
Pulmonary Targeting of Levofloxacin Using Microsphere-Based Dry Powder Inhalation

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Results and Discussion
2.1. Preparation of LVX-Loaded Microspheres
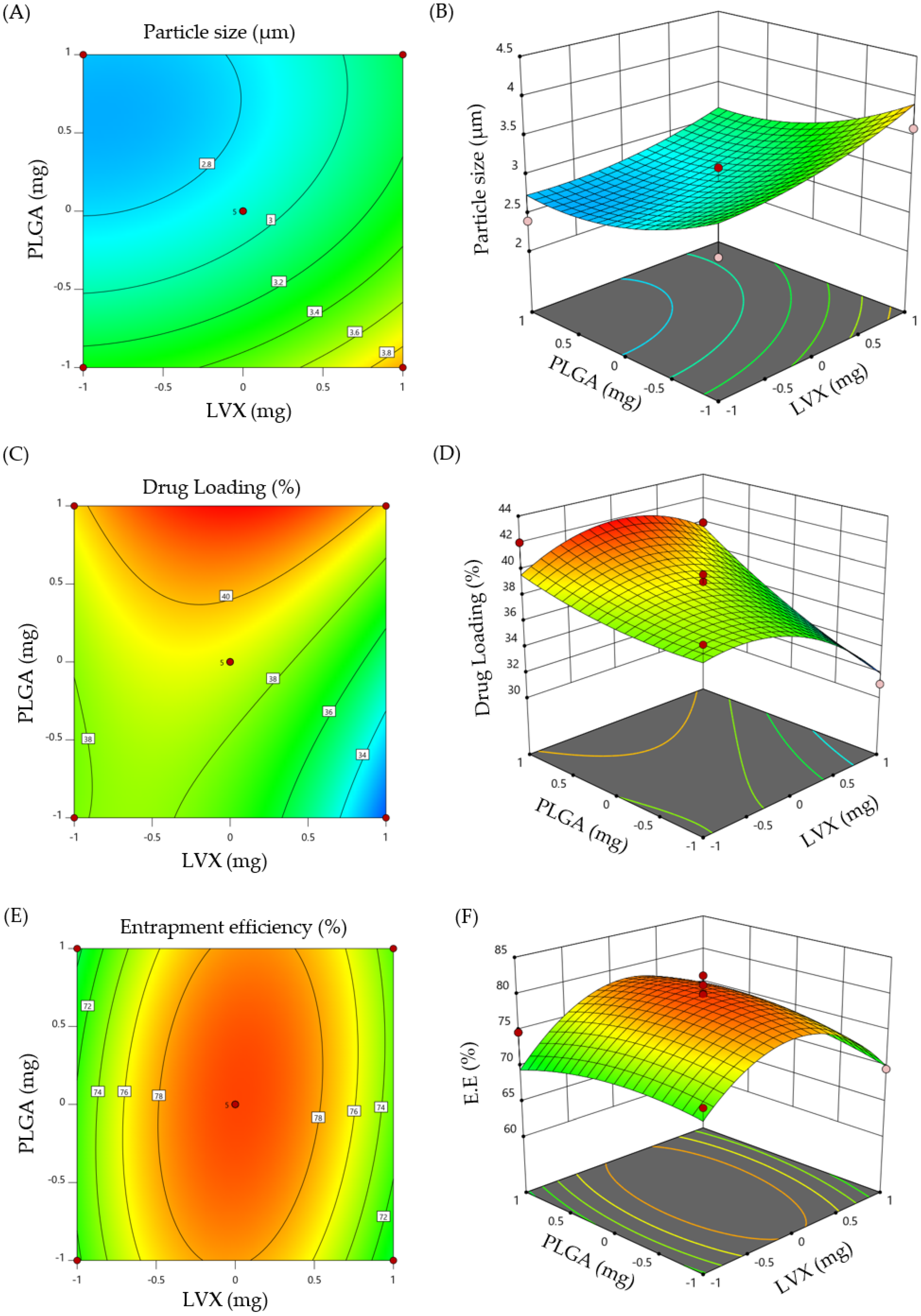
2.1.1. Central Composite Design (CCD)
2.1.2. Optimization of LVX-Loaded Microspheres
2.2. Characterization of Optimized LVX-Loaded Microspheres
2.2.1. Particle Size
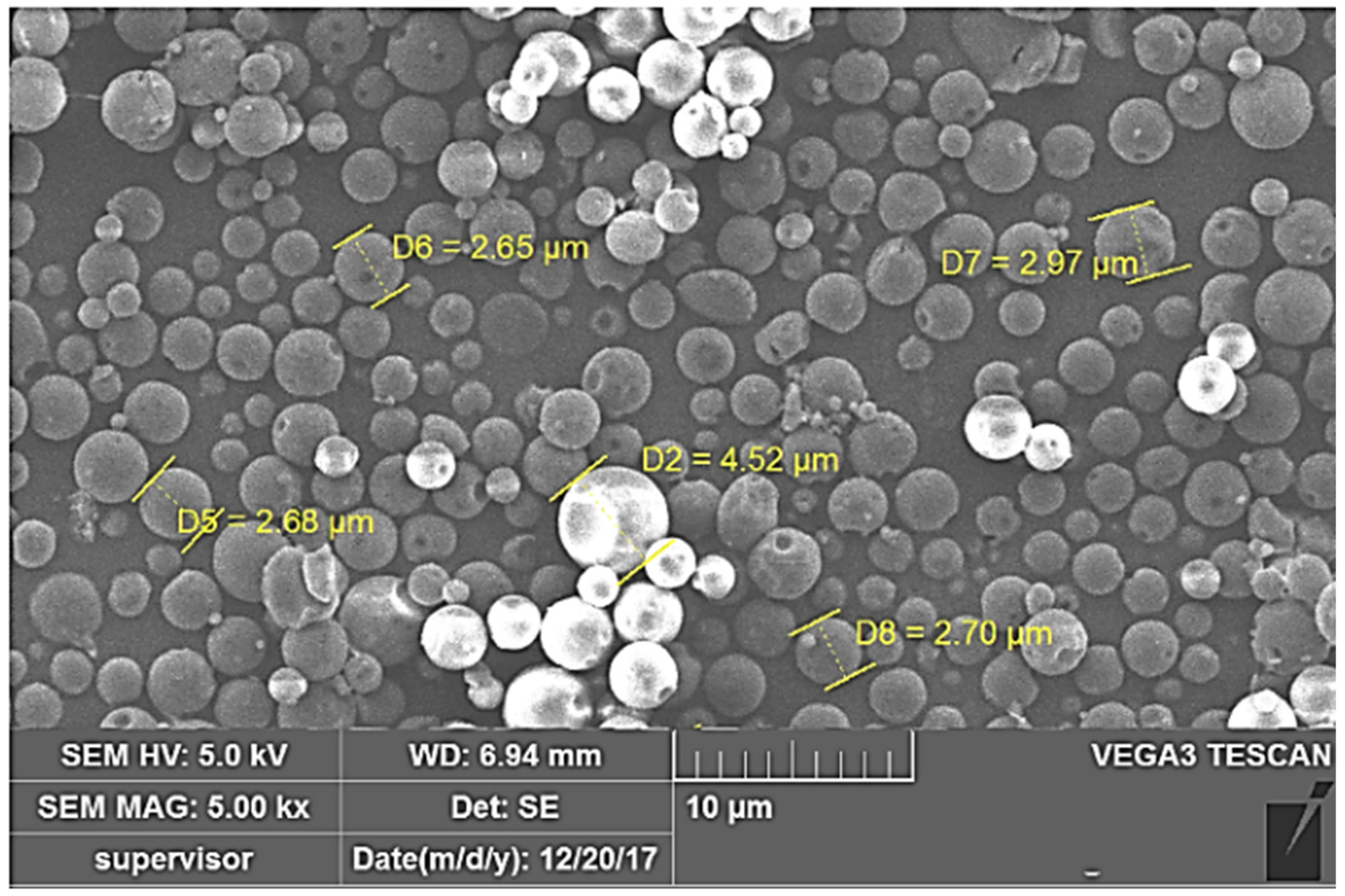
2.2.2. Particle Morphology
2.3. Micromeritic Characteristics of LVX-Loaded Microspheres
2.3.1. Moisture Content
2.3.2. Flow Properties
2.3.3. Aerodynamic Diameter
2.4. Structural Characteristics
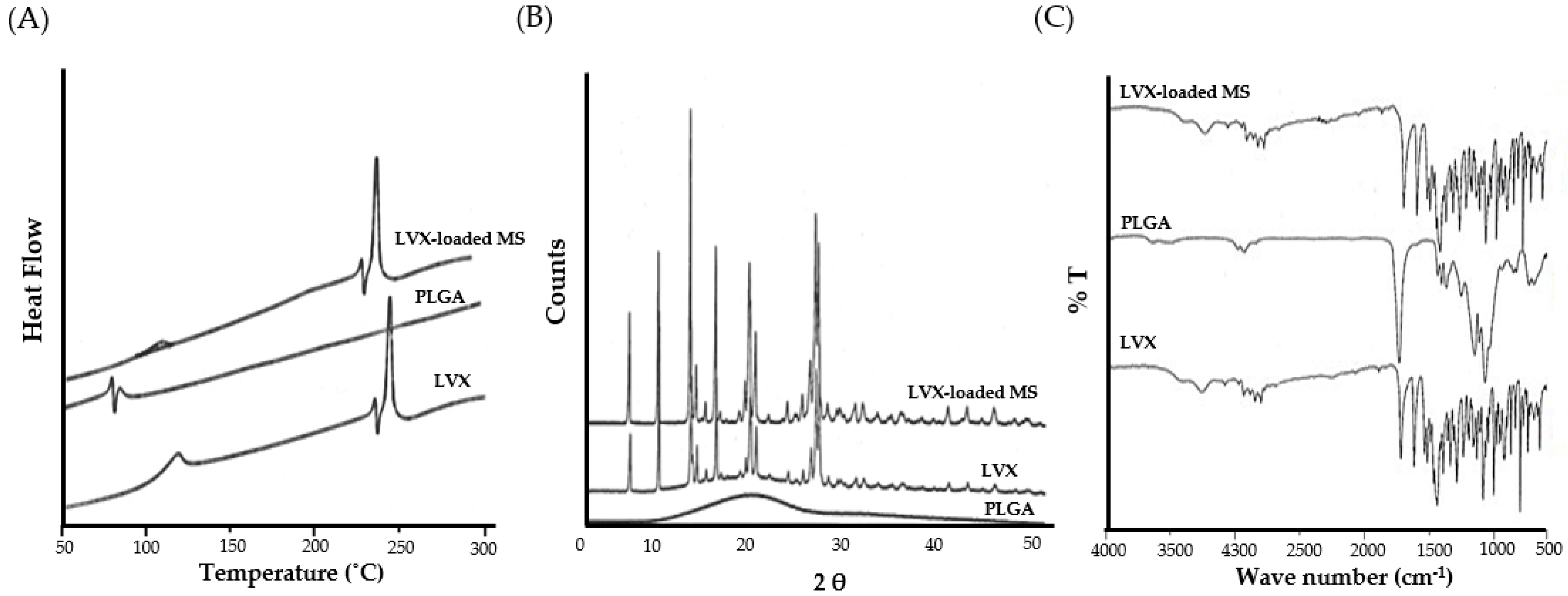
2.4.1. Differential Scanning Calorimetry (DSC)
