
[99mTc]Tc-iFAP Radioligand for SPECT/CT Imaging of the Tumor Microenvironment: Kinetics, Radiation Dosimetry, and Imaging in Patients

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Results
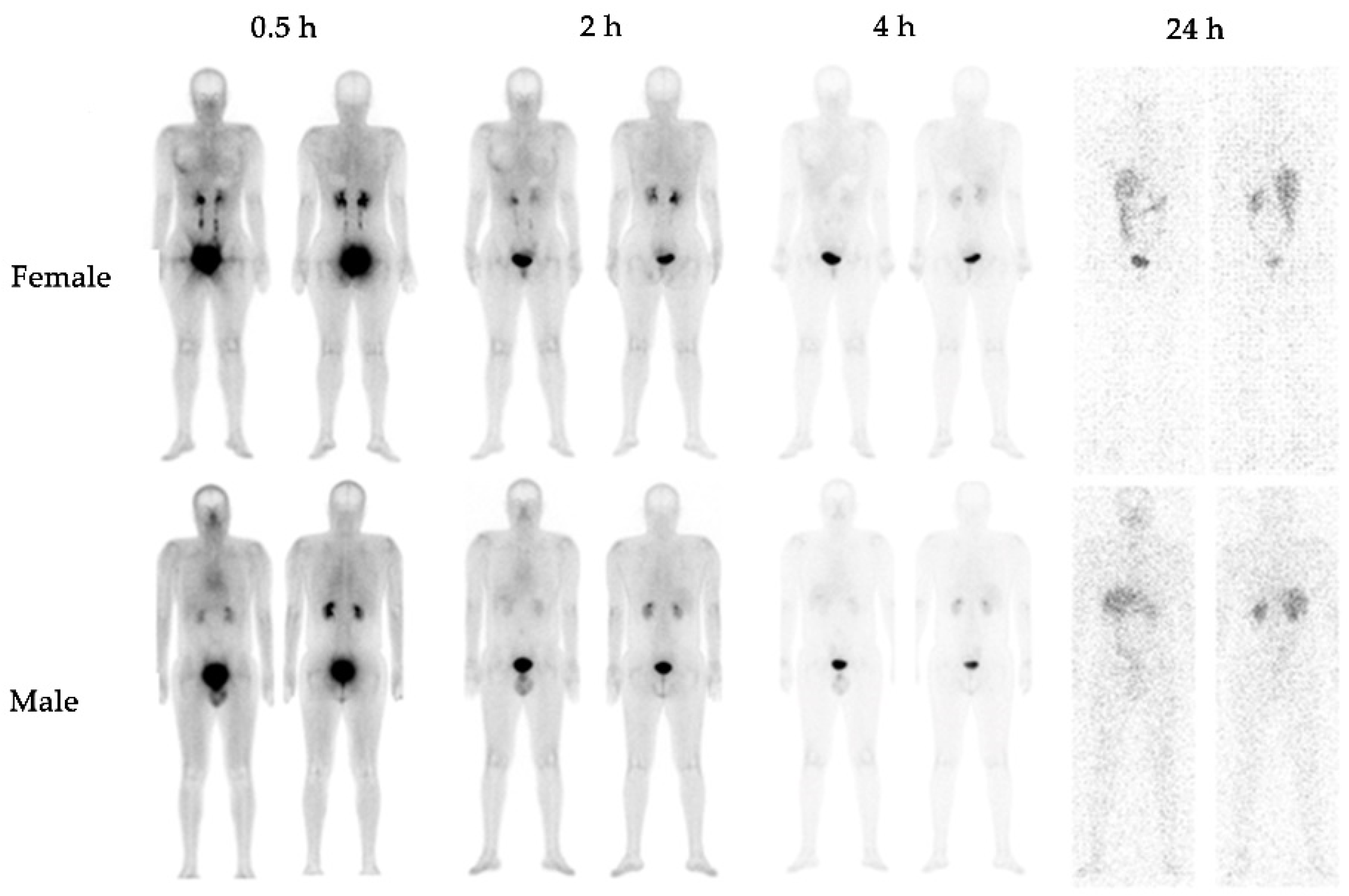
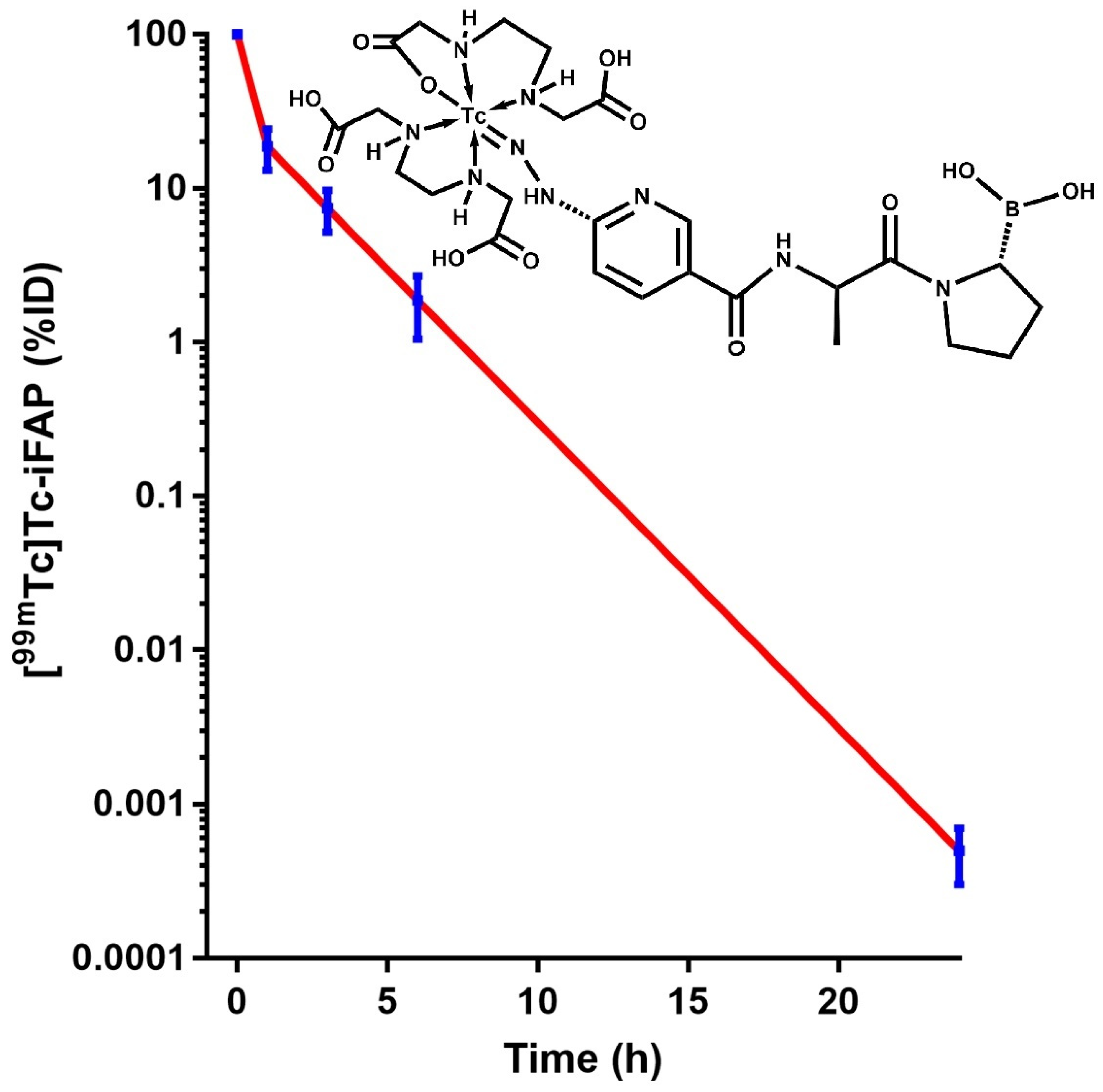
2.1. Biokinetics and Dosimetry
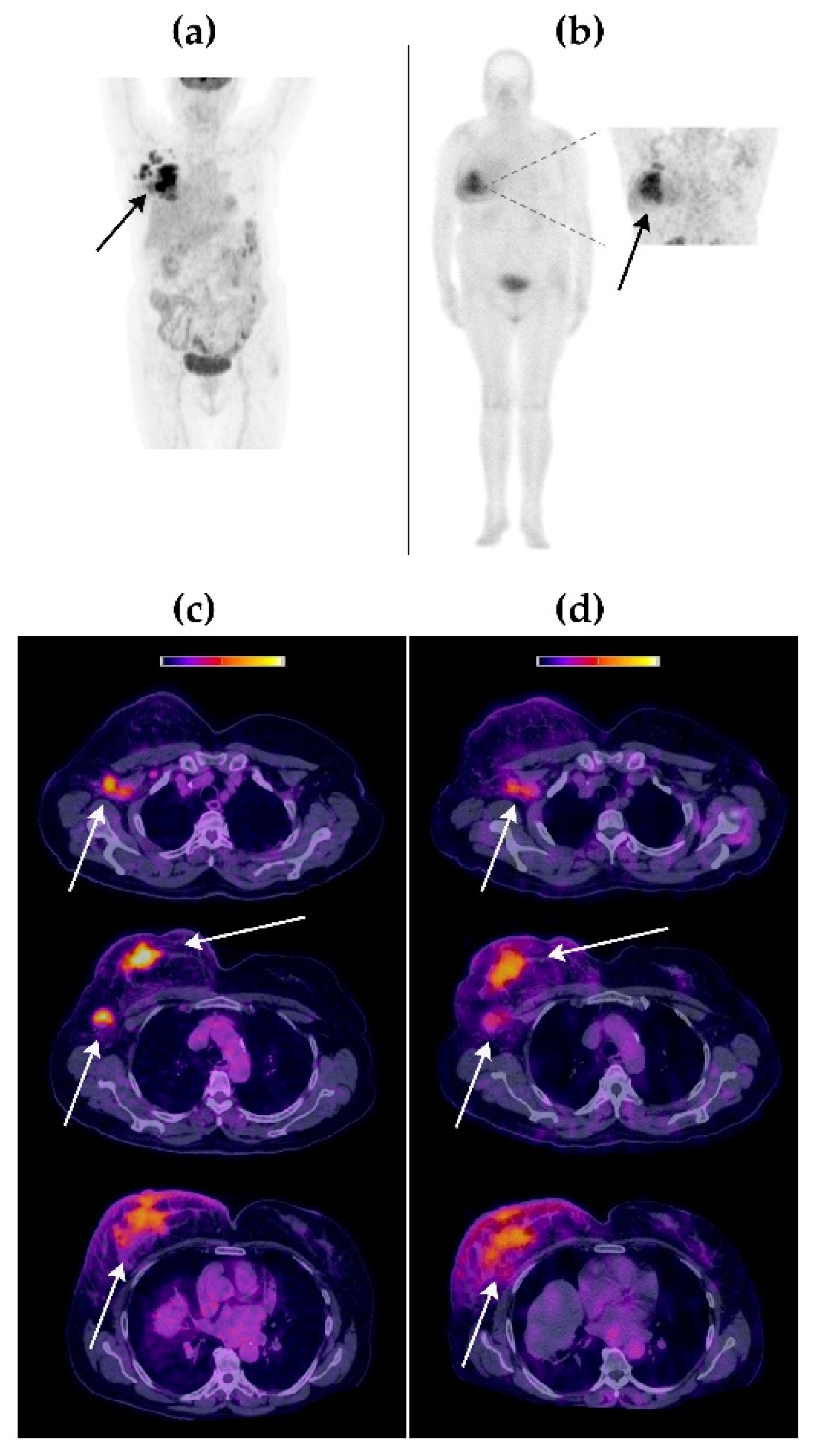
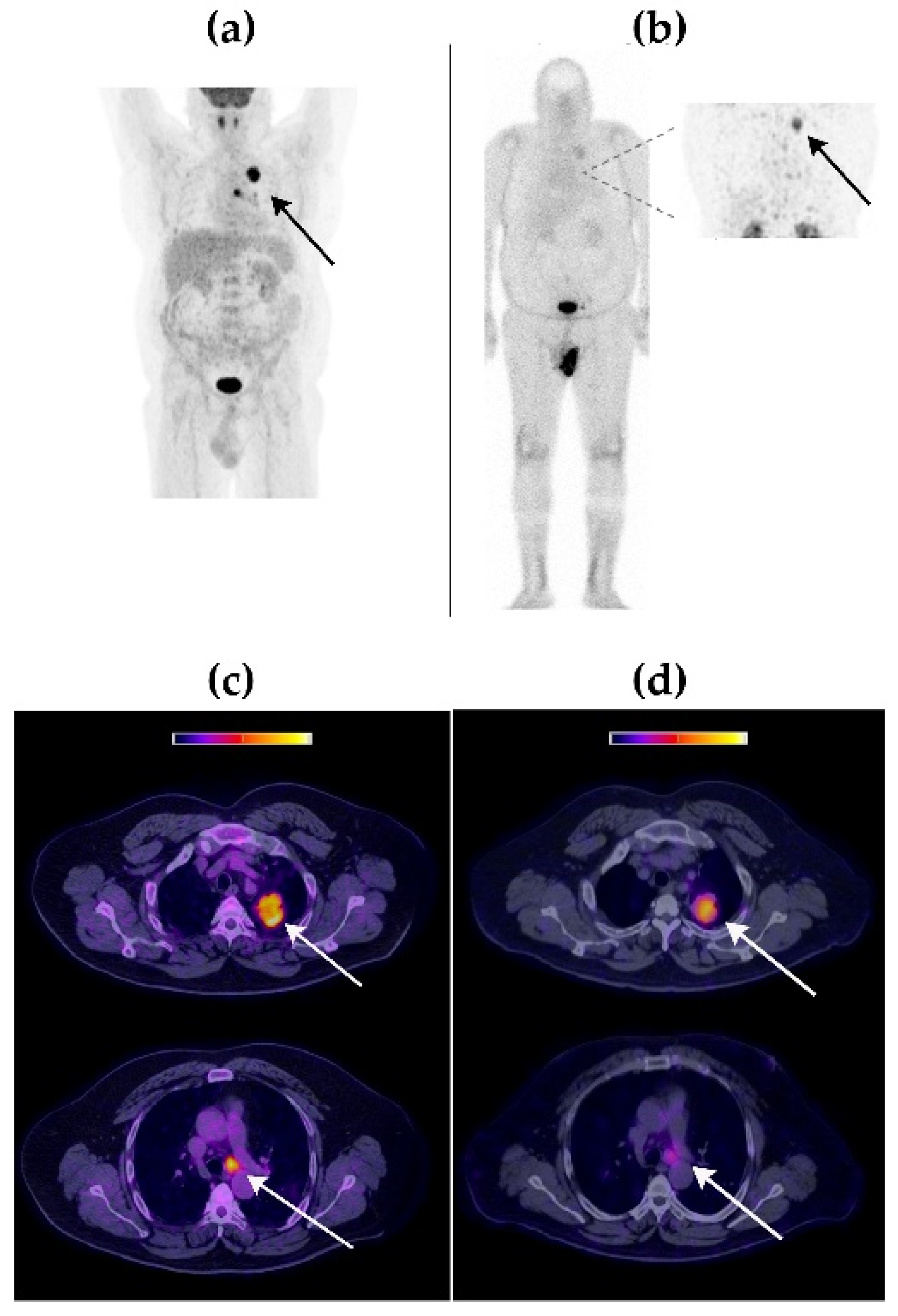
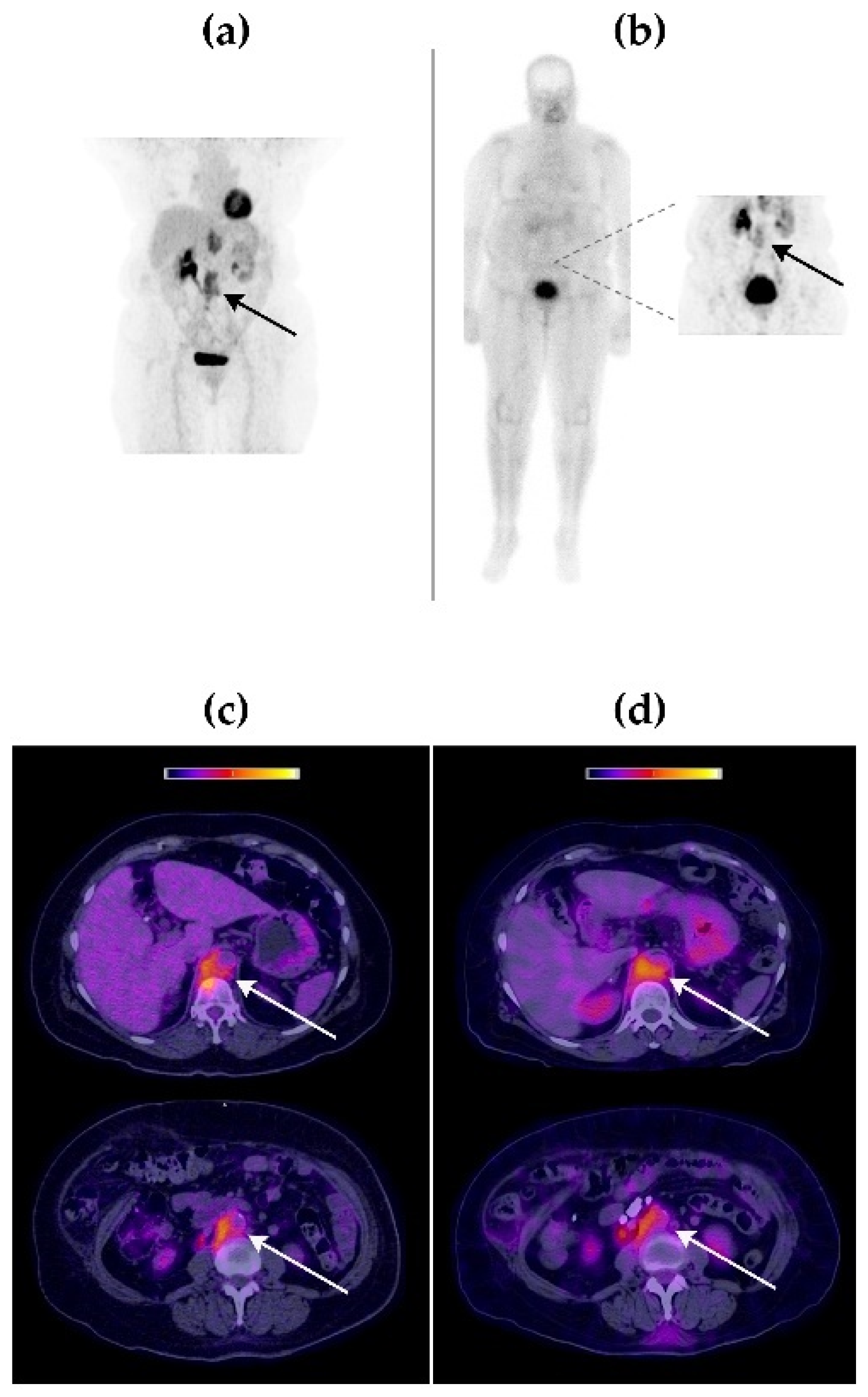
2.2. [99mTc]Tc-iFAP Tumor Imaging in Patients
3. Discussion
4. Materials and Methods
4.1. Reagents
4.2. [99mTc]Tc-iFAP Preparation
4.3. Volunteers and Patients
4.4. Image Acquisition
4.5. Image Analysis
4.6. Biokinetics and Dosimetry
4.7. Tumor Tissue Samples
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hamson, E.; JcKeane, F.M.; Tholen, S.; Schilling, O.; Gorrell, M.D. Understanding fibroblast activation protein (FAP): Substrates, activities, expression and targeting for cancer therapy. Proteom. Clin. Appl. 2014, 8, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Nurmik, M.; Ullmann, P.; Rodriguez, F.; Haan, S.; Letellier, E. In search of definitions: Cancer-associated fibroblasts and their markers. Int. J. Cancer 2020, 146, 895–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arneth, B. Tumor