
The Role of Bronchoalveolar Lavage in Systemic Sclerosis Interstitial Lung Disease: A Systematic Literature Review


 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
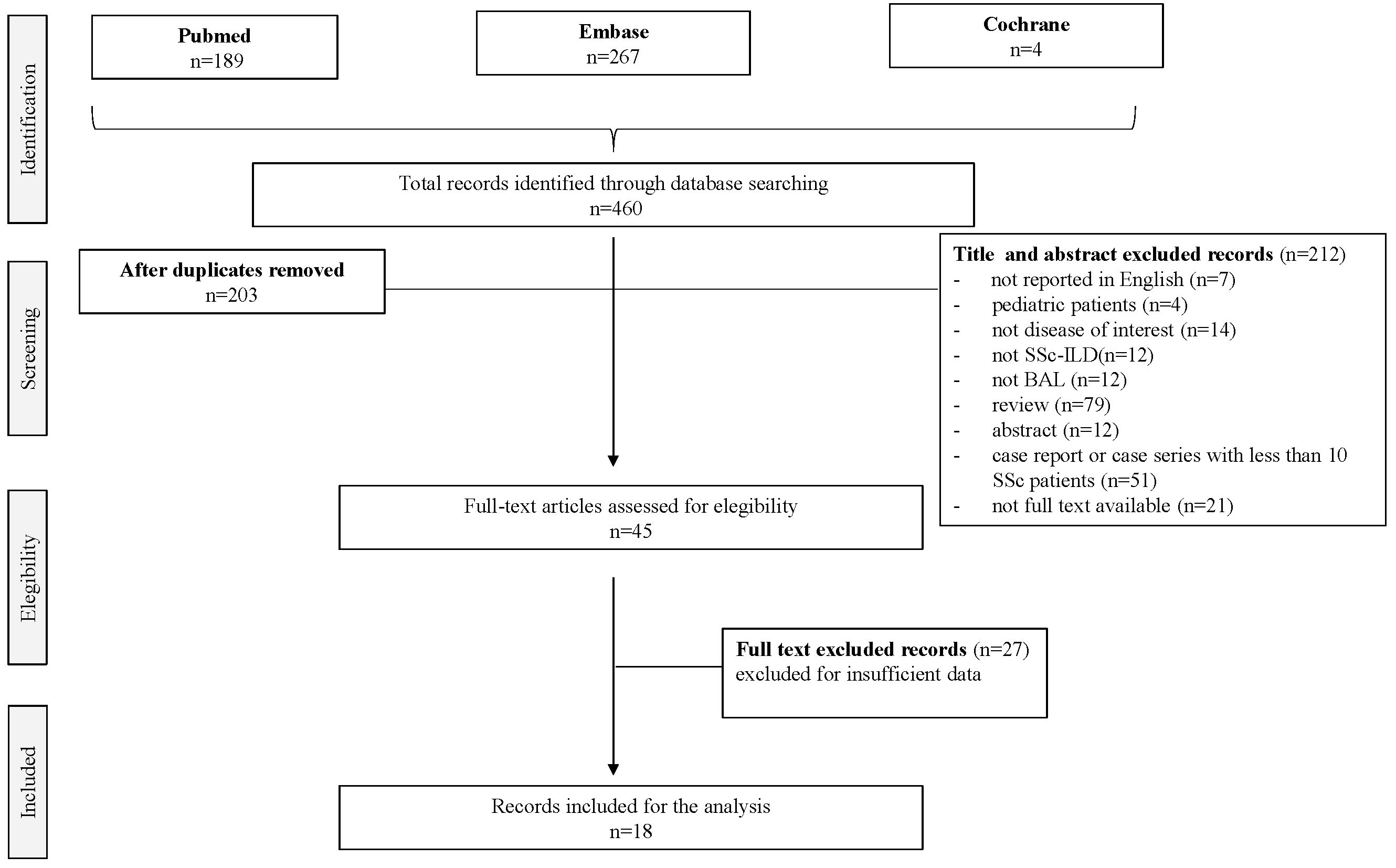
3.1. Study Selection
3.2. Study Characteristics
3.3. SSc Patients
3.4. Therapy
3.5. Pulmonary Function Tests (PFT)
3.6. HRCT Imaging
3.7. BAL
3.8. Prognosis
3.9. Subanalysis of Data from Patients with Alveolitis on BAL
4. Discussion
4.1. BAL Method
4.2. Patient’s Related Factors Could Influence BAL Results
4.3. The Role of Alveolitis as a Mirror of Lung Inflammation in ILD
4.4. The Role of Alveolitis in ILD Prognostic Evaluation
4.5. The Role of BAL Cytokine Expression
4.6. Correlation between BAL and Histopathological Pattern
4.7. Correlation between BAL and HRCT Features
4.8. Correlation of BAL and Pulmonary Functional Tests
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Orlandi, M.; Lepri, G.; Damiani, A.; Barsotti, S.; Di Battista, M.; Codullo, V.; Della Rossa, A.; Guiducci, S.; Allanore, Y. One year in review 2020: Systemic sclerosis. Clin. Exp. Rheumatol. 2020, 8 (Suppl. 125), 3–17. [Google Scholar]
- Volkmann, E.R.; Fischer, A. Update on morbidity and mortality in systemic sclerosis–related interstitial lung disease. J. Scleroderma Relat. Disord. 2021, 6, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Perelas, A.; Silver, R.M.; Arrossi, A.V.; Highland, K.B. Systemic sclerosis-associated interstitial lung disease. Lancet Respir. Med. 2020, 8, 304–320. [Google Scholar] [CrossRef] [PubMed]
- Desai, S.R.; Veeraraghavan, S.; Hansell, D.M.; Nikolakopolou, A.; Goh, N.S.; Nicholson, A.G.; Colby, T.V.; Denton, C.P.; Black, C.M.; du Bois, R.M.; et al. CT features of lung disease in patients with systemic sclerosis: Comparison with idiopathic pulmonary fibrosis and nonspecific interstitial pneumonia. Radiology 2004, 232, 560–567. [Google Scholar] [CrossRef]
- Fujita, J. Non-specific interstitial pneumonia as pulmonary involvement of systemic sclerosis. Ann. Rheum. Dis. 2001, 60, 281–283. [Google Scholar] [CrossRef] [Green Version]
- King, T.E. Nonspecific Interstitial Pneumonia and Systemic Sclerosis. Am. J. Respir. Crit. Care Med. 2002, 165, 1578–1579. [Google Scholar] [CrossRef]
- Launay, D.; Remy-Jardin, M.; Michon-Pasturel, U.; Mastora, I.; Hachulla, E.; Lambert, M.; Delannoy, V.; Queyrel, V.; Duhamel, A.; Matran, R.; et al. High resolution computed tomography in fibrosing alveolitis associated with systemic sclerosis. J. Rheumatol. 2006, 33, 1789–1801. [Google Scholar]
- Suliman, S.; Al Harash, A.; Roberts, W.N.; Perez, R.L.; Roman, J. Scleroderma-related interstitial lung disease. Respir. Med. Case Rep. 2017, 22, 109–112. [Google Scholar] [CrossRef]