2.4.2. X-ray Diffraction (XRD) Analysis
2.4.3. Fourier Transform Infra-Red (FTIR) Spectroscopy
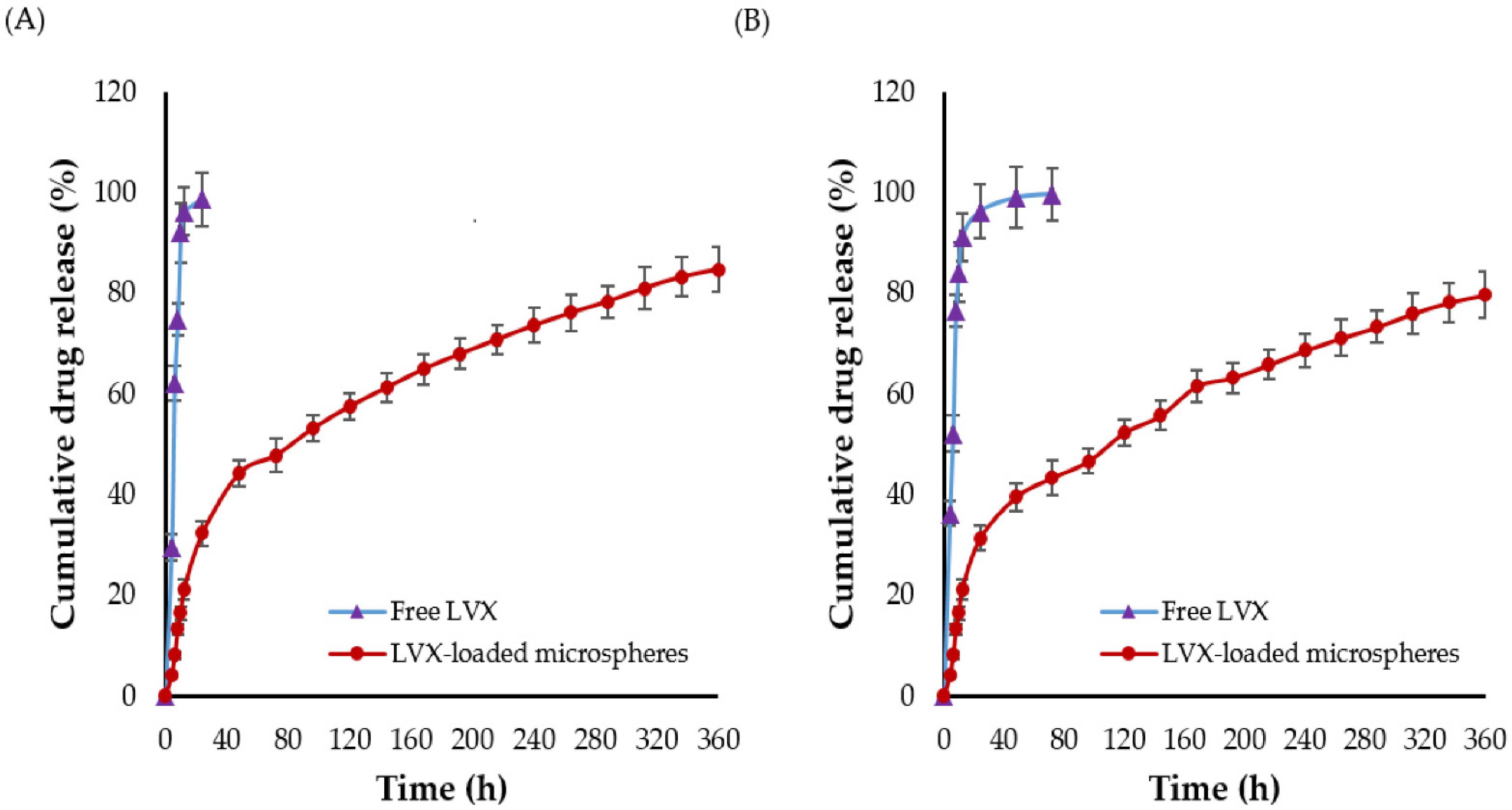
2.5. In Vitro Drug Release
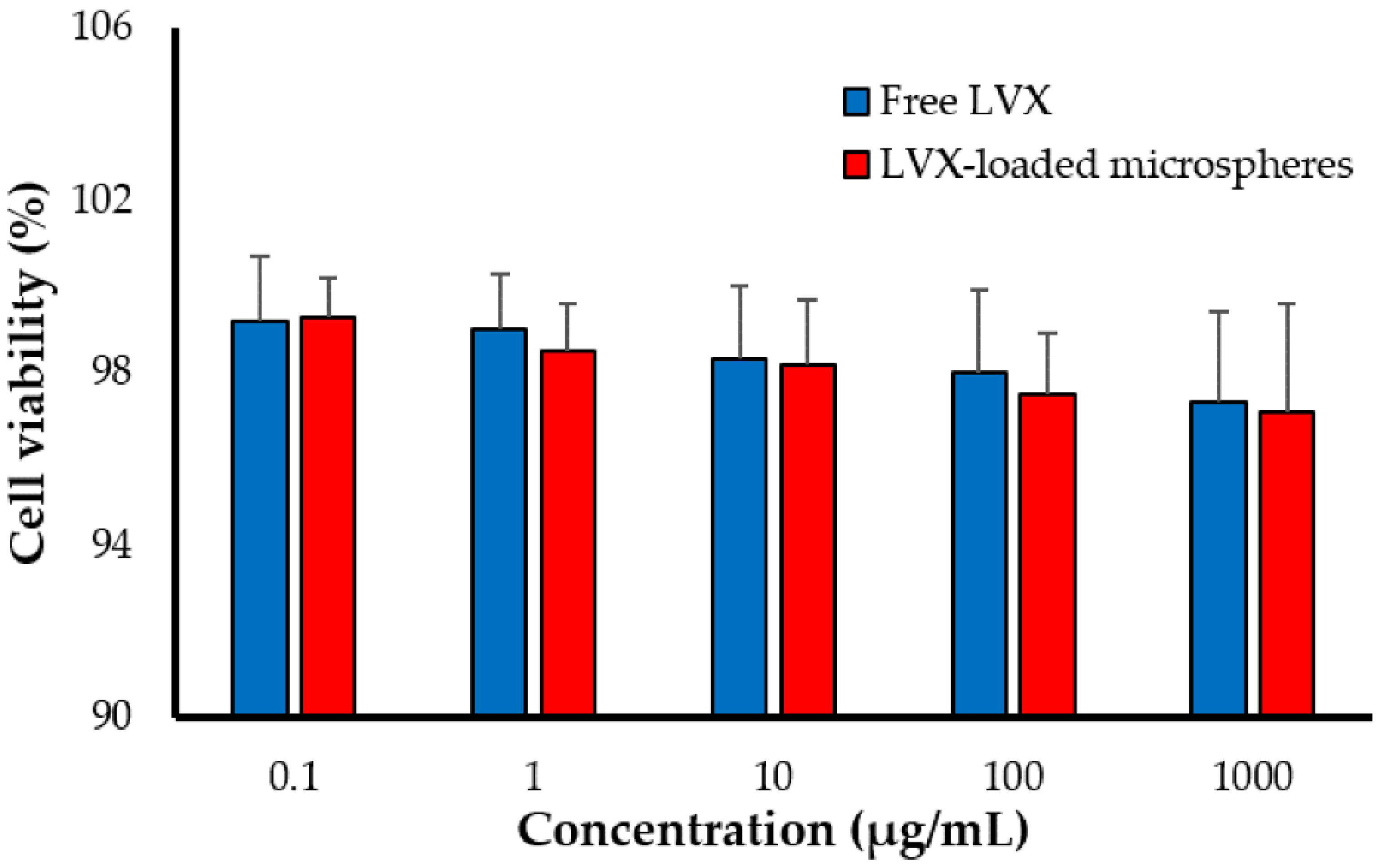
2.6. Cytotoxicity of LVX-Loaded PLGA Microspheres against Alveolar Macrophages
2.7. Stabilty Studies
2.8. In Vivo Studies
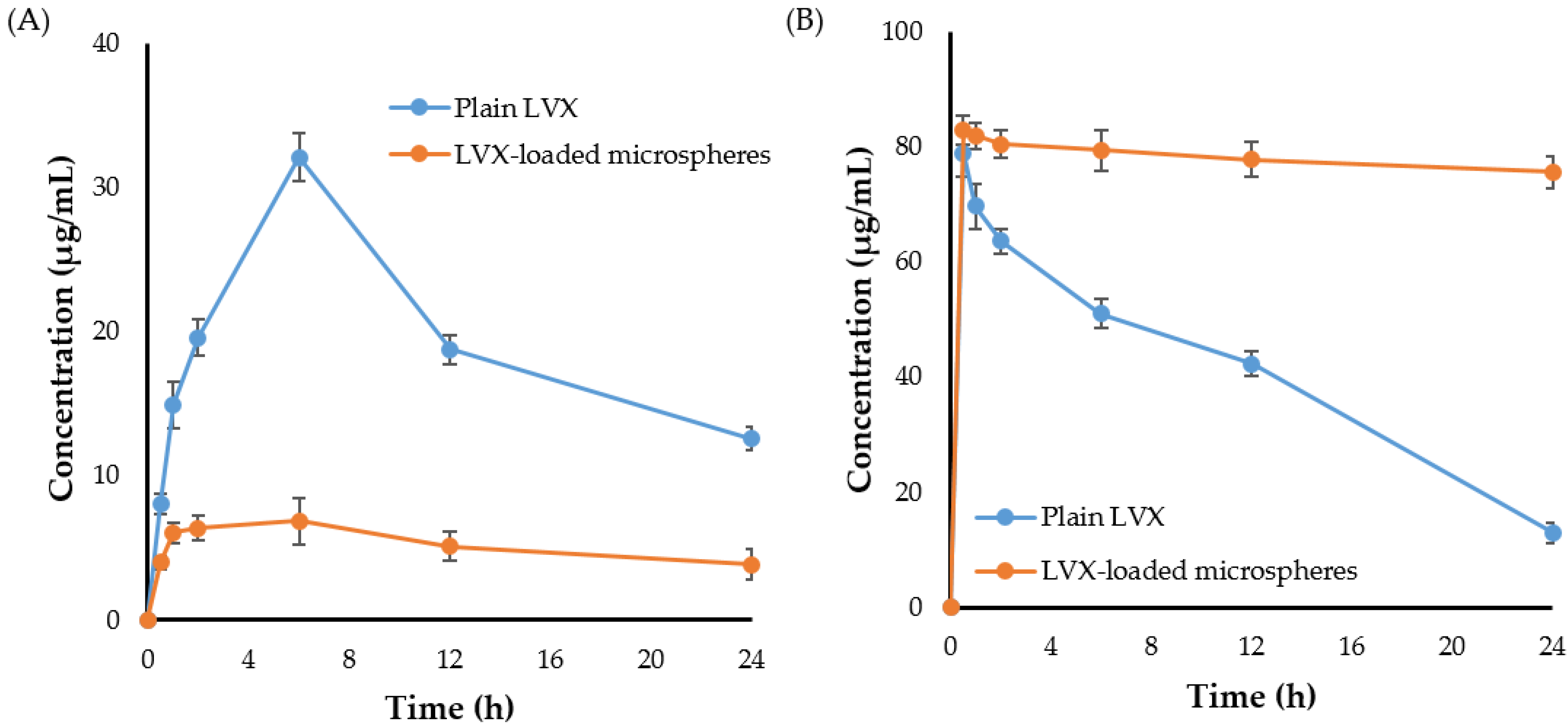
2.8.1. Pulmonary Pharmacokinetics
2.8.2. Biodistribution Study
3. Materials and Methods
3.1. Materials
3.2. Preparation and Optimization of LVX-Loaded PLGA Microspheres
3.2.1. Fabrication of LVX-Loaded Microspheres
3.2.2. Experimental Design
3.3. Structural Characterization of LVX-Loaded Microspheres
3.3.1. Differential Scanning Calorimetry (DSC) Studies
3.3.2. Powder X-ray Diffraction Analysis
