Traditional East Asian Herbal Medicine Treatment for Alzheimer’s Disease: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Registration and Design
2.2. Database Search
2.3. Eligibility Criteria
2.4. Outcome Assessment
2.5. Data Extraction
2.6. Quality Assessment of Individual Studies
2.7. Statistical Analysis
3. Results
3.1. Characteristics of Included Studies
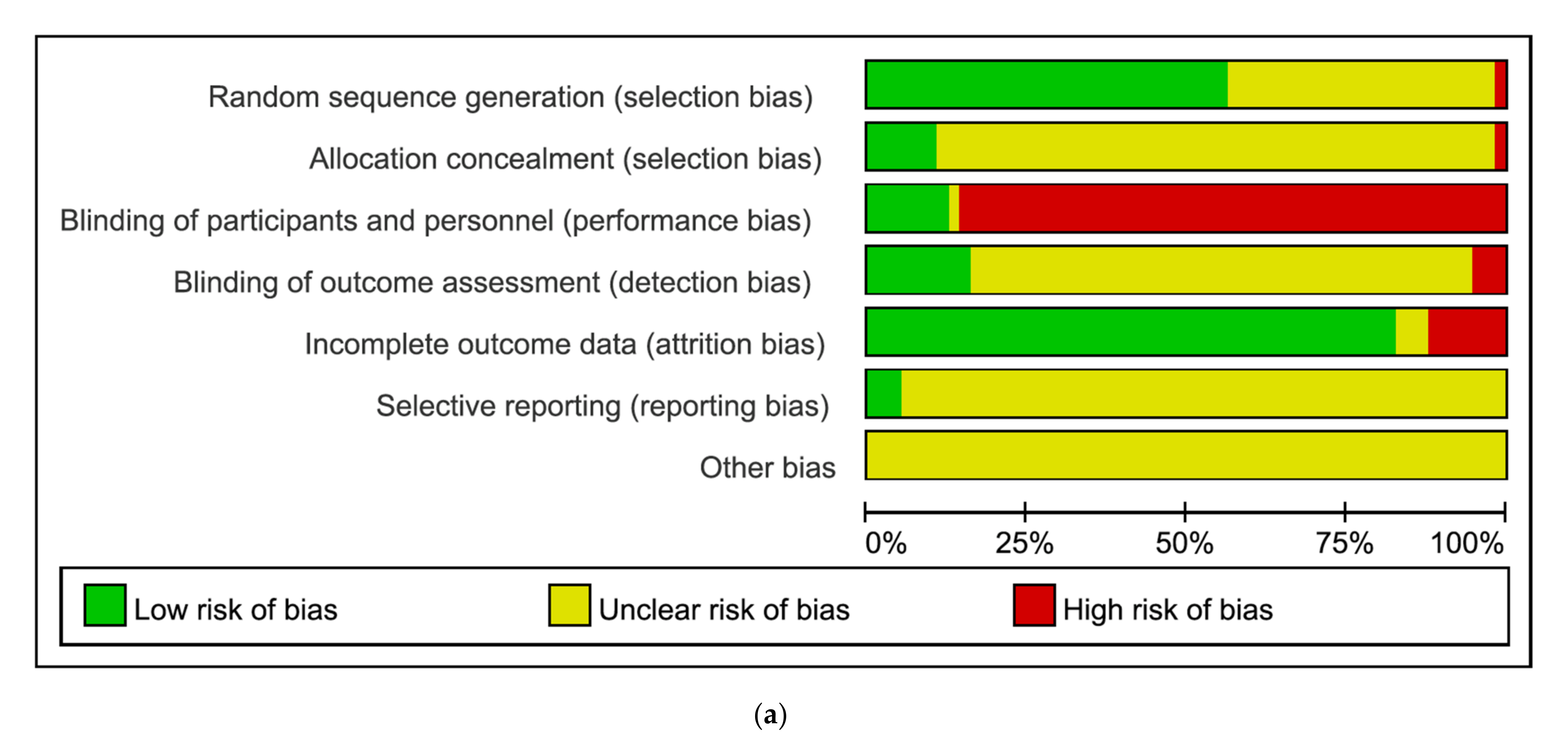
3.2. Risk of Bias Assessment
3.3. Synthesized Results
3.3.1. Cognitive Function
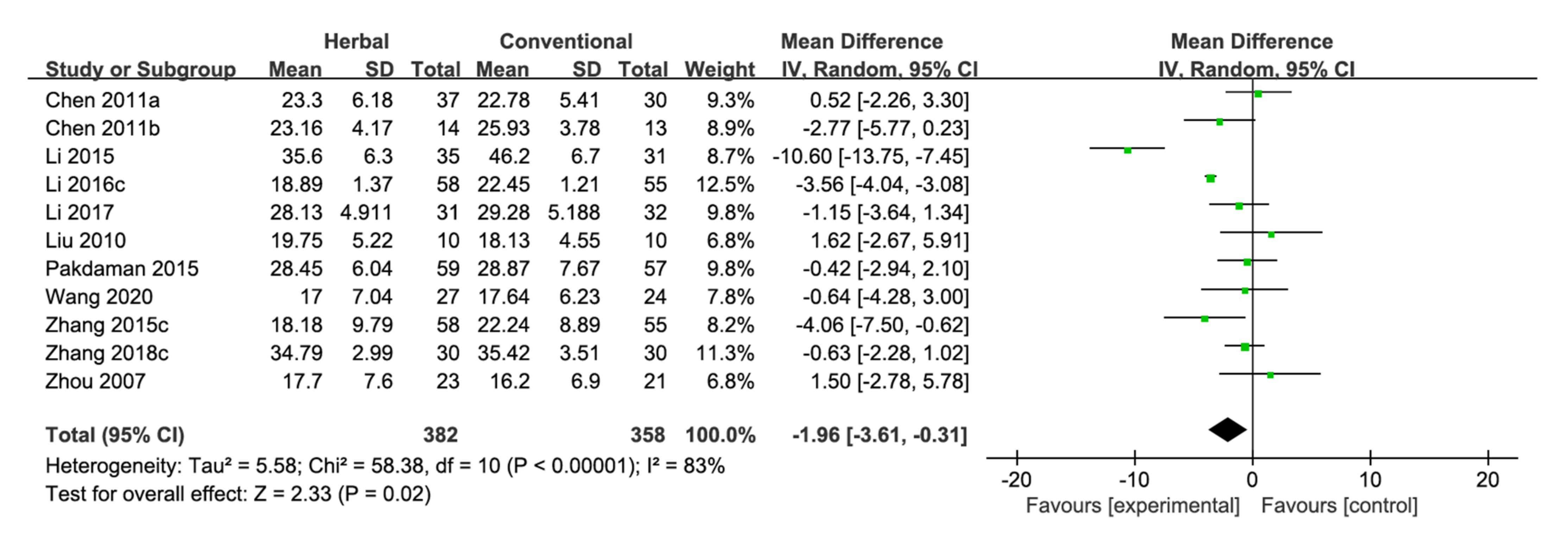
MMSE
- Herbal Medicine vs. Conventional Medicine
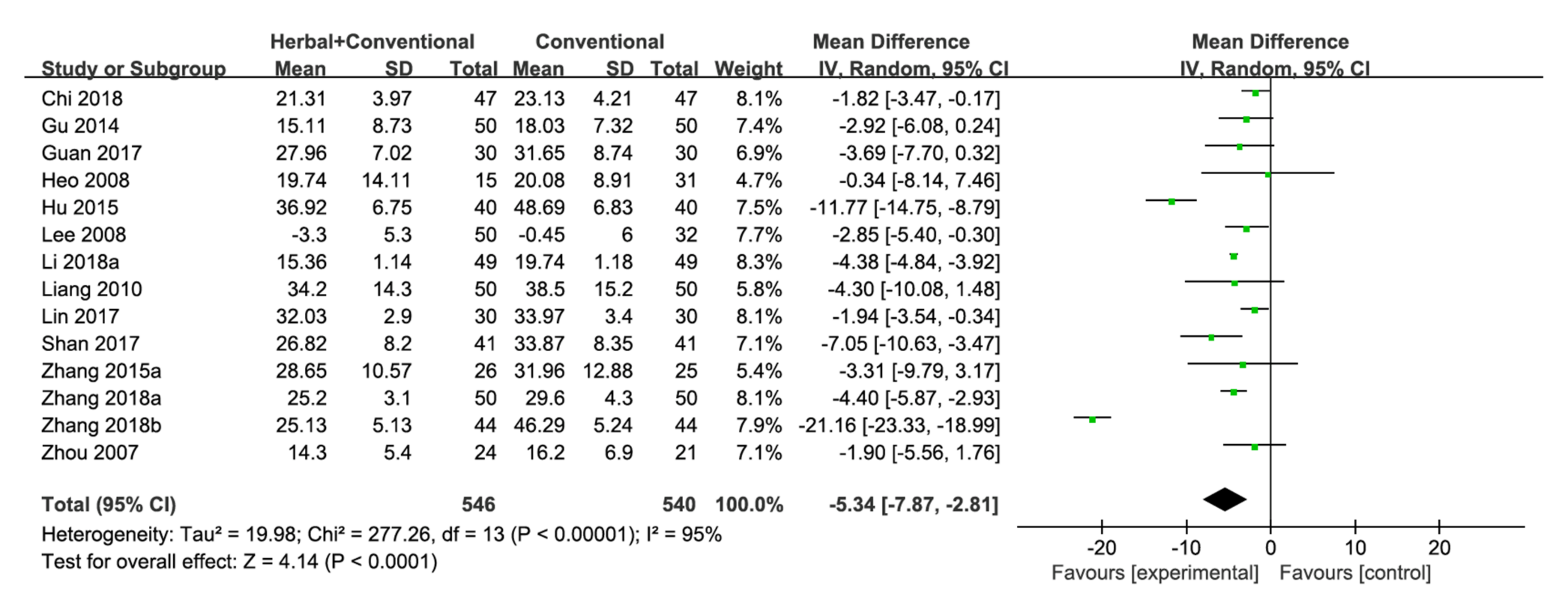
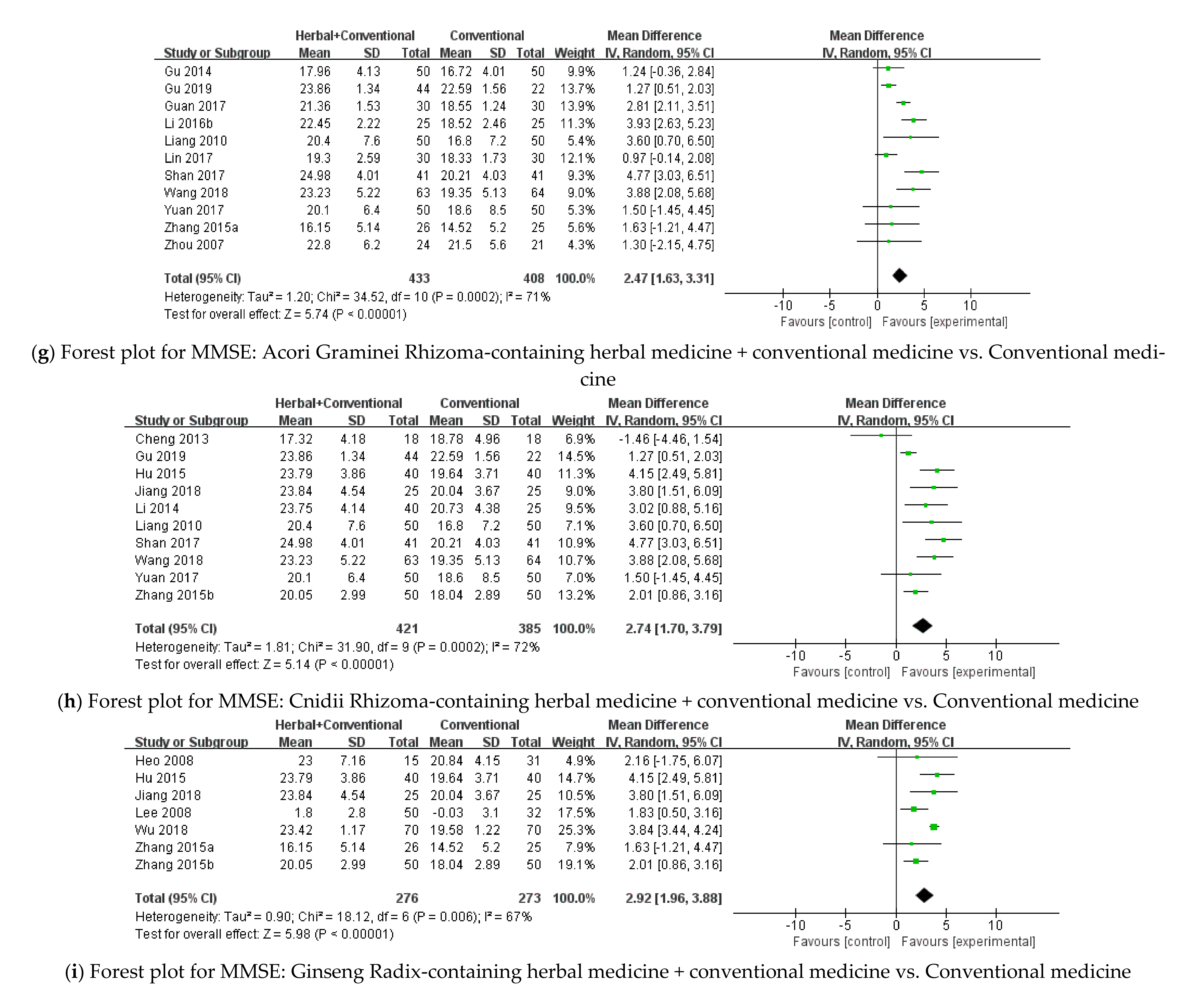
- Herbal Medicine + Conventional Medicine vs. Conventional Medicine
- Herbal Medicine vs. Placebo
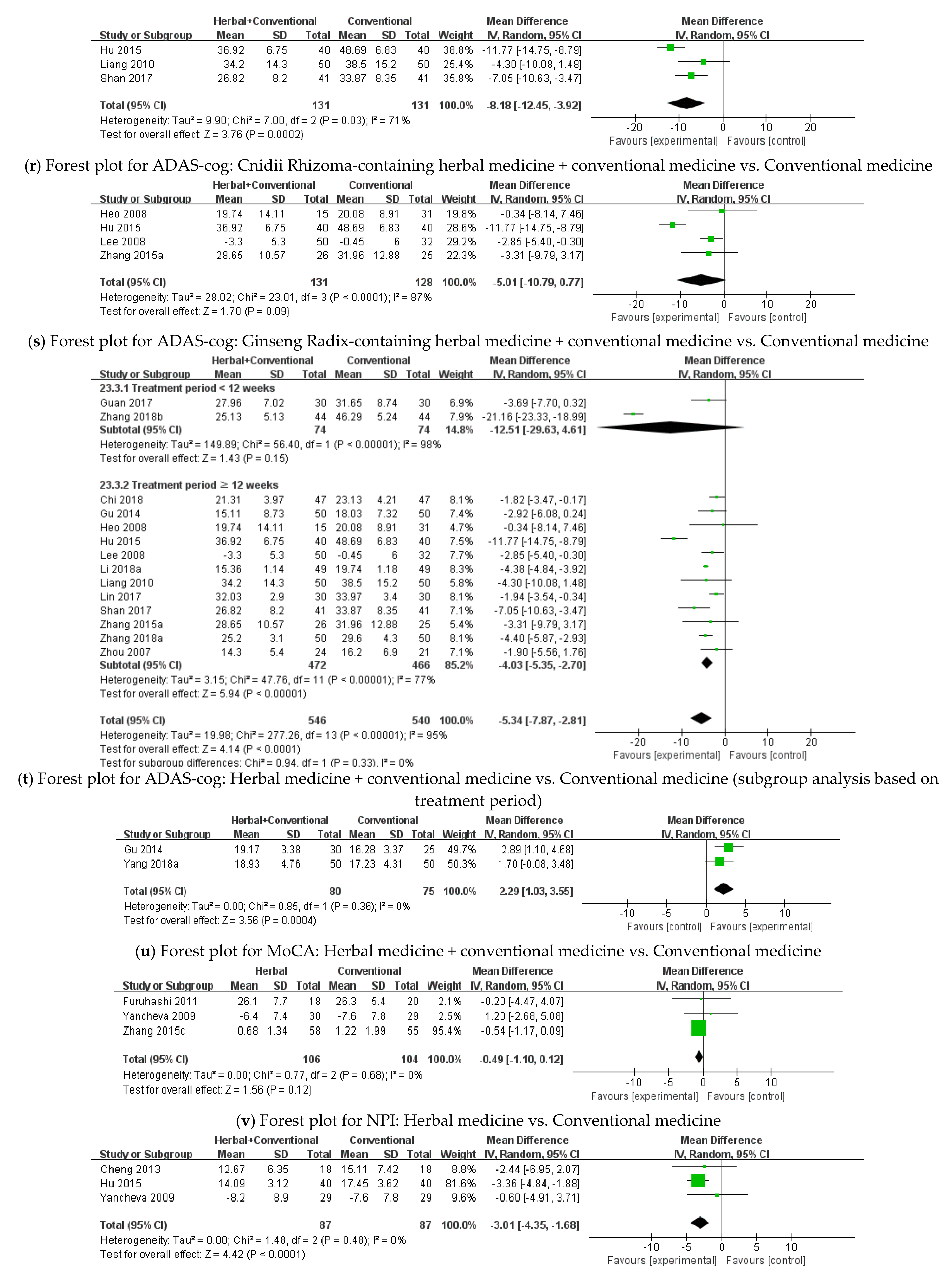
ADAS-cog
- Herbal Medicine vs. Conventional Medicine
MoCA
- Herbal Medicine + Conventional Medicine vs. Conventional Medicine
3.3.2. BPSD
NPI
- Herbal Medicine vs. Conventional Medicine
- Herbal Medicine + Conventional Medicine vs. Conventional Medicine
BEHAVE-AD
- Herbal Medicine + Conventional Medicine vs. Conventional Medicine
3.3.3. Plasma Amyloid-Beta
3.4. Safety Assessment
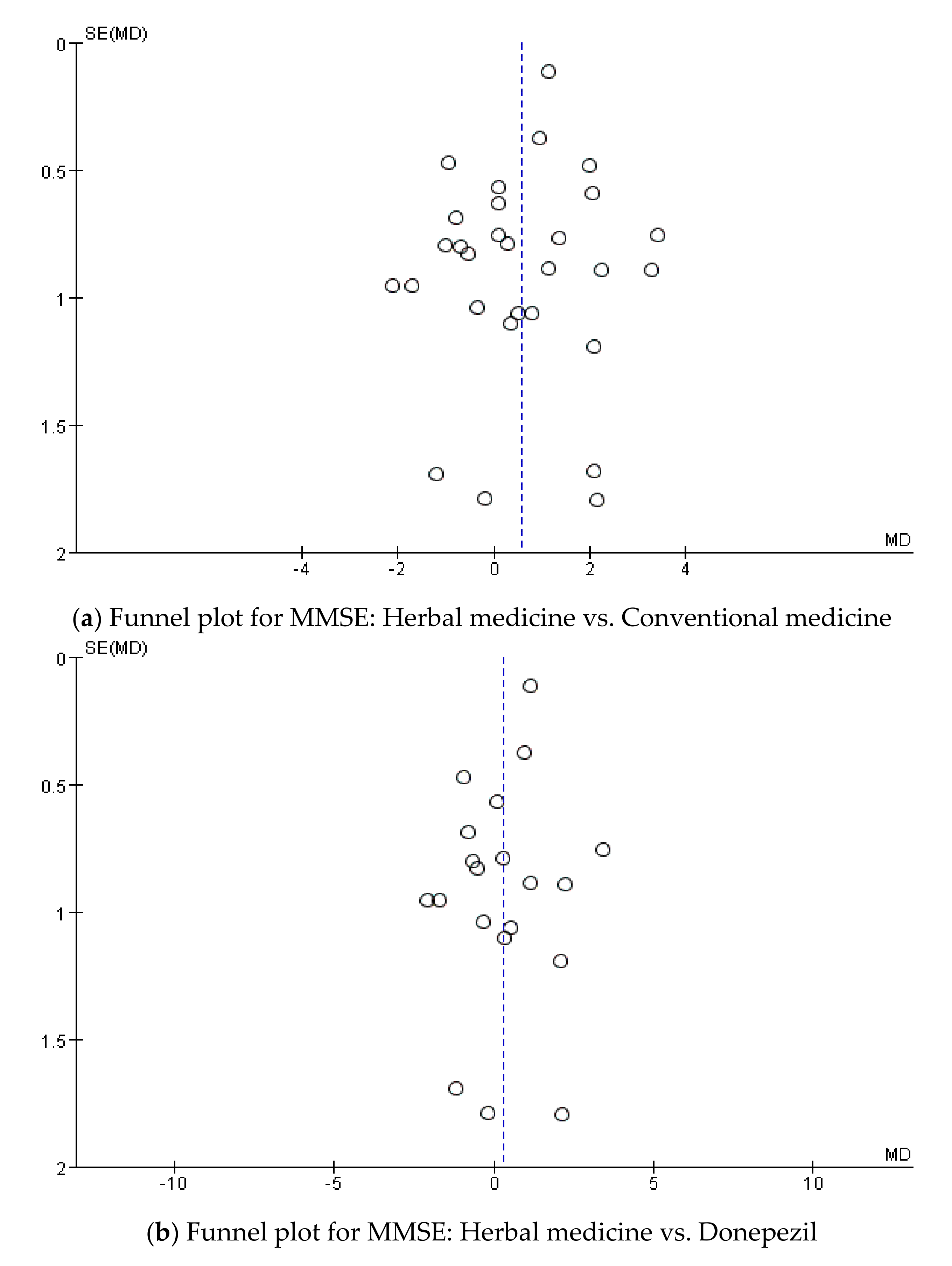
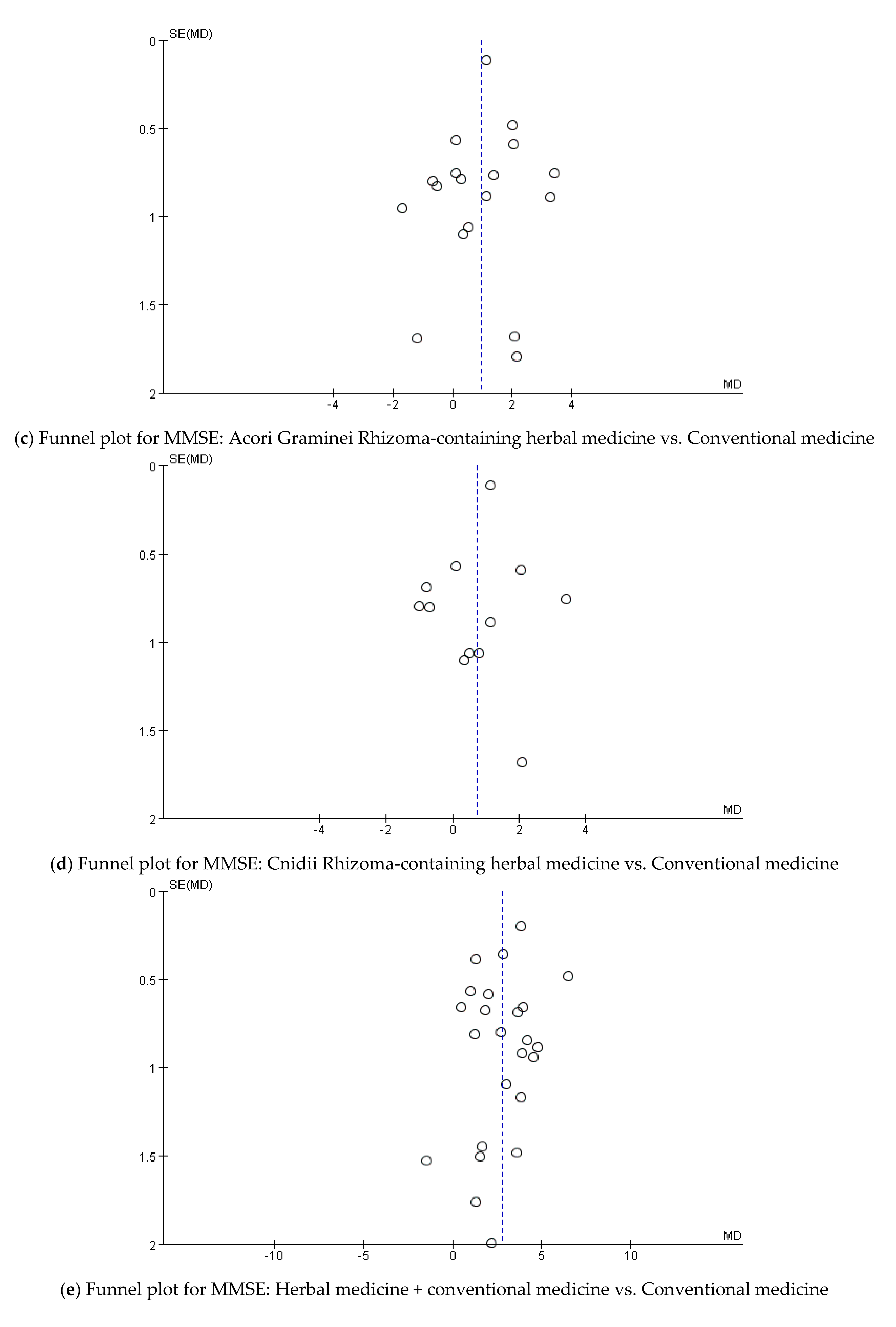
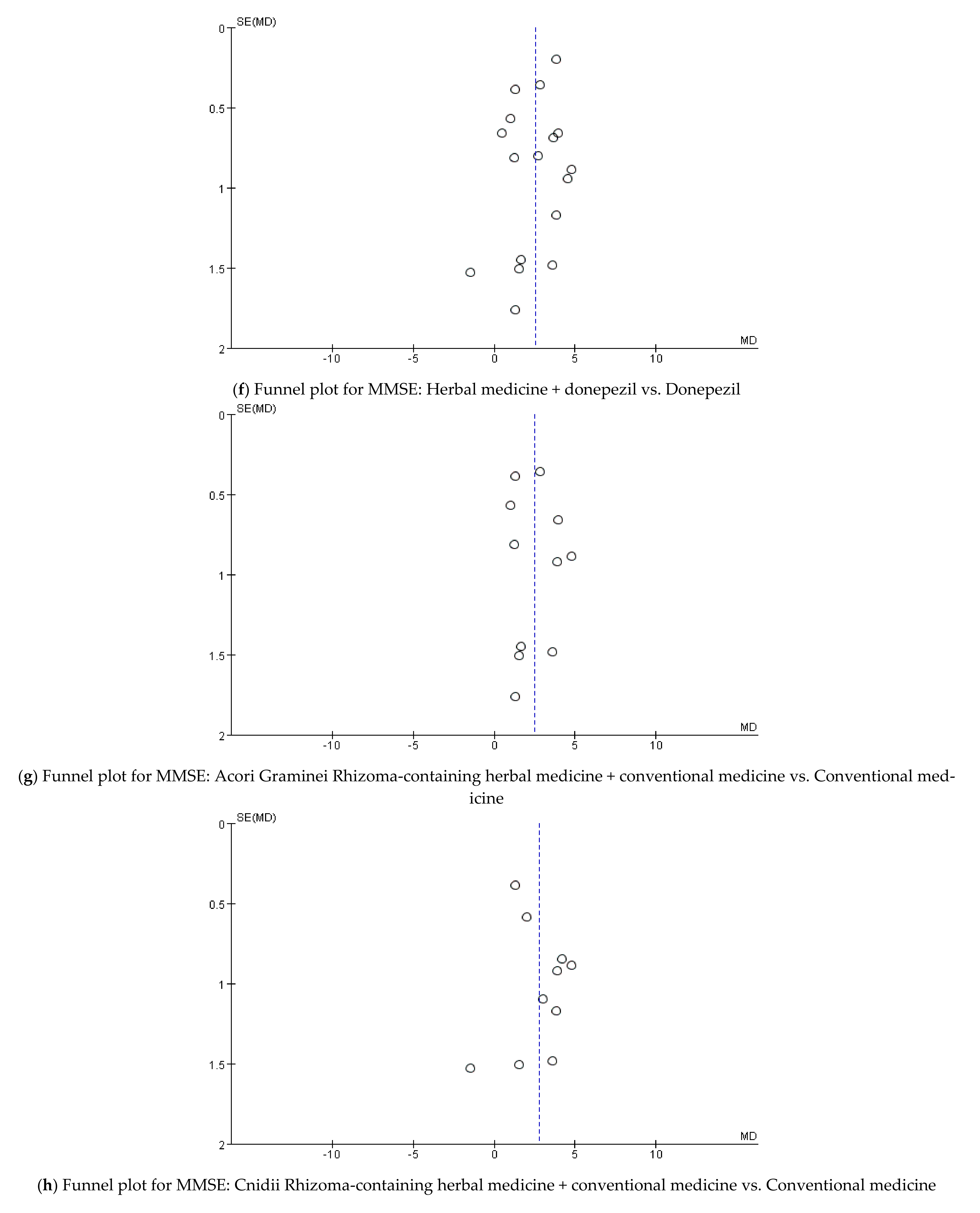
3.5. Publication Bias
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy
Appendix A.1. EMBASE
Appendix A.2. CENTRAL
- #1 MeSH descriptor: [Alzheimer Disease] explode all trees
- #2 Alzheimer* or Dementia: ti,ab,kw (Word variations have been searched)
- #3 MeSH descriptor: [Herbal Medicine] explode all trees
- #4 MeSH descriptor: [Medicine, East Asian Traditional] explode all trees
- #5 ‘Herbal medicine’ OR ‘Traditional Korean Medicine’ OR ‘Traditional Chinese Medicine’ OR ‘Kampo Medicine’ OR ‘Traditional Oriental Medicine’ OR ‘Herbal drug’ OR Herb* OR decoction OR ‘Chinese herb’: ti,ab,kw (Word variations have been searched)
- #6 ‘Randomized controlled trial’ OR ‘Controlled clinical trial’ OR Randomized OR ‘Clinical trial’ OR Random: ti,ab,kw (Word variations have been searched)
- #7 #1 or #2
- #8 #3 or #4 or #5 or #6
- #9 #7 and #8
Appendix A.3. CNKI
- #1 阿尔茨海默病
- #2 阿尔采莫氏病
- #3 老年性痴呆症
- #4 老年性痴呆
- #5 老年痴呆
- #6 OR/#1-#5
- #7 中药
- #8 漢方藥
- #9 #7 OR #8
- #10 #6 AND #9
Appendix A.4. OASIS
Appendix A.5. KTKP
Appendix A.6. CiNii
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Name of Herbal Medicine (Manufacturer, If Available) | Components |
|---|---|---|
| Furuhashi 2011 [20] | Yokukansan (Tsumura Co., Tokyo, Japan) | Atractylodis Rhizoma, Hoelen, Cnidii Rhizoma, Uncariae Ramulus et Uncus, Angelicae Gigantis Radix, Bupleuri Radix, Glycyrrhizae Radix |
| Furukawa 2017 [21] | Yokukansan (Tsumura Co., Tokyo, Japan) | Atractylodis Rhizoma, Hoelen, Cnidii Rhizoma, Uncariae Ramulus et Uncus, Angelicae Gigantis Radix, Bupleuri Radix, Glycyrrhizae Radix |
| Heo 2008 [22] | Korean red ginseng (Korea Ginseng Co., Daejoen, Korea) | Ginseng Radix |
| Lee 2008 [23] | Korean white ginseng powder (Nonghyup Co., Seoul, Korea) | Ginseng Radix |
| Liu 2013 [24] | Bushenhuatanyizhi Granule | Polygoni Multiflori Radix, Ginseng Radix, Acori Graminei Rhizoma, Bambusae Caulis in Taeniam, Pinelliae Rhizoma, Hoelen, Polygalae Radix |
| Mazza 2006 [25] | EGb 761® | Ginkgo biloba |
| Meng 2005 [26] | Naohuandan (Guizhou Pharmaceutical Factory, Guizhou, China) | Drynariae Rhizoma, Rehmanniae Radix Preparata, Acori Graminei Rhizoma, Ginseng Radix, Lumbricus |
| Pakdaman 2015 [27] | MLC601 (NeuroAiDTM) (Moleac, Singapole) | Hirudo, Saigae Tataricae Cornu, Scorpio, Eupolyphaga, Artificial Calculus Bovis, Paeoniae Radix Alba, Astragali Radix, Salviae Miltiorrhizae Radix, Cnidii Rhizoma, Angelicae Gigantis Radix, Polygalae Radix, Prunus Persica, Carthami Flos, Acori Graminei Rhizoma |
| Pan 2014 [28] | Shen-Zhi-Ling Oral Liquid (Shandong Wohua Pharmaceuticals, Shandong, China) | Codonopsis Pilosulae Radix, Cinnamomi Ramulus, Paeoniae Radix Alba, Glycyrrhizae Radix, Hoelen, Zingiberis Rhizoma, Polygalae Radix, Acori Graminei Rhizoma, Fossilia Ossis Mastodi, Ostreae Concha |
