
Radiopharmaceutical Labelling for Lung Ventilation/Perfusion PET/CT Imaging: A Review of Production and Optimization Processes for Clinical Use

 , ,
, ,
Abstract
:1. Introduction
2. Challenges of the Transition from 99mTc- to 68Ga-Labelled Radiopharmaceuticals for Lung Imaging
3. Lung Perfusion Imaging
3.1. [99mTc]Tc-MAA
3.1.1. Chemical Aspects of [99mTc]Tc-MAA Particles
3.1.2. Technical Aspects: [99mTc]Tc-MAA Preparation
3.1.3. Pharmacological Aspects
3.2. [68Ga]Ga-MAA
3.2.1. Chemical Aspects of [68Ga]Ga-MAA Particles
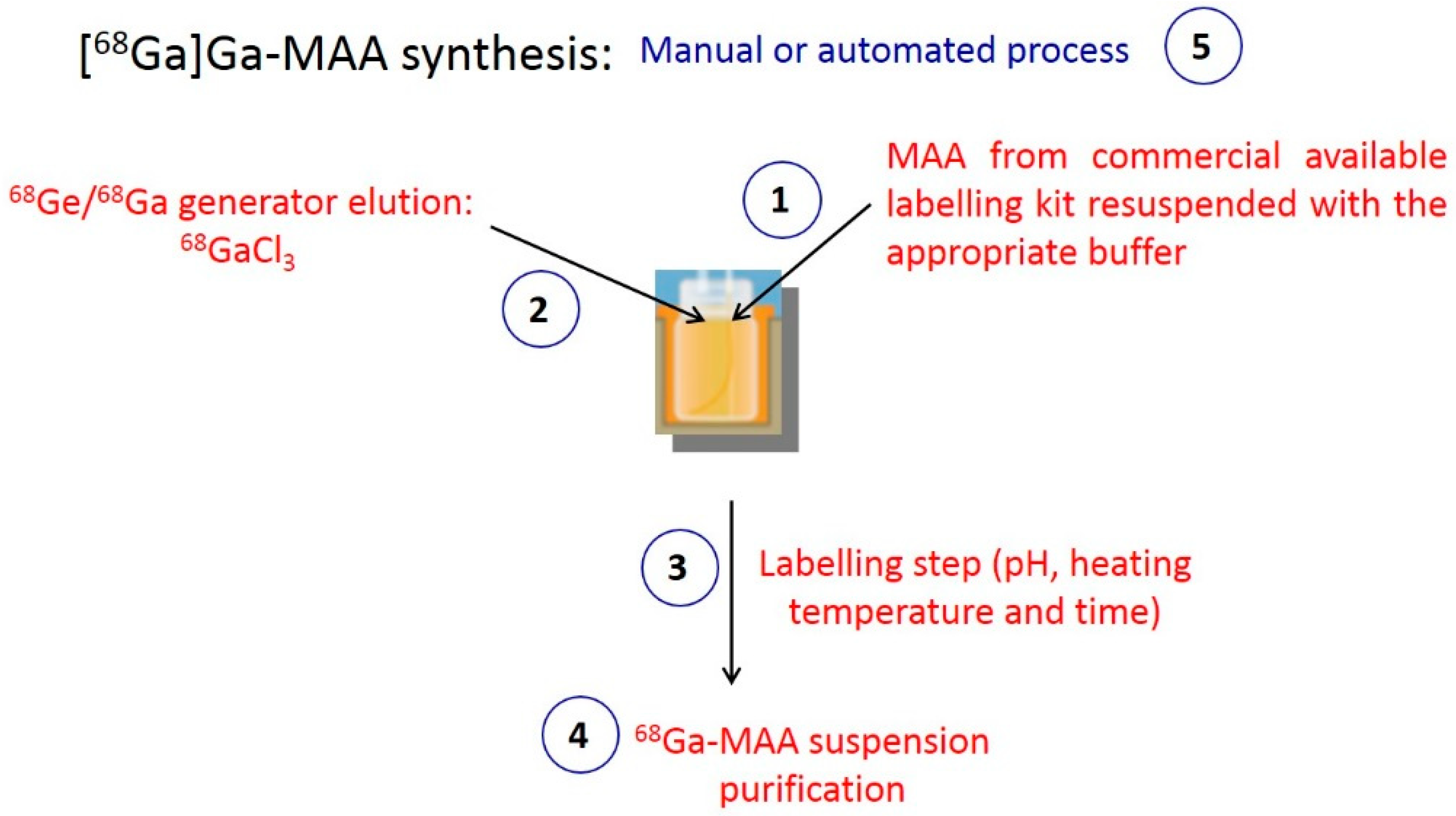
3.2.2. Technical Aspects: [68Ga]Ga-MAA Preparation
- MAA
- 68Ga eluate
- Labelling conditions
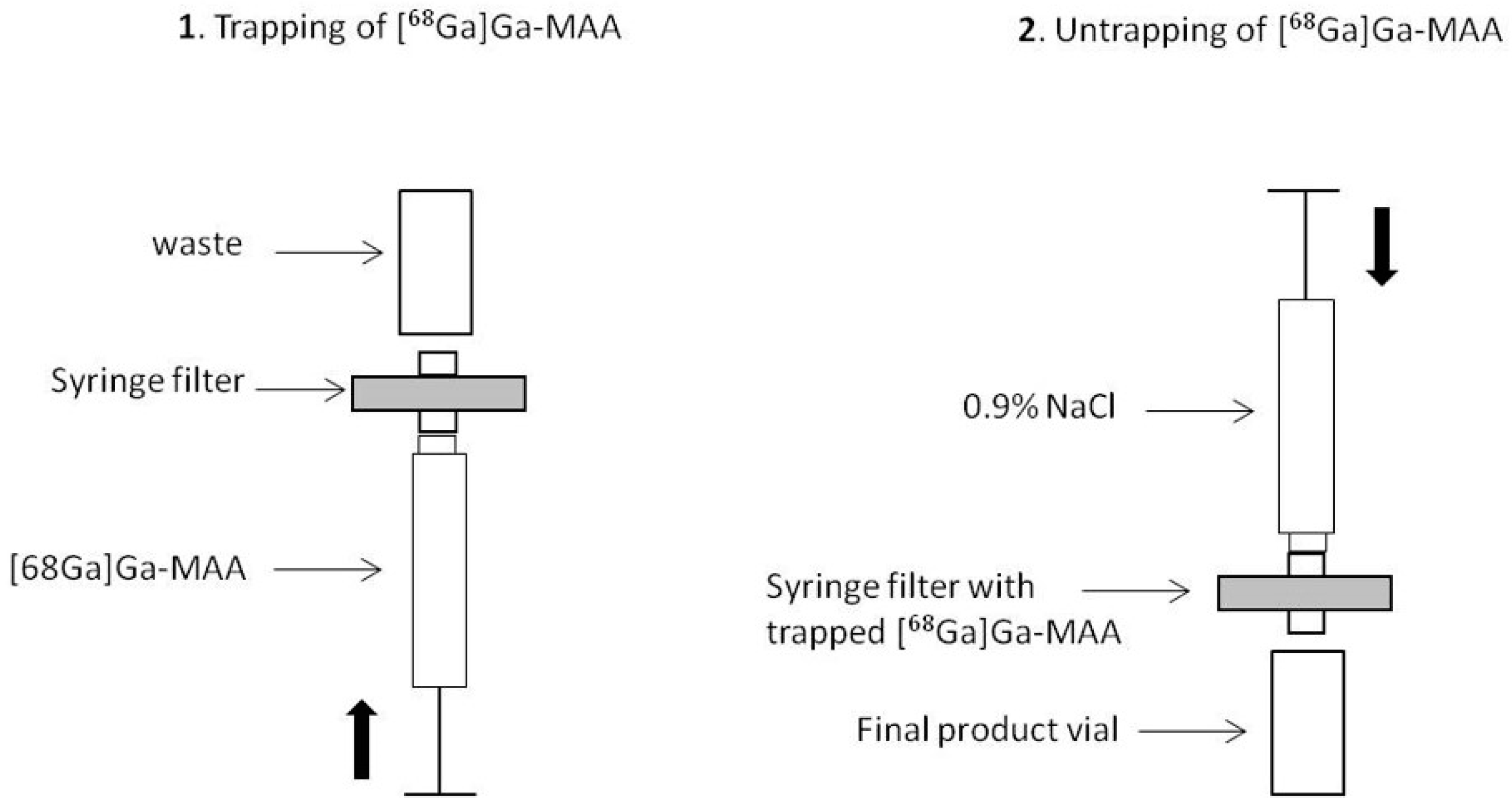
- [68Ga]Ga-MAA purification
- Manual or Automated Process
3.2.3. Pharmacological Aspects
4. Lung Ventilation Imaging
4.1. Aerosolized 99mTc-Labelled Carbon Nanoparticles (Technegas)
4.1.1. Physical and Chemical Aspects
4.1.2. Technical Aspects
- Crucible loading
- Simmer stage
- Burning stage
4.1.3. Pharmacological Aspects
4.2. Aerosolized 68Ga-Labelled Carbon Nanoparticles
4.2.1. Physical and Chemical Aspects
4.2.2. Technical Aspects
4.2.3. Pharmacological Aspects
5. Practical Considerations for an Optimal Clinical Use
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Le Roux, P.Y.; Siva, S.; Steinfort, D.P.; Callahan, J.; Eu, P.; Irving, L.B.; Hicks, R.J.; Hofman, M.S. Correlation of 68Ga Ventilation-Perfusion PET/CT with Pulmonary Function Test Indices for Assessing Lung Function. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2015, 56, 1718–1723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajc, M.; Schumichen, C.; Gruning, T.; Lindqvist, A.; Le Roux, P.Y.; Alatri, A.; Bauer, R.W.; Dilic, M.; Neilly, B.; Verberne, H.J.; et al. EANM guideline for ventilation/perfusion single-photon emission computed tomography (SPECT) for diagnosis of pulmonary embolism and beyond. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2429–2451. [Google Scholar] [CrossRef] [Green Version]
- Le Roux, P.Y.; Blanc-Beguin, F.; Bonnefoy, P.B.; Bourhis, D.; Camilleri, S.; Moreau-Triby, C.; Pinaquy, J.B.; Salaün, P.Y. Guide pour la re’ daction de protocoles pour la scintigraphie pulmonaire. Méd. Nucl. 2021, 45, 8. [Google Scholar] [CrossRef]
- Le Roux, P.Y.; Robin, P.; Salaun, P.Y. New developments and future challenges of nuclear medicine and molecular imaging for pulmonary embolism. Thromb. Res. 2018, 163, 236–241. [Google Scholar] [CrossRef]
- Le Roux, P.Y.; Hicks, R.J.; Siva, S.; Hofman, M.S. PET/CT Lung Ventilation and Perfusion Scanning using Galligas and Gallium-68-MAA. Semin. Nucl. Med. 2019, 49, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Beauregard, J.M.; Barber, T.W.; Neels, O.C.; Eu, P.; Hicks, R.J. 68Ga PET/CT ventilation-perfusion imaging for pulmonary embolism: A pilot study with comparison to conventional scintigraphy. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2011, 52, 1513–1519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotzerke, J.; Andreeff, M.; Wunderlich, G. PET aerosol lung scintigraphy using Galligas. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 175–177. [Google Scholar] [CrossRef] [PubMed]