Microenvironment. Medicina 2020, 56, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindner, T.; Loktev, A.; Altmann, A.; Giesel, F.; Kratochwil, C.; Debus, J.; Jäger, D.; Mier, W.; Haberkorn, U. Development of quinoline-based theranostic ligands for the targeting of fibroblast activation protein. J. Nucl. Med. 2018, 59, 1415–1422. [Google Scholar] [CrossRef] [Green Version]
- Loktev, A.; Lindner, T.; Mier, W.; Debus, J.; Altmann, A.; Jäger, D.; Giesel, F.; Kratochwil, C.; Barthe, P.; Roumestand, C.; et al. A tumor-imaging method targeting cancer-associated fibroblasts. J. Nucl. Med. 2018, 59, 1423–1429. [Google Scholar] [CrossRef]
- Loktev, A.; Lindner, T.; Burger, E.-M.; Altmann, A.; Giesel, F.; Kratochwil, C.; Debus, J.; Marmé, F.; Jäger, D.; Mier, W.; et al. Development of Fibroblast Activation Protein-Targeted Radiotracers with Improved Tumor Retention. J. Nucl. Med. 2019, 60, 1421–1429. [Google Scholar] [CrossRef]
- Kratochwil, C.; Flechsig, P.; Lindner, T.; Abderrahim, L.; Altmann, A.; Mier, W.; Adeberg, S.; Rathke, H.; Röhrich, M.; Winter, H.; et al. 68Ga-FAPI PET/CT: Tracer Uptake in 28 Different Kinds of Cancer. J. Nucl. Med. 2019, 60, 801–805. [Google Scholar] [CrossRef] [Green Version]