| Wang 2020 [29] | Jiannao Yizhi Formula (Beijing Kangrentang Pharmaceuticals, Beijing, China) | Ginseng Radix, Cnidii Rhizoma, Coptidis Rhizoma, Broussonetiae Fructus |
| Yancheva 2009 [30] | EGb 761® | Ginkgo biloba |
| Zhang 2015c [31] | Yishen Huazhuo Decoction (Shenzhen Sanjiu Modern Chinese Medicine Limited Company, Shenzhen, China) | Epimedii Herba, Ligustri Lucidi Fructus, Psoraleae Semen, Polygoni Multiflori Radix, Astragali Radix, Cnidii Rhizoma, Acori Graminei Rhizoma |
| Chen 2011a [32] | Bu Yuan Cong Nao Tang | Lycii Fructus, Polygoni Multiflori Radix, Psoraleae Semen, Cistanches Herba, Alpiniae Oxyphyllae Fructus, Astragali Radix, Acori Graminei Rhizoma, Curcumae Radix, Salviae Miltiorrhizae Radix, Cnidii Rhizoma, Pinelliae Rhizoma, Hirudo, Glycyrrhizae Radix |
| Chen 2011b [33] | Bushen Phlegm Stasis Compound | Astragali Radix, Polygoni Multiflori Radix, Psoraleae Semen, Cistanches Herba, Alpiniae Oxyphyllae Fructus, Acori Graminei Rhizoma, Curcumae Radix, Salviae Miltiorrhizae Radix, Cnidii Rhizoma, Lycii Fructus, Pinelliae Rhizoma, Hirudo, Glycyrrhizae Radix |
| Chen 2010 [34] | Compound Polygonum multiflorum extract | Polygoni Multiflori Radix, Polygonati Rhizoma, Morindae Radix, Angelicae Gigantis Radix, Alpiniae Oxyphyllae Fructus, Ginkgo Folium, Acori Graminei Rhizoma |
| Cheng 2013 [35] | Yangxueqingnao Granule (Tianjin Tasly Pharmaceuticals, Tianjin, China) | Angelicae Gigantis Radix, Cnidii Rhizoma, Cassiae Semen, Margaritifera Usta Concha, Rehmanniae Radix Preparata |
| Chi 2018 [36] | Bushen Tianjing Yisui Prescription | Astragali Radix, Folium Callicarpae Formosanae, Codonopsis Pilosulae Radix, Coicis Semen, Polygoni Multiflori Radix, Hoelen, Corni Fructus, Psoraleae Semen, Curculiginis Rhizoma, Spatholobi Caulis, Epimedii Herba, Angelicae Gigantis Radix, Crataegi Fructus, Cuscutae Semen, Rehmanniae Radix Preparata, Dioscoreae Rhizoma, Polygonati Rhizoma, Agrimoniae Herba, Saposhnikoviae Radix, Cervi Cornu, Sanguisorbae Radix, Morindae Radix, Cinnamomi Cortex |
| Gong 2019 [37] | “Reinforcing Kidney and Removing Blood Stasis” Formula | Alpiniae Oxyphyllae Fructus, Polygoni Multiflori Radix, Acori Graminei Rhizoma, Ginseng Radix, Epimedii Herba, Puerariae Radix, Paeoniae Radix Rubra, Salviae Miltiorrhizae Radix |
| Gu 2014 [38] | Dihuang Yizhi Formula | Rehmanniae Radix Preparata, Hominis Placenta, Salviae Miltiorrhizae Radix, Acori Graminei Rhizoma, Testudinis Plastrum, Hoelen Cum Radix, Alpiniae Oxyphyllae Fructus |
| Gu 2019 [39] | Yizhi Chidai Recipe | Rehmanniae Radix, Corni Fructus, Astragali Radix, Acori Graminei Rhizoma, Polygalae Radix, Curcumae Radix, Angelicae Gigantis Radix, Cnidii Rhizoma, Alpiniae Oxyphyllae Fructus, Cervi Cornus Colla, Rhei Rhizoma |
| Guan 2017 [40] | Di Yong Yizhi Granule | Rehmanniae Radix Preparata, Cistanches Herba, Morindae Radix, Codonopsis Pilosulae Radix, Liriopis Tuber, Cuscutae Semen, Zizyphi Spinosae Semen, Polygalae Radix, Lumbricus, Citri Pericarpium Hoelen, Salviae Miltiorrhizae Radix, Acori Graminei Rhizoma, Glycyrrhizae Radix |
| Guo 2011 [41] | Zhibai Dihuang Tang | Anemarrhenae Rhizoma, Phellodendri Cortex, Rehmanniae Radix Preparata, Corni Fructus, Dioscoreae Rhizoma, Alismatis Rhizoma, Hoelen, Moutan Cortex Radicis |
| Hu 2015 [42] | Bushen Tongluo Decoction | Polygonati Rhizoma, Rehmanniae Radix Preparata, Polygoni Multiflori Radix, Epimedii Herba, Cuscutae Semen, Ginseng Radix, Salviae Miltiorrhizae Radix, Notoginseng Radix, Polygalae Radix, Cnidii Rhizoma, Citri Pericarpium, Ginkgo Folium + additional herbs based on pattern identification |
| Huang 2018 [43] | Bushenyisui Formula (China Resources Sanjiu Medical & Pharmaceuticals, Shenzhen, China) | Psoraleae Semen, Astragali Radix, Epimedii Herba, Acori Graminei Rhizoma, Polygoni Multiflori Radix, Ligustri Lucidi Fructus, Cnidii Rhizoma |
| Jiang 2018 [44] | Jiannao Powder | Ginseng Radix, Cervi Parvum Cornu, Strychni Semen, Lumbricus, Hominis Placenta, Glycyrrhizae Radix, Lycii Fructus, Alpiniae Oxyphyllae Fructus, Gastrodiae Rhizoma, Scorpio, Galli Stomachichum Corium, Eupolyphaga, Angelicae Gigantis Radix, Cnidii Rhizoma, Curcumae Radix, Carthami Flos |