- Le Roux, P.Y.; Iravani, A.; Callahan, J.; Burbury, K.; Eu, P.; Steinfort, D.P.; Lau, E.; Woon, B.; Salaun, P.Y.; Hicks, R.J.; et al. Independent and incremental value of ventilation/perfusion PET/CT and CT pulmonary angiography for pulmonary embolism diagnosis: Results of the PECAN pilot study. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1596–1604. [Google Scholar] [CrossRef] [PubMed]
- Siva, S.; Thomas, R.; Callahan, J.; Hardcastle, N.; Pham, D.; Kron, T.; Hicks, R.J.; MacManus, M.P.; Ball, D.L.; Hofman, M.S. High-resolution pulmonary ventilation and perfusion PET/CT allows for functionally adapted intensity modulated radiotherapy in lung cancer. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2015, 115, 157–162. [Google Scholar] [CrossRef]
- Le Roux, P.Y.; Leong, T.L.; Barnett, S.A.; Hicks, R.J.; Callahan, J.; Eu, P.; Manser, R.; Hofman, M.S. Gallium-68 perfusion positron emission tomography/computed tomography to assess pulmonary function in lung cancer patients undergoing surgery. Cancer Imaging Off. Publ. Int. Cancer Imaging Soc. 2016, 16, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hicks, R.J.; Hofman, M.S. Is there still a role for SPECT-CT in oncology in the PET-CT era? Nat. Rev. Clin. Oncol. 2012, 9, 9. [Google Scholar] [CrossRef] [PubMed]
- Papagiannopoulou, D. Technetium-99m radiochemistry for pharmaceutical applications. J. Label. Compd. Radiopharm. 2017, 60, 502–520. [Google Scholar] [CrossRef]
- Liu, S.; Edwards, D.S. 99mTc-Labeled Small Peptides as Diagnostic Radiopharmaceuticals. Chem. Rev. 1999, 99, 2235–2268. [Google Scholar] [CrossRef]
- Wadas, T.J.; Wong, E.H.; Weisman, G.R.; Anderson, C.J. Coordinating radiometals of copper, gallium, indium, yttrium, and zirconium for PET and SPECT imaging of disease. Chem. Rev. 2010, 110, 2858–2902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewanjee, M.K. The chemistry of 99mTc-labeled radiopharmaceuticals. Semin. Nucl. Med. 1990, 20, 5–27. [Google Scholar] [CrossRef]
- Lin, M.S.; Winchell, H.S.; Shipley, B.A. Use of Fe(II) or Sn(II) alone for technetium labeling of albumin. J. Nucl. Med. 1971, 12, 8. [Google Scholar]
- Vanbilloen, H.P.; Verbeke, K.A.; De Roo, M.J.; Verbruggen, A.M. Technetium-99m labelled human serum albumin for ventriculography: A comparative evaluation of six labelling kits. Eur. J. Nucl. Med. 1993, 20, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Canziani, L.; Marenco, M.; Cavenaghi, G.; Manfrinato, G.; Taglietti, A.; Girella, A.; Aprile, C.; Pepe, G.; Lodola, L. Chemical and Physical Characterisation of Macroaggregated Human Serum Albumin: Strength and Specificity of Bonds with 99mTc and 68Ga. Molecules 2022, 27, 404. [Google Scholar] [CrossRef] [PubMed]
