
Good Response of Advanced Thymic Carcinoma with Low PD-L1 Expression to Chemotherapy plus Pembrolizumab as First-Line Therapy and to Pembrolizumab as Maintenance Therapy: A Case Report


 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
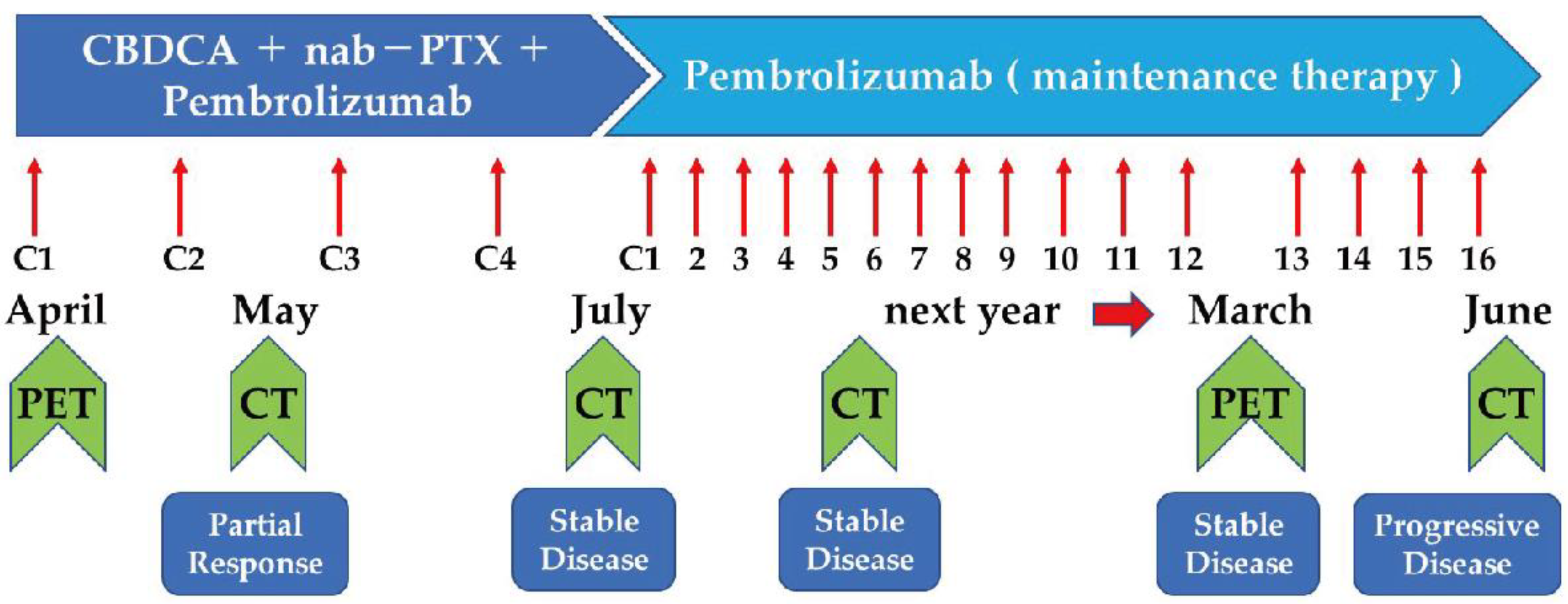
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Engels, E.A. Epidemiology of Thymoma and Associated Malignancies. J. Thorac. Oncol. 2010, 5, S260–S265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litvak, A.M.; Woo, K.; Hayes, S.; Huang, J.; Rimner, A.; Sima, C.S.; Moreira, A.L.; Tsukazan, M.; Riely, G.J. Clinical Characteristics and Outcomes for Patients with Thymic Carcinoma: Evaluation of Masaoka Staging. J. Thorac. Oncol. 2014, 9, 1810–1815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agatsuma, T.; Koizumi, T.; Kanda, S.; Ito, M.; Urushihata, K.; Yamamoto, H.; Hanaoka, M.; Kubo, K. Combination Chemotherapy with Doxorubicin, Vincristine, Cyclophosphamide, and Platinum Compounds for Advanced Thymic Carcinoma. J. Thorac. Oncol. 2011, 6, 2130–2134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirai, F.; Yamanaka, T.; Taguchi, K.; Daga, H.; Ono, A.; Tanaka, K.; Kogure, Y.; Shimizu, J.; Kimura, T.; Fukuoka, J.; et al. A multicenter phase II study of carboplatin and paclitaxel for advanced thymic carcinoma: WJOG4207L. Ann. Oncol. 2014, 26, 363–368. [Google Scholar] [CrossRef] [PubMed]
- du Vignaux, C.M.; Dansin, E.; Mhanna, L.; Greillier, L.; Pichon, E.; Kerjouan, M.; Clément-Duchêne, C.; Mennecier, B.; Westeel, V.; Robert, M.; et al. Systemic Therapy in Advanced Thymic Epithelial Tumors: Insights from the RYTHMIC Prospective Cohort. J. Thorac. Oncol. 2018, 13, 1762–1770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giaccone, G.; Kim, C.; Thompson, J.; McGuire, C.; Kallakury, B.; Chahine, J.J.; Manning, M.; Mogg, R.; Blumenschein, W.M.; Tan, M.T.; et al. Pembrolizumab in patients with thymic carcinoma: A single-arm, single-centre, phase 2 study. Lancet Oncol. 2018, 19, 347–355. [Google Scholar] [CrossRef]
- Katsuya, Y.; Fujita, Y.; Horinouchi, H.; Ohe, Y.; Watanabe, S.-I.; Tsuta, K. Immunohistochemical status of PD-L1 in thymoma and thymic carcinoma. Lung Cancer 2015, 88, 154–159. [Google Scholar] [CrossRef]
- Weissferdt, A.; Moran, C.A. Thymic Carcinoma, Part 1. Am. J. Clin. Pathol. 2012, 138, 103–114. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Gaspar, L.E.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: Cham, Switzerland; American Joint Commission on Cancer: Chicago, IL, USA, 2017. [Google Scholar]