- Giesel, F.L.; Adeberg, S.; Syed, M.; Lindner, T.; Jiménez-Franco, L.D.; Mavriopoulou, E.; Staudinger, F.; Tonndorf-Martini, E.; Regnery, S.; Rieken, S.; et al. FAPI-74 PET/CT Using Either 18F-AlF or Cold-Kit 68Ga Labeling: Biodistribution, Radiation Dosimetry, and Tumor Delineation in Lung Cancer Patients. J. Nucl. Med. 2021, 62, 201–207. [Google Scholar] [CrossRef]
- Ferdinandus, J.; Fragoso Costa, P.; Kessler, L.; Weber, M.; Hirmas, N.; Kostbade, K.; Bauer, S.; Schuler, M.; Ahrens, M.; Schildhaus, H.U.; et al. Initial clinical experience with 90Y-FAPI-46 radioligand therapy for advanced stage solid tumors: A case series of nine patients. J. Nucl. Med. 2022, 63, 727–734. [Google Scholar] [CrossRef]
- Watabe, T.; Liu, Y.; Kaneda-Nakashima, K.; Shirakami, Y.; Lindner, T.; Ooe, K.; Toyoshima, A.; Nagata, K.; Shimosegawa, E.; Haberkorn, U.; et al. Theranostics Targeting Fibroblast Activation Protein in the Tumor Stroma: 64Cu- and 225Ac-Labeled FAPI-04 in Pancreatic Cancer Xenograft Mouse Models. J. Nucl. Med. 2020, 61, 563–569. [Google Scholar] [CrossRef]