- Marenco, M.; Canziani, L.; De Matteis, G.; Cavenaghi, G.; Aprile, C.; Lodola, L. Chemical and Physical Characterisation of Human Serum Albumin Nanocolloids: Kinetics, Strength and Specificity of Bonds with 99mTc and 68Ga. Nanomaterials 2021, 11, 1776. [Google Scholar] [CrossRef]
- Hunt, A.P.; Frier, M.; Johnson, R.A.; Berezenko, S.; Perkins, A.C. Preparation of Tc-99m-macroaggregated albumin from recombinant human albumin for lung perfusion imaging. Eur. J. Pharm. Biopharm. 2006, 62, 26–31. [Google Scholar] [CrossRef]
- Schembri, G.P.; Roach, P.J.; Bailey, D.L.; Freeman, L. Artifacts and Anatomical Variants Affecting Ventilation and Perfusion Lung Imaging. Semin. Nucl. Med. 2015, 45, 373–391. [Google Scholar] [CrossRef] [PubMed]
- Shanehsazzadeh, S.; Jalilian, A.R.; Lahooti, A.; Geramifar, P.; Beiki, D.; Yousefnia, H.; Rabiee, A.; Mazidi, M.; Mirshojaei, S.F.; Maus, S. Preclinical Evaluation of 68Ga-MAA from Commercial Available 99mTc-MAA Kit. Iran. J. Pharm. Res. IJPR 2017, 16, 1415–1423. [Google Scholar] [PubMed]
- Malone, L.A.; Malone, J.F.; Ennis, J.T. Kinetics of technetium 99m labelled macroaggregated albumin in humans. Br. J. Radiol. 1983, 56, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Even, G.A.; Green, M.A. Gallium-68-labeled macroaggregated human serum albumin, 68Ga-MAA. Int. J. Radiat. Appl. Instrum. Part B Nucl. Med. Biol. 1989, 16, 319–321. [Google Scholar] [CrossRef]
- Watanabe, N.; Shirakami, Y.; Tomiyoshi, K.; Oriuchi, N.; Hirano, T.; Yukihiro, M.; Inoue, T.; Endo, K. Indirect labeling of macroaggregated albumin with indium-111 via diethylenetriaminepentaacetic acid. Nucl. Med. Biol. 1996, 23, 595–598. [Google Scholar] [CrossRef]
- Hnatowich, D.J. Labeling of tin-soaked albumin microspheres with 68Ga. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 1976, 17, 57–60. [Google Scholar]
- Velikyan, I. Prospective of 68Ga-radiopharmaceutical development. Theranostics 2014, 4, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathias, C.J.; Green, M.A. A convenient route to [68Ga]Ga-MAA for use as a particulate PET perfusion tracer. Appl. Radiat. Isot. Incl. Data Instrum. Methods Use Agric. Ind. Med. 2008, 66, 1910–1912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, A.; Subramanian, S.; Pandey, U.; Sarma, H.D.; Ram, R.; Dash, A. In-house preparation of macroaggregated albumin (MAA) for 68Ga labeling and its comparison with comercially available MAA. J. Radioanal. Nucl. Chem. 2016, 308, 817–824. [Google Scholar] [CrossRef]
- Hayes, R.L.; Carlton, J.E.; Kuniyasu, Y. A new method for labeling microspheres with 68Ga. Eur. J. Nucl. Med. 1981, 6, 531–533. [Google Scholar] [CrossRef]
- Maziere, B.; Loc’h, C.; Steinling, M.; Comar, D. Stable labelling of serum albumin microspheres with gallium-68. Int. J. Radiat. Appl. Instrum. Part A Appl. Radiat. Isot. 1986, 37, 360–361. [Google Scholar] [CrossRef]
