [Google Scholar] [CrossRef]
- Saeedi, M.; Morteza-Semnani, K.; Ghoreishi, M. The treatment of atopic dermatitis with licorice gel. J. Dermatol. Treat. 2003, 14, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Yamaguchi, T.; Funakushi, N.; Kuhara, T.; Fan, P.-S.; Ueki, R.; Suto, H.; Kase, Y.; Ikeda, S.; Ogawa, H. Oral administration of Yokukansan inhibits the development of atopic dermatitis-like lesions in isolated NC/Nga mice. J. Dermatol. Sci. 2009, 56, 37–42. [Google Scholar] [CrossRef]
- Cheng, H.-M.; Chiang, L.-C.; Jan, Y.-M.; Chen, G.-W.; Li, T.-C. The Efficacy and Safety of a Chinese Herbal Product (Xiao-Feng-San) for the Treatment of Refractory Atopic Dermatitis: A Randomized, Double-Blind, Placebo-Controlled Trial. Int. Arch. Allergy Immunol. 2010, 155, 141–148. [Google Scholar] [CrossRef]
- Yan, F.; Zhang, J.; Li, X.; Mo, X.; Liu, J.; Ye, S.; Lin, Y.; Qiu, X.; Lee, S.M.; Chen, D. Therapeutic Effects of Chinese Herbal Formula (PTQX) on NC/Nga Mice with Atopic Dermatitis-Like Skin Lesions. Evid.-Based Complement. Altern. Med. 2019, 2019, 8359252. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Chen, S.; Zhang, L.; Chen, G.; Chen, J. The Anti-Inflammatory and Anti-Pruritus Mechanisms of Huanglian Jiedu Decoction in the Treatment of Atopic Dermatitis. Front. Pharmacol. 2021, 12, 735295. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, A.-R.; Kim, H.S.; Kim, H.W.; Park, Y.H.; You, J.S.; Park, Y.M.; Her, E.; Kim, H.S.; Kim, Y.M.; et al. Rhamnus davurica leaf extract inhibits Fyn activation by antigen in mast cells for anti-allergic activity. BMC Complement. Altern. Med. 2015, 15, 80. [Google Scholar] [CrossRef]
- Nam, J.H.; Jung, H.W.; Chin, Y.W.; Yang, W.M.; Bae, H.S.; Kim, W.K. Spirodela polyrhiza extract modulates the activation of atopic dermatitis-related ion channels, Orai1 and TRPV3, and inhibits mast cell degranulation. Pharm. Biol. 2017, 55, 1324–1329. [Google Scholar] [CrossRef]
- Yang, N.-N.; Shi, H.; Yu, G.; Wang, C.-M.; Zhu, C.; Yang, Y.; Yuan, X.-L.; Tang, M.; Wang, Z.-L.; Gegen, T.; et al. Osthole inhibits histamine-dependent itch via modulating TRPV1 activity. Sci. Rep. 2016, 6, 25657. [Google Scholar] [CrossRef]
- Basnet, P.; Yasuda, I.; Kumagai, N.; Tohda, C.; Nojima, H.; Kuraishi, Y.; Komatsu, K. Inhibition of Itch-Scratch Response by Fruits of Cnidium monnieri in Mice. Biol. Pharm. Bull. 2001, 24, 1012–1015. [Google Scholar] [CrossRef]
- Andoh, T.; Al-Akeel, A.; Tsujii, K.; Nojima, H.; Kuraishi, Y. Repeated Treatment With the Traditional Medicine Unsei-in Inhibits Substance P-Induced Itch-Associated Responses Through Downregulation of the Expression of Nitric Oxide Synthase 1 in Mice. J. Pharmacol. Sci. 2004, 94, 207–210. [Google Scholar] [CrossRef]