- Hoffmann-Vold, A.M.; Maher, T.M.; Philpot, E.E.; Ashrafzadeh, A.; Barake, R.; Barsotti, S.; Bruni, C.; Carducci, P.; Carreira, P.E.; Castellví, I.; et al. The identification and management of interstitial lung disease in systemic sclerosis: Evidence-based European consensus statements. Lancet Rheumatol. 2020, 2, E71–E83. [Google Scholar] [CrossRef]
- Hoffmann-Vold, A.M.; Allanore, Y.; Alves, M.; Brunborg, C.; Airó, P.; Ananieva, L.P.; Czirják, L.; Guiducci, S.; Hachulla, E.; Li, M.; et al. Progressive interstitial lung disease in patients with systemic sclerosis-associated interstitial lung disease in the EUSTAR database. Ann. Rheum. Dis. 2021, 80, 219–227. [Google Scholar] [CrossRef]
- Klech, H. Technical recommendations and guidelines for bronchoalveolar lavage (BAL) report of the European Society of Pneumology Task Group on BAL. Eur. Respir. J. 1989, 2, 561–585. [Google Scholar]
- The BAL Cooperative Steering Committee. Bronchoalveolar lavage constituents in healthy individuals, idiopathic pulmonary fibrosis, and selected comparison groups. Am. Rev. Respir. Dis. 1990, 141, S169–S202. [Google Scholar]
- Meyer, K.C.; Raghu, G.; Baughman, R.P.; Brown, K.K.; Costabel, U.; du Bois, R.M.; Drent, M.; Haslam, P.L.; Kim, D.S.; Nagai, S.; et al. An official American Thoracic Society clinical practice guideline: The clinical utility of bronchoalveolar lavage cellular analysis in interstitial lung disease. Am. J. Respir. Crit. Care Med. 2012, 185, 1004–1014. [Google Scholar] [CrossRef] [PubMed]
- Silver, R.M.; Metcalf, J.F.; Stanley, J.H.; LeRoy, E.C. Interstitial lung disease in scleroderma. Analysis by bronchoalveolar lavage. Arthritis Rheum. 1984, 27, 1254–1262. [Google Scholar] [CrossRef]
- Silver, R.M.; Miller, K.S.; Kinsella, M.B.; Smith, E.A.; Schabel, S.I. Evaluation and management of scleroderma lung disease using bronchoalveolar lavage. Am. J. Med. 1990, 88, 470–476. [Google Scholar] [CrossRef]
- Harrison, N.K.; Glanville, A.R.; Strickland, B.; Haslam, P.L.; Corrin, B.; Addis, B.J.; Lawrence, R.; Millar, A.B.; Black, C.M.; Turner-Warwick, M. Pulmonary involvement in systemic sclerosis: The detection of early changes by thin section CT scan, bronchoalveolar lavage and 99mTc-DTPA clearance. Respir. Med. 1989, 83, 403–414. [Google Scholar] [CrossRef]
- Frigieri, L.; Mormile, F.; Grilli, N.; Mancini, D.; Ciappi, G.; Pagliari, G.; Magarò, M.; Flamini, G. Bilateral bronchoalveolar lavage in progressive systemic sclerosis: Interlobar variability, lymphocyte subpopulations, and functional correlations. Respiration 1991, 58, 132–140. [Google Scholar] [CrossRef]