3.3.3. Fourier Transform Infra-Red Spectroscopy (FTIR) Study
3.4. Characterization of LVX-Loaded Microspheres
3.4.1. Particle Size Determination
3.4.2. Microsphere Surface Morphology
3.4.3. Determination of Drug Loading and Encapsulation Efficiency
3.5. Micrometric Properties of Prepared Microspheres
3.5.1. Determination of Bulk Density (ρb)
3.5.2. Flowability Testing
3.5.3. Determination of Moisture Content
3.5.4. In Vitro Deposition by Andersen Cascade Impactor
3.6. In Vitro Studies on Drug Release of the Optimized Microspheres
3.7. In Vitro Cytotoxicity of LVX-Loaded PLGA Microspheres against Alveolar Murine Macrophages
3.8. Stability Studies
3.9. In Vivo Studies
3.9.1. Animals
3.9.2. Pharmacokinetic and Organ Biodistribution Study of LVX-Loaded Microspheres
3.10. Statistical Analysis
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smith, I. Mycobacterium tuberculosis pathogenesis and molecular determinants of virulence. Clin. Microbiol. Rev. 2003, 16, 463–496. [Google Scholar] [CrossRef] [Green Version]
- Gengenbacher, M.; Kaufmann, S.H.E. Mycobacterium tuberculosis: Success through dormancy. FEMS Microbiol. Rev. 2012, 36, 514–532. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y. Diagnosis and treatment of extrapulmonary tuberculosis. Tuberc. Respir. Dis. 2015, 78, 47–55. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Consolidated Guidelines on Tuberculosis 2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/340255/9789240022676-eng.pdf (accessed on 13 February 2021).