- Meduri, N.B.; Vandergriff, T.; Rasmussen, H.; Jacobe, H. Phototherapy in the management of atopic dermatitis: A systematic review. Photodermatol. Photoimmunol. Photomed. 2007, 23, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Evers, A.W.M.; Kleinpenning, M.M.; Smits, T.; Boezeman, J.; Van De Kerkhof, P.; Kraaimaat, F.W.; Gerritsen, M.J.P. Itch and scratching as predictors of time to clearance of psoriasis with narrow-band ultraviolet B therapy. Br. J. Dermatol. 2009, 161, 542–546. [Google Scholar] [CrossRef] [PubMed]
- Baltas, E.; Csoma, Z.; Bodai, L.; Ignacz, F.; Dobozy, A.; Kemény, L. Treatment of atopic dermatitis with the xenon chloride excimer laser. J. Eur. Acad. Dermatol. Venereol. 2006, 20, 657–660. [Google Scholar] [CrossRef]
- Sidbury, R.; Davis, D.M.; Cohen, D.E.; Cordoro, K.M.; Berger, T.G.; Bergman, J.N.; Chamlin, S.L.; Cooper, K.D.; Feldman, S.R.; Hanifin, J.M.; et al. Guidelines of care for the management of atopic dermatitis: Section 3. Management and treatment with phototherapy and systemic agents. J. Am. Acad. Dermatol. 2014, 71, 327–349. [Google Scholar] [CrossRef] [PubMed]
- Juarez, M.C.; Grossberg, A.L. Phototherapy in the Pediatric Population. Dermatol. Clin. 2020, 38, 91–108. [Google Scholar] [CrossRef] [PubMed]
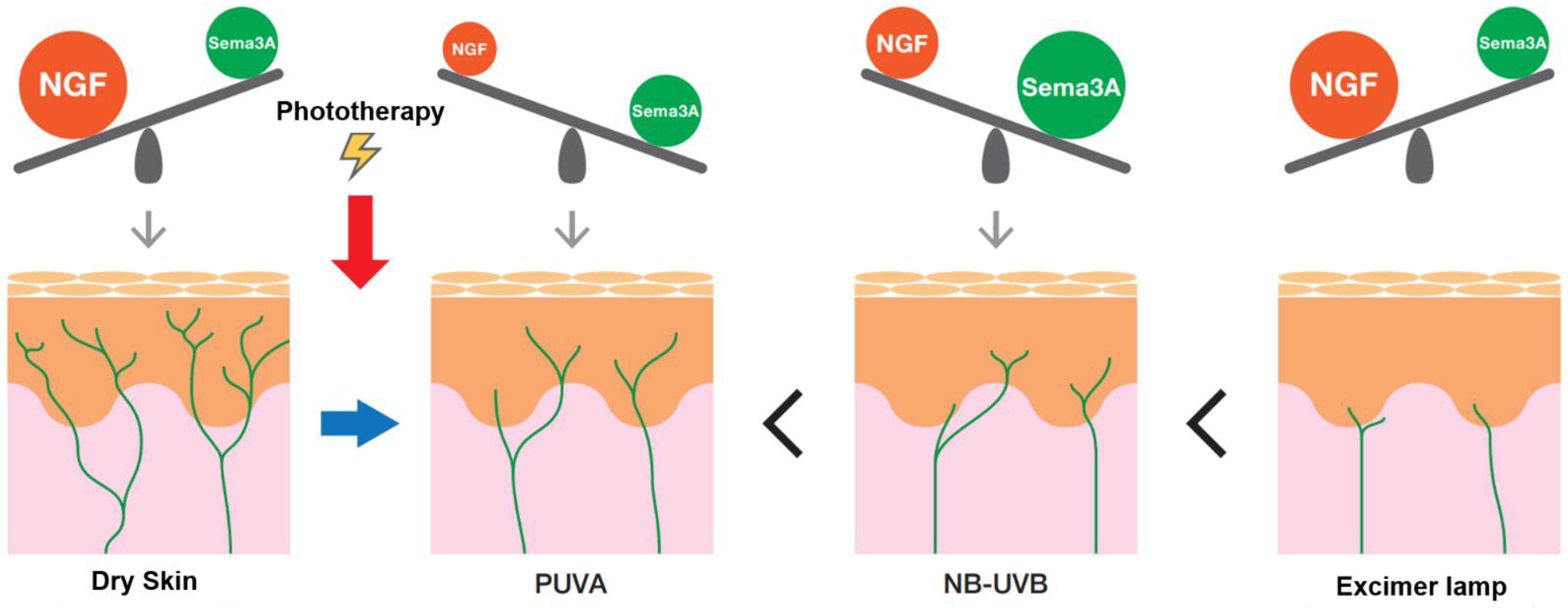
- Tominaga, M.; Tengara, S.; Kamo, A.; Ogawa, H.; Takamori, K. Psoralen-ultraviolet A therapy alters epidermal Sema3A and NGF levels and modulates epidermal innervation in atopic dermatitis. J. Dermatol. Sci. 2009, 55, 40–46. [Google Scholar] [CrossRef]
- Kamo, A.; Tominaga, M.; Tengara, S.; Ogawa, H.; Takamori, K. Inhibitory effects of UV-based therapy on dry skin-inducible nerve growth in acetone-treated mice. J. Dermatol. Sci. 2011, 62, 91–97. [Google Scholar] [CrossRef]
- Kamo, A.; Tominaga, M.; Kamata, Y.; Kaneda, K.; Ko, K.C.; Matsuda, H.; Kimura, U.; Ogawa, H.; Takamori, K. The Excimer Lamp Induces Cutaneous Nerve Degeneration and Reduces Scratching in a Dry-Skin Mouse Model. J. Investig. Dermatol. 2014, 134, 2977–2984. [Google Scholar] [CrossRef]
- Archier, E.; Devaux, S.; Castela, E.; Gallini, A.; Aubin, F.; Le Maître, M.; Aractingi, S.; Bachelez, H.; Cribier, B.; Joly, P.; et al. Carcinogenic risks of Psoralen UV-A therapy and Narrowband UV-B therapy in chronic plaque psoriasis: A systematic literature review. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 22–31. [Google Scholar] [CrossRef]
- Hearn, R.; Kerr, A.; Rahim, K.; Ferguson, J.; Dawe, R. Incidence of skin cancers in 3867 patients treated with narrow-band ultraviolet B phototherapy. Br. J. Dermatol. 2008, 159, 931–935. [Google Scholar] [CrossRef]