- Maus, S.; Buchholz, H.G.; Ament, S.; Brochhausen, C.; Bausbacher, N.; Schreckenberger, M. Labelling of commercially available human serum albumin kits with 68Ga as surrogates for 99mTc-MAA microspheres. Appl. Radiat. Isot. Incl. Data Instrum. Methods Use Agric. Ind. Med. 2011, 69, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Ament, S.J.; Maus, S.; Reber, H.; Buchholz, H.G.; Bausbacher, N.; Brochhausen, C.; Graf, F.; Miederer, M.; Schreckenberger, M. PET lung ventilation/perfusion imaging using 68Ga aerosol (Galligas) and 68Ga-labeled macroaggregated albumin. Recent Results Cancer Res. 2013, 194, 395–423. [Google Scholar]
- Amor-Coarasa, A.; Milera, A.; Carvajal, D.; Gulec, S.; McGoron, A.J. Lyophilized Kit for the Preparation of the PET Perfusion Agent [68Ga]-MAA. Int. J. Mol. Imaging 2014, 2014, 269365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mueller, D.; Kulkarni, H.; Baum, R.P.; Odparlik, A. Rapid Synthesis of 68Ga-labeled macroaggregated human serum albumin (MAA) for routine application in perfusion imaging using PET/CT. Appl. Radiat. Isot. Incl. Data Instrum. Methods Use Agric. Ind. Med. 2017, 122, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Persico, M.G.; Marenco, M.; De Matteis, G.; Manfrinato, G.; Cavenaghi, G.; Sgarella, A.; Aprile, C.; Lodola, L. 99mTc-68Ga-ICG-Labelled Macroaggregates and Nanocolloids of Human Serum Albumin: Synthesis Procedures of a Trimodal Imaging Agent Using Commercial Kits. Contrast Media Mol. Imaging 2020, 2020, 3629705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gültekin, A.; Cayir, M.C.; Ugur, A.; Bir, F.; Yüksel, D. Detection of Pulmonary Embolism with Gallium-68 Macroaggregated Albumin Perfusion PET/CT: An Experimental Study in Rabbits. Contrast Media Mol. Imaging 2020, 2020, 5607951. [Google Scholar] [CrossRef]
- Ayse, U.; Aziz, G.; Dogangun, Y. High-Efficiency Cationic Labeling Algorithm of Macroaggregated Albumin with 68Gallium. Nucl. Med. Mol. Imaging 2021, 55, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Blanc-Béguin, F.; Masset, J.; Robin, P.; Tripier, R.; Hennebicq, H.; Guilloux, V.; Vriamont, C.; Wargnier, C.; Cogulet, V.; Eu, P.; et al. Fully automated 68Ga-labeling and purification of macroaggregated albumin particles for lung perfusion PET imaging. Front. Nucl. Med. 2021, 1, 10. [Google Scholar] [CrossRef]
- Velikyan, I. 68Ga-Based radiopharmaceuticals: Production and application relationship. Molecules 2015, 20, 12913–12943. [Google Scholar] [CrossRef] [Green Version]
- Zhernosekov, K.P.; Filosofov, D.V.; Baum, R.P.; Aschoff, P.; Bihl, H.; Razbash, A.A.; Jahn, M.; Jennewein, M.; Rosch, F. Processing of generator-produced 68Ga for medical application. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2007, 48, 1741–1748. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.R.; Pecoraro, V.L. Thermodynamic binding constants for gallium transferrin. Biochemistry 1983, 22, 292–299. [Google Scholar] [CrossRef]
- Kotzerke, J.; Andreeff, M.; Wunderlich, G.; Wiggermann, P.; Zophel, K. Ventilation-perfusion-lungscintigraphy using PET and 68Ga-labeled radiopharmaceuticals. Nuklearmedizin. Nucl. Med. 2010, 49, 203–208. [Google Scholar]