- Lindner, T.; Altmann, A.; Krämer, S.; Kleist, C.; Loktev, A.; Kratochwil, C.; Giesel, F.; Mier, W.; Marme, F.; Debus, J.; et al. Design and Development of 99mTc-Labeled FAPI Tracers for SPECT Imaging and 188Re Therapy. J. Nucl. Med. 2020, 61, 1507–1513. [Google Scholar] [CrossRef]
- Liu, Y.; Watabe, T.; Kaneda-Nakashima, K.; Shirakami, Y.; Naka, S.; Ooe, K.; Toyoshima, A.; Nagata, K.; Haberkorn, U.; Kratochwil, C.; et al. Fibroblast activation protein targeted therapy using [177Lu]FAPI-46 compared with [225Ac]FAPI-46 in a pancreatic cancer model. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 871–880. [Google Scholar] [CrossRef]
- Ballal, S.; Yadav, M.P.; Moon, E.S.; Kramer, V.S.; Roesch, F.; Kumari, S.; Bal, C. First-In-Human Results on the Biodistribution, Pharmacokinetics, and Dosimetry of [177Lu]Lu-DOTA.SA.FAPi and [177Lu]Lu-DOTAGA.(SA.FAPi)2. Pharmaceuticals 2021, 14, 1212. [Google Scholar] [CrossRef]
- Lan, L.; Liu, H.; Wang, Y.; Deng, J.; Peng, D.; Feng, Y.; Wang, L.; Chen, Y.; Qiu, L. The potential utility of [68Ga]Ga-DOTA-FAPI-04 as a novel broad-spectrum oncological and non-oncological imaging agent-comparison with [18F]FDG. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 963–979. [Google Scholar] [CrossRef]