- World Health Organization. Updates on the Treatment of Drug-Susceptible Tuberculosis 2021. Available online: https://www.who.int/news/item/14-06-2021-who-announces-updates-on-the-treatment-of-drug-susceptible-tuberculosis_14062021 (accessed on 13 February 2021).
- Richeldi, L.; Covi, M.; Ferrara, G.; Franco, F.; Vailati, P.; Meschiari, E.; Fabbri, L.M.; Velluti, G. Clinical use of Levofloxacin in the long-term treatment of drug resistant tuberculosis. Monaldi Arch. Chest Dis. 2002, 57, 39–43. [Google Scholar]
- Pranger, A.D.; van der Werf, T.S.; Kosterink, J.G.W.; Alffenaar, J.W.C. The Role of Fluoroquinolones in the Treatment of Tuberculosis in 2019. Drugs 2019, 79, 161–171. [Google Scholar] [CrossRef] [Green Version]
- Lanoix, J.P.; Chaisson, R.E.; Nuermberger, E.L. Shortening Tuberculosis Treatment with Fluoroquinolones: Lost in Translation? Clin. Infect. Dis. 2016, 62, 484–490. [Google Scholar] [CrossRef] [Green Version]
- Aubry, A.; Pan, X.S.; Fisher, L.M.; Jarlier, V.; Cambau, E. Mycobacterium tuberculosis DNA gyrase: Interaction with quinolones and correlation with antimycobacterial drug activity. Antimicrob. Agents Chemother. 2004, 48, 1281–1288. [Google Scholar] [CrossRef] [Green Version]
- Johnson, J.L.; Hadad, D.J.; Boom, W.H.; Daley, C.L.; Peloquin, C.A.; Eisenach, K.D.; Jankus, D.D.; Debanne, S.M.; Charlebois, E.D.; Maciel, E.; et al. Early and extended early bactericidal activity of levofloxacin, gatifloxacin and moxifloxacin in pulmonary tuberculosis. Int. J. Tuberc. Lung Dis. 2006, 10, 605–612. [Google Scholar]
- Campbell, S.; Smeets, N. Drug Delivery: Localized and Systemic Therapeutic Strategies with Polymer Systems. In Functional Polymers; Jafar Mazumder, M.A., Sheardown, H., Al-Ahmed, A., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 1–56. [Google Scholar]
- Labiris, N.R.; Dolovich, M.B. Pulmonary drug delivery. Part I: Physiological factors affecting therapeutic effectiveness of aerosolized medications. Br. J. Clin. Pharmacol. 2003, 56, 588–599. [Google Scholar] [CrossRef]
- Murgia, X.; de Souza Carvalho, C.; Lehr, C.-M. Overcoming the pulmonary barrier: New insights to improve the efficiency of inhaled therapeutics. Eur. J. Nanomed. 2014, 6, 157–169. [Google Scholar] [CrossRef]
- Tse, J.Y.; Kadota, K.; Imakubo, T.; Uchiyama, H.; Tozuka, Y. Enhancement of the extra-fine particle fraction of levofloxacin embedded in excipient matrix formulations for dry powder inhaler using response surface methodology. Eur. J. Pharm. Sci. 2021, 156, 105600. [Google Scholar] [CrossRef] [PubMed]
- Laohapojanart, N.; Ratanajamit, C.; Kawkitinarong, K.; Srichana, T. Efficacy and safety of combined isoniazid-rifampicin-pyrazinamide-levofloxacin dry powder inhaler in treatment of pulmonary tuberculosis: A randomized controlled trial. Pulm. Pharmacol. Ther. 2021, 70, 102056. [Google Scholar] [CrossRef] [PubMed]
- Akdag Cayli, Y.; Sahin, S.; Buttini, F.; Balducci, A.G.; Montanari, S.; Vural, I.; Oner, L. Dry powders for the inhalation of ciprofloxacin or levofloxacin combined with a mucolytic agent for cystic fibrosis patients. Drug Dev. Ind. Pharm. 2017, 43, 1378–1389. [Google Scholar] [CrossRef]
- Mehta, P.; Bothiraja, C.; Kadam, S.; Pawar, A. Potential of dry powder inhalers for tuberculosis therapy: Facts, fidelity and future. Artif. Cells Nanomed. Biotechnol. 2018, 46, S791–S806. [Google Scholar] [CrossRef]
- Emami, F.; Mostafavi Yazdi, S.J.; Na, D.H. Poly(lactic acid)/poly(lactic-co-glycolic acid) particulate carriers for pulmonary drug delivery. J. Pharm. Investig. 2019, 49, 427–442. [Google Scholar] [CrossRef] [Green Version]
- Coowanitwong, I.; Arya, V.; Kulvanich, P.; Hochhaus, G. Slow release formulations of inhaled rifampin. AAPS J. 2008, 10, 342–348. [Google Scholar] [CrossRef] [Green Version]
- Lu, D.; Garcia-Contreras, L.; Xu, D.; Kurtz, S.L.; Liu, J.; Braunstein, M.; McMurray, D.N.; Hickey, A.J. Poly (lactide-co-glycolide) microspheres in respirable sizes enhance an in vitro T cell response to recombinant Mycobacterium tuberculosis antigen 85B. Pharm. Res. 2007, 24, 1834–1843. [Google Scholar] [CrossRef]