- Jung, D.-L.; Lee, S.-D.; Choi, I.-H.; Na, H.-S.; Hong, S.-U. Effects of electroacupuncture on capsaicin-induced model of atopic dermatitis in rats. J. Dermatol. Sci. 2014, 74, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Kim, Y.-K.; Yeom, M.; Lee, H.; Jang, H.; Park, H.-J.; Kim, K. Acupuncture improves symptoms in patients with mild-to-moderate atopic dermatitis: A randomized, sham-controlled preliminary trial. Complement. Ther. Med. 2018, 41, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Jiao, R.; Yang, Z.; Wang, Y.; Zhou, J.; Zeng, Y.; Liu, Z. The effectiveness and safety of acupuncture for patients with atopic eczema: A systematic review and meta-analysis. Acupunct. Med. 2020, 38, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Pfab, F.; Huss-Marp, J.; Gatti, A.; Fuqin, J.; Athanasiadis, G.I.; Irnich, D.; Raap, U.; Schober, W.; Behrendt, H.; Ring, J.; et al. Influence of acupuncture on type I hypersensitivity itch and the wheal and flare response in adults with atopic eczema–A blinded, randomized, placebo-controlled, crossover trial. Allergy 2009, 65, 903–910. [Google Scholar] [CrossRef]
- Pfab, F.; Kirchner, M.T.; Huss-Marp, J.; Schuster, T.; Schalock, P.C.; Fuqin, J.; Athanasiadis, G.I.; Behrendt, H.; Ring, J.; Darsow, U.; et al. Acupuncture compared with oral antihistamine for type I hypersensitivity itch and skin response in adults with atopic dermatitis: A patient- and examiner-blinded, randomized, placebo-controlled, crossover trial. Allergy 2012, 67, 566–573. [Google Scholar] [CrossRef]
- Napadow, V.; Li, A.; Loggia, M.L.; Kim, J.; Schalock, P.; Lerner, E.; Tran, T.-N.; Ring, J.; Rosen, B.R.; Kaptchuk, T.J.; et al. The Brain Circuitry Mediating Antipruritic Effects of Acupuncture. Cereb. Cortex 2014, 24, 873–882. [Google Scholar] [CrossRef]
- Park, H.-J.; Ahn, S.; Lee, H.; Hahm, D.; Kim, K.; Yeom, M. Acupuncture ameliorates not only atopic dermatitis-like skin inflammation but also acute and chronic serotonergic itch possibly through blockade of 5-HT2 and 5-HT7 receptors in mice. Brain Behav. Immun. 2021, 93, 399–408. [Google Scholar] [CrossRef]
- Akça, N.K.; Taşcı, S. Acupressure and Transcutaneous Electrical Acupoint Stimulation for Improving Uremic Pruritus: A Randomized, Controlled Trial. Altern. Ther. Health Med. 2016, 22, 18–24. [Google Scholar]
- Che-Yi, C.; Wen, C.Y.; Min-Tsung, K.; Chiu-Ching, H. Acupuncture in haemodialysis patients at the Quchi (LI11) acupoint for refractory uraemic pruritus. Nephrol. Dial. Transplant. 2005, 20, 1912–1915. [Google Scholar] [CrossRef]
- Pfab, F.; Hammes, M.; Bäcker, M.; Hussmarp, J.; Athanasiadis, G.; Tolle, T.; Behrendt, H.; Ring, J.; Darsow, U. Preventive effect of acupuncture on histamine-induced itch: A blinded, randomized, placebo-controlled, crossover trial. J. Allergy Clin. Immunol. 2005, 116, 1386–1388. [Google Scholar] [CrossRef]