- Senden, T.J.; Moock, K.H.; Gerald, J.F.; Burch, W.M.; Browitt, R.J.; Ling, C.D.; Heath, G.A. The physical and chemical nature of technegas. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 1997, 38, 1327–1333. [Google Scholar]
- Lloyd, J.J.; Shields, R.A.; Taylor, C.J.; Lawson, R.S.; James, J.M.; Testra, H.J. Technegas and Pertechnegas particle size distribution. Eur. J. Nucl. Med. 1995, 22, 473–476. [Google Scholar] [CrossRef]
- Mackey, D.W.; Burch, W.M.; Dance, I.G.; Fisher, K.J.; Willett, G.D. The observation of fullerenes in a Technegas lung ventilation unit. Nucl. Med. Commun. 1994, 15, 430–434. [Google Scholar] [CrossRef]
- Burch, W.M.; Sullivan, P.J.; McLaren, C.J. Technegas—A new ventilation agent for lung scanning. Nucl. Med. Commun. 1986, 7, 865–871. [Google Scholar] [CrossRef]
- Monaghan, P.; Provan, I.; Murray, C.; Mackey, D.W.; Van der Wall, H.; Walker, B.M.; Jones, P.D. An improved radionuclide technique for the detection of altered pulmonary permeability. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 1991, 32, 1945–1949. [Google Scholar]
- Isawa, T.; Teshima, T.; Anazawa, Y.; Miki, M.; Motomiya, M. Technegas for inhalation lung imaging. Nucl. Med. Commun. 1991, 12, 47–55. [Google Scholar] [CrossRef]
- Isawa, T.; Teshima, T.; Anazawa, Y.; Miki, M.; Soni, P.S. Technegas versus krypton-81m gas as an inhalation agent. Comparison of pulmonary distribution at total lung capacity. Clin. Nucl. Med. 1994, 19, 1085–1090. [Google Scholar]
- Pourchez, J.; Albuquerque-Silva, I.M.D.; Cottier, M.; Clotagatide, A.; Vecellio, L.; Durand, M.; Dubois, F. Generation and characterization of radiolabelled nanosized carbonaceous aerosols for human inhalation studies. J. Aerosol Sci. 2013, 55, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Scalzetti, E.M.; Gagne, G.M. The transition from technegas to pertechnegas. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 1995, 36, 267–269. [Google Scholar]
- Mackey, D.W.; Jackson, P.; Baker, R.J.; Dasaklis, C.; Fisher, K.J.; Magee, M.; Bush, V.; Burch, W.M.; Van der Wall, H.; Willett, G.D. Physical properties and use of pertechnegas as a ventilation agent. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 1997, 38, 163–167. [Google Scholar]
- Fanti, S.; Compagnone, G.; Pancaldi, D.; Franchi, R.; Corbelli, C.; Marengo, M.; Onofri, C.; Galassi, R.; Levorato, M.; Monetti, N. Evaluation of lung clearance of inhaled pertechnegas. Ann. Nucl. Med. 1996, 10, 147–151. [Google Scholar] [CrossRef]
- Sanchez-Crespo, A. Lung Scintigraphy in the Assessment of Aerosol Deposition and Clearance. Semin. Nucl. Med. 2019, 49, 47–57. [Google Scholar] [CrossRef]
- Hartmann, I.J.; Hagen, P.J.; Stokkel, M.P.; Hoekstra, O.S.; Prins, M.H. Technegas Versus 81mKr Ventilation–Perfusion Scintigraphy: A Comparative Study in Patients with Suspected Acute Pulmonary Embolism. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2001, 42, 8. [Google Scholar]