- Pang, Y.; Zhao, L.; Luo, Z.; Hao, B.; Wu, H.; Lin, Q.; Sun, L.; Chen, H. Comparison of 68Ga-FAPI and 18F-FDG Uptake in Gastric, Duodenal, and Colorectal Cancers. Radiology 2021, 298, 393–402. [Google Scholar] [CrossRef]
- Chen, H.; Pang, Y.; Wu, J.; Zhao, L.; Hao, B.; Wu, J.; Wei, J.; Wu, S.; Zhao, L.; Luo, Z.; et al. Comparison of [68Ga]Ga-DOTA-FAPI-04 and [18F] FDG PET/CT for the diagnosis of primary and metastatic lesions in patients with various types of cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1820–1832. [Google Scholar] [CrossRef]
- Guo, W.; Pang, Y.; Yao, L.; Zhao, L.; Fan, C.; Ke, J.; Guo, P.; Hao, B.; Fu, H.; Xie, C.; et al. Imaging fibroblast activation protein in liver cancer: A single-center post hoc retrospective analysis to compare [68Ga]Ga-FAPI-04 PET/CT versus MRI and [18F]-FDG PET/CT. Eur. J. Nucl Med. Mol. Imaging 2021, 48, 1604–1617. [Google Scholar] [CrossRef]
- Luo, Y.; Pan, Q.; Yang, H.; Peng, L.; Zhang, W.; Li, F. Fibroblast Activation Protein-Targeted PET/CT with 68Ga-FAPI for Imaging IgG4-Related Disease: Comparison to 18F-FDG PET/CT. J. Nucl. Med. 2021, 62, 266–271. [Google Scholar] [CrossRef]