| Li 2015 [45] | Bupi Yishen Decoction | Rehmanniae Radix Preparata, Corni Fructus, Polygoni Multiflori Radix, Lycii Fructus, Cuscutae Semen, Epimedii Herba, Ginseng Radix, Atractylodis Rhizoma Alba, Hoelen, Acori Graminei Rhizoma, Cnidii Rhizoma, Angelicae Gigantis Radix |
| Li 2018a [46] | Congrong Yizhi Capsules (Liao Yuan YuLong YaDong Pharmaceuticals, Liaoyuan, China) | Polygoni Multiflori Radix, Lumbricus, Nelumbinis folium, Echinopsis Radix, Cistanches Herba |
| Li 2016a [47] | Renshen Bujing Anshen Formula | Ginseng Radix, Dioscoreae Rhizoma, Angelicae Gigantis Radix, Hoelen, Cistanches Herba, Mori Fructus, Margaritifera Usta Concha, Rehmanniae Radix Preparata, Zizyphi Spinosae Semen, Cnidii Rhizoma, Fossilia Dentis Mastodi, Scutellariae Radix, Citri Pericarpium, Persicae Semen + additional herbs based on pattern identification |
| Li 2016b [48] | Huang Cong Formula | Rehmanniae Radix Preparata, Corni Fructus, Morindae Radix, Liriopis Tuber, Moutan Cortex Radicis, Alismatis Rhizoma, Hoelen Cum Radix, Acori Graminei Rhizoma, Notoginseng Radix, Achyranthis Radix, Glycyrrhizae Radix |
| Li 2016c [49] | Tonifying Kidney Prescription | Epimedii Herba, Psoraleae Semen, Polygoni Multiflori Radix, Astragali Radix, Cnidii Rhizoma, Ligustri Lucidi Fructus, Acori Graminei Rhizoma |
| Li 2014 [50] | Bushen Huoxue Decoction | Astragali Radix, Ligustri Lucidi Fructus, Ecliptae Herba, Eucommiae Cortex, Rubi Fructus, Curculiginis Rhizoma, Epimedii Herba, Cnidii Rhizoma, Salviae Miltiorrhizae Radix, Paeoniae Radix Rubra, Trogopterorum Faeces, Typhae Pollen |
| Li 2018b [51] | Bushen Yizhi Formula | Rehmanniae Radix Preparata, Lycii Fructus, Cnidii Rhizoma, Cnidii Fructus, Salviae Miltiorrhizae Radix, Polygoni Multiflori Radix, Acori Graminei Rhizoma, Ginseng Radix, Glycyrrhizae Radix, Ligustri Lucidi Fructus, Hirudo, Polygalae Radix |
| Li 2017 [52] | Modified Shuyu Pill | Dioscoreae Rhizoma, Rehmanniae Radix Preparata, Eucommiae Cortex, Lycii Fructus, Hoelen, Polygalae Radix, Acori Graminei Rhizoma |
| Li 2002 [53] | Danggui Shaoyao San | Angelicae Gigantis Radix, Cnidii Rhizoma, Paeoniae Radix Alba, Atractylodis Rhizoma Alba, Hoelen, Alismatis Rhizoma + additional herbs based on pattern identification |
| Liang 2010 [54] | Bushenyizhi Granule (Jiangyin Tianjiang Pharmaceuticals, Jiangyin, China) | Rehmanniae Radix Preparata, Morindae Radix, Cistanches Herba, Epimedii Herba, Dendrobii Herba, Liriopis Tuber, Hoelen, Salviae Miltiorrhizae Radix, Lumbricus, Corni Fructus, Acori Graminei Rhizoma, Polygalae Radix, Schisandrae Fructus, Cnidii Rhizoma, Hirudo |
| Lin 2006 [55] | 1. Taioxin 2. Bushen | 1. Taioxin: Codonopsis Pilosulae Radix, Polygalae Radix, Hoelen, Cinnamomi Ramulus, Acori Graminei Rhizoma 2. Bushen: Rehmanniae Radix, Lycii Fructus, Corni Fructus, Liriopis Tuber |
| Lin 2017 [56] | Phlegm-resolving Orifice-Opening Decoction | Arisaematis Rhizoma, Pinelliae Rhizoma, Lumbricus, Astragali Radix, Cistanches Herba, Hoelen, Acori Graminei Rhizoma, Polygalae Radix, Citri Pericarpium, Mume Fructus, Glycyrrhizae Radix |
| Lin 2018 [57] | Bu Shen Yi Sui Decoction | Epimedii Herba, Psoraleae Semen, Polygoni Multiflori Radix, Ligustri Lucidi Fructus, Cnidii Rhizoma, Acori Graminei Rhizoma |
| Liu 2010 [58] | Yizhi Jiannao Granule (Hunan Dekang Pharmaceuticals, Hunan, China) | Epimedii Herba, Cynomorii Herba, Dipsaci Radix, Acanthopanacis Cortex, Biotae Semen, Hirudo, Notoginseng Radix |
| Peng 2009 [59] | Yizhi Jiannao Granule (Hunan Dekang Pharmaceuticals, Hunan, China) | Epimedii Herba, Cynomorii Herba, Dipsaci Radix, Acanthopanacis Cortex, Biotae Semen, Hirudo, Notoginseng Radix |
| Shan 2017 [60] | Bushen Yizhi Granule | Rehmanniae Radix Preparata, Dendrobii Herba, Cistanches Herba, Morindae Radix, Liriopis Tuber, Lumbricus, Epimedii Herba, Hoelen, Salviae Miltiorrhizae Radix, Acori Graminei Rhizoma, Schisandrae Fructus, Corni Fructus, Cnidii Rhizoma, Polygalae Radix, Hirudo |
| Wu 2018 [61] | Huonaoshu Capsules (Huinan Changlong Biochemical Pharmaceuticals, Huinan, China) | Pig’s brain, Ginseng Radix, Liriopis Tuber, Schisandrae Fructus, Lycii Fructus, Rehmanniae Radix, Salviae Miltiorrhizae Radix |