- Tomassetti, S.; Colby, T.V.; Wells, A.U.; Poletti, V.; Costabel, U.; Matucci-Cerinic, M. Bronchoalveolar lavage and lung biopsy in connective tissue diseases, to do or not to do? Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X211059605. [Google Scholar] [CrossRef]
- Baughman, R.P. Technical aspects of bronchoalveolar lavage: Recommendations for a standard procedure. Sem. Respir. Crit. Care Med. 2007, 28, 475–485. [Google Scholar] [CrossRef] [Green Version]
- Bouros, D.; Wells, A.U.; Nicholson, A.G.; Colby, T.V.; Polychronopoulos, V.; Pantelidis, P.; Haslam, P.L.; Vassilakis, D.A.; Black, C.M.; du Bois, R.M. Histopathologic subsets of fibrosing alveolitis in patients with systemic sclerosis and their relationship to outcome. Am. J. Respir. Crit. Care Med. 2002, 165, 1581–1586. [Google Scholar] [CrossRef]
- Cailes, J.B.; O’Connor, C.; Pantelidis, P.; Southcott, A.M.; Fitzgerald, M.X.; Black, C.M.; du Bois, R.M. Neutrophil activation in fibrosing alveolitis: A comparison of lone cryptogenic fibrosing alveolitis and systemic sclerosis. Eur. Respir. J. 1996, 9, 992–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clements, P.J.; Goldin, J.G.; Kleerup, E.C.; Furst, D.E.; Elashoff, R.M.; Tashkin, D.P.; Roth, M.D. Regional differences in bronchoalveolar lavage and thoracic high-resolution computed tomography results in dyspneic patients with systemic sclerosis. Arthritis Rheum. 2004, 50, 1909–1917. [Google Scholar] [CrossRef] [PubMed]
- De Santis, M.; Bosello, S.L.; Peluso, G.; Pinnelli, M.; Alivernini, S.; Zizzo, G.; Bocci, M.; Capacci, A.; La Torre, G.; Mannocci, A.; et al. Bronchoalveolar lavage fluid and progression of scleroderma interstitial lung disease. Clin. Respir. J. 2012, 6, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Goh, N.S.; Veeraraghavan, S.; Desai, S.R.; Cramer, D.; Hansell, D.M.; Denton, C.P.; Black, C.M.; du Bois, R.M.; Wells, A.U. Bronchoalveolar lavage cellular profiles in patients with systemic sclerosis-associated interstitial lung disease are not predictive of disease progression. Arthritis Rheum. 2007, 56, 2005–2012. [Google Scholar] [CrossRef] [PubMed]
- Goldin, J.G.; Lynch, D.A.; Strollo, D.C.; Suh, R.D.; Schraufnagel, D.E.; Clements, P.J.; Elashoff, R.M.; Furst, D.E.; Vasunilashorn, S.; McNitt-Gray, M.F.; et al. Scleroderma Lung Study Research Group. High-resolution CT scan findings in patients with symptomatic scleroderma-related interstitial lung disease. Chest 2008, 134, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Hant, F.N.; Ludwicka-Bradley, A.; Wang, H.J.; Li, N.; Elashoff, R.; Tashkin, D.P.; Silver, R.M.; Scleroderma Lung Study Research Group. Surfactant protein D and KL-6 as serum biomarkers of interstitial lung disease in patients with scleroderma. J. Rheumatol. 2009, 36, 773–780. [Google Scholar] [CrossRef]