- Trujillo-Benítez, D.; Luna-Gutiérrez, M.; Ferro-Flores, G.; Ocampo-García, B.; Santos-Cuevas, C.; Bravo-Villegas, G.; Morales-Ávila, E.; Cruz-Nova, P.; Díaz-Nieto, L.; García-Quiroz, J.; et al. Design, Synthesis and Preclinical Assessment of 99mTc-iFAP for In Vivo Fibroblast Activation Protein (FAP) Imaging. Molecules 2022, 27, 264. [Google Scholar] [CrossRef]
- World Health Organization. Technical Report Series 611: Use of Ionizing Radiation and Radionuclides on Human Beings from Medical Research, Training, and Nonmedical Purposes—Report of a World Health Organization, Expert Committee: World Health Organization, Geneva, Switzerland. 1977. Available online: https://apps.who.int/iris/bitstream/handle/10665/41256/WHO_TRS_611.pdf?sequence=1&isAllowed=y (accessed on 6 April 2022).
- United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) 1993 Report: Sources, Effects and Risks of Ionizing Radiation. Report to the General Assembly, with Scientific Annexes. Available online: https://www.unscear.org/unscear/en/publications/1993.html (accessed on 6 April 2022).
- United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) 1994 Report: Sources, Effects and Risks of Ionizing Radiation. Report to the General Assembly, with Scientific Annexes. Available online: https://www.unscear.org/unscear/en/publications/1994.html (accessed on 6 April 2022).