- Sato, J.; Satouchi, M.; Itoh, S.; Okuma, Y.; Niho, S.; Mizugaki, H.; Murakami, H.; Fujisaka, Y.; Kozuki, T.; Nakamura, K.; et al. Lenvatinib in patients with advanced or metastatic thymic carcinoma (REMORA): A multicentre, phase 2 trial. Lancet Oncol. 2020, 21, 843–850. [Google Scholar] [CrossRef]
- Remon, J.; Girard, N.; Novello, S.; de Castro, J.; Bigay-Game, L.; Bernabé, R.; Greillier, L.; Mosquera, J.; Cousin, S.; Juan, O.; et al. PECATI: A Multicentric, Open-Label, Single-Arm Phase II Study to Evaluate the Efficacy and Safety of Pembrolizumab and Lenvatinib in Pretreated B3-Thymoma and Thymic Carcinoma Patients. Clin. Lung Cancer 2021, 23, e243–e246. [Google Scholar] [CrossRef] [PubMed]
- Cafaro, A.; Bongiovanni, A.; Di Iorio, V.; Oboldi, D.; Masini, C.; Ibrahim, T. Pembrolizumab in a Patient with Heavily Pre-Treated Squamous Cell Thymic Carcinoma and Cardiac Impairment: A Case Report and Literature Review. Front. Oncol. 2020, 10, 1478. [Google Scholar] [CrossRef] [PubMed]
- Wong-Chong, J.; Bernadach, M.; Ginzac, A.; Veyssière, H.; Durando, X. Pembrolizumab as a novel therapeutic option for patients with refractory thymic epithelial tumor: A case report. World J. Clin. Cases 2021, 9, 1139–1147. [Google Scholar] [CrossRef]
- Socinski, M.A.; Bondarenko, I.; Karaseva, N.A.; Makhson, A.M.; Vynnychenko, I.; Okamoto, I.; Hon, J.K.; Hirsh, V.; Bhar, P.; Zhang, H.; et al. Weekly nab-Paclitaxel in Combination with Carboplatin Versus Solvent-Based Paclitaxel Plus Carboplatin as First-Line Therapy in Patients With Advanced Non–Small-Cell Lung Cancer: Final Results of a Phase III Trial. J. Clin. Oncol. 2012, 30, 2055–2062. [Google Scholar] [CrossRef] [Green Version]
- Araya, T.; Kita, T.; Matsuoka, H.; Sakai, T.; Kimura, H.; Kasahara, K. Successful Treatment of Advanced Thymic Carcinoma with Carboplatin plus nab-Paclitaxel and Maintenance Monotherapy with nab-Paclitaxel: Two Case Reports. Case Rep. Oncol. 2020, 13, 1506–1512. [Google Scholar] [CrossRef] [PubMed]
- Giaccone, G.; Kim, C. Durable Response in Patients with Thymic Carcinoma Treated with Pembrolizumab after Prolonged Follow-Up. J. Thorac. Oncol. 2020, 16, 483–485. [Google Scholar] [CrossRef] [PubMed]
- Thomas, Q.D.; Basse, C.; Luporsi, M.; Girard, N. Pembrolizumab Plus Chemotherapy in Metastatic Thymic Carcinoma: A Case Report. Front. Oncol. 2021, 11, 814544. [Google Scholar] [CrossRef]