- Rawat, A.; Majumder, Q.H.; Ahsan, F. Inhalable large porous microspheres of low molecular weight heparin: In vitro and in vivo evaluation. J. Control. Release Off. J. Control. Release Soc. 2008, 128, 224–232. [Google Scholar] [CrossRef] [Green Version]
- Thomas, R.J. Particle size and pathogenicity in the respiratory tract. Virulence 2013, 4, 847–858. [Google Scholar] [CrossRef] [Green Version]
- Darquenne, C. Aerosol deposition in health and disease. J. Aerosol. Med. Pulm. Drug Deliv. 2012, 25, 140–147. [Google Scholar] [CrossRef] [Green Version]
- Champion Julie, A.; Mitragotri, S. Role of target geometry in phagocytosis. Proc. Natl. Acad. Sci. USA 2006, 103, 4930–4934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lippmann, M.; Yeates, D.B.; Albert, R.E. Deposition, Retention, and Clearance of Inhaled Particles. Br. J. Ind. Med. 1980, 37, 337–362. [Google Scholar] [CrossRef] [Green Version]
- Geiser, M. Morphological aspects of particle uptake by lung phagocytes. Microsc. Res. Tech. 2002, 57, 512–522. [Google Scholar] [CrossRef]
- Kwon, Y.B.; Kang, J.H.; Han, C.S.; Kim, D.W.; Park, C.W. The Effect of Particle Size and Surface Roughness of Spray-Dried Bosentan Microparticles on Aerodynamic Performance for Dry Powder Inhalation. Pharmaceutics 2020, 12, 765. [Google Scholar] [CrossRef]
- Shetty, N.; Cipolla, D.; Park, H.; Zhou, Q.T. Physical stability of dry powder inhaler formulations. Expert Opin. Drug Deliv. 2020, 17, 77–96. [Google Scholar] [CrossRef] [Green Version]
- Lu, X.-Y.; Chen, L.; Wu, C.-Y.; Chan, H.-K.; Freeman, T. The Effects of Relative Humidity on the Flowability and Dispersion Performance of Lactose Mixtures. Materials 2017, 10, 592. [Google Scholar] [CrossRef] [Green Version]
- Murata, S.; Ito, H.; Izumi, T.; Chikushi, A. Effect of the moisture content in aerosol on the spray performance of Stmerin D HFA preparations. Chem. Pharm. Bull. 2006, 54, 1276–1280. [Google Scholar] [CrossRef] [Green Version]
- Singh, D.J.; Lohade, A.A.; Parmar, J.J.; Hegde, D.D.; Soni, P.; Samad, A.; Menon, M.D. Development of Chitosan-based Dry Powder Inhalation System of Cisplatin for Lung Cancer. Indian J. Pharm. Sci. 2012, 74, 521–526. [Google Scholar] [CrossRef] [Green Version]
- Chaurasiya, B.; Zhao, Y.-Y. Dry Powder for Pulmonary Delivery: A Comprehensive Review. Pharmaceutics 2021, 13, 31. [Google Scholar] [CrossRef]
- Makadia, H.K.; Siegel, S.J. Poly Lactic-co-Glycolic Acid (PLGA) as Biodegradable Controlled Drug Delivery Carrier. Polymers 2011, 3, 1377–1397. [Google Scholar] [CrossRef]
- Sabry, H.S.; Al-Shohani, A.D.H.; Mahmood, S.Z. Formulation and Evaluation of Levofloxacin and Betamethasone Ophthalmic Emulgel. J. Pharm. Bioallied Sci. 2021, 13, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Denkbaş, E.B.; Seyyal, M.; Pişkin, E. 5-fluorouracil loaded chitosan microspheres for chemoembolization. J. Microencapsul. 1999, 16, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Patton, J.S.; Fishburn, C.S.; Weers, J.G. The Lungs as a Portal of Entry for Systemic Drug Delivery. Proc. Am. Thorac. Soc. 2004, 1, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Wang, L.; Tian, L.; Zhang, X.; Huang, G. Tadalafil-loaded PLGA microspheres for pulmonary administration: Preparation and evaluation. Braz. J. Pharm. Sci. 2019, 55, e17536. [Google Scholar] [CrossRef] [Green Version]
- Kuzmov, A.; Minko, T. Nanotechnology approaches for inhalation treatment of lung diseases. J. Control. Release 2015, 219, 500–518. [Google Scholar] [CrossRef] [Green Version]
- Borghardt, J.M.; Kloft, C.; Sharma, A. Inhaled Therapy in Respiratory Disease: The Complex Interplay of Pulmonary Kinetic Processes. Can. Respir. J. 2018, 2018, 2732017. [Google Scholar] [CrossRef] [Green Version]
- Saigal, A.; Ng, W.K.; Tan, R.B.; Chan, S.Y. Controlled Release Inhalable Polymeric Microspheres for Treatment of Pulmonary Arterial Hypertension. Curr. Pharm. Des. 2015, 21, 5868–5876. [Google Scholar] [CrossRef]