- Möller, W.; Felten, K.; Seitz, J.; Sommerer, K.; Takenata, S.; Wiebert, P.; Philipson, K.; Svartengren, M.; Kreyling, W.G. A generator for the production of radiolabelled ultrafine carbonaceous particles for deposition and clearance studies in the respiratory tract. J. Aerosol Sci. 2006, 37, 631–644. [Google Scholar] [CrossRef]
- Strong, J.C.; Agnew, J.E. The particle size distribution of technegas and its influence on regional lung deposition. Nucl. Med. Commun. 1989, 10, 425–430. [Google Scholar] [CrossRef]
- Lemb, M.; Oei, T.H.; Eifert, H.; Gunther, B. Technegas: A study of particle structure, size and distribution. Eur. J. Nucl. Med. 1993, 20, 576–579. [Google Scholar] [CrossRef]
- Blanc-Beguin, F.; Elies, P.; Robin, P.; Tripier, R.; Kervarec, N.; Lemarie, C.A.; Hennebicq, S.; Tromeur, C.; Cogulet, V.; Salaun, P.Y.; et al. 68Ga-Labelled Carbon Nanoparticles for Ventilation PET/CT Imaging: Physical Properties Study and Comparison with Technegas®. Mol. Imaging Biol. 2021, 23, 62–69. [Google Scholar] [CrossRef]
- Oehme, L.; Zophel, K.; Golgor, E.; Andreeff, M.; Wunderlich, G.; Brogsitter, C.; de Abreu, M.G.; Kotzerke, J. Quantitative analysis of regional lung ventilation and perfusion PET with 68Ga-labelled tracers. Nucl. Med. Commun. 2014, 35, 501–510. [Google Scholar] [CrossRef]
- Borges, J.B.; Velikyan, I.; Langstrom, B.; Sorensen, J.; Ulin, J.; Maripuu, E.; Sandstrom, M.; Widstrom, C.; Hedenstierna, G. Ventilation distribution studies comparing Technegas and “Gallgas” using 68GaCl3 as the label. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2011, 52, 206–209. [Google Scholar] [CrossRef] [Green Version]
- Bailey, D.L.; Eslick, E.M.; Schembri, G.P.; Roach, P.J. 68Ga PET Ventilation and Perfusion Lung Imaging-Current Status and Future Challenges. Semin. Nucl. Med. 2016, 46, 428–435. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Albumin Particles Labelled | 68Ga Eluate Pre-Purification | Labelling Conditions | Radiolabelling Yield (%) | Process Duration (min) | Manual/Automated Process | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Nature and Origin | Washed/Non-Washed | Yes/No | Method Used | pH | Buffer | Heating Time (min) | T °C | ||||
| Hnatowich et al. [26] | HSA microspheres. Commercial kit. | Non-washed | Yes | Anion exchange chromatography | 2.6–3 | 15 | 40–60 | 65.0 | 40 | Manual | |
| Hayes et al. [30] | HSA microspheres. Commercial kit. | Non-washed | Yes | Anion exchange chromatography | 4.8 | Sodium acetate solution | 10 | 37 | 97.4 ± 1.0 | Manual | |
| Maziere et al. [31] | HSA microspheres. Commercial kit. | Non-washed | Yes | Pre-concentration | 4.7 | 20 | 85 | 93.2 ± 2.5 | 40 | Manual | |
| Even and Green [24] | MAA. Commercial kit. | Washed | Yes | Pre-concentration | 4.7 | Sodium acetate buffer | 15 | 74 ± 1 | 77.0–97.0 | Manual | |
| Mathias et al. [28] | MAA. Commercial kit. | Washed | 5–6 | Sodium acetate solution | 15 | 75 | 81.6 ± 5.3 | 25 | Manual | ||
| Maus et al. [32] | MAA. Commercial kit. | Washed | Yes | Fractionation | 4 | HEPES | 20 | 75 | 85.0 ± 2.0 | 30 | Manual |