| Yang 2013 [62] | Yizhi Jiannao Granule (Hunan Dekang Pharmaceuticals, Hunan, China) | Epimedii Herba, Cynomorii Herba, Dipsaci Radix, Acanthopanacis Cortex, Biotae Semen, Hirudo, Notoginseng Radix |
| Yang 2018a [62] | Ma Huang Fu Zi Xi Xin Tang | Aconiti Lateralis Preparata Radix, Ephedrae Herba, Asia Radix, Zingiberis Rhizoma, Cinnamomi Cortex, Paeoniae Radix Alba, Gastrodiae Rhizoma, Epimedii Herba, Morindae Radix, Cuscutae Semen, Lycii Fructus, Glycyrrhizae Radix + additional herbs based on pattern identification |
| Yu 2012 [64] | Herbal medicine based on syndrome differentiation | Prescription based on syndrome differentiation (pattern identification) |
| Yang 2018b [65] | Tiaoxin (Jiangsu Tianjiang Pharmaceuticals, Jiangsu, China) | Astragali Radix, Acori Graminei Rhizoma, Polygalae Radix, Glycyrrhizae Radix, Bupleuri Radix |
| Yu 2006 [66] | “Reinforcing kidney, activating blood and resolving phlegm” Formula | Polygoni Multiflori Radix, Ligustri Lucidi Fructus, Polygonati Rhizoma, Cnidii Fructus, Sesami Semen Nigrum, Rehmanniae Radix Preparata, Alpiniae Oxyphyllae Fructus, Salviae Miltiorrhizae Radix, Cnidii Rhizoma, Paeoniae Radix Rubra, Acori Graminei Rhizoma, Arisaematis Rhizoma, Persicae Semen, Lumbricus, Carthami Flos, Puerariae Radix, Hirudo, Notoginseng Radix, Pinelliae Rhizoma |
| Yuan 2017 [67] | Bushen Yizhi Granule | Hirudo, Rehmanniae Radix Preparata, Cnidii Rhizoma, Morindae Radix, Schisandrae Fructus, Cistanches Herba, Polygalae Radix, Epimedii Herba, Acori Graminei Rhizoma, Dendrobii Herba, Corni Fructus, Liriopis Tuber, Lumbricus, Salviae Miltiorrhizae Radix, Hoelen |
| Zhang 2015b [67] | Shen Gui Yizhi Formula | Ginseng Radix, Angelicae Gigantis Radix, Polygoni Multiflori Radix, Astragali Radix, Salviae Miltiorrhizae Radix, Cnidii Rhizoma, Paeoniae Radix Rubra, Hirudo, Rehmanniae Radix Preparata, Cuscutae Semen, Pinelliae Rhizoma, Hoelen, Glycyrrhizae Radix |
| Zhang 2015a [69] | Yizhi Xingnao Fang | Ginseng Radix, Gastrodiae Rhizoma, Scutellariae Radix, Rhodiola Rosea, Acori Graminei Rhizoma, Alpiniae Oxyphyllae Fructus, Lumbricus |
| Zhang 2018b [70] | Qingxin Yizhi Decoction | Astragali Radix, Zizyphi Spinosae Semen, Lumbricus, Cannabis Semen, Paeoniae Radix Rubra, Alpiniae Oxyphyllae Fructus, Angelicae Gigantis Radix, Persicae Semen, Cinnamomi Ramulus, Glycyrrhizae Radix + additional herbs based on pattern identification |
| Zhang 2018c [71] | Dihuang Yinzi Decoction (China Resources Sanjiu Pharmaceuticals, Shenzhen, China) | Polygalae Radix, Acori Graminei Rhizoma, Rehmanniae Radix Preparata, Corni Fructus, Liriopis Tuber, Schisandrae Fructus, Dendrobii Herba, Cistanches Herba, Morindae Radix, Aconiti Lateralis Preparata Radix, Cinnamomi Cortex, Hoelen, Zingiberis Rhizoma Crudus, Jujubae Fructus, Menthae Herba |
| Zhang 2008 [72] | Shenghuangyizhi Granule | Cimicifugae Rhizoma, Astragali Radix, Ginseng Radix, Testudinis Plastrum |
| Zhang 2018a [73] | Compound Danshen Tablet (Beijing Tongrentang Technology Development Co., Beijing, China) | Salviae Miltiorrhizae Radix, Notoginseng Radix, Borneolum Syntheticum |
| Zhou 2007 [74] | Reinhartdt and Sea Cucumber Capsule (Zhejiang Hangkang Marine Biopharmaceuticals, Zhejiang, China) | Stichopus, Stichopus, Polygalae Radix, Acori Graminei Rhizoma |
| Zhu 2010 [75] | Yizhi Jiannao Granule (Hunan Dekang Pharmaceuticals, Hunan, China) | Epimedii Herba, Cynomorii Herba, Dipsaci Radix, Acanthopanacis Cortex, Biotae Semen, Hirudo, Notoginseng Radix |
| Wang 2018 [76] | Bushen Huatan Yizhi Decoction | Polygonati Rhizoma, Cistanches Herba, Alpiniae Oxyphyllae Fructus, Salviae Miltiorrhizae Radix, Hoelen Cum Radix, Curcumae Radix, Acori Graminei Rhizoma, Eucommiae Cortex, Polygalae Radix, Cnidii Rhizoma, Gastrodiae Rhizoma, Hominis Placenta, Glycyrrhizae Radix |
Appendix C







Appendix D





References
- Alzheimer’s Disease International. World Alzheimer Report 2014—Dementia and Risk Reduction: An Analysis of Protective and Modifiable Factors. Available online: https://www.alzint.org/u/WorldAlzheimerReport2014.pdf (accessed on 1 December 2020).