- Kesting, M.R.; Thurmueller, P.; Hölzle, F.; Wolff, K.; Holland-Letz, T.; Stücker, M. Electrical Ear Acupuncture Reduces Histamine-induced Itch (Alloknesis). Acta Derm. Venereol. 2006, 86, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Min, S.; Kim, K.-W.; Jung, W.-M.; Lee, M.-J.; Kim, Y.-K.; Chae, Y.; Lee, H.; Park, H.-J. Acupuncture for Histamine-Induced Itch: Association With Increased Parasympathetic Tone and Connectivity of Putamen-Midcingulate Cortex. Front. Neurosci. 2019, 13, 215. [Google Scholar] [CrossRef] [PubMed]
- Li, H.-P.; Wang, X.-Y.; Chen, C.; Li, J.-J.; Yu, C.; Lin, L.-X.; Yu, Z.-E.; Jin, Z.-Y.; Zhu, H.; Xiang, H.-C.; et al. 100 Hz Electroacupuncture Alleviated Chronic Itch and GRPR Expression Through Activation of Kappa Opioid Receptors in Spinal Dorsal Horn. Front. Neurosci. 2021, 15, 625471. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.S.; Pan, A.Z.; Zhen, Y.; Kang, M.R.; Zhang, B.; Yi, W.M. Antipruritic effects of electroacupuncture on morphine-induced pruritus model mice through the TLR2/4-MyD88-NF-kappaB pathway. Neuroreport 2019, 30, 331–337. [Google Scholar] [CrossRef]
- Lee, Y.-C.; Lin, C.-H.; Hung, S.-Y.; Chung, H.-Y.; Luo, S.-T.; MacDonald, I.; Chu, Y.-T.; Lin, P.-L.; Chen, Y.-H. Manual acupuncture relieves bile acid-induced itch in mice: The role of microglia and TNF-α. Int. J. Med Sci. 2018, 15, 953–960. [Google Scholar] [CrossRef]
- Tominaga, M.; Takamori, K. An Update on Peripheral Mechanisms and Treatments of Itch. Biol. Pharm. Bull. 2013, 36, 1241–1247. [Google Scholar] [CrossRef]
- Komiya, E.; Tominaga, M.; Kamata, Y.; Suga, Y.; Takamori, K. Molecular and Cellular Mechanisms of Itch in Psoriasis. Int. J. Mol. Sci. 2020, 21, 8406. [Google Scholar] [CrossRef]
- Yosipovitch, G.; Misery, L.; Proksch, E.; Metz, M.; Ständer, S.; Schmelz, M. Skin Barrier Damage and Itch: Review of Mechanisms, Topical Management and Future Directions. Acta Derm. Venereol. 2019, 99, 1201–1209. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Therapeutic Methods | Mechanisms of Action |
|---|---|---|
| Oral therapy | Antidepressants • SSRIs (Paroxetine, Fluvoxamine, and Sertraline), NaSSA (Mirtazapine) | Inhibits reuptake of serotonin. Activates the descending inhibitory system in CNS. |
| Analgesics • Pregabalin, Mirogabalin, Neurotropin | Pregabalin may inhibit calcium influx and the release of neurotransmitters, such as glutamate. Mirogabalin may inhibit calcium influx in the peripheral nervous system and suppress the release of neurotransmitter. Neurotropin inhibits neuropeptide release and decreases IENF density. | |
| Calcineurin inhibitor • Cyclosporine A | Activates T cells and inhibits immune cell infiltration. Inhibits the release of inflammatory cytokines. Decreases IENF density. Suppresses itch mediator receptor expression. | |