- Luna-Gutiérrez, M.; Ocampo-García, B.; Jiménez-Mancilla, N.; Ancira-Cortez, A.; Trujillo-Benítez, D.; Hernández-Jiménez, T.; Ramírez-Nava, G.; Hernández-Ramírez, R.; Santos-Cuevas, C.; Ferro-Flores, G. Targeted Endoradiotherapy with Lu2O3-iPSMA/-iFAP Nanoparticles Activated by Neutron Irradiation: Preclinical Evaluation and First Patient Image. Pharmaceutics 2022, 14, 720. [Google Scholar] [CrossRef]
- Afshar-Oromieh, A.; Hetzheim, H.; Kratochwil, C.; Benesova, M.; Eder, M.; Neels, O.C.; Eisenhut, M.; Kübler, W.; Holland-Letz, T.; Giesel, F.L.; et al. The Theranostic PSMA Ligand PSMA-617 in the Diagnosis of Prostate Cancer by PET/CT: Biodistribution in Humans, Radiation Dosimetry, and First Evaluation of Tumor Lesions. J. Nucl. Med. 2015, 56, 1697–1705. [Google Scholar] [CrossRef] [Green Version]
- Gabriel, M.; Decristoforo, C.; Kendler, D.; Dobrozemsky, G.; Heute, D.; Uprimny, C.; Kovacs, P.; Von Guggenberg, E.; Bale, R.; Virgolini, I.J. 68Ga-DOTA-Tyr3-octreotide PET in neuroendocrine tumors: Comparison with somatostatin receptor scintigraphy and CT. J. Nucl. Med. 2007, 48, 508–518. [Google Scholar] [CrossRef]
- International Commission on Radiological Protection (ICRP). Basic anatomical and physiological data for use in radiological protection: Reference values: ICRP publication 89. Ann. ICRP 2002, 32, 1–277. [Google Scholar]
- Ramírez-Nava, G.; Santos-Cuevas, C.; Ferro-Flores, G.; Ocampo-García, B.; Chairez, I.; Gómez-Argumosa, E.; Abundiz-López, L.; García-Pérez, F.O. Hybrid (2D/3D) Dosimetry of Radiolabeled Gold Nanoparticles for Sentinel Lymph Node Detection in Patients with Breast Cancer. Contrast Media Mol. Imaging 2020, 2020, 2728134. [Google Scholar] [CrossRef]
- Stabin, M.G.; Sparks, R.B.; Crowe, E. OLINDA/EXM: The second-generation personal computer software for internal dose assessment in nuclear medicine. J. Nucl. Med. 2005, 46, 1023–1027. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organ | Biokinetic Model | |
|---|---|---|
| Liver | R2 = 0.99 | 1.11 × 10−1 ± 1.74 × 10−2 |
| Kidneys | R2 = 1 | 1.22 × 10−1 ± 7.69 × 10−2 |
| Urinary bladder | R2 = 0.99 | 5.02 × 10−1 ± 1.23 × 10−1 |
| Remainder of the body | R2 = 0.99 | 3.04 ± 0.37 |
| Target Organ | Equivalent Doses (mSv/MBq) (Mean ± SD) |
|---|---|
| Adrenals | (2.23 ± 0.35) × 10−3 |
| Brain | (1.36 ± 0.21) × 10−3 |
| Breast | (1.14 ± 0.18) × 10−3 |
| Gallbladder Wall | (2.30 ± 0.36) × 10−3 |
| LLI Wall | (2.99 ± 0.45) × 10−3 |
| Small Intestine | (2.48 ± 0.37) × 10−3 |
| Stomach Wall | (1.93 ± 0.30) × 10−3 |
| ULI Wall | (2.31 ± 0.36) × 10−3 |
| Heart Wall | (1.87 ± 0.29) × 10−3 |
| Kidneys | (7.01 ± 1.09) × 10−3 |
| Liver | (2.23 ± 0.35) × 10−3 |
| Lungs | (1.63 ± 0.26) × 10−3 |
| Muscle | (1.74 ± 0.27) × 10−3 |
| Ovaries | (3.02 ± 0.47) × 10−3 |
| Pancreas | (2.27 ± 0.35) × 10−3 |
| Red Marrow | (1.73 ± 0.29) × 10−3 |
| Skin | (1.11 ± 0.17) × 10−3 |
| Spleen | (2.02 ± 0.32) × 10−3 |
| Testes | (2.10 ± 0.33) × 10−3 |
| Thymus | (1.62 ± 0.25) × 10−3 |
| Thyroid | (1.64 ± 0.25) × 10−3 |
| Urinary Bladder Wall | (2.15 ± 0.34) × 10−3 |
| Uterus | (4.27 ± 0.67) × 10−3 |
| Effective Dose (mSv/MBq) | (3.12 ± 0.49) × 10−3 |