- Alzheimer’s Disease International. World Alzheimer Report 2018—The State of the Art of Dementia Research: New Frontiers. Available online: https://www.alzint.org (accessed on 1 December 2020).
- Lane, C.A.; Hardy, J.; Schott, J.M. Alzheimer’s disease. Eur. J. Neurol. 2018, 25, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Weller, J.; Budson, A. Current understanding of Alzheimer’s disease diagnosis and treatment. F1000Research 2018, 7, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, G.P.; Clark, I.A.; Vissel, B. Inconsistencies and controversies surrounding the amyloid hypothesis of Alzheimer’s disease. Acta Neuropathol. Commun. 2014, 2, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briggs, R.; Kennelly, S.P.; O’Neill, D. Drug treatments in Alzheimer’s disease. Clin. Med. J. R Coll. Phys. London 2016, 16, 247–253. [Google Scholar] [CrossRef]
- Panza, F.; Lozupone, M.; Logroscino, G.; Imbimbo, B.P. A critical appraisal of amyloid-β-targeting therapies for Alzheimer disease. Nat. Rev. Neurol. 2019, 15, 73–88. [Google Scholar] [CrossRef]
- Filling the void for new Alzheimer ’s disease. Nat. Aging 2021, 1, 567–568. [CrossRef]
- Ho, Y.S.; So, K.F.; Chang, R.C. Drug discovery from Chinese medicine against neurodegeneration in Alzheimer’s and vascular dementia. Chin. Med. 2011, 6, 15. [Google Scholar] [CrossRef] [Green Version]
- Jeon, S.G.; Song, E.J.; Lee, D.; Park, J.; Nam, Y.; Kim, J.; Moon, M. Traditional oriental medicines and Alzheimer’s disease. Aging Dis. 2019, 10, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.S.; Kim, Y.J.; Sohn, E.; Yoon, J.; Kim, B.Y.; Jeong, S.J. Bojungikgi-tang, a traditional herbal formula, exerts neuroprotective effects and ameliorates memory impairments in alzheimer’s disease-like experimental models. Nutrients 2018, 10, 1952. [Google Scholar] [CrossRef] [Green Version]
- Kaushik, R.; Morkovin, E.; Schneeberg, J.; Confettura, A.D.; Kreutz, M.R.; Senkov, O.; Dityatev, A. Traditional Japanese herbal medicine Yokukansan targets distinct but overlapping mechanisms in aged mice and in the 5xFAD mouse model of Alzheimer’s disease. Front. Aging Neurosci. 2018, 10, 1–17. [Google Scholar] [CrossRef]
- Suzuki, T.; Futami, S.; Igari, Y.; Matsumura, N.; Watanabe, K.; Nakano, H.; Kigawa, Y. A Chinese herbal medicine, choto-san, improves cognitive function and activities of daily living of patients with dementia: A double-blind, randomized, placebo-controlled study. J. Am. Geriatr. Soc. 2005, 53, 2338–2340. [Google Scholar] [CrossRef] [PubMed]
- Watari, H.; Shimada, Y.; Matsui, M.; Tohda, C. Kihito, a traditional Japanese Kampo medicine, improves cognitive function in Alzheimer’s disease patients. Evid-Based Complement. Altern. Med. 2019, 2019, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, J.; Ni, J.; Lu, T.; Zhang, X.; Wei, M.; Li, T.; Liu, W.; Wang, Y.; Shi, Y.; Tian, J. Adding Chinese herbal medicine to conventional therapy brings cognitive benefits to patients with Alzheimer’s disease: A retrospective analysis. BMC Complement. Altern. Med. 2017, 17, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Jin, C.; Cho, S.-Y.; Park, S.-U.; Jung, W.-S.; Moon, S.-K.; Park, J.-M.; Ko, C.-N.; Cho, K.-H.; Kwon, S. Herbal medicine treatment for Alzheimer disease. Medicine 2020, 99, e21745. [Google Scholar] [CrossRef] [PubMed]
- PRISMA. Preferred Reporting Items for Ssystematic Reviews and Meta-Analyses (PRISMA). Available online: http://www.prismastatement.org. (accessed on 1 December 2020).
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Available online: http://handbook.cochrane.org. (accessed on 1 December 2020).
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furuhashi, Y.; Shin, K. Risperidone versus Yokukansan in the treatment of severe Alzheimer’s disease. Int. J. Clin. Med. 2011, 02, 166–170. [Google Scholar] [CrossRef] [Green Version]
- Furukawa, K.; Tomita, N.; Uematsu, D.; Okahara, K.; Shimada, H.; Ikeda, M.; Matsui, T.; Kozaki, K.; Fujii, M.; Ogawa, T.; et al. Randomized double-blind placebo-controlled multicenter trial of Yokukansan for neuropsychiatric symptoms in Alzheimer’s disease. Geriatr. Gerontol. Int. 2017, 17, 211–218. [Google Scholar] [CrossRef]
- Heo, J.H.; Lee, S.T.; Chu, K.; Oh, M.J.; Park, H.J.; Shim, J.Y.; Kim, M. An open-label trial of Korean red ginseng as an adjuvant treatment for cognitive impairment in patients with Alzheimer’s disease. Eur. J. Neurol. 2008, 15, 865–868. [Google Scholar] [CrossRef]
- Lee, S.T.; Chu, K.; Sim, J.Y.; Heo, J.H.; Kim, M. Panax ginseng enhances cognitive performance in Alzheimer disease. Alzheimer Dis. Assoc. Disord. 2008, 22, 222–226. [Google Scholar] [CrossRef]
- Liu, P.; Kong, M.; Liu, S.; Chen, G.; Wang, P. Effect of reinforcing kidney-essence, removing phlegm, and promoting mental therapy on treating Alzheimer’s disease. J. Tradit. Chin. Med. 2013, 33, 449–454. [Google Scholar] [CrossRef] [Green Version]
- Mazza, M.; Capuano, A.; Bria, P.; Mazza, S. Ginkgo biloba and donepezil: A comparison in the treatment of Alzheimer’s dementia in a randomized placebo-controlled double-blind study. Eur. J. Neurol. 2006, 13, 981–985. [Google Scholar] [CrossRef] [PubMed]
- Meng, R.S.; Li, Q.M.; Wei, C.X.; Chen, B.; Liao, H.Y.; Zhou, Y.T. Clinical observation and mechanism study on treatment of senile dementia with Naohuandan. Chin. J. Integr. Med. 2005, 11, 111–116. [Google Scholar] [PubMed]
- Pakdaman, H.; Harandi, A.A.; Hatamian, H.; Tabatabae, M.; Kasmaei, H.D.; Ghassemi, A.; Gharagozli, K.; Ashrafi, F.; Naeini, P.E.; Tavakolian, M.; et al. Effectiveness and safety of MLC601 in the treatment of mild to moderate Alzheimer’s disease: A multicenter, randomized controlled trial. Dement. Geriatr. Cogn. Disord. Extra 2015, 5, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Pan, W.; Wang, Q.; Kwak, S.; Song, Y.; Qin, B.; Wang, M.; Yamamoto, Y. Shen-Zhi-Ling oral liquid improves behavioral and psychological symptoms of dementia in Alzheimer’s disease. Evid.-Based Complement. Altern. Med. 2014, 2014, 913687. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Liu, N.; Zhang, S.; Yang, Y.; Wang, Z.Y.; Wei, Y. Clinical experience in treatment of Alzheimer’s disease with Jiannao Yizhi Formula (健脑益智方) and routine western medicine. Chin. J. Integr. Med. 2020, 26, 212–218. [Google Scholar] [CrossRef]
- Yancheva, S.; Ihl, R.; Nikolova, G.; Panayotov, P.; Schlaefke, S.; Hoerr, R. Ginkgo biloba extract EGb 761, donepezil or both combined in the treatment of Alzheimer’s disease with neuropsychiatric features: A randomised, double-blind, exploratory trial. Aging Ment. Health 2009, 13, 183–190. [Google Scholar] [CrossRef]
- Zhang, Y.; Lin, C.; Zhang, L.; Cui, Y.; Gu, Y.; Guo, J.; Wu, D.; Li, Q.; Song, W. Cognitive improvement during treatment for mild Alzheimer’s disease with a Chinese herbal formula: A randomized controlled trial. PLoS ONE 2015, 10, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Chen, L. Clinical Study on the Treatment of Senile Dementia with Kidney Deficiency and Phlegm-Blood Stasis by Bu Yuan Cong Nao Tang. Master’s Thesis, Liaoning University of Traditional Chinese, Liaoning, China, 2011. [Google Scholar]
- Chen, L.; Chen, M.; Liu, Z. Kidney Phlegm Stasis Compound treatment of Alzheimer disease clinical observation. J. Liaoning Univ. TCM 2011, 13, 190–191. [Google Scholar]
- Chen, L.; Huang, J.; Xue, L. Effect of Compound Polygonum Multiflorum Extract on Alzheimer’s disease. J. Cent. South Univ. 2010, 35, 612–615. [Google Scholar]
- Cheng, X.; Zang, D. Effect of nourishing Yangxueqingnao Granule combined with Donepezil on cognitive function and abnormal mental behavior in AD patients. Shandong Med. J. 2013, 53, 56–57. [Google Scholar]
- Chi, S.; Shen, Y. Clinical study on Bushen Tianjing Yisui Prescription combined with western medicine for Alzheimer’s disease. J. New Chin. Med. 2018, 50, 71–74. [Google Scholar]
- Gong, W.; He, J.; Mei, J.; Xia, X.; Xiao, X. Clinical observation on treatment of geriatric dementia by reinforcing kidney and removing blood stasis. Hubei J. TCM 2019, 41, 33–34. [Google Scholar]
- Gu, C.; Yuan, C.; Shen, T.; Ye, Q.; Liu, T.; An, H. A clinical observation on Dihuang Yizhi Formula combined with donepezil for 50 patients with Alzheimer’s disease. J. Tradit. Chin. Med. 2014, 55, 482–485. [Google Scholar]
- Gu, Z. The Clinical Research on Alzheimer’s Disease of Kidney Essence Deficieny Treated with Yizhi Chidai Recipe. Master’s Thesis, Xinjiang Medical University, Xinjiang, China, 2019. [Google Scholar]
- Guan, Y. Clinical study on comprehensive therapy for Alzheimer’s disease. Asia-Pac. Tradit. Med. 2017, 13, 113–114. [Google Scholar]
- Guo, Z.; Chen, X.; Xing, B.; Luo, K.; Shen, Y. Treatment of senile dementia with Zhibai Dihuang Tang and donepezil in 30 cases. Zhejiang JITCWM 2011, 21, 471–472. [Google Scholar]
- Hu, X.; Yu, C.; Li, J.; Wang, Y.; Zhou, J.; Cheng, W. Clinical analysis of Bushen Tongluo Decoction in treating 40 patients with Alzheimer disease. Chin. J. Exp. Tradit. Med. Formulae 2015, 21, 182–185. [Google Scholar]
- Huang, K.; Gu, Y.; Han, S.; Sun, G. Clinical effect of the treatment with Bushenyisui Formula on Alzheimer’s disease. Geriatr. Health Care 2018, 24, 26–29. [Google Scholar]
- Jiang, W.; Geng, B.; Wang, D.; Shan, F.; Wang, Y. Clinical observation of Jiannao Powder combined with donepezil in treating Alzheimer’s disease. Clin. J. Chin. Med. 2018, 27, 9–12. [Google Scholar]
- Li, H. Effect of Bupi Yishen Decoction in treating 35 Cases with Alzheimer’s disease. Chin. J. Exp. Tradit. Med. Formulae 2015, 21, 193–196. [Google Scholar]
- Li, H.; Ma, M.; Li, A.; Fu, G.; Huang, J.; Huang, L. Clinical study on Compoung Congrong Yizhi Capsules combined with rivastigmine in treatment of Alzheimer’s disease. Drugs Clin. 2018, 33, 2213–2217. [Google Scholar]
- Li, H.; Wang, Q.; Liu, L.; Bi, L.; Liu, S.; Liu, J. Application and effect of Renshen Bujing Anshen Formula with donepezil in the treatment of dementia. Hebei Med. J. 2016, 38, 3315–3320. [Google Scholar]
- Li, Q. Clinical Observation of Self-Designed Huang Cong Formula Combined with Donepezil in the Treatment of Alzheimer’s Disease. Master’s Thesis, Guangxi University of Chinese Medicine, Guangxi, China.