- Harush-Frenkel, O.; Bivas-Benita, M.; Nassar, T.; Springer, C.; Sherman, Y.; Avital, A.; Altschuler, Y.; Borlak, J.; Benita, S. A safety and tolerability study of differently-charged nanoparticles for local pulmonary drug delivery. Toxicol. Appl. Pharm. 2010, 246, 83–90. [Google Scholar] [CrossRef]
- O’Donnell, P.B.; McGinity, J.W. Preparation of microspheres by the solvent evaporation technique. Adv. Drug Deliv. Rev. 1997, 28, 25–42. [Google Scholar] [CrossRef]
- Abu Lila, A.S.; Soliman, M.S.; Kiran, H.C.; Gangadharappa, H.V.; Younes, K.M.; Khafagy, E.-S.; Shehata, T.M.; Ibrahim, M.M.; Abdallah, M.H. Tamoxifen-loaded functionalized graphene nanoribbons for breast cancer therapy. J. Drug Deliv. Sci. Technol. 2021, 63, 102499. [Google Scholar] [CrossRef]
- Hasan, A.A.; Samir, R.M.; Abu-Zaid, S.S.; Abu Lila, A.S. Revitalizing the local anesthetic effect of Mebeverine hydrochloride via encapsulation within ethosomal vesicular system. Colloids Surf. B Biointerfaces 2020, 194, 111208. [Google Scholar] [CrossRef] [PubMed]
- Al Saqr, A.; Khafagy, E.-S.; Alalaiwe, A.; Aldawsari, M.F.; Alshahrani, S.M.; Anwer, M.K.; Khan, S.; Lila, A.S.A.; Arab, H.H.; Hegazy, W.A.H. Synthesis of Gold Nanoparticles by Using Green Machinery: Characterization and In Vitro Toxicity. Nanomaterials 2021, 11, 808. [Google Scholar] [CrossRef]
- Beakawi Al-Hashemi, H.M.; Baghabra Al-Amoudi, O.S. A review on the angle of repose of granular materials. Powder Technol. 2018, 330, 397–417. [Google Scholar] [CrossRef]
- Krasucka, D.M.; Kos, K.; Cybulski, W.A.; Mitura, A.; Łysiak, E.; Pietroń, W.J. Karl Fisher determination of residual moisture in veterinary vaccines—Practical implementation in market monitoring. Acta Pol. Pharm. 2012, 69, 1364–1367. [Google Scholar]
- Sharma, R.; Saxena, D.; Dwivedi, A.K.; Misra, A. Inhalable microparticles containing drug combinations to target alveolar macrophages for treatment of pulmonary tuberculosis. Pharm. Res. 2001, 18, 1405–1410. [Google Scholar] [CrossRef]
- Kaur, J.; Muttil, P.; Verma, R.K.; Kumar, K.; Yadav, A.B.; Sharma, R.; Misra, A. A hand-held apparatus for “nose-only” exposure of mice to inhalable microparticles as a dry powder inhalation targeting lung and airway macrophages. Eur. J. Pharm. Sci. 2008, 34, 56–65. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formula | Coded Values | Actual Values of Independence Values | Responses Variables | ||||
|---|---|---|---|---|---|---|---|
| X1 | X2 | X1 (mg) | X2 (mg) | Y1 (µm) | Y2 (%) | Y3 (%) | |
| MS1 | 1.414 | 0 | 11.03 | 7.5 | 3.8 ± 0.45 | 32.9 ± 2.1 | 64.87 ± 4.8 |
| MS2 | 0 | 1.414 | 7.5 | 11.03 | 3.2 ± 0.37 | 41.98 ± 3.2 | 71.87 ± 6.5 |
| MS3 | +1 | +1 | 10 | 10 | 2.9 ± 0.31 | 39.97 ± 2.9 | 75.98 ± 6.3 |
| MS4 | −1 | −1 | 5 | 5 | 2.9 ± 0.30 | 39.09 ± 2.7 | 73.27 ± 5.9 |
| MS5 | 0 | −1.414 | 7.5 | 3.96 | 4.2 ± 0.29 | 36.98 ± 2.5 | 76.59 ± 6.2 |
| MS6 | 0 | 0 | 7.5 | 7.5 | 2.9 ± 0.19 | 38.87 ± 3.1 | 78.25 ± 6.1 |
| MS7 | −1 | +1 | 5 | 10 | 2.4 ± 0.17 | 42.03 ± 2.9 | 74.78 ± 5.8 |
| MS8 | 0 | 0 | 7.5 | 7.5 | 2.9 ± 0.20 | 39.09 ± 2.6 | 80.06 ± 6.8 |
| MS9 | 0 | 0 | 7.5 | 7.5 | 2.8 ± 0.19 | 39.65 ± 2.6 | 79.98 ± 6.5 |
| MS10 | 0 | 0 | 7.5 | 7.5 | 2.9 ± 0.19 | 38.93 ± 2.4 | 81.26 ± 5.9 |
| MS11 | 0 | 0 | 7.5 | 7.5 | 3.1 ± 0.21 | 38.76 ± 3.5 | 80.01 ± 5.7 |
| MS12 | −1.414 | 0 | 3.96 | 7.5 | 3.2 ± 0.18 | 34.09 ± 1.8 | 60.87 ± 4.7 |
| MS13 | +1 | −1 | 10 | 5 | 3.6 ± 0.22 | 31.09 ± 1.9 | 69.65 ± 4.5 |
| Parameters | Pure LVX | LVX-Loaded Microspheres |
|---|---|---|
| Bulk Density | 0.22 ± 0.02 g/cm3 | 0.39 ± 0.06 g/cm3 |
| Tapped Density | 0.31 ± 0.01 g/cm3 | 0.48 ± 0.08 g/cm3 |
| Carr’s Index | 29.03 | 18.75 |
| Hausner’s ratio | 1.41 | 1.23 |
| Angle of Repose (θ) | 42 ± 2° | 29 ± 1° |
| Parameters | Pure LVX | LVX-Loaded Microspheres |
|---|---|---|
| Recovered dose (RD (µg)) | 99.05 ± 0.99 | 91.76 ± 1.54 |
| Emitted dose (ED (µg)) | 82.34 ± 1.99 | 83.12 ± 2.18 |
| Fine particle dose (FPD (µg)) | 51.87 ± 1.23 | 67.98 ± 1.54 |
| Fine particle fraction (FPF (%)) | 53.70 ± 1.76 | 75.35 ± 1.42 |