- Kowal-Bielecka, O.K.; Kowal, K.; Lewszuk, A.; Bodzenta-Lukaszyk, A.; Walecki, J.; Sierakowski, S. Beta thromboglobulin and platelet factor 4 in bronchoalveolar lavage fluid of patients with systemic sclerosis. Ann. Rheum. Dis. 2005, 64, 484–486. [Google Scholar] [CrossRef] [Green Version]
- Moodley, Y.P.; Lalloo, U.G. Exhaled nitric oxide is elevated in patients with progressive systemic sclerosis without interstitial lung disease. Chest 2001, 119, 1449–1454. [Google Scholar] [CrossRef] [Green Version]
- Nagasawa, Y.; Takada, T.; Shimizu, T.; Narita, J.; Moriyama, H.; Terada, M.; Suzuki, E.; Gejyo, F. Inflammatory cells in lung disease associated with rheumatoid arthritis. Intern. Med. 2009, 48, 1209–1217. [Google Scholar] [CrossRef] [Green Version]
- Prasse, A.; Pechkovsky, D.V.; Toews, G.B.; Schäfer, M.; Eggeling, S.; Ludwig, C.; Germann, M.; Kollert, F.; Zissel, G.; Müller-Quernheim, J. CCL18 as an indicator of pulmonary fibrotic activity in idiopathic interstitial pneumonias and systemic sclerosis. Arthritis Rheum. 2007, 56, 1685–1693. [Google Scholar] [CrossRef] [Green Version]
- Salaffi, F.; Manganelli, P.; Carotti, M.; Baldelli, S. The differing patterns of subclinical pulmonary involvement in connective tissue diseases as shown by application of factor analysis. Clin. Rheumatol. 2000, 19, 35–41. [Google Scholar] [PubMed]
- Schmidt, K.; Martinez-Gamboa, L.; Meier, S.; Witt, C.; Meisel, C.; Hanitsch, L.G.; Becker, M.O.; Huscher, D.; Burmester, G.R.; Riemekasten, G. Bronchoalveoloar lavage fluid cytokines and chemokines as markers and predictors for the outcome of interstitial lung disease in systemic sclerosis patients. Arthritis Res. Ther. 2009, 11, R111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Southcott, A.M.; Jones, K.P.; Li, D.; Majumdar, S.; Cambrey, A.D.; Pantelidis, P.; Black, C.M.; Laurent, G.J.; Davies, B.H.; Jeffery, P.K.; et al. Interleukin-8. Differential expression in lone fibrosing alveolitis and systemic sclerosis. Am. J. Respir. Crit. Care Med. 1995, 151, 1604–1612. [Google Scholar] [CrossRef] [PubMed]
- Volpinari, S.; La Corte, R.; Bighi, S.; Ravenna, F.; Prandini, N.; Lo Monaco, A.; Trotta, F. Bronchoalveolar lavage in systemic sclerosis with lung involvement: Role and correlations with functional, radiological and scintigraphic parameters. Rheumatol. Int. 2011, 31, 1183–1188. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, N.; Abul, Y.; Bicakcigil, M.; Golabi, P.; Celikel, C.; Karakurt, S.; Yavuz, S. Induced sputum as a method for detection of systemic sclerosis-related interstitial lung disease. Rheumatol. Int. 2012, 32, 1921–1925. [Google Scholar] [CrossRef]