- Li, Q.; Zhang, Y.; Lin, C.; Guo, J.; Gu, Y.; Wu, D.; Zhang, L. Clinical observation of Tonifying Kidney Prescription for treating kidney deficiency of senile dementia. J. Basic Chin. Med. 2016, 22, 1065–1067. [Google Scholar]
- Li, T.; Mo, G.; Zhang, Y. Clinical observation of 65 cases of Bushen Huoxue Decoction for senile dementia. Pract. Geriatr. 2014, 28, 867–868. [Google Scholar]
- Li, W.; Huang, S.; Zhu, Y. Clinical effect of Bushen Yizhi Formula combined with clozapine on Alzheimer’s disase complicated with behavior disorders. Guangxi Med. J. 2018, 44, 2682–2687. [Google Scholar]
- Li, X. A Clinical Study on Mild and Moderate Alzheimer’s Disease of Kidney Deficiency and Marrow Depletion Syndrome Treated with Modified Shuyu Pill. Master’s Thesis, Hubei University of Chinese Medicine, Hubei, China, 2017. [Google Scholar]
- Li, Z.; Mu, Y.; Ouyang, Q. Clinic control research of Alzheimer’s disease by the combination of acupuncture and Danggui Shaoyao San (DGSYS) of TCM. Chin. J. Clin. Rehabil. 2002, 6, 2848–2849. [Google Scholar]
- Liang, J.; Tan, C.; Yang, B. Clinical observation on Bushenyizhi Granule combined with western medicine in treatment of Alzheimer’s disease. Chin. J. Integr. Med. Cardio/Cerebrovasc. Dis. 2010, 8, 39–41. [Google Scholar]
- Lin, S.; Wang, J.; Zhou, R.; Yu, Z. Clinical effect in treatment of Alzheimer disease based on the conditions of heart and kidney. Chin. J. Clin. Rehabil. 2006, 10, 162–164. [Google Scholar]
- Lin, Y. Efficacy of Phlegm-Resolving Orifice-Opening Decoction for Alzheimer’s Disease Patients with Phlegm-Turbidity Obstructing Orifices. Master’s Thesis, Fujian University of Tradtional Chinese Medicine, Fujian, China, 2017. [Google Scholar]
- Lin, Y.; Huang, K.; Han, S.; Gu, T. The influence of Bu Shen Yi Sui Decoction to the patients with Alzheimer’s disease on the symptoms and level of endocrine. Chin. J. Alzheimers Dis. Relat. Disord. 2018, 1, 33–37. [Google Scholar]
- Liu, P.; Dong, K. The effect of Yizhi Jiannao Granule on Il-1β and TNF-α expression in peripheral blood serum in patients with Alzheimer’s disease. Hunan J. Tradit. Chin. Med. 2010, 26, 1–3. [Google Scholar]
- Peng, X.; Dong, K. Clinical observation on acupuncture combined with Yizhi Jiannao Granules for treatment of Alzheimer’s disease. Chin. Acupunct. Moxibustion 2009, 29, 269–271. [Google Scholar]
- Shan, X.; Gou, C.; Hu, K. Analysis of clinical curative effect of donepezil hydrochloride tablets and Bushen Yizhi Granules in treatment of Alzheimer’s disease. China Foreign Med. Treat. 2017, 15, 15–17. [Google Scholar]
- Wu, W. Clinical observation of Compound Huonaoshu Capsules combined with donepezil in treatment of mild and moderate Alzheimer’s disease. Drugs Clin. 2018, 33, 2867–2871. [Google Scholar]
- Yang, P.; Dong, K. Clinical study of Yizhi Jiannao Granule in Alzheimer’s disease. J. New Chin. Med. 2013, 45, 56–58. [Google Scholar]
- Yang, X.; Du, S.; Zhang, L.; Yang, J.; Luo, Q. Clinical study of 30 cases of senile dementia treated with Ma Huang Fu Zi Xi Xin Tang combined with Donepezil. Jiangsu J. Tradit. Chin. Med. 2018, 50, 33–35. [Google Scholar]
- Yu, L.; Lin, S.; Zhou, R.; Tang, W.; Huang, P.; Dong, Y.; Wang, J.; Yu, Z.; Chen, J.; Wei, L.; et al. Chinese herbal medicine for patients with mild to moderate Alzheimer disease based on syndrome differentiation: A randomized controlled trial. J. Chin. Integr. Med. 2012, 10, 766–776. [Google Scholar] [CrossRef]
- Yang, X.; Li, N.; Xu, S.; Xu, L.; Lou, D.; Wang, J. Effacacy observation on Tiaoxin Prescription in treatment of mild Alzheimer disease. Acta Chin. Med. 2018, 33, 2020–2024. [Google Scholar]
- Yu, X. Clinical Observation on the Treatment of 42 Cases of Senile Dementia With the Method of Tonifying Kidney and Activating Blood and Dissipating Phlegm. Guid. J. TCM 2006, 12, 24–25. [Google Scholar]
- Yuan, H.; Zhang, J. Clinical observation on treating AD in TCM. Clin. J. Chin. Med. 2017, 9, 93–95. [Google Scholar]
- Zhang, H.; Zhao, H.; Liu, Y.; Zhang, X.; Sheng, X. Clinical observation on the treatment of Alzheimer’s disease by Shen Gui Yizhi Formula with Butylphthalide. Chin. Foreign Med. Res. 2015, 13, 43–45. [Google Scholar]
- Zhang, J. A Clinical Curatvie Effect Observation on Mild and Moderate Alzheimer’s Disease of Phlegm Turbidity Type Treated by Yizhi Xingnao Fang. Master’s Thesis, Shangdong University of Traditional Chinese Medicine, Shangdong, China, 2015. [Google Scholar]
- Zhang, L.; Peng, J. Qingxin Yizhi Decoction on improvig the quality of life, cognitive level and the biochemical indexes of SOD and MDA in AD patients. Shaanxi J. Tradit. Chin. Med. 2018, 39, 593–595. [Google Scholar]
- Zhang, L.; Wang, Y.; Zhou, J.; Ke, B.; Yang, Y.; Qin, J.; Huang, Y. Effects and mechanisms of Dihuang Yinzi Decoction on the treatment of Alzheimer’s disease patients. China J. Tradit. Chin. Med. Pharm. 2018, 33, 4948–4952. [Google Scholar]
- Zhang, Q.; Wei, J. Clinical observation on the treatment of Alzheimer’s disease by Shenghuangyizhi granule. J. Shandong Univ TCM. 2008, 32, 303–305. [Google Scholar]
- Zhang, W.; Hu, C.; Lu, Y.; Fu, M.; Liang, M. Study of Compound Danshen Tablets combined with donepezil on Alzheimer’s disease. China J. Mod. Med. 2018, 28, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Liang, L.; Yan, Y. Clinical study of Reinhartdt and Sea Cucumer Capsule combined with donepezil in treating Alzheimer’s disease. Chin. J. Integr. Tradit. West Med. 2007, 27, 110–113. [Google Scholar]
- Zhu, H.; Dong, K.; Wu, Y.; Zhang, T.; Li, R.; Hu, S.; Wang, H. Effect of reinforcing kidney and activating blood on cognitive function improvement in Alzheimer’s patients. Chin. J. Gerontol. 2010, 30, 1493–1495. [Google Scholar]
- Wang, S.; Zhang, X.; Ma, Y.; Zhao, J. Clinical efficacy of Bushen Huatan Yizhi Decoction combined with Butylphthalide and effect on oxidative stress, hemorheology and cognitive function in patients with Alzheimer’s disease. Chin. J. Exp. Tradit. Med. Formulae 2018, 24, 212–216. [Google Scholar]
- Eratne, D.; Loi, S.M.; Farrand, S.; Kelso, W.; Velakoulis, D.; Looi, J.C.L. Alzheimer’s disease: Clinical update on epidemiology, pathophysiology and diagnosis. Australas Psychiatry 2018, 26, 347–357. [Google Scholar] [CrossRef]
- Bredesen, D. The End of Alzheimer’s: The First Program to Prevent and Reverse Cognitive Decline; Avery, an Imprint of Penguin Random House: New York, NY, USA, 2017; pp. 7–9. [Google Scholar]
- FDA. FDA’s Decision to Approve New Treatment for Alzheimer’s Disease. Available online: https://www.fda.gov/drugs/news-events-human-drugs/fdas-decision-approve-new-treatment-alzheimers-disease (accessed on 24 July 2021).
- Knopman, D.S.; Jones, D.T.; Greicius, M.D. Failure to demonstrate efficacy of aducanumab: An analysis of the EMERGE and ENGAGE trials as reported by Biogen, December 2019. Alzheimers Dement. 2020, 17, 696–701. [Google Scholar] [CrossRef]
- Nature. Landmark Alzheimer’s Drug Approval Confounds Research Community. Available online: https://www.nature.com/articles/d41586-021-01546-2 (accessed on 24 July 2021).