- Nakagawa, K.; Matsuno, Y.; Kunitoh, H.; Maeshima, A.; Asamura, H.; Tsuchiya, R. Immunohistochemical KIT (CD117) Expression in Thymic Epithelial Tumors. Chest 2005, 128, 140–144. [Google Scholar] [CrossRef]
- Mok, T.S.K.; Wu, Y.-L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Cho, J.; Kim, H.S.; Ku, B.M.; Choi, Y.-L.; Cristescu, R.; Han, J.; Sun, J.-M.; Lee, S.-H.; Ahn, J.S.; Park, K.; et al. Pembrolizumab for Patients with Refractory or Relapsed Thymic Epithelial Tumor: An Open-Label Phase II Trial. J. Clin. Oncol. 2019, 37, 2162–2170. [Google Scholar] [CrossRef]
- Katsuya, Y.; Horinouchi, H.; Seto, T.; Umemura, S.; Hosomi, Y.; Satouchi, M.; Nishio, M.; Kozuki, T.; Hida, T.; Sukigara, T.; et al. Single-arm, multicentre, phase II trial of nivolumab for unresectable or recurrent thymic carcinoma: PRIMER study. Eur. J. Cancer 2019, 113, 78–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishii, Y.; Furuhashi, K.; Ito, K.; Sakaguchi, T.; Suzuki, Y.; Fujiwara, K.; Yasuma, T.; Kobayashi, T.; D’Alessandro-Gabazza, C.N.; Gabazza, E.C.; et al. Good Response of Advanced Thymic Carcinoma with Low PD-L1 Expression to Chemotherapy plus Pembrolizumab as First-Line Therapy and to Pembrolizumab as Maintenance Therapy: A Case Report. Pharmaceuticals 2022, 15, 889. https://doi.org/10.3390/ph15070889
Nishii Y, Furuhashi K, Ito K, Sakaguchi T, Suzuki Y, Fujiwara K, Yasuma T, Kobayashi T, D’Alessandro-Gabazza CN, Gabazza EC, et al. Good Response of Advanced Thymic Carcinoma with Low PD-L1 Expression to Chemotherapy plus Pembrolizumab as First-Line Therapy and to Pembrolizumab as Maintenance Therapy: A Case Report. Pharmaceuticals. 2022; 15(7):889. https://doi.org/10.3390/ph15070889
Chicago/Turabian StyleNishii, Yoichi, Kazuki Furuhashi, Kentaro Ito, Tadashi Sakaguchi, Yuta Suzuki, Kentaro Fujiwara, Taro Yasuma, Tetsu Kobayashi, Corina N. D’Alessandro-Gabazza, Esteban C. Gabazza, and et al. 2022. "Good Response of Advanced Thymic Carcinoma with Low PD-L1 Expression to Chemotherapy plus Pembrolizumab as First-Line Therapy and to Pembrolizumab as Maintenance Therapy: A Case Report" Pharmaceuticals 15, no. 7: 889. https://doi.org/10.3390/ph15070889
APA StyleNishii, Y., Furuhashi, K., Ito, K., Sakaguchi, T., Suzuki, Y., Fujiwara, K., Yasuma, T., Kobayashi, T., D’Alessandro-Gabazza, C. N., Gabazza, E. C., Taguchi, O., & Hataji, O. (2022). Good Response of Advanced Thymic Carcinoma with Low PD-L1 Expression to Chemotherapy plus Pembrolizumab as First-Line Therapy and to Pembrolizumab as Maintenance Therapy: A Case Report. Pharmaceuticals, 15(7), 889. https://doi.org/10.3390/ph15070889