| Hofman et al. [6] | MAA. Commercial kit. | Washed | Yes | SCX cartridge | 6.5 | Sodium acetate solution | 5 | 70 | ≥90.0 | Manual | |
| Ament et al. [33] | MAA. Commercial kit. | Washed | Yes | Fractionation | 4 | HEPES | 20 | 75 | 85.0 ± 2.0 | Manual | |
| Amor-Coarasa et al. [34] | MAA. Commercial kit. | Washed | No | 4.7 | Sodium acetate solution | 15 | 75 | 78.3 ± 3.1 | Manual | ||
| Yes | Combination of chromatographic exchange resins (cationic then anionic) | 4.7 | Sodium acetate solution | 15 | 75 | 97.6 ± 1.5 | Manual | ||||
| Jain et al. [29] | MAA. Homemade with and without SnCl2 | No | 6 | 15 | 75 | 77.6 | Manual | ||||
| Mueller et al. [35] | MAA. Commercial kit. | Washed and non-washed | Yes | SCX cartridge | 4.5 | Sodium acetate buffer | 10 | 115 | Not mentioned (non-washed) 75.0 (washed) | 20 (manual) 14 (automated) | Manual and automated |
| Shannehsazzadeh et al. [22] | MAA. Commercial kit. | Washed | Yes | Fractionation | 4 | HEPES | 8 | 75 | 90.0 -95.0 | Manual | |
| Persico et al. [36] | MAA. Commercial kit. | Washed | Yes | SCX cartridge | 6–6.5 | Sodium acetate buffer | 15 | 40 | 97.0 | Manual and automated | |
| Gultekin et al. [37] | MAA. Commercial kit. | Washed | Yes | PSH+ cartridge | 4–5 | HEPES | 7 | 90 | 80.0 | Manual | |
| Ayșe et al. [38] | MAA. Commercial kit. | Washed | Yes | PSH+ cartridge | 4–5 | HEPES | 7 | 90 | 85.0 ± 3.0 | 16 | Automated |
| Blanc-Béguin et al. [39] | MAA. Commercial kit. | Non washed | No | 4.3 | Sodium acetate solution | 5 | 60 | 96.0 ± 1.7 | 15 | Automated | |
| [68Ga]Ga-MAA Purification Conditions | Radiochemical Purity (%) | ||
|---|---|---|---|
| Process of Purification | Manual/Automated | ||
| Maziere et al. [31] | Centrifugation | Manual | 99.9 |
| Even and Green [24] | Centrifugation | Manual | 89.0 ± 5.0–98.4 ± 0.3 |
| Mathias et al. [28] | Centrifugation | Manual | 99.8 ± 0.1 |
| Maus et al. [32] | Sep-Pak C18 cartridge | Manual | >97.0 |
| Ament et al. [33] | Centrifugation | Manual | >97.0 |
| Amor-Coarasa et al. [34] | Centrifugation | Manual | >95.0 |
| Jain et al. [29] | Centrifugation | Manual | 98.0 ± 0.8 |
| Mueller et al. [35] | No purification | >95.0 | |
| Shannehsazzadeh et al. [22] | Centrifugation | Manual | 100.0 |
| Persico et al. [36] | No purification | 97.0 | |
| Gultekin et al. [37] | Centrifugation | Manual | 99.0 |
| Ayșe et al. [38] | No purification | 99.0 | |
| Blanc-Béguin et al. [39] | Filtration | Automated | 99.0 ± 0.6 |
| [99mTc]Tc-MAA | [68Ga]Ga-MAA | ||
|---|---|---|---|
| Labelling conditions | |||
| pH | 6 | 4–6.5 | |
| Heating temperature (°C) | Room temperature | 40–115 °C | |
| Heating time (min) | 0 | 5–20 min | |
| Total labelling time | 20 min | 15–40 min | |
| Size | |||
| µm | 10.0–90.0 | 15.0–75.0 | |
| Labelled MAA suspension stability | |||
| hours | 8 | 3 | |
| Labelled MAA in vitro serum stability | |||
| hours | 24 | 1 | |
| Biodistribution | In humans | In animals | |
| Lungs uptake | % | 98.0 [23] | |
| time | Immediately after injection | ||