- Xiang, Y.; Shang, H.; Gao, X.; Zhang, B. A comparison of the ancient use of Ginseng in traditional Chinese medicine with modern pharmacological experiments and clinical trials. Phyther. Res. 2008, 22, 851–858. [Google Scholar] [CrossRef]
- Yang, S. The Divine Farmer’s Materia Medica: A Translation of the Shen Nong Ben Cao Jing; Blue Poppy Press: Boulder, CO, USA, 1998; p. 21. [Google Scholar]
- May, B.H.; Lu, C.; Lu, Y.; Zhang, A.L.; Xue, C.C.L. Chinese Herbs for Memory Disorders: A Review and Systematic Analysis of Classical Herbal Literature. JAMS J. Acupunct. Meridian Stud. 2013, 6, 2–11. [Google Scholar] [CrossRef] [Green Version]
- Song, Z.; Yin, F.; Xiang, B.; Lan, B.; Cheng, S. Systems pharmacological approach to investigate the mechanism of acori tatarinowii rhizoma for Alzheimer’s disease. Evid.-Based Complement. Altern. Med. 2018, 2018, 1–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geng, Y.; Li, C.; Liu, J.; Xing, G.; Zhou, L.; Dong, M.; Li, X.; Niu, Y. Beta-asarone improves cognitive function by suppressing neuronal apoptosis in the beta-amyloid hippocampus injection rats. Biol. Pharm. Bull. 2010, 33, 836–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Xuan, L.; Chen, H.; Dai, S.; Ji, L.; Bao, Y.; Li, C. Neuroprotective Effects and Mechanism of β -Asarone against A β 1-42-Induced Injury in Astrocytes. Evid.-Based Complement. Altern Med. 2017, 2017, 8516518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, X.; Xu, X.; Li, F.; Xie, G.; Zhang, T. Anti-inflammatory treatment with β-asarone improves impairments in social interaction and cognition in MK-801 treated mice. Brain Res. Bull. 2019, 150, 150–159. [Google Scholar] [CrossRef]
- Wang, N.; Wang, H.; Li, L.; Li, Y.; Zhang, R. β-asarone inhibits amyloid-b by promoting autophagy in a cell model of Alzheimer’s disease. Front. Pharmacol. 2020, 10, 01529. [Google Scholar] [CrossRef]
- Saki, G.; Eidi, A.; Mortazavi, P.; Panahi, N.; Vahdati, A. Effect of β-asarone in normal and β-amyloid-induced Alzheimeric rats. Arch. Med. Sci. 2020, 16, 699–706. [Google Scholar] [CrossRef]
- Fan, L.H.; Wang, K.Z.; Cheng, B.; Wang, C.S.; Dang, X.Q. Anti-apoptotic and neuroprotective effects of Tetramethylpyrazine following spinal cord ischemia in rabbits. BMC Neurosci. 2006, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Qin, H.L.; Leng, J.; Ameeduzzafar Amjad, M.W.; Raja, M.A.G.; Hussain, M.A.; Bukhari, S.N.A. Synthesis and biological evaluation of new tetramethylpyrazine-based chalcone derivatives as potential anti-Alzheimer agents. Chem/Biol/Drug Des. 2018, 92, 1859–1866. [Google Scholar] [CrossRef]
- Wu, W.; Yu, X.; Luo, X.P.; Yang, S.H.; Zheng, D. Tetramethylpyrazine protects against scopolamine-induced memory impairments in rats by reversing the cAMP/PKA/CREB pathway. Behav. Brain Res. 2013, 253, 212–216. [Google Scholar] [CrossRef]
- Cheng, X.R.; Zhang, L.; Hu, J.J.; Sun, L.; Du, G.H. Neuroprotective effects of tetramethylpyrazine on hydrogen peroxide-induced apoptosis in PC12 cells. Cell Biol. Int. 2007, 31, 438–443. [Google Scholar] [CrossRef]
- Scheltens, P.; Blennow, K.; Breteler, M.M.B.; de Strooper, B.; Frisoni, G.B.; Salloway, S.; Van Der Flier, W.M. Alzheimer’s disease. Lancet 2016, 388, 505–517. [Google Scholar] [CrossRef]
- Jia, L.; Zhao, Y.; Liang, X. Current evaluation of the millennium phytomedicine—Ginseng (II): Collected chemical entities, modern pharmacology, and clinical applications emanated from traditional Chinese medicine. Curr. Med. Chem. 2009, 16, 2924–2942. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Jung, S.W.; Kim, S.Y.; Cho, I.H.; Kim, H.C.; Rhim, H.; Kim, M.; Nah, S.Y. Panax ginseng as an adjuvant treatment for Alzheimer’s disease. J. Ginseng Res. 2018, 42, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, S.H.; Lee, D.S.; Lee, D.J.; Kim, S.H.; Chung, S.; Yang, H.O. Effects of fermented ginseng on memory impairment and β-amyloid reduction in Alzheimer’s disease experimental models. J. Ginseng Res. 2013, 37, 100–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.S.; Ryu, Y.; Chae, Y. Acupoint selection based on pattern identification results or disease state. Integr. Med. Res. 2020, 9, 100405. [Google Scholar] [CrossRef]
- Kim, S.-H.; Jeong, J.-H.; Lim, J.-H.; Kim, B.-K. Acupuncture using pattern-identification for the treatment of insomnia disorder: A systematic review and meta-analysis of randomized controlled trials. Integr. Med. Res. 2019, 8, 216–226. [Google Scholar] [CrossRef]
- Jung, W.; Park, J.; Moon, S.; Hyun, S. Effect of herbal prescriptions in accordance with pattern identification in acute cerebral infarction patients: Based on fire-heat pattern. Evid.-Based Complement. Altern. Med. 2015, 2015, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Qiu, T.; Liu, Q.; Chen, Y.X.; Zhao, Y.F.; Li, Y.M. Aβ42 and Aβ40: Similarities and differences. J. Pept. Sci. 2015, 21, 522–529. [Google Scholar] [CrossRef]
- Jiao, F.; Yi, F.; Wang, Y.; Zhang, S.; Guo, Y.; Du, W.; Gao, Y.; Ren, J.; Zhang, H.; Liu, L.; et al. The validation of multifactor model of plasma Aβ42 and total-tau in combination with MoCA for diagnosing probable Alzheimer disease. Front. Aging Neurosci. 2020, 12, 212. [Google Scholar] [CrossRef]
- Janelidze, S.; Stomrud, E.; Palmqvist, S.; Zetterberg, H.; Van Westen, D.; Jeromin, A.; Song, L.; Hanlon, D.; Tan Hehir, C.A.; Baker, D.; et al. Plasma β-amyloid in Alzheimer’s disease and vascular disease. Sci. Rep. 2016, 6, 26801. [Google Scholar] [CrossRef]
- Risacher, S.L.; Fandos, N.; Romero, J.; Sherriff, I.; Pesini, P.; Saykin, A.J.; Apostolova, L.G. Plasma amyloid beta levels are associated with cerebral amyloid and tau deposition. Alzheimers Dement. Diagnosis Assess Dis. Monit. 2019, 11, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Shanthi, K.B.; Krishnan, S.; Rani, P. A systematic review and meta-analysis of plasma amyloid 1-42 and tau as biomarkers for Alzheimer’s disease. SAGE Open Med. 2015, 3, 2050312115598250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.H.; Huang, L.C.; Hsieh, S.W.; Huang, L.J. Dynamic Blood Concentrations of Aβ1–40 and Aβ1–42 in Alzheimer’s Disease. Front. Cell Dev. Biol. 2020, 8, 768. [Google Scholar] [CrossRef] [PubMed]
- Hadjichrysanthou, C.; Evans, S.; Bajaj, S.; Siakallis, L.C.; McRae-Mckee, K.; De Wolf, F. The dynamics of biomarkers across the clinical spectrum of Alzheimer’s disease. Alzheimers Res. Ther. 2020, 12, 1–16. [Google Scholar] [CrossRef]
- Fan, L.Y.; Tzen, K.Y.; Chen, Y.F.; Chen, T.F.; Lai, Y.M.; Yen, R.F.; Huang, Y.Y.; Shiue, C.Y.; Yang, S.Y.; Chiu, M.J. The relation between brain amyloid deposition, cortical atrophy, and plasma biomarkers in amnesic mild cognitive impairment and Alzheimer’s Disease. Front. Aging Neurosci. 2018, 10, 175. [Google Scholar] [CrossRef]
- Blennow, K. A Review of Fluid Biomarkers for Alzheimer’s Disease: Moving from CSF to Blood. Neurol. Ther. 2017, 6, 15–24. [Google Scholar] [CrossRef]
- Campbell, N.L.; Perkins, A.J.; Gao, S.; Skaar, T.C.; Li, L.; Hendrie, H.C.; Fowler, N.; Callahan, C.M.; Boustani, M.A. Adherence and tolerability of Alzheimer’s disease medications: A pragmatic randomized trial. J. Am. Geriatr. Soc. 2017, 65, 1497–1504. [Google Scholar] [CrossRef]
- Blanco-Silvente, L.; Castells, X.; Saez, M.; Barceló, M.A.; Garre-Olmo, J.; Vilalta-Franch, J.; Capellà, D. Discontinuation, efficacy, and safety of cholinesterase inhibitors for Alzheimer’s disease: A meta-analysis and meta-regression of 43 randomized clinical trials enrolling 16 106 patients. Int. J. Neuropsychopharmacol. 2017, 20, 519–528. [Google Scholar] [CrossRef]
- Cummings, J.; Reynders, R.; Zhong, K. Globalization of Alzheimer’s disease clinical trials. Alzheimers Res. Ther. 2011, 3, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Vickers, A.; Goyal, N.; Harland, R.; Rees, R. Do certain countries produce only positive results? A systematic review of controlled trials. Control Clin. Trials 1998, 19, 159–166. [Google Scholar] [CrossRef]







| Study | Severity of AD Sample Size (T/C) Mean Age (T/C) | Treatment Period (Weeks) | Intervention of Treatment Group | Intervention of Control Group | Outcomes |
|---|---|---|---|---|---|
| Furuhashi 2011 [20] | Severe 38(18/20) 82.8/83.1 | 4 | Yokukansan 22.5 g/d | Risperidone 1 mg/d | Barthel Index, MMSE, NPI *, CMAI * |
| Furukawa 2017 [21] | Mild to moderate 137(72/65) 78.3/78/5 | 4 | Yokukansan 7.5 g/d | Placebo 7.5 g/d | NPI-Q *, MMSE |
| Heo 2008 [22] | Mild to moderate 46(15/31) 67.73/66.68 | 12 | Korean red ginseng 9 g/d with usual treatment | Control: usual treatment (Treated with donepezil, rivastigmine, memantine for at least 6 months before randomization) | ADAS (total *, cog *, noncog), MMSE, CDR * |
| Lee 2008 [23] | N/A 82(50/32) 66.6/65.6 | 12 | Korean white ginseng powder 4.5 g/d + Usual treatment | Usual treatment | MMSE *, ADAS-cog *, ADAS-noncog |
| Liu 2013 [24] | Mild to moderate 60(30/30) 74/75 | 12 | Bushen-huatan-yizhi Granule 12 g/d | Piracetam 2.4 g/d | MMSE *, ADL *, serum SOD *, LPO *, TG * |
| Mazza 2006 [25] | Mild to moderate 60 (T:20/G:21/P:19) 66.2/64.5/69.8 | 96 | Ginkgo biloba 160 mg/d | 1. Donepezil 5 mg/d 2. Placebo | MMSE, SKT *, CGI * |
| Meng 2005 [26] | N/A 58 (30/28) 70.2/68.4 | 12 | Naohuandan 12 capsules/d | Piracetam 4.8 g/d | MMSE *, ADL * |
| Pakdaman 2015 [27] | Mild to moderate 116(59/57) 71.8/71.8 | 64 | MLC601 (NeuroAiDTM) 3 capsules/d | Donepezil according to clinical response and recommended maximum or tolerable dose. | MMSE, ADAS-cog |
| Pan 2014 [28] | N/A 91(45/46) 57.2/56.9 | 20 | Shen-Zhi-Ling Oral Liquid 30 cc/d | Placebo 30 cc/d | BEHAVE-AD, NPI, DFA of actigraph activity, MMSE |
| Wang 2020 [29] | Mild to moderate 51(27/24) 65.48/60.88 | 24 | Jiannao Yizhi Formula 10 g/d with Donepezil placebo 5 mg/d | Donepezil 5 mg/d with Jiannao Yizhi Formula placebo 10 g/d | ADAS-cog *, MMSE *, MoCA *, ADL, CMSS *, Serum Ach *, Aβ42 *, Tau * |
| Yancheva 2009 [30] | Mild to moderate 88(30/29/29) 69/66/68 | 22 | 1. Ginkgo biloba 240 mg/d with Donepezil placebo 2. Ginkgo biloba 240 mg/d with (Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period) | Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period with Ginkgo biloba extract placebo | SKT, CDT, Verbal fluency test, NPI (total, distress), GBS (total, ADL), HAM-D, CSS (Tinnitus, Dizziness) |