- Wells, A.U.; Hansell, D.M.; Haslam, P.L.; Rubens, M.B.; Cailes, J.; Black, C.M.; du Bois, R.M. Bronchoalveolar lavage cellularity: Lone cryptogenic fibrosing alveolitis compared with the fibrosing alveolitis of systemic sclerosis. Am. J. Respir. Crit. Care Med. 1998, 157 Pt 1, 1474–1482. [Google Scholar] [CrossRef]
- Behr, J.; Vogelmeier, C.; Beinert, T.; Meurer, M.; Krombach, F.; König, G.; Fruhmann, G. Bronchoalveolar lavage for evaluation and management of scleroderma disease of the lung. Am. J. Respir. Crit. Care Med. 1996, 154 Pt 1, 400–406. [Google Scholar] [CrossRef]
- van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A., Jr.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. 2013, 65, 2737–2747. [Google Scholar] [CrossRef] [Green Version]
- Marik, P.E.; Kaplan, D. Aspiration pneumonia and dysphagia in the elderly. Chest 2003, 124, 328–336. [Google Scholar] [CrossRef] [Green Version]
- Harrison, N.K.; Myers, A.R.; Corrin, B.; Soosay, G.; Dewar, A.; Black, C.M.; Du Bois, R.M.; Turner-Warwick, M. Structural features of interstitial lung disease in systemic sclerosis. Am. Rev. Respir. Dis. 1991, 144 Pt 1, 706–713. [Google Scholar] [CrossRef]
- Harrison, N.K.; McAnulty, R.J.; Haslam, P.L.; Black, C.M.; Laurent, G.J. Evidence for protein oedema, neutrophil influx, and enhanced collagen production in lungs of patients with systemic sclerosis. Thorax 1990, 45, 606–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, A.U.; Hansell, D.M.; Rubens, M.B.; Cullinan, P.; Haslam, P.L.; Black, C.M.; Du Bois, R.M. Fibrosing alveolitis in systemic sclerosis. Bronchoalveolar lavage findings in relation to computed tomographic appearance. Am. J. Respir. Crit. Care Med. 1994, 150, 462–468. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All BAL | BAL with Alveolitis | |
| 1447 pz | 186 pz | |
| Patients’ characteristics | ||
| lcSSc (%) | 63.4 | 61.8 |
| dcSSc (%) | 36.6 | 38.2 |
| Disease duration (years ± SD) | 5.4 ± 5.6 | 6.7 ± 7.0 |
| Female (% ± SD) | 78.6 | 77.8 |
| Mean age (years ± SD) | 49.7 ± 11.9 | 52.5 ± 10.1 |
| Never smokers (%) | 53.5 | |
| Former smokers (%) | 27.5 | |
| Current smokers (%) | 12.3 | |
| PFT | ||
| FVC (pred % ± SD) | 79.3 ± 19.7 | 87.2 ± 24.4 |
| FEV1 (pred % ± SD) | 72.8 ± 16.6 | |
| DLCO (pred % ± SD) | 54.8 ± 16.9 | 56.1 ± 14.3 |
| BALF cellularity | ||
| Neutrophils (% ± SD) | 6.3 ± 9.5 | 10.7 ± 6 |
| Lymphocytes (% ± SD) | 11.1 ± 9.4 | 5.9 ± 4.9 |
| Macrophages (% ± SD) | 62.5 | 81.3 ± 10.8 |
| Eosinophils (% ± SD) | 1.7 ± 2.1 | 1.8 ± 1.9 |