| No. | Age (Years) | Gender | Clinical Status | Type of Cancer | Extent of Cancer |
|---|---|---|---|---|---|
| 1 | 70 | Female | Initial assessment | Breast cancer (ductal carcinoma; SBR 8, G3, moderate DR, Ki67 70%). Triple-negative. | Primary, lymph node |
| 2 | 51 | Male | Initial assessment | Lung cancer, NSCLC (adenocarcinoma). | Primary, lymph node |
| 3 | 66 | Female | Recurrence | Cervical cancer (squamous cell carcinoma). | Lymph node |
| Primary Tumors | |||||
|---|---|---|---|---|---|
| Type of Cancer (No. of Patients) | Tracer | T/Bm | T/Bl | T/Bp | T/Bc |
| Breast (1) | [99mTc]Tc-iFAP | 3.7 | 3.3 | 4.1 | 3.1 |
| [18F]FDG | 4.2 | 2.9 | 7.4 | 8.3 | |
| Lung (2) | [99mTc]Tc-iFAP | 8.8 | 5.3 | 10.2 | 7.6 |
| [18F]FDG | 4.4 | 2.9 | 8.1 | 10.9 | |
| Cervical (3) | [99mTc]Tc-iFAP | n.a. | n.a. | n.a. | n.a. |
| [18F]FDG | n.a. | n.a. | n.a. | n.a. | |
| Average (1–3) | [99mTc]Tc-iFAP | 6.3 ± 3.6 | 4.3 ± 1.4 | 7.2 ± 4.3 | 5.4 ± 3.2 |
| [18F]FDG | 4.3 ± 0.1 | 2.9 ± 0.0 | 7.8 ± 0.5 | 9.6 ± 1.8 | |
| Lymph Node Metastases | |||||
| Breast (1) | [99mTc]Tc-iFAP | 2.2 | 2.0 | 2.5 | 1.9 |
| [18F]FDG | 2.8 | 2.0 | 5.0 | 5.7 | |
| Lung (2) | [99mTc]Tc-iFAP | 2.2 | 1.3 | 2.6 | 1.9 |
| [18F]FDG | 3.6 | 2.4 | 6.7 | 9.1 | |
| Cervical (3) | [99mTc]Tc-iFAP | 8.3 | 2.7 | 7.8 | 8.4 |
| [18F]FDG | 4.2 | 2.1 | 7.2 | 6.3 | |
| Average (1–3) | [99mTc]Tc-iFAP | 4.2 ± 3.5 | 2.0 ± 0.7 | 4.3 ± 3.0 | 4.1 ± 3.8 |
| [18F]FDG | 3.5 ± 0.7 | 2.2 ± 0.2 | 6.3 ± 1.2 | 7.0 ± 1.8 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coria-Domínguez, L.; Vallejo-Armenta, P.; Luna-Gutiérrez, M.; Ocampo-García, B.; Gibbens-Bandala, B.; García-Pérez, F.; Ramírez-Nava, G.; Santos-Cuevas, C.; Ferro-Flores, G. [99mTc]Tc-iFAP Radioligand for SPECT/CT Imaging of the Tumor Microenvironment: Kinetics, Radiation Dosimetry, and Imaging in Patients. Pharmaceuticals 2022, 15, 590. https://doi.org/10.3390/ph15050590
Coria-Domínguez L, Vallejo-Armenta P, Luna-Gutiérrez M, Ocampo-García B, Gibbens-Bandala B, García-Pérez F, Ramírez-Nava G, Santos-Cuevas C, Ferro-Flores G. [99mTc]Tc-iFAP Radioligand for SPECT/CT Imaging of the Tumor Microenvironment: Kinetics, Radiation Dosimetry, and Imaging in Patients. Pharmaceuticals. 2022; 15(5):590. https://doi.org/10.3390/ph15050590
Chicago/Turabian StyleCoria-Domínguez, Luis, Paola Vallejo-Armenta, Myrna Luna-Gutiérrez, Blanca Ocampo-García, Brenda Gibbens-Bandala, Francisco García-Pérez, Gerardo Ramírez-Nava, Clara Santos-Cuevas, and Guillermina Ferro-Flores. 2022. "[99mTc]Tc-iFAP Radioligand for SPECT/CT Imaging of the Tumor Microenvironment: Kinetics, Radiation Dosimetry, and Imaging in Patients" Pharmaceuticals 15, no. 5: 590. https://doi.org/10.3390/ph15050590
APA StyleCoria-Domínguez, L., Vallejo-Armenta, P., Luna-Gutiérrez, M., Ocampo-García, B., Gibbens-Bandala, B., García-Pérez, F., Ramírez-Nava, G., Santos-Cuevas, C., & Ferro-Flores, G. (2022). [99mTc]Tc-iFAP Radioligand for SPECT/CT Imaging of the Tumor Microenvironment: Kinetics, Radiation Dosimetry, and Imaging in Patients. Pharmaceuticals, 15(5), 590. https://doi.org/10.3390/ph15050590