| Zhang 2015c [31] | Mild 113(58/55) 72.79/72.97 | 24 | Yishen Huazhuo Decoction 100 mL/d with Donepezil placebo 5 mg/d | Donepezil 5 mg/d + Yishen Huazhuo Decoction placebo 100 mL/d | ADAS-cog *, MMSE, ADL, NPI |
| Chen 2011a [32] | mild to moderate 67(37/30) 73.89/75.27 | 12 | Bu Yuan Cong Nao Tang 100 mL/d | Donepezil 5 mg/d | MMSE *, ADAS-cog *, ADL * |
| Chen 2011b [33] | N/A 27(14/13) 72.36/74.38 | 12 | Bushen Phlegm Stasis Compound 100 mL/d | Piracetam 2.4 g/d | MMSE *, ADAS-cog *, ADL * |
| Chen 2010 [34] | Mild to moderate 149(120/29) 66.78/68.29 | 12 | Compound Polygonum multiflorum extract 30 mL/d | Piracetam 2.4 g/d | MMSE *, ADL * |
| Cheng 2013 [35] | N/A 36(18/18) 70.33/68.56 | 12 | Yang xue qing nao Granule 12 g/d with (Donepezil 5 mg/d for the first 2 weeks, 10 mg/d for the remaining period) | Donepezil 5 mg/d for the first 2 weeks, 10 mg/d for the remaining period | MMSE, NPI * |
| Chi 2018 [36] | Mild to severe 94(47/47) 75.36/74.17 | 24 | Bushen Tianjing Yisui Prescription 1 dose/d with (Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period) | Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period | ADAS-cog *, SIB *, BEHAVE-AD *, ADL *, HAMA *, CSDD * |
| Gong 2019 [37] | N/A 60(30/30) 73.32/72.46 | 12 | “Reinforcing Kidney and Removing Blood Stasis” Formula 300 mL/d | Piracetam 3.6 g/d | MMSE *, FAQ * |
| Gu 2014 [38] | Mild to moderate 100(50/50) 67.3/66.9 | 24 | Dihuang Yizhi Formula 1 pouch/d with Donepezil 5–10 mg/d | Donepezil 5–10 mg/d | MMSE *, MoCA *, ADAS-cog *, ADL * |
| Gu 2019 [39] | Mild to severe 66(44/22) 76.18/78.73 | 12 | Yizhi Chidai Prescription 400 mL/d with Donepezil 5 mg/d | Donepezil 5 mg/d | MMSE *, TCM symptoms * |
| Guan 2017 [40] | Mild to severe 60(30/30) 69.3/70.2 | 8 | Di Yong Yizhi Granule 1 dose/d with Donepezil 5 mg/d | Donepezil 5 mg/d | MMSE *, ADAS-cog *, ADL * |
| Guo 2011 [41] | Moderate to severe 60(30/30) 73.8/73/14 | 4 | Zhibai Dihuang Tang 1 dose/d with Donepezil 5 mg/d | Donepezil 5 mg/d | MMSE *, BEHAVE-AD * |
| Hu 2015 [42] | Mild to moderate 80(40/40) 68.4/69.2 | 24 | Bushen Tongluo Decoction 1 dose/d with (Donepezil 10 mg/d + Piracetam 2.4 g/d) | Donepezil 10 mg/d with Piracetam 2.4 g/d | MMSE *, ADAS-cog *, ADL *, NPI *, serum SOD *, MDA *, TNF-α *, IL-1 *, IL-6 * |
| Huang 2018 [43] | Mild 62(33/29) 72.3/72.8 | 24 | Bushenyisui Formula 1 dose/d with Donepezil placebo | Donepezil 5 mg/d + Bushenyisui formula placebo | MMSE * |
| Jiang 2018 [44] | Mild to moderate 50(25/25) 67.2/70.4 | 12 | Jiannao Powder 10 g/d with (Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period) | Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period | MMSE *, ADL *, HDS-R *, CSF (Aβ42, tau, p-tau) *, TCM symptom score * |
| Li 2015 [45] | N/A 66(35/31) 69.1/68.4 | 24 | Bupi Yishen Decoction 1 dose/d | Donepezil 10 mg/d | MMSE *, ADAS-cog *, ADL *, TCM symptoms *, serum SOD *, MDA *, T-AOC *, 8-iso-PGF2α *, ox-LDL * |
| Li 2018a [46] | N/A 98(49/49) 74.45/74.27 | 24 | Compound Congrong Yizhi Capsule 3.6 g/d with (Rivastigmine: First month 3 mg/d, second month 6 mg/d. If well tolerated, increased to 12 mg/d) | Rivastigmine: First month 3 mg/d, second month 6 mg/d. If well tolerated, increased to 12 mg/d | MMSE *, ADAS-cog *, BEHAVE-AD *, ADL *, serum Aβ *, IL-6 *, IL-1β *, BK * |
| Li 2016a [47] | N/A 98(49/49) 67.5/67.6 | 12 | Renshen Bujing Anshen Formula with Donepezil 20 mg/d | Donepezil 20 mg/d | BEHAVE-AD *, ACE-R *, Barthel Index * |
| Li 2016b [48] | N/A 50(25/25) 65.60/66.29 | 8 | Huang Cong Formula with Donepezil 5 mg/d | Donepezil 5 mg/d | ADAS-cog, TCM symptoms, MMSE *, FAQ *, HDS *, ADL * |
| Li 2016c [49] | Mild 113(58/55) 72.79/72.97 | 24 | Tonifying Kidney Prescription 1 pouch/d | Donepezil 5 mg/d | MMSE *, ADAS-cog *, ADL * |
| Li 2014 [50] | Mild to moderate 65(40/25) 73.55/74.12 | 12 | Bushen Huoxue Decoction 1 pouch/d with (Huperzine-A 200 μg/d + Nicergoline 20 mg/d) | Huperzine-A 200 μg/d with Nicergoline 20 mg/d | MMSE *, ADL * |
| Li 2018b [51] | N/A 100(50/50) 69.87/68.19 | 12 | Bushen Yizhi formula 600 mL/d with (Clozapine started with 25 mg/d and gradually increased to 200 mg/d) | Clozapine started with 25 mg/d and gradually increased to 200 mg/d | BEHAVE-AD *, serum MDA * and SOD * |
| Li 2017 [52] | Mild to moderate 63(31/32) 74.82/75.06 | 12 | Modified Shuyu Pill 30 mL/d | Donepezil 5 mg/d | MMSE *, ADAS-cog *, ADL *, SDSD * |
| Li 2002 [53] | Mild to moderate 32(18/14) 66/65 | 8 | Danggui Shaoyao San 1 dose/d | Nimodipine 60–120 mg/d | HDS *, MMSE, ADL, CGI |
| Liang 2010 [54] | Mild to severe 100(50/50) 72.6/71.7 | 24 | Bushenyizhi Granule 1 dose/d with (Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period) | Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period | ADAS-cog *, MMSE *, ADL *, TCM symptoms |
| Lin 2006 [55] | Mild to moderate 60(20/20/20) 76.37/74.43/72.63 | 12 | 1. Taioxin 20 mL/d 2. Bushen 20 mL/d | Donepezil 5 mg/d | 1.Taioxin: MMSE *, ADL, FOM *, BD, DS *, RVR * 2.Bushen: MMSE *, ADL, FOM, BD *, DS, RVR * |
| Lin 2017 [56] | Mild to moderate 60(30/30) 62.33/64.57 | 24 | Phlegm-resolving Orifice-opening Decoction 1 dose/d with Donepezil 5 mg/d | Donepezil 5 mg/d | MMSE *, ADAS-cog *, ADL *, TCM symptoms * |
| Lin 2018 [57] | Mild 66(33/33) 72.29/72.82 | 24 | Bu Shen Yi Sui Decoction + Donepezil placebo | Donepezil 5 mg/d with Bu Shen Yi Sui Decoction placebo | MMSE, ADL, TCM symptoms *, endocrine (testosterone, cortisol *, estradiol, thyroxine, growth hormone *, ACTH *) |
| Liu 2010 [58] | N/A 20(10/10) 61.5/62.3 | 12 | Yizhi Jiannao Granule 16.5 g/d | Donepezil 5 mg/d | MMSE *, ADAS-cog *, serum IL-1β *, TNF-α * |
| Peng 2009 [59] | Mild to moderate 56(28/28) 67.2/67.5 | 12 | Yizhi Jiannao Granule 16.5 g/d | Donepezil 5 mg/d | MMSE *, ADL * |
| Shan 2017 [60] | N/A 82(41/41) 67.32/68.02 | 24 | Bushen Yizhi Granules 1 pouch/d with (Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period) | Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period | MMSE *, ADAS-cog *, ADL *, TCM symptom * |
| Wu 2018 [61] | Mild to moderate 140(70/70) 70.0/71.0 | 24 | Compound Huonaoshu Capsule 6 granules/d with Donepezil 10 mg/d | Donepezil 10 mg/d | MMSE *, ADL *, EEG signals * |
| Yang 2013 [62] | Mild to moderate 60(30/30) 84.22/82.72 | 12 | Yizhi Jiannao Granule 11 g/d | Donepezil 5 mg/d | MMSE *, ADL *, homocysteine * |
| Yang 2018a [63] | N/A 55(30/25) 64.93/63.44 | 24 | Ma Huang Fu Zi Xi Xin Tang 1 dose/d with Donepezil 10 mg/d | Donepezil 10 mg/d | MMSE *, MoCA *, ADL * |
| Yu 2012 [64] | Mild to moderate 107(55/52) 74.7/76.4 | 48 | Herbal medicine based on syndrome differentiation | Donepezil 5 mg/d | MMSE *, FOM *, BD *, DS *, fMRI |
| Yang 2018b [65] | Mild 59(31/28) 72.66/73.12 | 12 | Tiaoxin 1 pouch/d | Donepezil 5 mg/d | MMSE *, FOM *, RVR *, BD *, DS * |
| Yu 2006 [66] | Mild to moderate 82(42/40) Mean 69 | 10 | “Reinforcing kidney, activating blood and resolving phlegm” Formula 1 pouch/d | Hydergine 3 mg/d for the first week, 6 mg/d for the remaining period | MMSE *, ADL * |
| Yuan 2017 [67] | N/A 100(50/50) 70.2/70.4 | 24 | Bushen Yizhi Granule 1 dose/day with (Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period) | Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period | MMSE * |
| Zhang 2015b [68] | Moderate to severe 100(50/50) 70/69 | 12 | Shen Gui Yizhi Formula 1 dose/d with Butylphthalide 0.6 g/d | Butylphthalide 0.6 g/d | MMSE *, ADL *, serum Aβ *, TCM symptoms * |
| Zhang 2015a [69] | Mild to moderate 51(26/25) 67.50/68.72 | 12 | Yizhi Xingnao Fang 1 dose/d with (Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period) | Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period | ADAS-cog *, MMSE *, ADL *, SDSD * |
| Zhang 2018b [70] | N/A 88(44/44) 72.91/72.87 | 4 | Qingxin Yizhi Decoction 1 dose/d with Donepezil 10 mg/d | Donepezil 10 mg/d | MMSE *, ADAS-cog *, ADL *, serum SOD *, MDA *, T-AOC *, ox-LDL * |
| Zhang 2018c [71] | Mild to moderate 60(30/30) 65.2/66.4 | 12 | Dihuang Yinzi Decoction 1 dose/d | Donepezil 5 mg/d | MMSE *, ADAS-cog *, ADL *, Levels of Notch1 *, ADAM10 *, BASE1 * |
| Zhang 2008 [72] | Moderate to severe 45(30/15) Mean 73.5 | 12 | Shenghuang-yizhi Granule 4 pouches/d | Piracetam 3.6 g/d | MMSE *, BBS * |
| Zhang 2018a [73] | N/A 100(50/50) 70.8/69.2 | 12 | Compound Danshen Tablet 2.88 g/d with (Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period) | Donepezil 5 mg/d for the first month, 10 mg/d for the remaining period | MMSE *, ADAS-cog *, ADL *, serum Glu * and Asp * |
| Zhou 2007 [74] | N/A 68(23/21/24) 76.1/74.8/75.4 | 24 | 1. Reinhartdt and Sea Cucumber Capsule 2.7 g/d 2. Reinhartdt and Sea Cucumber Capsule 2.7 g/d + Donepezil 5–10 mg/d | Donepezil 5–10 mg/d | MMSE *, ADAS-cog, ADL *, thyroid hormones |
| Zhu 2010 [75] | Mild to moderate 40(20/20) Mean 72.3 | 8 | Yizhi Jiannao Granule 16.5 g/d | Donepezil 5 mg/d | MMSE *, 8-IPF2α (blood, urine) * |
| Wang 2018 [76] | Mild to severe 127(63/64) 67.3/68.6 | 12 | Bushen Huatan Yizhi Decoction 1 dose/d + Butylphthalide 800 mg/d | Butylphthalide 800 mg/d | MMSE *, hematocrit *, whole blood high shear rate *, whole blood low shear rate *, erythrocyte aggregation index *, MDA *, SOD *, GSH-Px *, CAT * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Kwon, S.; Jin, C.; Cho, S.-Y.; Park, S.-U.; Jung, W.-S.; Moon, S.-K.; Park, J.-M.; Ko, C.-N.; Cho, K.-H. Traditional East Asian Herbal Medicine Treatment for Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Pharmaceuticals 2022, 15, 174. https://doi.org/10.3390/ph15020174
Lee J, Kwon S, Jin C, Cho S-Y, Park S-U, Jung W-S, Moon S-K, Park J-M, Ko C-N, Cho K-H. Traditional East Asian Herbal Medicine Treatment for Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Pharmaceuticals. 2022; 15(2):174. https://doi.org/10.3390/ph15020174
Chicago/Turabian StyleLee, JiEun, Seungwon Kwon, Chul Jin, Seung-Yeon Cho, Seong-Uk Park, Woo-Sang Jung, Sang-Kwan Moon, Jung-Mi Park, Chang-Nam Ko, and Ki-Ho Cho. 2022. "Traditional East Asian Herbal Medicine Treatment for Alzheimer’s Disease: A Systematic Review and Meta-Analysis" Pharmaceuticals 15, no. 2: 174. https://doi.org/10.3390/ph15020174
APA StyleLee, J., Kwon, S., Jin, C., Cho, S. -Y., Park, S. -U., Jung, W. -S., Moon, S. -K., Park, J. -M., Ko, C. -N., & Cho, K. -H. (2022). Traditional East Asian Herbal Medicine Treatment for Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Pharmaceuticals, 15(2), 174. https://doi.org/10.3390/ph15020174