| Antibiotics • Roxithromycin, Clarithromycin, Minomycin | Anti-inflammatory effects. Immunomodulation. Minomycin suppresses microglia. | |
| PDE4 inhibitor • Apremilast | Unknown | |
| Herbal remedies • Yokukansan (YKS), Xiao-Feng-Sang, Pei Tu Qing Xin (PTQX), and Huanglian Jiedu decoction (HLJDT), leaf extract of Rhamnus davurica (LERD), Spirodelae Herba (SH), Osthole, Cnidium monnieri, and Unsei-in | YKS and PTQX inhibit the infiltration of immune cells. HLJDT regulates DC functions. LERD inhibits the Fyn/Syk pathway in mast cells. SH modulates the activation of Orai1 and TPRV4 and inhibits mast cell degranulation. Osthole inhibits TRPV1 activation. Unsei-in inhibits the expression of NO synthase. | |
| Topical medication | Antidepressants • SNRI (Milnacipran) | Inhibits reuptake of serotonin. Activates the descending inhibitory system in CNS. |
| Antibiotics • Josamycin | Inhibits Staphylococcus aureus colonization. Inhibits Th2 cell differentiation. ⇒suppresses IL-31 production. | |
| Crotamiton | Inhibits TRPV1, TRPA1, and TRPV4 on nerves. | |
| PDE4 inhibitors • OPA-15406, crisaborole, and E6005 | Crisaborole modulates epidermal hyperplasia/proliferation and Th2 and Th17/Th22 transcriptional profiles. E6005 increases cAMP. | |
| Botulinum toxin type A | Blocks the release of acetylcholine and neurotransmitters from the presynaptic vesicle by deactivating SNARE proteins. Inhibits degranulation of mast cells. Normalizes the expression of nerve elongation factors and nerve repulsion factors. ⇒decreases IENF density. | |
| Phototherapy | PUVA and NB-UVB | Normalizes the expression of nerve elongation factors and nerve repulsion factors. ⇒decreases IENF density. |
| Excimer lamp | Decreases IENF density. | |
| Acupuncture therapy | Treatment LI11 blocks 5-HT2R and 5-HT7R. Treatments LI11, PC6, HT7, SP10, ST36 and HT3 decrease responses in the putamen, pMCC. Treatments LI4 and LI11 suppress GRPR expression via KOR activation. Treatments LI11 and SP10 inhibit the TLR2/4-MyD88-NF-κB pathway. Treatments LI4 and LI11 suppress activation of microglia. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toyama, S.; Tominaga, M.; Takamori, K. Treatment Options for Troublesome Itch. Pharmaceuticals 2022, 15, 1022. https://doi.org/10.3390/ph15081022
Toyama S, Tominaga M, Takamori K. Treatment Options for Troublesome Itch. Pharmaceuticals. 2022; 15(8):1022. https://doi.org/10.3390/ph15081022
Chicago/Turabian StyleToyama, Sumika, Mitsutoshi Tominaga, and Kenji Takamori. 2022. "Treatment Options for Troublesome Itch" Pharmaceuticals 15, no. 8: 1022. https://doi.org/10.3390/ph15081022
APA StyleToyama, S., Tominaga, M., & Takamori, K. (2022). Treatment Options for Troublesome Itch. Pharmaceuticals, 15(8), 1022. https://doi.org/10.3390/ph15081022