| BALF Biomarkers | ||
| KL-6 (U/mL) | 868 ± 718 | 1489 ± 1090 |
| SP-D (ng/mL) | 332 ± 216 | 252 ± 207 |
| Paper | Neutrophils (% ± SD) | Lymphocytes (% ± SD) | Macrophages (% ± SD) | Eosinophils (% ± SD) |
|---|---|---|---|---|
| Cailes et al. [21] | 3.00 | 6.00 | 85.00 | 1.00 |
| De Santis et al. [23] | 5.90 ± 10.50 | 4.30 | 6.10 | 1.10 ± 2.20 |
| Kowal-Bielecka et al. [27] | 5.40 ± 4.80 | 22.60 ± 13.70 | 70.20 ± 15.10 | - |
| Moodley et al. [28] | 10.30 ± 2.10 | 6.30 ± 2.20 | 79.60 ± 3.10 | 4.00 ± 1.00 |
| Nagasawa et al. [29] | 2.30 ± 2.90 | 17.20 ± 8.60 | 79.60 ± 9.30 | 1.00 ± 1.30 |
| Prasse et al. [30] | 9.00 ± 10.00 | 18.00 ± 10.00 | 69.00 ± 17.00 | 3.00 ± 2.00 |
| Salaffi et al. [30] | 4.10 ± 0.90 | 13.30 ± 2.10 | 80.90 ± 3.40 | 1.70 ± 0.70 |
| Yilmaz et al. [34] | 9.50 ± 12.30 | 18.80 ± 17.40 | 66.00 ± 19.50 | - |
| Cailes et al. [21] | FA-SSc (n = 45) % Patients | Molecular Level in BALF |
|---|---|---|
| MPO | 0 | 0 |
| Elastase | 106 (3–263) ng·mL−1 | |
| Elastase/α1–antitrypsin complex | 1.8(0.29–8.5) ng·mL−1 | |
| Collagenase | 0–60 m units | |
| Lactoferrin | 0.17 (0.03–1.03) ng·mL−1 | |
| Kowal-Bielecka et al. [27] | ||
| BTG | 29.7% (11/37) | 106.9 (15.2–229.0) IU/mL |
| PF4 | 21.6% (8/37) | 35.5 (7.0–53.0) IU/mL |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orlandi, M.; Meliante, L.A.; Damiani, A.; Tofani, L.; Bruni, C.; Guiducci, S.; Matucci-Cerinic, M.; Bellando-Randone, S.; Tomassetti, S. The Role of Bronchoalveolar Lavage in Systemic Sclerosis Interstitial Lung Disease: A Systematic Literature Review. Pharmaceuticals 2022, 15, 1584. https://doi.org/10.3390/ph15121584
Orlandi M, Meliante LA, Damiani A, Tofani L, Bruni C, Guiducci S, Matucci-Cerinic M, Bellando-Randone S, Tomassetti S. The Role of Bronchoalveolar Lavage in Systemic Sclerosis Interstitial Lung Disease: A Systematic Literature Review. Pharmaceuticals. 2022; 15(12):1584. https://doi.org/10.3390/ph15121584
Chicago/Turabian StyleOrlandi, Martina, Laura Antonia Meliante, Arianna Damiani, Lorenzo Tofani, Cosimo Bruni, Serena Guiducci, Marco Matucci-Cerinic, Silvia Bellando-Randone, and Sara Tomassetti. 2022. "The Role of Bronchoalveolar Lavage in Systemic Sclerosis Interstitial Lung Disease: A Systematic Literature Review" Pharmaceuticals 15, no. 12: 1584. https://doi.org/10.3390/ph15121584
APA StyleOrlandi, M., Meliante, L. A., Damiani, A., Tofani, L., Bruni, C., Guiducci, S., Matucci-Cerinic, M., Bellando-Randone, S., & Tomassetti, S. (2022). The Role of Bronchoalveolar Lavage in Systemic Sclerosis Interstitial Lung Disease: A Systematic Literature Review. Pharmaceuticals, 15(12), 1584. https://doi.org/10.3390/ph15121584