| % | 86.6 ± 0.7 [34] | 98.6 ± 0.7 [34] | |
| time | 2 h post-injection | ||
| Kidney uptake | % | 3.6 ± 2.1 [23] | 1.6 ± 0.4 (right kidney), 1.4 ± 0.2 (left kidney) [34] |
| time | 3 h after injection | 4 h after injection | |
| Bladder uptake | % | 5.1 ± 4.0 | 14 ± 1.7 |
| time | 3 h after injection | 4 h after injection [34] | |
| Stomach uptake | % | 3.5 ± 2.5 | |
| time | 4.4 after injection | ||
| Labelled Carbon Primary Nanoparticle Size (nm) | Labelled Carbon Secondary Aggregate Size (nm) | Count Median Diameter (nm) | Labelled Carbon Nanoparticle Thickness (nm) | Shape, Structure and Properties | Physical Properties | ||
|---|---|---|---|---|---|---|---|
| 99mTc labelling | Burch et al. [47] | ≤5.0 | |||||
| Strong et al. [58] | 140.0 ± 1.5 | ||||||
| Isawa et al. [49] | ≤200.0 | ||||||
| Lemb et al. [59] | 12.5 ± 1.65 (7–23) | 118.0 (60–160) | Primary hexagonally structured graphite particles | Hydrophobic properties. Inert properties | |||
| Mackey et al. [46] | Fullerenes | ||||||
| Lloyd et al. [45] | 100.0–300.0 | 158.0 ± 1.5 | |||||
| Senden et al. [44] | 30.0–60.0 | 5.0 | Thin hexagonal platelets with graphite planes oriented parallel to the Tc surface | Biological inertness | |||
| Möller et al. [57] | 10.0 | 100.0–200.0 | Hygroscopic properties | ||||
| Pourchez et al. [51] | 40.0 ± 2.9 | Hexagonal platelets of metallic technetium closely encapsulated with a thin layer of graphitic carbon | Hygroscopic properties | ||||
| Blanc-Béguin et al. [60] | 20.9 ± 7.2 | Thin hexagonal platelets with graphite planes oriented parallel to the Tc surface | |||||
| 68Ga labelling | Blanc-Béguin et al. [60] | 22.4 ± 10 | Several hundreds | Hexagonal shape Layered structure | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanc-Béguin, F.; Hennebicq, S.; Robin, P.; Tripier, R.; Salaün, P.-Y.; Le Roux, P.-Y. Radiopharmaceutical Labelling for Lung Ventilation/Perfusion PET/CT Imaging: A Review of Production and Optimization Processes for Clinical Use. Pharmaceuticals 2022, 15, 518. https://doi.org/10.3390/ph15050518
Blanc-Béguin F, Hennebicq S, Robin P, Tripier R, Salaün P-Y, Le Roux P-Y. Radiopharmaceutical Labelling for Lung Ventilation/Perfusion PET/CT Imaging: A Review of Production and Optimization Processes for Clinical Use. Pharmaceuticals. 2022; 15(5):518. https://doi.org/10.3390/ph15050518
Chicago/Turabian StyleBlanc-Béguin, Frédérique, Simon Hennebicq, Philippe Robin, Raphaël Tripier, Pierre-Yves Salaün, and Pierre-Yves Le Roux. 2022. "Radiopharmaceutical Labelling for Lung Ventilation/Perfusion PET/CT Imaging: A Review of Production and Optimization Processes for Clinical Use" Pharmaceuticals 15, no. 5: 518. https://doi.org/10.3390/ph15050518
APA StyleBlanc-Béguin, F., Hennebicq, S., Robin, P., Tripier, R., Salaün, P. -Y., & Le Roux, P. -Y. (2022). Radiopharmaceutical Labelling for Lung Ventilation/Perfusion PET/CT Imaging: A Review of Production and Optimization Processes for Clinical Use. Pharmaceuticals, 15(5), 518. https://doi.org/10.3390/ph15050518