| Mass median aerodynamic diameter (MMAD (µm)) | 4.24± 1.37 | 2.13 ± 1.24 |
| Geometric standard deviation (GSD) | 2.38 ± 1.09 | 3.61 ± 0.87 |
| Stability Condition | Time Point | Drug Loading (%) | Particle Size (μm) | Entrapment Efficiency (%) |
|---|---|---|---|---|
| 4 ± 1 °C ambient RH | Initial | 40.85 ± 2.09 | 2.86 ± 0.26 | 77.80 ± 1.98 |
| 2 weeks | 40.93 ± 2.13 | 2.87 ± 0.21 | 77.45 ± 1.56 | |
| 1 month | 40.68 ± 1.98 | 2.89 ± 0.24 | 77.76 ± 1.83 | |
| 2 months | 40.81 ± 1.09 | 2.93 ± 0.29 | 77.79 ± 1.11 | |
| 3 months | 40.34 ± 1.11 | 2.96 ± 0.26 | 77.82 ± 1.35 | |
| 6 months | 40.69 ± 2.01 | 2.99 ± 0.29 | 77.59 ± 1.55 | |
| 25 ± 2 °C 60 ± 5% RH | Initial | 40.85 ± 1.10 | 2.86 ± 0.26 | 77.80 ± 1.86 |
| 2 weeks | 40.67 ± 0.99 | 2.89 ± 0.21 | 77.91 ± 2.01 | |
| 1 month | 40.09 ± 1.56 | 2.91 ± 0.24 | 77.39 ± 1.72 | |
| 2 months | 40.63 ± 2.04 | 2.95 ± 0.29 | 77.69 ± 1.20 | |
| 3 months | 40.77 ± 1.87 | 2.97 ± 0.26 | 77.79 ± 1.71 | |
| 6 months | 40.81 ± 1.43 | 3.01 ± 0.29 | 77.81 ± 1.84 | |
| 40 ± 2 °C 75 ± 5% RH | Initial | 40.85 ± 1.25 | 2.86 ± 0.26 | 77.80 ± 1.77 |
| 2 weeks | 39.97 ± 1.22 | 2.90 ± 0.31 | 77.79 ± 2.00 | |
| 1 month | 39.09 ± 1.89 | 2.92 ± 0.28 | 77.32 ± 2.14 | |
| 2 months | 38.12 ± 1.59 | 2.98 ± 0.30 | 76.97 ± 0.99 | |
| 3 months | 37.64 ± 1.45 | 3.01 ± 0.22 | 76.01 ± 1.54 | |
| 6 months | 33.87 ± 1.37 | 3.03 ± 0.34 | 73.89 ± 1.64 |
| Pharmacokinetic Parameters | Plasma | Lung | ||
|---|---|---|---|---|
| Plain LVX | LVX-Loaded Microspheres | Plain LVX | LVX-Loaded Microspheres | |
| Cmax (μg/mL) | 32.08 ± 2.6 | 6.84 ± 0.76 | 78.92 ± 4.50 | 82.86 ± 5.76 |
| T1/2 (h) | 14.03 ± 0.71 | 22.68 ± 1.98 | 9.72 ± 0.51 | 248.75 ± 10.12 |
| AUC0–24 (μg/mL.h) | 468.59 ± 13.81 | 125.74 ± 14.13 | 964.04 ±14.84 | 1854.08 ± 23.62 |
| MRT (h) | 22.34 ± 2.15 | 33.78 ± 2.81 | 13.33 ± 0.87 | 359.14 ± 20.88 |
| Formulation | Organ | % Dose Detected | |||||
|---|---|---|---|---|---|---|---|
| 0.5 h | 1 h | 2 h | 6 h | 12 h | 24 h | ||
| Plain LVX | Serum | 9.70 ± 1.81 | 15.91 ± 2.18 | 18.80 ± 1.74 | 26.78 ± 2.51 | 17.65 ± 1.29 | 13.12 ± 1.11 |
| Lung | 78.95 ± 2.97 | 69.76 ± 2.26 | 60.53 ± 2.32 | 49.12 ± 1.34 | 42.79 ± 1.53 | 28.60 ± 1.79 | |
| Liver | 2.37 ± 1.06 | 3.01 ± 0.97 | 4.27 ± 1.11 | 5.05 ± 1.72 | 7.07 ± 1.65 | 8.35 ± 1.96 | |
| Spleen | 1.38 ± 0.40 | 2.75 ± 0.67 | 4.35 ± 1.02 | 4.19 ± 1.11 | 4.72 ± 0.98 | 5.04 ± 1.14 | |
| Kidney | ND * | 0.62 ± 0.20 | 1.17 ± 0.45 | 2.04 ± 0.41 | 1.78 ± 0.34 | 1.49 ± 0.47 | |
| LVX-loaded microspheres | Serum | 4.24 ± 1.45 | 5.8 ± 1.69 | 6.34 ± 1.74 | 6.525 ± 1.52 | 4.755 ± 1.49 | 3.735 ± 1.24 |
| Lung | 85.94 ± 3.61 | 82.32 ± 2.11 | 80.15 ± 2.43 | 78.05 ± 1.42 | 76.79 ± 1.68 | 74.11 ± 2.05 | |
| Liver | 1.71 ± 0.64 | 2.15 ± 0.79 | 2.68 ± 0.83 | 2.98 ± 1.01 | 3.36 ± 1.12 | 3.17 ± 0.98 | |
| Spleen | 0.55 ± 0.11 | 0.72 ± 0.16 | 0.95 ± 0.14 | 1.3 ± 0.19 | 0.81 ± 0.21 | 1.18 ± 0.26 | |
| Kidney | ND * | 0.57 ± 0.19 | 1.29 ± 0.23 | 1.69 ± 0.31 | 1.59 ± 0.45 | 0.45 ± 0.11 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Hagbani, T.; Vishwa, B.; Abu Lila, A.S.; Alotaibi, H.F.; Khafagy, E.-S.; Moin, A.; Gowda, D.V. Pulmonary Targeting of Levofloxacin Using Microsphere-Based Dry Powder Inhalation. Pharmaceuticals 2022, 15, 560. https://doi.org/10.3390/ph15050560
Al Hagbani T, Vishwa B, Abu Lila AS, Alotaibi HF, Khafagy E-S, Moin A, Gowda DV. Pulmonary Targeting of Levofloxacin Using Microsphere-Based Dry Powder Inhalation. Pharmaceuticals. 2022; 15(5):560. https://doi.org/10.3390/ph15050560
Chicago/Turabian StyleAl Hagbani, Turki, Bhavya Vishwa, Amr S. Abu Lila, Hadil Faris Alotaibi, El-Sayed Khafagy, Afrasim Moin, and Devegowda V. Gowda. 2022. "Pulmonary Targeting of Levofloxacin Using Microsphere-Based Dry Powder Inhalation" Pharmaceuticals 15, no. 5: 560. https://doi.org/10.3390/ph15050560
APA StyleAl Hagbani, T., Vishwa, B., Abu Lila, A. S., Alotaibi, H. F., Khafagy, E. -S., Moin, A., & Gowda, D. V. (2022). Pulmonary Targeting of Levofloxacin Using Microsphere-Based Dry Powder Inhalation. Pharmaceuticals, 15(5), 560. https://doi.org/10.3390/ph15050560